Back to Journals » Journal of Asthma and Allergy » Volume 15
Residual Dyspnea May Predict Small Airways Dysfunction and Poor Responsiveness to Single-Inhaler Triple Therapy in Asthmatic Patients
Authors Ito K ![]() , Tajiri T
, Tajiri T ![]() , Nishiyama H, Kurokawa R, Yap JMG, Takeda N, Fukumitsu K, Kanemitsu Y
, Nishiyama H, Kurokawa R, Yap JMG, Takeda N, Fukumitsu K, Kanemitsu Y ![]() , Fukuda S, Uemura T, Ohkubo H, Maeno K, Ito Y
, Fukuda S, Uemura T, Ohkubo H, Maeno K, Ito Y ![]() , Oguri T, Takemura M, Niimi A
, Oguri T, Takemura M, Niimi A ![]()
Received 11 July 2022
Accepted for publication 28 October 2022
Published 2 November 2022 Volume 2022:15 Pages 1561—1568
DOI https://doi.org/10.2147/JAA.S381953
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
Keima Ito,1 Tomoko Tajiri,1 Hirono Nishiyama,1 Ryota Kurokawa,1 Jenifer Maries Go Yap,1 Norihisa Takeda,1 Kensuke Fukumitsu,1 Yoshihiro Kanemitsu,1 Satoshi Fukuda,1 Takehiro Uemura,1 Hirotsugu Ohkubo,1 Ken Maeno,1 Yutaka Ito,1 Tetsuya Oguri,1,2 Masaya Takemura,1,2 Akio Niimi1
1Department of Respiratory Medicine, Allergy and Clinical Immunology, Nagoya City University Graduate School of Medical Sciences, Nagoya, Japan; 2Department of Education and Research Center for Community Medicine, Nagoya City University Graduate School of Medical Sciences, Nagoya, Japan
Correspondence: Tomoko Tajiri, Email [email protected]
Purpose: Recently, single-inhaler triple therapy (SITT) has demonstrated efficacy in patients with uncontrolled asthma who were symptomatic despite treatment with inhaled corticosteroids/long-acting β 2 agonists. However, the characteristics of patients who benefit from SITT remain unclear in the real-world. The aim of this study was to examine the predictors of responsiveness to SITT in patients with asthma.
Patients and Methods: A total of 45 patients with asthma who had regularly visited our respiratory clinic and were started on SITT from March 2019 to March 2021 were retrospectively analyzed. Patients’ demographic characteristics, residual respiratory symptoms, type 2 biomarkers, and lung function before SITT were assessed from the patients’ medical records. Predictors of responsiveness to four-week SITT were evaluated in these patients. The definition of responders was based on the physician-assessed global evaluation of treatment effectiveness.
Results: Thirty-four (75%) of 45 patients were identified as responders to SITT. Non-responders showed significantly lower forced vital capacity (FVC) (%predicted) values, and complained of dyspnea more frequently than responders before SITT (p = 0.01 and p = 0.02, respectively). There were no significant differences in demographic characteristics and type 2 biomarkers between responders and non-responders. Clinical predictors of poor response to SITT were residual dyspnea (OR = 0.14, p = 0.02), low FVC (%predicted) values (OR = 1.05, p = 0.01), and FVC (%predicted) < 80% (OR = 0.11, p = 0.02). Multivariate analysis showed that poor response to SITT was associated with residual dyspnea before SITT (OR = 0.14, p = 0.02). On the other hand, patients with residual dyspnea had significantly lower FEF25– 75 (%predicted) values than patients without residual dyspnea before SITT (p = 0.04).
Conclusion: Residual dyspnea, reflecting small airways dysfunction, may predict poor responsiveness to short-term SITT in patients with asthma.
