Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 13
Relationship Between sCD163 and mCD163 and Their Implication in the Detection and Typing of Leprosy
Authors Farag AGA ![]() , El Askary SA, Fathy WM, Elbassal F
, El Askary SA, Fathy WM, Elbassal F ![]() , Azzam AA, Tayel NR
, Azzam AA, Tayel NR ![]() , Abdul Karim SS, Shehata WA
, Abdul Karim SS, Shehata WA ![]()
Received 28 November 2019
Accepted for publication 17 March 2020
Published 2 June 2020 Volume 2020:13 Pages 379—389
DOI https://doi.org/10.2147/CCID.S240420
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Azza Gaber Antar Farag,1 Shymaa A El Askary,2 Waleed M Fathy,3 Fathia Elbassal,3 Ayman Ali Azzam,4 Nermin Reda Tayel,5 Samah Saad Abdul Karim,6 Wafaa Ahmed Shehata1
1Dermatology, Andrology & STDs Department, Faculty of Medicine, Menoufia University, Al Menoufia, Egypt; 2Medical Microbiology and Immunology Department, Faculty of Medicine, Menoufia University, Minufya, Egypt; 3Clinical Pathology Department, Faculty of Medicine, Menoufia University, Minufya, Egypt; 4Clinical Biochemistry Department, National Liver Institute, Menoufia University, Minufya, Egypt; 5Department of Molecular Diagnostics and Therapeutics, Genetic Engineering Biotechnology Research Institute, Sadat City, Egypt; 6Dermatology Department, Shebin ElKom Teaching Hospital, Minufya, Egypt
Correspondence: Azza Gaber Antar Farag
Dermatology, Andrology & STDs Department, Faculty of Medicine, Menoufia University, Shebin ElKom, Al Menoufia 32511, Egypt
Tel +20 109 778 7204
Fax +20 2482 226 454
Email [email protected]
Background: Leprosy is a chronic contagious disease caused by Mycobacterium lepraea. CD163 is a monocyte trans-membrane glycoprotein receptor (mCD163) that sheds from the cell surface and circulates as a soluble (serum) form (sCD163). Changes in the mCD163 and sCD163 levels could mirror the categorization of inflammatory procedure, demonstrating a possible use of CD163 as a diagnostic indicator of inflammation.
Objective: To investigate the possible role of CD163 (sCD163 and mCD163) in leprosy pathogenesis and to assess whether CD163 is a helpful inflammatory marker of leprosy development and typing.
Patients and Methods: This case control study included 70 leprosy patients and 30 healthy controls. Leprosy patients were classified according to the Madrid criteria (1953) into: tuberculoid leprosy (TT), border-line leprosy (BL), and lepromatous leprosy (LL). For all participants, complete blood count (CBC), serum CD163 using ELISA and monocytes positive for CD163 using flow cytometry were done.
Results: Leprosy patients had significantly low WBCs and platelet counts (p< 0.001) and had significantly higher sCD163 (p=0.025) and mCD163 (p=0.042) that were highest in LL followed by BL, then TT patients (p< 0.001). There was a significant positive correlation between mCD163 and sCD163 levels in leprosy patients (r=0.896, p< 0.001). ROC analysis revealed a significant role of serum sCD163 and of mCD163 positive monocytes in the detection (p< 0.001) and typing of leprosy (p=0.002 and p< 0.001, respectively).
Conclusion: Both sCD163 and mCD163 positive monocytes may have an active role in leprosy pathogenesis. They could be potential biomarkers for leprosy detection and typing.
Keywords: CD163 positive monocytes, flow cytometry, leprosy, sCD163
Introduction
Leprosy is a chronic contagious disease caused by an obligate intracellular bacillus, Mycobacterium leprae (ML) that targets Schwann cells, macrophages, and dendritic cells.1
In spite of the rapid reduction of registered leprosy cases in the last years, leprosy is still a major public health problem in several areas and hyper-endemic infection remains in many countries. According to official figures, 208,619 new leprosy cases were registered globally from 159 countries in 2018, with a prevalence rate of 0.2/10,000 at the end of 2018.2
Leprosy disease classification is defined within two poles; tuberculoid and lepromatous. In-between these two clinical forms, border-line was present.3 The clinical evolution of leprosy is based on the immune response of the host.4 At the tuberculoid pole of leprosy, typical epithelioid macrophages are predominant and the immune response is mediated through T helper (Th)1 lymphocytes, producing cytokines that prompt a pro-inflammatory reaction. While at the lepromatous end, inactivated foamy macrophages are predominant and the immunologic reaction is mediated by Th2 lymphocytes, which elicit a suppressive response. In the border-line forms (BT, BB, and BL) the cellular immune response shows a heterogeneous pattern that fluctuates between that of the two poles (LL and TT).5,6
CD163 (also recognized as p155, hemoglobin scavenger receptor, M130 and RM3/1) is a monocyte/macrophage-limited trans-membrane glycoprotein. It is a member of the scavenger receptor cysteine-rich family.7 CD163 actively sheds from the monocyte surface and circulates as a soluble form (sCD163). This shedding has an active role in controlling the inflammatory process.8 Also, it exhibits direct cytokine-like roles by reducing T-lymphocyte proliferation and activation.9
CD163 binds to hemoglobin (Hb) and haptoglobin complexes exhibiting potent anti-oxidative as well as anti-inflammatory properties. Also, in vivo binding of Hb to CD163 induces the release of IL-10 in addition to other anti-inflammatory intermediaries from macrophages.10 Additionally, increased CD163 shedding appears to be linked to the immunosuppressive switch of inflammation.11 CD163 acts as a bacterial sensor, increasing the likelihood that a different extracellular domain in CD163 is responsible for eliciting pro-inflammatory cytokines.12
Based on the previous data, sCD163 was investigated and identified as an indicator of disease severity in many infectious and inflammatory disorders such as proliferative glomerulonephritis,13 multiple sclerosis,14 Dengue,15 human malaria,16 tuberculosis17 and visceral leishmaniasis.18 However, in leprosy, only few studies were found and little is known about the role of CD163 in leprosy pathogenesis.18,19
Therefore, we aimed in this study to investigate the possible role of CD163 in leprosy pathogenesis through analysis of serum sCD163 and mCD163 monocytes' expression levels in different leprosy types. Also, our aim was extended to assess whether sCD163 and/or mCD163 could be a helpful inflammatory marker for early detection and typing of leprosy.
