Back to Journals » International Journal of Nephrology and Renovascular Disease » Volume 9
Renal cell carcinoma: links and risks
Authors Kabaria R, Klaassen Z, Terris M
Received 8 November 2015
Accepted for publication 21 January 2016
Published 7 March 2016 Volume 2016:9 Pages 45—52
DOI https://doi.org/10.2147/IJNRD.S75916
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Pravin Singhal
Reena Kabaria, Zachary Klaassen, Martha K Terris
Department of Surgery, Section of Urology, Augusta University, Augusta, GA, USA
Abstract: This review provides an overview of the incidence of renal cell carcinoma (RCC) and a summary of the most commonly associated risk factors. A literature review was performed with a focus on recent studies with a high level of evidence (large prospective cohort studies and meta-analyses). The incidence rate of RCC varies globally, with the rate rising rapidly in more developed regions, demonstrating the effects of increased use of diagnostic imaging and prevalence of modifiable risk factors. Based on the current evidence, cigarette smoking, obesity, and hypertension are the most well-established risk factors for sporadic RCC worldwide. Acquired cystic kidney disease is also a significant risk factor, specifically in dialysis patients. There is increasing evidence for an inverse association between RCC risk and moderate alcohol consumption. Certain analgesics and occupational exposure have been linked to an increased risk of RCC, although data are limited. Diets rich in fruits and vegetables may provide a protective effect.
Keywords: renal cell carcinoma, risk factors, incidence, smoking, obesity, hypertension
Introduction
Kidney and renal pelvis cancer is among the top ten most common cancers in the world.1,2 The most frequent type of renal neoplasm is renal cell carcinoma (RCC), which accounts for ~85% of all renal malignancies. Urothelial carcinoma of the renal pelvis accounts for the remaining 10%.3
RCC arises from the renal parenchyma, particularly from the cells of the nephron and can be further specified into histological subtypes. Clear cell RCC (70%), which arises from the proximal convoluted tubule, is the most common histological subtype, followed by papillary (10%–15%) and chromophobe RCC (5%).4
Epidemiology
Incidence and mortality
The incidence of RCC varies internationally. The incidence of renal cancer in more developed regions (eg, Europe and North America) is more than twice that of less developed regions (eg, Africa and South America). In Europe, an estimated 16/100,000 individuals were diagnosed with a renal malignancy, whereas in Africa, an estimated 1/100,000 individuals were diagnosed with a renal malignancy in 2012.1 The regional variation is likely due to a combination of a higher amount of incidental tumors discovered on diagnostic abdominal imaging (computerized tomography scan, ultrasound, and magnetic resonance imaging) and modifiable risk factors such as smoking, obesity, and hypertension.5
It is estimated that >320,000 new cases will be diagnosed in 2016 worldwide. The estimated number of deaths globally is 140,000 or 2.0/100,000 men and women. During the past 10 years, the incidence of RCC has increased worldwide, yet death rates have decreased or remained stable in most countries under study.1 This could be explained by the fact that the size of renal tumors at diagnosis is decreasing with time in developed countries, such as the USA, which is characterized by better survival outcome.6
Survival
Based on a large epidemiologic analysis from the US National Cancer Institute, the overall 5-year survival for kidney and renal pelvis cancer is 73%. The earlier the tumor is discovered, the greater the chance at survival. The 5-year relative survival rate is 92% for localized tumors (confined to the kidney), 65% for tumors spread to regional lymph nodes, and 12% for metastasized tumors.7
Sex and age
Worldwide, RCC is twice as common in males as females after adjusting for age. In addition, >50% of RCC is diagnosed among people aged 55–74 years.1
Race
Within the USA, renal malignancies are more common in African Americans, American Indians, and Alaska Native populations. The incidence of RCC is lower among Asians living in the USA and Asian countries. The highest incidence rates worldwide are observed in the Czech Republic (22/100,000 in men and 9.9/100,000 in women). The lowest rates are seen in most African and Asian populations, with the exception of Israel.8
Socioeconomic status
Population-based studies in the USA, Denmark, and the Netherlands show increased incidence of RCC with lower socioeconomic status.9–11
Genetic predisposition
Multiple studies indicate that a family history of RCC is associated with a twofold increased risk of RCC.9,12,13 Although the majority of RCC occurs sporadically, several familial syndromes involving mutations in tumor suppressor genes and oncogenes have been identified. Hereditary RCC accounts for 4% of all RCCs. Familial forms of RCC develop at an earlier age and are often multiple and bilateral.14 von Hippel–Lindau (VHL) disease, which is due to a tumor suppressor gene mutation of chromosome 3, is the most commonly inherited RCC. Other neoplasms associated with VHL include pheochromocytoma, retinal angiomas, and nervous system hemangioblastomas. There is a 69% chance of developing RCC before age 60 in VHL patients.15 Other genetic forms of RCC include tuberous sclerosis, hereditary papillary RCC, Birt–Hogg–Dube syndrome, and hereditary leiomyomatosis.
Established risk factors
Based on the current evidence presented later, cigarette smoking, obesity, and hypertension are the most well-established risk factors for sporadic RCC. Acquired cystic kidney disease (ACKD) is also a significant risk factor.
