Back to Journals » Drug Design, Development and Therapy » Volume 20
Research Progress on the Application and Mechanisms of Baihe Dihuang Decoction in Major Depressive Disorder
Authors Yang L, Wang Y, Wan H ![]() , Feng H, Liu Y, Xue G, Zhi Y, Zhang F, Liu Y, Zhang Z
, Feng H, Liu Y, Xue G, Zhi Y, Zhang F, Liu Y, Zhang Z ![]()
Received 6 November 2025
Accepted for publication 17 December 2025
Published 4 February 2026 Volume 2026:20 579207
DOI https://doi.org/10.2147/DDDT.S579207
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Longlong Yang,1,* Yilong Wang,1,* Hejia Wan,1,* Hao Feng,1,* Yi Liu,1 Guimin Xue,1 Yanle Zhi,1 Fengjiao Zhang,2 Yongsheng Liu,3 Zhiqiang Zhang1
1School of Pharmacy, Henan University of Chinese Medicine, Zhengzhou, Henan, People’s Republic of China; 2School of Food Science, Henan University of Animal Husbandry and Economy, Zhengzhou, Henan, People’s Republic of China; 3Medical Examination Center, Henan Provincial Hospital of Traditional Chinese Medicine (The Second Affiliated Hospital of Henan University of Chinese Medicine), Zhengzhou, Henan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhiqiang Zhang, School of Pharmacy, Henan University of Chinese Medicine, Zhengzhou, Henan, People’s Republic of China, Email [email protected]
Objective: The treatment of major depressive disorder (MDD) is often plagued by inadequate therapeutic efficacy, high relapse rates, and adverse drug effects. Baihe Dihuang Decoction (BHDH, Lily Bulb and Rehmannia Decoction), a classic Traditional Chinese Medicine (TCM) formula, shows promise for depression, but a comprehensive synthesis of modern evidence is warranted. This study aimed to review the clinical efficacy, pharmacological mechanisms, and safety profile of BDD for MDD to inform its clinical application and guide future research.
Methods: A systematic literature search was conducted in both English (PubMed, Web of Science) and Chinese (CNKI, Wanfang) databases from inception to June 2025. For clinical evidence, the search focused on “Baihe Dihuang Decoction”, “major depressive disorder/depression”, and “randomized controlled trial”. Supplementary searches using terms like “chemical constituents” and “pharmacological action” were performed for mechanistic studies. Relevant literature was subsequently summarized and analyzed.
Results: Current evidence suggests that BHDH, as an adjunct to conventional antidepressants, can improve the overall clinical response rate, reduce Hamilton Depression Rating Scale scores, and potentially alleviate adverse reactions. Its active constituents may exert antidepressant effects via multiple pathways, including monoaminergic neurotransmission modulation, neuroinflammation inhibition, hypothalamic-pituitary-adrenal axis regulation, hippocampal neuron protection, and gut microbiota modulation. However, its efficacy as a monotherapy and long-term safety profile require further validation through high-quality clinical trials.
Conclusion: BHDH possesses a multi-target pharmacological basis for antidepressant activity. Existing clinical evidence supports its effectiveness and relative safety as an adjunctive therapy for MDD. To better define its clinical role and advance TCM modernization, future research should prioritize rigorous randomized controlled trials, elucidate its formula compatibility mechanisms, and identify its key bioactive components.
Keywords: Baihe Dihuang decoction, history of development, chemical composition, major depressive disorder, mechanism of action
Introduction
Major depressive disorder (MDD) is primarily characterized by a persistently low mood, often accompanied by a loss of interest, emotional distress, low self-esteem, appetite loss, sleep disturbances, and other clinical manifestations. In severe cases, it may even lead to suicidal tendencies, making it one of the most common types of mental illness. The onset of MDD is complex and results from the interplay of multiple factors, including social, familial, and life circumstances. Individuals who have experienced childhood abuse, severe financial losses, or other adverse events are at a higher risk of developing MDD. Additionally, challenges in school and the workplace can also contribute to its onset.1 Although psychological therapies and medications are available for MDD, these treatments are often inaccessible or nonexistent in developing countries and impoverished regions. MDD has become the fourth leading disease worldwide, imposing a significant economic and social burden.2
Currently, several major theories or hypotheses have been proposed, including the monoamine hypothesis, inflammation and oxidative stress response, the hypothalamic-pituitary-adrenal (HPA) axis, reduced synaptic plasticity, secretion disorders of neurotrophic factors, and the microbiota-gut-brain (MGB) axis.3 Among these, the monoamine hypothesis is widely regarded by many scholars as a key mechanism underlying MDD.4 It suggests that an abnormal reduction in monoamine neurotransmitters-such as serotonin (5-HT), norepinephrine (NE), and dopamine (DA)-within synapses in the central nervous system is closely associated with the onset of MDD.5 Clinically, selective serotonin reuptake inhibitors (SSRIs), including fluoxetine, paroxetine, and sertraline, are commonly prescribed. While these medications provide therapeutic relief to some extent, prolonged use may lead to side effects and even suicidal tendencies in severe cases.6 Current clinical studies suggest that TCM formulas may not only help reduce patients’ excessive sensitivity to environmental stimuli but also alleviate certain symptoms associated with major depressive disorder. For instance, multiple randomized controlled trials have indicated that specific TCM compound formulations can demonstrate efficacy comparable or complementary to conventional antidepressants in improving particular symptom dimensions or quality-of-life indicators.7 Nevertheless, the overall body of evidence still requires further validation and integration. Taking BHDH as an example, the modern clinical and basic research evidence for such classic formulas has yet to be systematically synthesized, which obscures their specific mechanisms of action and clinical positioning. Therefore, this review systematically examines the historical origins, clinical efficacy, pharmacological mechanisms, and safety profile of BHDH, assesses the strengths and limitations of the current evidence, and aims to clarify the existing research landscape while informing future key research priorities.
Baihe Dihuang Decoction Historical Records
Within the theoretical framework of TCM, depression is primarily categorized as “Yu Syndrome”. Its core pathogenesis is considered to be emotional stagnation leading to Qi mechanism obstruction, which may subsequently result in dysfunction of the Zang-fu organs. Guided by TCM principles of syndrome differentiation and treatment, the management of Yu Syndrome typically focuses on key organs such as the liver, heart, and spleen. For instance, the initial stage often presents as liver Qi stagnation, manifesting as emotional depression and a sensation of distension in the chest and hypochondriac regions. If this stagnation persists and transforms into fire, it may disturb the heart spirit, leading to symptoms like irritability and insomnia. Furthermore, if liver stagnation affects the spleen’s transport function, symptoms such as poor appetite, fatigue, and excessive rumination may occur. This holistic perspective, centered on “Zang-fu differentiation”, provides the theoretical rationale for TCM interventions in depression. These interventions aim to soothe the liver and relieve stagnation, nourish the heart to calm the mind, and strengthen the spleen to resolve phlegm.8
Guided by this theoretical framework, clinical studies suggest that Chinese herbal formulas may not only help reduce patients’ hypersensitivity to environmental stimuli but also alleviate specific symptoms of major depressive disorder (eg, depressed mood, insomnia, and reduced appetite, which correspond to the manifestations of Yu Syndrome). Multiple studies indicate that certain classic herbal formulas demonstrate efficacy comparable or complementary to conventional antidepressants in improving depressive mood, sleep quality, and quality of life. 7 Nevertheless, current research is often limited by small sample sizes and methodological shortcomings, making it difficult to fully define the precise role of Chinese herbal medicine within comprehensive depression treatment plans. Therefore, large-scale, high-quality clinical trials are urgently needed to validate these findings.
Among numerous Chinese herbal formulas for treating depression, BHDH has a long history of medicinal use, originating from Jingui Yaolue (Essential prescriptions from the golden cabinet), written by Zhang Zhongjing during the Eastern Han dynasty. The text states: “For Baihe disease that has not been treated with emesis, purgation, or diaphoresis and remains unchanged, BHDH decoction is the primary remedy”. Later, during the Tang dynasty, Sun Simiao also documented this formula in Beiji Qianjin Yaofang (Essential prescriptions worth a thousand gold), maintaining both its name and therapeutic indications.
Usage of BHDH Decoction
The term “Baihe Disease” first appeared in Jin Kui Yao Lue (Synopsis of Prescriptions of the Golden Chamber), a classical text attributed to the Eastern Han dynasty physician Zhang Zhongjing (c. early 3rd century CE), where it was described as a distinct clinical entity. The disease is named after its core therapeutic herb, the lily bulb (Baihe), highlighting the herb’s central role in its treatment. The original text characterizes the condition with symptoms such as: “desiring food but being unable to eat, often remaining silent; wanting to lie down but finding no rest; wishing to move but being unable to walk; at times having an appetite, yet at other times being repelled by the smell of food; a sensation of cold without true cold, and of heat without true heat; a bitter taste in the mouth, and dark-colored urine. as if influenced by a spiritual presence”. According to ancient medical theory, its pathogenesis was attributed to “lingering residual heat after a febrile illness” or “emotional constraint leading to stagnation, which subsequently transforms into fire”. This pathological process results in a state of yin deficiency with internal heat affecting the heart and lungs. The core manifestations of Baihe Disease—persistent dysfunction in emotion, behavior, sensation, and somatic function—exhibit notable overlap with modern diagnostic categories such as MDD, anxiety disorders, and somatic symptom disorders. Consequently, the pathogenesis framework of “yin deficiency with internal heat in the heart and lungs” provides a foundational TCM theoretical model for diagnosing and treating these conditions. The formula BHDH embodies the corresponding therapeutic principle of “nourishing yin, clearing heat, and calming the heart to tranquilize the mind”, standing as the classic prescription exemplar for this specific pattern.
