Back to Journals » Patient Preference and Adherence » Volume 10
Relevance of low-pressure compression corsets in physiotherapeutic treatment of patients after mastectomy and lymphadenectomy
Authors Hansdorfer-Korzon R, Teodorczyk J, Gruszecka A, Wydra J, Lass P
Received 12 March 2016
Accepted for publication 4 May 2016
Published 4 July 2016 Volume 2016:10 Pages 1177—1187
DOI https://doi.org/10.2147/PPA.S108326
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Rita Hansdorfer-Korzon,1 Jacek Teodorczyk,2 Agnieszka Gruszecka,3 Jacek Wydra,4 Piotr Lass2,5
1Department of Physiotherapy, 2Department of Nuclear Medicine, 3Department of Informatics and Statistics, Medical University of Gdansk, Gdansk, 4Department of Oncological Surgery, “Szpital Morski im. PCK” Hospital in Gdynia, 5Department of Molecular Spectroscopy, Institute of Experimental Physics, University of Gdansk, Gdansk, Poland
Abstract: There is no fully effective treatment for secondary lymphedema. In patients with breast cancer, lymphedema may present immediately after axillary dissection or years later. It typically occurs in a limb (such as an arm), but it can also occur in the torso, especially in breast cancer patients. It is, therefore, essential to prevent or minimize the condition. The currently used compression therapy has varying efficiency. Thus, researchers are still looking for better solutions, especially for primary prevention. The aim of this study was to find whether compression corsets therapy with a class I compression garment could prevent truncal lymphedema on the operated side in females who underwent mastectomy and axillary lymph node dissection as the standard of care for breast cancer treatment without subsequent reconstruction. We also investigated whether this therapy is efficient in prevention and treatment of truncal lymphedema in patients who underwent mastectomy and additional radiotherapy, and finally whether this method could be implemented for pain reduction strategies in this treatment group. The study was carried out in 50 randomly selected breast cancer patients classified by the oncologist as candidates for surgery. The final study was completed in 37 patients who underwent mastectomy and lymphadenectomy. The study group was randomly divided into two subgroups: subgroup G (received compression corsets 1 month following the surgery) and subgroup K (control) in which the patients underwent no physiotherapeutic treatment. The size of truncal lymphedema was measured using ultrasound in presentation B. Measurements were carried out symmetrically on both sides of the chest wall. The patients were examined four times. The follow-up was for 7 months in total. After the second measurement, a randomly selected subgroup of patients received properly fitted compression corsets, which they had to wear throughout the study, whereas the control subgroup had no physiotherapy treatment. The results were statistically analyzed. In both subgroups, we analyzed the reduction of pain using a visual analog scale. The results strongly suggest that when properly fitted, class I compression corsets not only are an effective treatment for lymphedema but also could be used for antiedematous prevention in patients who underwent removal of axillary lymph nodes as well as radiotherapy. Results of these studies have also confirmed that the use of compression corsets could reduce pain associated with surgical treatment of breast cancer.
Keywords: breast cancer, lymphedema, compression
Introduction
In spite of the huge progress for cancer prevention throughout recent years, the incidence rate of breast cancer has not reduced. Breast cancer is the most common cancer and the most common cause of cancer-related deaths among females in developed and developing countries.1 The mortality rate has been decreasing in developed countries due to mammographic screening and effective treatment.2,3
As more females survive this disease, the number of patients affected by long-term side effects is increasing. Lymphedema is a frequent complication in oncological patients that results in cosmetic defect, dysfunction, pain, and psychological stress leading to deterioration of life quality.4
In the population of patients with breast cancer, the main reason of lymphedema is injury of the axillary lymphatic vessels by surgical operation and/or radiotherapy. Axillary lymphadenectomy and radiation treatment have synergistic effect on lymphedema severity. Lymphedema may appear early or a long time after axillary lymphadenectomy.5 It is a chronic condition with estimates of incidence ranging from 6% to 83%.6
The dissection of lymphatics and lymph nodes can affect regional integrity of the lymphatic system and, therefore, negatively impacts lymphatic outflow. Radiotherapy can similarly destroy lymphatic channels, contributing to further lymphatic drainage disturbance (Figure 1). Damage of the lymphatic system can modify lymphatic drainage pathway in affected quadrant of the body. With time, even after years, the lymphatic system can fail and lymph can accumulate, thus causing edema in the affected region. Extended swelling resulting from the lymph fluid backup in a particular region of the human body is termed lymphedema, a complication that is frequent in the population of patients after lymphadenectomy, especially in cases treated additionally with radiotherapy. Lymphedema most commonly affects a limb; it can appear also in the torso area, particularly in breast cancer patients (Figure 1). It is a reason of many complaints such as tightness, pitting, pain, and hardness.7
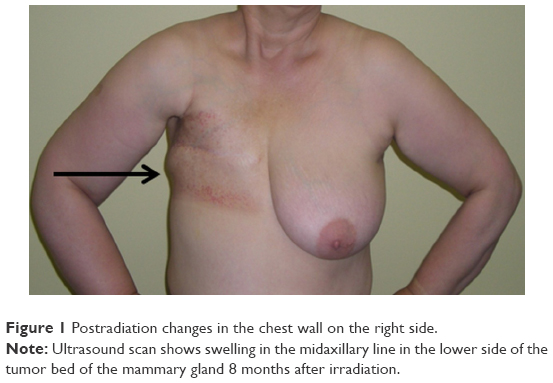 | Figure 1 Postradiation changes in the chest wall on the right side. |
Lymphedema is regarded as a progressive, disfiguring, and disabling disorder that is difficult to treat, and therefore, it is essential to prevent or minimize this condition.4 There are risk factors of lymphedema including undergoing a wide range of surgical procedures, cancer stage (metastasis), being overweight, undergoing chemotherapy and radiotherapy, and individual predispositions.8–10 Only multidisciplinary action can ensure early detection, further treatment, and relapse prevention.11 The main purpose of the therapy is to reduce the volume of fluid that accumulates in the affected area in order to prevent the progression of the disease. Modern treatment of secondary lymphedema after mastectomy usually affects the upper limb on the same side where the surgery was performed and is based on a complete decongestive therapy (CDT) introduced by Földi in 1989.12 The program consists of several components: manual lymph drainage (MLD), various types of compression techniques, physical workout, and special skin care of the region affected by edema.10,13,14 The CDT, which is the international standard according to the American Association of Lymphology and Oncology, is currently perceived as the most efficient treatment for secondary lymphedema.12,15 This method cannot be applied in patients suffering from cardiovascular disease, kidney disease, deep vein thrombosis, or lymphangitis.16 Thanks to the introduction of novel materials (elastomers), which are usable in the therapy of lymphedema (bandages, sleeves, and other kinds of compression clothing), compression treatment is gaining attractiveness. Elastic compression garments exert controlled pressure on edematous areas of the body for quite a long time and are removed for daily hygiene. The compression level is precisely adjustable within the specified parameters. At the beginning, compression treatment utilized compression bandages with low elasticity degree, but their use proved to be impractical in daily use because their application demands a lot of practice. Many patients did not cooperate due to the need of often removing and reapplying bandages.
