Back to Journals » Open Access Emergency Medicine » Volume 12
Relationship Between Initial Arterial Blood Gases and Coagulation Profiles – Analyzing the Prognosis and Outcomes in Patients with Multiple Injuries/Trauma
Authors Raffee LA ![]() , Oteir AO
, Oteir AO ![]() , Alawneh KZ
, Alawneh KZ ![]() , Alustath AMI
, Alustath AMI
Received 9 January 2020
Accepted for publication 25 March 2020
Published 15 April 2020 Volume 2020:12 Pages 87—92
DOI https://doi.org/10.2147/OAEM.S244941
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Liqaa A Raffee,1 Alaa O Oteir,2 Khaled Z Alawneh,3 Alaa MI Alustath1
1Department of Accident and Emergency Medicine, Faculty of Medicine, Jordan University of Science and Technology, Irbid 22110, Jordan; 2Program of Paramedicine, Department of Allied Medical Sciences, Faculty of Applied Medical Sciences, Jordan University of Science and Technology, Irbid, Jordan; 3Department of Diagnostic Radiology and Nuclear Medicine, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan
Correspondence: Liqaa A Raffee
Department of Accident and Emergency Medicine, Faculty of Medicine, Jordan University of Science and Technology, Irbid 22110, Jordan
Tel +962 27200600-45030
Fax +962 27095777
Email [email protected]
Purpose: Trauma is recognized as a significant health concern across the world. The increase in the mortality rate of multiple trauma (MT) patients serves as a major issue for health-care providers. The study investigates the relationship between the initial arterial blood gases and coagulation profiles among the multiple injured/trauma patients.
Patients and Methods: A retrospective study design was used, and 137 acute trauma patients’ data were included from the King Abdullah University Hospital (KAUH) from 1 January 2014 to 1 October 2017.
Results: The results showed that patients were mainly male (79.6%) and had RTA (71.5%). They had a normal pH (50.4%) and pCO2 (68.6%) while decreasing HCO3 (51.1%). An increasing level of pCO2 (45%) along with PT (28%), PTT (17%) and INR (23%) is observed. It also showed a decreasing level of platelets (39%). The overall findings showed a close association of the blood gases and coagulation indicators.
Conclusion: The study concludes that to control the coagulation markers, the blood gases of the patients should be screened and monitored.
Keywords: acidosis, hemorrhagic shock, hypothermia, oxygen, resuscitative hemodilution
Introduction
Hemorrhagic shock occurs due to loss in blood volume resulting from insufficient perfusion and oxygen supply to the vital organs causing impaired cardiac pre-load.1 The pre-hospital resuscitation and monitoring of trauma patients rely on clinical experience and few basic parameters, including consciousness, breathing rate, and quality, heart rate, and quality, and blood pressure, especially systolic. However, even when these basic clinical parameters are close to normal, the possibility of the shock is high at the cellular and organ levels.2 The complete resuscitation from shock is indicated through the successful reversal of anaerobic metabolism and tissue acidosis. Also, the normalization of disturbed microvascular perfusion and oxygen supply are the key therapeutic factor that prevents multiple organ failure (MOF).3
Traumatologists develop a wide range of scoring systems based on physiological parameters (such as respiratory rate, blood pressure, and consciousness level), to measure and quantify the extent and severity of trauma.4,5 The condition of severe trauma is a major global public health issue as it accounts for one in ten mortalities. The uncontrolled post-traumatic bleeding is the primary cause that leads to potentially preventable death among multiple injured patients. Following the traumatic injury, the abnormal arterial blood gas (ABG) is known to be an important marker for poor outcome along with occult malperfusion.6 This is the reason, ABG is used as a screening tool among the patient sustaining trauma for the occult injury.7 Significant contributors to coagulation dysfunction after trauma include acidosis, hypothermia, and resuscitative hemodilution. The observation of coagulopathy is known as a major cause of early hospitalization among trauma patients. The longer hospital stays with increased requirements of blood transfusion, and mortality is categorized under the hemostatic manifestation.