The naming of the formula Baihe Dihuang Decoction (Lily Bulb and Rehmannia Decoction) directly originates from its classical documentation in Jin Gui Yao Lüe (Essentials from the Golden Cabinet), which specifies “seven lily bulbs” and “fresh rehmannia juice”. This record not only establishes the sovereign herbs but also prescribes a unique preparation process. The key steps include: “seven lily bulbs. wash the lily bulbs with water, soak overnight until white foam appears, discard the water, then add two sheng of spring water, decoct until one sheng remains, remove the dregs, and add the rehmannia juice”. Modern pharmacological research provides a scientific basis for these traditional procedures.9–11 First, the white foam that appears after soaking the lily bulbs is related to their colchicine content; this step aims to reduce the level of this component, as while colchicine can be used to treat gout, long-term intake may cause adverse reactions.11 Second, the requirement to use fresh rehmannia juice is due to its rich catalpol content, which is sensitive to pH and can undergo chemical changes in the body. This explains the normal phenomenon of possible darkening of stool after taking the decoction.12 These findings indicate that the traditional preparation details not only reflect the empirical understanding of medication safety by ancient practitioners but also provide important practical references for modern pharmaceutical research and process optimization.
Functions and Indications
According to ancient texts, BHDH decoction has the effects of clearing heat, nourishing yin, and tonifying the heart and lungs. Lily bulb is known for its functions of clearing the heart, calming the mind, moistening the lungs, and nourishing yin. R. glutinosa is recognized for its ability to clear heat, generate fluids, and cool the blood.13 When used together, these two herbs work synergistically to nourish yin, tonify the heart and lungs, and clear the heart to calm the mind. In modern clinical practice, this formula is primarily used to treat yin deficiency with internal heat affecting the heart and lungs, presenting symptoms such as restlessness, insomnia, disordered eating, and a bitter taste in the mouth. It is widely applied in the treatment of insomnia, MDD, anxiolytic, antitumor and mood disorders (Figure 1), including menopausal syndrome in women.14
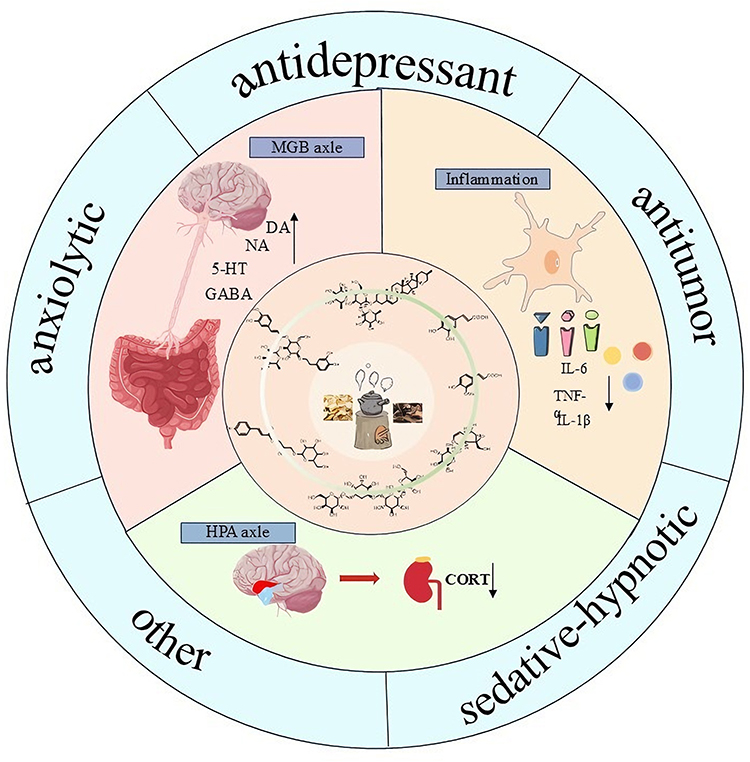 |
Figure 1 Pharmacological Activity of BHDH. |
Chemical Composition of BHDH Decoction
Chemical Components in Lily Bulb
Modern pharmacological studies of TCM have identified a range of active components in lily bulbs. The main components extracted include lily polysaccharides, steroidal saponins, alkaloids, flavonoids, and phenolic compounds. Among these, steroidal saponins are the key active components responsible for the decoction’s sedative and hypnotic effects, as well as for regulating gut microbiota and 5-HT, thereby exerting antidepressant properties.15 Lily polysaccharides, flavonoids, and phenolic compounds also possess antioxidant effects, helping to neutralize free radicals. Additionally, oxidative stress has been widely recognized as a key factor in the development of symptoms such as depression and insomnia.
Polysaccharides
The primary active components in lily bulbs are polysaccharides, which possess biological activities such as immune regulation, antioxidation, blood glucose reduction, anti-aging, and anti-tumor effects.16
Steroidal Saponins
Currently, all saponins extracted and isolated from lily bulbs are steroidal saponins. A total of 53 types have been identified in the Lilium genus (Supplementary Table 1 and Supplementary Figure 1).
Phenolics
Genus Lilium contains abundant phenolic compounds, which represent a major class of bioactive components in this genus (Supplementary Table 2 and Supplementary Figure 2A).
Flavonoids
Currently, 13 flavonoids have been extracted from lily bulbs, including (+)-catechol, rutin, dihydromyricetin, eriodictyol, myricetin, quercetin, etc. (Supplementary Table 3 and Supplementary Figure 2B).
Alkaloids and Other Components in Lily Bulb
Alkaloids are also one of the active components in lily bulb. Currently, 11 alkaloids have been extracted (87~101), including 3 steroidal alkaloids (Supplementary Table 4 and Supplementary Figure 3).
Components From R. Glutinosa
R. glutinosa here refers to its fresh or dried tuber. Its chemical components include iridoid glycosides, polysaccharides, phenylethanol glycosides, etc. Modern pharmacological studies have shown that R. glutinosa has effects such as lowering blood sugar, improving the central nervous, anti-tumor properties, delaying aging, and exhibiting antibacterial activity.84
R. Glutinosa Polysaccharides
R. Glutinosa polysaccharides (RGPs) are one of the primary bioactive components in R. glutinosa. demonstrating significant effects in anti-inflammatory, antioxidant, blood sugar-lowering, and neuroregulatory activities, with no reports of significant toxicity.85
Iridoids in R. Glutinosa
Iridoids are the most abundant compounds in R. glutinosa, with Catalpols being the main active components (Supplementary Table 5 and Supplementary Figure 4).
Ionones From R. Glutinosa
The ionones in R. glutinosa are primarily composed of monoterpenes and sesquiterpenes. The hydroxyl group at position 5 can form glycosides with glucose and other sugars (Supplementary Table 6 and Supplementary Figure 5A).
Phenylethanol From R. Glutinosa
The phenylethanol compounds in R. glutinosa mainly exist as glycosides. Acteoside is a representative compound and serves as a key component in R. glutinosa (Supplementary Table 7 and Supplementary Figure 5B).
Triterpenoids and Flavones From R. Glutinosa
Triterpenoids and flavones in R. glutinosa are primarily found in the leaves. The triterpenoids and flavones that have been isolated and identified from R. glutinosa are shown in the figure below (Supplementary Table 8 and Supplementary Figure 6).
Lignans and Phenolic Acids From R. Glutinosa
The lignans and phenolic acids from R. glutinosa are shown in the table below (Supplementary Table 9 and Supplementary Figure 7).
Alkaloids and Other Classes From R. Glutinosa
In addition to the components mentioned above, R. glutinosa contains various other types of components, such as alkaloids, amino acids, volatile oils, and inorganic elements (Supplementary Table 10 and Supplementary Figure 8).
Component Analysis of BHDH Decoction
Regarding the active components of the BHDH decoction, Hu et al Employed “multi-site component profile characterization - multi-index efficacy integration - multi-dimensional data analysis” to identify the intersection of active components with antidepressant effects in the decoction.86 The potential pharmacologically active components were confirmed through in vitro cell viability assays, revealing that compounds such as regaloside A, B, C, catalpol, and isoacteoside may be the main active substances underlying its antidepressant effects. Peng et al used the TCMIP database to explore the active components of the BHDH decoction. A total of 12 components from lily bulb were collected, mostly saponins, and 38 components from R. glutinosa, including iridoid glycosides and amino acids.87 Research findings indicated 10 active components associated with antidepressant activity: 4 from lily bulb, including regaloside D, steroidal saponins, lily glycoside C, and 6-O-β-D-Glucopyranosyl-3β,26-dihydroxy-Δ5-cholesten-16,22-dione-3-O-α-L-mnopyranosyl-(1→2)-β-D-glucopyranoside. In addition, other 6 components from R. glutinosa include glutamic acid, L-arginine, xanthostrumarin, adenosine, mannosaccharide, and sucrose. Mao et al used LC-MS to qualitatively analyze the difference in the chemical component between single decoction and combined (BHDH) decoctions.88 The results indicated that the decoction of lily bulb contained 35 chemical compounds, while that of fresh R. glutinosa contained 36 components. In the BHDH decoction, 69 chemical components were found, including 16 organic acids, 6 sugars and glycosides, 8 amino acids and peptides, and 3 alkaloids (Table 1 and Supplementary Figure 9).
