Back to Journals » Clinical Ophthalmology » Volume 19
Renaissance of an Emerging Pathogen—Pythium insidiosum Keratitis: An Indian Perspective
Received 18 September 2025
Accepted for publication 15 December 2025
Published 18 December 2025 Volume 2025:19 Pages 4811—4830
DOI https://doi.org/10.2147/OPTH.S568552
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Bharat Gurnani,1 Kirandeep Kaur2
1Department of Cataract, Cornea and Refractive Surgery, Gomabai Netralaya and Research Centre, Neemuch, MP, 458441, India; 2Department of Cataract, Pediatric Ophthalmology and Strabismus, Gomabai Netralaya and Research Centre, Neemuch, MP, 458441, India
Correspondence: Bharat Gurnani, Department of Cataract, Cornea and Refractive Surgery, Gomabai Netralaya and Research Centre, Neemuch, MP, 458441, India, Tel +919080523059, Email [email protected]
Abstract: Pythium insidiosum keratitis is an aggressive, vision-threatening corneal infection increasingly recognized across India, particularly among agricultural workers during monsoon season. Frequently misclassified as fungal keratitis, it responds poorly to conventional antifungals because the oomycete has a cellulose- and β-glucan–rich wall and lacks ergosterol, leading to therapeutic delay and rapid stromal melt. Indian cohorts have refined a practical diagnostic signature such as tentacular or reticular peripheral infiltrates with guttering, early endothelial plaque and hypopyon, and minimal satellite lesions. Calcofluor white and KOH show broad, ribbon-like, sparsely septate filaments; blood agar often grows colonies while Sabouraud shows scant growth; IVCM reveals thin, linear, right-angle branching hyphae; and PCR/ITS sequencing confirms species. Emerging immunology indicates early evasion of pattern-recognition receptors (TLR/CLR pathways) followed by dysregulated neutrophilic inflammation that accelerates collagenolysis. Management in India has converged on a surgery-first bias for deep or progressive disease early therapeutic keratoplasty with wide margins combined with targeted medical therapy: topical linezolid 0.2% and azithromycin 1% (± minocycline systemically), aggressive lubrication, and stromal melt mitigation (oral doxycycline, cautious steroids only post-control). Adjuncts include cyanoacrylate for impending perforation and intracameral/ intrastromal antibiotics in selected cases. Outcomes improve with rapid organism-specific therapy, meticulous peri-operative planning, and vigilant recurrence surveillance. India’s experience underscores priorities for the next decade: point-of-care diagnostics (LAMP/CRISPR), standardized drug susceptibility platforms, optimized peri-keratoplasty protocols, and host-directed immunomodulation to temper destructive inflammation without impairing clearance. This review synthesizes epidemiology, clinical diagnostics, immunopathogenesis, and management, translating India-derived insights into a pragmatic framework for regions confronting the global spread of Pythium keratitis.
Keywords: Pythium insidiosum, keratitis, India, cellulose cell wall, tentacular infiltrates, keratoplasty, immunotherapy
Introduction
Pythium insidiosum, once considered an obscure aquatic pathogen confined largely to veterinary infections, has rapidly transformed into a significant and uniquely challenging cause of human keratitis.1 Over the past decade, its clinical recognition has expanded dramatically, particularly in India, where microbial keratitis already represents a major cause of preventable corneal blindness. In this setting—characterized by agricultural exposure, water-associated trauma, and variable access to tertiary eye care—Pythium keratitis has shifted from an infrequently encountered organism to a pathogen of considerable public health concern.2 This epidemiologic re-emergence has required clinicians to reassess long-held assumptions about atypical keratitis and to adopt diagnostic and therapeutic strategies tailored to the specific biology of Pythium. Historically, global reports of Pythium keratitis were limited to sporadic cases from Thailand, Australia, and the United States. However, India now accounts for the highest number of documented cases worldwide, with increasing reports from states such as Tamil Nadu, Karnataka, Odisha, and West Bengal.3 Several tertiary eye hospitals have documented Pythium in 2–5% of microbial keratitis isolates—an extraordinary rise from earlier decades when it was nearly absent from the literature. This increased detection reflects both heightened awareness and improved laboratory confirmation, but also environmental and occupational conditions that foster zoospore proliferation.4 India’s substantial agrarian workforce, combined with monsoon-related flooding and extensive interaction with stagnant water, creates ideal conditions for exposure, especially following corneal trauma with vegetative material.5
The clinical challenge of Pythium keratitis stems largely from its close resemblance to fungal ulcers. Patients often present with reticular or tentacular infiltrates, dense stromal involvement, or hypopyon—features that mimic filamentous fungi and lead to empirical antifungal treatment.6 Yet Pythium is not a fungus; it is an oomycete with a cellulose-rich cell wall and an absence of ergosterol, rendering conventional antifungal agents such as natamycin, voriconazole, and amphotericin B ineffective.7 This biological mismatch contributes directly to treatment delays, rapid stromal melt, and high rates of perforation. Recognizing this risk, Indian clinicians have played a leading role in describing distinctive clinical clues—such as peripheral guttering, early endothelial plaques, and linear tentacular extensions—that help differentiate Pythium from fungal keratitis.8 Diagnosis remains another critical barrier. On KOH or calcofluor white staining, Pythium filaments appear broad, ribbon-like, and sparsely septate, overlapping with mucorales and complicating early interpretation. Sabouraud dextrose agar, a standard fungal medium, often yields poor or delayed growth. Indian laboratories have demonstrated more reliable recovery on blood agar, where characteristic colonies appear within 24–48 hours, although definitive identification often requires leaf incubation techniques.9 Molecular tools—including PCR assays and ITS sequencing—provide excellent specificity but are largely restricted to specialized centers. Advances such as in vivo confocal microscopy, which demonstrates thin, linear, right-angled stromal filaments, have proven especially valuable in resource-limited settings and often raise suspicion before culture confirmation.10 Therapeutically, the Indian experience has driven a paradigm shift. Persistent antifungal failures prompted systematic exploration of alternative antimicrobial agents.11 Clinical evidence now supports the use of topical linezolid 0.2% and azithromycin 1% as first-line therapy—an approach that contrasts sharply with management of fungal or bacterial keratitis.12 Oral tetracyclines, such as doxycycline and minocycline, are frequently added for their stromal-protective effects and immunomodulatory benefits. Nevertheless, medical therapy alone is often insufficient. Early therapeutic keratoplasty (TPK) with wide excision remains central to management, though recurrence within the graft and postoperative complications such as endothelial plaques continue to pose challenges. Indian protocols emphasize perioperative systemic antibiotics, delayed initiation of topical steroids, and meticulous postoperative surveillance to reduce reinfection risk.1 Beyond clinical observations, Indian research has begun to elucidate the immunopathogenesis of Pythium keratitis. Emerging evidence suggests that Pythium evades early immune recognition by masking molecular patterns normally detected by Toll-like and C-type lectin receptors, allowing unchecked stromal invasion.2 The subsequent host response is delayed yet intense, dominated by heavy neutrophilic infiltration and marked pro-inflammatory cytokine release, which accelerates stromal breakdown and collagenolysis.3 Understanding these host–pathogen interactions offers opportunities to explore adjunctive, host-directed therapies aimed at tempering destructive inflammation while maintaining microbial control. Finally, the Indian experience highlights critical systemic and public health considerations. Many affected individuals present late after receiving empirical antifungals from peripheral centers or traditional healers, by which time corneal damage is often irreversible. This underscores the urgent need for community education, improved referral pathways, and point-of-care diagnostics in secondary eye-care facilities. National programs such as the NPCB have begun to recognize atypical pathogens like Pythium within broader corneal blindness strategies, reflecting a shift toward more comprehensive microbial surveillance. Collectively, India has played a pivotal role in defining the epidemiology, clinical phenotype, laboratory diagnosis, therapeutic protocols, and immunological underpinnings of Pythium keratitis. What was once a rare zoonotic pathogen has emerged as a global ophthalmic threat, and the Indian experience now serves as the primary knowledge base guiding international clinicians and researchers. This review differs from our earlier publications by integrating the most recent epidemiological patterns and consolidating several advances that were not previously available. In particular, we highlight newly emerging diagnostic tools—including AI-assisted AS-OCT interpretation, high-specificity IVCM features, and rapid molecular platforms such as LAMP and RPA—and we summarize evolving concepts in biosensor-based detection and host-directed therapy. This review also provides an updated synthesis of translational insights into immunopathogenesis and incorporates current refinements in early surgical decision-making. Together, these additions offer a forward-looking perspective that extends beyond our prior work and reflects the latest developments in the field.
Methodology
Search Strategy
A structured literature search was conducted to identify relevant publications on Pythium insidiosum keratitis. The search was performed across major biomedical databases, including PubMed/MEDLINE, Scopus, Web of Science, and Google Scholar. Additional sources such as reference lists of key articles, conference proceedings, and institutional case series from Indian tertiary eye-care centers were reviewed to capture region-specific data.
Search Terms
The following MeSH terms and free-text keywords were used in various combinations: “Pythium insidiosum”, “Pythium keratitis”, “Oomycete keratitis”, “Pythium infection”, “microbial keratitis”, “corneal ulcer”, “linezolid”, “azithromycin”, “therapeutic keratoplasty”, “India”, “epidemiology”, “diagnosis”, “zoospore”, “immunopathogenesis”. Boolean operators (AND/OR) were applied to maximize sensitivity.
Time Frame
Given the sharp rise in reported cases in the past decade, the primary search included studies from 1988 to 2025. Earlier historical reports were included selectively to provide context for epidemiological evolution.
Inclusion Criteria
Studies were included if they met the following criteria: Discussed human ocular infection caused by Pythium insidiosum. Reported clinical features, diagnosis, microbiology, management, outcomes, or immunopathogenesis. Provided original data, such as case reports, case series, observational studies, or laboratory studies. Articles from India and other global regions were included to allow comparative interpretation.
Exclusion Criteria
The following were excluded: Studies describing only Veterinary Pythiosis without ophthalmic relevance. Articles lacking primary data (eg, commentaries without clinical or laboratory details). Reports where keratitis etiology remained unconfirmed or mixed infections without clear attribution to Pythium. Non-English publications lacking available translations.
Study Selection Process
Two reviewers independently screened the titles and abstracts for relevance. Full-text articles meeting the eligibility criteria were assessed and synthesized. Any disagreements were resolved by discussion and consensus.
Data Extraction and Synthesis
Key information extracted included: Demographics and geographic distribution, clinical hallmarks and diagnostic features, laboratory findings (KOH/CFW, culture, PCR), medical therapy (linezolid, azithromycin, adjuncts), surgical management (TPK timing, techniques, outcomes), recurrence patterns and prognostic factors, immunological and pathogenesis insights. Given the heterogeneity of available literature, a narrative synthesis approach was used rather than a meta-analysis. Indian cohort data were given emphasis due to the high regional prevalence and contribution to global understanding.
