Back to Journals » Pharmacogenomics and Personalized Medicine » Volume 14
Relationship Between Interleukin-6 −174G/C Genetic Variant and Efficacy of Methotrexate Treatment in Psoriatic Arthritis Patients
Authors Sokolik R ![]() , Iwaszko M, Świerkot J
, Iwaszko M, Świerkot J ![]() , Wysoczańska B, Korman L, Wiland P, Bogunia-Kubik K
, Wysoczańska B, Korman L, Wiland P, Bogunia-Kubik K
Received 26 May 2020
Accepted for publication 11 November 2020
Published 28 January 2021 Volume 2021:14 Pages 157—166
DOI https://doi.org/10.2147/PGPM.S264555
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin Bluth
Renata Sokolik,1,* Milena Iwaszko,2,* Jerzy Świerkot,1 Barbara Wysoczańska,2 Lucyna Korman,1 Piotr Wiland,1 Katarzyna Bogunia-Kubik2
1Department of Rheumatology and Internal Medicine, Wrocław Medical University, Wrocław, Poland; 2Laboratory of Clinical Immunogenetics and Pharmacogenetics, Hirszfeld Institute of Immunology and Experimental Therapy, Polish Academy of Sciences, Wrocław, Poland
*These authors contributed equally to this work
Correspondence: Milena Iwaszko
Hirszfeld Institute of Immunology and Experimental Therapy, Polish Academy of Sciences, Weigla 12, Wrocław 53-114, Poland
Tel +48 71 3709960
Fax +48 71 3371382
Email [email protected]
Introduction: The purpose of the study was to investigate whether single-nucleotide polymorphisms (SNPs) IL-6 − 174 G/C and IL-6R Asp358Ala are associated with susceptibility to psoriatic arthritis (PsA) or affect response to treatment with methotrexate (MTX).
Patients and Methods: Seventy-four patients diagnosed with PsA and qualified for MTX treatment were enrolled to the study. The control group consisted of 120 healthy individuals. Polymorphisms IL-6 − 174 G/C and IL-6R Asp358Ala were genotyped using a polymerase chain reaction (PCR) amplification employing LightSNiP assays.
Results: A significant association between the IL-6 − 174 CC genotype and an improved clinical outcome of MTX therapy was observed. A good response was more frequently observed among PsA patients bearing the IL-6 − 174 CC genotype than patients with the GC or GG genotypes (P = 0.007). On the other hand, patients carrying the IL-6 − 174 GC genotype less frequently responded to MTX treatment as compared to patients with other genotypes (P = 0.006). With respect to the IL-6R Asp358Ala SNP, there were no significant differences in genotype and allelic frequencies in relation to clinical outcome of MTX treatment. No association was found between the IL-6 − 174 G/C or IL-6R Asp358Ala SNPs and PsA susceptibility.
Conclusion: Results from this study provide evidence that the IL-6 − 174 G/C polymorphism might influence efficacy of MTX treatment.
Keywords: psoriatic arthritis, methotrexate treatment, IL-6 − 174G/C polymorphism, IL-6R Asp358Ala polymorphism
Plain Language Summary
Psoriatic arthritis (PsA) is a disease caused by the immune system attacking its own tissues. PsA is a form of inflammatory arthritis and it affects joints as well as skin.
A first-line drug for a treatment of PsA is methotrexate (MTX). This drug can be very effective on some, however a substantial group of patients responds to the therapy partially or not at all.
The exact cause of PsA is not known, but it is well established that a genetic background plays an important role in the disease development.
Also, it is supposed that genetic factors may influence response to the PsA treatment.
The aim of this research was to investigate whether changes in genes encoding the interleukin-6 (IL-6) and interleukin-6 receptor (IL-6R) might have an effect on the response to MTX in PsA patients. Two variants within these genes were selected: IL 6 −174 G/C in the IL-6 gene and IL-6R Asp358Ala in the IL-6R gene.
Interleukin-6 belongs to a group of small proteins called cytokines. Cytokines are produced by numerous immune system cells and are important in the regulation of immunity and inflammation.
The research was performed on 74 PsA patients treated with MTX.
The results showed that patients with the C variant of the IL-6 −174 G/C gene responded significantly better to the therapy with MTX.
This study showed that the IL-6 −174 G/C genetic variant could affect the response to MTX in PsA patients.
Introduction
Psoriatic arthritis (PsA) is a multifactorial chronic inflammatory disease manifested by joint inflammation and cutaneous psoriasis.
The precise etiology of PsA remains unknown, however both genetic and environmental factors contribute to development of this immune-mediated disease. Twin and family studies demonstrated strong heritability of PsA and pointed to a strong genetic component underlying the etiology of this disease.1 Conventional synthetic disease modifying anti-rheumatic drugs (csDMARDs), including methotrexate (MTX), constitute the first line therapy for PsA. This immunomodulatory agent is one of the most commonly prescribed medications for this disorder, however patients display variable responses to treatment.2,3 Although the exact mechanism of action of MTX in the context of PsA is not completely understood, it has been reported that therapy with this drug results in decreased production of interleukin-6 (IL-6).4,5
Interleukin-6 is a multifunctional cytokine characterized by a broad range of biologic activities, comprising immune regulation, inflammation and oncogenesis.6 Synthesis of acute-phase protein7 and transition between acute and chronic inflammation is stimulated by IL-6.8 Also, this cytokine exerts an effect on bone metabolism and mediates bone resorption through stimulation of osteoclast cell formation.9 Moreover, IL-6 is associated with increased vascular endothelial growth factor (VEGF) expression, leading to pannus development. In addition, IL-6 is involved in inflammatory process by inducing differentiation of activated B cells into antibody-producing cells, differentiation of CD8+ T cells into cytotoxic T cells and by playing a crucial role in Th17 development. The IL-6 interacts with its specific interleukin-6 receptor (IL-6R) and the IL-6-IL-6R complex associates with glycoprotein 130 subunits (gp130), leading to activation of signaling cascade.10 The receptors for IL-6 exist as soluble as well as membrane-bound forms. Signaling through soluble IL-6R, called the trans-signaling pathway, is responsible for pro-inflammatory activities of IL-6. On the other hand, the pathway via the membrane-bound IL-6R, known as classic-signaling, mediates anti-inflammatory and regenerative properties of this cytokine.11
The production of IL-6 protein might be partially determined on the genetic level by polymorphisms located within the promoter region of its gene. The IL-6 −174 polymorphism has been implicated in the regulation of the IL-6 levels. This SNP consists of a G to C substitution at position −174 in the promoter region of the IL-6 gene. The G allele has been associated with increased transcriptional activity and higher levels of IL-6 in in vitro and in vivo studies.12 The IL-6R Asp358Ala has also been demonstrated to affect levels of circulating soluble IL-6 receptor (sIL-6R).13 It has been established that the IL-6R C allele is associated with increased sIL-6R levels. The presence of the IL-6R CC genotype correlated with higher sIL-6R concentrations in patients diagnosed with asthma, diabetes as well as coronary heart disease.14–17 Moreover, healthy individuals carrying the IL-6R C allele displayed substantially increased sIL-6R levels.14,15,18 The relevance of the IL-6 −174 polymorphism in pathogenesis of autoimmune disorders was examined in numerous studies. However, this polymorphism has not been widely studied in the context of its potential impact on PsA pathogenesis and only two studies regarding the role of this SNP in context of the disease exist. To date, there are also no studies evaluating a possible role of functional interleukin-6 receptor (IL-6R) Asp358Ala (rs2228145) polymorphism in PsA pathology. A brief summary of studies performed to date regarding associations of these polymorphisms and arthritis as well as dermal diseases can be found in Table 1.