Understanding of MDD From the Perspective of TCM
From the perspective of TCM, MDD falls under the categories of “emotional disorders” and “stagnation diseases”. Throughout history, TCM literature has documented it under various terms such as “epileptic disorders”, “stagnation disorders”, and “Baihe disease”.89 As early as the Spring and Autumn period, the Huangdi Neijing (Yellow Emperor’s Inner Canon) documented the relationship between emotions and the five organs, and based on the Five Elements Theory, it proposed the treatment method of “joy overcoming sadness”. Similarly, in Shennong Bencaojing, herbs such as “Fu Yi” and “He Huan” are noted as treatments for MDD. Later, during the Eastern Han Dynasty, Zhang Zhongjing in the Jingui Yaolue recommended the use of BHDH decoction to treat “Baihe disease”. “Baihe disease”, attributing the main causes of the disease to the heart and lungs. In TCM, the heart is seen as the ruler of the body, governing the blood vessels, while the lungs are considered the assistant, responsible for circulating energy through the vessels. When heat affects both, it causes the vessels to overheat (Figure 2). Clinically, disturbances in eating, sensory functions, sleep, and behavior are commonly observed, which resemble the clinical symptoms of MDD. Today, BHDH decoction and its modified formulas, or a combination with antidepressant Western drugs, are frequently used to treat MDD triggered by various causes, with significant clinical success.
 |
Figure 2 BHDH for depression in Traditional Chinese Medicine Theory. |
Summary of Clinical Evidence for BHDH in Treating Depression
Prior to exploring the fundamental pharmacological mechanisms of Baihe BHDH, a systematic evaluation of its clinical evidence is essential to clarify its therapeutic position. This section synthesizes findings from existing randomized controlled trials (RCTs) and meta-analyses, focusing on its efficacy and safety profile as an adjunctive therapy for depression.
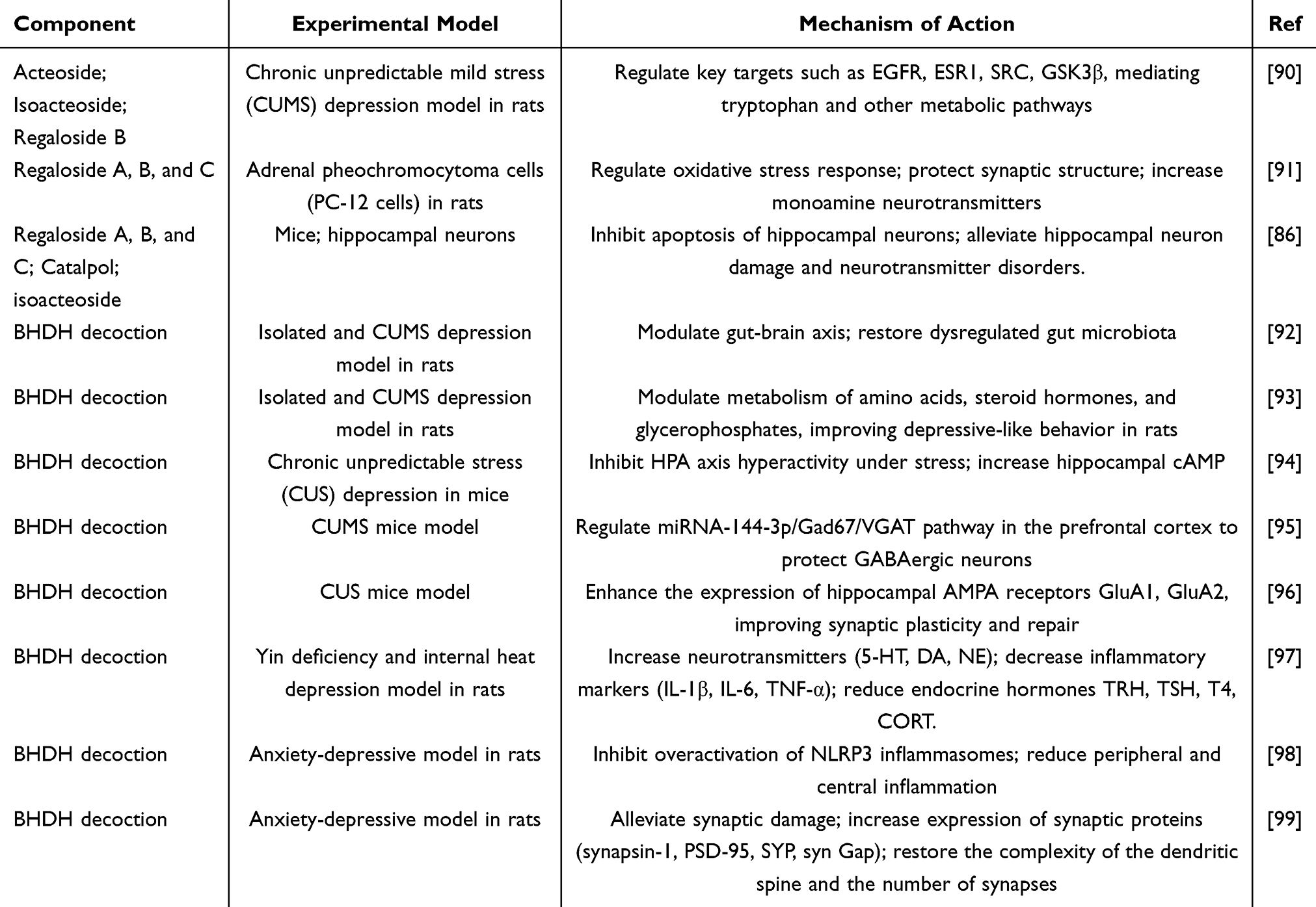 |
Table 1 Research on the Mechanisms of Baihe Dihuang Decoction in Treating Depression |
A 2022 systematic review and meta-analysis, which included 13 RCTs (up to March 2021) involving 878 patients with depression (451 in BHDH combination groups, 427 in control groups), provides the highest level of current evidence.100 While informative, this analysis acknowledges limitations such as the modest number of studies and heterogeneity among them, underscoring the need for future large-scale trials.
Clinical Efficacy Evidence
As shown in Table 2, available clinical studies consistently report that combining BHDH with conventional antidepressants (eg, SSRIs) is associated with improved therapeutic outcomes compared to antidepressants alone.
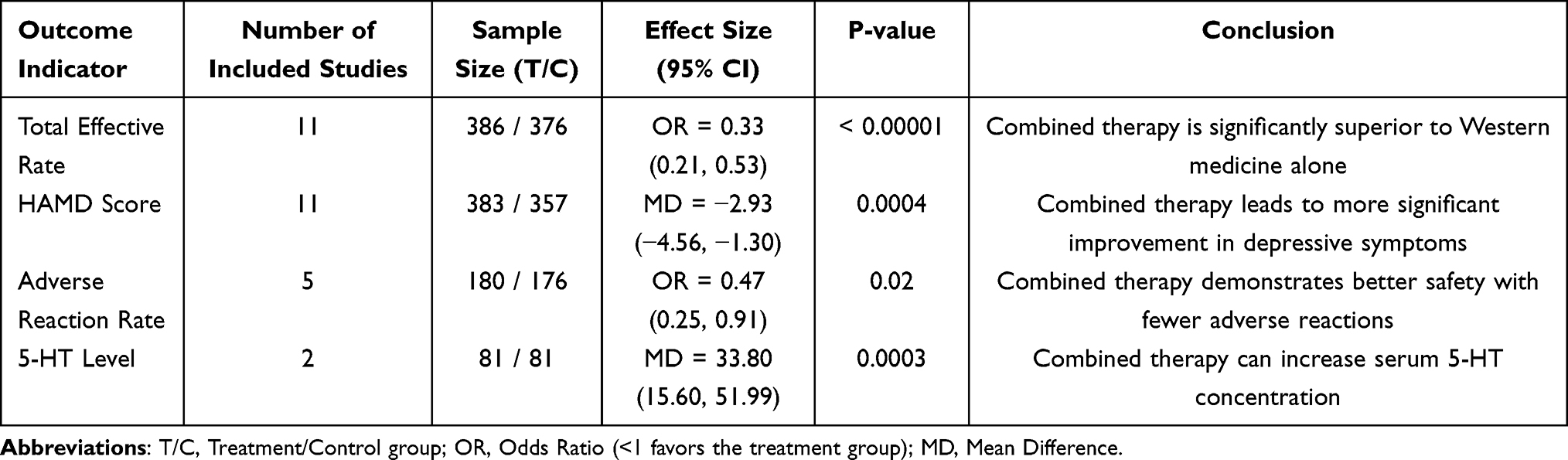 |
Table 2 Summary of Meta-Analysis on Key Clinical Outcome Indicators for Baihe Dihuang Decoction Combined with Conventional Western Medicine in Treating Depression |
Overall Efficacy: Meta-analysis results indicate a significantly higher total effective rate for the combination therapy versus antidepressant monotherapy (OR = 0.33, 95% CI: 0.21–0.53).100
Core Symptom Improvement: The Hamilton Depression Rating Scale (HAMD) is a primary endpoint for assessing depression severity. The combination regimen demonstrated a greater reduction in HAMD scores (Mean Difference, MD = −2.93), suggesting enhanced efficacy in alleviating core symptoms like depressed mood and anhedonia.100
Secondary Outcomes and Biomarkers: Some studies evaluated additional scales (eg, for anxiety, somatic symptoms, sleep) and neurochemical indicators. Positive trends were observed for improving comorbid anxiety, sleep disturbances, and quality of life. Notably, combination therapy significantly increased peripheral blood levels of 5-HT and NE, providing a potential biochemical correlate for its clinical effects that aligns with the monoamine hypothesis of depression.100
Safety Evidence
Safety is a critical consideration in treatment evaluation. Pooled data from meta-analyses suggest that adding BHDH may improve the tolerability profile of antidepressant regimens.
Adverse Event Incidence
A pooled analysis from five studies reporting adverse reactions found a significantly lower overall incidence in the BHDH combination group versus the antidepressant-alone group (OR = 0.47, 95% CI: 0.25–0.91).100 Common adverse events (eg, nausea, constipation, dizziness, drowsiness) occurred with relatively lower frequency in the combination group.
Analysis of Potential Safety Benefits
This observed safety advantage may be attributed to several factors: (1) The multi-target modulation by BHDH may allow effective treatment with lower doses of concomitant antidepressants, potentially reducing dose-dependent side effects. (2) The TCM actions of BHDH, described as “nourishing yin and clearing heat”, may help counteract certain side effects of Western medicine, such as dryness and agitation. However, the observation period in most included studies was relatively short (2–8 weeks), highlighting the need for long-term safety and follow-up data in future research.