Patients and Methods
This case-control study was conducted on 70 leprosy patients. They were compared with 30 age- and sex-matched healthy volunteers (a control group) who had no past or family history of leprosy and submitted to careful dermatological exam to exclude the presentation of leprosy at the time of recruitment. All participants were recruited from the Outpatient Clinic of Dermatology, Andrology and STDs Department, Faculty of Medicine, Menoufia University during the period from January 2018 to February 2019. The diagnosis of leprosy was based on the clinical aspects of the lesions and confirmed by histopathological assessment of skin lesions. We included newly diagnosed leprosy patients who did not start the multiple drug therapy (MDT), of both sexes and any age. Exclusion criteria for selected subjects were presence of any diseases (eg, HIV, HTLV1, diabetes) that may have an affect on the immune reaction or on the clinical consequence of leprosy. Pregnant and lactating females were also excluded.
The study protocol was approved by the Ethical Committee of Human Right of Research at Menoufia University (IRB approval number and date 5/2018DERM), and was in accordance with the Declaration of Helsinki.
Written informed consent form was signed by each participant included in this study after they were informed about the study. All data were kept and preserved.
Dermato-neurologic clinical examination was done for all patients. Proper evaluation of skin lesions was performed to determine the distribution, clinical variants and criteria of each type of leprosy. Leprosy patients were classified according to the Madrid (1953) criteria into three clinical forms: tuberculoid leprosy (TT, n=27), borderline leprosy (BL, n= 10), and lepromatous leprosy (LL, n=33). Patients having TT had less than five sharp demarcated anesthetic erythematous or erythematous-hypochromic plaques. Patients with LL had multiple, bilateral hypochromic spots, diffuse erythematous plaques and erythematous-violet bright infiltrated nodules.18
After collection of blood and tissue samples, patients were treated following the standard multidrug therapy (MDT).
Blood Sample Studies
Under complete aseptic conditions, blood was collected from all subjects after overnight fasting. Blood samples were sent to Microbiology and Immunology department, Faculty of Medicine, Menoufia University for assessment of complete blood count, sCD163 serum level, and CD163 positive monocytes.
Complete Blood Count
CBC was performed by an automatic hematology analyzer (XT-1800I/SYSMEX, Japan).
sCD163 Serum Level
Blood samples were transferred into plain tubes, left at 37°C for 30 min to clot, and then centrifuged for 10 min at 4,000xg. The serum obtained was put into aliquots and kept at −80°C until time of analysis for determination of human sCD163 level using ELISA kit according to the manufacturer’s instructions (Shanghai SunRedbio (SRB) Technology, China), based on a double-antibody sandwich ELIZA assay. Standards and test samples were added to monoclonal antibody enzyme which was pre-coated with serum CD163 monoclonal antibody, incubated, and; followed by washing with PBS buffer. Then, sCD163 antibodies labeled with biotin were added, and combined with streptavidin-HRP to form immune complex; then incubation and washing were carried out again to remove the uncombined enzyme. Chromogen solution A, B were added, the color of the liquid changed to blue, and with the effect of acid, the color finally became yellow. The chroma of color and the concentration of the H sCD163 of sample were positively correlated.
CD163 Positive Monocytes
The anti-coagulated blood was drawn into a sterile BD Vacutainer EDTA blood collection tube, and stored at room temperature (20°C–25°C) until it was ready for staining and lysing according to the manufacturer’s instructions (Boster Biological Technology, Pleasanton, CA, USA).
For each sample a set of BD tubes were labeled. The panel of antibodies used included CD163PE (rabbit polyclonal anti-Human CD163 antibody) (Boster Biological Technology, Pleasanton, CA, USA) and CD14 FITC (mouse monoclonal anti-Human CD14 antibody) (BD Franklin Lakes, New Jersey, USA). 100 µL of whole blood was transferred into each flow tube. 10 µL of each antibody was added and mixed well. The mixture was incubated at 2–8°C for 30–45 minutes.
After incubation, 2 mL of lysing solution (BD FACS™ lysing solution) was added to each tube and left for 5–10 minutes until complete lysis of RBCs occurred. Un-reacted antibody was removed by washing the cells twice in 2 mL phosphate buffered saline (PBS).
Finally the cells were suspended in 200 µL of PBS for final flow cytometric analysis. As a control for analysis, 100 µL of cells were put in a separate tube as auto-control (R & D Systems, Inc., Minneapolis, MN, USA).
Flow cytometric analysis: data were acquired on a FACS caliber flow cytometer (BD immune cytometry systems, San Jose, CA, USA). The instrument set-up was checked using QC windows beads (flow cytometry standard, San Juan, PR). Forward scatter and side scatter measurements were made using linear amplifiers, whereas fluorescence measurements were made with logarithmic amplifiers and flow cytometric two parameters dot plots and quadrant statistics were generated by cell quest software (Becton Dickinson immune-cytometer systems). Analysis was performed after gating around a monocyte population on a forward scatter versus side scatter dot-plot. Second gate was subsequently put on the CD14 and CD163 double positive monocyte population. The percentage of positive cells for CD163 was made by estimation of the percentage of CD163 on CD14 positive monocytes. Figure 1 demonstrated flow cytometry analysis of circulating monocytes.
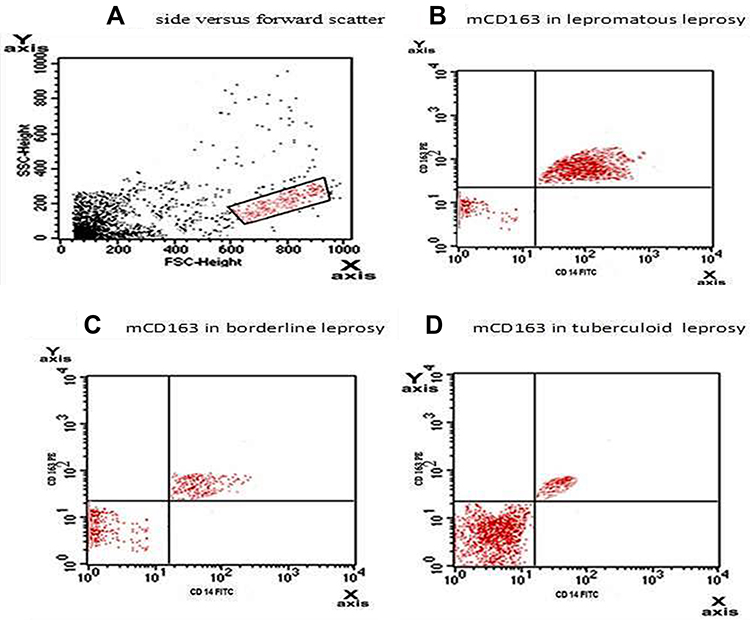 |
Figure 1 (A) Forward scatter versus side scatter with primary gate on the monocyte region depending on cell size and granularity. (B-D) The monocyte area was selected where double positive for both CD163 PE and CD 14 FITC. The single CD14 FITC positive are in the lower right quadrant, single CD163 PE positive are in the upper left quadrant, double positive are in the upper right quadrant. LL had significantly higher mCD163 (46.68±22.17) than BL (16.80±8.71) and TL (14.72±3.41) (p<0.001), but insignificant difference between BL and TL (p=0.1). Abbreviations: CD, cluster of differentiation; PE, phycoerythrin; FITC, fluorescein isothiocyanate; mCD, membrane bound cluster of differentiation; LL, lepromatous leprosy; BL, border-line leprosy; TL, tuberculoid leprosy; SSC, side scatter; FSC, forward scatter. |
Statistical Analysis
The current data were tabulated and analyzed statistically by IBM personal computer and statistical package SPSS version 20 (SPSS Inc., Chicago, IL, USA).