Keywords: single-inhaler triple therapy, long-acting muscarinic antagonists, asthma, small airways dysfunction, dyspnea
Introduction
Asthma is primarily characterized by chronic inflammation of the airways. It presents with clinical symptoms such as wheezing, cough, and dyspnea, with variability due to increased airway hyperresponsiveness and airway contraction accompanied by airway remodeling.1 Treatment with inhaled corticosteroids (ICSs) and long-acting β2 agonists (LABAs) improves asthma control and mortality. However, a recent report from Japan showed that 76% of patients with asthma do not have adequate disease control despite treatment with ICSs or ICSs/LABAs.2
Long-acting muscarinic antagonists (LAMAs) have long been widely used as a treatment for chronic obstructive pulmonary disease (COPD), but they have also been shown to be effective in asthma. The effectiveness of adding LAMAs in patients with residual asthma symptoms to treatment with low to medium dose ICSs has been shown, which was equivalent to the efficacy of adding LABAs.3–5 Furthermore, several clinical trials have shown the efficacy of adding LAMAs in patients with insufficiently controlled asthma to treatment with medium to high-dose ICSs and LABAs, which is expected to improve lung function and to reduce asthma exacerbations.6,7 Despite this, the prescription rate of tiotropium for asthma has been as low as 5% to 12% in Japan.2,8–10 LAMAs have not yet been widely used for the treatment of asthma. One reason for this may be due to reluctance to prescribe multiple inhalation devices, which may potentially be associated with poor medication adherence and lead to deterioration of asthma control.11
Recently, the effectiveness of ICS/LABA/LAMA combination therapy for asthma has been shown, and it is available for use in clinical practice.12,13 ICS/LABA/LAMA combination therapy is expected to improve adherence14 and to increase the use of LAMAs for asthma. Exploratory subgroup analyses of previous randomized, controlled trials (RCTs) showed that the effectiveness of add-on therapy with LAMA (tiotropium) to ICS was high in patients with high airway reversibility or airway obstruction,15 and was observed regardless of the type 2 phenotypes defined by the blood eosinophil counts, serum total/specific IgE levels, and fractional exhaled nitric oxide (FeNO) concentration.16–18 However, the characteristics of patients who benefit from ICS/LABA/LAMA combination therapy (single-inhaler triple therapy: SITT) remain unclear. Although post hoc analyses of TRIMARAN and TRIGGER studies reported that SITT was highly effective in patients with high airway reversibility19 or airway obstruction,20 in real-world clinical practice, the patient background is more diverse than that in RCTs, and patients with a smoking history or those with comorbid COPD are included. In this regard, there are only a limited number of reports examining the predictors of responsiveness to SITT specifically in real-world clinical practice. Since SITT will be increasingly started as first-line treatment of asthma, to identify the predictors of responsiveness to SITT is important to deliver SITT to patients with asthma appropriately.
The aim of this study was to assess the clinical characteristics of patients with asthma who were started on SITT in our hospital and to examine the predictors of responsiveness. We hypothesized that airway obstruction, which was previously reported in the RCTs, could be a predictor of responsiveness to SITT in these patients from the perspective of real-world clinical practice.
Materials and Methods
Subjects and Measurements
This was a retrospective, cohort study that analyzed the data of adult patients with asthma who had regularly visited our respiratory clinic and were newly started on SITT from March 2019 to March 2021 and continued SITT for at least four weeks. The indication for SITT was determined by the asthma specialists based on the latest Global Initiative for Asthma (GINA) at the time. Demographic characteristics, residual respiratory symptoms (cough, sputum, dyspnea), blood tests (blood eosinophil and neutrophil counts, serum total IgE levels, and serum specific IgE antibodies), FeNO levels and lung function [forced vital capacity (FVC), FEV1, forced expiratory flow between 25% and 75% of FVC (FEF25–75)] were assessed before SITT administration from the patients’ medical records. Next, these measurements were compared between patients who responded to four-weeks’ SITT and those who did not, to determine predictors of responsiveness to four-weeks’ SITT.
The definition of responder to treatment was based on the physician-assessed global evaluation of treatment effectiveness (GETE) at four weeks. In the GETE, treatment responsiveness was rated as excellent (complete control of asthma), good (marked improvement of asthma), moderate (discernible but limited improvement of asthma), poor (no appreciable change in asthma symptoms) or worsening.21 Patients with excellent, good, and moderate responses were considered responders according to the previous study.22 The determination of the presence or absence of residual respiratory symptoms and of responder or non-responder were performed independently by two respiratory specialists (KI and TT) to ensure that their results were consistent. If their evaluations did not agree, the determination was based on mutual consultation.
