Back to Journals » Drug Design, Development and Therapy » Volume 19
Remifentanil-Propofol versus Propofol Alone in Patients with Severe Traumatic Brain Injury: A Retrospective Cohort Study on Anesthesia Outcomes
Authors Zhu J, Wei H, Jiang M, Li T, Wu R, Chen H
Received 12 June 2025
Accepted for publication 12 November 2025
Published 27 November 2025 Volume 2025:19 Pages 10561—10569
DOI https://doi.org/10.2147/DDDT.S546712
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Jianbin Zhu, Haixiang Wei, Minying Jiang, Ting Li, Ruizhu Wu, Hualiang Chen
Department of Anesthesiology, The First Hospital of Nanping City, Nanping, Fujian, 353000, People’s Republic of China
Correspondence: Hualiang Chen, Email [email protected]
Objective: To compare the effects of remifentanil-propofol versus propofol alone on anesthesia outcomes in patients undergoing surgery for severe traumatic brain injury (TBI).
Methods: In this single-center, retrospective cohort study, we analyzed the data of 113 consecutive severe TBI (GCS < 9) patients who underwent emergency neurosurgery. Patients were allocated into two groups based on the anesthesia maintenance regimen: the control group (n=56) received a continuous infusion of propofol alone, while the observation group (n=57) received a combination of remifentanil and propofol. The groups were well-matched at baseline. We compared anesthesia recovery times, hemodynamic parameters (SpO2, MAP, HR) at various time points, postoperative pain (VAS) and agitation (RSAS) scores, levels of inflammatory (TNF-α, IL-6) and neurological damage (S-100β, NSE) biomarkers, and 3-month neurological outcomes using the Glasgow Outcome Scale (GOS).
Results: Compared to the control group, the observation group demonstrated significantly shorter extubation time (13.54 ± 3.23 vs 24.79 ± 5.71 min, P < 0.001) and awakening time (8.72 ± 2.43 vs 17.21 ± 3.96 min, P < 0.001). The remifentanil-propofol regimen was associated with superior intraoperative hemodynamic stability for MAP and HR (Group and Interaction effects, P < 0.05). At 24 hours postoperatively, the observation group also exhibited lower VAS and RSAS scores (both P < 0.05), as well as reduced elevations in TNF-α, IL-6, S-100β, and NSE levels (all P < 0.05). Critically, a significantly higher proportion of patients in the observation group achieved a “Good Recovery” on the GOS at 3 months (54.39% vs 25.00%, P = 0.001).
Conclusion: For severe TBI surgery, remifentanil-propofol is associated with faster emergence, better hemodynamic control, reduced pain/agitation, attenuated neuro-inflammation, and improved long-term recovery versus propofol alone, suggesting significant clinical benefits. Prospective studies are warranted for confirmation.
Keywords: remifentanil, propofol, traumatic brain injury, anesthesia, clinical effects
A Letter to the Editor has been published for this article.
Introduction
Traumatic Brain Injury (TBI) is a common and serious clinical condition, causing significant health and socioeconomic burden worldwide.1 With the continuous progress of social development and industrialization, the incidence of TBI is gradually increasing, making it one of the important global public health issues.2 The treatment and rehabilitation of TBI have always been of great concern, with surgical intervention being one of the key steps to improve patient prognosis.3 In the surgical treatment of TBI patients, the choice of anesthesia is crucial for the smooth progress of the surgery and the impact on postoperative recovery.4 Propofol is a widely used intravenous anesthetic in clinical practice, characterized by rapid and smooth induction and recovery, and is widely used in various surgeries.5 However, the use of propofol anesthesia alone in TBI patients may have limitations, such as inadequate postoperative pain control and unstable intraoperative hemodynamics, affecting postoperative recovery.
