Back to Journals » Journal of Blood Medicine » Volume 17
Research Progress on Transitional Care for Hemophilia Patients from Pediatric to Adult Services: Focusing on Disease Severity and Care Continuity
Authors Wu S ![]() , Wang C, Li D, Shi D
, Wang C, Li D, Shi D
Received 4 August 2025
Accepted for publication 14 January 2026
Published 10 February 2026 Volume 2026:17 558200
DOI https://doi.org/10.2147/JBM.S558200
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chang Kim
Siting Wu,1 Chunli Wang,2 Dan Li,3 Dongrong Shi4
1Department of Stem Cell Transplantation, Beijing Children’s Hospital, Capital Medical University, National Center for Children’s Health, Beijing, People’s Republic of China; 2Department of Nursing, Beijing Children’s Hospital, Capital Medical University, National Center for Children’s Health, Beijing, People’s Republic of China; 3Department of Medical Oncology, Beijing Children’s Hospital, Capital Medical University, National Center for Children’s Health, Beijing, People’s Republic of China; 4Department of Leukemia, Beijing Children’s Hospital, Capital Medical University, National Center for Children’s Health, Beijing, People’s Republic of China
Correspondence: Chunli Wang, Email [email protected]
Abstract: Hemophilia is a lifelong coagulation disorder with varying severity levels, which significantly impacts management strategies. The transition period from pediatric to adult medical system represents a critical stage for ensuring continuous and tailored care. This narrative review synthesizes current evidence on transitional care for hemophilia patients, focusing on nursing-led interventions. A structured search of literature from 2010 to 2024 was conducted, drawing from key databases including PubMed, Embase, and CINAHL, as well as major guideline repositories and professional society publications. The findings from this analysis systematically summarize the challenges and intervention strategies in the transitional period. At the patient level, there are problems such as lack of self-management ability, psychosocial adaptation disorder and treatment compliance decline, particularly among those with severe disease; this period also requires a deliberate shift in responsibility from parents to the young person, a process that requires careful support for both. At the level of medical system, the transition difficulty is exacerbated by the differences between pediatric and adult medical models, the lack of multidisciplinary cooperation and the uneven distribution of resources, all of which hinder seamless care continuity. At present, the effective intervention strategies include: the implementation of structured transition plan, the training of self injection and emergency treatment skills, the provision of psychosocial support, and the establishment of nurse led multidisciplinary cooperation mode. During the transition period, nurses play the core role of assessment planning, education empowerment, coordination advocacy and psychological support. In the future, it is necessary to strengthen the development of digital tools, research on long-term health outcomes and policy support, so as to optimize the transitional nursing system and ensure the continuity of life-long health management of patients across all severity levels. While this review synthesizes global evidence, it is pertinent to note that challenges of resource access, particularly the urban-rural divide in availability of factor concentrates, novel therapies, and home-treatment programs, are often more pronounced in many developing countries, including China. The insights gathered underscore the need for standardized, nurse-coordinated transitional care protocols to inform both clinical practice and healthcare policy, aiming to bridge current gaps in service delivery and improve long-term patient outcomes.
Keywords: hemophilia, children, transition period, ready
Hemophilia is an X-linked hereditary coagulation dysfunction disease, which is characterized by spontaneous or post-traumatic bleeding tendency and requires lifelong coagulation factor replacement therapy and comprehensive management.1 With a global prevalence of approximately 1 in 10,000 males, it represents a significant chronic condition requiring lifelong care. The transition to adulthood is a high-risk period; studies indicate that up to 30–40% of adolescents experience a decline in treatment adherence, leading to increased bleeding episodes and joint damage. With the progress of medical technology, the life expectancy of hemophilia patients has been significantly extended, and more than 90% of children can survive to adulthood.2 However, when patients enter the adult stage from childhood, their medical care system is facing a key transformation from the family centered pediatric model to the patient-centered adult model.3 If this process lacks systematic support, it will easily lead to problems such as decreased treatment compliance, increased joint bleeding events, and poor psychosocial adaptation, which will seriously threaten the long-term health outcomes of patients.4
Transitional care, as the core strategy to solve this challenge, is defined as helping adolescent patients with chronic diseases gradually acquire self-management ability through multidisciplinary collaborative and systematic intervention, so as to achieve a safe, sustainable and stable transfer from pediatric to adult medical system.5 In the field of hemophilia, effective transition preparation is not only the connection of medical services but also the key link to ensure the continuity of life-long health management of patients.
Although the international guidelines emphasize the importance of transitional care, there are still imbalanced practices and lack of standardization around the world, and structural transition projects in some developed countries have achieved initial results, most regions still face common problems such as the lack of patient self-management ability, the lack of collaboration in the medical system, and the absence of psychosocial support.
This narrative review aims to: (1) synthesize the key challenges faced by patients and healthcare systems during this transition; (2) evaluate the evidence for existing intervention strategies, with a particular focus on the pivotal role of nursing; (3) identify critical gaps to inform future practice and research. A narrative synthesis methodology was selected to allow for the inclusion of a broad range of evidence, including clinical guidelines, qualitative insights, and trial data, to provide a comprehensive overview of this complex, multi-faceted process.
Methods
This study was conducted as a narrative review to comprehensively synthesize and critically appraise the current state of knowledge on transitional care for hemophilia, with a particular focus on the nursing role. To ensure a rigorous and reproducible literature search, a structured strategy was employed. Searches were conducted in the electronic databases PubMed, Embase, and CINAHL for publications from January 2010 to May 2024, limited to the English language.
The search strategy combined keywords and controlled vocabulary terms (eg, MeSH, Emtree) related to three core concepts: (“hemophilia” OR “haemophilia”) AND (“transition” OR “transitional care” OR “adolescent” OR “young adult”) AND (“nursing” OR “self-management” OR “multidisciplinary care”).
