Back to Journals » Clinical Ophthalmology » Volume 15
Reported Patient Satisfaction and Spectacle Independence Following Bilateral Implantation of the PanOptix® Trifocal Intraocular Lens
Received 4 June 2021
Accepted for publication 28 June 2021
Published 6 July 2021 Volume 2021:15 Pages 2907—2912
DOI https://doi.org/10.2147/OPTH.S323337
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Clayton Blehm,1 Richard Potvin2
1Gainesville Eye Associates, Gainesville, GA, USA; 2Science in Vision, Bend, OR, USA
Correspondence: Richard Potvin
Science in Vision, 127 NW Revere Ave, Bend, OR, 97703, USA
Tel +1 407-697-6008
Email [email protected]
Purpose: To assess the spectacle independence and satisfaction of subjects after bilateral implantation of the PanOptix® trifocal intraocular lens (IOL) at the time of cataract surgery.
Design: Single site, prospective, single-arm study.
Methods: Eligible subjects interested in a trifocal IOL to potentially reduce dependence on spectacles for near, intermediate and distance vision were enrolled and followed for 3 months after the second eye surgery. Visual acuity and refractive data were collected 1 month and 3 months postoperative, including the uncorrected and best distance-corrected binocular visual acuities at distance (4m), intermediate (60 cm) and near (40cm). A patient satisfaction and spectacle independence questionnaire were administered at the 3-month visit.
Results: A total of 30 subjects successfully completed the study. Eighty-five percent of eyes (51/60) had a refraction within 0.50 D of plano with ≤ 0.50 D of refractive cylinder. One subject (3%) reported needing glasses for distance work, 3 (10%) for intermediate work and 4 (13%) for near work. Ninety percent or more of all subjects reported never wearing glasses or wearing them only a little at all working distances. Ninety percent or more were able to function without glasses at all 3 working distances all or most of the time. More than ninety percent of subjects reported being “com.pletely” or “mostly” satisfied with their vision without glasses or contact lenses at all three distances and overall.
Conclusion: A high percentage of patients are likely to achieve spectacle independence for distance, intermediate and near vision with this trifocal IOL.
Keywords: cataract surgery, spectacle independence, presbyopia correction, trifocal IOL, toric trifocal IOL
Plain Language Summary
Patients who are having cataract surgery may be interested in reducing their need for glasses at one or more working distances. The best alternative to provide good vision at distance, intermediate (eg, computer) and near (reading) may be a trifocal intraocular lens (IOL). This is because such an IOL can create a focal point at all three of the distances above.
The primary interest in our study was whether subjects implanted with a specific trifocal felt they had achieved the goal of being less dependent on spectacles. We were also interested in their reported satisfaction with their vision at various distances.
Ninety percent or more of subjects reported being able to function without glasses or contact lenses most or all of the time at all working distances. This trifocal IOL appears to be a good vision correction option for patients interested in reducing their need for glasses after cataract surgery.
Introduction
Many patients presenting for cataract surgery are interested in reducing their dependence on spectacles. If their desire is to be less spectacle-dependent for distance, intermediate (eg, computer use) and near (eg, reading) then the preferred option is likely to be a trifocal IOL. That is because these lenses provide 3 distinct foci. This is in contrast to extended depth of focus (EDOF) IOLs, which extend distance vision into the intermediate range but generally do not provide as good near vision.1,2 Bifocal IOLs are another option, but they only provide two distinct foci and can be problematic for intermediate vision.3,4 The extra focal point provided by a trifocal IOL does not appear to have a material effect on visual quality relative to a bifocal IOL.4
There are a several trifocal IOL designs available worldwide. All but one are limited to providing an intermediate focus that is half the dioptric distance of the near focus, which results in an intermediate distance that can be quite long for computer or cell phone use.5 The FineVision trifocal (PhysIOL, Liège, Belgium) is based on a 1.75 D intermediate focus and a 3.50 D near focus at the IOL plane, which provides intermediate vision around 80cm and near vision around 40cm.6 Similarly, the AT Lisa tri IOL (Carl Zeiss Meditec, Jena, Germany) has an intermediate focus of 1.66 D and a near focus of 3.33 D.7 The range of best intermediate vision with these lenses is well beyond where most patients would hold a cell phone or tablet.8
The PanOptix® IOL (Alcon, Fort Worth, USA) employs a unique optical design to avoid this limitation with the intermediate focus. It was designed as an aspheric diffractive quadrifocal IOL. However, the light energy from the first diffractive focus (around 120 cm) is redistributed to distance. The second and third diffractive foci provide vision at intermediate (~60 cm) and near (~40 cm).9 The result of this design is that the PanOptix trifocal shows better intermediate vision at 60 cm than the FineVision or AT Lisa trifocals.10–12 Clinical results reported previously also show that patients have a good range of vision with contrast sensitivity values in a normal range.13–15 This lens design has also been reported to produce a better overall defocus curve than the previous trifocals mentioned, tested with both high and low contrast acuity charts.3 At present, the PanOptix IOL is the only trifocal IOL approved for use in the USA.