Application of sequential pneumatic compression (SPC) requires a deep analysis of any possible contraindications (primarily, inflammation and thrombosis). There is no standard time determined for the application of compression. According to the consensus of the International Society of Lymphology in 2013, usefulness of SPC has not yet been sufficiently tested.17 According to Uzkeser and Karatay, addition of SPC to the therapy may not provide any additional benefit for upper extremity impairments.18 Numerous sorts of compression clothing that not only enhance the venous return and alleviate edema, but also reduce the risk of tissue injuries are more efficacious and more likely to be applied by patients. They are designed to be worn during day and night. The results of compression therapy are promising.11,12 The pressure exerted on the edematous body parts not only enhances both lymphatic and venous circulation, but additionally stimulates muscles which build a natural pumping system reducing excess volume of protein-rich lymph, thus reducing the risk of fibrosis and infection in course of lymphedema.19
In contrast to the well-organized physiotherapy received by breast cancer patients with edema in the upper limb, the possibilities of implementing rehabilitation in patients with lymphedema of the chest area are significantly limited. It should be emphasized that the area of the chest is often subjected to radiotherapy in breast cancer patients, which also irreversibly damages the lymphatic system affecting lymph drainage.20 In such patients, multichamber pneumatic jackets are employed (Figure 2). According to the basic principle of lymphatic drainage (according to Vodder),12 clothes activate the first group of functional lymph nodes and lymph vessels above the injury site. Compression starts from the cisterna chyli region, and then continues in the chest including the healthy side and the back. Only after lymphatic massage of those parts of the body, drainage of the upper limb of the operated side begins.
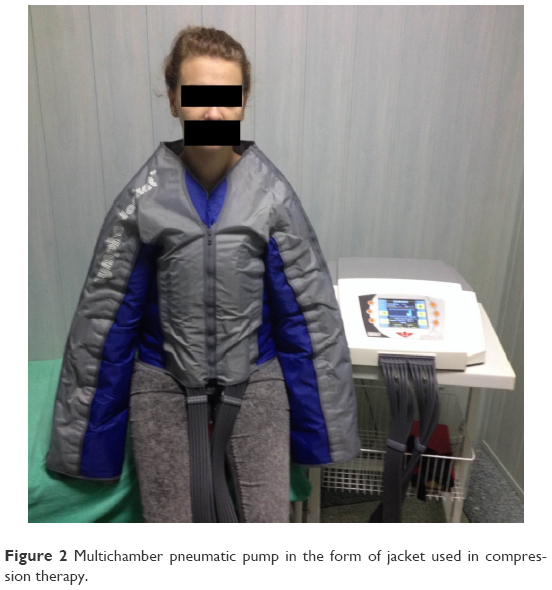 | Figure 2 Multichamber pneumatic pump in the form of jacket used in compression therapy. |
In the literature, cases concerning swelling of the chest area after breast cancer treatment are most commonly discussed in the group of patients after breast-conserving treatment. Breast-conserving therapy consists of two stages: surgery involving excision of the primary lesion with a margin of healthy tissue with axillary lymphadenectomy and subsequent irradiation of preserved breast and adjacent tissue. As a result of such treatment, lymphedema of breast, chest wall, and armpit frequently occurs. For this purpose, a compression camisole or foam rubber padding under the bra is applied. External compression is essential in order to prevent progression of secondary tissue changes.21
Pain is an important early symptom of lymphedema. Patients may also feel fullness, heaviness, and have a feeling of tension.22,23 If compression therapy is not applied, fibrosis processes occur, and their precise mechanisms are not yet understood. The progress of fibrosis varies from patient to patient and depends on individual predisposition.24
Through the course of our practice with patients who underwent breast cancer surgery and axillary lymph node dissection, we have encountered lymphedema localized on the chest wall, which may occur at various times after the surgery. It causes considerable pain with both physical and mental discomfort (Figure 3). Lymphedema often occurs in this location in spite of the implementation of CDT with MLD.
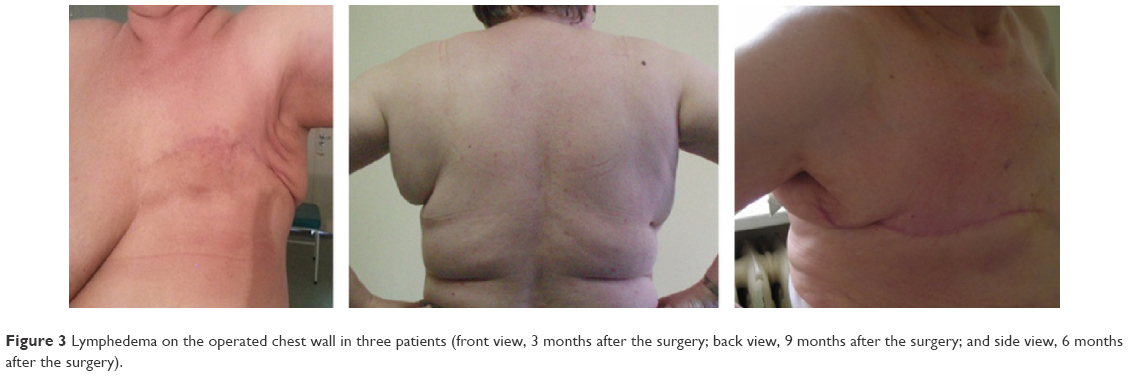 | Figure 3 Lymphedema on the operated chest wall in three patients (front view, 3 months after the surgery; back view, 9 months after the surgery; and side view, 6 months after the surgery). |
Aim of the study
The aim of the study is to find the response in women who underwent mastectomy with axillary lymph node dissection:
- Compression therapy with class I compression corsets implemented no later than 1 month after the surgery can prevent truncal lymphedema on the operated side.