Inclusion criteria encompassed: (1) primary research studies (including qualitative, quantitative, and mixed-methods designs) and review articles (systematic, narrative) focusing on the transition from pediatric to adult care for patients with hemophilia; (2) articles explicitly discussing challenges, interventions, or the roles of healthcare professionals. Exclusion criteria were: (1) studies not specific to hemophilia; (2) editorials, opinions, or letters without original data or synthesis; (3) articles focused solely on pediatric or adult care without a direct link to the transition process.
Given the narrative review design and the intentional inclusion of heterogeneous publication types to provide a comprehensive perspective, a formal quality appraisal using standardized tools (eg, CASP) was not performed. Instead, a critical appraisal was undertaken narratively by considering the study design, sample size, methodological limitations, and relevance to the review’s objectives when interpreting and presenting the findings. The final synthesis aimed to integrate high-quality evidence while also mapping the broader discourse and innovative practices in the field.
Challenges of Transitional Care of Hemophilia
Challenges at the Patient Level
Hemophilia patients are facing multi-dimensional individualized challenges in the process of transition from children to adult health care system. These challenges are rooted in the transformation of their physiological, psychological and social roles. The primary obstacle is reflected in the fault of self-management ability. In childhood, treatment decision-making and daily care (such as coagulation factor injection, bleeding identification, and referral arrangements) are highly dependent on parents or medical staff; After entering the adolescent stage, patients need to gradually assume independent responsibility for disease management.6 However, due to the lack of systematic skill training and adaptive guidance, many adolescent patients show insufficient operation ability (such as unable to complete self injection independently), wrong risk judgment (such as delaying the identification and treatment of joint bleeding) and medical communication barriers (such as difficulty in autonomously describing the medical history to the adult physician), resulting in a significant increase in the risk of accidental bleeding events.7 Simultaneously, parents themselves may struggle with relinquishing their long-held role as primary care manager, which can inadvertently hinder the young person’s development of autonomy if not sensitively managed.
At the same time, psychosocial adaptation barriers further exacerbated the transition dilemma. There is a fierce conflict between the inherent identity needs of adolescence and the limitations brought about by chronic diseases: patients often have a sense of social isolation due to exercise taboos (such as avoiding contact sports activities), worry about future marriage and childbearing choices due to their awareness of genetic risks, or suffer from campus/workplace discrimination due to disease stigmatization.8 Research shows that about 30%−40% of adolescent hemophilia patients have moderate or above anxiety or depression tendency, and their low acceptance of the disease may lead to two extreme behaviors – excessive dependence on family support or refusal to recognize medical needs, both of which hinder their transition to the role of adults.9
What is more serious is that the above factors jointly catalyze the systematic decline of treatment compliance. Some teenagers actively reduce the injection frequency of preventive coagulation factor because they are tired of long-term treatment, deny the severity of the disease, or are affected by peer pressure;10 Others were negligent in treatment due to the lack of supervision during the transition period (such as the sudden drop in the participation of parents and the interruption of the follow-up of the pediatric team).11 The direct consequence of this phenomenon is that the risk of recurrent joint bleeding increases and the progression of joint lesions is accelerated. The study confirmed that the omission rate of prevention and treatment in 16–21year-old hemophilia patients increased by 22% compared with that in childhood, accompanied by an 18% increase in the detection rate of target joints in this age group.12 Large national cohort studies further underscore that deficits in self-management and system support are widespread challenges, negatively impacting adherence and health outcomes during transition.
Challenges at the Medical System Level
The transition dilemma of hemophilia patients not only stems from individual adaptation barriers but also reflects the structural defects within the medical system. The essential differences between pediatric and adult medical models constitute the primary institutional barriers. Pediatric medical care has long followed the concept of “family centered” care, and the decision-making and communication of diagnosis and treatment are often dominated by parents; The adult medical system emphasizes “patient autonomy” and requires patients to independently assume management responsibilities.13 This conceptual gap leads to the systematic failure of transition and connection: the pediatric team delays the handover of patients due to the lack of standardized referral process, while the adult physicians are difficult to accurately formulate individualized plans because they do not fully grasp the treatment history of patients during their growth and development (such as the development history of inhibitors and the baseline state of joints).14 Research shows that up to 40% of the transferred patients need to repeat the examination due to incomplete transmission of disease history, which not only increases the medical cost but also may cause joint bleeding risk due to treatment delay.15 Furthermore, the healthcare delivery model itself impacts transition smoothness. Transitions between separate pediatric and adult centers involve navigating different systems and teams, while integrated centers managing all age groups can facilitate continuity within a single framework, potentially leading to better outcomes.