Epidemiology
The epidemiology of Pythium insidiosum keratitis in India has undergone a striking transformation in the past decade, with rising case notifications from multiple states. While earlier considered sporadic or anecdotal, recent multicenter reports now identify Pythium as a significant contributor to microbial keratitis, accounting for 2–5% of cases in tertiary eye care hospitals.1 Geographic distribution has not been uniform: coastal and riverine belts appear disproportionately affected, likely reflecting the pathogen’s preference for warm, aquatic environments where zoospore proliferation is greatest. States such as Pondicherry,2 Tamil Nadu,3 Andhra Pradesh4 and Odisha,5 have reported clusters, though isolated cases from central and northern India suggest that the organism’s reach may extend beyond traditionally recognized ecological niches. This regional patterning underscores the interplay between environment and occupation in shaping disease burden. The typical patient profile in India further highlights this ecological link. Most affected individuals are outdoor or agricultural workers, particularly those involved in paddy cultivation, fishing, or manual labour in standing water.6 Ocular trauma with vegetative material or direct exposure to contaminated water is a consistent risk factor across studies, emphasizing how occupational hazards translate into microbial vulnerability. Unlike other opportunistic ocular infections, systemic immunosuppression has not emerged as a major predisposing factor.7 Indeed, many patients are otherwise healthy young adults whose livelihoods place them in direct contact with high-risk environments. This demographic skew not only magnifies the socioeconomic consequences of visual loss but also illustrates why Pythium has become a uniquely Indian challenge. Another important feature of the epidemiology is its seasonal clustering. Several Indian centers have observed peak caseloads in the months following the monsoon, when stagnant water, humid soil, and flooding events provide ideal conditions for Pythium growth and dispersal. Monsoon-related agricultural activity further increases exposure, creating a confluence of risk factors.2 The seasonal rhythm of Pythium keratitis resembles patterns seen in other filamentous keratitis pathogens but with a sharper and more consistent correlation to rainfall and waterlogged environments. Such clustering carries important implications for surveillance, resource allocation, and public awareness campaigns, allowing eye care facilities in endemic regions to anticipate and prepare for seasonal surges.8 From an epidemiologic standpoint, the Indian experience has been pivotal in transforming global understanding of Pythium keratitis. India’s high case volumes have enabled recognition of its clinical profile, refined diagnostic cues, and clarified risk factors with far greater precision than scattered case reports elsewhere. As surveillance continues to expand and molecular confirmation becomes more accessible, it is likely that the true burden of Pythium keratitis in India will prove even greater than current estimates. The combination of environmental predisposition, occupational exposure, and seasonal vulnerability makes India a natural epicenter for this pathogen, with lessons that resonate across other tropical and subtropical regions now beginning to report their own emerging cases. Over the past decade, Pythium insidiosum keratitis has transitioned from a rare clinical entity to a significant and increasingly recognized cause of microbial keratitis in tropical and subtropical regions. India continues to report the highest burden globally, particularly in agricultural states where warm, humid climates promote zoospore proliferation in stagnant water sources. Recent surveillance data from tertiary centers indicate that Pythium now accounts for 5–10% of ulcers initially presumed to be fungal, marking a substantial rise compared to older reports where it was virtually absent from keratitis registries. Misdiagnosis remains a major contributor to poor outcomes, with up to 50% of untreated or late-treated cases requiring therapeutic keratoplasty, and over 30% resulting in severe visual impairment. Emerging international reports from Southeast Asia and parts of the Middle East suggest that Pythium may be under-recognized rather than truly rare, with environmental and occupational exposures—especially agricultural labour, trauma in paddy fields, and water-related injuries—driving incidence. Increased reporting may also reflect better diagnostic suspicion, improved microbiological techniques, and heightened clinician awareness. Although most published reports highlight a high burden of Pythium keratitis in coastal regions such as Puducherry, Tamil Nadu, Andhra Pradesh, and Odisha, emerging data indicate that the pathogen is also present in several other coastal states including Karnataka, West Bengal, Gujarat, Maharashtra, and Goa but with fewer confirmed cases. The lower numbers from these regions likely reflect under-recognition, limited laboratory confirmation, and reporting gaps rather than true absence of disease, particularly because the environmental conditions (standing water, paddy fields, aquaculture zones, warm–humid climate) are comparable. Beyond farmers, multiple other occupational groups appear to be at elevated risk, including fishermen, aquaculture workers, paddy-field laborers, sanitation workers exposed to sewage or wet soil, and individuals engaged in activities involving prolonged exposure to stagnant or floodwater. Recent case series from high-burden districts also suggest increased susceptibility among young adults engaged in manual outdoor labour, as well as individuals with frequent minor ocular trauma in humid settings. Incorporating these broader epidemiological patterns provides a more complete understanding of India’s geographic and occupational risk landscape.9 Figure 1 depicts the epidemiological distribution of Pythium insidiosum keratitis.
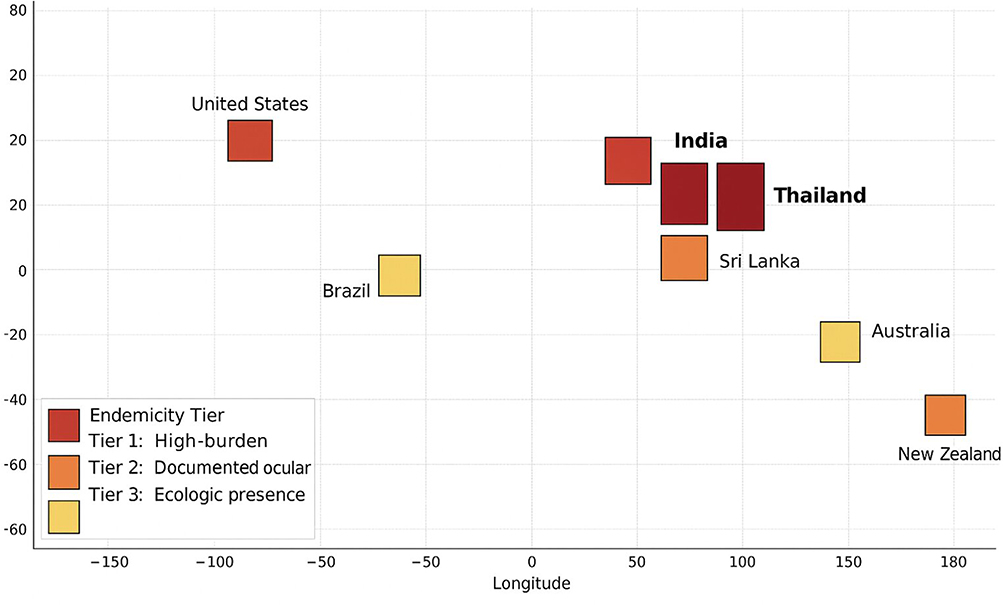 |
Figure 1 Depicts the epidemiological distribution of Pythium insidiosum keratitis. India and Thailand are highlighted in bold to indicate high endemicity of Pythium insidiosum cases. |
Microbiology and Pathogenesis
The microbiology of Pythium insidiosum distinguishes it fundamentally from both bacteria and fungi, and explains many of the diagnostic and therapeutic challenges clinicians encounter. Unlike true fungi, the cell wall of Pythium is composed primarily of cellulose and sparse β-1,3-glucan, with complete absence of chitin, a defining fungal marker.10 This structural composition not only contributes to its misidentification under the microscope but also underlies its poor response to conventional antifungal therapy. Recent biochemical studies have also highlighted the presence of hydroxyproline-rich proteins, which may contribute to rigidity and environmental resilience, as well as interactions with host tissue.11 The plasma membrane notably lacks ergosterol, further explaining the ineffectiveness of polyenes and azoles, the cornerstone drugs for fungal keratitis. The life cycle of Pythium insidiosum is equally relevant to its pathogenicity. It reproduces asexually through motile biflagellate zoospores, which are released in aquatic environments and exhibit chemotaxis toward damaged corneal epithelium.12 Upon reaching the corneal surface, the zoospores encyst, adhere firmly, and germinate into hyphae. These hyphae penetrate the corneal stroma, proliferating rapidly and causing tissue necrosis, melt, and eventual perforation if unchecked. This ability to exploit even minor epithelial breaches explains why ocular trauma with vegetative matter or water splash is such a consistent risk factor in endemic Indian settings.13 The invasive hyphae often track deep within the stroma, producing clinical signs such as tentacular infiltrates and endothelial plaques. The pathogenesis of Pythium keratitis is shaped as much by host response as by the organism’s intrinsic virulence. Early in infection, Pythium demonstrates remarkable immune evasion strategies. By masking its β-glucan components, it effectively blunts recognition by host pattern recognition receptors, particularly Dectin-1 and Toll-like receptor 4 (TLR4).14 This dampened signalling delays the activation of innate immune pathways and cytokine release. Partial activation through TLR2 pathways leads to a muted inflammatory response, insufficient for effective clearance but enough to allow stromal invasion. Only later in the course of disease does the host mount a more robust immune response, characterized by delayed IL-1β release and neutrophil influx.15 Unfortunately, by this stage the infection is well established, and the inflammatory response becomes exaggerated and destructive, contributing to collagenolysis, corneal melt, and scarring. This biphasic interaction—early immune evasion followed by delayed, hyperinflammatory damage helps explain the aggressive clinical course and poor prognosis of Pythium keratitis despite appropriate surgical and medical interventions.16 In sum, the unique cell wall architecture, aquatic life cycle with zoospore-driven invasion, and immunological stealth collectively define the microbiology and pathogenesis of Pythium insidiosum. These insights, many of which have been derived from Indian case series and laboratory investigations, underscore why Pythium behaves differently from classical fungal pathogens and demand a distinct diagnostic and therapeutic paradigm.16 Early diagnosis is critical in Pythium keratitis, as the window during which corneal damage remains potentially reversible is narrow. The most appropriate and actionable stage for diagnosis is within the first 3–5 days of symptom onset, when the organism is largely confined to the anterior to mid-stroma and before enzymatic collagenolysis accelerates tissue melt. During this early phase, characteristic features—such as tentacular infiltrates, reticular or “sinewy” stromal patterns, peripheral guttering, and early endothelial plaques—are most evident and can be captured reliably using AS-OCT and in vivo confocal microscopy. At this stage, prompt initiation of organism-directed therapy (linezolid ± azithromycin) can halt progression and, in many cases, prevent the rapid stromal necrosis that necessitates therapeutic keratoplasty. Delayed diagnosis, particularly after deep stromal invasion or limbal extension, significantly reduces the likelihood of medical salvage and is associated with higher rates of perforation and recurrence. Emphasizing diagnosis during this early, pre-melt phase is therefore essential to preserving corneal integrity and improving outcomes. Figure 2 depicts the microbiology and pathogenesis of Pythium insidiosum keratitis.