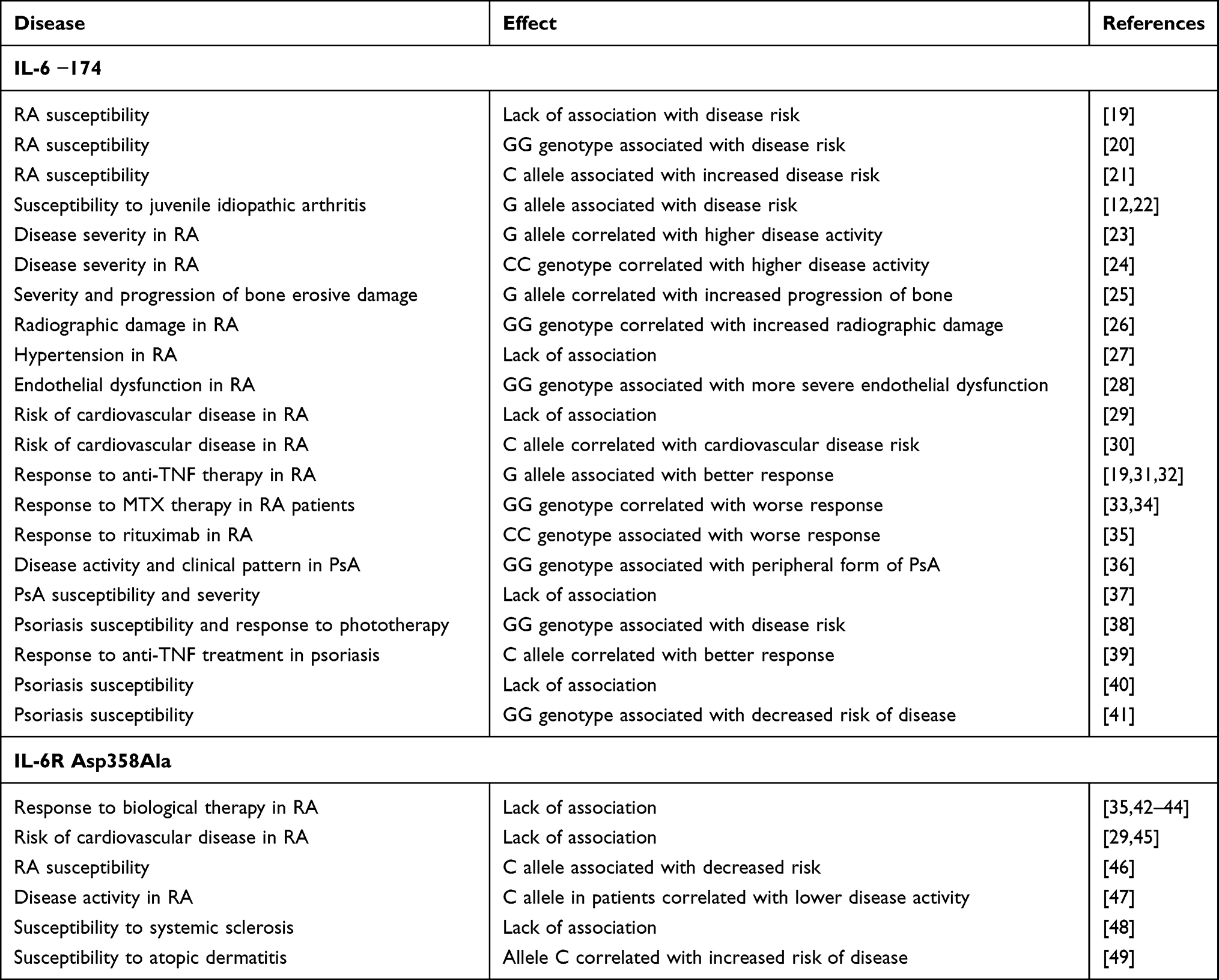 |
Table 1 Summary of Studies Performed Up to Date in Regard to Associations of the IL-6 −174 G/C and IL-6R Asp358Ala Polymorphisms and Arthritis as Well as Dermal Diseases |
The objective of this study was to investigate whether single-nucleotide polymorphisms (SNPs) IL-6 −174 G/C (rs1800795) and IL-6R Asp358Ala (rs2228145) are associated with susceptibility to PsA or affect response to treatment with MTX.
Methods
Patients
In total, 74 patients with PsA from the Department of Rheumatology and Internal Medicine of Wroclaw Medical University were included in the study. All the patients were diagnosed with PsA according to the Classification Criteria for Psoriatic Arthritis (CASPAR) and were naïve to MTX or other csDMARDs. The control group consisted of 120 age and gender matched healthy blood donors without any family history of autoimmune disorders. All the participants were of Caucasian ancestry.
Demographic data and complete medical history were collected from each patient. The clinical and laboratory evaluation included a count of swollen and tender joints (SJC and TJC, respectively), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), rheumatoid factor (RF), visual analogue scale (VAS; range, 0 to 100 mm) of pain, health assessment questionnaire (HAQ), global health assessment by the patient and the physician. Disease activity was measured using disease activity score (DAS28). Psoriasis severity was assessed using the psoriasis area severity index (PASI).
Criteria excluding patients from this study comprised of: age below 18; coexistence of other systemic diseases of connective tissue besides PsA; clinically significant impairment of hepatic and renal function; infections with hepatotropic viruses; infections resistant to therapy; ongoing history of cancer or uncontrolled diabetes; alcohol abuse; pregnancy or breastfeeding; prior treatment with csDMARDs or biologic agents; insufficient clinical records; unwillingness or inability to cooperate.
The main characteristics of patients are summarized in Table 2. Thirty-one subjects were females and the mean ± SD age of the patients was 46.0 ± 10.9 years. PsA was classified as oligoarticular in 12 patients and polyarticular in 62 patients. All the patients were negative for rheumatoid factor. The mean age at the onset of psoriasis was 29.4 ± 14.2 years. Mean age at PsA onset was 37.5 ± 12.1 years. Fifty-four patients had type 1 psoriasis, the rest had type 2 psoriasis.