Evidence Summary and Research Prospects
In summary, current clinical evidence supports the use of BHDH as an adjunctive therapy to conventional antidepressants, demonstrating advantages in improving response rates, enhancing core symptom reduction, and potentially lowering the incidence of adverse reactions. These clinical benefits are corroborated by favorable changes in relevant neurochemical biomarkers. These findings establish a clear clinical rationale for investigating BHDH’s pharmacological mechanisms, such as neurotransmitter modulation, neuroinflammation inhibition, and hippocampal neuroprotection, which are discussed in subsequent sections.
Future research should prioritize rigorously designed, large-sample, long-term, high-quality RCTs. Key areas of focus should include evaluating BHDH’s efficacy across different depression subtypes, its effectiveness as a monotherapy, and its long-term safety profile.
Mechanism of Action of BHDH Decoction in Treating MDD
Currently, the antidepressant effects of BHDH decoction are primarily associated with the nervous system, endocrine system, and immune-inflammatory response. Pan and Pan et al have developed models of MDD characterized by Yin deficiency and internal heat to investigate the therapeutic mechanisms of BHDH decoction. The results indicate that BHDH decoction can significantly improve symptoms of Yin deficiency and internal heat-type MDD, further confirming that its antidepressant action is linked to its ability to regulate pathways in the nervous system, endocrine system, and immune-inflammatory response, contributing to its therapeutic effects.101
Regulation of the Nervous System
Regulation of Amino Acid Metabolism
Small molecule amino acids such as tryptophan (Trp), tyrosine (Tyr), glutamate (Glu), and γ-aminobutyric acid (GABA) are essential neurotransmitters in the human body.102 Among them, Trp is an indispensable amino acid that cannot be synthesized by the human body and must be obtained through food and produced by the gut microbiota. The metabolism of Trp primarily involves the pathways of 5-HT and kynurenine (KYN). Increasing 5-HT is crucial for treating MDD, as it is predominantly synthesized by chromaffin cells in the intestinal epithelium. Trp is converted into 5-HT by tryptophan hydroxylase (TPH). Additionally, Trp can also follow the KYN pathway, where part of it is converted into neurotoxic quinolinic acid (QA) within microglial cells. An increase in QA can contribute to the onset of MDD. Another portion of Trp is converted into the neuroprotective kynurenic acid (KA) within astrocytes. KA regulates the production of glutamine (Gln), which is then converted into Glu. As an excitatory neurotransmitter in the brain, Glu is further converted into GABA, an inhibitory neurotransmitter, under the action of the rate-limiting enzyme glutamate decarboxylase (GAD). The Glu/GABA ratio, within an optimal range, can enhance learning and memory. However, if this ratio becomes too high, it may cause inhibitory effects and lead to memory impairment and the development of MDD.103
Feng et al investigated the effects of BHDH decoction on the serum and fecal metabolomics of depressed rats. The results indicated that amino acid metabolism plays an important role in both the onset and treatment of MDD.92 Mou combined network pharmacology and metabolomics and conducted a comprehensive analysis of the mechanisms by which BHDH decoction treats MDD. One of the findings indicated that this mechanism is related to amino acid regulation.90 Based on metabolomics, Hu et al explored the mechanisms of BHDH decoction in treating MDD. Their results revealed that the levels of Trp, KYN, and other metabolites were abnormal in the rats of the model group (Figure 3).
 |
Figure 3 The antidepressant mechanism of BHDH decoction through the regulation of Trp. Abbreviations: TPH1, Tryptophan hydroxylase; 5-HTP, 5-Hydroxytryptophan; IDO1, Indoleamine 2,3-dioxygenase 1; IDO, Indoleamine 2,3-dioxygenase. |
The miRNA-144-3p/Gad67/VGAT Pathway in the Protective Effect of BHDH Decoction on GABA Damage in Neurons
Pan investigated the protective effect of BHDH decoction-containing serum on corticosterone (CORT)-induced neuronal damage and explored whether the mechanism was related to correcting the imbalance between excitatory and inhibitory neurotransmitters.97 The results showed that BHDH decoction increased the expression of VGAT and Gad67 proteins and genes, promoted GABA synthesis and transport, increased GABA expression, restored the imbalance, and improved GABA damage in CORT-induced Neuro-2a neurons. In addition, Xue conducted experiments in mice to confirm that the antidepressant effects of BHDH decoction were linked to the restoration of GABAergic interneuron dysfunction in the prefrontal cortex. The findings revealed that BHDH decoction reduced the expression of miRNA-144-3p in the prefrontal cortex, increased the expression of Gad67 and VGAT, affected presynaptic GABA synthesis and transport, enhanced GABA release, improved synaptic transmission efficiency, and restored the function of GABAergic neurons in receiving and encoding output information, thereby exerting its antidepressant effect.95 Therefore, the miRNA-144-3p/Gad67/VGAT pathway plays a role in the protective effects of BHDH decoction-containing serum against CORT-induced impairment of GABA expression.
Enhance the Levels of 5-HT, DA, NE, and Other Monoamine Neurotransmitters in the Brain
Studies have shown that monoamine neurotransmitters like DA, 5-HT, and NE are crucial in maintaining the chemical balance within the brain. If these substances are either too high or too low, they can lead to the development of MDD.104 Xue investigated the antidepressant mechanism of BHDH decoction using CUMS combined with isolation rearing to establish a depression model in rats.105 The results indicated that the levels of 5-HT, DA, and NE in the hippocampus of the treatment group were significantly higher than those in the model group, while the activity of monoamine oxidase was significantly reduced. This suggests that BHDH decoction regulates the nervous system by reducing the activity of monoamine oxidase in the brain, thereby increasing the levels of monoamine neurotransmitters and exerting antidepressant effects.
Regulation of the Endocrine System
Steroid hormones include two categories: sex hormones and adrenal cortex hormones. Among them, the adrenal cortex hormones involved in the HPA axis play an important role in the pathophysiology of MDD. Studies have shown that in patients with MDD, dysfunction of the HPA axis leads to the secretion of corticotropin-releasing hormone (CRH) from the hypothalamus, which then stimulates the release of adrenocorticotropic hormone (ACTH) from the pituitary. ACTH, carried through the bloodstream, stimulates the adrenal cortex to release cortisol (COR), resulting in elevated levels of CRH, ACTH, and COR in the plasma.106 As a stress hormone influenced by the HPA axis, COR plays a key role in coordinating various physiological processes. However, excessive levels of COR can lead to cognitive impairments and negative emotions.107 Guan et al investigated the effects of BHDH decoction on a mouse model of depression induced by social isolation and CUMS. The results revealed that, compared to the model group, both high and low doses of BHDH decoction significantly reduced the levels of CORT and ACTH in the serum of mice, thereby preventing HPA-axis hyperactivity and alleviating depressive symptoms.108
Regulation of the Immune-Inflammatory Response
Immune-inflammatory response plays a critical role in the pathogenesis of MDD. Experimental and clinical studies have shown that immune-inflammatory responses contribute to MDD by enabling immune cells to release a variety of immune factors into the blood-brain barrier. This activation triggers an immune response within the brain, causing disruptions in specific brain regions and eventually leading to the development of MDD.109 Experimental research has demonstrated that many MDD patients, even without other diseases, experience increased levels of inflammatory factors such as IL-1, IL-6, and TNF-β. Additionally, certain pro-inflammatory immunotherapy has been found to induce varying degrees of MDD.110 Jia et al found that elevated levels of IL-2 in MDD patients contribute to the exacerbation of MDD.111 Zhao et al discovered that the levels of IL-1β and IL-6 were elevated in brain regions associated with lipopolysaccharide (LPS) stress in mice.112 Additionally, LPS induced more severe depressive-like behaviors compared to the CUMS model. Therefore, IL-1β, IL-6, and IL-4 can serve as indicators for assessing the severity of MDD in patients. Liu et al constructed a network of active components and key targets of BHDH decoction, discovering that it may exert therapeutic effects on severe MDD through the release of IL-6.113 Wang explored the impact of BHDH decoction on changes in IL-4 within the serum of depression model in rats. The results showed that the serum IL-4 in the model group was significantly lower than those in the control group, while the serum IL-4 in the treatment group was significantly higher.1 Zhou observed the effects of BHDH decoction on CUMS rats and found that BHDH decoction could significantly improve depression-like behaviors in CUMS rats by downregulating serum IL-1β (Figure 4).