In evaluating the success of any multifocal IOL there are two important subjective measures of success. One is the level of spectacle independence that patients report after implantation and the other is their satisfaction with their postoperative vision. The Patient Reported Spectacle Independence Questionnaire (PRSIQ) was specifically designed to collect spectacle independence data based on patient reporting of spectacle use in terms of “need, wear and function”.16
The purpose of the current study was to evaluate the level of reported spectacle independence and satisfaction of subjects bilaterally implanted with the PanOptix trifocal IOL, with associated refractive and visual acuity data.
Methods
This study was a prospective, single-arm study of outcomes after bilateral implantation of the PanOptix trifocal IOL at a single clinical site, evaluating subjective satisfaction, visual function, and refractive data. An institutional review board (Salus IRB, Austin, TX, USA) approved the study. All enrolled subjects signed an IRB-approved informed consent document. The study was conducted in compliance with the tenets of the Declaration of Helsinki, Good Clinical Practice (GCP), and International Harmonization (ICH) guidelines. The study was also registered with clinicaltrials.gov (NCT04126187). Collected data are not available for sharing.
Subjects over 40 years old who were eligible for cataract surgery and interested in a trifocal IOL to potentially reduce dependence on spectacles for near, intermediate and distance vision were invited to participate. A screening evaluation was used to establish that they were appropriate candidates for trifocal IOL implantation (toric or non-toric), with no preoperative ocular pathology (eg, diabetic retinopathy, corneal dystrophy), no prior corneal or intraocular surgery, or any other pre-existing condition which might confound the results of the study. Subjects had to have regular corneal astigmatism with a magnitude that could be treated with a non-toric IOL or a toric IOL in the approved ranges for the PanOptix lens.
All subjects had cataract surgery with implantation of the trifocal IOL and were followed for 3 months after the second eye surgery. The surgeon’s standard procedure for cases that did not include use of a femtosecond laser system was followed. Toric IOL planning included using a calculator that considered posterior corneal astigmatism. Suggested IOL sphere power, cylinder power and orientation were confirmed using intraoperative aberrometry (the ORA System® with Verifeye+ Technology™, Alcon Laboratories, Inc., Fort Worth, TX, USA). Visual acuity and refractive data were collected 1 month and 3 months postoperative. The PRSIQ was used to evaluate patient satisfaction and spectacle independence 3 months after surgery. Monitoring for adverse events was conducted at all study visits. The primary measure of interest was the subject-reported spectacle independence at the 3-month visit for distance vision, intermediate vision, near vision and overall. Secondary measures of interest were the uncorrected and best distance-corrected binocular visual acuities at distance (4m), intermediate (60 cm) and near (40cm).
All clinical data and questionnaire responses were collected on appropriate case report forms and tabulated in Microsoft Access (Microsoft, Redmond, WA, USA). Statistical analyses were performed using Statistica 12 (TIBCO Software Inc., Palo Alto, CA, USA). There was no control group, so descriptive statistics were primarily reported. Where appropriate, statistical testing of parametric variables was based on an analysis of variance (ANOVA), with a statistical significance of p ≤ 0.05 selected. To compare data over time a repeated-measures ANOVA was used, matching subject data at both time points. Finally, a specific sample size cannot be determined for a single-arm study such as this, but a sample of 30 subjects (60 eyes) was considered sufficient.
Results
A total of 30 subjects were bilaterally implanted with the toric or non-toric version of the PanOptix IOL between May of 2020 and February of 2021. Table 1 contains a summary of the subject demographics, and the preoperative and operative characteristics of the group. IOL sphere power (p = 0.16) and average keratometry (p = 0.20) were not statistically significantly different between the toric and non-toric IOLs, but preoperative corneal cylinder was significantly higher in the toric group (p < 0.01), as expected. All subjects completed their 3-month visit, though two subjects missed their 1-month visit.