Procedure for Clinical Examinations
In our respiratory clinic, all patients with asthma regularly undergo a meticulous work-up in the morning. All participants underwent examinations including blood tests, FeNO measurement, and spirometry within six months before SITT administration. The presence of an atopic predisposition was defined as at least one serum specific IgE antibody against eight aeroallergens (house dust mite, Japanese cedar pollen, mixed Gramineae pollens (orchard grass, sweet vernal grass, Bermuda grass, Timothy grass and reeds), mixed weed pollens (ragweed, mugwort, goldenrod, dandelion and oxeye daisy), mixed molds (Penicillium, Cladosporium, Aspergillus, Candida, Alternaria), Trichophyton rubrum, and cat and dog dander (ImmunoCAP® total IgE and ImmunoCAP® specific IgE, Phadia K.K., Tokyo, Japan)) was positive (≥0.35 UA/mL). Spirometry was performed using the Chestac-8900 (Chest, Tokyo, Japan) adhering to the ERS/ATS guidelines.23 Patients were not withdrawn from asthma-related medications before spirometry. FeNO levels at an oral expiratory flow rate of 50 mL/s were measured using a Sievers NOA71 280i chemiluminescence analyzer (GE Analytical Instruments, Boulder, CO, USA).24
This study complying with the Declaration of Helsinki was approved by the Ethics Committee of Nagoya City University (60–21-0044). Written informed consent was waived by the ethics committee due to the retrospective nature of this study. Instead, an opt-out document was posted on the hospital website to offer patients the opportunity to refuse participation.
Statistical Analysis
Data obtained from patients were analyzed using JMP 14.2 software (SAS Institute Inc.). Data are shown as medians (25th percentile, 75th percentile). Categorical variables are presented as number (%). The Wilcoxon rank-sum test or Fisher’s exact test was used to compare the two patients’ groups: responders and non-responders. Multivariate logistic regression analysis was performed to identify factors contributing to responsiveness to four-week SITT. Variables with p < 0.10 on univariate analyses for pretreatment indices were included in the multivariate analysis. Nonnormally distributed data were log-transformed. Elderly (≥65 years), high body mass index (≥25 kg/m2), high blood eosinophil count (≥300/μL), and high FeNO (≥25 ppb) groups were defined on the basis of previous reports.24–27 Significance was set at p < 0.05.
Results
Patients’ Characteristics and Comparison of Responders and Non-Responders
Table 1 shows the demographic characteristics, residual respiratory symptoms, biomarkers, and lung function of all studied patients before SITT administration. The effectiveness of SITT was confirmed in 34 (75%) of 45 patients. The breakdown of the drugs of SITT was as follows: 23 patients used fluticasone furoate/umeclidinium/vilanterol (FF/UMEC/VI) 100/62.5/25 μg/day; 19 patients used budesonide/glycopyrrolate/formoterol fumarate (BUD/GLY/FF) 640/19.2/28.8 μg/day (160/4.8/7.2 μg two inhalations twice daily, only for patients with comorbid COPD); and 3 patients used mometasone furoate/glycopyrrolate/indacaterol (MF/GLY/IND) 160/50/150 μg/day. SITT was started to improve adherence in 11 patients taking ICSs/LABAs and tiotropium, to step-up treatment in 25 patients and for initial treatment in 9 patients. Residual respiratory symptoms before starting SITT were cough in 25 patients (56%), dyspnea in 22 patients (49%), and sputum in 7 patients (16%).
 |
Table 1 Characteristics of the Studied Patients and Comparison of Responders and Non-Responders |
Patients’ characteristics, biomarkers, and lung functions were compared between the responder and non-responder groups (Table 1). There were no significant differences in demographic characteristics (such as body mass index, smoking history, and disease duration), type 2 biomarkers (blood eosinophil counts, serum total IgE levels, FeNO levels), and blood neutrophil counts between the two groups. There was no significant difference in the proportion of patients who inhaled UMEC or GLY between the two groups. Non-responders complained of dyspnea more frequently (82% vs 38%, p = 0.02) than responders before SITT administration. In addition, non-responders showed significantly lower FVC (%predicted) values [110% (92.5% to 117.9%) vs 85.5% (72.4% to 102.2%), p = 0.01] than responders.
Predictors of Responsiveness to SITT in Patients with Asthma
Univariate and multivariate logistic regression analyses to further clarify the predictors of responsiveness to SITT were performed (Table 2). On univariate analysis, clinical predictors of poor response to SITT were dyspnea (odds ratio (OR) = 0.14, p = 0.02), low FVC (%predicted) values (OR = 1.05, p = 0.01), and FVC (%predicted) <80% (OR = 0.11, p = 0.02). Next, multivariate analysis was performed for factors with p < 0.10 on the univariate analysis. FEV1 (%predicted) and FVC (%predicted) values were excluded from this analysis because they were confounded with FEV1 (%predicted) <80% and FVC (%predicted) <80%, respectively. On multivariate analysis, poor response to SITT was associated with residual dyspnea before SITT (OR = 0.14, p = 0.02).