Cigarette smoking
Tobacco exposure is a major risk factor for RCC. According to the US Surgeon General and the International Agency for Research on Cancer, there is sufficient evidence from several cohort and case–control studies to support causality between tobacco smoking and development of RCC.16,17 The overall relative risk for ever-smokers compared to never smokers is ~1.38 for both sexes based on a comprehensive meta-analysis of 24 studies involving North America, Europe, and Australia.18 The relative risk is lower in former smokers as compared to current smokers. The risk is directly related to duration of smoking and increases with cumulative dose (number of cigarettes smoked per day) and decreases with long-term smoking cessation >10 years.18 In a large cohort study of ~250,000 US veterans >26 years, the relative risk for renal cancer increased significantly with the number of cigarettes smoked per day, from 1.31 for 1–9, 1.37 for 10–20, 1.6 for 21–39, and 2.06 for ≥40.19 There is evidence to support that never smokers exposed to environmental tobacco smoke at home or work are also at increased risk of RCC.20,21 With respect to histological RCC subtype, a prospective study comparing the relationship between smoking and RCC subtypes demonstrated that active smoking was significantly more common with clear cell (23%) and papillary RCC (26%) than benign histology (14%) and chromophobe RCC (6%).22
Individuals who are current smokers or have a history of tobacco exposure present with more aggressive forms of RCC and experience worst cancer-specific survival and overall survival. In the USA, tobacco exposure is associated with higher pathological tumor, lymph node, and metastasis classification.23 A North American study found a dose-dependent relationship between duration of smoking and survival in individuals with nonmetastatic clear cell RCC: each pack-year of smoking was associated with a 1% increase in mortality. This suggests that smoking may have an ongoing effect on the progression of RCC. Compared to nonsmokers, smokers have a higher incidence of impaired performance status and medical comorbidities, including chronic obstructive pulmonary disease and coronary artery disease, which may explain why overall survival is worst in smokers.24
There are multiple mechanisms that explain how tobacco exposure promotes the development of RCC. Cigarette smoke induces oxidative stress and injury in the kidney and causes renal impairment.25,26 The free radicals contained in cigarette smoke cause oxidative DNA damage, which may lead to the development of cancer.27 For example, 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanone is the most abundant N-nitrosamine present in cigarette smoke and a known carcinogen. It induces DNA damage and has been associated with increased risk of RCC.28 Chromosome 3p aberrations are the most frequently identified genetic alterations in RCC. Benzo[α]pyrene diol expoxide, a major constituent of cigarette smoke, induced chromosome 3p aberrations in cultured peripheral blood lymphocytic cells from individuals with RCC, suggesting that chromosome 3p may be a specific molecular target of cigarette carcinogens.29 Another major component of tobacco, nicotine, has been shown to stimulate pathological angiogenesis and accelerate tumor growth.30 Furthermore, a study examining the histopathological changes brought about by 6 weeks of cigarette smoke in rat kidneys showed lymphocytic infiltration of the interstitium and intraluminal hyaline deposition in specifically the proximal tubules, which is predominantly where RCC originates.31
Obesity
Obesity, which in adults is defined by the World Health Organization as a body mass index (BMI) ≥30 kg/m2, increases the risk of RCC among both men and women.32 The prevalence of overweight (BMI ≥25 to <30 kg/m2) individuals and obesity has been on the incline in the past 3 decades, particular in developed countries.33 In the USA, more than one-third of adults and almost 17% of children and adolescents are obese.34 The increasing prevalence of obesity is likely a contributor to the increasing incidence of RCC.
There are various methods to assess obesity. BMI and body weight are measures of total body fat, whereas waist and hip circumference are measures of central adiposity. A large prospective cohort study of >340,000 Europeans demonstrated that increased BMI, body weight, and hip and waist circumference were related to an increased risk of RCC in females. However, among males, a low rather than high hip circumference was related to an increased RCC risk after accounting for body weight. This suggests that body fat distribution may be more predictive in males, particularly hip circumference.35 Obesity follows a dose–response pattern between increasing obesity and increasing magnitude of risk. A quantitative summary analysis of 14 studies from Australia, the People’s Republic of China, Canada, the USA, Italy, and France revealed a relative risk of 1.07 per unit increase in BMI in both sexes.32 Bjørge et al demonstrated a similar relationship in a large cohort of Norwegian men and women. In their study, they calculated a relative risk of 1.05 per unit increase in BMI.36 Morbidly obese (BMI ≥35 kg/m2) individuals were shown to be at 71% increased risk compared to normal weight individuals in the USA.37 Obesity early in adulthood along with obesity near diagnosis of RCC are both associated with an increased risk of renal cancer.38,39
Obese patients are technically more challenging surgically as there are significant increases in blood loss and operative time with increasing BMI.40 Although obesity is an established risk factor in the development of RCC, the relationship between obesity and overall or cancer-specific survival of individuals with RCC is inconsistent. A large prospective cohort study consisting of >900,000 US adults demonstrated a dose-dependent relationship between increasing body weight and overall death rates in patients with RCC.41 Since tumor stage at the time of diagnosis predicts survival outcome,42 one may hypothesize that increased BMI may be associated with advanced tumor stage. However, data indicate that obese patients are not at a greater risk of advanced tumor stage at the time of diagnosis.39,43 Surprisingly, two American studies show improved disease-specific survival for obese patients.44,45 Furthermore, Korean and German studies suggest that being underweight at the time of surgery worsens cancer-specific survival by more than four times that of normal weight individuals.46,47 BMI is an imperfect measurement of body fat as it does not distinguish between fat and muscle and between visceral and subcutaneous fat. Based on the results of multiple Japanese studies, visceral obesity rather than BMI may be a more useful predictor of disease-recurrence survival rather than BMI since high visceral fat has been associated with longer cancer-specific survival and overall survival.48–50