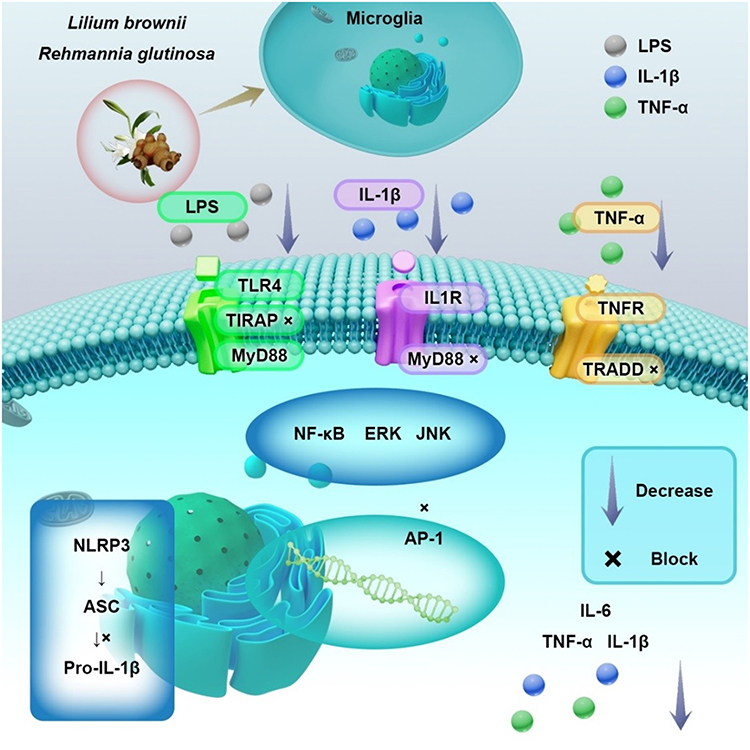 |
Figure 4 BHDH decoction regulates the immune system for antidepressant effects. Abbreviations: TLR-4, Toll-like receptor 4; TIRAP, Toll/interleukin-1 receptor (TIR) domain-containing adapter protein; IL1R, Interleukin-1 receptor; MyD88, Myeloid differentiation primary response 88; TNFR, Tumor necrosis factor receptor; TRADD, TNFR-associated death domain protein; ERK, Extracellular signal-regulated kinase; JNK, c-Jun N-terminal kinase; AP-1, Activator protein-1; NLRP3, NOD-like receptor family pyrin domain-containing 3; ASC, Apoptosis-associated speck-like protein; Pro-IL-1β, Pro-interleukin-1β. |
Antidepressant Effects by Modulating the MGB Axis
It is well established that MDD is often accompanied by a loss of appetite and gastrointestinal dysfunction, which leads to malnutrition and weakened immunity, thus further exacerbating depressive symptoms. Research has shown a close relationship between the gut microbiota and MDD, with MGB dysfunction being one of the primary causes of the condition Research progress of microecological food in improving depression by regulating the Gut microbiota.114 Disruption of the gut microbiota results in changes in the diversity and abundance of bacterial species. For example, in MDD patients compared to healthy individuals, the abundance of Bacteroides is increased, while the abundance of Blautia and Eubacterium is reduced, disturbing the balance between symbiotic and pathogenic bacteria.115 This imbalance undermines the integrity of the gut barrier, triggering an inflammatory response that allows harmful substances to enter the bloodstream and, through the vagus nerve, the central nervous system. This, in turn, induces inflammation and neuronal damage and contributes to the development and progression of MDD. Additionally, the metabolic products arising from gut dysbiosis, such as short-chain fatty acids (SCFAs) and 5-HT, affect the brain and can precipitate MDD. Furthermore, the gut microbiota can influence the HPA axis, adding another mechanism through which MDD is triggered.116
Feng et al investigated the relationship between the antidepressant effects of BHDH decoction and the gut microbiota.93 They administered BHDH decoction to rat models of MDD induced by isolation rearing and CUMS. The results revealed that, compared to the model group, the treatment group showed varying degrees of repair in the colon mucosa and also reversed the gut microbiota imbalance, increasing the abundance of Bacteroides, Lactobacillus, and Bacillus species. Through an in vitro study of the antidepressant effects of BHDH decoction based on the gut microbiota and PC12 cells, Wei tested low, medium, and high concentrations of BHDH decoction on healthy rats and rat models of MDD induced by CUMS and isolation rearing.117 The gut microbiota was cultured in vitro and counted. The results showed that, except for the low-dose group, which showed no significant difference, the other BHDH decoction-treated groups suppressed the growth of Escherichia coli, Enterococcus faecalis, Bacteroides fragilis, and Bifidobacterium, while promoting the growth of Lactobacillus (Figure 5). Ma et al through their research on the mechanisms of BHDH decoction and its active components in the gut-brain axis against MDD, found that the primary ingredient, acteoside, could reverse gut microbiota dysbiosis and inhibit the inflammatory response caused by impaired intestinal permeability or blood-brain barrier leakage, thus achieving therapeutic effects for MDD.118
 |
Figure 5 Antidepressant mechanism of BHDH decoction in regulating gut microbiota. Abbreviations: SCFAs, short-chain fatty acids. Notes: Microbial taxa annotation: Genus names followed by “spp.” indicate representative species within that genus. Bacteroides spp. are core commensals involved in polysaccharide metabolism; Eubacterium spp. are butyrate producers supporting gut barrier function; Blautia spp. are acetate producers linked to metabolic and immune modulation. |
Conclusion
MDD imposes a substantial burden on individuals and society, for which both modern medicine and TCM offer valuable therapeutic perspectives. The classic formula BHDH, first recorded by Zhang Zhongjing during the Eastern Han Dynasty for treating “Baihe Disease”, aligns closely with modern diagnostic criteria for MDD. This alignment provides a historical and theoretical foundation for its modern application, which is supported by contemporary clinical evidence.
Current pharmacological research indicates that BHDH may intervene in MDD through multiple pathways, including modulation of the nervous, endocrine, and immune-inflammatory systems as well as the gut microbiota (Figure 6). This multi-target action is consistent with TCM’s holistic view of “multi-component, multi-target, multi-pathway” therapy. However, the research landscape reveals significant imbalances: while evidence regarding neurotransmitter regulation and HPA axis modulation is relatively robust, investigations into neuroinflammation and the gut-brain axis remain preliminary and lack conclusive evidence chains.
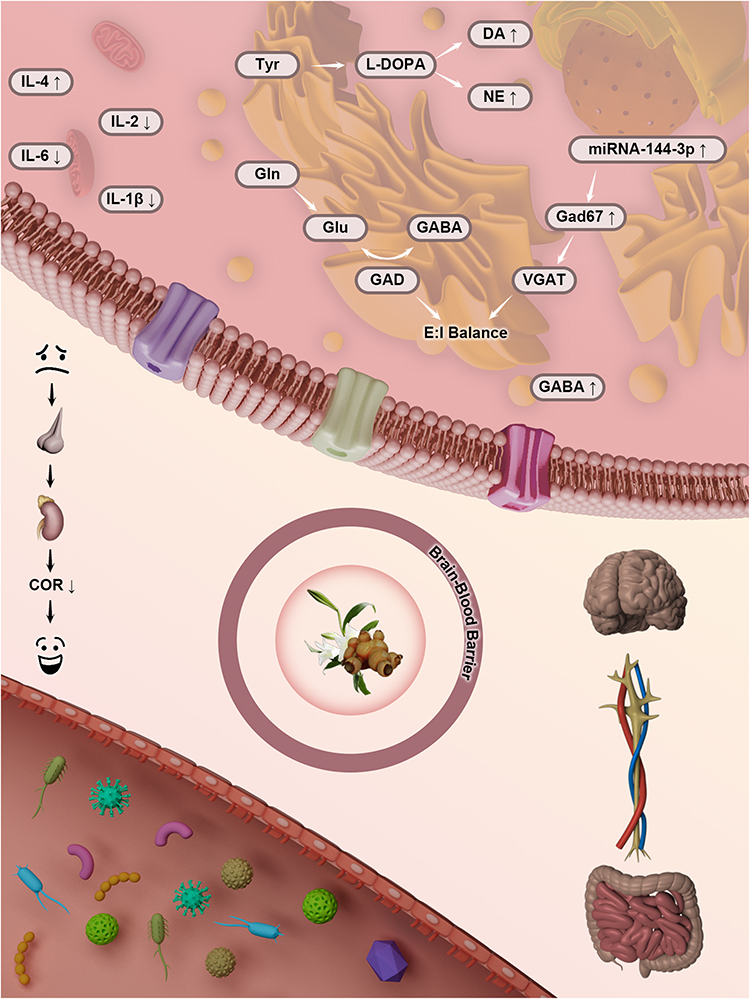 |
Figure 6 Mechanism of antidepressant action of BHDH decoction. |
More critically, fundamental limitations impede the translation of BHDH from potential to definitive application. First, mechanistic studies often remain at the level of correlation, lacking exploration of precise molecular targets and causal pathways. Second, research tends to be fragmented, focusing on individual herbs or compounds rather than elucidating the formula’s synergistic effects. Finally, a major translational gap exists; most mechanistic findings derive from animal models, with insufficient validation using biological samples from MDD patients. This creates considerable uncertainty for clinical application.
Addressing these gaps requires focused future efforts: 1) employing advanced technologies to establish causal mechanisms beyond correlation; 2) adopting systems biology approaches to construct integrated “component-target-pathway-disease” networks that explain the formula’s holistic nature; 3) establishing a translational research framework that incorporates mechanistic biomarker studies in high-quality clinical trials and validates findings with human-derived models; 4) developing precision application strategies by identifying responder subgroups via biomarkers or TCM syndrome differentiation.
The findings of this study have direct implications for practice and research. Clinically, BHDH could be considered an adjunctive option for patients with inadequate response or intolerance to first-line therapies, particularly those with symptoms like anxiety or insomnia, or with patterns of yin deficiency with internal heat. At the policy level, funding should prioritize translational studies that integrate multi-omics technologies and bridge basic and clinical research, while also promoting the development of TCM-specific evaluation methodologies.
In conclusion, while BHDH holds notable potential for MDD treatment, its transformation into an evidence-based therapy depends on systematically overcoming the outlined limitations. Future work must achieve deeper mechanistic understanding, a complete scientific elucidation of the formula’s synergy, and the construction of robust translational bridges. This process is crucial not only for BHDH but may also provide a generalizable methodological framework for modernizing TCM in the treatment of complex diseases, ultimately benefiting patients with MDD.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study completed with the support of the China Postdoctoral Science Foundation (Grant No. 2022TQ0098 and 2024M760844). Natural Science Foundation of Henan Province (242300421296), Science and technology in Henan Province (242102310082, and 252102231013).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Qi W, Xiaobai L. The effect of acute stress on patients with mental disease. Chin J Psych. 2020;53(03):204–18.