Remifentanil, as a highly efficient short-acting μ-opioid receptor agonist, has rapid and potent analgesic effects and is widely used for adjunctive analgesia and sedation in anesthesia.6 Recent studies7,8 have shown that the combined use of remifentanil with propofol in surgical anesthesia is superior to using propofol alone. However, its clinical effects in TBI patient anesthesia and its impact on postoperative recovery have not been sufficiently studied and confirmed. Therefore, this study aims to retrospectively analyze the clinical data of TBI patients admitted to our hospital in the past two years, compare the clinical effects of remifentanil combined with propofol versus propofol alone in TBI patient anesthesia, and explore their effects on patient anesthesia recovery, intraoperative hemodynamic stability, postoperative pain, agitation control, inflammatory response, neurological injury, and prognosis recovery.9,10 The goal is to provide a more scientific and effective anesthesia management strategy for the surgical treatment of TBI patients.
Data and Methods
Study Design and Patient Selection
This single-center, retrospective cohort study was approved by the Medical Ethics Committee of The First Hospital of Nanping City (Approval No.: NPFH2021-ETH-032). The requirement for informed consent was waived due to the retrospective nature of the study, patient data will not be shared with third parties. Patient data confidentiality was maintained. We reviewed the clinical data of 113 consecutive patients with severe traumatic brain injury (TBI) who underwent emergency neurosurgery at our hospital between January 2022 and January 2024.
All procedures performed in this study involving human participants were conducted in accordance with the ethical standards of the institutional and/or national research committee and with the principles of the Declaration of Helsinki (as revised in 2013).
Inclusion and Exclusion Criteria
Inclusion Criteria: ① Patients aged ≥ 18 years with a clinical and radiological (CT scan) diagnosis of severe TBI (Glasgow Coma Scale [GCS] score < 9) upon emergency department admission; ② Time from injury to surgery < 12 hours; ③ American Society of Anesthesiologists (ASA) physical status II-IV; ④ Patients who received general anesthesia with either propofol alone or a remifentanil-propofol combination as per the study protocol; ⑤ Availability of complete clinical data for analysis.
Exclusion Criteria: ① Pre-existing severe organ dysfunction (eg, heart failure NYHA Class III–IV, severe hepatic or renal insufficiency); ② History of previous cranial neurosurgery or intracranial infection; ③ Coexisting immune, neurological, or hematological disorders that could confound outcome assessment; ④ Known allergy or contraindication to any drug used in the study protocol; ⑤ Pregnant or lactating women.
Based on the anesthesia maintenance regimen, patients were allocated into two groups: the Control group (n=56) received propofol infusion alone, and the Observation group (n=57) received a remifentanil-propofol combination.
Anesthesia Management
All patients were managed according to a standardized institutional protocol for severe TBI. Upon arrival in the operating room, standard monitoring was established, including electrocardiogram (ECG), non-invasive blood pressure (NIBP), pulse oximetry (SpO2), and capnography (PetCO2). An arterial catheter was placed in the radial artery for continuous blood pressure monitoring. Depth of anesthesia was monitored using the Bispectral Index (BIS, Covidien, USA), with a target range of 40–60.
Anesthesia Induction: After preoxygenation, anesthesia was induced intravenously with midazolam (0.03–0.05 mg/kg), fentanyl (2–4 µg/kg), propofol (1.5–2.5 mg/kg), and rocuronium (0.6 mg/kg) to facilitate orotracheal intubation.
Anesthesia Maintenance: Following intubation, mechanical ventilation was initiated to maintain PetCO2 at 35–40 mmHg.
Control Group: Anesthesia was maintained with a continuous intravenous infusion of propofol at 4–6 mg·kg−1·h−1.
Observation Group: Anesthesia was maintained with a continuous infusion of propofol at 4–6 mg·kg−1·h−1 and remifentanil at 0.10–0.25 µg·kg−1·min−1.
In both groups, the infusion rates of propofol and remifentanil were titrated in real-time to maintain hemodynamic stability (MAP > 65 mmHg and within 20% of baseline) and the target BIS value. Supplemental doses of rocuronium were administered as needed to maintain neuromuscular blockade.