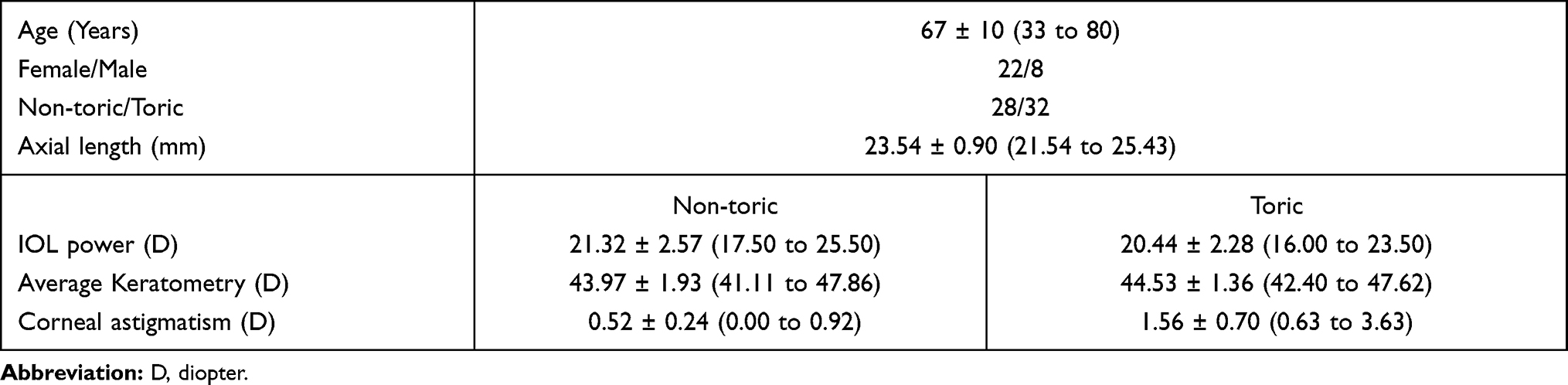 |
Table 1 Demographic, Preoperative and Operative Summary (30 Subjects, 60 Eyes) |
Table 2 contains a summary of the PRSIQ results. Only one subject reported needing glasses for distance work, and 87% (26/30) reported no need for glasses for near work. Ninety percent or more of all subjects reported never wearing glasses or wearing them only a little at the various test distances. Similarly, 90% or more of subjects reported being able to function without glasses at any distance all or most of the time. More than ninety percent of subjects reported being “completely” or “mostly” satisfied with their vision without glasses or contact lenses at all three distances, and overall.
 |
Table 2 PRSIQ Summary Data (n = 30) |
Table 3 contains the refractive data by eye and the associated monocular uncorrected and best corrected distance visual acuity. There were no statistically significant differences in any of the variables between the toric and non-toric lenses (p > 0.19 in all cases). Eighty-five percent of eyes (51/60) had a refraction within 0.50 D of plano with ≤ 0.50 D of refractive cylinder. Of the subjects with both eyes in that range (n = 22), none wore glasses for distance and all but one (95%) reported no need for glasses at any distance. All but one also reported functioning without glasses all or most of the time at all distances and all were “completely” or “mostly” satisfied with their vision without glasses or contact lenses at all three distances, and overall.
 |
Table 3 Postoperative Refractive and VA Data by Eye at 3 Months |
Figure 1 shows the binocular uncorrected and best distance corrected VA by test distance for all subjects at 3 months postoperative. As can be seen, the mean logMAR acuity was best at intermediate (60 cm) in both states of correction but differed by less than half a line from the other test distances. Best distance corrected visual acuity was better than uncorrected acuity at all test distances, though again the mean differences at all distances were 2 letters or less.
 |
Figure 1 Binocular uncorrected and distance-corrected VA by test distance at 3 months. Abbreviation: logMAR, log of the minimum angle of resolution. |
Bilateral YAG capsulotomies were performed on two subjects at their 1-month visit. An additional 6 subjects were scheduled for capsulotomy at or after their 3-month visit, all based on reported visual quality. Three subjects were treated for dry eye over the course of the study. There were no surgical or postoperative adverse events in any eye.
Discussion
The current study was designed to determine the level of spectacle independence and satisfaction reported by subjects bilaterally implanted with the only trifocal IOL currently approved for use in the USA.