A review of the literature provides that none of the previous studies3,8,9 has assessed the association between initial arterial blood gases and initial coagulation profiles among acute trauma patients in Jordan.10,11 Particularly the research concerning the prognostic value of ABG is limited.6 Accordingly, earlier researches stated that the ABG changes can be effective form appropriate prediction of the traumatic injury severity.12,13 However, no study has been conducted in this regard. Therefore, the present study assesses the relationship between initial arterial blood gases and initial coagulation profiles in acute trauma patients presented to the emergency department at King Abdullah University Hospital (KAUH), Northern Jordan. It intends to assess the prognostic ABG value in multiple trauma patients. This study also evaluates this association and its effect on the prognosis outcomes among these patients. The study results are likely to help in the rapid triaging of acute trauma patients, which would also help to identify high-risk patients developing severe complications. The present study conducted a laboratory assessment of the patients based on its objectivity for measuring the resuscitation adequacy.14
Patients and Methods
Study Design and Setting
The present study uses a retrospective study design to investigate the relationship between initial arterial blood gases and coagulation profiles as well as to assess the prognosis and outcomes in patients with multiple trauma. The study was conducted at King Abdullah University Hospital (KAUH) located in Northern Jordan.
Study Participants
The study included cases of multiple trauma, who were admitted in a hemorrhagic shock state to the hospital’s Emergency Room.
Inclusion and Exclusion Criteria
The inclusion criteria for this study were patients of both the genders, aged between 18 and 80 years. Participants were also included if presented to the ER (Emergency Room) having multiple trauma, in the period from 2015 to 2018. Patients were excluded if they were victims of the Syrian war, pregnant, younger than 18 years, and/or had incomplete medical records.
Data Collection
The data was extracted from the database of KAUH. The medical records of all the acute trauma patients referred to the hospital ER from January 2015 to December 2018 were assessed. This includes their demographics, arterial blood gases (ABS) profile, trauma type, transport type, and diagnosis.
Data Analysis
The data defining clinical characteristics of the patients and depicting the relationship between coagulation factors and blood gases was gathered, coded, uploaded, and analyzed in SPSS software version 20 (IBM Corporation, USA). Mean, and standard deviation (SD) were computed for the participants’ demographics, while Chi-square and Spearman correlation analysis was also conducted for examining the coagulation factors and blood gases. Multiple regression was also conducted for the collected data. The significance value was determined as (p<0.05).
Ethical Approval
The Institutional Review Board (IRB) of KAUH approved the study, patient consent to review their medical records was not required by the IRB of KAUH. Moreover, this study was conducted in accordance with the Helsinki Declaration (APPROVAL NUMBER 423/2017).
Results
Initially, the demographic details of the recruited participants were collected. A total of 137 patients were included in the study, where most of the participants were male (79.6%). Also, the mean (SD) age was 41.3 ± 19.4 years old. The general clinical characteristics of the participants are presented in Table 1. It is found that 63 patients were the one who was assessed for the first time were presented to ER while the transferred patients (transferred patients are patients transferred to KAUH hospital from other hospitals) were 71. Also, the BP of most of the patients was recorded to be normal, ie, 83, followed by patients with decreased patients systolic BP (23) and with increased BP (13). The pulse rate of most of the patients was also recorded to be normal (72), while for 46 patients, it was found increasing, and for 4 patients, it was decreasing. Majority of the patients had normal body temperature (113), while only 5 patients were found to have increased temperature and just one for the decreasing body temperature. The trauma analysis reveals that 84 patients suffered from multiple trauma, while 49 did not. The most injured body region was the head, followed by the chest, abdominal, and pelvis.
 |
Table 1 General Clinical Characteristics |
Table 2 includes the clinical characteristics of the participants. It reveals that trauma was majorly caused by RTA for both males and females (p-value = 0.439). 50 percent of the female had normal PH level, which was the same for males (50.9%). pCO2 level was also normal for both the genders. HCO3 level was found to be increased for females (71.4%), whereas it was normal for men (53.6%). High pO2 level was found among females, while it was low for males (47.3%). O2 Sat, PT, PTT, INR and Platelets were normal for both the genders. Among all the variables, the significant p-value was only found for HCO3 (ie, a p-value of 0.047).