Hemodynamic Management: Intraoperative hypotension (MAP < 65 mmHg or a decrease > 20% from baseline) was primarily managed with fluid boluses (crystalloids) and, if refractory, with intravenous boluses of norepinephrine (4–8 µg). Bradycardia (HR < 50 beats/min) was treated with atropine (0.5 mg IV).
Postoperative Management: At the end of surgery, the decision to extubate was made by the attending anesthesiologist based on standard criteria: hemodynamic stability, adequate spontaneous ventilation, core temperature > 36°C, and return of protective airway reflexes. Patients who did not meet extubation criteria were transferred to the neurosurgical ICU for continued sedation and mechanical ventilation. For extubated patients, postoperative analgesia was provided with intravenous dezocine (0.1 mg/kg) upon emergence.
Observation Indicators
- Anesthesia indicators: Anesthesia maintenance time, time to extubation, and awakening time (time from cessation of anesthetics to eye opening on command).
- Hemodynamic indicators: At pre-operation (T0), 30 minutes after anesthesia induction (T1), immediately after surgery (T3), and 24 hours after surgery (T3), patient’s levels of oxygen saturation (SpO2), mean arterial pressure (MAP), and heart rate (HR) were measured using electrocardiographic monitoring.
- Pain and agitation: At 1 hour and 24 hours after surgery, the Visual Analog Scale (VAS)11 was used to assess pain, with scores ranging from 0 to 10, and the Ricker Sedation-Agitation Scale (RSAS)12 was used to assess agitation, with scores ranging from 1 to 7.
- Inflammation and neurologic factor indicators: Before surgery and 24 hours after surgery, 5 mL of fasting elbow venous blood was collected from patients, and the supernatant was obtained by routine centrifugation. Enzyme-linked immunosorbent assay was used to measure the levels of tumor necrosis factor-alpha (TNF-α), interleukin-6 (IL-6), S-100β, and neuron-specific enolase (NSE).
- Prognosis and recovery: Patients were followed up at 3 months after surgery, and the Glasgow Outcome Scale (GCS)13 was used to evaluate prognosis. Scores ranged from 1 to 5: 1 = death; 2 = vegetative state with minimal responsiveness; 3 = severe disability requiring assistance for daily living; 4 = moderate disability with independence in daily living; 5 = good recovery with ability to live normally.
Statistical Analysis
GraphPad Prism 8 was used for graphing, and SPSS 20.0 was used for data analysis. Descriptive statistics for continuous data were presented as ( ), and independent sample t-tests, paired t-tests, and repeated measures analysis of variance were used. Descriptive statistics for categorical data were presented as n (%), and the chi-square test was used for analysis. A P-value < 0.05 indicated statistical significance.
), and independent sample t-tests, paired t-tests, and repeated measures analysis of variance were used. Descriptive statistics for categorical data were presented as n (%), and the chi-square test was used for analysis. A P-value < 0.05 indicated statistical significance.
Results
A total of 113 patients were included in the final analysis, comprising 56 allocated to the control group (propofol alone) and 57 to the observation group (remifentanil-propofol). The comparison of baseline demographic and clinical characteristics between the two groups is summarized in Table 1. No statistically significant differences were observed in any of the recorded baseline variables (all P > 0.05), indicating that the two groups were well-matched and comparable.