- The use of compression corsets is purposeful and efficient in the prevention and treatment of truncal lymphedema on the operated side in patients who underwent mastectomy and additional radiotherapy.
- The use of compression corsets is indicated and effective in reduction of pain associated with the breast cancer surgical treatment.
Materials and methods
This study was accepted by the institutional bioethics committee of Medical University of Gdansk, Poland. During the first visit by the oncological surgeon, patients gave written informed consent. The study was carried out in 50 randomly selected breast cancer patients classified by the oncologist as candidates for surgery. During the entire observation period (7 months),13 13 patients were excluded: eight patients due to the serious illness after chemotherapy, which made it impossible for them to get to the place of examination, two patients withdrew because of severe viral infection, and three patients required reoperation. Eventually, the study was completed with 37 patients who underwent total mastectomy without breast reconstruction. All of the patients had their axillary lymph nodes removed.
The study group was randomly divided into two subgroups: subgroup G was composed of 19 women who received a compression corset within 1 month following the surgery and subgroup K (control subgroup) was composed of 18 women who had no physiotherapeutic treatment for the entire period of observation.
The average age of the patients in both subgroups was 62 and it demonstrated no statistically significant difference (Table 1; Figure 4).
 | Table 1 The average age of patients in both subgroups |
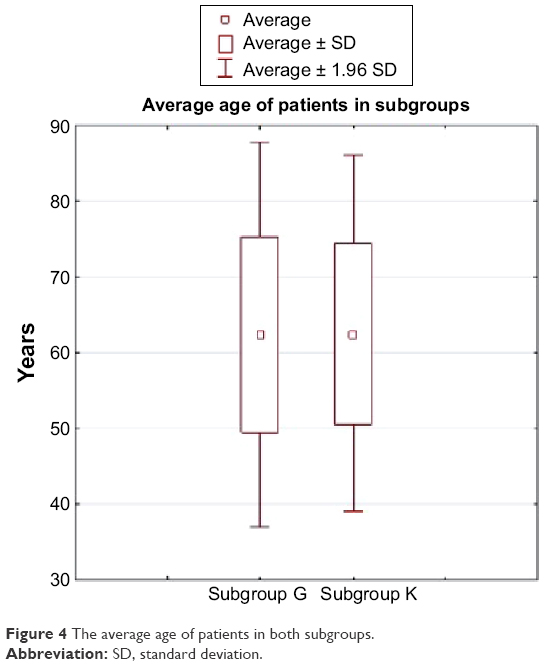 | Figure 4 The average age of patients in both subgroups. |
A comparative analysis of body mass index (BMI) was performed. In both the subgroup of patients wearing compression corsets and in the control subgroup, median BMI values were not significantly different and were within normal limits (Table 2).
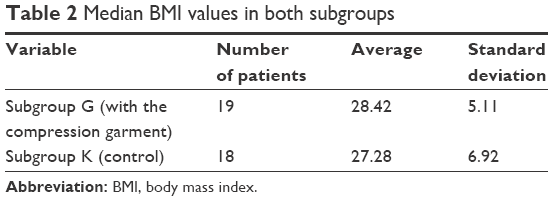 | Table 2 Median BMI values in both subgroups |
Methods
The size of truncal lymphedema was measured in the study group of patients using the ultrasound method in two-dimensional presentation (Voluson E8, linear probe ML6-15, GE Healthcare, Milwaukee, WI, USA). Measurements were carried out symmetrically on both sides of the chest wall in the midaxillary line just below the mammary gland (measuring point 1 and measuring point 2, Figure 5). The measurement was carried out using a thick layer of gel to avoid any alteration of the results caused by the pressure of the ultrasound probe. Symmetrical measurements of the ratio of the subcutaneous tissue thickness on the operated versus healthy sides of the body provided the value of the asymmetry independent of the following factors: variable hydration of the patient, ambient temperature, seasonal influences, or hormonal influences. With the asymmetry factor, it became possible to eliminate the impact of changes in the body fat thickness.
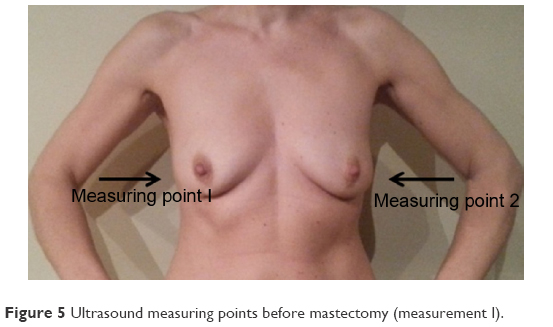 | Figure 5 Ultrasound measuring points before mastectomy (measurement I). |
The patients were examined four times: baseline examination immediately prior to surgery was the first date for observation (measurement I, Figure 5); second examination was performed 1 month after the surgery (measurement II, Figure 6); third examination was performed after 2 months from the second (measurement III, Figure 6); and the final examination, which was the completion of the observation, was performed after 4 months from the third (measurement IV, Figure 6). The follow-up was for 7 months in total. The aim of the first examination was to determine any baseline irregularities (eg, asymmetries, anomalies) in the examined body region. After measurement II, a subgroup of randomly selected patients received a properly fitted compression corset (Figure 7), which they had to wear throughout the study. Thus, the patients were divided into two subgroups: with a compression corset, subgroup G; and without a compression corset, control subgroup K.