Multiple mechanisms linking obesity to increased risk of RCC have been proposed. Adipose tissue secretes molecules known as adipokines into the blood stream, which play a role in energy balance, macromolecule metabolism, and signaling to the rest of the body. Adipokines such as leptin and interleukin-6 support tumor growth and circulate at higher levels in obese patients. In contrast, obese patients have lower levels of adiponectin, which has tumor suppressive effects.51 Aberrations in hypoxia-detecting pathways underlie most cases of sporadic RCC.52 Obesity induces renal damage and tissue hypoxia that may predispose to tumor formation.53 In vitro experiments show that RCC expresses elevated amounts of insulin and insulin-like growth factor-1 receptor protein, which have been shown to play a significant role in the development and progression of RCC.54 In addition, lipid peroxidation that has been shown to promote renal tumorigenesis in vitro is increased among the obese.55
Hypertension
Hypertension is a significant risk factor for RCC. Several studies conducted in the USA and in the People’s Republic of China show a dose-dependent increase in RCC with increasing blood pressure measurement taken at baseline clinic visit.37,56–58 An 18-year follow-up of a Norwegian cohort revealed that compared to the reference systolic pressure of <130 mmHg, the relative risk in women with systolic pressure 130–149 mmHg was 1.7, with levels 150–169 mmHg the risk was 2.0, and with levels ≥170 mmHg, the risk was 2.0.59 In a large prospective European cohort study, both elevated systolic and diastolic blood pressures were associated with a two- to threefold increased RCC risk that was independent of sex, BMI, smoking, and use of antihypertensives.60 Multiple studies consisting of patients from Europe and the USA report similar results.61–63 The risk decreases with reduction in blood pressure over time, which suggests that the risk of RCC can be modified with better blood pressure control.64,65 Antihypertensives, namely diuretics, have been implicated in earlier studies, but current evidence suggests that it is the underlying disorder of hypertension rather than the treatment that increases the risk of RCC.66–70 Perioperative blood pressure ≥150/100 mmHg negatively affects the overall survival in Korean patients with RCC.46 Yet, in a study of RCC cases in the USA, a self-reported history of hypertension was associated with a better overall survival.71 The biological mechanism underlying the relationship between elevated blood pressure and increased risk of RCC remains unknown. One theory suggests that the chronic renal hypoxia accompanying hypertension promotes tumor cell proliferation and angiogenesis by a transcription factor known as hypoxia inducible factor.72 Similar to individuals with elevated BMI, patients with essential hypertension also exhibit increased lipid peroxidation, which has been implicated in the pathogenesis of RCC.55
Acquired cystic kidney disease
ACKD occurs in patients with end-stage renal disease on dialysis. The frequency of ACKD increases with the duration of dialysis.73 Over 50% of patients on dialysis for >3 years will develop renal cystic changes.74 A comprehensive review of the literature shows that there is up to a 50-fold increased risk of RCC in patients with ACKD compared to the general population. ACKD-associated RCC tumors tend to be more common in males and often bilateral and multicentric.75,76 RCC can develop at any time in patients on dialysis with ACKD, even after renal transplantation, although RCC is more likely to involve the native kidney than the transplanted kidney.77,78 The prevalence of RCC in patients with ACKD is 19%, whereas the prevalence in native kidneys after renal transplantation is 5%. This suggests that renal transplantation may reduce risk of RCC in dialysis patients.79
Risk factors with conflicting or limited evidence
Alcohol
Multiple well-conducted systematic reviews examining several studies from Europe, North America, Australia, and Asia suggest that moderate alcohol consumption reduces the risk of RCC.80–83 Although the majority of the literature supports a link between alcohol consumption and risk of RCC, some American and Japanese studies suggest there is no association.37,56,84 A large prospective cohort study of >100,000 American participants showed an inverse relationship between alcohol consumption and RCC risk in both males and females with all types of alcoholic beverages, including wine, beer, and liquor.85 Two large international meta-analyses summarized a specific dose–response relationship and found that 5–12 g/d increment of alcohol intake corresponded to at least a 5% statistically significant decreased risk of RCC. When these associations were examined separately by sex, alcohol specifically from wine reduced the risk of RCC in females whereas alcohol from beer and liquor reduced the risk of RCC in males. This suggests sex-specific and alcoholic beverage-specific differences in the association between alcohol intake and RCC risk.86,87
Analgesics
There is mixed evidence supporting analgesics as a risk factor for RCC.88–91 A recent large meta-analysis of 20 studies from North America, Europe, and Australia including >8,000 cases of renal cancer showed that the use of acetaminophen and nonaspirin nonsteroidal anti-inflammatory drugs was associated with an increased risk of renal cancer. No overall increased risk was found for aspirin, but a significant risk was found when the analysis was restricted to non-US countries. Although the majority of studies specifically address RCC, some studies grouped RCC and urothelial carcinoma of the renal pelvis together.92
Diabetes mellitus
A history of diabetes mellitus is reported to be associated with increased risk of RCC in some North American, Asian, and European studies93–99 but not in other studies in the USA and Italy when correcting for confounding factors, such as BMI, smoking, and hypertension.37,62
Diet
Epidemiologic studies evaluating dietary habits and risk of RCC are inconsistent. The majority of studies performed in North America, Europe, and Australia suggest that high consumption of fruits and vegetables may be associated with reduced risk of RCC, but not all.37,100–105 A meta-analysis of seven North American and European studies indicates that the risk of RCC is inversely associated with dietary fiber intake in the form of vegetable and legume fiber but not with fruit and cereal fiber intake.106 Another meta-analysis of 12 studies performed in North America, Europe, Australia, and Russia specifically focusing on cruciferous vegetable intake found that increased intake may reduce the risk of RCC.107 Asian and North American studies indicate that excess risk may be associated with heavy meat consumption108–111 and high fat dairy products,112 although data are limited.