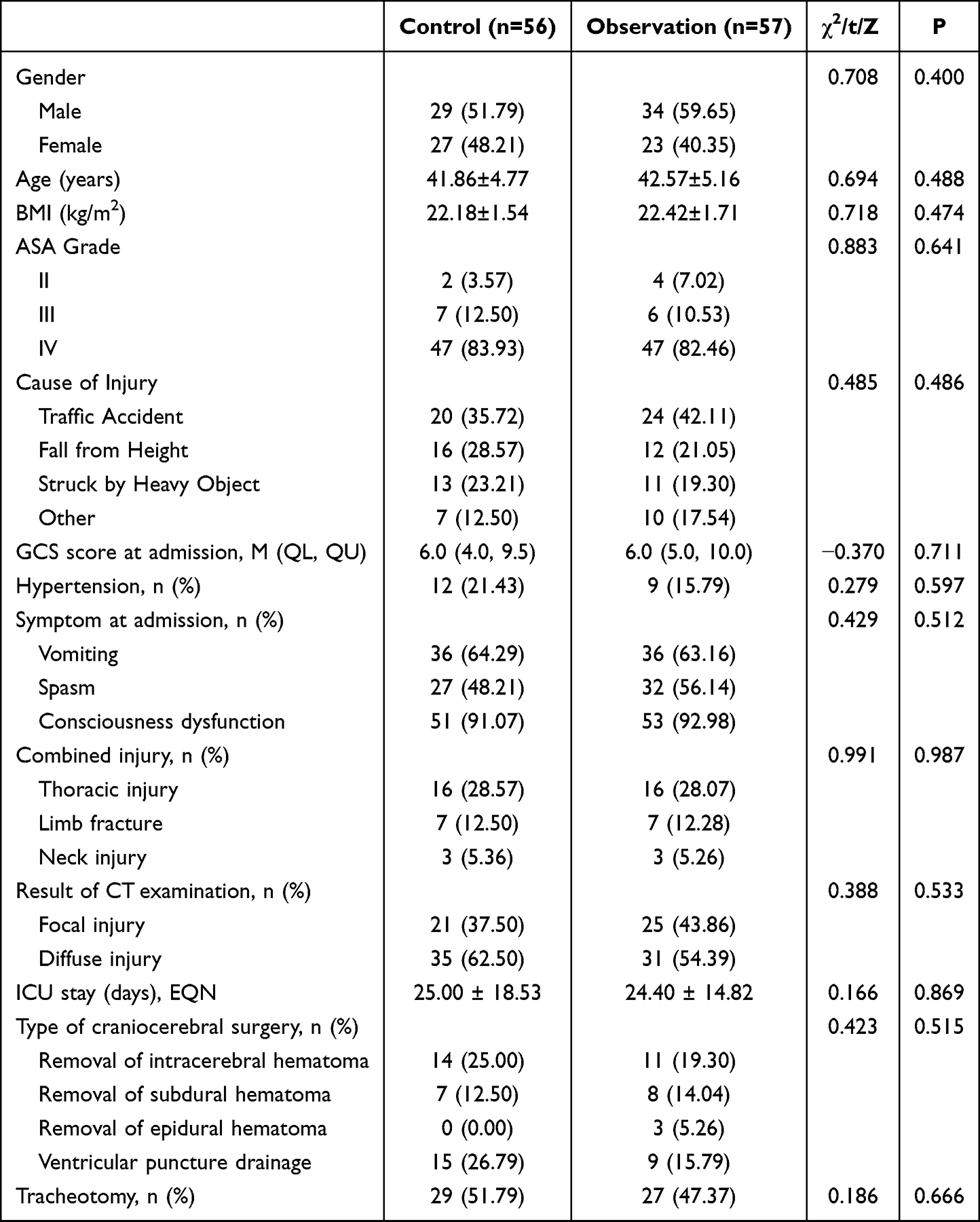 |
Table 1 Comparison of Baseline Data |
Comparison of Anesthesia Indicators
The comparison of anesthesia maintenance time between the two groups was not statistically significant (P > 0.05). The extubation time and awakening time in the observation group were significantly shorter than those in the control group (P < 0.05), as shown in Table 2.
 |

Comparison of Hemodynamic Indicator Levels
As shown in Figure 1, there were statistically significant differences in SpO2, MAP, and HR between the two groups at different time points, as well as significant interaction effects between time and grouping (SpO2: FGroup=6.387, FTime=308.129, FInteraction=25.974, P < 0.05; MAP: FGroup=24.439, FTime=434.852, FInteraction=36.975, P < 0.05; HR: FGroup=9.064, FTime=348.757, FInteraction=16.918, P < 0.05).
 |
Figure 1 Comparison of Hemodynamic Indicator Levels ( Note: *P < 0.05 compared to T0; #P < 0.05 between groups. |

Comparison of Pain and Agitation
As depicted in Figure 2, the VAS scores and RSAS scores of both groups increased at 24 hours postoperatively compared to 1 hour postoperatively, with the observation group showing a smaller change in magnitude (P < 0.05).