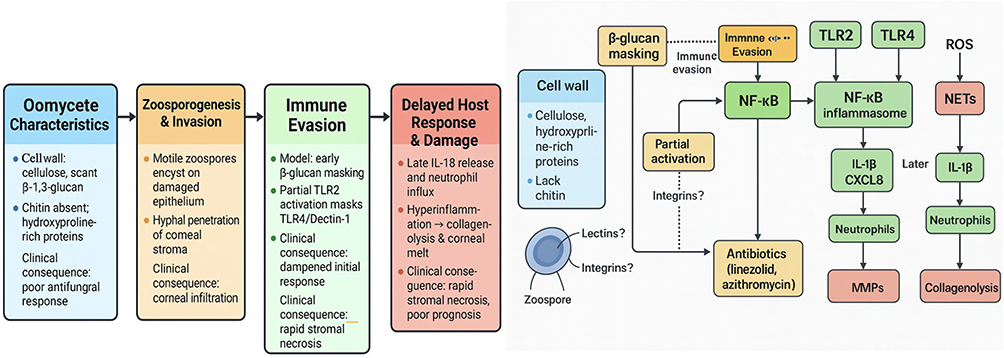 |
Figure 2 Depicts the microbiology and pathogenesis of Pythium insidiosum keratitis. |
Mechanism of Resistance
Although true antimicrobial resistance in Pythium insidiosum is not yet well-defined, emerging observations suggest that reduced responsiveness may develop under therapeutic pressure. Laboratory studies have shown variable susceptibility to linezolid and macrolides across environmental isolates, raising the possibility of strain-specific differences rather than uniform sensitivity. Clinically, delayed presentation, deep stromal invasion, and biofilm-like organization within necrotic tissue may mimic resistance by limiting drug penetration rather than reflecting true genetic resistance. The absence of ergosterol-targeted pathways also means that prior antifungal exposure does not induce resistance but can delay appropriate therapy, indirectly worsening outcomes. Ongoing genomic and transcriptomic work is beginning to identify stress-response pathways and efflux mechanisms that may contribute to reduced drug efficacy, underscoring the need for standardized susceptibility testing and longitudinal surveillance as antibiotic-based regimens become widely adopted.2,9,17
Clinical Features
The clinical presentation of Pythium insidiosum keratitis is often dramatic, with patients reporting severe ocular pain, photophobia, watering, and rapidly worsening vision. Unlike bacterial keratitis, the pain is often disproportionate to the size of the infiltrate, and progression may be swift despite empirical antifungal therapy.2 A history of antecedent trauma with vegetative matter or exposure to contaminated water is frequently elicited, particularly in patients from rural and agrarian backgrounds. On slit-lamp examination, several distinctive features have now been recognized as highly suggestive of Pythium keratitis. The most characteristic are feathery, branching “tentacular” infiltrates that radiate outward from the central lesion into the peripheral stroma, creating a reticular or net-like pattern.9 Peripheral guttering is another important diagnostic clue, where localized thinning occurs at the margins of the infiltrate, giving a hollowed-out appearance. In many cases, a reticular or plaque like stromal infiltrate develops, which can be mistaken for deep fungal infection. In the early course of the disease, endothelial plaques may be minimal or absent, in contrast to the dense endothelial exudates seen with aggressive fungal keratitis.17 However, progression can be rapid, with extensive stromal necrosis, thinning, and corneal melt leading to impending perforation. Certain red flags help distinguish Pythium keratitis from fungal ulcers at the bedside. Chief among these is the lack of clinical response to natamycin or azole antifungals within 48–72 hours of therapy initiation. Instead of improvement, the infiltrates often continue to expand, with circumferential spread into the periphery and deep stromal invasion despite maximal antifungal therapy.1 This paradoxical worsening under antifungal coverage should immediately raise suspicion of Pythium, especially when accompanied by tentacular extensions or guttering. Unlike typical fungal ulcers, satellite lesions are uncommon, and hypopyon, though present, tends to be sterile and disproportionate to the severity of stromal disease. Collectively, these clinical observations have been shaped by extensive experience in Indian tertiary care centers, where large case series have allowed the delineation of a clinical signature of Pythium keratitis. Recognition of these features at an early stage is vital for initiating organism-specific therapy, planning timely surgical intervention, and preventing catastrophic visual outcomes.17
Diagnosis
Clinical Indicators
The clinical diagnosis of Pythium insidiosum keratitis in India hinges on the ability to recognize subtle but distinctive features at the slit lamp, often in patients with a history of rural exposure. One of the earliest and most reliable bedside indicators is the presence of tentacular stromal extensions linear infiltrates radiating outward from the central lesion into uninvolved cornea.16 These “feathery arms” or reticular projections are highly suggestive of Pythium and differ from the satellite lesions typically seen in fungal ulcers. Accompanying this is peripheral guttering, a unique phenomenon in which the peripheral corneal stroma thins and excavates, producing a hollowed-out appearance adjacent to the infiltrate. Together, tentacular spread and guttering are now considered hallmark features in Indian case series.18 Another important clue, especially emphasized by tertiary eye care centers in Tamil Nadu, West Bengal, and Karnataka, is the rapid peripheral creep of the infiltrate. Unlike fungi, which often remain localized before expanding centripetally, Pythium frequently extends circumferentially toward the limbus, threatening early pan-corneal involvement.19 This extension is often observed in patients with antecedent water or soil trauma, such as paddy farmers exposed to muddy fields during monsoons, or in those injured with vegetative material. Such an exposure history, when combined with rapid clinical progression, strongly raises suspicion of Pythium in the Indian setting. Other subtle but useful signs include a plaque-like stromal infiltrate, which appears as a flat, whitish lesion resembling disciform keratitis, and a relatively clean epithelial surface compared to the depth of stromal involvement.20 Endothelial plaque formation may be minimal in early stages, which can mislead clinicians accustomed to fungal patterns. Hypopyon, when present, tends to be sterile and small relative to the aggressiveness of the stromal disease. Importantly, the poor or absent response to natamycin or azole antifungals within 48–72 hours serves as a red flag. Indian ophthalmologists have highlighted that continued progression despite intensive antifungal therapy is a critical differentiator of Pythium keratitis from filamentous fungal infections.21 From an Indian perspective, where microbial keratitis is among the leading causes of corneal blindness, the ability to recognize these features early is crucial. In resource-limited rural settings where laboratory confirmation may be delayed, reliance on these clinical markers can be life-saving for the cornea. Widespread training of ophthalmologists and residents in recognizing tentacular infiltrates, guttering, and peripheral creep has already improved early suspicion rates in endemic regions.22
Laboratory Diagnosis
The laboratory diagnosis of Pythium insidiosum keratitis in India has evolved significantly over the past decade, guided by the need for practical, cost-effective methods that can be adopted in diverse clinical settings. The standard workflow typically begins with direct smear examination, proceeds to culture confirmation, and incorporates advanced tools when available.23 Smear-based microscopy remains the first-line test in most Indian eye hospitals. Corneal scrapings examined with 10% potassium hydroxide (KOH) and calcofluor white reveal characteristic broad, ribbon-like, sparsely septate hyphae. A bright cellulose signal is often noted with calcofluor, while stains designed to highlight chitin, such as lactophenol cotton blue, frequently yield negative or weak results is an important distinction from fungal keratitis.24 Gram’s stain can occasionally show thick-walled hyphae but lacks sensitivity. The diagnostic value of smears in India lies in their rapid turnaround, affordability, and applicability in rural centers. Culture techniques provide definitive identification and have been optimized locally. Unlike filamentous fungi, Pythium demonstrates robust growth on blood agar and chocolate agar, often producing colonies within 24–48 hours.25 In contrast, growth on Sabouraud dextrose agar is weak or absent, which can mislead clinicians who rely solely on fungal culture media. Some reference centers employ zoospore induction methods—using grass leaves or aquatic plant material—to stimulate the production of motile biflagellate zoospores, confirming the organism’s identity.26 Although labour-intensive, this technique has been invaluable in research and teaching settings. Confirmatory methods are increasingly available at tertiary institutions. Polymerase chain reaction (PCR) targeting the internal transcribed spacer (ITS) region provides rapid, highly specific confirmation of Pythium DNA. In surgical cases, histopathology of excised corneal buttons often demonstrates hyphae infiltrating the stroma with accompanying inflammatory response, supporting the diagnosis.27 Periodic acid-Schiff (PAS) and Gomori methenamine silver (GMS) staining may reveal hyphae, although the absence of chitin continues to complicate interpretation. Adjunctive diagnostic tools complement microbiology in challenging cases. In vivo confocal microscopy (IVCM) has gained traction in India as a non-invasive method that can demonstrate broad, non-septate, right-angled filaments within the corneal stroma, raising suspicion before cultures finalize.28 Anterior segment optical coherence tomography (AS-OCT), while not specific, provides valuable insights into the depth and extent of stromal involvement, informing surgical decision-making. These adjuncts are particularly useful in high-volume centers where rapid triage of keratitis is essential. From an Indian perspective, the strength of this stepwise laboratory workflow lies in its adaptability. Rural centers can rely on smears and blood agar cultures for early suspicion, while tertiary institutions incorporate molecular and imaging adjuncts for confirmation.29 Together, these approaches have enabled Indian ophthalmology to lead the global refinement of Pythium keratitis diagnostics, bridging the gap between clinical suspicion and organism-specific therapy. Table 1 depicts the comparative features of Pythium keratitis versus fungal keratitis.