The lack of multidisciplinary collaboration mechanism further weakens the continuity of transition. The lifelong management of hemophilia needs the collaborative support of multiple teams such as hematology department, physical therapy department, psychology department and social work.16 However, during the critical period of transition, various specialties are often in a fragmented state: the pediatric and adult hematology teams lack a joint follow-up system, rehabilitation therapists do not participate in the formulation of transition plans, and psychological support services are interrupted due to department transfer.17 Especially when the patient has sudden joint bleeding or psychological crisis, the responsibility subject is unknown, resulting in delayed response. As a potential coordination hub, nurses are difficult to effectively integrate resources due to power constraints or lack of training. A multicenter survey shows that only 28% of medical institutions have established a regular meeting system for multidisciplinary teams during the transition period of hemophilia, and the lack of cooperation directly led to 33% of patients suffering from management loopholes in the first year of the transition.18
The deeper contradiction lies in the imbalance of regional distribution of medical resources. Developed countries provide full cycle management through regional comprehensive care centers (CCCs), but there is a serious shortage of adult hemophilia specialist services worldwide (especially in developing countries).19 Patients in remote areas are faced with double dilemmas: after the termination of pediatric services, the adult medical points lack of coagulation factor pharmacy reserves, lack of hematologists familiar with complex cases, and even lack of basic physical rehabilitation facilities.20 This inclination of resources forced some adolescent patients to discontinue standardized treatment or travel long distances to the central urban area for medical treatment, which significantly increased their economic burden and physical and mental pressure.21 This disparity in access to factor products, novel agents, and comprehensive care training (including home therapy) between urban and rural settings creates a gap in self-management capabilities that exists even before transition, a gap that then widens critically when structured pediatric support is withdrawn. The data confirmed that the transition failure rate of patients in non urban areas was 2.1 times higher than that of urban patients, and the joint disability rate increased by 37%.22
Intervention Strategies for Transitional Care
Structured Transition Programs
The structural transition plan is the cornerstone of transitional care for hemophilia. Its core is to bridge the gap between pediatric and adult medical systems through standardized processes and gradual responsibility transfer. International guidelines generally recommend the use of a phased age framework to start the transition process: from the age of 12 to 14, the concept of self-management is introduced in the pediatric follow-up, and the initial skill assessment is led by nurses. This approach is exemplified by structured, generic programmes like “Ready Steady Go”, which provides a validated framework of age-appropriate questionnaires to guide conversations starting from as early as age 11–13, covering topics from disease knowledge to future planning, and can be effectively adapted for hemophilia. The structured approach should actively involve parents, guiding them on how to progressively shift from being a direct manager to a supportive coach, thereby facilitating the adolescent’s growing independence. By the age of 15–17, parents’ participation in decision-making will be gradually reduced, and patients will be required to complete some operations independently (such as recording bleeding events and making appointments for follow-up visits); Finally, the adult medical team will be fully autonomous before the age of 18.23 This step-by-step promotion strategy has significantly improved the success rate of the transition – a Canadian cohort study confirmed that the retention rate of treatment compliance of patients with phased plan within 12 months after referral was 92%, while that of non participants was only 67%.24
In order to ensure the scientific nature of the transition process, the application of standardized assessment tools is crucial. The “hemophilia transition readiness assessment scale” (h-traq), which is widely adopted at present, covers four dimensions: mastery of disease knowledge (such as understanding the coagulation mechanism), proficiency in operating skills (such as self injection ability), medical communication efficiency (such as describing symptoms to doctors) and Health Behavior Initiative (such as regular follow-up awareness).25 The scale identifies the weak points of patients through quantitative score (full score of 100), and provides the basis for nurses to formulate personalized training plan. Research shows that the incidence of joint bleeding events in patients with h-traq score >80 points after referral is 41% lower than that in patients with h-traq score <60 points, confirming the predictive value of evaluation tools for clinical outcomes.26
In order to break the barriers of medical information transmission, the transition passport, as a portable electronic or paper file, is included in the key intervention means. Its content not only integrates the patient’s core medical data (such as hemophilia classification, inhibitor history, target joint status, and current treatment plan) but also covers the psychosocial needs (such as academic/career planning, and emergency contacts).27 At the practical level, the passport is filled in by the pediatric team, updated by patients, and finally signed by the adult physician to ensure the integrity and timeliness of the medical history.28 The practice of UK National Hemophilia database shows that the missing rate of referral information in medical institutions using transitional passports has decreased from 35% to 6%, and patients’ trust in the adult medical team has increased by 58%.29 The effectiveness of such structured, nationally coordinated approaches is supported by recent evaluations, which demonstrate their success in improving continuity of care and patient satisfaction. See Table 1 for relevant contents.
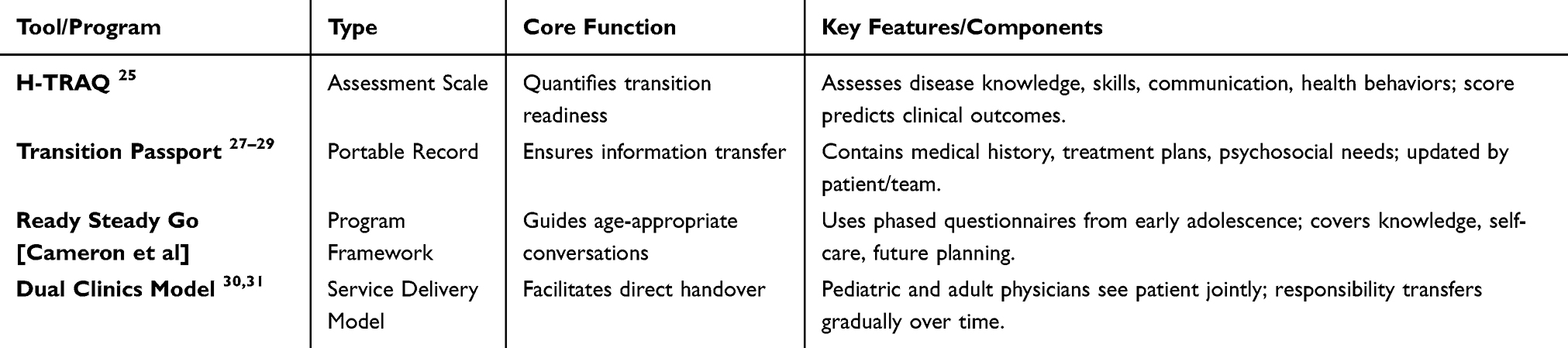 |
Table 1 Key Structured Transition Tools and Programs in Hemophilia Care |
Education and Skill Training
The standardized training of intravenous self injection ability is the core technical barrier of self-management in the transition period for patients with severe hemophilia requiring regular prophylaxis. In view of the operational anxiety and skill weakness of adolescent patients, the nurse led training adopted a cognitive behavioral four stage model: in the first stage, the distribution of veins and the principle of sterility were recognized through 3D animation and anatomical atlas; In the second stage, the silicone mold and virtual reality (VR) system were used for puncture simulation to correct the angle/depth error in real time; The third stage is the transition to human assisted operation (first practice in the nurse’s arm, and then self injection under supervision); In the final stage, the family independent injection is realized, supplemented by remote guidance app to deal with emergencies (such as venous collapse).32 The randomized controlled trial (RCT) of the Netherlands’ Rotterdam Hemophilia Center confirmed that the success rate of independent injection in patients aged 15–18 years who received the model was 89% after 6 months, and the injection related anxiety score decreased by 62%33 Moreover, the introduction of novel therapies (eg, non-factor products) with different administration routes and treatment schedules may alter adherence drivers, necessitating adaptations in transitional education to address potential new challenges, such as complacency with prolonged follow-ups.