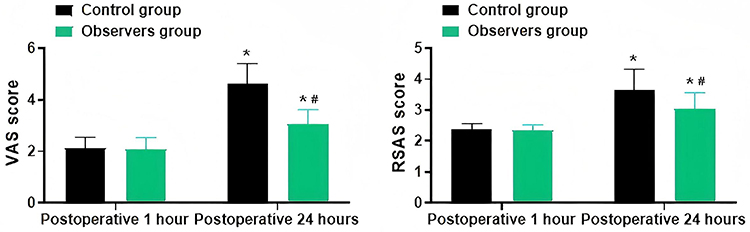 |
Figure 2 Comparison of Pain and Agitation ( Note: *P < 0.05 compared to 1 hour postoperatively; #P < 0.05 between groups. |

Comparison of Inflammatory and Neurological Factor Levels
As illustrated in Figure 3, the levels of TNF-α, IL-6, S-100β, and NSE in both groups increased at 24 hours postoperatively compared to preoperative levels, with the observation group showing a smaller change in magnitude (P < 0.05).
 |
Figure 3 Comparison of Inflammatory and Neurological Factor Levels ( Note: *P < 0.05 compared to 1 hour postoperatively; #P < 0.05 between groups. |

Comparison of Prognosis and Recovery
There were no deaths in either group. The proportion of good prognosis and recovery was higher in the observation group compared to the control group (P < 0.05), as shown in Table 3.
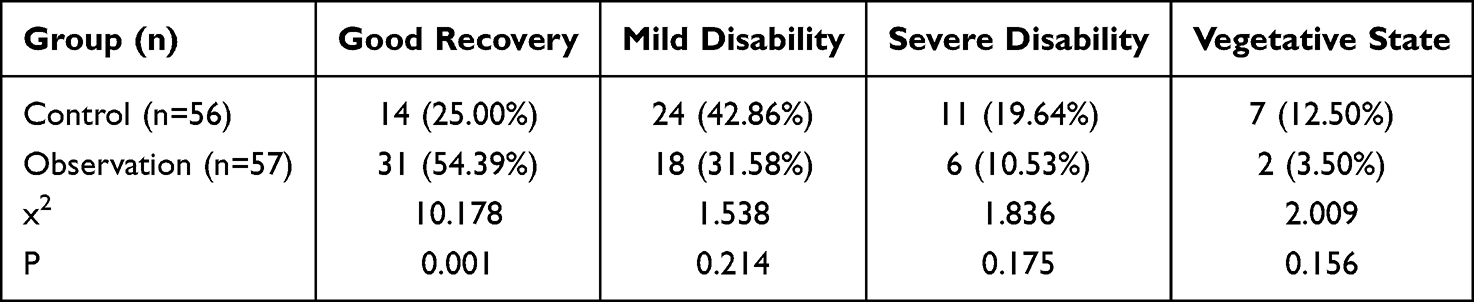 |
Table 3 Comparison of Prognosis and Recovery [n(%)] |
Discussion
Traumatic Brain Injury (TBI) is a complex and severe neurological condition often caused by external forces acting on the head, leading to significant disruption in brain structure and function.14 Data shows that TBI results in millions of people losing their quality of life due to disability or death each year, significantly impacting the quality of life of patients and their families, as well as their social functioning.15 Early diagnosis and treatment are crucial for TBI patients. While significant progress has been made in emergency care and surgical treatment, the postoperative recovery of patients remains unsatisfactory. Postoperative recovery depends not only on the effectiveness of surgical treatment but also on the management of anesthesia during and after surgery.16 Therefore, selecting appropriate anesthetic drugs and effective anesthesia management strategies is crucial for the surgical treatment and postoperative recovery of TBI patients. Propofol, as a commonly used anesthetic drug, has the advantages of rapid onset and recovery and is widely used in various surgeries and medical procedures. However, its sole use may have limitations such as unstable intraoperative hemodynamics, inadequate postoperative pain control, and limited neuroprotective effects.17 Therefore, finding a safer and more effective anesthesia management strategy is an urgent clinical need. In recent years, remifentanil, as a potent analgesic, has been widely used in clinical anesthesia management.18 Remifentanil has the advantages of rapid onset, potent analgesia, and hemodynamic stability. It not only provides excellent anesthesia but also alleviates intraoperative and postoperative pain, thereby improving the surgical experience and postoperative recovery of patients. Therefore, this study attempted to explore the application effect of combining remifentanil with propofol in anesthesia for TBI patients and its impact on patients’ postoperative recovery.