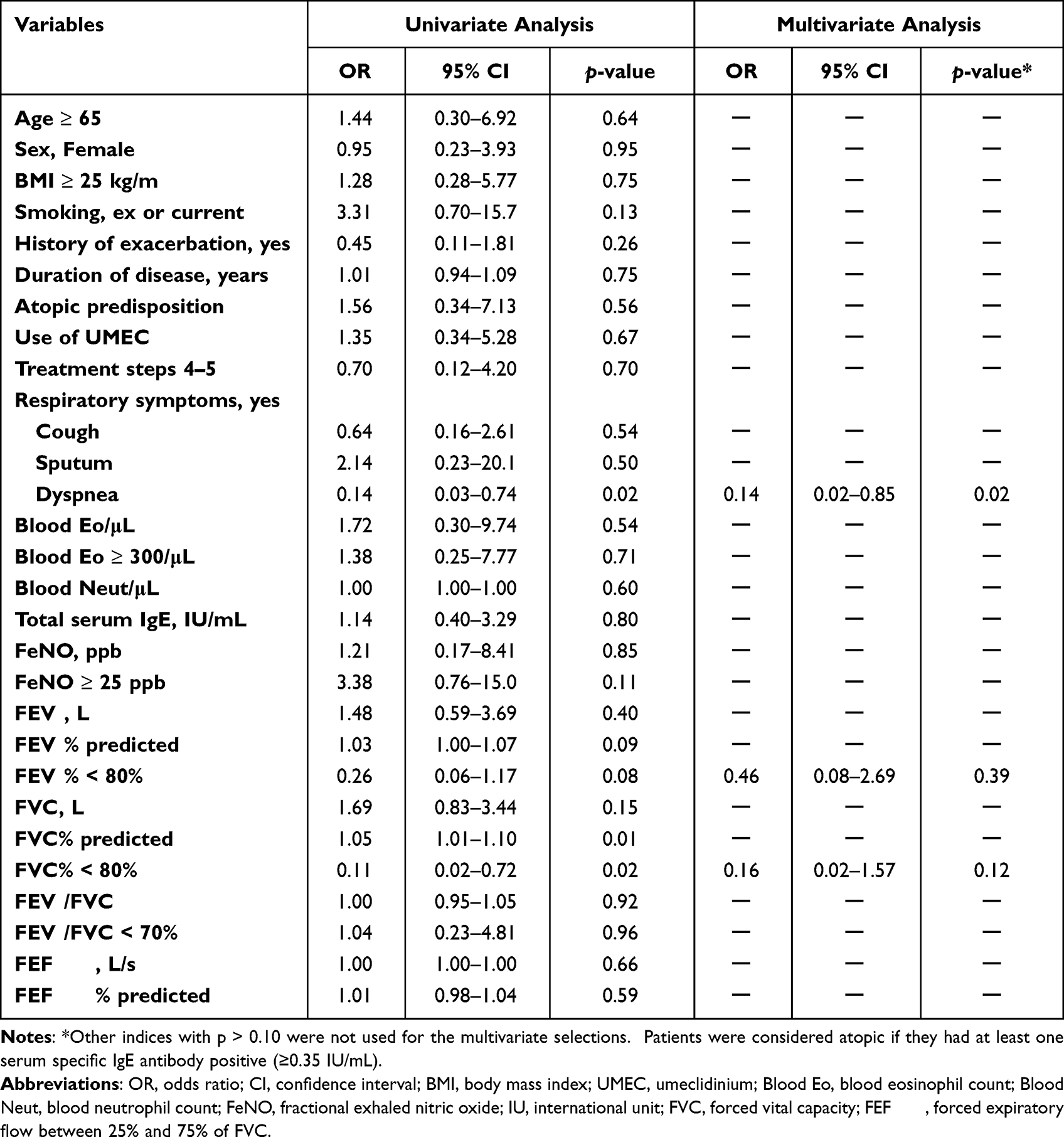 |
Table 2 Predictors of Responsiveness to SITT: Univariate and Multivariate Analyses |
Finally, clinical characteristics and lung functions were compared between patients with and without residual dyspnea (data not shown). Patients with residual dyspnea had significantly lower FEF25–75 (%predicted) values [24.8% (12.4% to 48.6%) vs 31.5% (24.6% to 71.1%), p = 0.04] than patients without residual dyspnea before SITT.
Discussion
In the present study, short-term SITT was effective in 75% of asthmatic patients, independent of patients’ characteristics or type 2 phenotype, which was consistent with previous studies of the efficacy of long-term SITT for asthma.12,13 Furthermore, to the best of our knowledge, this study was the first to demonstrate that residual dyspnea may predict poor responsiveness to short-term SITT in asthma patients.