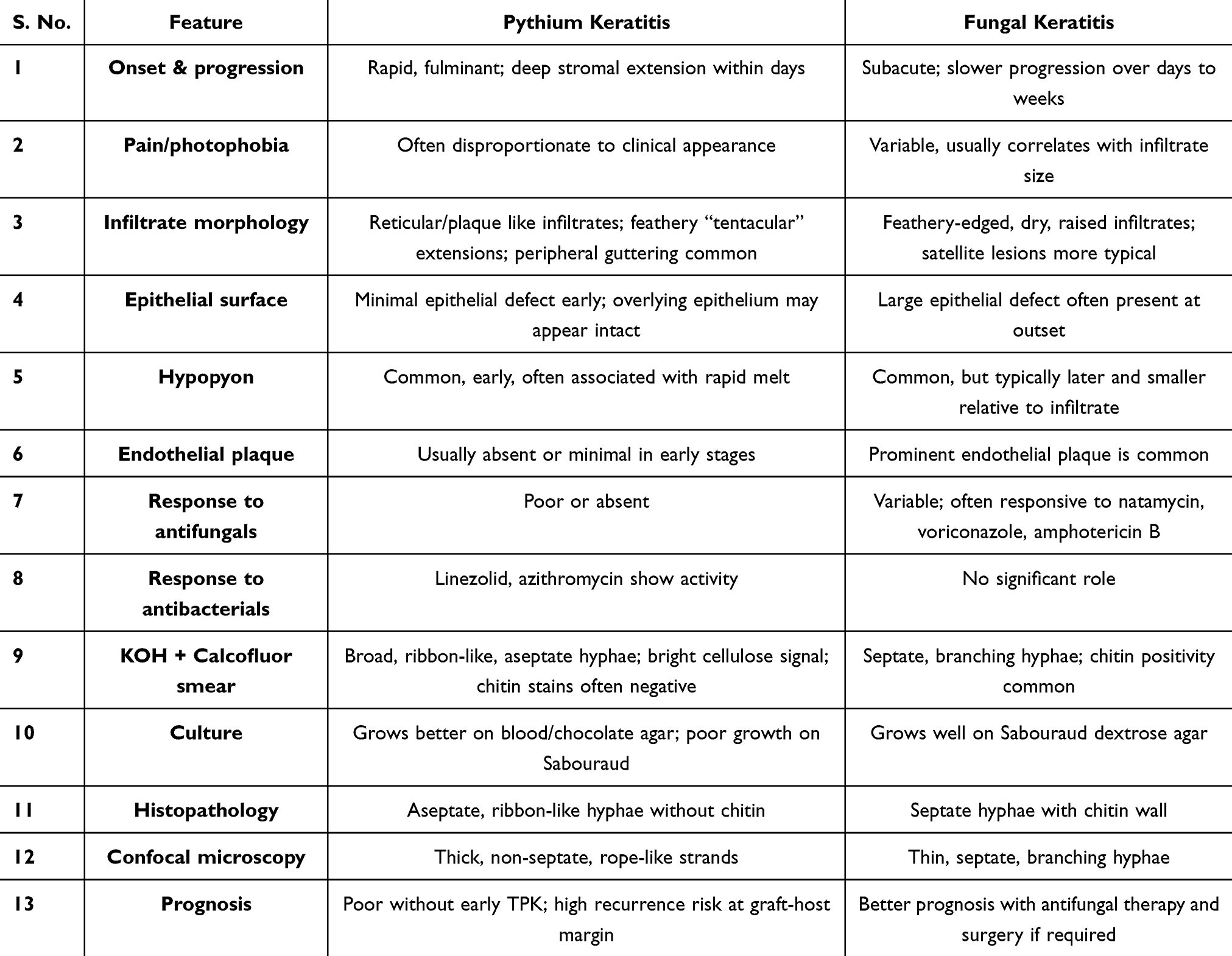 |
Table 1 Depicts the Comparative Features of Pythium Keratitis versus Fungal Keratitis |
Immunopathogenesis—What Indian Cohorts Teach Us
Insights from Indian cohorts have been pivotal in shaping our current understanding of the immunopathogenesis of Pythium keratitis. Unlike classical bacterial or fungal keratitis, where inflammation is often immediate and proportional to microbial burden, Pythium follows a distinctive “stealth then storm” paradigm.30 In the early stages of infection, corneal tissue invasion occurs silently, with little overt inflammation. Clinical observations from tertiary centers in Tamil Nadu, Puducherry, and Odisha consistently describe ulcers that initially appear deceptively indolent despite deep stromal penetration. This clinical impression correlates with immunological data demonstrating low levels of pro-inflammatory cytokines IL-1β and TNF-α during the early phase. The organism achieves this stealth mode through immune evasion mechanisms such as masking β-glucan motifs, which prevents effective activation of Dectin-1 and TLR4 pathways and blunts early innate responses. As infection progresses, however, this quiet phase gives way to an abrupt inflammatory surge.30 Indian studies have documented a late rise in IL-8, a potent neutrophil chemoattractant, coinciding with the onset of severe stromal infiltration, suppuration, and corneal melt. Clinically, this translates to the rapid progression, collagenolysis, and tissue necrosis seen after a short window of apparent stability.31 Histopathological studies from Indian corneal buttons reinforce this, demonstrating massive neutrophil infiltration in later stages, often disproportionate to the viable organism load. Thus, the bulk of corneal destruction in Pythium keratitis results not from direct microbial lysis but from host-mediated damage triggered by delayed immune recognition.32 These findings carry important therapeutic implications. Conventional strategies aimed at simply suppressing inflammation may be counterproductive if applied indiscriminately in early stages. Instead, therapies that unmask the organism early, enhance timely pathogen recognition, and prime innate responses may improve outcomes by reducing the destructive late hyperinflammation.33 This paradigm also underscores the rationale for exploring immunomodulators or adjunctive therapies tailored to the unique kinetics of Pythium pathogenesis. By elucidating this distinct immune trajectory, Indian cohorts have provided critical mechanistic insights that not only explain clinical aggressiveness but also highlight future avenues for host-directed interventions. Figure 3 depicts the immunopathogenesis of Pythium insidiosum keratitis.
 |
Figure 3 Depicts the immunopathogenesis of Pythium insidiosum keratitis. |
Management
Medical Therapy—Evidence Based from Indian Cohorts
The management of Pythium insidiosum keratitis represents one of the most challenging frontiers in Indian corneal practice. Over the last decade, large case series from Indian tertiary centers have demonstrated that conventional antifungal agents are ineffective as monotherapy, primarily due to the oomycete’s cellulose-rich, ergosterol-deficient cell wall.2 This failure of polyenes and azoles has forced a paradigm shift toward repurposed antibacterials and experimental adjuncts. Among antibiotics, linezolid has emerged as the cornerstone. Topical linezolid 0.2–0.4% eye drops, instilled hourly in the acute phase and gradually tapered, consistently demonstrate activity against Pythium isolates in vitro and in vivo.34 Clinical cohorts from Tamil Nadu and West Bengal confirm improved outcomes when linezolid is initiated early, with reduced recurrence and better graft clarity following keratoplasty. Azithromycin 1% eye drops, used alone or in combination, have shown synergistic effects, possibly due to their ability to disrupt protein synthesis and inhibit biofilm formation.9 Some centers have also tried systemic azithromycin as an adjunct, particularly in deep stromal infections, although evidence remains anecdotal. Combination therapy with linezolid plus azithromycin is increasingly adopted in Indian protocols, reflecting both laboratory synergy and clinical benefit. Adjunctive strategies are under active exploration. Cellulose-targeting therapies—such as cellulase and cellulose biosynthesis inhibitors (CBIs) hold promise in disrupting the pathogen’s unique cell wall structure, although these remain largely experimental.20 Tetracyclines (oral doxycycline or minocycline) are sometimes added for their anti-collagenolytic effects, aiming to reduce stromal melt rather than direct antimicrobial action. In parallel, interest is growing in immune-modulatory approaches, including topical toll-like receptor (TLR) agonists, designed to unmask the organism and enhance early host recognition. While still in preclinical stages, these strategies reflect the translational research momentum driven by Indian experience.34 Evidence from Indian cohorts highlights important trends in the medical management of Pythium keratitis. Early initiation of linezolid–azithromycin–based therapy has been associated with improved response rates, yet overall success with medical therapy alone remains modest, with many series reporting progression requiring therapeutic keratoplasty in 30–40% of cases. Adherence can also be challenging, as hourly dosing regimens, limited access to compounded linezolid preparations, and delayed presentation often reduce treatment effectiveness. Major clinical barriers include deep stromal invasion at the time of diagnosis, rapid melt despite therapy, and difficulty achieving adequate drug levels in full-thickness infiltrates. Integrating structured follow-up protocols, improving availability of topical formulations, and adopting point-of-care diagnostics to enable earlier initiation of appropriate therapy may help overcome these limitations and enhance clinical outcomes in high-burden regions.2–5,35 Overall, the Indian approach to medical management is pragmatic and evidence-informed: early suspicion, rapid switch to antibacterials, combination therapy where feasible, and aggressive monitoring for failure or recurrence. Yet, despite these advances, medical therapy alone remains insufficient for many patients, underscoring the continued need for timely surgical intervention as part of a combined strategy. Table 2. Highlights the practical drug regimens used for Pythium keratitis in Indian centers. Table 3. Depicts the reported and practical drug combinations for Mixed Pythium–Fungal Keratitis in Indian centers.