Qualitative data were presented as number and percent, whereas quantitative data were described using mean ± SD. Student’s t-test was used to compare two groups of quantitative variables. Kruskal–Wallis and Mann–Whitney tests were used to compare three and two groups of nonparametric variables, respectively. P-value less than 0.05 was considered statistically significant.
Results
Demographic and Clinical Data of Studied Subjects
All patients' data were collected before starting MDT treatment. Their personal data and clinical characteristics are demonstrated in Table 1. Patient and control groups were matched as regards to demographic characteristics except occupation and socioeconomic status, as leprosy patients were of significantly low socioeconomic level (P=0.002) and had no work (p=0.029) (Table 1).
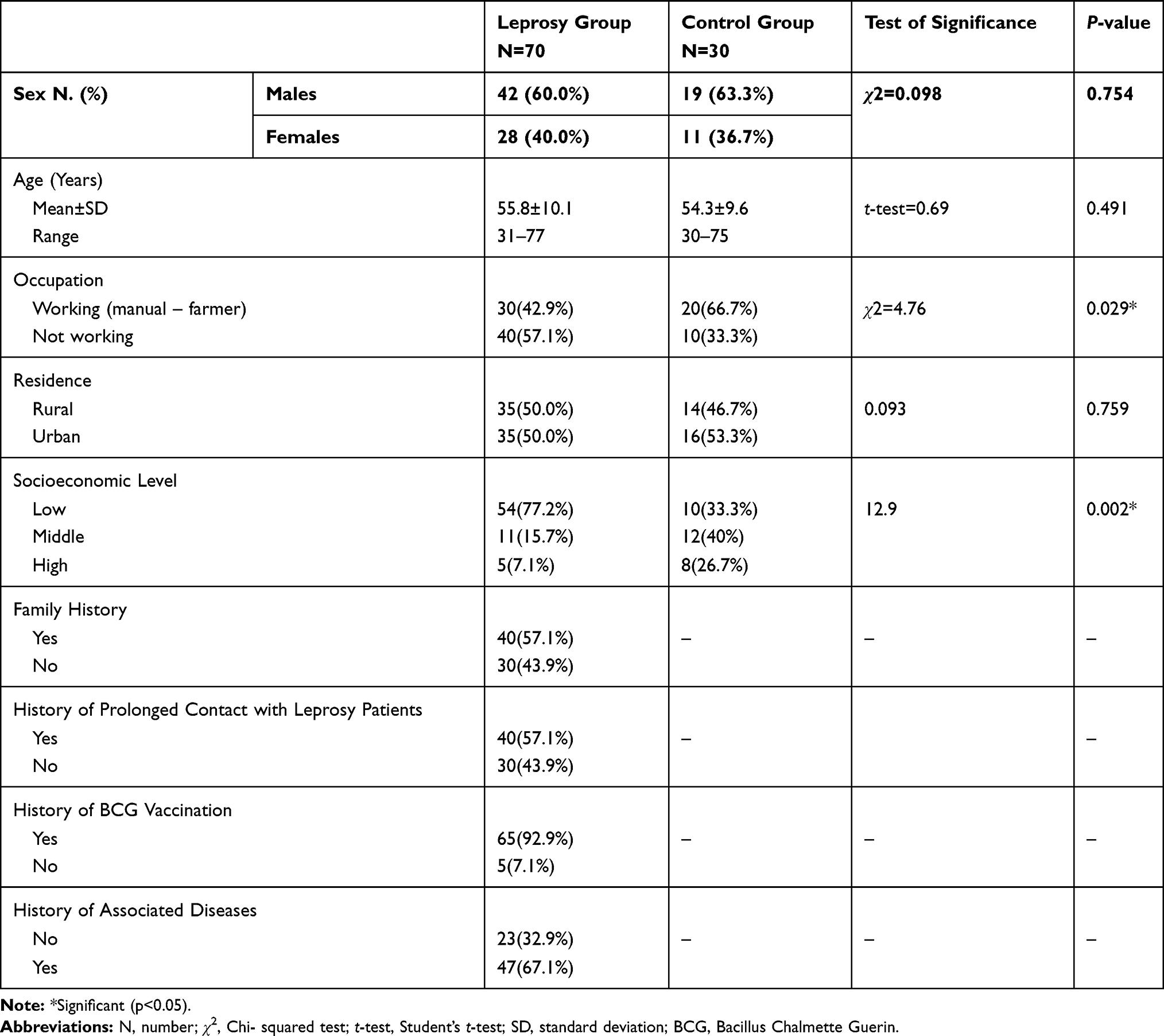 |
Table 1 Demographic and Clinical Data of Studied Subjects |
CBC, Serum sCD163 and mCD163 Positive Monocytes in Studied Subjects
Regarding CBC, WBCs and platelet counts were significantly lower in leprosy patients than controls (p<0.001). However, serum sCD163 and mCD163 positive monocytes were significantly higher (p<0.025 and p=0.042 respectively) (Table 2).