In the present study, regarding lung function, non-responders to SITT showed significantly lower FVC (%predicted) values than responders, and patients with residual dyspnea showed significantly lower FEF25–75 (%predicted) values, which is an indicator of peripheral airway obstruction,28 than those without residual dyspnea. Recently, in a large cohort study assessing associations of biomarkers, physiological test, and imaging markers with small airways dysfunction (SAD) in asthma, decreases in FVC values and FEF25–75 values were used as indicators to reflect SAD.29 A classical physiological study showed that dyspnea is associated with peripheral airway obstruction (in other words, SAD).30 Based on these findings, the results of the present study suggest that patients with residual dyspnea associated with SAD may respond poorly to short-term SITT.
The usefulness of LAMAs in improving the patency of small airways has been documented in patients with asthma.31 The previous studies showed that tiotropium and GLY exerted a potent suppressive effect on lung inflammation and remodeling in the small airways.32,33 In addition, even in the context of triple therapy, the usefulness of LAMAs in small airway has been documented in patients with asthma. In a study of asthma patients who smoked, triple therapy with an extra-fine formulation was superior to dual therapy with ICS/LABA for effects on small airway outcomes, such as FEF25–75, the difference to respiratory resistance at 5Hz and 20Hz (R5-R20), and the reactance curve (AX).34 These results, which showed that triple therapy was effective for SAD, are inconsistent with the results of the present study. Since an extra-fine formulation of SITT was not used in more than half of the patients in the present study, it was suspected that this may have been a reason for the poor responsiveness to SITT in patients with residual dyspnea.
In the IRIDIUM study, which evaluated a once-daily SITT via Breezhaler, which is not an extra-fine formulation, an improvement in FEF25–75 was observed over 52-week treatment.12 The major difference between this study and the present study was the treatment duration (52 weeks and four weeks, respectively). Because a small number of extra-fine particles will reach the small airways, even with a coarse particle formulation,28 long-term treatment may have been effective in SAD over time. Meanwhile, in the TRIMARAN and TRIGGER studies, which evaluated SITT with an extra-fine formulation, and the CAPTAIN study, which evaluated a once-daily SITT via Ellipta (not an extrafine formulation), it was not known how these SITTs acted on small airways.13,35 Thus, whether SITT could improve SAD in patients with asthma remains essentially unknown. In addition, there is little evidence that SITT improves dyspnea in asthmatic patients.
Currently, patients who are considered to have good indications for SITT (or triple therapy) include patients with poorly controlled asthma on medium-dose ICSs/LABAs, especially those who are considered to benefit less from ICSs because of low type 2 phenotype,13,36 patients on high-dose ICSs/LABAs, especially with persistent airflow obstruction,20 and patients for whom biologics are not indicated.36 On the other hand, high serum total IgE levels (>430 μg/L) have been reported to be predictors of a poor response to adding tiotropium in patients with uncontrolled asthma.37 The results of the present study also suggest that residual dyspnea may predict a poor response to short-term SITT in patients with asthma. Because dyspnea has been reported to be associated with SAD,30 the mechanisms underlying the correlation between residual dyspnea and poor response may be: (1) M3 receptors are denser in the larger bronchi than in the small/peripheral bronchi;38 and, (2) due to problems with the inhaled particle formulation or duration of treatment, SITT agents did not achieve sufficient peripheral lung deposition and penetration and did not improve SAD.
The present study has several limitations. First, this was a retrospective study conducted at a single tertiary asthma care center with a small sample size (n = 45). Second, treatment responsiveness to SITT in this study was based on the GETE. Subjective and objective indicators, such as questionnaires and lung function tests, were not used. Therefore, future prospective studies, using questionnaires, such as the Leicester Cough Questionnaire, the St. George’s Respiratory Questionnaire, the Cough and Sputum Assessment Questionnaire,39–41 or the Leicester Cough Monitor42 are needed. Third, although there was no difference in efficacy between patients who inhaled UMEC and GLY in this study, the different SITT devices with different characteristics were not actually taken into account due to the small sample sizes. Tiotropium had been the only LAMA indicated for asthma, but the effectiveness of various SITTs in recent reports has made it possible to use different LAMAs and devices for asthma treatment. In future studies, difference in LAMAs and devices should be considered. Fourth, impulse oscillometry (IOS), a measure of SAD, was not performed. However, FEF25–75 is thought to reflect volume-dependent closure of small airways as well,28 and there is currently no gold standard tool for the assessment or diagnosis of SAD.31
Even considering these limitations, the present study showed, for the first time, that the residual symptom of dyspnea, as well as objective measurements of SAD, could be predictive of responsiveness to SITT in real-world clinical practice. Although residual dyspnea may predict poor responsiveness to SITT, we do not believe that asthmatic patients with residual dyspnea should not be treated with SITT. Since this study only examined short-term effectiveness, SITT may be effective in asthmatic patients with residual dyspnea when used for the appropriate duration and with the appropriate device for SITT. However, further prospective studies are needed to clarify these speculations.