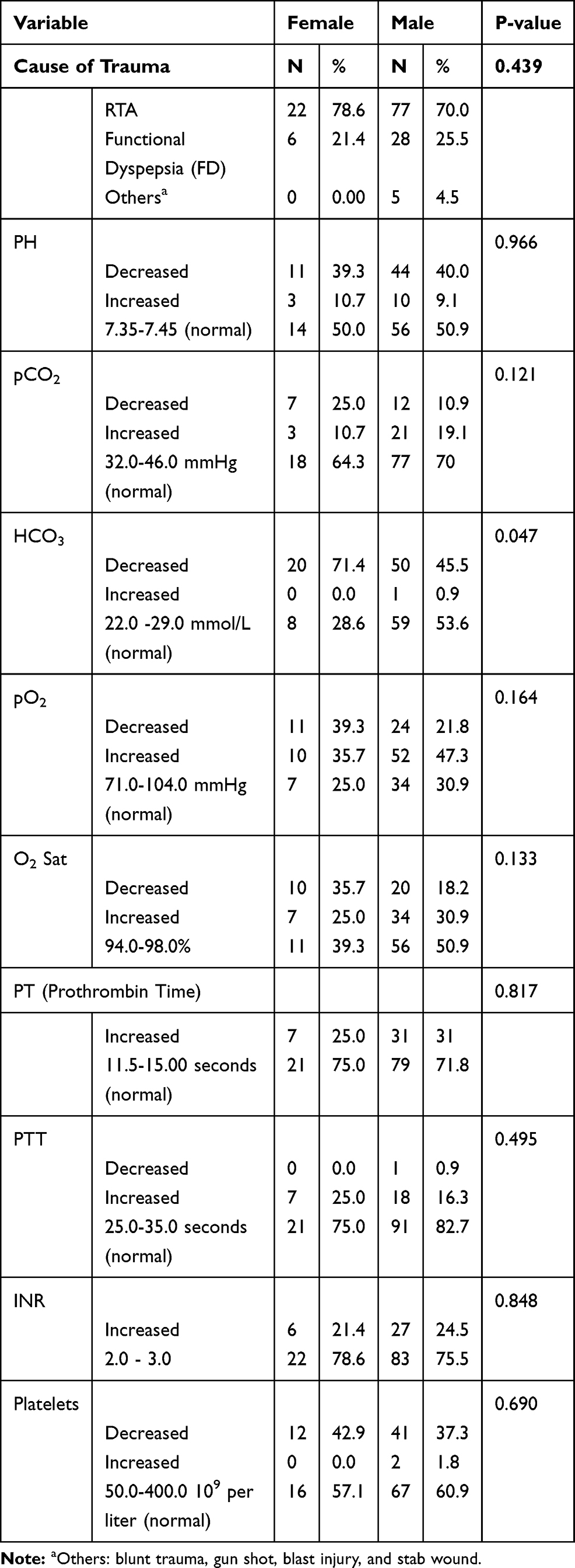 |
Table 2 Clinical Characteristic of the Participants |
Table 3 shows the Spearman correlation between coagulation factors and blood gases. The study found a significant and positive correlation between PT and HCO3 (p = 0.000), PT and pO2 sat (p = 0.004), PT and O2 sat (p = 0.000), and PT and platelets (p = 0.000). In addition, a significant and positive correlation between PTT and PH (p = 0.001), PTT and HCO3 (p = 0.000), PTT and PO2 sat (0.049), and PTT and platelets (p = 0.000) was found. Moreover, a positive and significant correlation has been found between INR and HCO3 (p = 0.000), INR and pO2 sat (p = 0.000), PTT and O2 sat (p = 0.000), and INR and Platelets (p = 0.000).