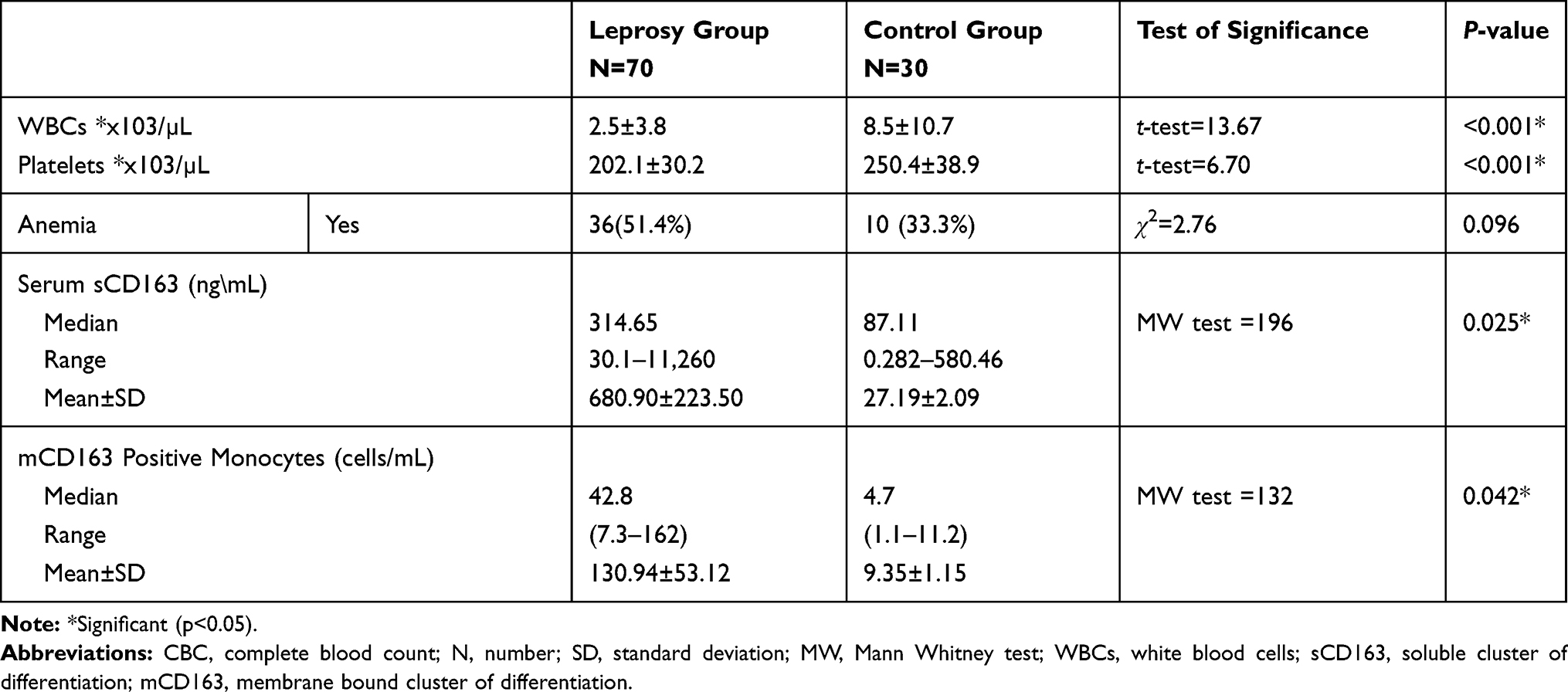 |
Table 2 Comparison Between Patients and Controls Regarding Complete Blood Count (CBC), Serum sCD163 and Flow Cytometric Assessment |
The Relation of Leprosy Types with Serum sCD163, mCD163 Positive Monocytes, and CBC
Serum sCD163 and mCD163 positive monocytes showed significant step-wise up-regulations from tuberculoid to borderline then lepromatous leprosy (p<0.001 for both). mCD163 positive monocytes were significantly higher in LL than BB and TL (p<0.001), but an insignificant difference between BB and TL was observed (p=0.1).
The decreased WBCs and platelet counts in leprosy patients were of more significant decrease in lepromatous followed by borderline then tuberculoid form (p=0.032 and p=0.024 respectively) (Table 3).
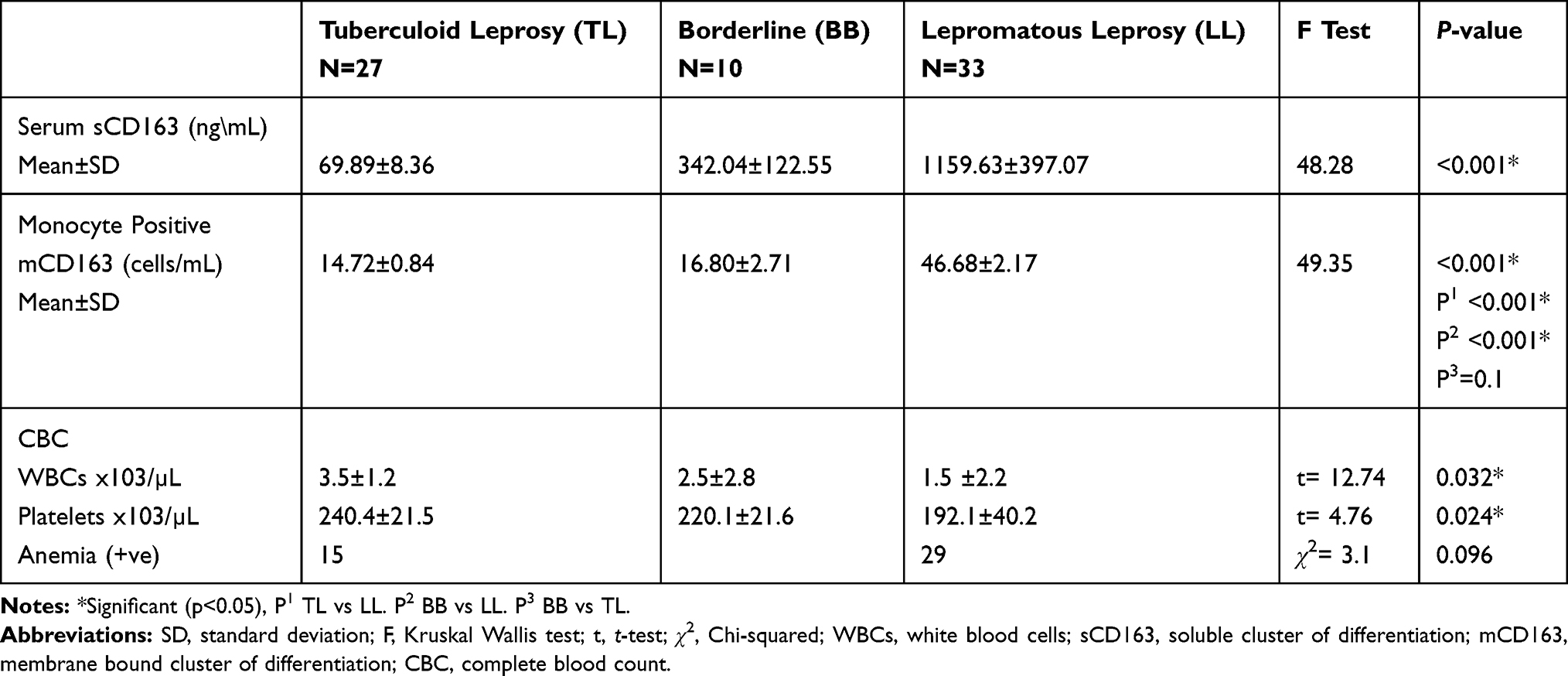 |
Table 3 Comparison Between the Studied Leprosy Types Regarding Laboratory Data |
Correlation Between mCD163 Positive Monocytes and sCD163 Serum Levels in Leprosy Patients
There was a significant positive correlation between mCD163 positive monocytes and sCD163 serum levels in the investigated leprosy patients (r=0.896, p<0.001) (Figure 2).