Surgery, as a potent stressor, often induces intense physiological responses in patients, affecting the changes in hemodynamic parameters, which may impact the patient’s prognosis.19 The results of this study show that the perioperative levels of SpO2, MAP, and HR in both groups exhibited a trend of initial increase followed by decrease, with the observation group showing smaller fluctuations compared to the control group. The VAS scores and RSAS scores of both groups increased at 24 hours postoperatively compared to 1 hour postoperatively, with the observation group showing smaller fluctuations compared to the control group. The proportion of patients with good prognosis in the observation group was higher than that in the control group. These results are consistent with previous studies,20,21 indicating that compared to the sole use of propofol, the combination of remifentanil and propofol in TBI surgery patients can stabilize the patients’ hemodynamic levels, effectively alleviate perioperative pain and agitation, and contribute to the patients’ postoperative recovery. The reasons for this are as follows: ① Remifentanil has the effect of dilating cerebral blood vessels and improving blood flow, thereby maintaining the hemodynamic stability of brain tissue; ② Remifentanil can also act synergistically with propofol to dilate peripheral brain vessels, reduce venous tension, prevent sudden blood pressure rise, and exert a neuroprotective effect; ③ Remifentanil can also protect brain tissue by inhibiting the neuroendocrine system, prolonging analgesic effects, reducing the production of oxygen free radicals, inhibiting brain tissue metabolism, and reducing the risk of cerebral edema and intracranial hypertension. Additionally, the results of this study also showed that the extubation time and awakening time of patients in the observation group were shorter than those in the control group, which may be related to factors such as the rapid metabolism of remifentanil after administration, contributing to the shortened awakening time.
Research22 indicates that the impact of TBI on the body is not only due to direct mechanical damage, but also involves complex changes in inflammation and the nervous system. S-100β, a low molecular weight calcium-binding protein, is primarily concentrated in astrocytes in the nervous system and cells of the anterior pituitary lobe. TBI-induced brain tissue damage leads to a significant increase in S-100β levels in cerebrospinal fluid, which then enters the bloodstream through the damaged blood-brain barrier, resulting in elevated serum S-100β concentrations.23 Meanwhile, NSE mainly exists in brain neurons and neuroendocrine cells. Under normal circumstances, its content in serum is low. However, after brain tissue damage, NSE is released into cerebrospinal fluid and blood, causing a sharp increase in serum NSE concentration.24 TNF-α is primarily produced by monocytes and serves as the initiator of inflammatory responses. It can activate various immune cells during acute brain injury, exacerbating the inflammatory response and thus aggravating brain tissue damage.25 IL-6, a pleiotropic cytokine produced by monocytes and macrophages, participates in the cascade of inflammatory reactions, and its levels are positively correlated with the severity of early neurological dysfunction in brain injury patients.26 The results of this study show that TNF-α, IL-6, S-100β, and NSE levels in both groups increased at 24 hours postoperatively compared to preoperative levels, with smaller fluctuations in the observation group compared to the control group, suggesting that the application of remifentanil combined with propofol may further alleviate the impact of surgery on patients’ brain injury. The reasons for this may be related to the neuroprotective effects of propofol and remifentanil. Propofol can reduce the expression of free radicals and inflammatory factors, while remifentanil has a certain antihypertensive effect in cranial surgery, which is beneficial for temporarily reducing cerebral oxygen consumption and thus protecting brain cells.