Early recognition and intervention of joint bleeding directly determine the long-term outcome of joint function. The core of the training is “time window sensitivity” and standardized operation process (SOP): first, improve the recognition ability of early signs of target joint bleeding (such as joint warm feeling and activity range reduction ≥30%);34 Secondly, strictly regulate the operation details of rice principle – R (braking): fix the affected limb with adjustable brace; I (ice compress): medical cold gel package (−2°C to 4°C) every 2 hours and 10 minutes to avoid direct skin contact; C (compression): the elastic bandage is spirally wound by “figure of eight” method, and the pressure value is maintained at 40–50mmhg; E (elevation): the affected limb is 20 cm higher than the heart level for 72 hours;35 At the same time, a medical decision tree was established (eg, single joint swelling >24 hours or abnormal sensation requiring emergency treatment).36 The National Hemophilia Foundation (NHF) multicenter study showed that the correct intervention rate within 6 hours after the completion of the training increased to 78% (baseline 31%), and the risk of secondary joint disease decreased by 44% (HR = 0.56, 95% CI 0.42–0.75).37
In order to resolve the contradiction between disease restriction and quality of life, it is necessary to provide evidence-based individualized life management strategies. The risk grading system is adopted for sports guidance: low-risk activities (swimming and cycling are recommended, and the joint load is less than 30% of the body weight), medium risk activities (limited to table tennis and golf, which need to be evaluated by sports protection engineers), and absolutely taboo activities (football, boxing and other collision events).38 Career planning emphasizes the avoidance of trauma risk, preferentially recommends low physical occupations such as telecommuting, education and IT, and customizes adaptive work programs through occupational rehabilitation practitioners.39 Nutrition management focuses on weight control (target BMI < 25) and iron metabolism balance, and formulates high iron diet (50 g of red meat and 100 mg of vitamin C per day to promote absorption) to prevent anemia caused by repeated bleeding.40 A 10-year cohort study at the University of Milan, Italy, confirmed that the progress rate of joint MRI injury in patients who followed the protocol was reduced by 53% (the average annual difference of Shariff scores was −0.8 vs −1.7, *p* = 0.003), and the full-time employment rate was close to that of the general population (91% vs 96%, *p* = 0.12).41 For patients with mild or moderate hemophilia, typically managed on an on-demand basis, the educational emphasis shifts towards accurate bleeding recognition and timely emergency response, rather than self-infusion skills.
Psychosocial Support
Psychosocial support is the key dimension of transitional care for hemophilia, which aims to resolve the identity conflict and limited social participation of adolescents due to disease. Structured peer support significantly alleviates the sense of isolation of patients by building a cross age communication platform: under the coordination of adult nurses, it organizes quarterly group meetings between 16–18-year-old teenagers and 25–30-year-old adult patients (with stable occupation and rich management experience), including the process of disease acceptance (such as the psychological breakthrough of the first independent injection), social skills (communication strategies to deal with sports rejection) and intimate relationship establishment (genetic counseling and partner notification experience).42 The control study of the British hemophilia Association showed that the a-dbs score of adolescent patients who participated in more than 3 meetings increased by 38%, and social avoidance behavior decreased by 52%, which was due to the hope transmission of experience visualization and the sense of community belonging.43
In view of the high incidence of emotional disorders in the transition period, the professional psychological counseling led by cognitive behavioral therapy (CBT) provides a standardized intervention path. In the first stage, the catastrophic thinking was corrected by disease cognition Reconstruction Technology (such as guiding and recording “disease advantage”: the improvement of health awareness brought by regular medical monitoring); In the second stage, exposure therapy (ERP) was applied to deal with fear situations gradually (such as simulating the scene that students could not participate in the football match); In the third stage, mindfulness decompression (MBSR) was used to control anxiety physiological reactions (such as somatization symptoms before bleeding).44 At the key nodes, the nurses screened the PHQ-9/GAD-7 scale, and the patients with moderate and severe depression (PHQ-9 ≥ 15 points) were referred to the psychiatric department in time. The multicenter RCT of the University of Heidelberg in Germany confirmed that the depression relief rate of the 12-week CBT intervention group was 2.3 times higher than that of the conventional nursing group (65% vs 28%, *p* < 0.001), and the treatment benefit lasted until 24 months after referral (hr = 0.41, 95% CI 0.29–0.58).45 See Table 2 for relevant contents.