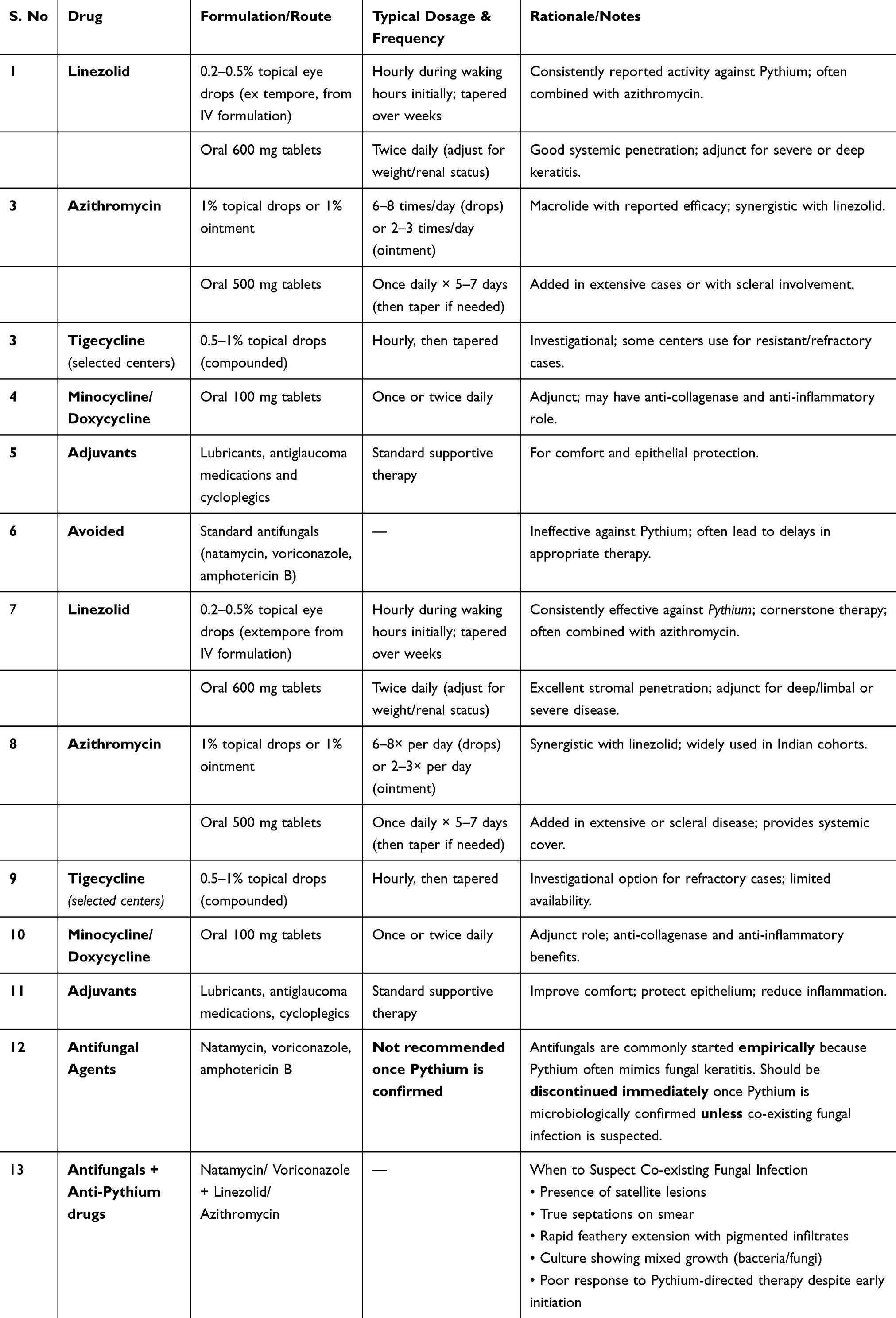 |
Table 2 Highlights the Practical Drug Regimens Used for Pythium Keratitis in Indian Centers |
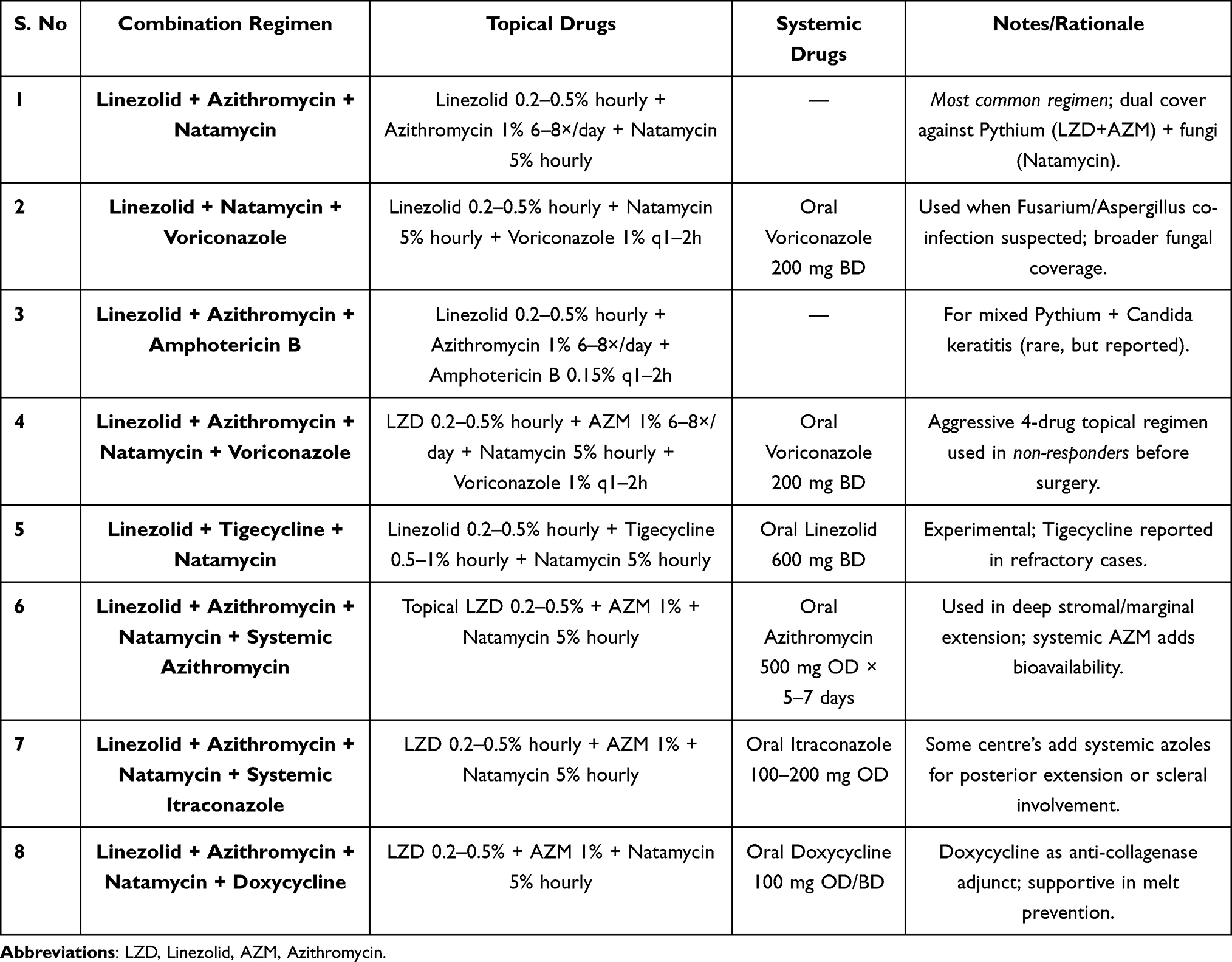 |
Table 3 Depicts the Reported and Practical Drug Combinations for Mixed Pythium–Fungal Keratitis in Indian Centers |
Surgical Therapy
Surgical intervention, particularly therapeutic penetrating keratoplasty (TPK), remains the cornerstone of management in advanced cases of Pythium keratitis. Medical therapy alone is often inadequate once the infection progresses to involve the deep stroma, shows rapid extension, or when there is an impending or established corneal perforation. In such situations, early surgical intervention is critical to limit disease progression and prevent intraocular extension.2 The guiding principle of TPK in Pythium keratitis is generous excision with wide margins of uninvolved corneal tissue, typically extending at least 1–1.5 mm beyond the clinically apparent infiltrate. This aggressive approach helps reduce the risk of residual organism at the graft–host junction, which is a major contributor to recurrence.36 During the procedure, meticulous interface irrigation with appropriate antimicrobial solutions is advocated to minimize residual microbial load. In the postoperative period, targeted antimicrobial therapy must be continued aggressively, and the introduction of corticosteroids should be delayed until there is clear microbiological and clinical evidence of infection control.12 This is in contrast to routine fungal or bacterial keratitis, where topical steroids are often considered earlier to control inflammation. Despite timely and well-executed TPK, the risk of recurrence in Pythium keratitis remains significantly higher than in fungal keratitis, necessitating close postoperative monitoring. Repeat TPK or adjunctive measures may be required in recurrent or non-resolving cases. Thus, while surgical therapy offers the best chance of eradicating infection and preserving globe integrity, outcomes are often guarded, and a multidisciplinary approach combining surgical vigilance with tailored medical therapy remains essential.37 Figure 4 depicts the surgical checklist for managing Pythium insidiosum keratitis.
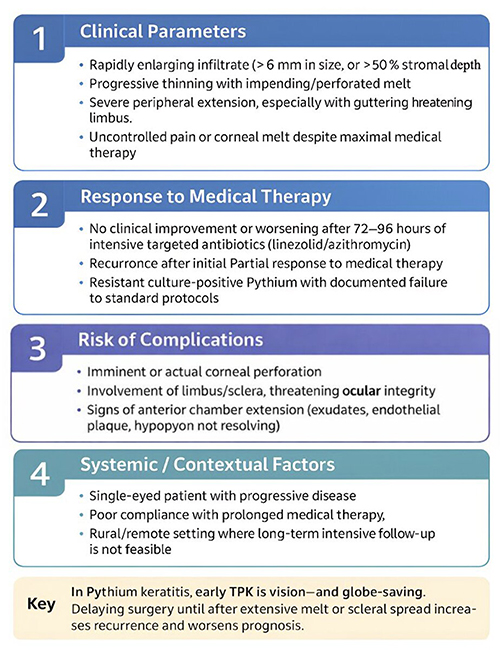 |
Figure 4 Depicts the surgical checklist for managing Pythium insidiosum keratitis. |
Practical Approach for Rapid Diagnosis—An Indian Perspective
In India, where the majority of reported cases of Pythium keratitis have emerged, a pragmatic and stepwise approach is crucial given the rapid course and high morbidity associated with this infection. The first and most important step is a high index of suspicion in any keratitis case with history of exposure to soil or contaminated water, especially when slit-lamp biomicroscopy reveals tentacular infiltrates, peripheral guttering, or a reticular plaque-like appearance.2 Once suspected, patients should undergo urgent microbiological evaluation, with direct smear and culture being prioritized for same-day reporting. Given the characteristic cellulose positivity on calcofluor/KOH mount and rapid blood or chocolate agar growth, early laboratory confirmation can significantly alter outcomes. Confirmation by leaf incarnation is a must as this is the gold standard.9 Pending culture results, empirical initiation of linezolid and/or azithromycin therapy is recommended, as multiple reports from India suggest favourable outcomes compared to conventional antifungals, which are largely ineffective. If the clinical course deteriorates within 24–48 hours, or when deep stromal infiltrates manifest, progressive tentacular extensions, or descemetocele formation are observed, an early therapeutic penetrating keratoplasty (TPK) becomes the cornerstone of management.34 Unlike fungal keratitis, conservative waiting can be disastrous in Pythium, as delayed intervention often results in rapid corneal melt, perforation, or intraocular extension. Therefore, surgical decision-making should be proactive rather than reactive, with wide excision margins (≥1–1.5 mm of clear cornea) considered essential to reduce recurrence. The postoperative phase demands vigilant monitoring for rim recurrence, which can occur in up to one-third of cases despite meticulous TPK. Any suspicion of recurrence at the graft–host junction warrants prompt re-intervention, either with re-TPK or localized excision, to prevent intraocular invasion.35 Adjunctive therapy with targeted antimicrobials should be continued aggressively, and topical corticosteroids should be withheld until infection control is unequivocally established. From an expert perspective, this Indian experience underscores two key lessons: first, that speed and time of diagnosis and intervention directly translates into globe salvage; and second, that surgical aggressiveness must be tempered with vigilant postoperative care, as incomplete clearance and premature immunosuppression remain the Achilles’ heel of Pythium management. The practical pathway adopted in India is early and high index of suspicion, microbiology-driven therapy, and timely surgical intervention which has now become a model for global management of this unique and challenging pathogen.2 Figure 5 depicts the diagnostic algorithm for managing Pythium insidiosum keratitis.