Limitations
However, it is important to note that although this study has obtained some meaningful results, there are also some limitations. Firstly, the sample size of this study is relatively small, which may affect the reliability and generalizability of the results. Secondly, the study design adopted retrospective analysis, which may have issues with information bias and confounding factors. Additionally, this study lacks long-term follow-up results, making it impossible to comprehensively assess the long-term prognosis and recovery of patients, which is crucial for the rehabilitation process of TBI patients. Finally, this study was conducted only in a single medical institution, lacking support from multicenter data, which may limit the representativeness and reliability of the results. Therefore, in future research, we will improve and refine the above shortcomings to further enhance the credibility of the research results and the effectiveness of clinical applications.
Conclusion
In this retrospective cohort study of patients with severe traumatic brain injury, the use of a remifentanil-propofol anesthetic regimen, compared to propofol alone, was associated with several more favorable perioperative outcomes. Specifically, the remifentanil-propofol combination was correlated with accelerated anesthesia recovery, demonstrated better stability in intraoperative hemodynamics, and showed improvements in perioperative pain and agitation levels. Furthermore, this regimen was linked to a reduction in postoperative inflammatory and neural damage biomarkers and was associated with better recovery quality at the 3-month follow-up.
These findings suggest that the remifentanil-propofol combination may be a valuable anesthetic strategy for severe TBI patients undergoing surgery. However, given the observational nature of this study, further prospective, randomized controlled trials are warranted to confirm these associations and establish causal efficacy.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Capizzi A, Woo J, Verduzco-Gutierrez M. Traumatic brain injury: an overview of epidemiology, pathophysiology, and medical management. Med Clin North Am. 2020;104(2):213–238. doi:10.1016/j.mcna.2019.11.001
2. Scarboro M, McQuillan KA. Traumatic Brain Injury Update. AACN Adv Crit Care. 2021;32(1):29–50. doi:10.4037/aacnacc2021331
3. Wiles MD. Management of traumatic brain injury: a narrative review of current evidence. Anaesthesia. 2022;77(1):102–112. doi:10.1111/anae.15608
4. Meyfroidt G, Bouzat P, Casaer MP, et al. Management of moderate to severe traumatic brain injury: an update for the intensivist. Intensive Care Med. 2022;48(6):649–666. doi:10.1007/s00134-022-06702-4
5. Chernova AP, Shormanov VK, Davydkina AE. [Propofol: use, toxicology and assay features]. Sud Med Ekspert. 2022;65(5):46–51. Norwegian. doi:10.17116/sudmed20226505146
6. Hughes LM, Irwin MG, Nestor CC. Alternatives to remifentanil for the analgesic component of total intravenous anaesthesia: a narrative review. Anaesthesia. 2023;78(5):620–625. doi:10.1111/anae.15952
7. Ikiz C, Gunenc F, Iyilikci L, et al. Effects of propofol and propofol-remifentanil combinations on haemodynamics, seizure duration and recovery during electroconvulsive therapy. Turk J Anaesthesiol Reanim. 2021;49(1):44–51. doi:10.5152/TJAR.2020.157
8. Chen J, Ying X, Yang D. Propofol combined with remifentanil reduces the adverse reactions of patients undergoing laparoscopic cholecystectomies. Am J Transl Res. 2021;13(6):6560–6567.
9. Doyle DJ, Hendrix JM, Garmon EH. American Society of Anesthesiologists Classification. In: StatPearls. Treasure Island (FL): StatPearls Publishing LLC; 2024.