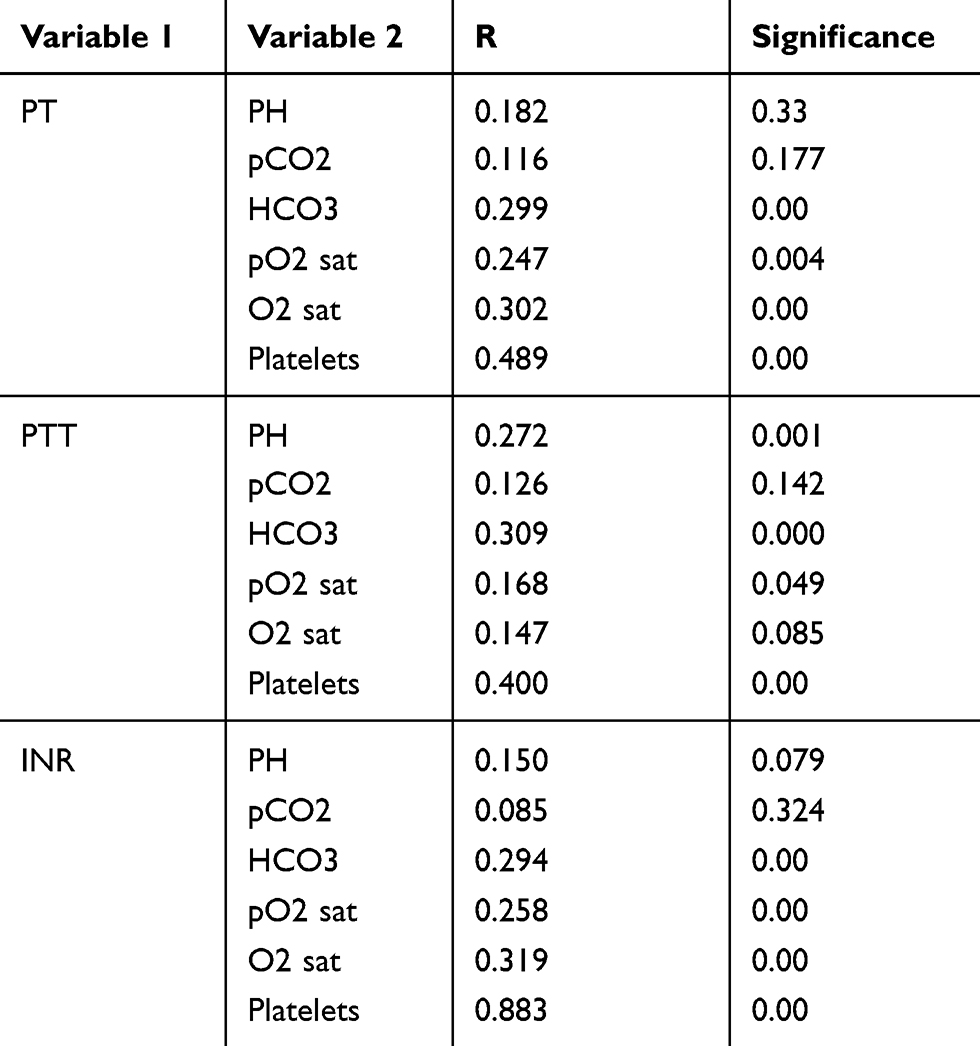 |
Table 3 Correlation Between Coagulation Factors and Blood Gases |
Table 4 shows the results for the multiple regression analysis. It reveals a significant relationship between the diagnosis and the clinical factors. It is because the value found was (p-value = 0.000).