Occupation exposure
There are numerous studies examining the risk of RCC in relation to occupational exposures worldwide; however, the data remain limited and inconclusive. Table 1 lists the various occupational exposures that have been connected to an elevated risk of RCC.113–127
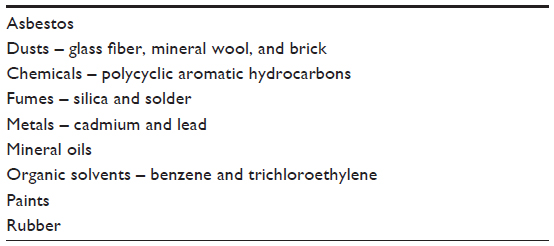 | Table 1 Occupational exposures associated with risk of RCC |
Summary
The overall incidence of RCC internationally continues to trend upward. The liberal use of diagnostic abdominal imaging detecting incidental renal tumors is likely a contributor along with established risk factors, such as smoking, obesity, and hypertension. Several studies support a dose-dependent increase in the risk of RCC for all three major risk factors and a decrease in risk with smoking cessation, weight loss, and blood pressure control. Thus, a focus on these modifiable risk factors may help prevent future cases of RCC. Moderate alcohol consumption may be associated with a decreased risk of RCC. Certain analgesics and occupational exposure have been linked to increased risk, although data are limited. Diets rich in fruits and vegetables may provide a protective effect. Additional studies are needed to explain all factors that may play a role in the development of RCC.
Disclosure
The authors report no conflicts of interest in this work.
References
Ferlay J, Soerjomataram I, Ervik M, et al. GLOBOCAN 2012: Estimated Cancer Incidence and Mortality Worldwide: IARC Cancer Base No. 11. Lyon: International Agency for Research on Cancer; 2014. | |
Ferlay J, Steliarova-Foucher E, Lortet-Tieulent J, et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries in 2012. Eur J Cancer. 2013;49:1374. | |
Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin. 2008;58:71–96. | |
Chow WH, Dong LM, Devesa SS. Epidemiology and risk factors for kidney cancer. Nat Rev Urol. 2010;7(5):245–257. | |
Mathew A, Devesa SS, Fraumeni JF Jr, Chow WH. Global increases in kidney cancer incidence, 1973–1992. Eur J Cancer Prev. 2002;11:171–178. | |
Cooperberg MR, Mallin K, Ritchey J, Villalta JD, Carroll PR, Kane CJ. Decreasing size at diagnosis of stage I renal cell carcinoma: analysis from the National Cancer Data Base, 1993 to 2004. J Urol. 2008;179:2131–2135. | |
Howlader N, Noone AM, Krapcho M, et al. SEER Cancer Statistics Review, 1975–2012. Bethesda, MD: National Cancer Institute; 2015. | |
Znaor A, Lortet-Tieulent J, Laversanne M, Jemal A, Bray F. International variations and trends in renal cell carcinoma incidence and mortality. Eur Urol. 2015;67:519. | |
Mellemgaard A, Engholm G, McLaughlin JK, Olsen JH. Risk factors for renal cell carcinoma in Denmark: I. Role of socioeconomic status, tobacco use, beverages, and family history. Cancer Causes Control. 1994;5:105–113. | |
Aarts MJ, van der Aa MA, Coebergh JW, Louwman WJ. Reduction of socioeconomic inequality in cancer incidence in the South of the Netherlands during 1996–2008. Eur J Cancer. 2010;46:2633–2646. | |
Jeffreys M, Sarfati D, Stevanovic V, et al. Socioeconomic inequalities in cancer survival in New Zealand: the role of extent of disease at diagnosis. Cancer Epidemiol Biomarkers Prev. 2009;18:915–921. | |
Clague J, Lin J, Cassidy A, et al. Family history and risk of renal cell carcinoma: results from a case-control study and systematic meta-analysis. Cancer Epidemiol Biomarkers Prev. 2009;18:801–807. | |
Gago-Dominguez M, Yuan JM, Castelao JE, Ross RK, Yu MC. Family history and risk of renal cell carcinoma. Cancer Epidemiol Biomarkers Prev. 2001;10:1001–1004. | |
Choyke PL, Glenn GM, Walther MM, Zbar B, Linehan WM. Hereditary renal cancers. Radiology. 2003;226(1):33–46. | |
Maher ER, Yates JRW, Harries R, et al. Clinical-features and natural-history of von Hippel-Lindau disease. Q J Med. 1990;77:1151–1163. | |
Office of the Surgeon General, Office on Smoking and Health. The Health Consequences of Smoking: 50 Years of Progress: A Report of the Surgeon General. Atlanta: Centers for Disease Control and Prevention; 2014. | |
International Agency for Research on Cancer. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans: Tobacco Smoke and Involuntary Smoking. Vol. 83. Lyon: IARC Press; 2004. | |
Hunt JD, van der Hel OL, McMillan GP, Boffetta P, Brennan P. Renal cell carcinoma in relation to cigarette smoking: meta-analysis of 24 studies. Int J Cancer. 2005;114:101. | |
McLaughlin JK, Hrubec Z, Heineman EF, Blot WJ, Fraumeni JF Jr. Renal cancer and cigarette smoking in a 26-year follow-up of U.S. veterans. Public Health Rep. 1990;105:535. | |