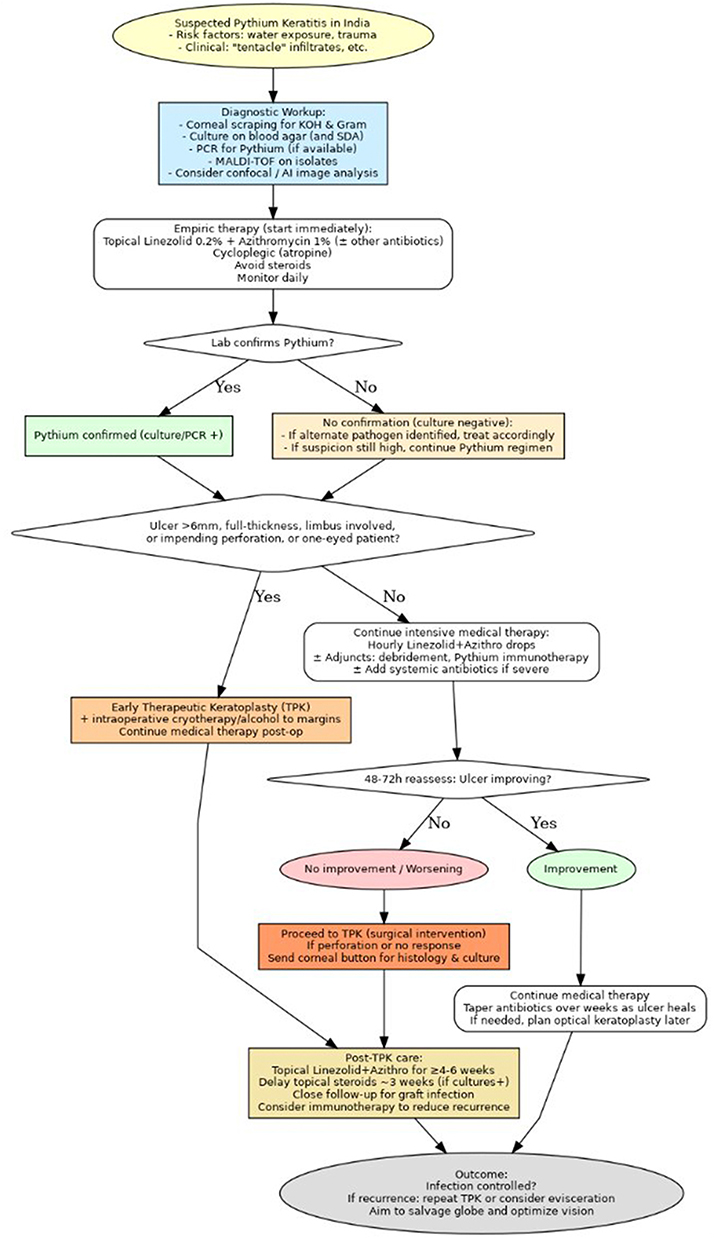 |
Figure 5 Depicts the diagnostic algorithm for managing Pythium insidiosum keratitis. |
Advanced Surgical Interventions in Endemic Countries
In countries such as Thailand, where Pythium keratitis has historically been a well-recognized entity, the surgical philosophy has traditionally been even more radical than in India. While India has shifted toward early therapeutic penetrating keratoplasty (TPK) with organism-specific medical cover, Thai centers have often favoured definitive globe-sacrificing surgeries—including evisceration, enucleation, or even exenteration—as the treatment of choice in severe or non-responsive cases.32 Although rare, such interventions have been reported in Southeast Asian case series, particularly where patients presented late. The rationale behind this aggressive stance is rooted in the historically poor outcomes with medical therapy (conventional antifungals being ineffective) and the high recurrence rates post-keratoplasty reported in earlier series. In fact, several Thai studies from the 1990s and 2000s highlighted that primary enucleation/evisceration yielded higher cure rates than attempted keratoplasty, as attempts at globe preservation often ended in recurrence and delayed definitive surgery.32 Figure 6 depicts stepwise management pathway with decision points for early TPK.
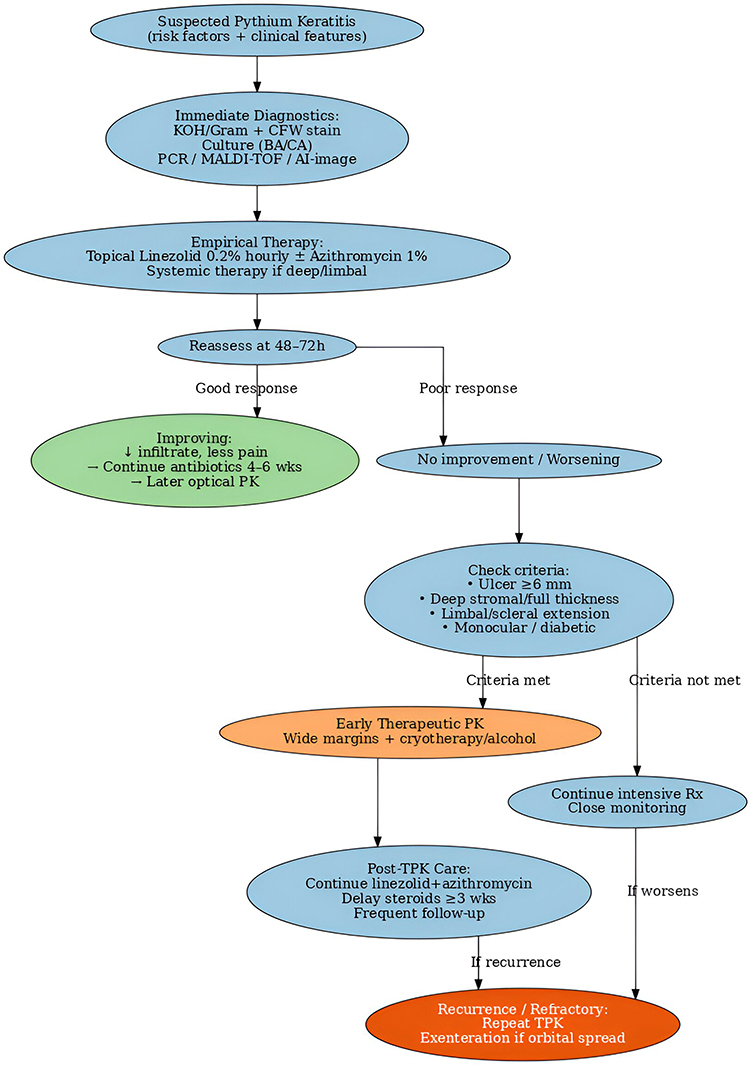 |
Figure 6 Depicts stepwise management pathway with decision points for early therapeutic penetrating keratoplasty. KOH − Potassium hydroxide, CFW − Calcofluor white, PCR – Polymerase chain reaction, MALDI-TOF – Matrix Assisted Laser Desorption Ionization-Time of Flight, AI – Artificial intelligence, ↓ – Reduction, PK – Penetrating keratoplasty, TPK – Therapeutic penetrating keratoplasty, Rx – Treatment. |
Outcomes and Prognosis
The ultimate visual outcomes in Pythium keratitis are dictated less by the sophistication of available therapeutics and more by the rapidity of accurate diagnosis and the timeliness of surgical intervention. Delay of even a few days can shift the prognosis from corneal salvage to irreversible loss of the eye, underscoring the unforgiving natural history of this organism.38 Early suspicion, laboratory confirmation, and proactive surgical therapy with therapeutic penetrating keratoplasty (TPK) can significantly alter the trajectory of the disease. Patients who undergo timely TPK, particularly before perforation or intraocular extension, often retain a useful anatomical globe and may even achieve functional visual rehabilitation with secondary optical procedures.39 However, recurrence remains the Achilles’ heel of surgical therapy. The organism’s propensity to infiltrate subtly beyond the clinically visible margins means that if even minute foci of hyphae are left behind at the graft–host junction, rim recurrence is almost inevitable This recurrence is usually aggressive and can compromise even a well-performed graft within days. As a result, close and vigilant postoperative surveillance is indispensable, with a low threshold for re-intervention.2 Unlike fungal keratitis, where inflammation can sometimes be tempered with topical corticosteroids the early postoperative period, in Pythium keratitis such immunosuppression can be disastrous if introduced prematurely. When compared directly to fungal ulcers, Pythium keratitis demonstrates a much faster rate of tissue destruction, often leading to deep stromal melt or descemetocele within days.9 Yet, paradoxically, the same aggressive course makes the role of decisive early surgery more rewarding by swiftly removing infected tissue and re-establishing structural integrity, the clinician can sometimes salvage both the globe and vision. In centers with established diagnostic and surgical pathways, success rates are steadily improving, and long-term outcomes, though guarded, are far more encouraging than a decade ago.40 From an expert perspective, the prognosis in Pythium keratitis hinges on two pillars: speed and decisiveness. Speed in recognizing and confirming the pathogen, and decisiveness in adopting early, wide, and aggressive TPK rather than persisting with futile medical therapy. Where these principles are applied, the narrative shifts from inevitable blindness to realistic prospects of visual rehabilitation, a transformation that represents one of the most significant advances in managing this newly recognized corneal pathogen.41
Public Health & Systems Perspective
From a public health standpoint, Pythium keratitis poses unique challenges in India, where agricultural exposure, monsoon-related surges, and limited early diagnostic capacity converge to create a high disease burden. The first point of contact for most patients remains district hospitals, secondary-level centers, or teaching institutions, where ophthalmologists and general physicians may be unfamiliar with the distinctive clinical appearance of Pythium.1 Awareness-building among these first-contact providers is therefore critical, enabling earlier suspicion and timely referral to tertiary corneal units before catastrophic progression occurs. Diagnostic strengthening at the grassroots level also has the potential to transform outcomes. Introducing point-of-care microbiological tools, such as rapid 10% KOH plus calcofluor white staining, can empower even modestly equipped laboratories to differentiate Pythium from fungal keratitis within hours.42 Embedding referral triggers directly into electronic medical record (EMR) systems or order sets—for example, flagging cases with reticular or tentacular infiltrates that fail to respond to antifungals—could standardize care pathways and reduce delays in escalation. From a preventive standpoint, the monsoon season represents a predictable period of heightened risk, especially in endemic districts where paddy cultivation and waterlogged fields increase exposure.39 Incorporating seasonal messaging into local health campaigns, eye hospital outreach programs, and agricultural advisories could raise community awareness of early symptoms and the importance of urgent consultation. Likewise, simple protective strategies for farm workers, including the distribution and promotion of affordable protective eyewear, could reduce the incidence of soil- and water-related corneal trauma that often precedes infection.6 Taken together, these measures reflect a shift from viewing Pythium keratitis solely as an ophthalmic problem to approaching it as a systems-level challenge that spans public health, occupational safety, and clinical care. The Indian experience highlights that combating this pathogen requires not only surgical and pharmacological advances but also integration of awareness, diagnostics, and preventive strategies into the health system. This multipronged approach has the potential to significantly reduce the morbidity of what is otherwise an aggressive and sight-threatening condition.2
Research Gaps and Priorities
Despite growing recognition of Pythium keratitis as a distinct clinical entity, substantial gaps remain in diagnostics, therapeutics, and systems-level knowledge, which continue to constrain patient outcomes. One of the most pressing needs is the development of rapid, point-of-care diagnostic tools. Current reliance on conventional microscopy and culture often results in delays, while clinical overlap with fungal keratitis can mislead first-line providers.17 The design of cellulose-targeted fluorescent probes and Pythium-specific PCR kits represents a promising frontier, enabling rapid, accurate, and field-adaptable detection. Such innovations could transform case detection in endemic districts, especially if integrated into cost-effective, portable diagnostic platforms. In terms of treatment, there is a critical gap in drug development. While linezolid and azithromycin have shown relative efficacy, their pharmacokinetics and pharmacodynamics in the corneal microenvironment remain poorly characterized. Rigorous studies on optimized dosing, tissue penetration, and toxicity profiles are urgently needed. Beyond this, novel therapeutic avenues such as cellulose biosynthesis inhibitors offer the potential for pathogen-specific ophthalmic formulations that could revolutionize management, particularly as adjuncts to surgical therapy.20 Another underexplored area is immunotherapy. The unique immune response elicited by Pythium spp. offers an opportunity for standardized antigen preparation and carefully designed clinical trials assessing the safety and efficacy of localized immune-priming adjuncts. If successful, such interventions could reduce recurrence rates and improve graft survival post-TPK. Finally, there is a strong case for establishing a national registry of Pythium keratitis in India, coordinated across tertiary eye centers. A multicenter dataset would enable robust evaluation of surgical timing, graft dimensions, recurrence risk factors, and drug-response protocols, thereby refining clinical guidelines and improving evidence-based care. Such a registry could also provide invaluable insights for global ophthalmology, given India’s unique position at the epicenter of this pathogen’s recognition and management. From an expert standpoint, closing these gaps requires a multi-pronged research strategy that spans laboratory innovation, clinical pharmacology, immunology, and public health infrastructure. Only through coordinated efforts can the shift be made from reactive treatment to proactive control, ultimately redefining the prognosis of Pythium keratitis worldwide.2,9,17 Emerging therapeutic research is increasingly focused on exploiting the unique structural and biological features of Pythium compared with bacterial and fungal pathogens. Its cellulose-rich, chitin-deficient cell wall, absence of ergosterol, and distinct β-glucan masking mechanisms have opened avenues for novel drug targets that differ fundamentally from antifungal or antibacterial approaches. Potential candidates under investigation include cellulose-binding agents, β-glucan–targeting molecules, oomycete-specific enzyme inhibitors, and host-directed immunomodulators that modulate neutrophilic inflammation without compromising pathogen clearance. Highlighting these distinctions may help guide future therapeutic development and encourage exploration of drugs tailored specifically to oomycete biology.