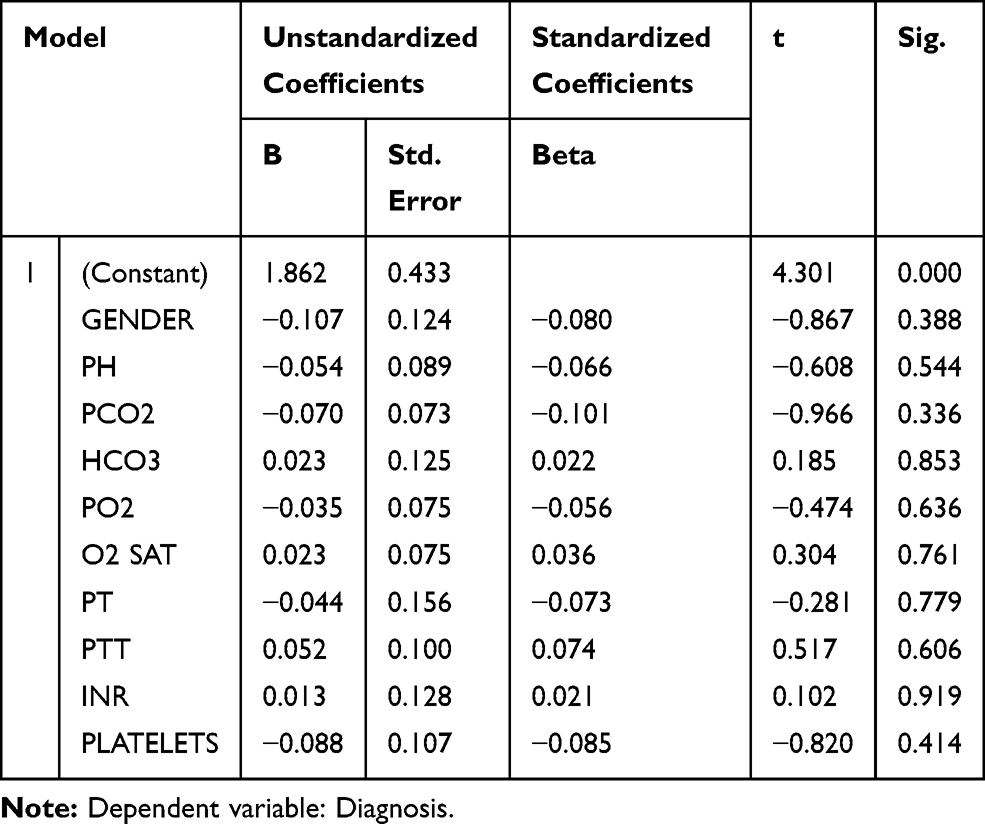 |
Table 4 Regression Analysis |
Discussion
The present study has investigated the association between the arterial blood gases and coagulation profile of the multiple trauma patients. The findings of this research showed that the prognostic ability of ABG indices concerning the complications associated with the multiple trauma patients. The findings showed that decreased bicarbonate serves as a predictor for the high risk of multiple trauma among patients. The sample results are presented by Mohsenian et al,12 which showed decreased bicarbonate as the significant prognosis marker for the AHF patients. PCO2 was also demonstrated to lead to worse outcomes concerning the multiple trauma patients, which was linked to high-risk trauma patients. The findings of the study do not present the mechanistic link between the ABG findings and the clinical results, and thereby, only presents possible mechanism speculations. Concerning the present study, only a few researches are found concerning the ABG prognostic value. For instance, Burri et al15 demonstrated that pH presentation is a substantial predictor of the short and long-run outcomes for patients in the critical care unit. While, the findings of Minana et al16 showed that PCO2 and PO2 at admission were not linked with the mortality, which disregards the use of the ABG for the prognosis assessment. The discrepancies in the results might be because of the different population characteristics, as well as sample size. However, the present study showed that male gender, RTA, low systolic blood pressure, low bicarbonate, and PCO2 were associated as the predictors of multiple injuries/trauma. These found risk factors have been consistently been stated by earlier researches.
The analysis of the collected data showed that most of the patients who visited the emergency room of the hospital were male. Abhilash et al17 observed a similar reporting where the percentage of males was 73.6%. The reason behind the increase of males in the ER is because, in Jordan, the male population generally performs the outdoor task while females generally prefer to stay at home, which makes males more vulnerable to the injuries. Similarly, the mean age of the multiple trauma patients in the study is 41.34 ± 19.41 years. This is consistent with the earlier reports which were conducted in other regions such as India17 and Iran, which are also recognized as developing regions.14 Concerning the clinical characteristics of the patients, RTA is observed to be the most primary source of trauma among the patients. This is because of the increasing traffic on the road and its development as an urban setting. Systematic research on the Saudi population by Mansuri et al18 also concluded similar results stating that almost 79.5 percent of the population reported fractures and injuries due to road accidents.