Theis RP, Dolwick Grieb SM, Burr D, Siddiqui T, Asal NR. Smoking, environmental tobacco smoke, and risk of renal cell cancer: a population-based case-control study. BMC Cancer. 2008;8:387. | |
Hu J, Ugnat AM, Canadian Cancer Registries Epidemiology Research Group. Active and passive smoking and risk of renal cell carcinoma in Canada. Eur J Cancer. 2005;41(5):770–778. | |
Patel NH, Attwood KM, Terrance MH, et al. Comparative analysis of smoking as a risk factor among renal cell carcinoma histological subtypes. J Urol. 2015;194(3):640–646. | |
Sweeney C, Farrow DC. Differential survival related to smoking among patients with renal cell carcinoma. Epidemiology. 2000;11:344–346. | |
Kroeger N, Klatte T, Birkhauser FD, et al. Smoking negatively impacts renal cell carcinoma overall and cancer-specific survival. Cancer. 2012;118:1795–1802. | |
Arany I, Grifoni S, Clark JS, Csongradi E, Maric C, Juncos LA. Chronic nicotine exposure exacerbates acute renal ischemic injury. Am J Physiol Renal Physiol. 2011;301(1):F125–F133. | |
Gambaro G, Verlato F, Budakovic A. Renal impairment in chronic cigarette smokers. J Am Soc Nephrol. 1998;9(4):562–567. | |
Zaremba T, Olinski R. Oxidative DNA damage – analysis and clinical significance. Postepy Biochem. 2010;56:124–138. | |
Clague J, Shao L, Lin J, et al. Sensitivity to NNKOAc is associated with renal cancer risk. Carcinogenesis. 2009;30:706. | |
Zhu Y, Horikawa Y, Yang H, Wood CG, Habuchi T, Wu X. BPDE induced lymphocytic chromosome 3p deletions may predict renal cell carcinoma risk. J Urol. 2008;179:2416–2421. | |
Heeschen C, Jang JJ, Weis M, et al. Nicotine stimulates angiogenesis and promotes tumor growth and atherosclerosis. Nat Med. 2001;7:833–839. | |
Cobanoglu B, Ozercan IH, Ozercan MR, Yalcin O. The effect of inhaling thinner and/or cigarette smoke on rat kidneys. Inhal Toxicol. 2007;19:303. | |
Bergstrom A, Hsieh CC, Lindblad P, Lu CM, Cook NR, Wolk A. Obesity and renal cell cancer – a quantitative review. Br J Cancer. 2001;85:984–990. | |
Ng M, Fleming T, Robinson M, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384:766–781. | |
Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of obesity among adults: United States, 2011-2012. NCHS Data Brief. 2013; 131(131):1–8. | |
Pischon T, Lahmann PH, Boeing H, et al. Body size and risk of renal cell carcinoma in the European Prospective Investigation into Cancer and Nutrition (EPIC). Int J Cancer. 2006;118:728. | |
Bjørge T, Tretli S, Engeland A. Relation of height and body mass index to renal cell carcinoma in two million Norwegian men and women. Am J Epidemiol. 2004;160:1168–1176. | |
Macleod LC, Hotaling JM, Wright JL, et al. Risk factors for renal cell carcinoma in the VITAL study. J Urol. 2013;190:1657. | |
Beebe-Dimmer JL, Colt JS, Ruterbusch JJ, et al. Body mass index and renal cell cancer: the influence of race and sex. Epidemiology. 2012;23(6):821–828. | |
Leiba A, Kark JD, Afek A, et al. Adolescent obesity and paternal country of origin predict renal cell carcinoma: a cohort study of 1.1 million 16 to 19-year-old males. J Urol. 2013;189:25–29. | |
Donat SM, Salzhauer EW, Mitra N, Yanke BV, Snyder ME, Russo P. Impact of body mass index on survival of patients with surgically treated renal cell carcinoma. J Urol. 2006;175:46–52. | |
Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med. 2003;348:1625–1638. | |
Shuch BM, Lam JS, Belldegrun AS, Figlin RA. Prognostic factors in renal cell carcinoma. Semin Oncol. 2006;33(5):563–575. | |
Schips L, Lipsky K, Zigeuner R, et al. Does overweight impact on the prognosis of patients with renal cell carcinoma? A single center experience of 683 patients. J Surg Oncol. 2004;88:57–61. | |
Kamat AM, Shock RP, Naya Y, Rosser CJ, Slaton JW, Pisters LL. Prognostic value of body mass index in patients undergoing nephrectomy for localized renal tumors. Urology. 2004;63:46–50. | |
Yu ML, Asal NR, Geyer JR. Later recurrence and longer survival among obese patients with renal cell carcinoma. Cancer. 1991;68:1648–1655. | |
Park B, Jeong BC, Seo SI, Jeon SS, Choi HY, Lee HM. Influence of body mass index, smoking, and blood pressure on survival of patients with surgically-treated, low stage renal cell carcinoma: a 14-year retrospective cohort study. J Korean Med Sci. 2013;28:227–236. | |
Haferkamp A, Pritsch M, Bedke J, et al. The influence of body mass index on the long-term survival of patients with renal cell carcinoma after tumour nephrectomy. BJU Int. 2008;101:1243–1246. | |