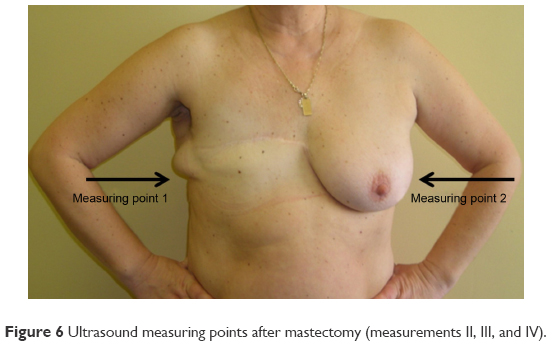 | Figure 6 Ultrasound measuring points after mastectomy (measurements II, III, and IV). |
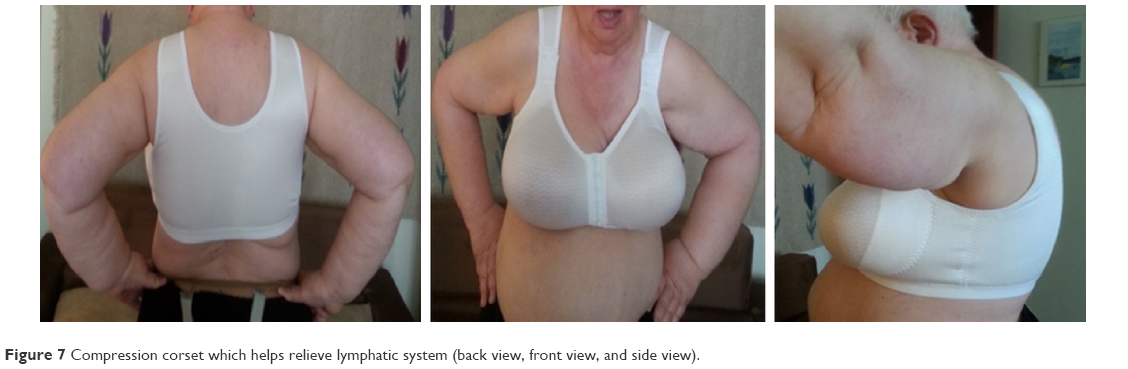 | Figure 7 Compression corset which helps relieve lymphatic system (back view, front view, and side view). |
In the study, low-pressure compression corsets were used, made of flexible fabric with soft, fine-grained inner lining (micro-massage texture).22 The compression garment had seamless cups. The side support for the breast and the prosthesis (bi-elastic) exerted additional controlled pressure on body tissues, aiding lymphatic drainage and accelerating the scar healing process. High built-up back and underarm openings provided good hold of the regions of the axilla and back affected by lymphedema.
The ultrasound examination results were used to calculate the thickness ratios of the subcutaneous tissue on the chest wall on the operated side compared to the other side.
The statistical analysis was based on the nonparametric Mann–Whitney U-test. In both subgroups (G and K), nonparametric Friedman analysis of variance (ANOVA) test was carried out.
In both subgroups, the reduction of pain associated with the surgery was analyzed. This analysis used the visual analog scale. It is a simple method used for measuring subjective variables such as pain, which can take values in a continuous manner and cannot be precisely measured with the available instruments.
During the second (measurement II) and final (measurement IV) ultrasound examination, patients of the compression corsets subgroup (G) and the control subgroup (K) were asked to indicate the intensity of pain using a 10-point scale, where 0 value was assigned for completely free from pain and 10 value represented unbearable pain (Figure 8). The pain intensity, expressed in numeric values, made it possible to compare the differences during the control examination carried out after 4 months. Due to its apparent simplicity and universality, this method is used as one of the most common tools to measure the intensity of pain.
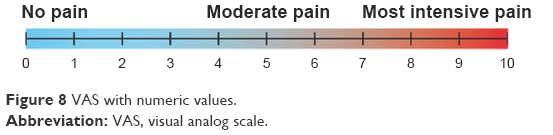 | Figure 8 VAS with numeric values. |
Results
The test is designed for repeated results; it verifies similarity between the examinations I, II, III, and IV within the same subgroup. The conclusions drawn on the basis of the analysis (at the significance level P=0.0000) show that there is a statistically significant difference between the compression corsets subgroup (G) and the control subgroup (K) in the average ratios of thickness of the subcutaneous tissue of the chest wall in the final measurement (measurement IV after 7 months of follow-up).
The ultrasonography test, performed after mastectomy with axillary lymphadenectomy, showed the occurrence of edema in all the patients of both subgroups (measurement II). It is a natural reaction after any surgical intervention. After this test, some randomly selected patients received the compression corsets and the remaining patients were selected to constitute the control subgroup. In both subgroups, we observed reduction of edema parallel to regression of acute and subacute posttraumatic, postoperative changes (measurement III – 4 months after surgery). Pronounced difference in the lymphedema degree between subgroups was demonstrated 6 months after surgery (Figures 9–11).