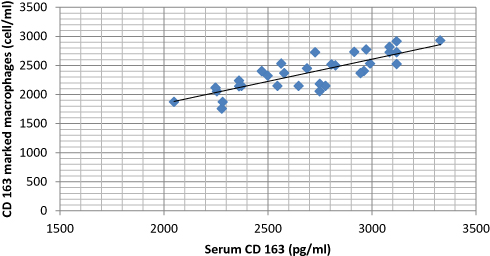 |
Figure 2 Correlation between mCD163 positive monocytes and sCD163 serum levels in leprosy patients (r=0.896, p<0.001). Abbreviations: m, membrane bound; CD, cluster of differentiation; s, soluble. |
Baseline Data in Leprosy Patients in Relation to Serum sCD163 and mCD163 Positive Monocytes
Family history, low socioeconomic level and positive history of contact with leprosy cases were significantly associated with high serum sCD163 (p=0.029, p <0.001, p=0.002 respectively) and mCD163 positive monocytes level (p <0.001, p=0.025, p=0.029 respectively) (Table 4).
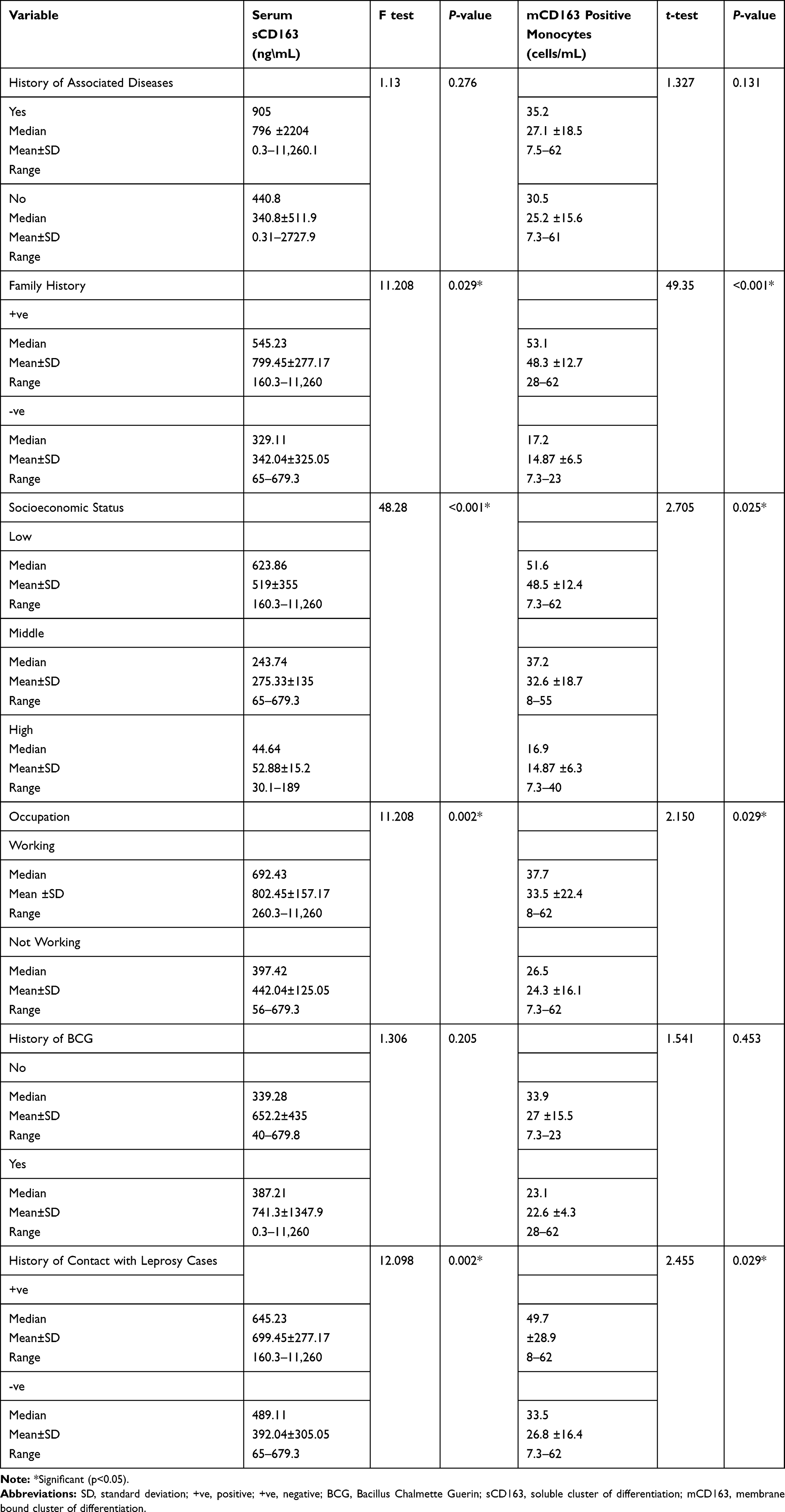 |
Table 4 Baseline Data in Leprosy Patients in Relation to Serum sCD163 and mCD163 Positive Monocytes |
Correlation Between WBCs and Platelet Counts with mCD163 Positive Monocytes and sCD163 Serum Levels in Leprosy Patients
The demonstrated low WBCs and platelet counts in our leprosy patients were negatively correlated with high serum (sCD163) and monocyte membrane bound mCD163 (P<0.001 for all) (Table 5).