We found no apparent difference in refractive and visual acuity results between the toric and non-toric versions of this IOL. This is consistent with findings from prior studies.17,18 The monocular refractive results and the associated monocular visual acuities also appear consistent with data previously reported, as are the binocular visual acuities.7,9–12,17–19 Results compare favorably to the data in the US pivotal trial submitted to support FDA approval of this trifocal IOL.20
Unfortunately, there is little standardization in terms of determining spectacle independence. Results from different studies are often based on different questionnaires, so direct comparisons are generally limited. However, it does appear that the reported spectacle independence rates in the current study are consistent with those reported for the same lens in prior studies,2,19,21 and with the results reported in the pivotal US clinical trial submitted to the FDA to support approval of the lens.20 One previously published study did use the same PRSIQ questionnaire when evaluating the same trifocal IOL. Results here are directly comparable and show similar success.22 In most studies, as with the current one, the need for spectacles was reported most often for near vision, though the reported use of spectacles was low (< 20%). Results in the current study showed 90% of subjects wore glasses little or none of the time for near work, while the figure was 95% in those subjects with a correction within 0.50D of intended with ≤ 0.50 D of refractive cylinder.
A relatively high number of YAG capsulotomies were performed or scheduled in the early postoperative period in this study.23 This is related to a site policy regarding the desire to avoid any light scatter that might negatively affect patients’ subjective vision. It has been noted that laxity or folds of the capsular bag can cause a linear streak glare pattern which can be addressed with a capsulotomy. Patient-reported visual disturbances, rather than reduced VA, are more often the driver of YAG capsulotomy when a multifocal IOL has been implanted.24
The current study does have limitations, the most apparent being the relatively small sample size and the single site. Quality of vision data (eg, low contrast acuity, subjective questionnaire data related to visual disturbances) were not collected. As a single-arm study, comparisons are limited to results in the clinical literature.
Results in this study indicate that the PanOptix trifocal IOL is a good alternative for patients seeking to reduce their dependence on spectacles across a wide range of vision, with a high likelihood of overall spectacle independence.
Acknowledgments
Maryann Thomas, research coordinator at Gainesville Eye Associates, provided data collection and administration support for this study. This research was conducted with support from Alcon, in the form of an investigator-initiated study grant (IIT # 50130835).
Disclosure
Richard Potvin is a consultant to Alcon and Carl Zeiss Meditec. Clayton Blehm reports grants from Alcon, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Rementería-Capelo LA, García-Pérez JL, Gros-Otero J, Carrillo V, Pérez-Lanzac J, Contreras I. Real-world evaluation of visual results and patient satisfaction for extended range of focus intraocular lenses compared to trifocal lenses. Int Ophthalmol. 2021;41(1):163–172. PMID: 32844238. doi:10.1007/s10792-020-01563-6
2. Cochener B, Boutillier G, Lamard M, Auberger-Zagnoli C. A comparative evaluation of a new generation of diffractive trifocal and extended depth of focus intraocular lenses. J Refract Surg. 2018;34(8):507–514. PMID: 30089179. doi:10.3928/1081597X-20180530-02
3. Martínez de Carneros-llorente A, Martínez de Carneros A, Martínez de Carneros-llorente P, Jiménez-Alfaro I. Comparison of visual quality and subjective outcomes among 3 trifocal intraocular lenses and 1 bifocal intraocular lens. J Cataract Refract Surg. 2019;45(5):587–594. PMID: 30853317. doi:10.1016/j.jcrs.2018.12.005
4. Yoon CH, Shin IS, Kim MK. Trifocal versus bifocal diffractive intraocular lens implantation after cataract surgery or refractive lens exchange: a Meta-analysis. J Korean Med Sci. 2018;33(44):e275. PMID: 30369857; PMCID: PMC6200906. doi:10.3346/jkms.2018.33.e275