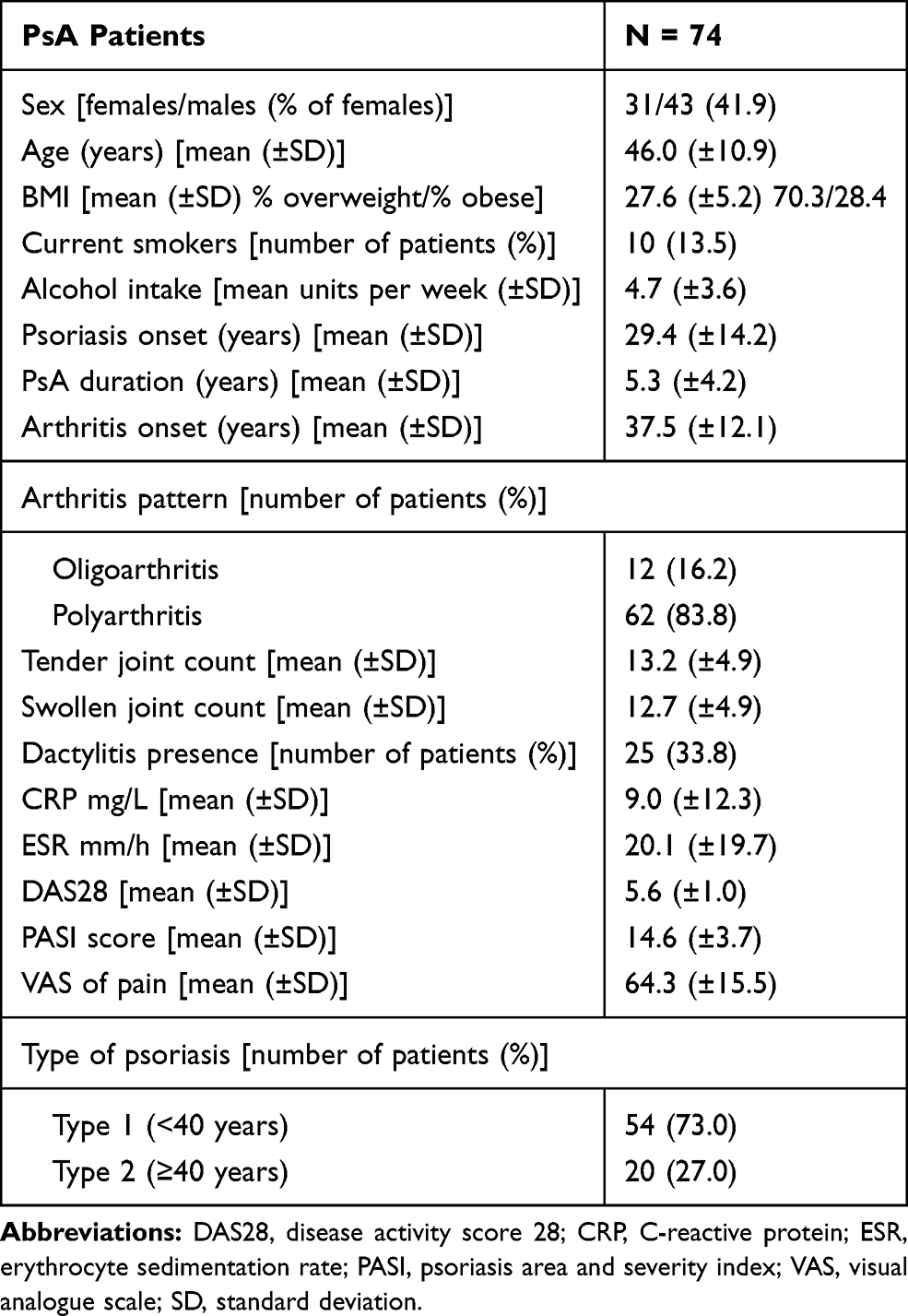 |
Table 2 Demographic and Clinical Characteristics of the Study Subjects |
The patients were administered with MTX dose of 25 mg/week orally. All the patients supplemented folic acid dose of 10 mg/week during treatment. Efficacy of MTX treatment was evaluated using the American College of Rheumatology definition of 20% improvement (ACR20).50 Patients were considered as ACR20 responders when they achieved an improvement of at least 20% in both tender and swollen joint counts (TJC and SJC), as well as at least 20% improvement in 3 of the 5 following measures: the physician’s global assessment of disease activity, the patient’s global assessment of the disease activity, the patient’s functional ability assessment and acute-phase reactant value (CRP). As a secondary outcome measure, psoriatic arthritis response criteria (PsARC) were employed. These criteria comprise of: TJC, SJC (assessing 68 and 66 joints, respectively, including distal interphalangeal joints of hands and feet), PtGA, and PhGA. Improvement by at least 30% in at least 2 of 4 measurements, one of which had to be a joint count, without decrease in any measurement, was defined as a positive outcome of therapy.51,52 In addition, Dactylitis Severity Score (DSS) was also used as a secondary outcome measure. Each digit with dactylitis was classified in accordance to a four level scale from 0 to 3 (0 = no dactylitis, 1 = mild dactylitis, 2 = moderate dactylitis, 3 = severe dactylitis), where scores greater than 0 indicate a presence of dactylitis and a total score was calculated as a sum of scores for all 20 digits.
The study was approved by Wrocław Medical University Ethics Committee and written informed consents were obtained from all participants. The study was conducted in accordance with the Declaration of Helsinki.
IL-6 and IL-6R Genotyping
For the present study the selection of genetic variants within the IL-6 as well as IL-6R genes was based on available literature analysis as well as search results from HapMap and NCBI dbSNP databases. Information regarding predicted functional consequences of SNPs was obtained using SNPinfo Web Server.53 Studied SNPs were characterized with minor allele frequencies above 10% (1000 Genomes Project).54
Genomic DNA was isolated from peripheral blood taken on EDTA using Maxwell 16 Blood DNA Purification Kit (Promega Corp., Madison, WI, USA) following the instruction of the manufacturer.
The IL-6 −174 G/C (rs1800795) and IL-6R Asp358Ala (rs2228145) genetic variants were determined by real-time polymerase chain reaction (PCR) amplifications and melting-curve analysis using LightSNiP typing assay (TIB-MolBiol, Berlin, Germany). The real-time PCRs were carried out on a LightCycler 480 Real-Time PCR system (Roche Applied Science, Mannheim, Germany) in accordance to the manufacturer’s recommendations. The reagents used for each reaction included 1.6 μL MgCl2, 14.4 μL H2O, 1 μL of LightSNiP reagent mix (containing premixed primers and probes specific for each variant; designed and manufactured by TIB Molbiol) and 2 μL of FastStart DNA Master HybProbe (Roche Diagnostics), which were set up in a final volume of 20 μL containing 1 μL of DNA solution. The cycling conditions were as follows: initial denaturation at 95 °C for 10 minutes, followed by 45 cycles of denaturation at 95 °C for 10 seconds, annealing at 60 °C for 10 seconds, and extension at 72 °C for 15 seconds. Fluorescence was assessed at the end of each annealing phase. The melting curve analysis of the amplification products was performed at 95 °C for 30 seconds, 40 °C for 2 minutes, and 75 °C with a ramp of 1.5 °C/s and continuous acquisition of data.
Statistical Analysis
Genotype frequencies in cases and controls were tested for Hardy–Weinberg equilibrium using Population Genetics package for R. Means and standard deviations were calculated for continuous data and proportions for categorical ones. Comparisons between nonparametric variables were performed using the Mann–Whitney U-test. Fishers exact test was used to compare categorical variables. A p value < 0.05 was considered statistically significant. All statistical calculations were performed with R software environment (version 3.2.3; x86_64-pc-linux-gnu).55
Results
Genotype and Allele Frequencies of the IL-6 −174 G/C and IL-6R Asp358Ala Polymorphisms in PsA Patients and Healthy Individuals
The genotype and allele frequencies of the IL-6 −174 G/C and IL-6R Asp358Ala polymorphisms observed in patients and controls are presented in Table 3.