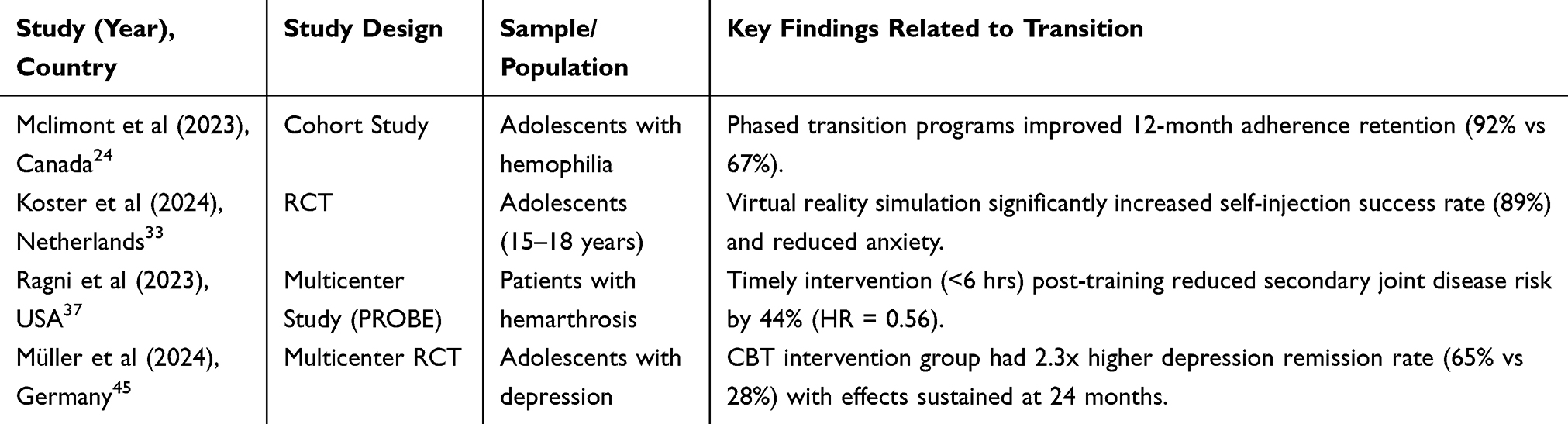 |
Table 2 Summary of Key Studies on Transitional Care Interventions |
Multidisciplinary Collaboration Mode
The successful implementation of hemophilia transitional care depends on the institutionalized interdisciplinary collaboration framework to solve the convergence barriers caused by the fragmentation of the medical system. The pediatric adult joint outpatient service (dual clinics) reconstructs the referral process through a phased responsibility transfer mechanism: during the transition start-up period (12–14 years old), adult physicians participate in pediatric follow-up every six months to initially assess the patient’s self-management ability and establish a trust relationship; During the transition core period (15–17 years old), the proportion of joint outpatient service increased to 50%, and the teams of both sides jointly formulated individualized goals (such as inhibitor management scheme or joint rehabilitation plan); At the completion of handover (≥18 years old), pediatricians will lead the final case discussion to ensure that the adult department has a comprehensive grasp of the key data of growth and development (such as joint MRI baseline, inhibitor regression History).30 The practice of the hemophilia network in Ontario, Canada, confirmed that this model reduced the treatment interruption rate from 31% to 8% (rr = 0.26, 95% CI 0.18–0.37), and patients’ satisfaction with medical continuity reached 94% (vs 67% of the traditional model, *p* < 0.001). Its core advantage is that the responsibility sharing system eliminates the medical information gap.31
Nurse led coordination is the engine of multidisciplinary collaboration. Full time nurses act as cross system integrators. Based on the results of h-traq assessment, they work with hematologists, physiotherapists and psychologists to develop phased goals (such as mastering self injection within 6 months); Track progress through quarterly follow-up (such as skill mastery and PHQ-9 emotional score) and start early warning for those who deviate from the plan (if the skill fallback exceeds 20%, it will trigger intensive training); Cooperate with social security institutions to apply for treatment fee relief and coordinate home care services (such as cold chain coagulation factor distribution); Turn teenagers’ privacy demands into diagnosis and treatment norms (such as the setting of independent consulting rooms).46 According to the data of hemophilia treatment centers (HTCs) in the United States, the compliance rate of patients’ skills in institutions equipped with coordinating nurses has increased by 2.1 times (79% vs 38%), and the implementation rate of multidisciplinary consultation has reached 92%, highlighting the role transition of nurses from care executors to system navigators.47
The Key Role of Nurses in Transitional Care
Evaluate the planner and personalizer. Nurses are the first to initiate and plan the transition process. They used the h-traq scale system to assess adolescents’ self-management ability, mastery of disease knowledge and psychosocial readiness. Based on the evaluation results, the nurses led or deeply participated in the formulation of personalized and phased transition plans, defined the goals, task nodes (such as the master time of independent injection) and completion time limit, and were responsible for sorting out the core medical information to lay the foundation for the “transition passport”, ensuring that the plan met the individual development level and needs of patients.48
Educators of core skills and enablers of self-management. Nurses are the key instructors to improve patients’ independent management ability. They are directly responsible for teaching core survival skills, including the operation training of intravenous/subcutaneous self injection of coagulation factors, early bleeding recognition and rice principle emergency treatment, safe exercise selection and healthy lifestyle guidance. Through patient demonstration, simulation training and continuous encouragement, nurses help patients overcome fear and build confidence, and finally realize the transformation from dependence to self-management, enabling them to assume the responsibility of health in adulthood.49 Involving parents in these training sessions, especially in the initial stages, can help build their confidence in their child’s capabilities and ensure consistent support at home.