Advances in Diagnostics
Significant breakthroughs in diagnostic technology have reshaped the clinical approach to Pythium keratitis, reducing diagnostic delays that previously spanned days to weeks.
Advanced Point-of-Care Imaging (AS-OCT & IVCM)
Recent enhancements in anterior-segment imaging have greatly improved early recognition of Pythium keratitis. AS-OCT now allows rapid, non-invasive identification of features such as tentacular hyperreflective tracks, granular stromal dots, peripheral guttering, and early endothelial plaques—patterns that help distinguish Pythium from fungal ulcers. In vivo confocal microscopy further supports diagnosis by demonstrating broad, ribbon-like filaments with right-angled branching (8–12 µm), a finding shown to have high sensitivity and specificity. Together, these imaging tools enable early, confident suspicion of Pythium keratitis and help shorten the time to organism-directed therapy.43
Rapid Molecular Diagnostics
Rapid molecular diagnostics have greatly shortened the time needed to confirm Pythium keratitis, reducing the delay from several days to under an hour. PCR assays targeting ITS or 18S rDNA provide high diagnostic accuracy, with sensitivities around 96% and specificities close to 98%. LAMP assays offer simple, color-based detection and have shown excellent early sensitivity, while recombinase polymerase amplification (RPA) delivers ultra-rapid results in roughly 20 minutes. These technologies are especially valuable in secondary eye-care settings where culture facilities are limited, enabling faster initiation of organism-directed therapy.44
Lateral Flow Immunoassays (LFIA)
Prototype 15-minute antigen detection strips have shown >90% accuracy and require no instrumentation, making them ideal for peripheral clinics.45
Emerging Biosensor Technologies
Cutting-edge aptamer-based electrochemical biosensors and smartphone-linked readers can detect Pythium antigens in under 10 minutes. These devices promise high specificity, low cost, and portability—key attributes for field deployment in endemic regions.46
Artificial Intelligence (AI) for Automated Diagnosis
Recent advances in anterior-segment imaging have greatly improved the early recognition of Pythium keratitis. High-resolution AS-OCT now allows rapid, non-invasive visualization of distinctive stromal patterns such as tentacular hyperreflective tracks, granular dot-like infiltrates, peripheral guttering, and early endothelial plaques, all of which strongly favour a diagnosis of Pythium over fungal keratitis. In vivo confocal microscopy complements this by identifying the pathogen’s characteristic broad, ribbon-shaped filaments with right-angled branching, measuring approximately 8–12 µm, features that have demonstrated high sensitivity and specificity in clinical studies. Together, these imaging modalities enhance early diagnostic confidence and facilitate timely initiation of organism-directed therapy, reducing the risk of delays that often worsen clinical outcomes.47
Advances in Therapy
Future Therapeutic Possibilities
Ongoing translational research is steadily expanding the therapeutic horizon for Pythium keratitis, focusing on strategies that go beyond antimicrobial therapy alone. Emerging host-directed immunomodulatory approaches aim to temper the destructive inflammatory cascade while preserving pathogen clearance, thereby reducing stromal melt and improving visual outcomes. Parallel advances in cellulose-targeting diagnostic and therapeutic probes are being explored to exploit the unique cell wall biology of Pythium, enabling more precise organism detection and ultimately facilitating targeted drug delivery. In addition, biosensor-guided treatment algorithms—integrating real-time pathogen detection with point-of-care decision support—are under development to personalize therapy and optimize timing of interventions such as keratoplasty. Together, these innovations hold promise for lowering recurrence rates, improving graft survival, and ultimately reducing the need for emergency therapeutic keratoplasty in severe or refractory disease.43
Conclusion
The Indian experience has been pivotal in reframing Pythium keratitis from a clinical curiosity into a rapidly destructive oomycete infection requiring early recognition, organism-directed therapy, and timely surgical intervention. Anchoring care to India-specific workflows—fast-track KOH and calcofluor microscopy, early use of linezolid and azithromycin, and proactive therapeutic keratoplasty with wide margins—has significantly improved outcomes and now serves as a reproducible model for other regions where Pythium is emerging. Looking ahead, rapid molecular diagnostics and targeted therapeutic approaches hold promise for reducing delays and mitigating the severe inflammatory damage characteristic of this disease. India’s frontline contributions have not only advanced local patient care but also provided a practical global blueprint for managing this increasingly recognized pathogen.
Funding
No external support, either public or private, was received for the conduct of this study.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Gurnani B, Kaur K. Pythium Keratitis. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025. PMID: 34424645.
2. Gurnani B, Christy J, Narayana S, Rajkumar P, Kaur K, Gubert J. Retrospective multifactorial analysis of Pythium keratitis and review of literature. Indian J Ophthalmol. 2021;69(5):1095–1101. doi:10.4103/ijo.IJO_1808_20 PMID: 33913840; PMCID: PMC8186601.
3. Hasika R, Lalitha P, Radhakrishnan N, Rameshkumar G, Prajna NV, Srinivasan M. Pythium keratitis in South India: incidence, clinical profile, management, and treatment recommendation. Indian J Ophthalmol. 2019;67(1):42–47. doi:10.4103/ijo.IJO_445_18 PMID: 30574890; PMCID: PMC6324135.
4. Sane SS, Madduri B, Mohan N, Mittal R, Raghava JV, Fernandes M. Improved Outcome of Pythium Keratitis With a Combined Triple Drug Regimen of Linezolid and Azithromycin. Cornea. 2021;40(7):888–893. doi:10.1097/ICO.0000000000002503 PMID: 32947406.
5. Vishwakarma P, Mohanty A, Kaur A, et al. Pythium keratitis: clinical profile, laboratory diagnosis, treatment, and histopathology features post-treatment at a tertiary eye care center in Eastern India. Indian J Ophthalmol. 2021;69(6):1544–1552. doi:10.4103/ijo.IJO_2356_20 PMID: 34011738; PMCID: PMC8302330.
6. Khode D, Hepat A, Mudey A, Joshi A. Health-Related Challenges and Programs Among Agriculture Workers: a Narrative Review. Cureus. 2024;16(3):e57222. doi:10.7759/cureus.57222 PMID: 38686223; PMCID: PMC11056488.
7. Kyriakaki ED, Symvoulakis EK, Chlouverakis G, Detorakis ET. Causes, occupational risk and socio-economic determinants of eye injuries: a literature review. Med Pharm Rep. 2021;94(2):131–144. doi:10.15386/mpr-1761 Epub 2021 Apr 29. PMID: 34013184; PMCID: PMC8118212.
8. Thanathanee O, Enkvetchakul O, Rangsin R, Waraasawapati S, Samerpitak K, Suwan-apichon O. Outbreak of Pythium keratitis during rainy season: a case series. Cornea. 2013;32(2):199–204. doi:10.1097/ICO.0b013e3182535841 PMID: 22902492.
9. Gurnani B, Kaur K, Agarwal S, et al. Pythium insidiosum Keratitis: past, Present, and Future. Ophthalmol Ther. 2022;11(5):1629–1653. doi:10.1007/s40123-022-00542-7 Epub 2022 Jul 5. PMID: 35788551; PMCID: PMC9255487.
10. Li M, Zhu D, Diao Q, et al. Clinical Features, Microbiological Characteristics, and Drug Sensitivity Analysis of Rare Human Spinal Pythiosis Strain. J Fungi. 2024;10(12):812. doi:10.3390/jof10120812 PMID: 39728308; PMCID: PMC11676036.
11. Li S, Wang Y, Zhou J, Wang J, Zhang M, Chen H. Structural Characterization, Cytotoxicity, and the Antifungal Mechanism of a Novel Peptide Extracted from Garlic (Allium sativa L.). Molecules. 2023;28(7):3098. doi:10.3390/molecules28073098 PMID: 37049861; PMCID: PMC10095746.
12. Hou H, Wang Y, Tian L, Wang F, Sun Z. Pythium insidiosum keratitis reported in China, raising the alertness to this fungus-like infection: a case series. J Med Case Rep. 2021;15(1):619. doi:10.1186/s13256-021-03189-3 PMID: 34915928; PMCID: PMC8680372.
13. Torricelli AA, Wu J, Singh V, Wilson SE. The corneal fibrosis response to epithelial-stromal injury. Exp Eye Res. 2016;142:110–118. doi:10.1016/j.exer.2014.09.012 PMID: 26675407; PMCID: PMC4683352.
14. Chatterjee S, Agrawal D, Gomase SN. Clinical differentiation of Pythium keratitis from fungal keratitis and development of a scoring system. Indian J Ophthalmol. 2022;70(10):3515–3521. doi:10.4103/ijo.IJO_870_22 PMID: 36190038; PMCID: PMC9789832.