The present study showed a decrease in the HCO3 level for the patients. These findings are supported by Parvizi et al,19 which also found its decreasing level among Iranian patients. The study found an association of the arterial blood gases and the coagulopathy profile of the patients. It is because the shock in the multiple trauma patients leads to activation of the inflammatory cascade and hypoperfusion among the patients. Concerning the present study findings, the results of a previous study12 list bleeding as a trauma-related death among the patients which could have been prevented. This highlights that coagulopathy causes in the multiple trauma patients are multifactorial, which comprise of the platelet’s dilution and consumption along with the platelet’s dysfunctionality.
The results of the present study show the trauma burden of the ED in Jordan. It also reveals that there is a significant relationship between the blood gases and coagulation indicators. This is also supported in the literature, which differs in terms of its design, scope, and objectives.20,21 The findings showed that efforts must be instigated for reducing the struggles of the medical provider. This means ensuring the presence of computed scam, blood bank, tomography scan, and more for meeting the care needs of the trauma patients. This emphasized that hospitals in Jordan need to understand the significance of emergency primary care at the hospitals for effectively managing the trauma patients and using interventional practices at the early stages which saves them from the potential adverse effect.
The study has certain limitations in terms of its retrospective design and analysis of a certain region which limits its result transferability. This serves as a starting point for future studies that could use a qualitative study design and evaluate the perspective of the medical service provider and the struggles; they must go through to save the lives of the multiple injured patients. Accordingly, future researches can use the same objective for assessing the association of the initial arterial blood gases with the coagulation profile in other counties, which helps expand the study area. Future analysis can help in illuminating new insights on the problem, which may reveal new information, ultimately enhancing the study scope.
Conclusion
The present study aimed to assess the relationship between the initial arterial blood gases and coagulation profile of the multiple injured patients. Based on the retrospective analysis of the Jordanian patients, the findings suggest that male gender, RTA, low systolic blood pressure, low bicarbonate, and PCO2 should be used as parameters for initially assessing the patients for multiple trauma or injuries. The results highlight that the use of these parameters can help in the determination of the patient’s conditions, and the treatment procedure to be adopted. It also concludes that admitted patients in the emergency room were male. Accordingly, the results show that RTA was the substantial cause of multiple injury trauma among Jordanian patients. The findings conclude a significant relationship between the blood gases and coagulation indicators. Additionally, it highlights the need to initiate awareness programs for the patients, along with training programs for the physicians and paramedical team for the management of the trauma and the urgent diagnosis of treatment. The timely practices of the associated personnel can assist in providing the necessary care in the prevention of the patient’s premature deaths.
Abbreviations
ABG, Arterial Blood Gases; AAAM, Association for the Advancement of Automotive Medicine; HCO3, Bicarbonate; BP, Blood Pressure; mmHg, millimeter Mercury; bpm, pulse per minute; ED, Emergency Department; ER, Emergency Room; FD, Functional Dyspepsia; IRB, Institutional Review Board; INR, International Normalized Ratio; KAUH, King Abdullah University Hospital; MOF, Multiple Organ Failure; MT, Multiple Trauma; pCO2, Partial Pressure of Carbon Dioxide; PTT, Partial Thromboplastin Time; mmol, millimole; Ph, Potential Hydrogen; PT, Prothrombin Time; RTA, Road Traffic Accident; SD, Standard Deviation; SPSS, Statistical Package for Social Sciences.