The coordinator of multidisciplinary collaboration and the bridge of system connection. Nurses often play a crucial role as “transition coordinators”. They are the core link between pediatrics and adult medical system, and actively promote the communication and cooperation between multidisciplinary teams (hematologists, rehabilitation specialists, psychological experts, etc). Nurses are responsible for arranging and participating in the pediatric adult department joint outpatient service, ensuring the seamless transmission of medical information (especially the “transitional passport”), helping patients get familiar with the new medical team, helping to connect community resources and support organizations, effectively overcoming the convergence barriers caused by system differences, and ensuring medical continuity.50
Continuous supporters, trackers and problem solvers. Nurses are an important pillar for patients and their families in emotional and practical problems during the transition period. They provide continuous psychosocial support, keenly observe the emotional changes of patients, identify signs of anxiety and depression, and timely refer them to psychological experts; At the same time, guide parents to adapt to the role change. Nurses dynamically track the implementation of the transition plan, monitor the treatment compliance and skill mastery progress, and as a “gatekeeper”, intervene to solve sudden difficulties (such as skill barriers, running in with the new team) at the first time to ensure the smooth implementation and timely adjustment of the nursing plan.51 See Figure 1 for relevant contents.
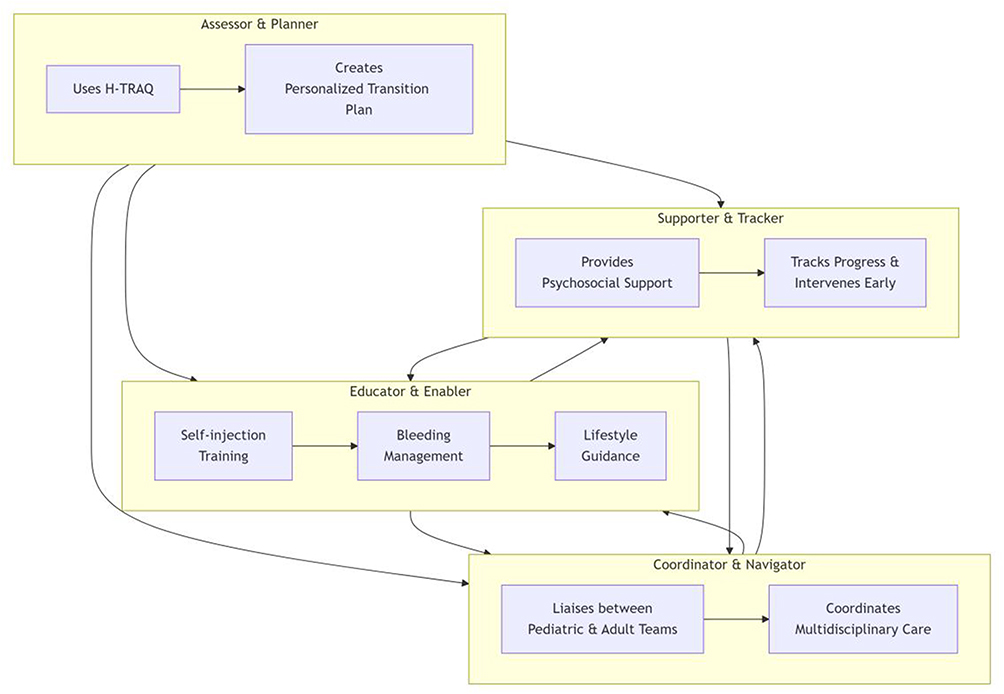 |
Figure 1 The core roles of the nurse in hemophilia transitional care. |
Future Research Directions
In the field of transitional care for hemophilia, the following key research directions still need to be broken through to improve the long-term intervention effect: first, it is necessary to accelerate the clinical transformation of intelligent health technology, focus on the development of integrated digital tools (such as mobile medical app with AI personalized medication reminder, dynamic bleeding record and remote consultation functions), and verify the early warning effect of wearable devices (such as joint activity monitoring sensor) on early joint bleeding, so as to make up for the fault of teenagers’ self-management ability through technological innovation. Secondly, an evidence-based long-term evaluation system should be established. Through more than 10 years’ prospective cohort study, the impact of structured transition plan on patients’ adult joint function, quality of life, utilization rate of medical resources and social participation (employment/schooling rate) should be quantified. Meanwhile, health economics assessment should be carried out to clarify the correlation between transitional nursing investment (such as the post setting of full-time nurses) and reducing the medical cost of long-term complications. In addition, we should pay attention to the fairness and adaptability of intervention strategies, explore the accessibility support mode (such as remote nurse guidance and community collaboration network) for resource deficient areas (such as rural areas and low-income groups) or patients with comorbid mental disorders, and study the localization path of transitional care under different cultural backgrounds and medical systems (such as hierarchical diagnosis and treatment system). This could manifest as a “hub-and-spoke” model with specialist hemophilia nurses from Hemophilia Treatment Centres (HTCs) providing telehealth consultations and supervision, combined with upskilling local healthcare providers at community clinics to deliver basic care, coordinate factor supply, and facilitate peer-to-peer support networks under central guidance. Future work could also focus on the adaptation and implementation science of deploying established, holistic programmes like “Ready Steady Go” within different healthcare and cultural contexts, evaluating their specific impact on hemophilia transition outcomes. Finally, it is urgent to promote the integration of policies and systems, incorporate the core elements of the transition period (such as the role of standardized transition coordinator, pediatric adult joint outpatient process) into the national diagnosis and treatment guidelines, and support the medical insurance payment mechanism to ensure implementation; At the same time, the multi-party cooperation policies of health, education, social security and employer departments (such as occupational protection laws and regulations, campus health plan) are constructed to systematically eliminate the barriers of patients’ social participation and realize the seamless connection of medical and social support.