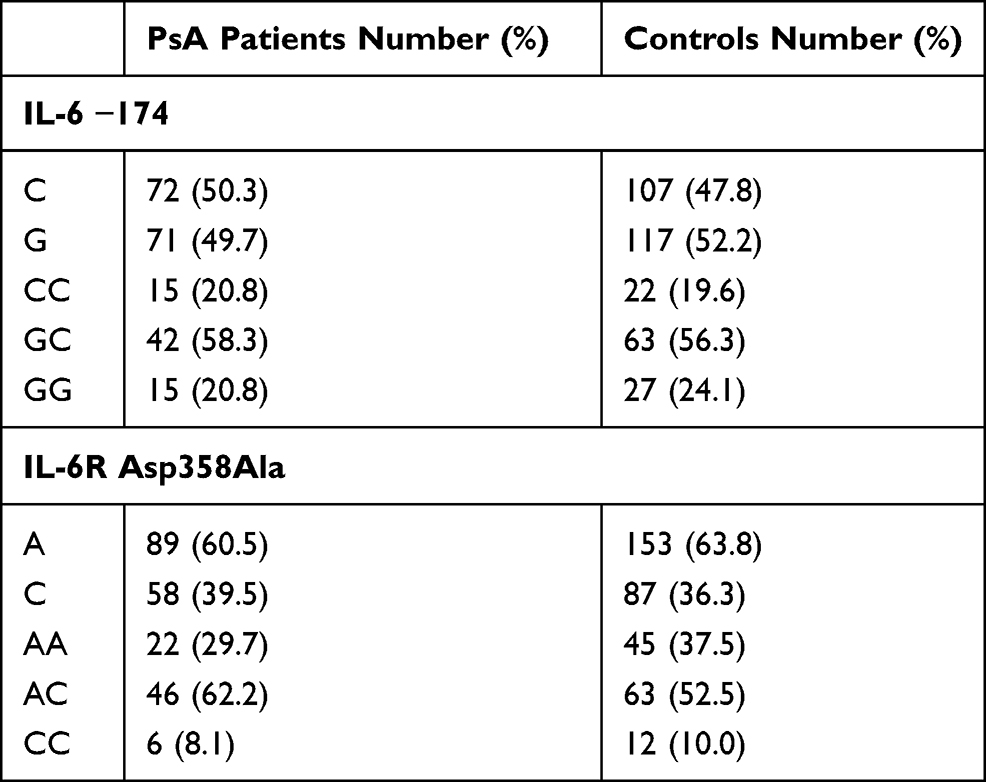 |
Table 3 The IL-6 −174 G/C and IL-6R Asp358Ala Genotypes and Alleles Frequencies in PsA Patients and Healthy Subjects |
Distribution of the genotypes and alleles of the IL-6 −174 G/C and IL-6R Asp358Ala polymorphisms among patients and controls were in agreement with the Hardy–Weinberg equilibrium.
The frequencies of the IL-6 −174 CC, IL-6 −174 GC, and IL-6 −174 GG genotypes within the patient group were 20.8%, 58.3%, and 20.8%, respectively, and 19.6%, 56.3%, 24.1%, respectively, in the control group. The genotype and allele frequencies of the IL-6 −174 G/C polymorphism did not differ between PsA patients and healthy controls.
With respect to the IL-6R Asp358Ala SNP, the frequencies of the AA, AC, and CC genotypes were 29.7%, 62.2%, and 8.1%, respectively, within the patient group, and 37.5%, 52.5%, 10.0%, respectively, in the control group. There were no significant differences between distribution of the IL-6R Asp358Ala genotypes and alleles in PsA patients and controls.
Analysis of Clinical Features of PsA Patients in Relation to the IL-6 −174 G/C and IL-6R Asp358Ala Genetic Variants
The relationships of the IL-6 −174 G/C and IL-6R Asp358Ala genetic variants with baseline clinical parameters, including DAS28, CRP, ESR, TJC, SJC, and pain intensity, as well as presence of dactylitis, were examined and their results are shown in Table 4.
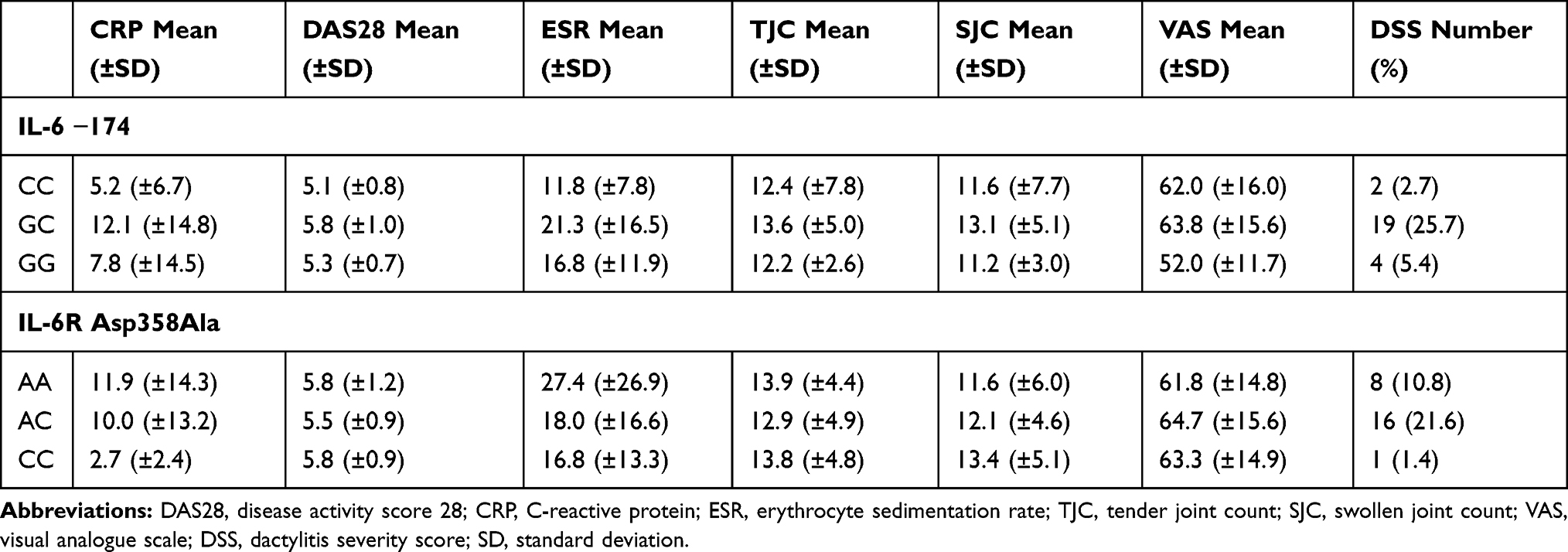 |
Table 4 Clinical Features at Baseline According to the IL-6 −174 G/C and IL-6R Asp358Ala Genotypes and Alleles Distribution of PsA Patients |
The genotype and allele frequencies of the IL-6 −174 G/C polymorphism did not differ between PsA patients with respect to CRP or ESR level. No significant association between the IL-6 −174 G/C polymorphism and DAS28 was also observed. No significant differences were also observed in TJC, SJC, PASI score or pain intensity with respect to genotypes and alleles of the IL-6 −174 G/C. Similarly, no relations between studied polymorphisms and presence of dactylitis were found.
Considering the IL-6R Asp358Ala polymorphism, there were no differences in genotype and allele distributions among PsA patients concerning CRP or ESR level. No correlation between the IL-6R Asp358Ala polymorphism and TJC, SJC or pain intensity has been observed. The analysis also revealed no statistically significant differences between DAS28 score or presence of dactylitis and the IL-6R Asp358Ala genetic variant.
Relationships Between the IL-6 −174 G/C and IL-6R Asp358Ala Gene Polymorphisms and Clinical Outcome of Treatment with MTX
The clinical outcome of MTX treatment with respect to the IL-6 −174 G/C and IL-6R Asp358Ala genetic variants is presented in Tables 5 and 6.