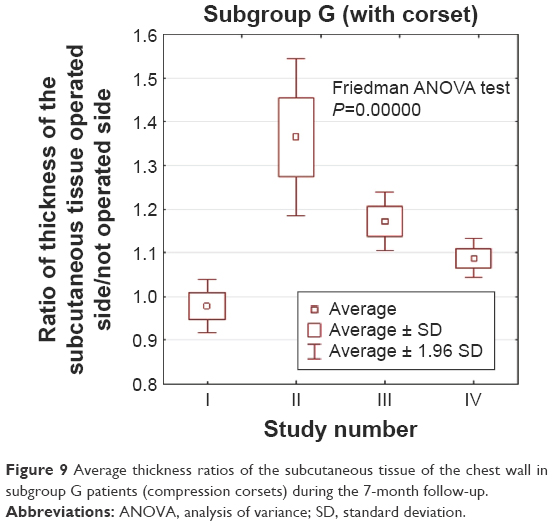 | Figure 9 Average thickness ratios of the subcutaneous tissue of the chest wall in subgroup G patients (compression corsets) during the 7-month follow-up. |
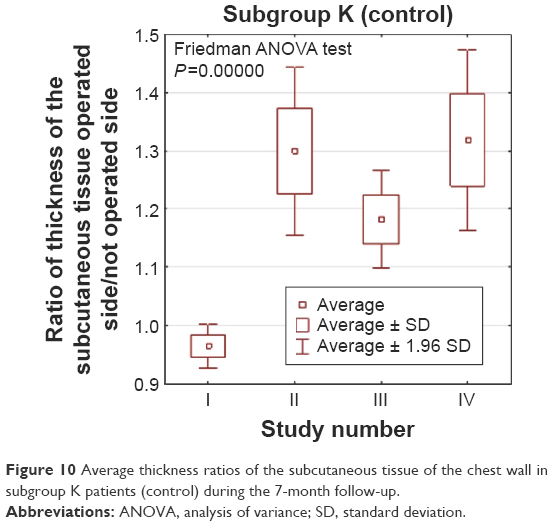 | Figure 10 Average thickness ratios of the subcutaneous tissue of the chest wall in subgroup K patients (control) during the 7-month follow-up. |
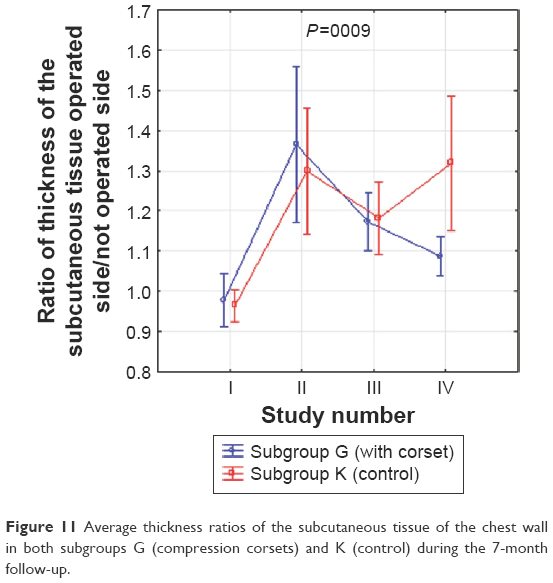 | Figure 11 Average thickness ratios of the subcutaneous tissue of the chest wall in both subgroups G (compression corsets) and K (control) during the 7-month follow-up. |
Also, some selected patients in each subgroup were undergoing radiotherapy throughout the observation. The obtained results, presented in Figures 12 and 13, also confirm the positive effects of the compression corsets therapy in patients after the radiotherapy treatment.
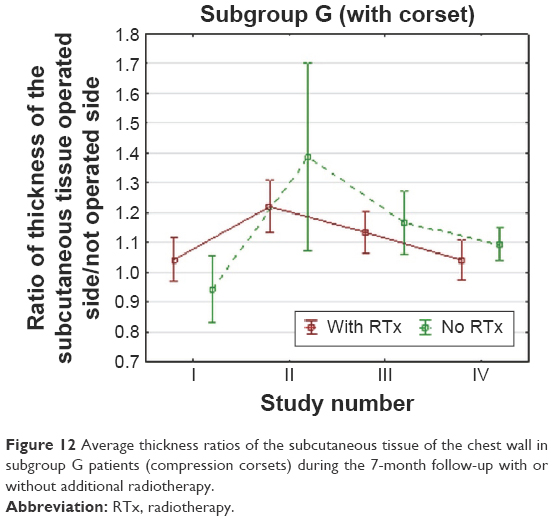 | Figure 12 Average thickness ratios of the subcutaneous tissue of the chest wall in subgroup G patients (compression corsets) during the 7-month follow-up with or without additional radiotherapy. |
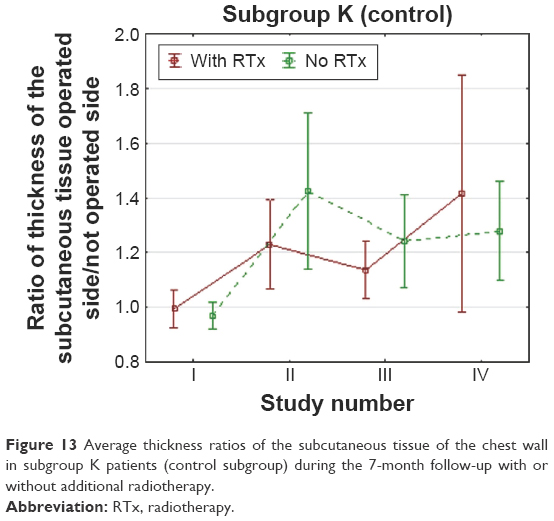 | Figure 13 Average thickness ratios of the subcutaneous tissue of the chest wall in subgroup K patients (control subgroup) during the 7-month follow-up with or without additional radiotherapy. |
Comparing the average thickness ratios of the subcutaneous tissue of the chest wall of the operated side to the opposite side during the 7-month follow-up in both subgroups (Figure 14), significant antiedematous effects were observed in the compression corsets subgroup (subgroup G) even after radiotherapy. Edema was clearly reduced (Figure 14).
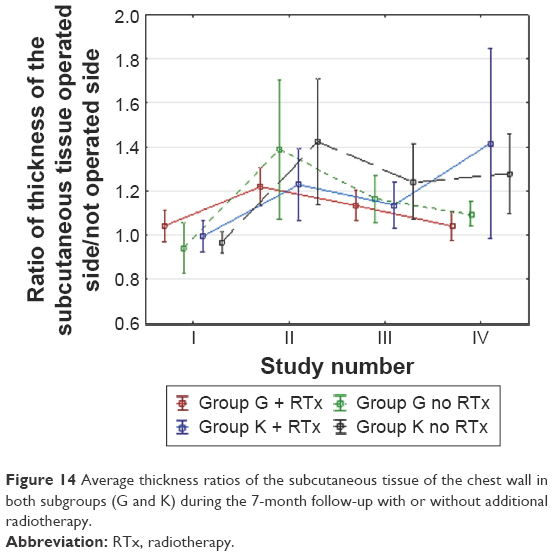 | Figure 14 Average thickness ratios of the subcutaneous tissue of the chest wall in both subgroups (G and K) during the 7-month follow-up with or without additional radiotherapy. |
On the other hand, in the control subgroup (subgroup K), the increase in thickness of the subcutaneous tissue was even higher during the final examination than immediately after the surgery. Edema was increased in this group (Figure 14; Table 3).