15. Cronkite DA, Strutt TM. The Regulation of Inflammation by Innate and Adaptive Lymphocytes. J Immunol Res. 2018;2018:1467538. doi:10.1155/2018/1467538 PMID: 29992170; PMCID: PMC6016164.
16. Gurnani B, Kaur K. Understanding barriers, recommended solutions, and future prospects for the diagnosis and management of Pythium insidiosum keratitis. Indian J Ophthalmol. 2023;71(12):3584–3586. doi:10.4103/IJO.IJO_1041_23 Epub 2023 Nov 20. PMID: 37991287; PMCID: PMC10788758.
17. Cao B, Gonugunta VT, Radhakrishnan N, et al. Outcomes of Pythium keratitis: a meta-analysis of individual patient data. Curr Ophthalmol Rep. 2022;10(4):198–208. doi:10.1007/s40135-022-00302-7 Epub 2022 Nov 10. PMID: 37250102; PMCID: PMC10211475.
18. Gurnani B, Kaur K. Leap forward in clinical and photographic diagnosis of Pythium insidiosum keratitis. Indian J Ophthalmol. 2023;71(9):3263–3264. doi:10.4103/IJO.IJO_355_23 PMID: 37602622; PMCID: PMC10565910.
19. Gurnani B, Kaur K, Tandon A. Letter Regarding: randomized Double-Masked Placebo-Controlled Trial for the Management of Pythium Keratitis: combination of Antibiotics Versus Monotherapy. Cornea. 2023;42(12):e22–e23. doi:10.1097/ICO.0000000000003350 Epub 2023 Jul 18. PMID: 37487172.
20. Gurnani B, Natarajan R, Mohan M, Kaur K. Breaking-Down Barriers: proposal of Using Cellulose Biosynthesis Inhibitors and Cellulase Enzyme as a Novel Treatment Modality for Vision Threatening Pythium Insidiosum Keratitis. Clin Ophthalmol. 2024;18:765–776. doi:10.2147/OPTH.S450665 PMID: 38495678; PMCID: PMC10941664.
21. Gurnani B, Kaur K. Predicting Prognosis Based on Regional Prevalence, Ulcer Morphology and Treatment Strategy in Vision-Threatening Pythium insidiosum Keratitis. Clin Ophthalmol. 2023;17:1307–1314. doi:10.2147/OPTH.S412274 PMID: 37181081; PMCID: PMC10167989.
22. Hoffman J, Yadav R, Ebong A, Arunga S, Leck A. Managing microbial keratitis in resource-limited settings. Community Eye Health. 2024;37(124):11–14. Epub 2025 Jan 31. PMID: 40115630; PMCID: PMC11921248.
23. Acharya M, Farooqui JH, Gaba T, Gandhi A, Mathur U. Delhi Infectious Keratitis Study: update on Clinico-Microbiological Profile and Outcomes of Infectious Keratitis. J Curr Ophthalmol. 2020;32(3):249–255. doi:10.4103/JOCO.JOCO_113_20 PMID: 32775799; PMCID: PMC7382511.
24. Assaf JF, Yazbeck H, Venkatesh PN, et al. Automated Detection of Filamentous Fungal Keratitis on Whole Slide Images of Potassium Hydroxide Smears with Multiple Instance Learning. Ophthalmol Sci. 2024;5(2):100653. doi:10.1016/j.xops.2024.100653 PMID: 39811263; PMCID: PMC11731208.
25. Gurnani B, Kaur K. Comment on: sensitivity and specificity of potassium hydroxide and calcofluor white stain to differentiate between fungal and Pythium filaments in corneal scrapings from patients of Pythium keratitis. Indian J Ophthalmol. 2022;70(6):2204. doi:10.4103/ijo.IJO_345_22 PMID: 35648022; PMCID: PMC9359274.
26. Das S, Sharma S, Kar S, Sahu SK, Samal B, Mallick A. Is inclusion of Sabouraud dextrose agar essential for the laboratory diagnosis of fungal keratitis? Indian J Ophthalmol. 2010;58(4):281–286. doi:10.4103/0301-4738.64122 PMID: 20534916; PMCID: PMC2907027.
27. Kumar M, Shukla PK. Use of PCR targeting of internal transcribed spacer regions and single-stranded conformation polymorphism analysis of sequence variation in different regions of rrna genes in fungi for rapid diagnosis of mycotic keratitis. J Clin Microbiol. 2005;43(2):662–668. doi:10.1128/JCM.43.2.662-668.2005 PMID: 15695661; PMCID: PMC548091.
28. Infectious Disease Clinical Research Program Trauma Infectious Disease Outcomes Study Group. Heaton SM, Weintrob AC, Downing K, et al. Histopathological techniques for the diagnosis of combat-related invasive fungal wound infections. BMC Clin Pathol. 2016;16:11. doi:10.1186/s12907-016-0033-9 PMID: 27398067; PMCID: PMC4937573
29. Siddiqui Y, Yin J. Anterior Segment Applications of Optical Coherence Tomography Angiography. Semin Ophthalmol. 2019;34(4):264–269. doi:10.1080/08820538.2019.1620805 Epub 2019 Jun 12. PMID: 31188047.
30. Ahirwar LK, Sharma S. Elevated Levels of Interleukins, Leukocyte Protein and Cathelicidin Antimicrobial Peptide are Strongly Associated with Early to Mid-Stage of Pythium insidiosum Infection in Rabbit Corneas. Curr Eye Res. 2022;47(5):677–687. doi:10.1080/02713683.2021.2023192 Epub 2022 Mar 22. PMID: 35179411.
31. Qazi BS, Tang K, Qazi A. Recent advances in underlying pathologies provide insight into interleukin-8 expression-mediated inflammation and angiogenesis. Int J Inflam. 2011;2011:908468. doi:10.4061/2011/908468 Epub 2011 Dec 22. PMID: 22235381; PMCID: PMC3253461.
32. Puangsricharern V, Chotikkakamthorn P, Tulvatana W, et al. Clinical Characteristics, Histopathology, and Treatment Outcomes of Pythium Keratitis: a Retrospective Cohort Study. Clin Ophthalmol. 2021;15:1691–1701. doi:10.2147/OPTH.S303721 PMID: 33935486; PMCID: PMC8080432
33. Chen L, Deng H, Cui H, et al. Inflammatory responses and inflammation-associated diseases in organs. Oncotarget. 2017;9(6):7204–7218. doi:10.18632/oncotarget.23208 PMID: 29467962; PMCID: PMC5805548.
34. Gurnani B, Kaur K. Anti-infective therapies for Pythium insidiosum keratitis. Expert Rev Anti Infect Ther. 2024;22(10):805–817. doi:10.1080/14787210.2024.2403146 Epub 2024 Sep 13. PMID: 39268901.
35. Agarwal S, Iyer G, Srinivasan B, et al. Clinical profile, risk factors and outcome of medical, surgical and adjunct interventions in patients with Pythium insidiosum keratitis. Br J Ophthalmol. 2019;103(3):296–300. doi:10.1136/bjophthalmol-2017-311804 Epub 2018 Sep 11. PMID: 30206158.
36. Gurnani B, Kaur K. Therapeutic Keratoplasty 2023. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025. PMID: 37276297.
37. Nonpassopon M, Jongkhajornpong P, Aroonroch R, Koovisitsopit A, Lekhanont K. Predisposing Factors, Clinical Presentations, and Outcomes of Contact Lens-Related Pythium Keratitis. Cornea. 2021;40(11):1413–1419. doi:10.1097/ICO.0000000000002651 PMID: 33470674.
38. Acharya M, Singh A, Nidhi V, Tiwari A, Chaudhari I. Outcomes of keratoplasty in a cohort of Pythium insidiosum keratitis cases at a tertiary eye care center in India. Indian J Ophthalmol. 2024;72(8):1124–1129. doi:10.4103/IJO.IJO_3108_23 Epub 2024 Jul 29. PMID: 39078955; PMCID: PMC11451789.
39. Bacorn C, Luu KY, Li JY. Fungal Keratitis: diagnostic Characteristics of the Potassium Hydroxide Preparation With Calcofluor White in Northern California. Cornea. 2022;41(3):347–352. doi:10.1097/ICO.0000000000002907 PMID: 34743097.
40. Liu HY, Hopping GC, Vaidyanathan U, Ronquillo YC, Hoopes PC, Moshirfar M. Polymerase Chain Reaction and Its Application in the Diagnosis of Infectious Keratitis. Med Hypothesis Discov Innov Ophthalmol. 2019;8(3):152–155. PMID: 31598517; PMCID: PMC6778471.
41. Gurnani B, Kaur K, Venugopal A, et al. Pythium insidiosum keratitis - A review. Indian J Ophthalmol. 2022;70(4):1107–1120. doi:10.4103/ijo.IJO_1534_21 PMID: 35325996; PMCID: PMC9240499.
42. Krysik K, Wroblewska-Czajka E, Lyssek-Boron A, Wylegala EA, Dobrowolski D. Total Penetrating Keratoplasty: indications, Therapeutic Approach, and Long-Term Follow-Up. J Ophthalmol. 2018;2018:9580292. doi:10.1155/2018/9580292 PMID: 29850220; PMCID: PMC5933013.
43. Gurnani B, Kaur K. Advancing diagnostics in Pythium insidiosum keratitis: the emerging role of point-of-care imaging and biosensor-based detection devices. Expert Rev Med Devices. 2025;2:1–6. doi:10.1080/17434440.2025.2582616 Epub ahead of print. PMID: 41147335.
44. Ting DSJ, Gopal BP, Deshmukh R, Seitzman GD, Said DG, Dua HS. Diagnostic armamentarium of infectious keratitis: a comprehensive review. Ocul Surf. 2022;23:27–39. doi:10.1016/j.jtos.2021.11.003 Epub 2021 Nov 13. PMID: 34781020; PMCID: PMC8810150.
45. Di Nardo F, Chiarello M, Cavalera S, Baggiani C, Anfossi L. Ten Years of Lateral Flow Immunoassay Technique Applications: trends, Challenges and Future Perspectives. Sensors. 2021;21(15):5185. doi:10.3390/s21155185 PMID: 34372422; PMCID: PMC8348896.
46. Liu CW, Tsutsui H. Sample-to-answer sensing technologies for nucleic acid preparation and detection in the field. SLAS Technol. 2023;28(5):302–323. doi:10.1016/j.slast.2023.06.002 Epub 2023 Jun 9. PMID: 37302751.
47. Zhang Z, Wang Y, Zhang H, et al. Artificial intelligence-assisted diagnosis of ocular surface diseases. Front Cell Dev Biol. 2023;11:1133680. doi:10.3389/fcell.2023.1133680 PMID: 36875760; PMCID: PMC9981656.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.