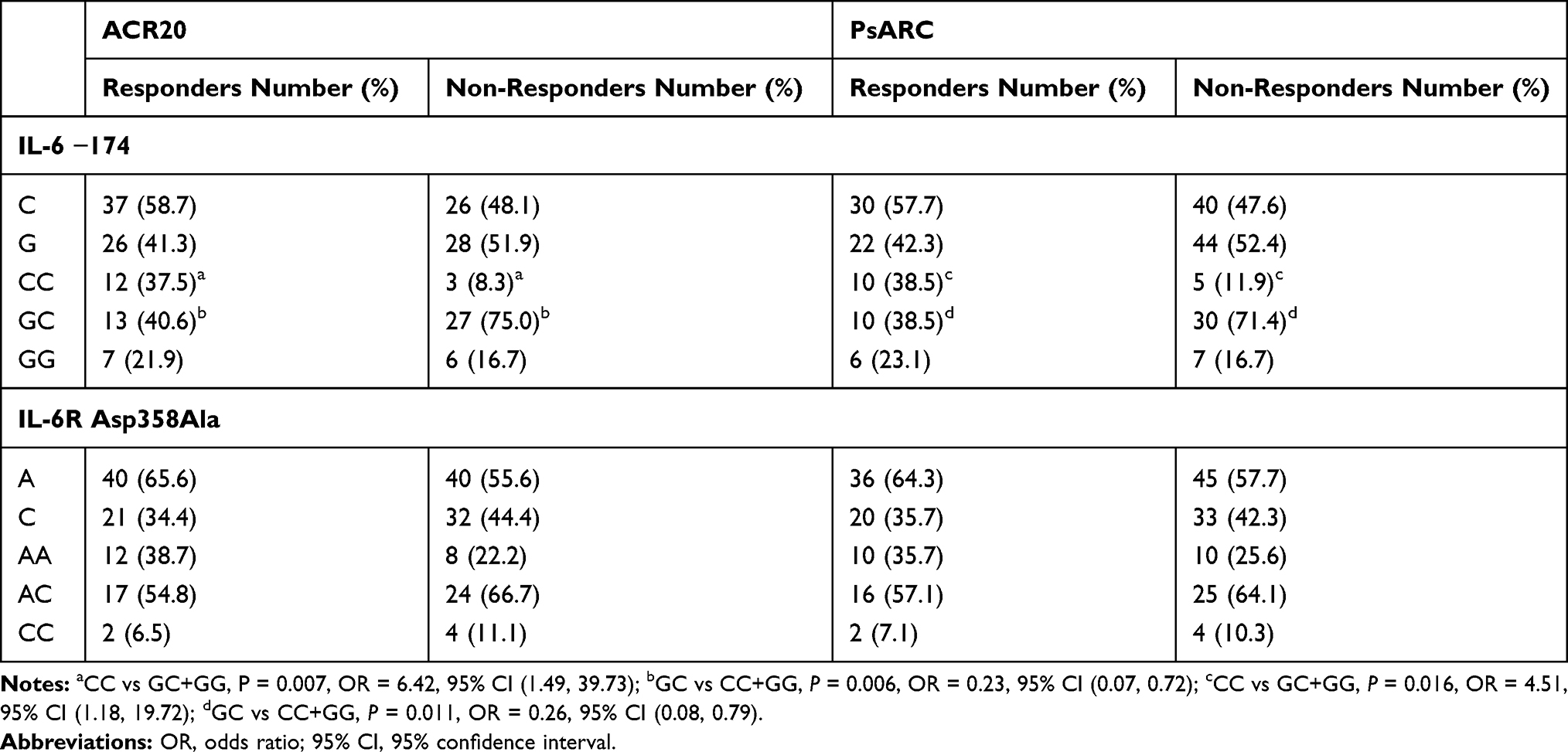 |
Table 5 Genotypes and Alleles Frequencies of the IL-6 −174 G/C and IL-6R Asp358Ala Polymorphisms in Psoriatic Arthritis Patients in Relation to Response in Accordance to the ACR20 and PsARC Criteria |
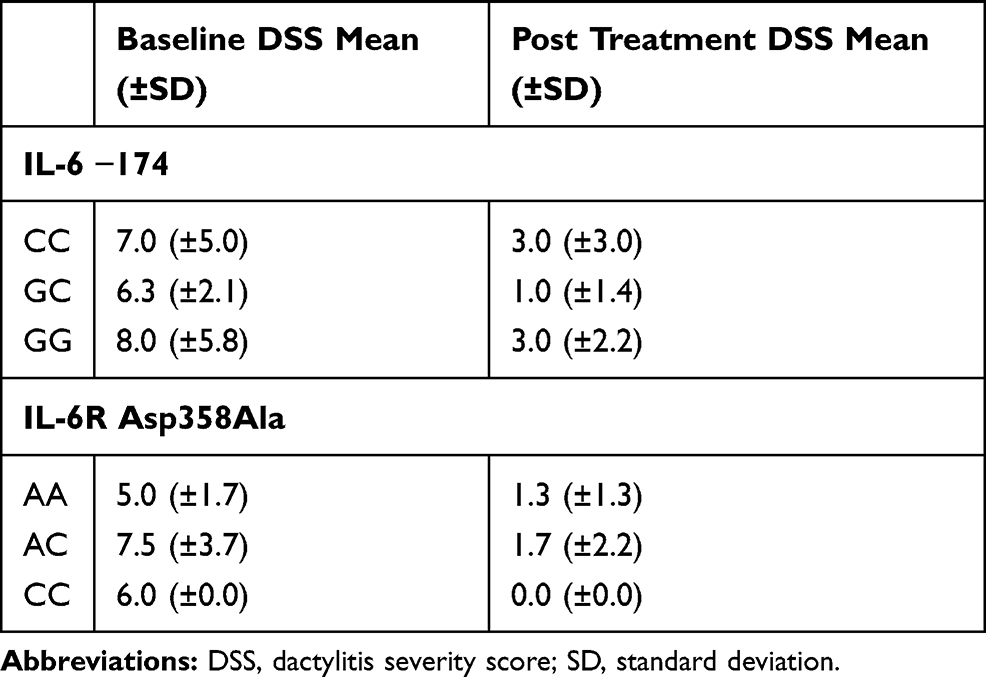 |
Table 6 Genotypes Frequencies of the IL-6 −174 G/C and IL-6R Asp358Ala Polymorphisms in Psoriatic Arthritis Patients in Relation to Response Assessed by the Dactylitis Severity Score |
There was a significant association between the IL-6 −174 G/C polymorphism and efficacy of MTX therapy. A response to MTX in accordance to the ACR20 criteria was more frequently observed among patients bearing the IL-6 −174 CC genotype than in patients with the IL-6 −174 GC or GG genotypes (P = 0.007; OR = 6.42; 95% CI = (1.49, 39.73)). On the other hand, patients carrying the IL-6 −174 GC genotype responded less frequently to MTX treatment, as judged by the ACR20 criteria and compared to patients with the IL-6 −174 CC or GG genotypes (P = 0.006; OR = 0.23; 95% CI (0.07, 0.72)). Similar, though less significant, trends were observed when a response to MTX was classified by the PsARC criteria. Patients with the IL-6 −174 CC genotype were more frequent among responders’ group in comparison to other genotypes (P = 0.016; OR = 4.51; 95% CI (1.18, 19.72)). Also, patients carrying the IL-6 −174 GC genotype responded to the treatment in accordance to the PsARC classification less frequently than other patients (P = 0.011; OR = 0.26; 95% CI (0.08, 0.79)). No associations have been observed between the studied polymorphisms and response to MTX measured as the dactylitis severity score.
With respect to the IL-6R Asp358Ala polymorphism, there were no significant differences in genotype and allelic frequencies in relation to response to MTX treatment.