2. Charlson F, Ommeren MV, Flaxman A, Cornett J, Saxena S. New WHO prevalence estimates of mental disorders in conflict settings: a systematic review and meta-analysis. Lancet. 2019;394(10194):240–248. doi:10.1016/S0140-6736(19)30934-1
3. Malhi GS, Mann JJ. Depression. Lancet. 2018;392(10161):2299–2312. doi:10.1016/s0140-6736(18)31948-2
4. Liu L, Wang H, Chen X, Zhang Y, Zhang H, Xie P. Gut microbiota and its metabolites in depression: from pathogenesis to treatment. EBio Med. 2023;90:104527. doi:10.1016/j.ebiom.2023.104527
5. Yao J, Yang YT, Al QD, et al. Review of research progress on neurotransmitter function and depression. Chin Pharmacolog Bull. 2023;39(07):1217–1221.
6. Li Y. Research on the understanding and treatment mechanism of depression in traditional Chinese medicine. Popular Sci Technol. 2020;22(07):87–89+95.
7. Dang C, Wang Q, Li Q, Xiong Y, Lu Y. Chinese herbal medicines for the treatment of depression: a systematic review and network meta-analysis. Front Pharmacol. 2024;15:1295564. doi:10.3389/fphar.2024.129556
8. Li C, Huang J, Cheng YC, Zhang YW. Traditional Chinese medicine in depression treatment: from molecules to systems. Front Pharmacol. 2020;11:586. doi:10.3389/fphar.2020.00586
9. Xu JJ, Liu J, Xu JY, Zheng XC. Historical evolution and research progress of the classical prescription of Baihe Dihuang decoction. Jilin J Trad Chin Med. 2024;44(04):475–480. doi:10.13463/j.cnki.jlzyy.2024.04.024
10. Di ZB, Liu Y, Liu F, et al. Quality evaluation of the classic famous prescriptions Baihe Dihuang decoction based on dual wavelength fingerprint spectrum and content determination. Central South Pharm. 2022;20(09):2094–2099.
11. Liu JW, Ren JJ, Lan JQ, Gong YQ, Liu JF. Research progress on the pharmacological effects of colchicine. Asia-Pacific Trad Med. 2024;20(11):225–231.
12. Lang XN, Feng X, Li L, Fu XY. Research progress on the antioxidant mechanism of catalpol. Tianjin Pharm. 2024;36(02):69–75.
13. Ji G, Ou HJ, Zhou LL, Chen ZH. Research progress on chemical composition and pharmacological effects of Lily Dihuang decoction and prediction and analysis of quality markers. Clin Ration Drug Use. 2024;17(20):173–176. doi:10.15887/j.cnki.13-1389/r.2024.20.051
14. Hu YJ, Zhao XJ, Chen C, Song YM, Fu XJ. Bibliometrics analysis of Baihe Dihuang decoction based on CNKI database. J Shandong Univ Trad Chin Med. 2019;43(03):217–223. doi:10.16294/j.cnki.1007-659x.2019.03.002
15. Hu ZD, Tian S, Miao YY, Miao MS. Chemical composition, pharmacological research, and clinical application of Baihe. Pharmacol Clini Chin Mater Med. 2022;38(04):241–246. doi:10.13412/j.cnki.zyyl.20211015.001
16. Bai GJ, Chen SD, Zhang PZ, Xiong SH, Wu ZF, Wang YQ. Research progress on chemical structural characterization and biological activities of lily polysaccharides. Chin Trad Herbal Drugs. 2022;53(20):6583–6592.
17. Mimaki Y, Sashida Y. Steroidal saponins from the bulbs of Lilium brownii. Phytochemistry. 1990;29(7):2267–2271. doi:10.1016/0031-9422(90)83050-B
18. Wu JH, Lin DX, Jun TG, Ji HW, Ding XL, Tao GJ. Screening of steroidal saponins from the bulbs of Lilium brownii var. colchesteri by combination of high performance liquid chromatography-electrospray ionization mass spectrometry and electron impact mass spectrometry. Se Pu. 2001;19(5):403–406.
19. Haladova M, Mucaji P, Budesinsky M, Vokac K, Cvacka J, Grancai D. Spirostanol saponins from the bulbs of Lilium candidum. Chem Nat Compd. 2011;46(6):1004–1005. doi:10.1007/s10600-011-9812-9
20. Mimaki Y, Sashida Y, Shimomura H. Lipid and steroidal constituents of Lilium auratum var. Platyphyllum AND L. tenuifolium. Phytochemistry. 1989;28(12):3453–3458. doi:10.1016/0031-9422(89)80363-2
21. Mimaki Y, Nakamura O, Sashida Y, Satomi Y, Nishino A, Nishino H. Steroidal saponins from the bulbs of Lilium longiflorum and their antitumour-promoter activity. Phytochemistry. 1994;31(1):221–232.
22. Mimaki Y, Satou T, Kuroda M, Sashida Y, Hayakeyama Y. New steroidal constituents from the bulbs of Lilium candidum. Chem Pharm Bull. 1998;46(11):1829. doi:10.1016/0031-9422(94)85030-5
23. Zhou ZL, Shi RB, Liu B, Zhou JM, Yi WQ, Xia JM. Steroidal saponins and phenylic constituents from Lilium lancifolium and their anti-oxidant activities. Chin Traditional Herbal Drugs. 2011;42(01):21–24.
24. Zhou ZL, Feng ZC, Fu CY, Zhang HL, Xia JM. Steroidal and phenolic glycosides from the bulbs of lilium pumilum DC and their potential Na+/K+ ATPase inhibitory activity. Molecules. 2012;17(9):10494–10502. doi:10.3390/molecules170910494
25. Munafo JP, Gianfagna TJ. Quantitative analysis of steroidal glycosides in different organs of Easter lily (Lilium longiflorum Thunb.) by LC-MS/MS. J Agri Food Chem. 2011;59(3):995–1004. doi:10.1021/jf1036454
26. Zhu M, Luo J, Lv H, Kong L. Determination of anti-hyperglycaemic activity in steroidal glycoside rich fraction of lily bulbs and characterization of the chemical profiles by LC-Q-TOF-MS/MS. J Funct Foods. 2014;6:585–597. doi:10.1016/j.jff.2013.12.002
27. Nan ZD, Zhu YD, Deng CF, et al. Nitrogenous chemical constituents and their antitumor activities evaluation in vitro from the aerial parts of Corydalis impatiens (pall.) Fisch. Nat Product Res. 2025;39(5):1027–1038. doi:10.1080/14786419.2023.2291704
28. Huang JJ, Gao Y, Li WM, Ye XL. Quantitative determination of dioscin in bulbus lilii by HPLC-ELSD. Chin J Exp Trad Med Formulae. 2011;17(05):110–112.
29. Zhou J, Zhao XM, An RF, et al. Four new steroidal glycosides from Lilium lancifolium Thunb. and their antitumor activity. Fitoterapia. 2024;173:105808. doi:10.1016/j.fitote.2023.105808
30. Hu WY, Duan JA, Qian DW, Wang DW. Studies on chemical constituents in fresh fleshy scaleleaf of Lilium lancifolium. China J Chin Materia Medica. 2007;32(16):1656–1659.
31. Yukiko M, Reina T, Yoshihiro M. Novel steroidal glycosides from the Bulbs of Lilium pumilum. Molecules. 2015;20(9):16255–16265. doi:10.3390/molecules200916255
32. Mimaki Y, Satou T, Kuroda M, Sashida Y, Hatakeyama Y. Steroidal saponins from the bulbs of Lilium candidum. Phytochemistry. 1999;51(4):567–573. doi:10.1016/S0031-9422(99)00022-9
33. Hou X, Chen F. Studies on chemical constituents of Lilium brownii. Acta Pharma Sin. 1998;33(12):923–926.
34. Astrid O, Damba T. Extracts from the Mongolian traditional medicinal plants Dianthus versicolor Fisch. and Lilium pumilum Delile stimulate bile flow in an isolated perfused rat liver model. J Ethnopharmacol. 2010;131(3):555–561. doi:10.1016/j.jep.2010.07.029
35. Munafo JP Jr, Ramanathan A, Jimenez LS, Gianfagna TJ. Isolation and structural determination of steroidal glycosides from the Bulbs of Easter Lily (Lilium longiflorum Thunb.). J Agri Food Chem. 2010;58(15):8806–8813. doi:10.1021/jf101410d
36. Luo J, Li L, Kong L. Preparative separation of phenylpropenoid glycerides from the bulbs of Lilium lancifolium by high-speed counter-current chromatography and evaluation of their antioxidant activities. Food Chem. 2012;131(3):1056–1062. doi:10.1016/j.foodchem.2011.09.112
37. Wang T, Huang H, Zhang Y, et al. Role of effective composition on antioxidant, anti-inflammatory, sedative-hypnotic capacities of 6 common edible lilium varieties. J Food Sci. 2015;80(4–5–6):H857–H868. doi:10.1111/1750-3841.12787
38. Mimaki Y, Sashida Y. Steroidal and phenolic constituents of Lilium speciosum. Chem Pharm Bull. 1991;30(3):937–940.
39. Shimomura H, Sashida Y, Mimaki Y. New phenolic glycerol glucosides, regaloside, D, E, and F from the bulbs of Lilium species. J Pharmacog. 1989;43(1):64–70.
40. Shimomura H, Sashida Y, Mimaki Y. Bitter phenylpropanoid glycosides from Lilium speciosum var. rubrum. Phytochemistry. 1986;25(12):2897–2899. doi:10.1016/S0031-9422(00)83765-6
41. Guo HF, Zhang YL, Niu LX, Luo JR. Petal pigments of eight wild Lilium species native to China. J Northwest a F Univ. 2015;43:98–104.