Conclusions
In summary, short-term SITT showed clinical efficacy for asthmatic patients, independent of patients’ characteristics or type 2 phenotype. Residual dyspnea may predict poor responsiveness to short-term SITT in asthmatic patients, and SAD may be associated with a poor response to SITT. In order to identify predictors of responsiveness to SITT for patients with asthma in real-world clinical practice, further studies are needed.
Abbreviations
COPD, chronic obstructive pulmonary disease; FEF25–75, forced expiratory flow between 25% and 75% of FVC; FeNO, fractional exhaled nitric oxide; FVC, forced vital capacity; GETE, global evaluation of treatment effectiveness; GLY, glycopyrrolate; ICSs, inhaled corticosteroids; LABAs, long-acting β2 agonists; LAMAs, long-acting muscarinic antagonists; SAD, small airways dysfunction; SITT, single inhaler triple therapy; UMEC, umeclidinium.
Data Sharing Statement
Datasets are available on request.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of Nagoya City University (60-21-0044). Written informed consent was waived by the ethics committee due to the retrospective nature of this study. Instead, an opt-out document was posted on the hospital website to offer patients the opportunity to refuse participation.
Funding
There is no funding to report.
Disclosure
Dr Kensuke Fukumitsu reports grants from Novartis Pharma and GSK; personal fees from AstraZeneca, Boehringer Ingelheim, Novartis Pharma, and Kyorin, outside the submitted work. Dr Yoshihiro Kanemitsu reports grants and/or personal fees from Novartis Pharma, MSD, Sanofi, AstraZeneca, GSK, and Kyorin, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Global Initiative for Asthma. Global strategy for asthma management and prevention; 2022. Available from: https://ginasthma.org/gina-reports/.
2. Adachi M, Hozawa S, Nishikawa M, Yoshida A, Jinnai T, Tamura G. Asthma control and quality of life in a real-life setting: a cross-sectional study of adult asthma patients in Japan (ACQUIRE-2). J Asthma. 2019;56(9):1016–1025. doi:10.1080/02770903.2018.1514628
3. Peters SP, Kunselman SJ, Icitovic N, et al. Tiotropium bromide step-up therapy for adults with uncontrolled asthma. N Engl J Med. 2010;363(18):1715–1726. doi:10.1056/NEJMoa1008770
4. Kerstjens HA, Casale TB, Bleecker ER, et al. Tiotropium or salmeterol as add-on therapy to inhaled corticosteroids for patients with moderate symptomatic asthma: two replicate, double-blind, placebo-controlled, parallel-group, active-comparator, randomised trials. Lancet Respir Med. 2015;3(5):367–376. doi:10.1016/S2213-2600(15)00031-4
5. Paggiaro P, Halpin DMG, Buhl R, et al. The effect of tiotropium in symptomatic asthma despite low- to medium-dose inhaled corticosteroids: a randomized controlled trial. J Allergy Clin Immunol Pract. 2016;4(1):104–113.e2. doi:10.1016/j.jaip.2015.08.017
6. Kerstjens HAM, Engel M, Dahl R, et al. Tiotropium in asthma poorly controlled with standard combination therapy. N Engl J Med. 2012;367(13):1198–1207. doi:10.1056/NEJMoa1208606
7. Ohta K, Ichinose M, Tohda Y, et al. Long-term once-daily tiotropium respimat® is well tolerated and maintains efficacy over 52 weeks in patients with symptomatic asthma in Japan: a randomised, placebo-controlled study. PLoS One. 2015;10(4):e0124109. doi:10.1371/journal.pone.0124109
8. Tamada T, Sugiura H, Takahashi T, et al. Coexisting COPD in elderly asthma with fixed airflow limitation: assessment by DLco %predicted and HRCT. J Asthma. 2017;54(6):606–615. doi:10.1080/02770903.2016.1247168
9. Matsunaga K, Hamada K, Oishi K, Yano M, Yamaji Y, Hirano T. Factors Associated with physician-patient discordance in the perception of asthma control. J Allergy Clin Immunol Pract. 2019;7(8):2634–2641. doi:10.1016/j.jaip.2019.04.046