Discussion
The IL-33 cytokine plays a crucial role in development of persistent inflammation, acting as a potent mediator of an inflammatory response. The IL-6 is involved in the pathogenesis of rheumatoid arthritis (RA) and psoriasis, disorders that share common pathobiology with PsA. The pathological role of IL-6 in RA development has been highlighted by studies conducted on murine arthritis models. Blockade of IL-6 signaling by gene knockout or administration of anti-IL-6 or anti-IL-6R antibodies leads to suppression of the disease development.56–58 This beneficial effect has been confirmed on human organisms, resulting in the introduction of a humanized anti-IL-6 receptor monoclonal antibody Tocilizumab as a novel drug in RA therapy. Levels of circulating IL-6 are elevated both in RA and psoriasis as well as in numerous other autoimmune and chronic inflammatory diseases. It suggests that deregulation of signaling pathways mediated by IL-6 may contribute to autoimmune pathology.
The obtained results revealed an association of the IL-6 −174 G/C polymorphism with clinical outcome in PsA patients treated with MTX. Individuals carrying the IL-6 −174 G allele responded less effectively to the therapy than those with the IL-6 −174 CC genotype. These observations are in agreement with studies reporting an association of the IL-6 −174 G/C polymorphism with RA. The IL-6 −174 GG genotype was more common in RA patients displaying increased radiographic damage.26 Also, the IL-6 −174 G allele was associated with susceptibility to juvenile RA and presence of the IL-6 −174 GG genotype correlated with higher pain scores in JIA patients.12
In accordance to our knowledge, only two studies to date investigated the possible impact of the IL-6 −174 G/C polymorphism in context of PsA.36,37 In the study performed by Cubino et al the IL-6 −174 GG genotype was associated with a peripheral form of PsA.36 However, in a study conducted by Balding et al no associations were observed, neither with disease susceptibility, nor clinical characteristics.37 With respect to the possible influence of the IL-6 −174 G/C genetic variant on MTX efficacy, no study involving PsA patients has been performed to date. However, two groups examined the association of the IL-6 −174 G/C polymorphism with efficacy of the MTX treatment in patients with RA.33,34 Pawlik et al reported significantly worse response to MTX therapy among patients possessing the IL-6 −174 GG genotype.33 In addition, in a study by Ruiz et al the IL-6 −174 GG genotype was associated with a higher risk of failure in therapeutic response to MTX or leflunomide (lef).34 However, after stratifying patients’ groups in accordance to MTX or lef, a significant association was observed only in patients treated with lef.
The results of the present study are concordant with previous reports concerning the Polish population in context of the role of the IL-6 −174 G/C polymorphism in the pathogenesis of immunological disorders.23,38,40 In a study by Pawlik et al patients homozygous for the IL-6 −174 G allele were characterized with higher disease severity assessed by DAS28 score.23 Also, the IL-6 −174 GG genotype was overrepresented in patients diagnosed with psoriasis in comparison to a control group and this genotype was associated with almost a twofold increased risk of psoriasis.38 However, another study did not report any significant differences between Polish patients with psoriasis and healthy controls.42 On the other hand, the association of the IL-6 −174 GG genotype with susceptibility to psoriasis and response to anti-TNF therapy was reported by di Renzo et al.39 In line with these findings, in a study conducted by Boca et al the IL-6 −174 CC genotype was less frequent in the patients’ group and conferred protection against psoriasis.41
This polymorphism was also implicated in systemic lupus erythematosus (SLE) pathogenesis and recent meta-analysis indicated that the IL-6 −174 G allele predisposes, particularly in the European population, to SLE development.59 Furthermore, a significantly increased frequency of the IL-6 −174 GG genotype was observed in patients with diabetes mellitus.60,61 Also, the same genotype correlated with disease activity in systemic sclerosis patients.62 On the other hand, no relationships were detected between the IL-6 −174 G/C polymorphism and development of RA or type I diabetes.63 Data from the present study also did not expose any significant associations between this SNP and susceptibility to PsA.
Regarding the IL-6R Asp358Ala SNP, the results derived from the present study suggest a lack of association between this polymorphism and predisposition to PsA or response to MTX treatment. In agreement with these results, in previous studies on RA patients there were no significant relationships between the IL-6R Asp358Ala genetic variants and clinical outcome of therapy, neither with rituximab, tocilizumab, nor anti-TNF agents.35,42,43 Also, no significant correlations were detected between this SNP and susceptibility to systemic sclerosis.48 However, some studies reported an association of the IL-6R Asp358Ala allele C with increased risk of atopic dermatitis and decreased risk of RA.46,49
It should be noted that the relatively limited sample size constitutes a major limitation of the present study that could result in a statistical power insufficient to detect small or moderate effects. Therefore, further studies on larger patient cohorts are necessary to confirm findings of the present study.
In conclusion, this is the first report regarding the possible impact of IL-6 −174 G/C polymorphism on the efficacy of methotrexate treatment in PsA. The results from the present study suggest an involvement of the IL-6 −174 G/C polymorphism in pathomechanisms determining the PsA. The presence of the IL-6 −174 CC genotype among PsA patients predisposed to a favorable response to MTX therapy. With respect to the IL-6R rs2228145 polymorphism the obtained data did not reveal any significant associations with PsA susceptibility or clinical outcome of MTX treatment, indicating that this SNP may not be involved in the genetic background of PsA. However, the results demonstrated in this study require validation in larger cohorts as well as in populations of different ethnic origin.