42. Gao J, Zhang T, Jin ZY, et al. Structural characterisation, physicochemical properties and antioxidant activity of polysaccharide from Lilium lancifolium Thunb. Food Chem. 2015;169(15):430–438. doi:10.1016/j.foodchem.2014.08.016
43. Jin L, Zhang Y, Yan L, Guo Y. Phenolic compounds and antioxidant activity of bulb extracts of six Lilium Species Native to China. Molecules. 2012;17(8):9631–9678. doi:10.3390/molecules17089361
44. Satou T, Mimaki Y, Kuroda M, Sashida Y, Hatakeyama Y. A pyrroline glucoside ester and steroidal saponins from Lilium martagon. Phytochemistry. 1996;41(4):1225–1230. doi:10.1016/0031-9422(95)00723-7
45. Mašterová I, Uhrin D, Tomko J. Lilaline—a flavonoid alkaloid from Lilium candidum. Phytochemistry. 1987;26(6):1844–1845. doi:10.1016/S0031-9422(00)82304-3
46. Chun HE. Supercritical fluid extraction high performance liquid chromatography determination of colchicine in lily. Nat Prod Res Dev. 2003;15(1):5–8.
47. Hu M, Zhang S, Chen Y, Wang G. Chemical composition analysis of Lilium brownii var. viridulum baker and the effect of postharvest primary processing on its quality. Appl Sci. 2023;13(19):2076–3417. doi:10.3390/app131910795
48. Hong XX, Kong LY. Two new chlorophenyl glycosides from the bulbs of Lilium brownii var. viridulum. J Asian Nat Prod Res. 2012;14(8):769–775. doi:10.1080/10286020.2012.691096
49. Avula B, Wang YH, Ali Z, Smillie TJ, Khan IA. Chemical fingerprint analysis and quantitative determination of steroidal compounds from Dioscorea villosa, Dioscorea species and dietary supplements using UHPLC-ELSD. Biomed Chromatogr. 2014;28(2):281–294. doi:10.1002/bmc.3019
50. Nishimura H, Sasaki H, Morota T, Chin M, Mitsuhashi H. Six iridoid glycosides from Rehmannia glutinosa. Phytochemistry. 1990;28(10):2705–2709. doi:10.1016/S0031-9422(00)98072-5
51. Liu YF, Liang D, Luo H, Hao ZY, Yu DQ. Hepatoprotective iridoid glycosides from the roots of Rehmannia glutinosa. J Natural Prod. 2012;75(9):1625–1631. doi:10.1021/np300509z
52. Morota T, Sasaki H, Nishimura H, Sugama K, Chin M, Mitsuhashi H. Two iridoid glycosides from Rehmannia glutinosa. Phytochemistry. 1989;28(8):2149–2153. doi:10.1016/S0031-9422(00)97934-2
53. Kitagawa I, Fukuda Y, Taniyama T, et al. Absolute stereostructures of rehmaglutins a, b, and d: three new iridoids isolated from Chinese rehmanniae radix. Chem Pharm Bull. 1986;34(3):1399–1402.
54. Kim SS, Son YO, Chun JC, et al. Antioxidant property of an active component purified from the leaves of paraquat-tolerant Rehmannia glutinosa. Redox Rep. 2005;10(6):311–318. doi:10.1179/135100005X83734
55. Liu YF, Shi GR, Wang Z, et al. Bioactive iridoid glycosides from the whole plants of Rehmannia chingii. J Nat Prod. 2016;79(2):428–433. doi:10.1021/acs.jnatprod.5b01126
56. Wang T, Gui M, Liu H, et al. Secretion of catalpol from Rehmannia glutinosa roots to the rhizosphere. Acta Physiol Plant. 2010;32(1):141–144. doi:10.1007/s11738-009-0389-x
57. Li YS, Zi-Jun C, Zhu DY. A novel bis-furan derivative, two new natural furan derivatives from Rehmannia glutinosa and their bioactivity. Nat Product Res. 2005;19(2):165–170. doi:10.1080/14786410410001704787
58. Hong-Xia HU, Pei-Ming Y. Studies on chemical constituents of Picrorhiza scrophulariiflora pennell. Chin J Pharmaceut. 2005;36(06):336–339.
59. Yoshikawa M, Fukuda Y, Taniyama T, Kitagawa I. Absolute stereostructures of rehmaglutin C and glutinoside: a new iridoid lactone and a new chlorinated iridoid glucoside from Chinese Rehmanniae Radix. Chem Pharm Bull. 2008;34(3):1403–1406. doi:10.1248/cpb.34.1403
60. Yanjie W, Dengqun L, Minjian Q, Xian’en L. Simultaneous determination of catalpol, aucubin, and geniposidic acid in different developmental stages of rehmannia glutinosa leaves by high performance liquid chromatography. J Anal Meth Chem. 2016;2016:4956589. doi:10.1155/2016/4956589
61. Li X, Zhou M, Shen P, et al. Chemical constituents from Rehmannia glutinosa. China J Chin Materia Medica. 2011;36(22):3125.
62. Sasaki H, Nishimura H, Morota T, Katsuhara T, Chin M, Mitsuhashi H. Norcarotenoid glycosides of Rehmannia glutinosa var. Purpurea. 1991;30(5):1639–1644.
63. Lee SY, Kim JS, Choi RJ, Kim YS, Lee JH, Kang SS. A new polyoxygenated triterpene and two new aeginetic acid quinovosides from the roots of Rehmannia glutinosa. Chem Pharm Bull. 2011;59(6):742–746. doi:10.1248/cpb.59.742
64. Feng WS, Li M, Zheng XK, Song K, Zhang MH. Study on chemical constituents of immunosuppressive parts from the roots of Rehmannia glutinosa. Chin Pharm J. 2014;49(17):1496–1502.
65. Bianco A, Guiso M, Martino M, et al. Iridoids from endemic sardinian Linaria species. Phytochemistry. 1996;42(1):89–91. doi:10.1016/0031-9422(95)00892-6
66. Boros CA, Stermitz FR. Iridoids. An updated review. Part 1. J Natural Prod. 1990;53(5):1055–1147. doi:10.1021/np50071a001
67. Kitagawa I, Fukuda Y, Taniyama T, Yoshikawa M. Chemical studies on crude drug processing. VIII. On the constituents of Rehmanniae Radix. (2): absolute stereostructures of rehmaglutin c and glutinoside isolated from Chinese Rehmanniae Radix, the Dried Root of Rehmannia glutinosa Libosch. Chemin form. 1996;27(13):1096–1100.
68. Yoshikawa M, Fukuda Y, Taniyama T, Cha BC, Kitagawa I. Absolute configurations of rehmaionosides A, B, and C and rehmapicroside: three new ionone glucosides and a new monoterpene glucoside from Rehmanniae Radix. Chem Pharm Bull. 1986;34(5):2294–2297. doi:10.1248/cpb.34.2294
69. Kitagawa I, Hori K, Kawanishi T, Kobayashi M, Kawanishi F. [On the constituents of the root of fukuchiyama-jio, the hybrid of Rehmannia glutinosa var. purpurea and R. glutinosa forma hueichingensis. Yakugaku Zasshi. 1998;118(10):464. doi:10.1248/yakushi1947.118.10_464
70. Feng W, Lv Y, Zheng X, Zhang Y, Cao Y, Pei Y. A new megastigmane from fresh roots of Rehmannia glutinosa. Acta Pharmaceutica Sinica B. 2013;3(5):333–336. doi:10.1016/j.apsb.2013.07.001
71. Fu GM, Shi S. A new carotenoid glycoside from Rehmannia glutinosa. Nat Product Res. 2011;25(13):1213–1218. doi:10.1080/14786419.2010.514268
72. Champavier Y, Comte G, Vercauteren J, Allais DP, Chulia AJ. Norterpenoid and sesquiterpenoid glucosides from Juniperus phynicea and Galega officinalis. Phytochemistry. 1999;50(7):1219–1223. doi:10.1016/S0031-9422(98)00697-9
73. Sasaki H, Nishimura H, Chin M, Mitsuhashi H. Hydroxycinnamic acid esters of phenethylalcohol glycosides from Rehmannia glutinosa var. Purpurea. Phytochemistry. 1989;28(3):875–879. doi:10.1016/0031-9422(89)80134-7
74. Nishioka M, Matsumoto M, Nishioka I. Four caffeoyl glycosides from callus tissue of Rehmannia glutinosa. Phytochemistry. 1986;25(7):1633–1636. doi:10.1016/S0031-9422(00)81224-8
75. Mitsuhashi H, Sasaki H, Morota T, Chin (chen zhengxiong) M, Mitsuhashi H. Six glycosides from Rehmannia glutinosavar.Purpurea. Phytochemistry. 1990;29(10):3303–3306. doi:10.1016/0031-9422(90)80204-T
76. Zhang YL, Feng WS, Zheng XK, et al. Three new ursane-type triterpenes from the leaves of Rehmannia glutinosa. Fitoterapia -Milano. 2013;89:15–19. doi:10.1016/j.fitote.2013.05.013
77. Srivastava S, Huang SF, Jagtap MS. Assessment of the effect of Rehmannia glutinosa Leaf extract in maintaining skin health: a proof-of-concept, double-blind, randomized, placebo-controlled clinical trial. Clin Cosmet Invest Dermatol. 2024;17:863–875. doi:10.2147/CCID.S448928
78. Kitagawa I, Taniyama T, Shibuya H, Noda T, Yoshikawa M. Chemical studies on crude drug processing. V. On the constituents of ginseng radix rubra (2): comparison of the constituents of white ginseng and red ginseng prepared from the same Panax ginseng root. Yakugaku Zasshi. 1987;107(7):495–505. doi:10.1248/yakushi1947.107.7_495
79. Shu P, Cai S, Zhao X, et al. Chemical constituents from the Roots of Rehmannia glutinosa. Records Nat Prod. 2023;17(4):615–621. doi:10.25135/rnp.380.2211.2625
80. Hu XY, Dou DQ, Pei YP, Fu WW. Chemical constituents of roots of Ranunculus ternatus thunb. J Chin Pharmaceut Sci. 2006;15:127–129.