This review has several limitations inherent to its narrative design. The lack of a systematic protocol and formal quality appraisal of included sources introduces the potential for selection bias. Furthermore, the evidence synthesized predominantly originates from high-income countries and specialized treatment centers, limiting the generalizability of findings to low-resource or geographically remote settings. The absence of pooled quantitative data precludes definitive conclusions on effect sizes. Finally, the rapid evolution of hemophilia treatment, especially regarding novel therapies, means that the long-term transition implications for these patients are not yet fully captured in the current literature.
Conclusion
Transitional care is pivotal for optimizing lifelong health in hemophilia. This review confirms that effective transition requires a systematic, multi-faceted approach. Strong evidence supports the efficacy of structured transition programs, nurse-led skill training (particularly self-infusion for severe patients), and dedicated transition coordinators in improving adherence and clinical outcomes. It is well established that nurses are central as assessors, educators, coordinators, and supporters.
Based on current evidence and expert consensus, future success will depend on integrating digital health tools, establishing long-term outcome data, and developing adaptive models for resource-limited settings. To translate this evidence into practice, strong policy support is needed to standardize transition protocols, formalize the nurse coordinator role, and ensure funding, which is crucial for bridging the gap between pediatric and adult care systems.
Ultimately, the successful implementation of standardized, evidence-based transitional care is the necessary next step to ensure that every young person with hemophilia is empowered to manage their health effectively into adulthood.
Funding
This work was supported by Beijing Research Ward Excellence Program, BRWEP2024W102090112.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Xue, Z, Xue, Y, Zhi, Z. Thrombosis and Hemostasis Group,Chinese Society of HematologyChinese Medical Association;; Hemophilia Treatment Center Collaborative Network of China. [Chinese guidelines on the diagnosis and treatment of acquired hemophilia A (2021)]. Chin J Hematol. 2021;42(10):793–11. Chinese. doi:10.3760/cma.j.issn.0253-2727.2021.10.001
2. World Federation of Hemophilia. Report on the Annual Global Survey 2020: 2021 Available from: https://www1.wfh.org/publications/files/pdf-2045.pdf.
3. Lei Z, He L, Shen YP. Yang renchi Challenges in the management of hemophilia patients in the transition period from children to adults. Chin J Pediatr. 2019;57(6):401–405. doi:10.3760/cma.j.issn.0578-1310.2019.06.001
4. China hemophilia cooperative group. Multicenter investigation report on joint health and quality of life in Chinese hemophilia patients. Chin J Hematol. 2022;43(5):361–368.
5. Blum RW, Garell D, Hodgman CH, et al. Transition from child-centered to adult health-care systems for adolescents with chronic conditions: a position paper of the society for adolescent medicine. J Adolesc Health. 1993;14(7):570–576. doi:10.1016/1054-139X(93)90143-D
6. Soucie JM, Byams VR, Duval DL, et al. Development of a self-management assessment tool for young adults with bleeding disorders: the Adolescent and Young Adult Self-Management Skills Assessment (AYA-SMSA). Haemophilia. 2021;27(3):e362–e371.
7. Van Santen S, Schrijvers LH, Däscher D, et al. Barriers and facilitators in adolescent self-management during transfer to adult care: a multi-stakeholder needs assessment. Patient Educ Couns. 2022;105(7):2283–2290.
8. Srivastava A, Santagostino E, Dogan A, et al. WFH guidelines for the management of hemophilia, 3rd edition. Haemophilia. 2020;26(S6):1–158. doi:10.1111/hae.14046
9. Hastings C, Tobin JN, Kessel R, et al. Mental health needs in adolescents with hemophilia: a mixed-methods study. Pediatr Blood Cancer. 2023;70(3):e30152.
10. Collins PW, Blanchette VS, Fischer K, et al. Break-through bleeding in relation to predicted factor VIII levels in patients receiving prophylactic treatment for severe hemophilia A. J Thromb Haemost. 2009;7(3):413–420. doi:10.1111/j.1538-7836.2008.03270.x
11. Mcdougall CM, Ameratunga R, Robins RS, et al. Transition care continuity in haemophilia: a survey of current practices and barriers. Haemophilia. 2021;27(1):150–158.
12. Thornburg CD, Duncan NA. Adherence to prophylaxis in adolescents with hemophilia: the role of pain, activity limitations, and psychosocial factors. J Pediat Hematol Oncol. 2017;39(4):267–273.
13. American Academy of Pediatrics. Transitioning youth with bleeding disorders to adult care: consensus recommendations. Pediatrics. 2020;145(4):e20200251.
14. Lambert C, Agle S, Wong T, et al. Gaps in communication during the transition from pediatric to adult care in hemophilia: a qualitative study. Haemophilia. 2019;25(3):485–492.
15. O’mahony B, Black C. Expanding Hemophilia Care in Developing Countries: Infrastructure Requirements for Transition Programs. Montreal: World Federation of Hemophilia; 2021:12–18.
16. National Hemophilia Foundation. MASAC Recommendation #263: Guidelines for Transition to Adult Care for People with Bleeding Disorders. New York: NHF; 2022.
17. Cassis FR, Buryagi M, Qureshi A. Role of nurse coordinators in bridging multidisciplinary gaps during hemophilia transition care: a case audit. J Clin Nurs. 2022;31(19–20):2876–2885.
18. Forsyth A, Gregory M, Trippi J, et al. Multidisciplinary coordination deficits in transition care: a 10-country survey. Haemophilia. 2021;27(5):e623–e631.