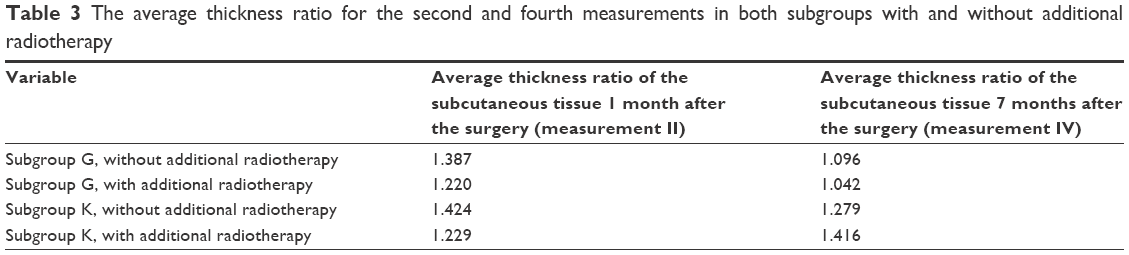 | Table 3 The average thickness ratio for the second and fourth measurements in both subgroups with and without additional radiotherapy |
In both subgroups, based on the results obtained using the visual analog scale, we assessed whether the application of compression corsets no later than 1 month after the surgery was efficient in pain reduction associated with breast cancer surgery. As many as 58% of patients wearing the compression corsets (subgroup G) showed reduction of pain in the chest and shoulder joint on the operated side, while in the control subgroup (subgroup K), reduction of these symptoms occurred in 33% of patients (Figure 15).
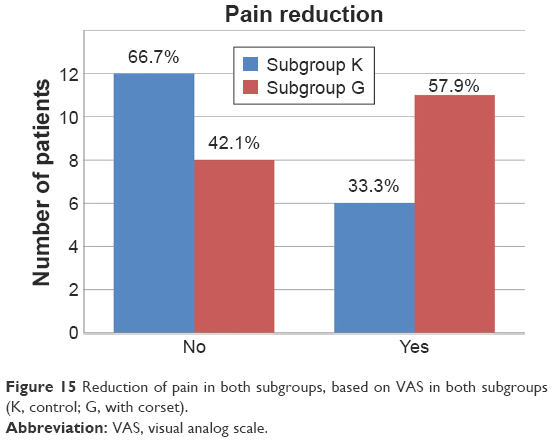 | Figure 15 Reduction of pain in both subgroups, based on VAS in both subgroups (K, control; G, with corset). |
Discussion
Lymphedema in breast cancer patients is a significant, chronic, refractory complication and negatively influences the quality of life.25 If not treated at an early stage, treatment is difficult. Developed lymphedema is not completely curable; so, its prevention is crucial.4 The main risk factor for lymphedema among patients after breast cancer treatment is axillary lymphadenectomy or radiotherapy, but other factors may influence the formation of lymphedema, considering that even sentinel node biopsy may contribute to lymphedema in up to 6% of patients.26 All patients from subgroup K had developed lymphedema localized in the chest wall during 6 months following mastectomy with axillary lymph node dissection, whereas marked lymphedema reduction was achieved during the same period in subgroup G.
Ozcinar et al reported that axillary dissection and radiotherapy to regional lymphatics were related to lymphedema.27 Radiotherapy leads to secondary lymphedema, causing obstruction in the lymph vessels due to scarring and fibrosis of their vessel walls.8,10 Our study shows the importance of the antiedematous impact observed in the subgroup of patients wearing the compression corsets after radiotherapy. Among the patients who wore the compression garment, greater reduction of lymphedema (after the same time) was observed in patients who were not subjected to additional radiotherapy; but in the entire subgroup, the edema tendency was reduced. On the other hand, in the control subgroup (subgroup K), the increase in thickness of subcutaneous tissue was even higher during the final examination than immediately after the surgery.
Mahamaneerat et al found that the risk of lymphedema is increased in patients with a BMI >30.28 In the present study BMI was 28.42 for subgroup G and 27.28 for subgroup K.
Mak et al found that an arm or chest infection is a major risk factor for development or aggravation of lymphedema.29 Our study shows that in patients of the control subgroup (without the compression corsets), lymphedema had an escalating tendency, although no inflammation or infection occurred.
Because of the advancing character of lymphedema, the results of the therapy are influenced by the time of diagnosis, promptitude of introduction, and the kind of treatment. Clinical examinations of lymphedema, for example, by metric measurements, are widely employed, but not adequate because of late detection of disease.30,31 Formation of lymphedema after breast cancer surgery is determined by many clinical and pathological determinants which complicate the definition of the optimal medication.32 Gurdal et al concluded that both concurrent application of intermittent pneumatic compression with lymphatic drainage performed by the patient and manual lymphatic drainage with bandaging are efficacious and well-tolerated treatment options.33 In Ugur et al’s study, decongestive therapy was given to 22 (18%) of 124 patients who developed lymphedema, and 16 (73%) of the patients treated benefited from the treatments. The ratio of patients who accepted such therapy was relatively small, but the ratio of success of treatment in patients who were treated was high. This seems to be connected to the physicians who do not consider the importance of the treatment of lymphedema.4
The problem relates particularly to long-term treatments where the aim is to perpetuate improvement and to prevent rapid relapse of lymphedema. The best way to achieve this goal is to implement continuous compression therapy. Constant compression applied to the region affected by lymphedema improves normal vessel regrowth. The most commonly used materials for this purpose are bandages with a low degree of elasticity and compression garments such as compression sleeves and gloves. Some centers also apply compression pumps. Studies have shown that the exerted compression removes more water than protein, which is the reason for rapid recurrence of edema when the compression is not maintained.34 According to the consensus of the International Society of Lymphology of 2013, the usefulness of SPC requires further study.17
Treatment of acquired lymphedema consists of manual lymphatic drainage, compression therapy, physical rehabilitation, and careful skin care (prevention of infection). By appropriate manual techniques, the therapist allows improves lymphatic circulation, preventing the consequences caused by lymphatic stasis. Drainage always starts from the nodes and the lymph vessels located as close as possible to the sites where the lymph returns to the venous system. This enables the venous system to drain the lymph and helps to create new lymphatic channels.7
The nonoperated side of thorax is the area draining lymph from the defective, postlymphadenectomy side. In addition to the basic techniques, more techniques can be employed in the area of median sagittal watershed with the gravity center on axillo-axillary anastomoses, which stimulates lymphangiomotoricity of the normal vessels. This therapeutic scheme is established on the presumption that in order to remove excess lymph from the thorax on the affected side, and then from the upper extremity on the side of lymphadenectomy, it is required to enhance lymphangiomotoricity of the superficial lymphatic vessels on the nonoperated side of the thorax. In order to achieve a more complete result, further manual techniques can be applied by concentrating on the intercostal space, the epigastrium, and the peripheral part of the chest.