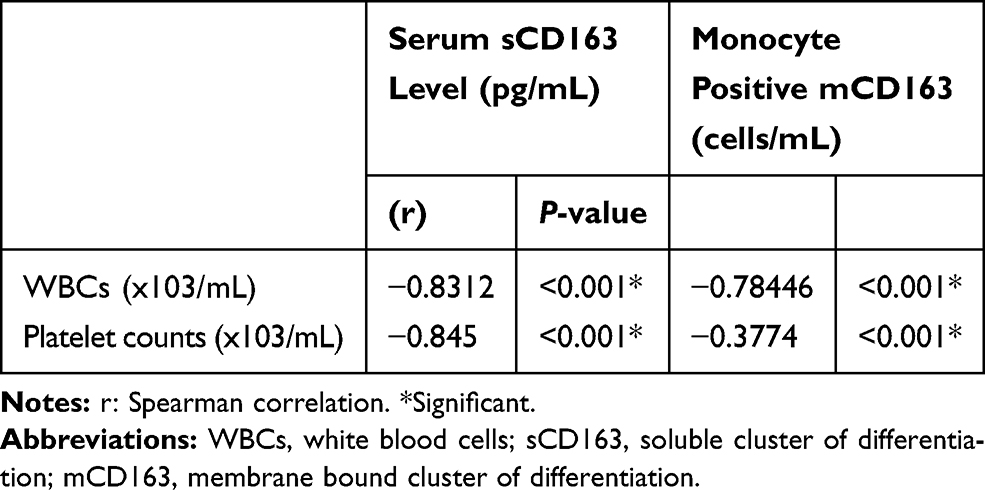 |
Table 5 Correlation Between WBCs and Platelet Counts with Serum sCD163 and mCD163 Positive Monocytes |
ROC Analysis of Serum sCD163 and mCD163 in the Leprosy Detection
sCD163 is a good positive test for leprosy detection (p<0.001), having 100.11 pg/mL best cut off value, area under the curve was 0.87, sensitivity of 92.9% and specificity was 90% (Figure 3A). Also, mCD163 is a significantly good test to diagnose leprosy as the area under the curve was 0.96, with sensitivity of 91.4% and specificity 90% and having 10.95 cells/mL as best cut off (p<0.001) (Figure 3B).
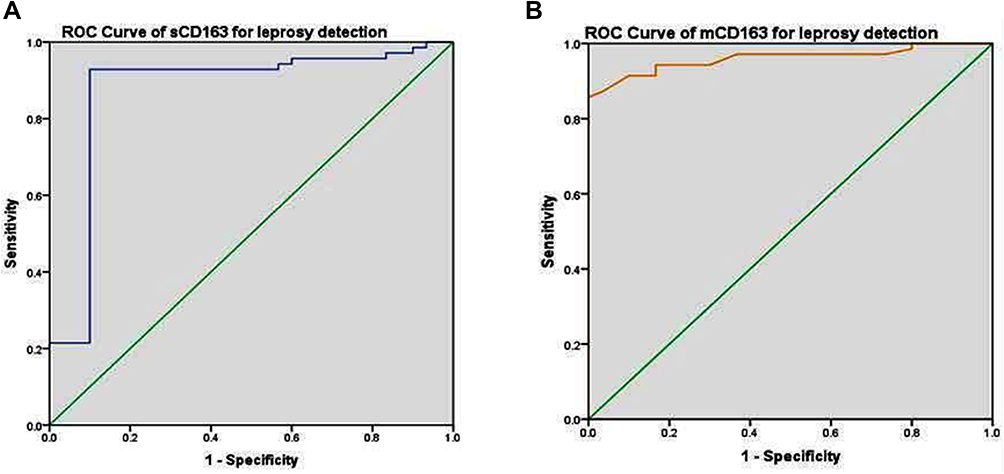 |
Figure 3 Receiver operator characteristic (ROC) curve analysis in the detection of leprosy. (A) Serum sCD163: area under the curve was 0.87, best cut off was 100.11 pg/mL, sensitivity of 92.9% and specificity of 90% (p<0.001). (B) Monocytes mCD163: area under the curve was 0.96 and best cut off was 10.95 cells/mL with sensitivity of 91.4% and specificity of 90% (p<0.001). Abbreviations: m, membrane bound; CD, cluster of differentiation; s, soluble. |
ROC Analysis of Serum sCD163 and mCD163 in the Typing of Leprosy
Both sCD163 and mCD163 are good positive indicators for lepromatous leprosy (p=0.002 and <0.001 respectively). sCD163 had area under the curve of 0.83 with 84.8% sensitivity and 80% specificity for differentiation of leprosy types with best cut off level of 379.13 pg/mL (Figure 4A). mCD163 had area under the curve of 0.93 with 87.9% sensitivity and 80% specificity for differentiation of leprosy types with best cut off level of 22.5 cells/mL (Figure 4B).
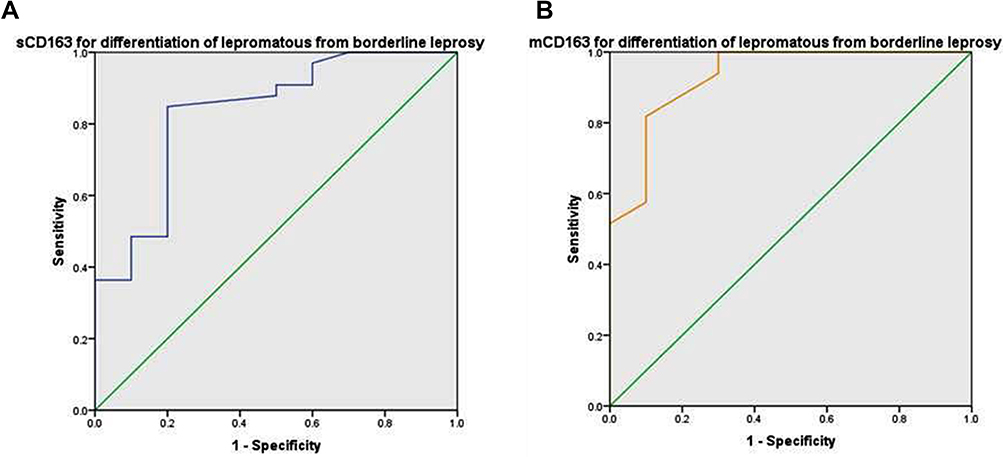 |
Figure 4 Receiver operator characteristic (ROC) curve analysis in the typing of leprosy. (A) Serum sCD163: area under the curve was 0.83 with sensitivity of 84.8% and specificity of 80% for differentiation between border-line and lepromatous leprosy types with best cut off level of 379.13 pg/mL (p =0.002). (B) Monocytes mCD163: area under the curve was 0.93 with sensitivity of 87.9% and specificity of 80% for differentiation between border-line and lepromatous leprosy types with best cut off level of 22.5 cells/mL (p<0.001). Abbreviations: m, membrane bound; CD, cluster of differentiation; s, soluble. |
Discussion
Many investigators had positive conclusions regarding the probable diagnostic value of sCD163 as a monitor of inflammatory and infectious clinical conditions.13–18 Our results demonstrated, for the first time, the clinical utility of both serum sCD163 and mCD163 measurements as simple indicators for discriminating leprosy patients from healthy ones and for leprosy disease pathogenesis and severity state.