10. Bodien YG, Barra A, Temkin NR, et al. Diagnosing level of consciousness: the limits of the glasgow coma scale total score. J Neurotrauma. 2021;38(23):3295–3305. doi:10.1089/neu.2021.0199
11. Bielewicz J, Daniluk B, Kamieniak P. VAS and NRS, same or different? Are visual analog scale values and numerical rating scale equally viable tools for assessing patients after microdiscectomy? Pain Res Manag. 2022;2022:5337483. doi:10.1155/2022/5337483
12. Cho SA, Ahn S-M, Kwon W, et al. Comparison of remimazolam and desflurane in emergence agitation after general anesthesia for nasal surgery: a prospective randomized controlled study. Korean J Anesthesiol. 2024;77:432–440. doi:10.4097/kja.23953
13. Anestis DM, Marinos K, Tsitsopoulos PP. Comparison of the prognostic validity of three simplified consciousness assessment scales with the glasgow coma scale. Eur J Trauma Emerg Surg. 2023;49(5):2193–2202. doi:10.1007/s00068-023-02286-w
14. van Veen E, Nieboer D, Kompanje EJO, et al. Comparative effectiveness of mannitol versus hypertonic saline in patients with traumatic brain injury: a CENTER-TBI study. J Neurotrauma. 2023;40(13–14):1352–1365. doi:10.1089/neu.2022.0465
15. Maleki MS, Mazaheri SA, Hosseini SH, et al. Epidemiology of traumatic brain injury in iran: a systematic review and meta-analysis. Iran J Public Health. 2023;52(9):1818–1831. doi:10.18502/ijph.v52i9.13565
16. Denchev K, Gomez J, Chen P, et al. Traumatic brain injury: intraoperative management and intensive care unit multimodality monitoring. Anesthesiol Clin. 2023;41(1):39–78. doi:10.1016/j.anclin.2022.11.003
17. Hewson DW, Hardman JG, Bedforth NM. Patient-maintained propofol sedation for adult patients undergoing surgical or medical procedures: a scoping review of current evidence and technology. Br J Anaesth. 2021;126(1):139–148. doi:10.1016/j.bja.2020.07.053
18. Ren W, Matsusaki T, Bright AO, et al. Association between the remifentanil dose during anesthesia and postoperative pain. Acta Med Okayama. 2022;76(2):187–193. doi:10.18926/AMO/63413
19. Meguro S, Haga N, Imai H, et al. Association between surgical stress and biochemical recurrence after robotic radical prostatectomy. Jsls. 2021;25(1):
20. Huang J, Tian WJ. Effects of remifentanil combined with propofol on hemodynamics and oxidative stress in patients undergoing resection of rectal carcinoma. World J Gastrointest Surg. 2023;15(12):2774–2782. doi:10.4240/wjgs.v15.i12.2774
21. Atashkhoei S, Pouya K, Hakimi P, et al. Remifentanil with or without propofol as anesthesia agents for trans- vaginal ultrasonography oocyte retrieval (TUGOR) on pregnancy and anesthesia outcomes: a randomized controlled trial. Curr Rev Clin Exp Pharmacol. 2021;16(2):182–190. doi:10.2174/1574884715666200623161856
22. Thomas I, Dickens AM, Posti JP, et al. Serum metabolome associated with severity of acute traumatic brain injury. Nat Commun. 2022;13(1):2545. doi:10.1038/s41467-022-30227-5
23. Amoo M, Henry J, O’Halloran PJ, et al. S100B, GFAP, UCH-L1 and NSE as predictors of abnormalities on CT imaging following mild traumatic brain injury: a systematic review and meta-analysis of diagnostic test accuracy. Neurosurg Rev. 2022;45(2):1171–1193.
24. Mozaffari K, Dejam D, Duong C, et al. Systematic review of serum biomarkers in traumatic brain injury. Cureus. 2021;13(8):e17056. doi:10.7759/cureus.17056
25. Hegdekar N, Sarkar C, Bustos S, et al. Inhibition of autophagy in microglia and macrophages exacerbates innate immune responses and worsens brain injury outcomes. Autophagy. 2023;19(7):2026–2044. doi:10.1080/15548627.2023.2167689
26. Ciryam P, Gerzanich V, Simard JM. Interleukin-6 in traumatic brain injury: a janus-faced player in damage and repair. J Neurotrauma. 2023;40(21–22):2249–2269. doi:10.1089/neu.2023.0135
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.