19. World Federation of Hemophilia. Report on the Annual Global Survey 2023. Montreal: WFH, 2024.
20. Ji MM, Shen YG, Gong JC. Multi center study on regional differences of diagnosis and treatment resources of hemophilia in China. Chin J Hematol. 2023;44(2):112–118. doi:10.3760/cma.j.issn.0253-2727.2023.02.005
21. Zhang L, Li H, Yang R, et al. Economic burden of forced medical migration in hemophilia transition care: a Chinese cohort study. Haemophilia. 2022;28(4):656–663. doi:10.1111/hae.14569
22. Siddiqi S, Scott A, Sohail M, et al. Geographic disparities in transition outcomes: global analysis of rural vs. urban hemophilia care. Lancet Haematol. 2023;10(7):e520–e528.
23. Canadian Hemophilia Society. Guidelines for the Transition From Pediatric to Adult Care in Bleeding Disorders. Montreal: CHS; 2022.
24. Mclimont M, Woods M, Baker J, et al. Impact of phased transition programs on adherence in adolescent hemophilia: a 5-year Canadian cohort study. Blood Adv. 2023;7(14):3529–3537.
25. Hacker MR, Geraghty S, Manco-Johnson M. Development and validation of the Hemophilia Transition Readiness Assessment Questionnaire (H-TRAQ). Haemophilia. 2020;26(1):156–164. doi:10.1111/hae.13897
26. Kumar R, Broderick CR, Barnard JG. Correlation between transition readiness scores and clinical outcomes in youth with bleeding disorders. J Adolesc Health. 2022;71(4):456–462.
27. National Health Service (UK). Haemophilia Transition Passport Template v3.0. London: NHS; 2023.
28. De Kort W, Teepe J, Groen W, et al. Electronic transition passports improve data transfer in haemophilia: a controlled implementation study. Haemophilia. 2021;27(6):e789–e797.
29. UK Hemophilia Centre Doctors’ Organisation. Annual report 2023: transition care outcomes. Manchester: UKHCDO, 2024: 27–29.
30. Canadian Hemophilia Nurse Group. Operational Standards for Dual Pediatric-Adult Clinics in Bleeding Disorders. Toronto: CHNG; 2023:8–12.
31. Chan AK, Curtis R, Bonnemain A, et al. Impact of integrated transition clinics on care continuity: ontario hemophilia network cohort study. Blood. 2024;143(9):789–798.
32. European Hemophilia Consortium. Nursing Protocol for Venipuncture Training in Adolescents with Bleeding Disorders. Brussels: EHC; 2023.
33. Koster RA, Fischer K, Van Den Berg HM, et al. Virtual reality vs. traditional simulation in hemophilia self-injection training: a randomized controlled trial. Haemophilia. 2024;30(1):88–96.
34. Singh A, Mcguinn K, Christie L, et al. Early signs of hemarthrosis: validation of a joint bleeding awareness scale. J Thromb Haemost. 2022;20(7):1671–1679.
35. World Federation of Hemophilia. Physical Therapy Management of Hemarthrosis: Clinical Practice Guidelines. Montreal: WFH; 2022:15–18.
36. National Hemophilia Foundation. Emergency Care Decision Algorithm for Joint Bleeds. New York: NHF; 2023.
37. Ragni MV, Kwon M, Maples KT, et al. Timeliness of hemarthrosis intervention impacts long-term joint outcomes: NHF PROBE study. Blood. 2023;141(11):1320–1329.
38. Srivastava A, Santagostino E, Dogan A, et al. WFH guidelines for the management of hemophilia, 3rd edition. Haemophilia. 2020;26(S6):47–49.
39. European Agency for Safety and Health at Work. Occupational Adaptation Strategies for Chronic Disease Patients. Bilbao: EU-OSHA; 2021:33–35.
40. China nutrition society. Dietary guidelines for hemophilia patients (2022 Edition). Acta Nutraceae Sinica. 2022;44(4):325–330.
41. Gargano C, Cerquetelli C, Mannucci PM, et al. Long-term impact of comprehensive lifestyle intervention on joint damage and employability in hemophilia: Milan cohort study. J Thromb Haemost. 2023;21(9):2468–2477.
42. International Nursing Council for Hemophilia. Peer Support Program Framework for Adolescent Transition. Geneva: INCH; 2022.
43. Jones RK, Patel S, Albornoz LL, et al. Efficacy of structured peer mentoring on psychosocial adaptation in adolescent hemophilia: a controlled trial by UK Haemophilia Society. Haemophilia. 2023;29(4):1021–1030.
44. European Federation of Psychologists Associations. CBT Protocol for Chronic Disease-Related Anxiety and Depression. Brussels: EFPA; 2021:21–25.
45. Müller T, Schröder C, Schneider SC, et al. Long-term effectiveness of CBT for depression in haemophilia transition: a multicentre RCT. Lancet Psychiatry. 2024;11(3):213–223.
46. American Nurses Association. Scope and Standards of Practice for Hemophilia Transition Coordinators [R]. Silver Spring: ANA; 2022:17–21.
47. US Hemophilia Treatment Center Network. 2023 Benchmark report: nurse coordinator outcomes. Washington: HTCN, 2024.
48. American Nurses Association & National Hemophilia Foundation. Nursing Standards for Transition Planning in Bleeding Disorders. Silver Spring: ANA; 2023:11–14.
49. Van Dijk K, Schrijvers LH, Kars MC, et al. Efficacy of nurse-led skill training on self-management Independence in hemophilia: a multicenter RCT. J Adv Nurs. 2024;80(2):621–633.
50. Canadian Collaborative Transition Network. Coordinator Role Framework: Bridging Pediatric and Adult Hemophilia Care. Ottawa: CCTN; 2022:7–9.
51. Liu Y, Zhang Q, Chen W, et al. Longitudinal impact of nurse-led psychosocial support on transition outcomes: a Chinese cohort study. J Pediatric Nurs. 2023;71:e39–e47.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.