5. Charness N, Dijkstra K, Jastrzembski T, Weaver S, Champion M Monitor viewing distance for younger and older workers.
6. Sheppard AL, Shah S, Bhatt U, Bhogal G, Wolffsohn JS. Visual outcomes and subjective experience after bilateral implantation of a new diffractive trifocal intraocular lens. J Cataract Refract Surg. 2013;39(3):343–349. PMID: 23332118. doi:10.1016/j.jcrs.2012.09.017
7. Mendicute J, Kapp A, Lévy P, et al. Evaluation of visual outcomes and patient satisfaction after implantation of a diffractive trifocal intraocular lens. J Cataract Refract Surg. 2016;42(2):203–210. PMID: 27026443. doi:10.1016/j.jcrs.2015.11.037
8. Long J, Cheung R, Duong S, Paynter R, Asper L. Viewing distance and eyestrain symptoms with prolonged viewing of smartphones. Clin Exp Optom. 2017;100(2):133–137. PMID: 27716998. doi:10.1111/cxo.12453
9. Kohnen T. First implantation of a diffractive quadrafocal (trifocal) intraocular lens. J Cataract Refract Surg. 2015;41(10):2330–2332. PMID: 26703312. doi:10.1016/j.jcrs.2015.11.012
10. Sezgin Asena B. Visual and refractive outcomes, spectacle independence, and visual disturbances after cataract or refractive lens exchange surgery: comparison of 2 trifocal intraocular lenses. J Cataract Refract Surg. 2019;45(11):1539–1546. PMID: 31587938. doi:10.1016/j.jcrs.2019.06.005
11. Ribeiro FJ, Ferreira TB. Comparison of visual and refractive outcomes of 2 trifocal intraocular lenses. J Cataract Refract Surg. 2020;46(5):694–699. PMID: 32358262. doi:10.1097/j.jcrs.0000000000000118
12. Gundersen KG, Potvin R. Trifocal intraocular lenses: a comparison of the visual performance and quality of vision provided by two different lens designs. Clin Ophthalmol. 2017;11:1081–1087. PMID: 28652693; PMCID: PMC5472417. doi:10.2147/OPTH.S136164
13. Bissen-Miyajima H, Ota Y, Hayashi K, Igarashi C, Sasaki N. Results of a clinical evaluation of a trifocal intraocular lens in Japan. Jpn J Ophthalmol. 2020;64(2):140–149. PMID: 31900871. doi:10.1007/s10384-019-00712-4
14. Alió JL, Plaza-Puche AB, Alió Del Barrio JL, et al. Clinical outcomes with a diffractive trifocal intraocular lens. Eur J Ophthalmol. 2018;28(4):419–424. PMID: 29619883. doi:10.1177/1120672118762231
15. Alfonso JF, Fernández-Vega-Cueto L, Fernández-Vega L, Montés-Micó R. Visual function after implantation of a Presbyopia-correcting trifocal intraocular lens. Ophthalmic Res. 2020;63(2):152–164. PMID: 31390634. doi:10.1159/000500834
16. Morlock R, Wirth RJ, Tally SR, Garufis C, Heichel CWD. Patient-Reported Spectacle Independence Questionnaire (PRSIQ): development and validation. Am J Ophthalmol. 2017;178:101–114. PMID: 28341605. doi:10.1016/j.ajo.2017.03.018
17. Carreno E, Carreno EA, Carreno R, et al. Refractive and visual outcomes after bilateral implantation of a trifocal intraocular lens in a large population. Clin Ophthalmol. 2020;14:369–376. doi:10.2147/OPTH.S238841
18. Rementería-Capelo LA, Contreras I, García-Pérez JL, Blázquez V, Ruiz-Alcocer J. Visual quality and patient satisfaction with a trifocal intraocular lens and its new toric version. J Cataract Refract Surg. 2019;45(11):1584–1590. PMID: 31587937. doi:10.1016/j.jcrs.2019.06.014
19. Donmez O, Asena BS, Kaskaloglu M, Akova YA. Patients satisfaction and clinical outcomes of binocular implantation of a new trifocal intraocular lens. Int Ophthalmol. 2020;40:1069–1075. doi:10.1007/s10792-020-01390-9
20. Modi S, Lehmann R, Maxwell A, et al. Visual and patient-reported outcomes of a diffractive trifocal intraocular lens compared with those of a monofocal intraocular lens. Ophthalmology. 2021;128(2):197–207. PMID: 33004211. doi:10.1016/j.ophtha.2020.07.015
21. Hovanesian JA, Jones M, Allen Q. The PanOptix trifocal IOL vs the ReSTOR 2.5 active focus and ReSTOR 3.0-add multifocal lenses: a Study of Patient Satisfaction, Visual Disturbances, and Uncorrected Visual Performance. Clin Ophthalmol. 2021;15:983–990. doi:10.2147/OPTH.S285628
22. Tran DB, Owyang A, Hwang J, Potvin R. Visual acuity, quality of vision, and patient-reported outcomes after bilateral implantation with a trifocal or extended depth of focus intraocular lens. Clin Ophthalmol. 2021;15:403–412. doi:10.2147/OPTH.S295503
23. Biber JM, Sandoval HP, Trivedi RH, Fernández de Castro LE, French JW, Solomon KD. Comparison of the incidence and visual significance of posterior capsule opacification between multifocal spherical, monofocal spherical, and monofocal aspheric intraocular lenses. J Cataract Refract Surg. 2009;35(7):1234–1238. doi:10.1016/j.jcrs.2009.03.013
24. Shah VC, Russo C, Cannon R, Davidson R, Taravella MJ. Incidence of Nd: yAGcapsulotomy after implantation of AcrySof multifocal and monofocal intraocular lenses: a case controlled study. J Refract Surg. 2010;26(8):565–568. PMID: 20349858. doi:10.3928/1081597X-20100303-01
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.