10. Nagase H, Adachi M, Matsunaga K, et al. Prevalence, disease burden, and treatment reality of patients with severe, uncontrolled asthma in Japan. Allergol Int. 2020;69(1):53–60. doi:10.1016/j.alit.2019.06.003
11. Melani AS, Bonavia M, Cilenti V, et al. Inhaler mishandling remains common in real life and is associated with reduced disease control. Respir Med. 2011;105(6):930–938. doi:10.1016/j.rmed.2011.01.005
12. Kerstjens HAM, Maspero J, Chapman KR, et al. Once-daily, single-inhaler mometasone-indacaterol-glycopyrronium versus mometasone-indacaterol or twice-daily fluticasone-salmeterol in patients with inadequately controlled asthma (IRIDIUM): a randomised, double-blind, controlled phase 3 study. Lancet Respir Med. 2020;8(10):1000–1012. doi:10.1016/S2213-2600(20)30190-9
13. Lee LA, Bailes Z, Barnes N, et al. Efficacy and safety of once-daily single-inhaler triple therapy (FF/UMEC/VI) versus FF/VI in patients with inadequately controlled asthma (CAPTAIN): a double-blind, randomised, phase 3A trial. Lancet Respir Med. 2021;9(1):69–84. doi:10.1016/S2213-2600(20)30389-1
14. Zhang S, King D, Rosen VM, Ismaila A. Impact of single combination inhaler versus multiple inhalers to deliver the same medications for patients with asthma or COPD: a systematic literature review. Int J Chron Obstruct Pulmon Dis. 2020;15:417–438. doi:10.2147/COPD.S234823
15. Peters SP, Bleecker ER, Kunselman SJ, et al. Predictors of response to tiotropium versus salmeterol in adults with asthma. J Allergy Clin Immunol. 2013;132(5):1068–1074. doi:10.1016/j.jaci.2013.08.003
16. Kerstjens HAM, Moroni-Zentgraf P, Tashkin DP, et al. Tiotropium improves lung function, exacerbation rate, and asthma control, independent of baseline characteristics including age, degree of airway obstruction, and allergic status. Respir Med. 2016;117:198–206. doi:10.1016/j.rmed.2016.06.013
17. Casale TB, Bateman ED, Vandewalker M, et al. Tiotropium respimat add-on is efficacious in symptomatic asthma, independent of T2 phenotype. J Allergy Clin Immunol Pract. 2018;6(3):923–935.e9. doi:10.1016/j.jaip.2017.08.037
18. Casale TB, Aalbers R, Bleeker ER, et al. Tiotropium respimat® add-on therapy to inhaled corticosteroids in patients with symptomatic asthma improves clinical outcomes regardless of baseline characteristics. Respir Med. 2019;158:97–109. doi:10.1016/j.rmed.2019.09.014
19. Singh D, Virchow JC, Canonica GW, et al. Determinants of response to inhaled extrafine triple therapy in asthma: analyses of TRIMARAN and TRIGGER. Respir Res. 2020;21(1):285. doi:10.1186/s12931-020-01558-y
20. Singh D, Virchow JC, Canonica GW, et al. Extrafine triple therapy in patients with asthma and persistent airflow limitation. Eur Respir J. 2020;56(3):2000476. doi:10.1183/13993003.00476-2020
21. Bousquet J, Siergiejko Z, Swiebocka E, et al. Persistency of response to omalizumab therapy in severe allergic (IgE-mediated) asthma. Allergy. 2011;66:671–678. doi:10.1111/j.1398-9995.2010.02522.x
22. Hoshino Y, Koya T, Kagamu H, et al. Effect of inhaled corticosteroids on bronchial asthma in Japanese athletes. Allergol Int. 2015;64:145–149. doi:10.1016/j.alit.2014.10.004
23. Miller MR, Crapo R, Hankinson J, et al. General considerations for lung function testing. Eur Respir J. 2005;26:153–161. doi:10.1183/09031936.05.00034505
24. Dweik RA, Boggs PB, Erzurum SC, et al. An official ATS clinical practice guideline: interpretation of exhaled nitric oxide levels (FENO) for clinical applications. Am J Respir Crit Care Med. 2011;184(5):602–615. doi:10.1164/rccm.9120-11ST
25. Inoue H, Niimi A, Takeda T, et al. Pathophysiological characteristics of asthma in the elderly: a comprehensive study. Ann Allergy Asthma Immunol. 2014;113(5):527–533. doi:10.1016/j.anai.2014.08.002