Kaneko G, Miyajima A, Yuge K, et al. Visceral obesity is associated with better recurrence-free survival after curative surgery for Japanese patients with localized clear cell renal cell carcinoma. Jpn J Clin Oncol. 2015;45(2):210–216. | |
Park YH, Lee JK, Kim KM, et al. Visceral obesity in predicting oncologic outcomes of localized renal cell carcinoma. J Urol. 2014;192:1043–1049. | |
Lee HW, Jeong BC, Seo SI, et al. Prognostic significance of visceral obesity in patients with advanced renal cell carcinoma undergoing nephrectomy. Int J Urol. 2015;22(5):455–461. | |
Klinghoffer Z, Yang B, Kapoor A, Pinthus JH. Obesity and renal cell carcinoma: epidemiology, underlying mechanisms and management considerations. Expert Rev Anticancer Ther. 2009;9:975–987. | |
Khandekar MJ, Cohen P, Spiegelman BM. Molecular mechanisms of cancer development in obesity. Nat Rev Cancer. 2011;11:886–895. | |
Sharifi N, Farrar WL. Perturbations in hypoxia detection: a shared link between hereditary and sporadic tumor formation? Med Hypotheses. 2006;66:732–735. | |
Solarek W, Czarnecka AM, Escudier B, et al. Insulin and IGFs in renal cancer risk and progression. Endocr Relat Cancer. 2015;22(5):R253–R264. | |
Gago-Dominguez M, Castelao JE. Lipid peroxidation and renal cell carcinoma: further supportive evidence and new mechanistic insights. Free Radic Biol Med. 2006;40:721–733. | |
Setiawan VW, Stram DO, Nomura AM, Kolonel LN, Henderson BE. Risk factors for renal cell cancer: the multiethnic cohort. Am J Epidemiol. 2007;166:932–940. | |
Shen T, Shu XO, Xiang YB, et al. Association of hypertension and obesity with renal cell carcinoma risk: a report from the Shanghai Men’s and Women’s Health Studies. Cancer Causes Control. 2015;26(8):1173–1180. | |
Flaherty KT, Fuchs CS, Colditz GA, et al. A prospective study of body mass index, hypertension, and smoking and the risk of renal cell carcinoma (United States). Cancer Causes Control. 2005;16:1099. | |
Vatten LJ, Trichopoulos D, Holmen J, Nilsen TI. Blood pressure and renal cancer risk: the HUNT Study in Norway. Br J Cancer. 2007;97:112–114. | |
Weikert S, Boeing H, Pischon T, et al. Blood pressure and risk of renal cell carcinoma in the European prospective investigation into cancer and nutrition. Am J Epidemiol. 2008;167(4):438–446. | |
Coughlin SS, Neaton JD, Randall B, Sengupta A. Predictors of mortality from kidney cancer in 332,547 men screened for the Multiple Risk Factor Intervention Trial. Cancer. 1997;79:2171–2177. | |
Zucchetto A, Dal Maso L, Tavani A, et al. History of treated hypertension and diabetes mellitus and risk of renal cell cancer. Ann Oncol. 2007;18:596–600. | |
Brennan P, van der Hel O, Moore LE, et al. Tobacco smoking, body mass index, hypertension and kidney cancer risk in central and eastern Europe. Br J Cancer. 2008;99:1912–1915. | |
Chow WH, Gridley G, Fraumeni JF Jr, Järvholm B. Obesity, hypertension, and the risk of kidney cancer in men. New Engl J Med. 2000;343:1305–1311. | |
Colt JS, Schwartz K, Graubard BI, et al. Hypertension and risk of renal cell carcinoma among white and black Americans. Epidemiology. 2011;22:797–804. | |
Fraser GE, Phillips RL, Beeson WL. Hypertension, antihypertensive medication and risk of renal carcinoma in California Seventh-Day Adventists. Int J Epidemiol. 1990;19:832–838. | |
Fryzek JP, Poulsen AH, Johnsen SP, McLaughlin JK, Sørensen HT, Friis S. A cohort study of antihypertensive treatments and risk of renal cell cancer. Br J Cancer. 2006;92:1302–1306. | |
Grove JS, Nomura A, Severson RK, Stemmermann GN. The association of blood pressure with cancer incidence in a prospective study. Am J Epidemiol. 1991;134:942–947. | |
Heath CW Jr, Lally CA, Calle EE, McLaughlin JK, Thun MJ. Hypertension, diuretics, and antihypertensive medications as possible risk factors for renal cell cancer. Am J Epidemiol. 1997;45:607–613. | |
Chow WH, McLaughlin JK, Mandel JS, Wacholder S, Niwa S, Fraumeni JF Jr. Risk of renal cell cancer in relation to diuretics, antihypertensive drugs, and hypertension. Cancer Epidemiol Biomarkers Prev. 1995;4(4):327–331. | |
Parker A, Freeman LB, Cantor K, Lynch C. Self-report of smoking, obesity and hypertension history and survival among a cohort of Iowa renal cell carcinoma cases. Ann Epidemiol. 2000;10(7):467–468. | |
Haase VH. The VHL/HIF oxygen-sensing pathway and its relevance to kidney disease. Kidney Int. 2006;69:1302–1307. | |
Heinz-Peer G, Schoder M, Rand T, Mayer G, Mostbeck GH. Prevalence of acquired cystic kidney disease and tumors in native kidneys of renal transplant recipients: a prospective US study. Radiology. 1995;195:667. | |