Acknowledgments
The authors are very thankful to all the associated personnel in any reference that contributed to/for this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cannon JW, Longo DL. Hemorrhagic shock. N Engl J Med. 2018;378(4):370–379. doi:10.1056/nejmra1705649
2. Moore J, Fraser JF. Clinical implications of monitoring tissue perfusion in cardiogenic shock. In: Pinto Lima A., Silva E, editors. Monitoring Tissue Perfusion in Shock. Cham: Springer;2018:193–206. doi:10.1007/978-3-319-43130-7_14
3. Jousi M, Reitala J, Lund V, et al. The role of pre-hospital blood gas analysis in trauma resuscitation. World J Emerg Surg. 2010;5(1):10. doi:10.1186/1749-7922-5-10
4. Lichtveld RA, Spijkers AT, Hoogendoorn JM, et al. Triage revised trauma score change between first assessment and arrival at the hospital to predict mortality. Int J Emerg Med. 2008;1(1):21. doi:10.1007/s12245-008-0013-7
5. Holena DN, Wiebe DJ, Carr BG, et al. Lead-time bias and interhospital transfer after injury: trauma center admission vital signs underpredict mortality in transferred trauma patients. J Am Coll Surg. 2017;224(3):255–263. doi:10.1016/j.jamcollsurg.2016.11.016
6. Park JJ, Choi DJ, Yoon CH, et al. The prognostic value of arterial blood gas analysis in high‐risk acute heart failure patients: an analysis of the Korean Heart Failure (KORHF) registry. Eur J Heart Fail. 2015;17(6):601–611. doi:10.1002/ejhf.276
7. Martini WZ. Coagulation complications following trauma. Mil Med Res. 2016;3:35. doi:10.1186/s40779-016-0105-2
8. Johansson PI, Sørensen AM, Perner A, et al. Disseminated intravascular coagulation or acute coagulopathy of trauma shock early after trauma? An observational study. Crit Care. 2011;15(6):R272. doi:10.1186/cc10553
9. Vohra T, Paxton J. Abnormal arterial blood gas and serum lactate levels do not alter disposition in adult blunt trauma patients after early computed tomography. West J Emerg Med. 2013;14(3):212. doi:10.5811/westjem.2012.3.6905
10. Bhardwaj V, Kapoor PM, Irpachi K, et al. Basic arterial blood gas biomarkers as a predictor of mortality in tetralogy of fallot patients. Ann Card Anaesth. 2017;20(1):67. doi:10.4103/0971-9784.197839
11. Radjou A. Early predictive factors of hypofibrinogenemia in acute trauma patients. J Emerg Trauma Shock. 2018;11(1):2. doi:10.4103/JETS.JETS_83_17
12. Mohsenian L, Khoramian MK, Mazloom SS. Prognostic value of arterial blood gas indices regarding the severity of traumatic injury and fractures of the femur and pelvis. Bull Emerg Trauma. 2018;6(4):318. doi:10.29252/beat-060408
13. Dumont TM, Visioni AJ, Rughani AI, Tranmer BI, Crookes B. Inappropriate prehospital ventilation in severe traumatic brain injury increases in-hospital mortality. J Neurotrauma. 2010;27(7):1233–1241. doi:10.1089/neu.2009.1216
14. Bozorgi F, Khatir IG, Ghanbari H, et al. Investigation of frequency of the lethal triad and its 24 hours prognostic value among patients with multiple traumas. Open Access Maced J Med Sci. 2019;7(6):962. doi:10.3889/oamjms.2019.217
15. Burri E, Potocki M, Drexler B, et al. Value of arterial blood gas analysis in patients with acute dyspnea: an observational study. Crit Care. 2011;15(3):R145. doi:10.1186/cc10268
16. Miñana G, Núñez J, Bañuls P, et al. Prognostic implications of arterial blood gases in acute decompensated heart failure. Eur J Intern Med. 2011;22(5):489–494. doi:10.1016/j.ejim.2011.01.014
17. Abhilash KP, Chakraborthy N, Pandian GR, et al. Profile of trauma patients in the emergency department of a tertiary care hospital in South India. J Family Med Prim Care. 2016;5(3):558. doi:10.4103/2249-4863.197279
18. Mansuri FA, Al-Zalabani AH, Zalat MM, et al. Road safety and road traffic accidents in Saudi Arabia: a systematic review of existing evidence. Saudi Med J. 2015;36(4):418. doi:10.15537/smj.2015.4.10003
19. Parvizi R, Safaii N, Neghargar S, et al. Comparison of arterial and venous blood gas values in cardiac surgery. Rawal Med J. 2008;33:4.
20. Qu Z, Wang G, Xu C, et al. The effects of platelet apheresis on blood saving and coagulation in bilateral total hip replacement: a prospective study on 60 patients. Int J Surg. 2016;34:58–63. doi:10.1016/j.ijsu.2016.08.233
21. Stein P, Studt JD, Albrecht R, et al. The impact of prehospital tranexamic acid on blood coagulation in trauma patients. Anesth Analg. 2018;126(2):522–529. doi:10.1213/ane.0000000000002708
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.