Acknowledgments
This work was supported by the National Centre of Science (Poland) – grant no. 2016/21/B/NZ5/01901 and ST-924/2015.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rahman P, Elder JT. Genetic epidemiology of psoriasis and psoriatic arthritis. Ann Rheum Dis. 2005;64:37–39. doi:10.1136/ard.2004.030775
2. Dernis E, Lavie F, Salliot C, et al. Pharmacological treatment (biotherapy excluded) of peripheral psoriatic arthritis: development of recommendations for clinical practice based on data from the literature and experts opinion. Joint Bone Spine. 2009;76(5):524–531. doi:10.1016/j.jbspin.2009.03.002
3. Ritchlin CT, Kavanaugh A, Gladman DD, et al. Treatment recommendations for psoriatic arthritis. Ann Rheum Dis. 2009;68(9):1387–1394. doi:10.1136/ard.2008.094946
4. Kraan MC, Smeets TJ, van Loon MJ, et al. Differential effects of leflunomide and methotrexate on cytokine production in rheumatoid arthritis. Ann Rheum Dis. 2004;63:1056–1061. doi:10.1136/ard.2003.014738
5. Straub RH, Müller-Ladner U, Lichtinger T, et al. Decrease of interleukin 6 during the first 12 months is a prognostic marker for clinical outcome during 36 months treatment with disease-modifying anti-rheumatic drugs. Br J Rheumatol. 1997;36:1298–1303. doi:10.1093/rheumatology/36.12.1298
6. Assier E, Boissier MC, Dayer JM. Interleukin-6: from identification of the cytokine to development of targeted treatments. Joint Bone Spine. 2010;77:532–536. doi:10.1016/j.jbspin.2010.07.007
7. Heinrich PC, Castell JV, Andus T. Interleukin-6 and the acute phase response. Biochem J. 1990;265(3):621–636. doi:10.1042/bj2650621
8. Kaplanski G, Marin V, Montero-Julian F, Mantovani A, Farnarier C. IL-6: a regulator of the transition from neutrophil to monocyte recruitment during inflammation. Trends Immunol. 2003;24(1):25–29. doi:10.1016/S1471-4906(02)00013-3
9. Kotake S, Sato K, Kim KJ, et al. Interleukin-6 and soluble interleukin-6 receptors in the synovial fluids from rheumatoid arthritis patients are responsible for osteoclast-like cell formation. J Bone Miner Res. 1996;11:88–95. doi:10.1002/jbmr.5650110113
10. Le Goff B, Blanchard F, Berthelot JM, Heymann D, Maugars Y. Role for interleukin-6 in structural joint damage and systemic bone loss in rheumatoid arthritis. Joint Bone Spine. 2010;77:201–205. doi:10.1016/j.jbspin.2010.03.002
11. Scheller J, Rose-John S. Interleukin-6 and its receptor: from bench to bedside. Med Microbiol Immunol. 2006;195(4):173–183. doi:10.1007/s00430-006-0019-9
12. Fishman D, Faulds G, Jeffery R, et al. The effect of novel polymorphisms in the interleukin-6 (IL-6) gene on IL-6 transcription and plasma IL-6 levels, and an association with systemic-onset juvenile chronic arthritis. J Clin Invest. 1998;102(7):1369–1376. doi:10.1172/JCI2629
13. Galicia JC, Tai H, Komatsu Y, et al. Polymorphisms in the IL-6 Receptor (IL-6R) gene: strong evidence that serum levels of soluble IL-6R are genetically influenced. Genes Immun. 2004;5(6):513–516. doi:10.1038/sj.gene.6364120
14. Ferreira RC, Freitag DF, Cutler AJ, et al. Functional IL6R 358Ala allele impairs classical IL-6 receptor signaling and influences risk of diverse inflammatory diseases. PLoS Genet. 2013;9(4):e1003444. doi:10.1371/journal.pgen.1003444
15. IL6R Genetics Consortium Emerging Risk Factors Collaboration. Interleukin-6 receptor pathways in coronary heart disease: a collaborative meta-analysis of 82 studies. Lancet. 2012;379(9822):1205–1213. doi:10.1016/S0140-6736(11)61931-4
16. Revez JA, Bain L, Chapman B, et al. A new regulatory variant in the interleukin-6 receptor gene associates with asthma risk. Genes Immun. 2013;14(7):441–446. doi:10.1038/gene.2013.38
17. Wang Y, Hu H, Wu J, et al. The IL6R gene polymorphisms are associated with sIL-6R, IgE and lung function in Chinese patients with asthma. Gene. 2016;585(1):51–57. doi:10.1016/j.gene.2016.03.026
18. Reich D, Patterson N, Ramesh V, et al. Admixture mapping of an allele affecting interleukin 6 soluble receptor and interleukin 6 levels. Am J Hum Genet. 2007;80:16–726. doi:10.1086/513206
19. Schotte H, Schmidt H, Gaubitz M, et al. Interleukin-6 promoter haplotypes are associated with etanercept response in patients with rheumatoid arthritis. Clin Rheumatol. 2015;34(12):2021–2028. doi:10.1007/s10067-015-3107-7
20. Zavaleta-Muniz SA, Martin-Marquez BT, Gonzalez-Lopez L, et al. The −174G/C and −572G/C interleukin 6 promoter gene polymorphisms in mexican patients with rheumatoid arthritis: a Case-Control Study. Clin Dev Immunol. 2013;2013:959084. doi:10.1155/2013/959084
21. Li F, Xu J, Zheng J, et al. Association between interleukin-6 gene polymorphisms and rheumatoid arthritis in Chinese han population: a case control study and a meta-analysis. Sci Rep. 2014;4:5714. doi:10.1038/srep05714
22. Ogilvie EM, Fife MS, Thompson SD, et al. The Ϫ174G allele of the interleukin-6 gene confers susceptibility to systemic arthritis in children: a multi- center study using simplex and multiplex juvenile idiopathic arthritis families. Arthritis Rheum. 2003;48:3202–3206. doi:10.1002/art.11300
23. Pawlik A, Wrzesniewska J, Florczak M, et al. IL-6 promoter polymorphism in patients with rheumatoid arthritis. Scand J Rheumatol. 2005;34(2):109–113. doi:10.1080/03009740510026373
24. Wielińska J, Dratwa M, Świerkot J, et al. Interleukin 6 gene polymorphism is associated with protein serum level and disease activity in polish patients with rheumatoid arthritis. HLA. 2018;92:38–41. doi:10.1111/tan.13355
25. Ceccarelli F, Perricone C, Fabris M, et al. Transforming growth factor β 869C/T and interleukin 6-174G/C polymorphisms relate to the severity and progression of bone-erosive damage detected by ultrasound in rheumatoid arthritis. Arthritis Res Ther. 2011;13:R111. doi:10.1186/ar3396
26. Marinou I, Healy J, Mewar D, et al. Association of interleukin-6 and interleukin-10 genotypes with radiographic damage in rheumatoid arthritis is dependent on autoantibody status. Arthritis Rheum. 2007;56(8):2549–2556. doi:10.1002/art.22814
27. Panoulas VF, Douglas KMJ, Smith JP, et al. Transforming growth factor-b1 869T/C, but not interleukin-6#174G/C, polymorphism associates with hypertension in rheumatoid arthritis. Rheumatology. 2009;48:113–118. doi:10.1093/rheumatology/ken443
28. Palomino-Morales R, Gonzalez-Juanatey C, Vazquez-Rodriguez TR, et al. Interleukin-6 gene −174 promoter polymorphism is associated with endothelial dysfunction but not with disease susceptibility in patients with rheumatoid arthritis. Clin Exp Rheumatol. 2009;6:964–970.
29. López-Mejías R, García-Bermúdez M, González-Juanatey C, et al. Lack of association between IL6 single nucleotide polymorphisms and cardiovascular disease in Spanish patients with rheumatoid arthritis. Atherosclerosis. 2011;219(2):655–658. doi:10.1016/j.atherosclerosis.2011.07.124
30. Panoulas VF, Stavropoulos-Kalinoglou A, Metsios GS, et al. Association of interleukin-6 (IL-6)-174G/C gene polymorphism with cardiovascular disease in patients with rheumatoid arthritis: the role of obesity and smoking. Atherosclerosis. 2009;204(1):178–183. doi:10.1016/j.atherosclerosis.2008.08.036
31. Davila-Fajardo CL, Marquez A, Pascual-Salcedo D, et al. Confirmation of −174G/C interleukin-6 gene promoter polymorphism as a genetic marker predicting antitumor necrosis factor treatment outcome. Pharmacogenet Genomics. 2014;24(1):1–5. doi:10.1097/FPC.0000000000000013
32. Jančić I, Šefik-Bukilica M, Živojinović S, et al. Influence of promoter polymorphisms of the TNF-α (−308G/A) and IL-6 (−174G/C) genes on therapeutic response to etanercept in rheumatoid arthritis. J Med Biochem. 2015;34(4):414–421. doi:10.2478/jomb-2014-0060
33. Pawlik A, Czerny B, Dabrowska-Zamojcin E, et al. The influence of IL-6 polymorphism on efficacy of treatment of rheumatoid arthritis patients with methotrexate and prednisone. Pol Arch Med Wewn. 2005;114(3):843–847.