Brennan JF, Stilmant MM, Babayan RK, Siroky MB. Acquired renal cystic disease: implications for the urologist. Br J Urol. 1991;67(4):342–348. | |
Lee HH, Choi KH, Yang SC, Han WK. Renal cell carcinoma in kidney transplant recipients and dialysis patients. Korean J Urol. 2012;53(4):229–233. | |
Truong LD, Krishnan B, Cao JT, Barrios R, Suki WN. Renal neoplasm in acquired cystic kidney disease. Am J Kidney Dis. 1995;26:1–12. | |
Matson MA, Cohen EP. Acquired cystic kidney disease: occurrence, prevalence, and renal cancers. Medicine (Baltimore). 1990;69:217–226. | |
Neuzillet Y, Lay F, Luccioni A, et al. De novo renal cell carcinoma of native kidney in renal transplant recipients. Cancer. 2005;103:251–257. | |
Schwarz A, Vatandaslar S, Merkel S, Haller H. Renal cell carcinoma in transplant recipients with acquired cystic kidney disease. Clin J Am Soc Nephrol. 2007;2:750–756. | |
Lee JE, Hunter DJ, Spiegelman D, et al. Alcohol intake and renal cell cancer in a pooled analysis of 12 prospective studies. J Natl Cancer Inst. 2007;99:801–810. | |
Song DY, Song S, Song Y, Lee JE. Alcohol intake and renal cell cancer risk: a meta-analysis. Br J Cancer. 2012;106:1881–1890. | |
Mahabir S, Leitzmann MF, Virtanen MJ, et al. Prospective study of alcohol drinking and renal cell cancer risk in a cohort of Finnish male smokers. Cancer Epidemiol Biomarkers Prev. 2005;14:170–175. | |
Bellocco R, Pasquali E, Rota M, et al. Alcohol drinking and risk of renal cell carcinoma: results of a meta-analysis. Ann Oncol. 2012;23:2235–2244. | |
Washio M, Mori M, Mikami K, et al. Cigarette smoking and other risk factors for kidney cancer death in a Japanese population: Japan Collaborative Cohort Study for evaluation of cancer risk (JACC study). Asian Pac J Cancer Prev. 2014;14:6523–6528. | |
Karami S, Daugherty SE, Purdue MP. A prospective study of alcohol consumption and renal cell carcinoma risk. Int J Cancer. 2015;137:238–242. | |
Cheng G, Xie L. Alcohol intake and risk of renal cell carcinoma: a meta-analysis of published case-control studies. Arch Med Sci. 2011;7:648–657. | |
Xu X, Zhu Y, Zheng X, Xie L. Does beer, wine or liquor consumption correlate with the risk of renal cell carcinoma? A dose-response meta-analysis of prospective cohort studies. Oncotarget. 2015; 6(15):13347–13358. | |
McCredie M, Pommer W, McLaughlin JK, et al. International renal cell cancer study. II. Analgesics. Int J Cancer. 1995;60:345–349. | |
Gago-Dominguez M, Yuan JM, Castelao JE, Ross RK, Yu MC. Regular use of analgesics is a risk factor for renal cell carcinoma. Br J Cancer. 1999;81:542–548. | |
Kaye JA, Myers MW, Jick H. Acetaminophen and the risk of renal and bladder cancer in the general practice research database. Epidemiology. 2001;12:690–694. | |
Cho E, Curhan G, Hankinson SE, et al. Prospective evaluation of analgesic use and risk of renal cell cancer. Arch Intern Med. 2011; 171(16):1487–1493. | |
Choueiri TK, Je Y, Cho E. Analgesic use and the risk of kidney cancer: a meta-analysis of epidemiologic studies. Int J Cancer. 2014;134(2):384–396. | |
Joh HK, Willett WC, Cho E. Type 2 diabetes and the risk of renal cell cancer in women. Diabetes Care. 2011;34:1552. | |
Lindblad P, Chow WH, Chan J, et al. The role of diabetes mellitus in the aetiology of renal cell cancer. Diabetologia. 1999;42:107–112. | |
Washio M, Mori M, Khan M, et al; JACC Study Group. Diabetes mellitus and kidney cancer risk: the results of Japan Collaborative Cohort Study for evaluation of cancer risk (JACC Study). Int J Urol. 2007;14:393–397. | |
Larsson SC, Wolk A. Diabetes mellitus and incidence of kidney cancer: a meta-analysis of cohort studies. Diabetologia. 2011;54:1013–1018. | |
Bao C, Yang X, Xu W, et al. Diabetes mellitus and incidence and mortality of kidney cancer: a meta-analysis. J Diabetes Complications. 2013;27:357–364. | |
Noto H, Tsujimoto T, Noda M. Significantly increased risk of cancer in diabetes mellitus patients: a meta-analysis of epidemiological evidence in Asians and non-Asians. J Diabetes Investig. 2012;3(1):24–33. | |
Habib SL, Prihoda TJ, Luna M, Werner SA. Diabetes and risk of renal cell carcinoma. J Cancer. 2012;3:42–48. | |
Rashidkhani B, Lindblad P, Wolk A. Fruits, vegetables and risk of renal cell carcinoma: a prospective study of Swedish women. Int J Cancer. 2005;113:451–455. | |
Brock KE, Ke L, Gridley G, et al. Fruit, vegetables, fiber and micronutrients and risk of US renal cell carcinoma. Br J Nutr. 2012;108:1077–1085. | |