In individuals treated with radiotherapy, manual techniques should be performed on the dorsal side for the stimulation of lymphatics in order to enhance lymphatic flow from the upper extremity (Figure 16).20
 | Figure 16 Directions of manual lymph drainage after axillary lymphadenectomy (substitute lymphatic flow areas are depicted in blue and regions of edema and so-called gravity points are in yellow). |
Publications on MLD mostly concern limited number of patients and most studies do not randomize patients to different groups. Most reports suggest that accuracy in performance of physiotherapeutic procedures is the critical determining factor for success, especially in MLD, which should last 45 minutes at a pressure of 30–40 mmHg. Relatively high costs, extensive time required to perform MLD, frequent inaccuracy of the treatment, instability in the strength of the exerted pressure, and considerable difficulties in cooperation with patients are the main barriers to success.35
Compression corsets may be used as an alternative for lymphatic drainage, especially after axillary lymph node dissection or radiotherapy.
Compression corsets used in the present study have a specific compression value of 18.987 mmHg (Table 4) corresponding to class I compression, which makes it possible to apply an appropriate compression force to body tissues.36,37
 | Table 4 Measurement protocol specifying the class of compression of the fabric37 |
Compression corsets of low compression class presented in the work are designed for use around the clock. They are well tolerated by patients and a constant external pressure helps to maintain the results of treatment. Continuously maintained pressure in the site of swelling activates lymphangiomotorics, and the corsets exert appropriate pressure depending on the work or resting of muscles. The corsets allow “dosage” of external compression. They may also aid in reducing the size of edema by increasing interstitial hydrostatic pressure, and according to Starling forces, they reduce the formation of lymph. Literature confirms that the use of compression corsets significantly improves the outcome of lymphedema even during chronic phase.38 Unfortunately, most of the available studies still present research on the use of only gloves and compression sleeves.
Analysis of the existing literature shows that tendencies in lymphedema treatment slowly but surely turn from time-consuming and costly MLD in favor of special compression garments.10,29 Our study on the use of compression therapy method with class I compression corsets applied to patients not later than 1 month after breast cancer surgery with simultaneous lymphadenectomy confirms the high utility of this technique. We show here antiedematous prevention in the chest wall on the operated side as well as prevention and treatment of lymphedema in patients undergoing additional radiotherapy.
It is unclear why patients develop lymph fluid reservoirs on the chest wall. We suppose that collateral lymphatic channels’ insufficiency in the chest may be the reason. Therapy should be focused on moving the protein-rich fluid retained in the interstitium to the regions of the skin with well-functioning physiological lymphatic drainage. Such a substitute region for lymph flow, in the case of lymphedema of the upper limb, is usually localized to the trunk.20 It is known that the effect of the treatment depends not only on the above-mentioned risk factors of lymphedema development in patients after surgical treatment of breast cancer, but also on the individual genetically related abundance of collateral lymphatic channels, which can be activated in the course of appropriate treatment.39
Compression stockings and compression sleeves available for patients are sewn in standard sizes or are custom-made. In spite of certain difficulties, chest corsets can be made in standard sizes as underwear and, therefore, do not need to be custom-made, which is convenient for the patients.7
Conclusion
Surgical treatment of breast cancer with axillary lymphadenectomy may be followed by development of lymph fluid reservoirs on the chest wall. In addition to individual predisposition, the most likely cause is the lack of any further proceedings, which would consolidate the results achieved by MLD. Class I compression corsets should constitute an integral element of comprehensive therapy to prevent and combat lymphostasis. When properly fitted, not only are they an effective treatment for lymphedema, but also they are used for antiedematous prevention in patients who underwent the removal of axillary lymph nodes as well as radiotherapy. Results of the present study have also confirmed that the use of compression corsets in reduction of pain associated with the surgical treatment of breast cancer is purposeful and efficient. There is an urgent need for developing rehabilitation protocols for breast cancer patients, including broad, modern, and comprehensive approaches for physiotherapeutic treatment.
Disclosure
The authors report no conflicts of interest in this work.