34. Ruiz-Padilla AJ, Gamez-Nava JI, Saldaña-Cruz AM, et al. The −174G/C interleukin-6 gene promoter polymorphism as a genetic marker of differences in therapeutic response to methotrexate and leflunomide in rheumatoid arthritis. Biomed Res Int. 2016;2016:1–10. doi:10.1155/2016/4193538
35. Fabris M, Quartuccio L, Lombardi S, et al. The CC homozygosis of the −174G>C IL-6 polymorphism predicts a lower efficacy of rituximab therapy in rheumatoid arthritis. Autoimmun Rev. 2012;11:315–320. doi:10.1016/j.autrev.2010.06.012
36. Cubino N, Montilla C, Usategui-Martín R, et al. Association of IL1Β (−511 A/C) and IL6 (−174 G > C) polymorphisms with higher disease activity and clinical pattern of psoriatic arthritis. Clin Rheumatol. 2016;35(7):1789–1794. doi:10.1007/s10067-016-3301-2
37. Balding J, Kane D, Livingstone W, et al. Cytokine gene polymorphisms: association with psoriatic arthritis susceptibility and severity. Arthritis Rheum. 2003;48(5):1408–1413. doi:10.1002/art.10935
38. Białecka M, Ostasz R, Kurzawski M, et al. IL6−174G>C polymorphism is associated with an increased risk of psoriasis but not response to treatment. Exp Dermatol. 2015;24(2):146–147. doi:10.1111/exd.12577
39. Di Renzo L, Bianchi A, Saraceno R, et al. −174G/C IL-6 gene promoter polymorphism predicts therapeutic response to TNF-α blockers. Pharmacogenet Genomics. 2012;22(2):134–142. doi:10.1097/FPC.0b013e32834e5e7b
40. Baran W, Szepietowski JC, Mazur G, Baran E. IL-6 and IL-10 promoter gene polymorphisms in psoriasis vulgaris. Acta Derm Venereol. 2008;88(2):113–116. doi:10.2340/00015555-0427
41. Boca AN, Talamonti M, Galluzzo M, et al. Genetic variations in IL6 and IL12B decreasing the risk for psoriasis. Immunol Lett. 2013;156(1–2):127–131. doi:10.1016/j.imlet.2013.09.028
42. Enevold C, Baslund B, Linde L, et al. Interleukin-6-receptor polymorphisms rs12083537, rs2228145, and rs4329505 as predictors of response to tocilizumab in rheumatoid arthritis. Pharmacogenet Genomics. 2014;24(8):401–405. doi:10.1097/FPC.0000000000000071
43. Hassan B, Maxwell JR, Hyrich KL, et al. Genotype at the sIL-6R A358C polymorphism does not influence response to anti-TNF therapy in patients with rheumatoid arthritis. Rheumatology. 2010;49(1):43–47. doi:10.1093/rheumatology/kep372
44. Maldonado-Montoro M, Cañadas-Garre M, González-Utrilla A, et al. Influence of IL6R gene polymorphisms in the effectiveness to treatment with tocilizumab in rheumatoid arthritis. Pharm J. 2018;18:167–172.
45. Ibrahim I, McAllister K, Plant D, et al. Investigation of an interleukin-6 receptor gene polymorphism (rs2228145) as a predictor of cardiovascular mortality in inflammatory polyarthritis: results from the Norfolk Arthritis Register: table 1. Ann Rheum Dis. 2014;73(4):787–788. doi:10.1136/annrheumdis-2013-204330
46. Marinou I, Walters K, Winfield J, et al. A gain of function polymorphism in the interleukin 6 receptor influences RA susceptibility. Ann Rheum Dis. 2010;69(6):1191–1194. doi:10.1136/ard.2008.100644
47. Lamas JR, Rodríguez-Rodríguez L, Varadé J, et al. Influence of IL6R rs8192284 polymorphism status in disease activity in rheumatoid arthritis. J Rheumatol. 2010;37(8):1579–1581. doi:10.3899/jrheum.091455
48. Cénit MC, Simeón CP, Fonollosa V, et al. No evidence of association between functional polymorphisms located within IL6R and IL6ST genes and systemic sclerosis. Tissue Antigens. 2012;80(3):254–258. doi:10.1111/j.1399-0039.2012.01915.x
49. Esparza-Gordillo J, Schaarschmidt H, Liang L, et al. A functional IL-6 receptor (IL6R) variant is a risk factor for persistent atopic dermatitis. J Allergy Clin Immunol. 2013;132(2):371–377. doi:10.1016/j.jaci.2013.01.057
50. Goupille P. Psoriatic arthritis. Joint Bone Spine. 2005;72(6):466–470. doi:10.1016/j.jbspin.2005.10.006
51. Fransen J, Antoni C, Mease PJ, et al. Performance of response criteria for assessing peripheral arthritis in patients with psoriatic arthritis: analysis of data from randomised controlled trials of two tumour necrosis factor inhibitors. Ann Rheum Dis. 2006;65:1373–1378. doi:10.1136/ard.2006.051706
52. Mease PJ, Antoni CE, Gladman DD, et al. Psoriatic arthritis assessment tools in clinical trials. Ann Rheum Dis. 2005;64 Suppl 2(Suppl 2):ii49–ii54. doi:10.1136/ard.2004.034165
53. Xu Z, Taylor JA. SNPinfo: integrating GWAS and candidate gene information into functional SNP selection for genetic association studies. Nucleic Acids Res. 2009;37(suppl_2):W600–W605. doi:10.1093/nar/gkp290
54. Auton A, Brooks LD, Durbin RM, et al. A global reference for human genetic variation. Nature. 2015;526:68–74.
55. R Core Team. R: A Language and Environment for Statistical Computing [Internet]. Vienna, Austria: R Foundation for Statistical Computing; 2016. Available from: http://www.R-project.org/.
56. Nowell MA, Richards PJ, Horiuchi S, et al. Soluble IL-6 receptor governs IL-6 activity in experimental arthritis: blockade of arthritis severity by soluble glycoprotein 130. J Immunol. 2003;171(6):3202–3209. doi:10.4049/jimmunol.171.6.3202
57. Sasai M, Saeki Y, Ohshima S, et al. Delayed onset and reduced severity of collagen-induced arthritis in interleukin-6-deficient mice. Arthritis Rheum. 1999;42(8):1635–1643. doi:10.1002/1529-0131(199908)42:8<1635::AID-ANR11>3.0.CO;2-Q
58. Takagi N, Mihara M, Moriya Y, et al. Blockage of interleukin-6 receptor ameliorates joint disease in murine collagen-induced arthritis. Arthritis Rheum. 1998;41:2117–2121. doi:10.1002/1529-0131(199812)41:12<2117::AID-ART6>3.0.CO;2-P
59. Lee YH, Lee HS, Choi SJ, et al. The association between interleukin-6 polymorphisms and systemic lupus erythematosus: a meta-analysis. Lupus. 2012;21(1):60–67. doi:10.1177/0961203311422711
60. Illig T, Bongardt F, Schopfer A, et al. Significant association of the interleukin-6 gene polymorphisms C-174G and A-598G with type 2 diabetes. J Clin Endocrinol Metab. 2004;89:5053–5058. doi:10.1210/jc.2004-0355
61. Vozarova B, Fernandez-Real JM, Knowler WC, et al. The interleukin-6 (−174) G/C promoter polymorphism is associated with type-2 diabetes mellitus in native Americans and Caucasians. Hum Genet. 2003;112:409–413.
62. Sfrent-Cornateanu R, Mihai C, Balan S, et al. The IL - 6 promoter polymorphism is associated with disease activity and disability in systemic sclerosis. J Cell Mol Med. 2006;10(4):955–959. doi:10.1111/j.1582-4934.2006.tb00538.x
63. Xu W-D, Zhou M, Peng H, et al. Lack of association of IL-6 polymorphism with rheumatoid arthritis/type 1 diabetes: a meta-analysis. Joint Bone Spine. 2013;80(5):477–481. doi:10.1016/j.jbspin.2012.11.005
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.