26. To M, Hitani A, Kono Y, et al. Obesity-associated severe asthma in an adult Japanese population. Respir Investig. 2018;56(6):440–447. doi:10.1016/j.resinv.2018.07.003
27. Nadif R, Siroux V, Oryszczyn MP, et al. Heterogeneity of asthma according to blood inflammatory patterns. Thorax. 2009;64(5):374–380. doi:10.1136/thx.2008.103069
28. Lipworth B, Manoharan A, Anderson W. Unlocking the quiet zone: the small airway asthma phenotype. Lancet Respir Med. 2014;2(6):497–506. doi:10.1016/S2213-2600(14)70103-1
29. Postma DS, Brightling C, Baldi S, et al. Exploring the relevance and extent of small airways dysfunction in asthma (ATLANTIS): baseline data from a prospective cohort study. Lancet Respir Med. 2019;7(5):402–416. doi:10.1016/S2213-2600(19)30049-9
30. McFadden ER. Exertional dyspnea and cough as preludes to acute attacks of bronchial asthma. N Engl J Med. 1975;292:555–559. doi:10.1056/NEJM197503132921103
31. Rogliani P, Ritondo BL, Puxeddu E, Cazzola M, Calzetta L. Impact of long-acting muscarinic antagonists on small airways in asthma and COPD: a systematic review. Respir Med. 2021;189:106639. doi:10.1016/j.rmed.2021.106639
32. Kumawat K, Koopmans T, Gosens R. β-catenin as a regulator and therapeutic target for asthmatic airway remodeling. Expert Opin Ther Targets. 2014;18(9):1023–1034. doi:10.1517/14728222.2014.934813
33. Hsiao YH, Tseng CM, Su KC, et al. Glycopyrronium bromide inhibits lung inflammation and small airway remodeling induced by subchronic cigarette smoke exposure in mice. Respir Physiol Neurobiol. 2018;249:16–22. doi:10.1016/j.resp.2017.12.005
34. Jabbal S, Cr K, Lipworth B. Randomized controlled trial of triple versus dual inhaler therapy on small airways in smoking asthmatics. Clin Exp Allergy. 2020;50:1140–1147. doi:10.1111/cea.13702
35. Virchow JC, Kuna P, Paggiaro P, et al. Single inhaler extrafine triple therapy in uncontrolled asthma (TRIMARAN and TRIGGER): two double-blind, parallel-group, randomised, controlled phase 3 trials. Lancet. 2019;394(10210):1737–1749. doi:10.1016/S0140-6736(19)32215-9
36. Agusti A, Fabbri L, Lahousse L, Singh D, Papi A. Single inhaler triple therapy (SITT) in asthma: systematic review and practice implications. Allergy. 2021;70:1–9. doi:10.15036/arerugi.70.1
37. Cheng WC, Wu BR, Liao WC, et al. Clinical predictors of the effectiveness of tiotropium in adults with symptomatic asthma: a real-life study. J Thorac Dis. 2018;10(6):3661–3669. doi:10.21037/jtd.2018.05.139
38. Ikeda T, Anisuzzaman ASM, Yoshiki H, et al. Regional quantification of muscarinic acetylcholine receptors and β-adrenoceptors in human airways. Br J Pharmacol. 2012;166(6):1804–1814. doi:10.1111/j.1476-5381.2012.01881.x
39. Birring SS, Prudon B, Carr AJ, Singh SJ, Morgan MDL, Pavord ID. Development of a symptom specific health status measure for patients with chronic cough: Leicester Cough Questionnaire (LCQ). Thorax. 2003;58(4):339–343. doi:10.1136/thorax.58.4.339
40. Jones PW, Quirk FH, Baveystock CM, Littlejohns P. A self-complete measure of health status for chronic airflow limitation. The St. George’s respiratory questionnaire. Am Rev Respir Dis. 1992;145(6):1321–1327. doi:10.1164/ajrccm/145.6.1321
41. Crawford B, Monz B, Hohlfeld J, et al. Development and validation of a cough and sputum assessment questionnaire. Respir Med. 2008;102(11):1545–1555. doi:10.1016/j.rmed.2008.06.009
42. Vertigan AE, Kapela S, Birring SS, Gibson PG. Feasibility and clinical utility of ambulatory cough monitoring in an outpatient clinical setting: a real-world retrospective evaluation. ERJ Open Res. 2021;7:00319–2021. doi:10.1183/23120541.00319-2021
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.