References
Ozmen V. Breast cancer in the world and Turkey. J Breast Health. 2008;4:6–12. | ||
Tuncer AM. Asian Pacific Organization for Cancer Prevention, Cancer Report. Ankara: New Hope in Health, Breast Cancer; 2010:412–416. | ||
DeSantis C, Siegel R, Bandi P, Jemal A. Breast cancer statistics. CA Cancer J Clin. 2011;61:409–418. | ||
Ugur S, Arici C, Yaprak M, et al. Risk factors of breast cancer-related lymphedema. Lymphat Res Biol. 2013;11:72–75. | ||
Ridner SH, Dietrich MS, Kidd N. Breast cancer treatment-related lymphedema self-care: education, practices, symptoms, and quality of life. Support Care Cancer. 2011;19(5):631–637. | ||
Clark B, Sitzia J, Harlow W. Incidence and risk of arm oedema following treatment for breast cancer: a three-year follow-up study. QJM. 2005;98(5):343–348. | ||
Bell LR, inventor; Lindahl EZ, inventor; Available from http://www.google.com/search?tbo=p&tbm=pts&hl=en&q=inassignee:%22Lightening2+LLC%22. Lightening2 LLC, assignee. Compression garment. United States patent US 187164. 2002 Jul 1. | ||
Paskett ED, Dean JA, Oliveri JM, Harrop JP. Cancer-related lymphedema risk factors, diagnosis, treatment, and impact: a review. J Clin Oncol. 2012;30:3726–3733. | ||
Newman B, Lose F, Kedda MA, et al. Possible genetic predisposition to lymphedema after breast cancer. Lymphat Res Biol. 2012;10:2–13. | ||
Dominick SA, Madlensky L, Natarajan L, Pierce JP. Risk factors associated with breast cancer-related lymphedema in the WHEL Study. J Cancer Surviv. 2013;7:115–123. | ||
Meneses KD, McNees MP. Upper extremity lymphedema after treatment for breast cancer: a review of the literature. Ostomy Wound Manage. 2007;53:16–29. | ||
Vignes S, Porcher R, Arrault M, Dupuy A. Long-term management of breast cancer-related lymphedema after intensive decongestive physiotherapy. Breast Cancer Res Treat. 2007;101:285–290. | ||
Fu MR, Ridner SH, Armer J. Post-breast cancer. Lymphedema: part 1. Am J Nurs. 2009;109:48–54. | ||
Holcomb SS. Identification and treatment of different types of lymphedema. Adv Skin Wound Care. 2006;19:103–108. | ||
Martín ML, Hernández MA, Avendaño C, Rodríguez F, Martínez H. Manual lymphatic drainage therapy in patients with breast cancer related lymphoedema. BMC Cancer. 2011;11:94. | ||
Turk G, Khorshid L. The complete decongestive therapy in management developing in relation with mastectomy. J Breast Health. 2011;7:96–100. | ||
International Society of Lymphology. The diagnosis and treatment of peripheral lymphedema. 2013 consensus document of the International Society of Lymphology. Lymphology. 2013;46:1–11. | ||
Uzkeser H, Karatay S. Intermittent pneumatic compression pump in upper extremity impairments of breast cancer-related lymphedema. Turk J Med Sci. 2013;43(1):99–103. | ||
Cheville AL, McGarvey CL, Petrek JA, Russo SA, Taylor ME, Thiadens SR. Lymphedema management. Semin Radiat Oncol. 2003;13:290–301. | ||
Bringezu G, Schreiner O. Lehrbuch der Entstauungstherapie 2: Behandlungskonzepte für die Praxis. Vol 47. Springer-Verlag, 2013. German. | ||
Pritschow H, Schuchhardt C. Lymphedema management and complete physical decongestive therapy. A manual for treatment. Köln Viavital-Verl. 2010:183–185. | ||
Badger CM, Peacock JL, Mortimer PS. A randomized, controlled, parallel-group clinical trial comparing multilayer bandaging followed by hosiery versus hosiery alone in the treatment of patients with lymphedema of the limb. Cancer. 2000;88:2832–2837. | ||
Szuba A, Achalu R, Rockson SG. Decongestive lymphatic therapy for patients with breast carcinoma associated lymhedema. A randomized prospective study of a role for adjunctive intermittent pneumatic compression. Cancer. 2002;95:2260–2267. | ||
Sakorafas GH, Peros G, Cataliotti L, Vlastos G. Lymphedema following axillary lymph node dissection for breast cancer. Surg Oncol. 2006;15:153–165. | ||
Hayes S, Di Sipio T, Rye S, et al. Prevalence and prognostic significance of secondary lymphedema following breast cancer. Lymphat Res Biol. 2011;9:135–141. | ||
Barranger E, Dubernard G, Fleurence J, Antoine M, Darai E, Uzan S. Subjective morbidity and quality of life after sentinel node biopsy and axillary lymph node dissection for breast cancer. J Surg Oncol. 2005;92:17–22. | ||
Ozcinar B, Guler SA, Kocaman N, Ozkan M, Gulluoglu BM, Ozmen V. Breast cancer related lymphedema in patients with different loco-regional treatments. Breast. 2012;21:361–365. | ||
Mahamaneerat WK, Shyu CR, Stewart BR, Armer JM. Breast cancer treatment, BMI, post-op swelling/lymphoedema. J Lymphoedema. 2008;3:38–44. | ||
Mak SS, Yeo W, Lee YM, et al. Risk factors for the initiation and aggravation of lymphoedema after axillary lymph node dissection for breast cancer. Hong Kong Med J. 2009;15:8–12. | ||
Stanton AB, Badger C, Sitzia J. Non-invasive assessment of the lymphedematous limb. Lymphology. 2000;33:122–135. | ||
Hansdorfer-Korzon R, Bakuła S, Nowakowski M. Znaczenie przezpowłokowej ultrasonografii w prezentacji B w porównaniu z metodą pomiaru obwodów kończyn w rozpoznawaniu wczesnych stadiów obrzęku limfatycznego u kobiet po mastektomii. [The role of B-mode ultrasound examination compared to limb circumference measurement in the diagnosis of early of lymphatic edema in women after mastectomy]. Fizjoterapia Polska. 2005;5:31–40. Polish. | ||
Uzkeser H, Karatay S, Erdemci B, Koc M, Senel K. Efficacy of manual lymphatic drainage and intermittent pneumatic compression pump use in the treatment of lymphedema after mastectomy: a randomized controlled trial. Breast Cancer. 2015;22:300–307. | ||
Gurdal SO, Kostanoglu A, Cavdar I, et al. Comparison of intermittent pneumatic compression with manual lymphatic drainage for treatment of breast cancer-related lymphedema. Lymphat Res Biol. 2012;10:129–135. | ||
Partsch H, Flour M, Smith PC; International Compression Club; Indications for compression therapy in venous and lymphatic disease consensus based on experimental data and scientific evidence. Under the auspices of the IUP. Int Angiol. 2008;27:193–219. | ||
Huang TW, Tseng SH, Lin CC, et al. Effects of manual lymphatic drainage on breast cancer-related lymphedema: a systematic review and meta-analysis of randomized controlled trials. World J Surg Oncol. 2013;24:11–15. | ||
Rabe E. Compression Guide. Bonn: Rabe Medical Publishing; 2009:87–89. | ||
Anita Dr Helbig GmbH: Messprotokoll-Materialprufung Artikel Nr 96376, Brannenburg 2011. | ||
Devoogdt N, Van Kampen M, Geraerts I, Coremans T, Christiaens MR. Different physical treatment modalities for lymphoedema developing after axillary lymph node dissection for breast cancer: a review. Eur J Obstet Gynecol Reprod Biol. 2010;149:3–9. | ||
Vignes S, Porcher R, Arrault M, Dupuy A. Long-term management of breast cancer-related lymphedema after intensive decongestive physiotherapy. Breast Cancer Res Treat. 2007;101:285–290. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.