Lee JE, Mannisto S, Spiegelman D, et al. Intakes of fruit, vegetables, and carotenoids and renal cell cancer risk: a pooled analysis of 13 prospective studies. Cancer Epidemiol Biomarkers Prev. 2009;18:1730–1739. | |
Lof M, Sandin S, Lagiou P, Trichopoulos D, Adami HO, Weiderpass E. Fruit and vegetable intake and risk of cancer in the Swedish women’s lifestyle and health cohort. Cancer Causes Control. 2011;22(2):283–289. | |
Bertoia M, Albanes D, Mayne ST, Männistö S, Virtamo J, Wright ME. No association between fruit, vegetables, antioxidant nutrients and risk of renal cell carcinoma. Int J Cancer. 2010;126:1504–1512. | |
Weikert S, Boeing H, Pischon T, et al. Fruits and vegetables and renal cell carcinoma: findings from the European prospective investigation into cancer and nutrition (EPIC). Int J Cancer. 2006;118:3133–3139. | |
Huang TB, Ding PP, Chen JF, et al. Dietary fiber intake and risk of renal cell carcinoma: evidence from a meta-analysis. Med Oncol. 2014;31(8):125. | |
Zhao J, Zhao L. Cruciferous vegetables intake is associated with lower risk of renal cell carcinoma: evidence from a meta-analysis of observational studies. PLoS One. 2013;8(10):e75732. | |
McLaughlin JK, Gao YT, Gao RN, et al. Risk factors for renal cell cancer in Shanghai, China. Int J Cancer. 1992;52:562–565. | |
Washio M, Mori M, Mikami K, et al. Risk factors for renal cell carcinoma in a Japanese population. Asian Pac J Cancer Prev. 2014;15:9065–9070. | |
Hu J, Mao Y, White K. Diet and vitamin or mineral supplements and risk of renal cell carcinoma in Canada. Cancer Causes Control. 2003;14:705–714. | |
Dellavalle CT, Daniel CR, Aschebrook-Kilfoy B, et al. Dietary intake of nitrate and nitrite and risk of renal cell carcinoma in the NIH-AARP Diet and Health Study. Br J Cancer. 2013;108:205–212. | |
Brock KE, Gridley G, Chiu BC, Ershow AG, Lynch CF, Cantor KP. Dietary fat and risk of renal cell carcinoma in the USA: a case-control study. Br J Nutr. 2009;101(8):1228–1238. | |
Sali D, Boffetta P. Kidney cancer and occupational exposure to asbestos: a meta-analysis of occupational cohort studies. Cancer Causes Control. 2000;11:37–47. | |
Smith AH, Shearn VI, Wood R. Asbestos and kidney cancer: the evidence supports a causal association. Am J Ind Med. 1989;16:159–166. | |
Karami S, Boffetta P, Stewart PS, et al. Occupational exposure to dusts and risk of renal cell carcinoma. Br J Cancer. 2011;104:1797–1803. | |
Pesch B, Haerting J, Ranft U, Klimpel A, Oelschlägel B, Schill W. Occupational risk factors for renal cell carcinoma: agent-specific results from a case-control study in Germany. MURC Study Group. Multicenter urothelial and renal cancer study. Int J Epidemiol. 2000;29:1014–1024. | |
EL-Safty IA, Gadallah M, Shouman AE, Nessim DE. Subclinical nephrotoxicity caused by smoking and occupational silica exposure among Egyptian industrial workers. Arch Med Res. 2003;34:415–421. | |
Shannon H, Muir A, Haines T, Verma D. Mortality and cancer incidence in Ontario glass fiber workers. Occup Med (Lond). 2005;55:528–534. | |
Stone RA, Youk AO, Marsh GM, Buchanich JM, Smith TJ. Historical cohort study of US man-made vitreous fiber production workers IX: summary of 1992 mortality follow up and analysis of respiratory system cancer among female workers. Occup Environ Med. 2004;46:55–67. | |
Steenland K. One agent, many diseases: exposure-response data and comparative risks of different outcomes following silica exposure. Am J Ind Med. 2005;48:16–23. | |
McCredie M, Stewart JH. Risk factors for kidney cancer in New South Wales, IV. Occupation. Br J Ind Med. 1993;50:349–354. | |
Karami S, Boffetta P, Brennan P, et al. Renal cancer risk and occupational exposure to polycyclic aromatic hydrocarbons and plastics. J Occup Environ Med. 2011;53:218–223. | |
Boffetta P, Fontana L, Stewart P, et al. Occupational exposure to arsenic, cadmium, chromium, lead and nickel, and renal cell carcinoma: a case-control study from Central and Eastern Europe. Occup Environ Med. 2011;68:723–728. | |
Kelsh MA, Alexander DD, Mink PJ, Mandel JH. Occupational trichloroethylene exposure and kidney cancer: a meta-analysis. Epidemiology. 2010;21:95–102. | |
Il’yasova D, Schwartz GG. Cadmium and renal cancer. Toxicol Appl Pharmacol. 2005;207:179–186. | |
Hu J, Mao Y, White K. Renal cell carcinoma and occupational exposure to chemicals in Canada. Occup Med. 2002;52(3):157–164. | |
Bruning T, Pesch B, Wiesenhutter B, et al. Renal cell cancer risk and occupational exposure to trichloroethylene: results of a consecutive case-control study in Arnsberg, Germany. Am J Ind Med. 2003;43:274–285. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.