As previously reported,20–22 our result showed detectable levels of circulating sCD163 in healthy subjects. This could be of precise interest in clinical circumstances when a patient’s sCD163 is to be serially checked during a disease or its therapeutic course.20,23
In agreement with previous information,18 we observed significant up-regulation of sCD163 and mCD163 levels in leprosy patients compared to their matched peers. Additionally, both forms of CD163 were expressively higher in LL and could differentiate LL form from other forms (TT and BL). Also, on the tissue level, Moura et al reported that CD163 mRNA was higher in LL than BL skin lesions.19
CD163 acts as a bacterial receptor leading to entry of ML into host cells.12 This hypothesis is reinforced by the fact that ML uptake was more active in CD163-transfected HEK293 cells, consequently strengthening the role of CD163 as a receptor for mycobacterial. Also, CD163 blockade was found to prevent uptake of ML by human monocytes.19
Bacterioferritins are mycobacteria secreted proteins,24,25 which are essential for iron homeostasis in these pathogens.26 As CD163 is linked to Hb clearance, high CD163 level may help in the supply of iron which is needed for survival and presence of numerous mycobacteria.27 Moura et al showed larger amount of iron in LL skin than in tuberculoid lesions.19 That could be as a result of demonstrated high CD163 in LL patients compared to TT and BL in this study.
Apart from its role in hemoglobin clearance, CD163 also has an immune-regulatory function.28 In LL, high sCD163 was positively correlated with IL-10.19 This IL-10 induces more CD163 mRNA, facilitating antigen load and adaptive immune reaction to infective agents.29
Shedding of CD163 from membranes of cultured monocytes was associated with reduced expression of its membrane bound form.8,30 Also, one human study showed that circulating sCD163 levels inversely correlate with the mCD163 concentrations in blood monocytes.31 However, in the current study we demonstrated a significant positive correlation between sCD163 serum levels and mCD163 membrane bound amounts, suggesting that the source of sCD163 may be resident tissue macrophages and not only blood monocytes.
Hematologic alterations, such as leukopenia, anemia, and thrombocytopenia were observed in MB leprosy, especially in its lepromatous form.32,33 Consistent with this data, our study revealed a significant decrease in WBCs and platelet counts in the investigated leprosy patients. These results could be a manifestation of bone marrow involvement by circulating ML, interfering with the normal bone marrow function.33
Sociodemographic risk indications of sanitation, crowding and poverty possibly increase leprosy transmission. Regarding occupation, performing manual and/or agricultural work could be associated with poverty and poor living conditions, resulting in high levels of exposure to ML and chances of leprosy development.34 Additionally, family history and prolonged contact with leprosy cases increase the chances of contracting the disease.35 Consistent with this, our findings revealed that a high percentage of the studied leprosy patients were of low socio-economic level, performed manual and agricultural work, had positive family history and prolonged contact with leprosy cases. Moreover, we observed that low socioeconomic level and contact with leprosy cases were significantly associated with high serum sCD163 and mCD163 positive monocytes, that may reflect development of severe form of leprosy (LL). Therefore, the health teams should be advised to carry out an annual clinical evaluation as well as follow-up of the cases with the highest risk. BCG vaccination for contacts with absence of leprosy signs and symptoms could be also recommended.35
Conclusion
Both sCD163 and mCD163 positive monocytes may have an active role in leprosy pathogenesis. They could be potential biomarkers for leprosy detection and typing. CD163 targeting may open the door for development of hopeful new therapeutic agents in leprosy management programs.
Acknowledgments
We are thankful to administrative and technical staff at Dermatology Clinic, Microbiology and Immunology and Pathology Departments, Faculty of Medicine, Menoufia University, Egypt, who kindly helped during this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. de Sousa JR, Pagliari C, de Almeida DS, et al. Th9 cytokines response and its possible implications in the immunopathogenesis of leprosy. J Clin Pathol. 2018;70:521–527. doi:10.1136/jclinpath-2016-204110
2. WHO Expert Committee on Specifications for Pharmaceutical Preparations. Geneva; New Delhi: World Health Organization; 2019
3. Talhari C, Talhari S, Penna GO. Clinical aspects of leprosy. Clin Dermatol. 2015;33:26–37. doi:10.1016/j.clindermatol.2014.07.002
4. Modlin RLT. innate immune response in leprosy. Curr Opin Immunol. 2010;22:48–54. doi:10.1016/j.coi.2009.12.001
5. Aarão TL, de Sousa JR, Botelho BS, Fuzii HT, Quaresma JA. Correlation between nerve growth factor and tissue expression of IL-17 in leprosy. Microb Pathog. 2016;90:64–68. doi:10.1016/j.micpath.2015.11.019
6. Aarão TL, Esteves NR, Esteves N, et al. Relationship between growth factors and its implication in the pathogenesis of leprosy. Microb Pathog. 2014;77:66–72. doi:10.1016/j.micpath.2014.10.005
7. Ritter M, Buechler C, Langmann T, Schmitz G. Genomic organization and chromosomal localization of the human CD163 (M130) gene: a member of the scavenger receptor cysteine-rich superfamily. Biochem Biophys Res Commun. 1999;260:466–474. doi:10.1006/bbrc.1999.0866
8. Hintz KA, Rassias AJ, Wardwell K, et al. Endotoxin induces rapid metalloproteinase-mediated shedding followed by up-regulation of the monocyte hemoglobin scavenger receptor CD163. J Leukoc Biol. 2002;72:711–717.