81. Myintyre DD, Vogel HJ. Complete assignment of the 1 H-NMR spectrum of stachyose by two-dimensional NMR spectroscopy. J Nat Prod. 1989;52(5):1008–1014. doi:10.1021/np50065a015
82. Han Y, Jung HW, Lee JY, et al. 2,5-dihydroxyacetophenone isolated from Rehmanniae Radix Preparata inhibits inflammatory responses in lipopolysaccharide-stimulated RAW264.7 macrophages. J Med Food. 2012;15(6):505–510. doi:10.1089/jmf.2011.1940
83. Fan XL, Liu YL, Cao YG, et al. Study on the chemical constituents of fresh rehmannia glutinosa ‘Huai Zhong No. 1’. Acta Pharma Sin. 2021;56(11):3097–3103. doi:10.16438/j.0513-4870.2021-0777
84. Zhang RX, Li MX, Jia ZP. Rehmannia glutinosa: review of botany, chemistry and pharmacology. J Ethnopharmacol. 2008;117(2):199–214. doi:10.1016/j.jep.2008.02.018
85. Li M, Ren Y, Lin Z, et al. Structural identification and anti-stomatitis activity of one arabinose-rich polysaccharide from Rehmannia glutinosa. Int J Biol Macromol. 2025;284(1):138006. doi:10.1016/j.ijbiomac.2024.138006
86. Hu C, Zhao HQ, Liu J, et al. Spectrum-effect relationship combined with bioactivity evaluation to discover the main antidepressant active components of Baihe Dihuang decoction. Acta Pharma Sin. 2024;59(05):1364–1373.
87. Peng XJ, Yang XJ, Chen YB, et al. Action mechanism of Baihe Dihuang decoction on depression based on integrative pharmacology of traditional Chinese medicine. China J Chin Materia Medica. 2018;43(07):1338–1344. doi:10.19540/j.cnki.cjcmm.20180115.021
88. Mao QC, Ma K, Y WJ, et al. Study of the changes of chemical composition in single frying and co-decoction of Baihe Dihuang decoction based on LC-MS method. J Liaoning Univ Trad Chin Med. 2024;26(02):77–82. doi:10.13194/j.issn.1673-842x.2024.02.013
89. He ZN, Zhang PT. Discussion on treating cancer related depression from five internal organs. J Trad Chin Med. 2020;61(20):1790–1793. doi:10.13288/j.11-2166/r.2020.20.009
90. Hu C, Yang H, Zhao HQ, et al. Antidepressant mechanism of Baihe Dihuang Decoction based on metabolomics and network pharmacology. China J Chin Materia Medica. 2025;50(01):10–20. doi:10.19540/j.cnki.cjcmm.20240712.710
91. Zhao YQ, Zhang HW, Zhang ZL, Li YJ, Wang YM. Fingerprinting and network Pharmacology based quality markers of Lilii Bulbus. Chin J Pharmaceut Anal. 2024;44(05):893–902. doi:10.16155/j.0254-1793.2024.05.18
92. Feng X, Liu YQ, Liu B, et al. Metabonomics study on the intervention of baihe dihuang decoction in depressed rats. Acta Chin Med Pharmacol. 2023;51(09):36–45. doi:10.19664/j.cnki.1002-2392.230190
93. Feng X, Liu B, Liu YQ, et al. Effects of Baihe Dihuang decoction on intestinal flora of depressed rats. World Chin Med. 2024;19(06):780–787.
94. Si-Qun G, Kui-Yuan Z, Ning X, Yuan-Yuan J, Ning Z. Serum pharmacochemistry study of Dihuang Yinzi. Chin J Exp Trad Med Formulae. 2011;17(08):74–78.
95. Xue X, Pan J, Zhang H, Lu Y, Mao Q, Ma K. Baihe Dihuang (Lilium Henryi Baker and Rehmannia Glutinosa) decoction attenuates somatostatin interneurons deficits in prefrontal cortex of depression via miRNA-144-3p mediated GABA synthesis and release. J Ethnopharmacol. 2022;292:115218. doi:10.1016/j.jep.2022.115218
96. Zhao HQ, Tang L, Liu Y, et al. Mechanism of Baihe Dihuang decoction activating AMPA receptor to improve anxiety and depression-like behavior in chronic unpredictability stress mice. China J Trad Chin Med Pharm. 2023;38(05):1955–1960.
97. Pan WC, Chi XS, Wang Y, et al. Improvement effects of Baihe Dihuang decoction on emotional symptoms in depression rats with Yin deficiency and internal heat syndrome. Chin Trad Patent Med. 2023;45(05):1652–1657.
98. Pan J, Pan WC, Chi XS, et al. Mechanism of Baihe Dihuang Decoction in the treatment of depression with Yin deficiency and internal heat. Chin J Exp Trad Med Formulae. 2022;28(12):31–38. doi:10.13422/j.cnki.syfjx.20220117
99. Zhao HQ, Liu J, Meng P, et al. Effect of Baihe Dihuang decoction on synaptic plasticity of hippocampus in rats with anxious depression. China J Chin Materia Medica. 2021;46(05):1205–1210. doi:10.19540/j.cnki.cjcmm.20201221.401
100. Peng L, Zhang XF, Guo DY, et al. Evaluation of the clinical efficacy of the classic prescription “baihe dihuang decoction” based on meta-analysis. Evid Based Complement Alternat Med. 2022;2022:8559176. doi:10.1155/2022/8559176
101. Zhang H, Xue X, Pan J, et al. Integrated analysis of the chemical-material basis and molecular mechanisms for the classic herbal formula of Lily Bulb and Rehmannia Decoction in alleviating depression. China Med. 2021;16(1):107. doi:10.1186/s13020-021-00519-x
102. Yang JH, Zhang DS, Jing YS. The effects of amino acid-based neurotransmitters on neurological diseases and their underlying mechanisms. Chin J Pharmacol Toxicol. 2021;35(09):642.
103. Xu QK, Hao GS. Research progress on the relationship between depressive disorder and kynurenine pathway and its metabolites. J Neurosci Mental Health. 2022;22(02):139–143.
104. Rani S, Yadav S, Ghorai SM. Cross-talk between peptide neurotransmitters and their role in homeostasis of brain, behavior, and immunity. Current Psych Res Rev. 2025;21(2):22. doi:10.2174/0126660822262191231024081805
105. Xue J, Li J. Effects of Baihe Dihuang decoction on the behavior and monoamine neurotransmitter and monoamine oxidase of hippocampus in CUMS rats. Acta Chin Med Pharmacol. 2018;46(01):109–111. doi:10.19664/j.cnki.1002-2392.180027
106. Mikulska J, Juszczyk G, Gawrońska-Grzywacz M, Herbet M. HPA axis in the patho mechanism of depression and schizophrenia: new therapeutic strategies based on its participation. Brain Sci. 2021;11(10):1298. doi:10.3390/brainsci11101298
107. Baj J, Forma A, Kowalska B, et al. Multi-elemental analysis of human optic chiasm—A new perspective to reveal the pathomechanism of nerve fibers’ degeneration. Int J Environ Res Public Health. 2022;19(7):4420. doi:10.3390/ijerph19074420
108. Jia-Qi G, Yan S, Hai-Wei C. Anti-depressive effect of Baihe Dihuang decoction in mice model. China J Trad Chin Med Pharm. 2013;28(06):1875–1877.
109. Beurel E, Toups M, Nemeroff CB. The bidirectional relationship of depression and inflammation: double trouble. Neuron. 2020;107(2):234–256. doi:10.1016/j.neuron.2020.06.002
110. Bouas AP, Rheinheimer J, Lagopoulos J. Why Severe COVID-19 Patients Are at Greater Risk of Developing Depression: a Molecular Perspective. Neuroscientist. 2020;28(1):11–19. doi:10.1177/1073858420967892
111. Jia S, Jia J, Jia M. Changes and clinical significance of serum brain-derived neurotrophic factor, substance P and interleukin-2 levels in patients with depression of different disease severity. Henan Med Res. 2022;31(11):2026–2029.
112. Zhao X, Cao F, Liu Q, et al. Behavioral, inflammatory and neurochemical disturbances in LPS and UCMS-induced mouse models of depression. Behav Brain Res. 2017;364:494–502. doi:10.1016/j.bbr.2017.05.064
113. Peng XJ, Yang XJ, Chen YB, Lu L, Liu F. Action mechanism of Baihe Dihuang decoction on depression based on integrative pharmacology of traditional Chinese medicine. China J Chin Materia Medica. 2018;43(07):1338–1344.
114. Zhang J, He J, Hu J, Ji Y, Lou Z. Exploring the role of gut microbiota in depression: pathogenesis and therapeutic insights. Asian J Psychiatry. 2025;105:104411. doi:10.1016/j.ajp.2025.104411
115. Mehta I, Juneja K, Nimmakayala T, et al. Gut microbiota and mental health: a comprehensive review of gut-brain interactions in mood disorders. Cureus. 2025;17(3):81447. doi:10.7759/cureus.81447
116. Tan Y, Xu M, Lin D. Review of research progress on intestinal microbiota based on metabolism and inflammation for depression. Arch Microbiol. 2024;206(4):146. doi:10.1007/s00203-024-03866-z
117. Wei T. In Vitro Antidepressant Effects of Baihe Dihuang Decoction Based on Gut Microbiota and PC12 Cells. [Master] 2022.
118. Mao Q, Zhang H, Zhang Z, et al. Co-decoction of Lilii bulbus and Radix Rehmannia Recens and its key bioactive ingredient verbascoside inhibit neuroinflammation and intestinal permeability associated with chronic stress-induced depression via the gut microbiota-brain axis. Phytomedicine. 2024;129:155510. doi:10.1016/j.phymed.2024.155510
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.