9. Frings W, Dreier J, Sorg C. Only the soluble form of the scavenger receptor CD163 acts inhibitory on phorbol ester-activated T-lympho cytes, whereas membrane-bound protein has no effect. FEBS Lett. 2002;526:93–96. doi:10.1016/S0014-5793(02)03142-3
10. Philippidis P, Mason JC, Evans BJ, et al. Hemoglobin scavenger receptor CD163 mediates interleukin 10 release and heme oxygenase-1 synthesis: anti-inflammatory monocyte-macrophage responses in vitro, in resolving skin blisters in vivo, and after cardiopulmonary bypass surgery. Circ Res. 2004;94:119–126. doi:10.1161/01.RES.0000109414.78907.F9
11. Moestrup SK, Møller HJ. CD163: a regulated hemoglobin scavenger receptor with a role in the anti-inflammatory response. Ann Med. 2004;36:347–354. doi:10.1080/07853890410033171
12. Fabriek BO, van Bruggen R, Deng DM, et al. The macrophage scavenger receptorCD163 functions as an innate immune sensor for bacteria. Blood. 2009;113:887–892. doi:10.1182/blood-2008-07-167064
13. Li J, Liu CH, Xu DL, Gao B. Significance of CD163-positive macrophages in proliferative glomer- ulonephritis. Am J Med Sci. 2015;350:387–392. doi:10.1097/MAJ.0000000000000569
14. Stilund M, Gjelstrup MC, Petersen T, et al. Biomarkers of inflammation and axonal degeneration/damage in patients with newly diagnosed multiple sclerosis: contributions of the soluble CD163 CSF/serum ratio to a biomarker panel. PLoS One. 2015;10(4):e0119681. doi:10.1371/journal.pone.0119681
15. Ab-Rahman HA, Rahim H, AbuBakar S, Wong P-F. Macrophage activation syndrome-associ- ated markers in severe dengue. Int J Med Sci. 2016;13:179–186. doi:10.7150/ijms.13680
16. Mendonca VR, Luz NF, Santos NJ, et al. Association between the haptoglobin and heme oxygenase 1 genetic profiles and soluble CD163 in susceptibility to and severity of human malaria. Infect Immun. 2012;80:1445–1454. doi:10.1128/IAI.05933-11
17. Lastrucci C, Benard A, Balboa L, et al. Tuberculosis is associated with expansion of a motile, permissive and immunomodulatory CD16+ monocyte population via the IL-10/STAT3 axis. Cell Res. 2015;25(12):1333–1351. doi:10.1038/cr.2015.123
18. Silva RL, Santos MB, Almeida PL, et al. sCD163 levels as a biomarker of disease severity in leprosy and visceral leishmaniasis. PLOS. 2017;11(3):e0005486.
19. Moura DF, de Mattos KA, Amadeu TP, et al. CD163 favors Mycobacterium leprae survival and persistence by promoting anti-inflammatory pathways in lepromatous macro- phages. Eur J Immunol. 2012;42:2925–2936. doi:10.1002/eji.201142198
20. Moller HJ, Aerts H, Gronbaek H, et al. Soluble CD163: a marker molecule for monocyte/macrophage activity in disease. Scand J Clin Lab Invest Suppl. 2002;62(7):29–33. doi:10.1080/003655102762377466
21. Moller HJ, Peterslund NA, Graversen JH, Moestrup SK. Identification of the hemoglobin scavenger receptor/CD163 as a natural soluble protein in plasma. Blood. 2002;99(1):378–380. doi:10.1182/blood.V99.1.378
22. Moller HJ, Petersen PH, Rejnmark L, Moestrup SK. Biological variation of soluble CD163. Scand J Clin Lab Invest. 2003;63(1):15–21. doi:10.1080/00365510310000439
23. Moller HJ, de Fost M, Aerts H, Hollak C, Moestrup SK. Plasma level of the macrophage-derived soluble CD163 is increased and positively correlates with severity in Gaucher’s disease. Eur J Haematol. 2004;72:135–139. doi:10.1046/j.0902-4441.2003.00193.x
24. Pessolani MC, Smith DR, Rivoire B, et al. Purification, characterization, gene sequence, and significance of a bacterioferritin from Mycobacterium leprae. J Exp Med. 1994;180:319–327. doi:10.1084/jem.180.1.319
25. Gupta V, Gupta RK, Khare G, Salunke DM, Tyagi AK. Crystal structure of Bfr A from Mycobacterium tuberculosis: incorporation of selenomethionine results in cleavage and demetallation of haem. PLoS One. 2009;4:e8028. doi:10.1371/journal.pone.0008028
26. Barry CE
27. Quadri LEN, Ratledge C. Iron metabolism in the tubercle bacillus and other mycobacteria. In: Cole ST, Eisenach KD, McMurray DN, Jacobs WRJ, editors. Tuberculosis and the Tubercle Bacillus. ASM Press, Washington, District of Columbia; 2005:341–357.
28. Zuwała-Jagiełło J. Haemoglobin scavenger receptor: function in relation to disease. Acta Biochim Pol. 2006;53(2):257–268. doi:10.18388/abp.2006_3338
29. Mocellin S, Panelli MC, Wang E, Nagorsen D, Marincola FM. The dual role of IL‐10. Trends Immunol. 2003;24:36–43. doi:10.1016/S1471-4906(02)00009-1
30. Sulahian TH, Pioli PA, Wardwell K, Guyre PM. Cross-linking of FcγR triggers shedding of the hemoglobin haptoglobin scavenger receptor CD163. J Leukoc Biol. 2004;76(1):271–277. doi:10.1189/jlb.1003523
31. Davis BH, Zarev PV. Human monocyte CD163 expression inversely correlates with soluble CD163 plasma levels. Cytometry B Clin Cytom. 2005;63:16–22. doi:10.1002/cyto.b.20031
32. Halim NKD, Ogbeide E. Haematological alteration in Leprosy patients treated with dapsone. East Afr Med J. 2002;79(2):100–102. doi:10.4314/eamj.v79i2.8912
33. BINITHA MP, SARITHA SN, RIYAZ N, MARY V. Pancytopenia due to lepromatous involvement of the bone marrow: successful treatment with multidrug therapy. Lepr Rev. 2013;84:145–150.
34. Majumder N. Socio-economic and health status of leprosy affected person: a study in Jharkhand. Indian J Lepr. 2015;87(3):145–154.
35. Rodrigues TSV, Gomes LC, Cortela DCB, Silva EA, Silva CAL. Factors associated with leprosy in children contacts of notified adults in an endemic region of Midwest Brazil. J Pediatr (Rio J). 2019. doi:10.1016/j.jped.2019.04.004
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.