Back to Journals » Risk Management and Healthcare Policy » Volume 14
Relationship Between Frequency and Intensity of Menopausal Symptoms and Quality of Life Among Polish Nurses
Authors Kupcewicz E, Drężek–Skrzeszewska M, Roszuk W, Jóźwik M
Received 20 October 2020
Accepted for publication 17 December 2020
Published 11 January 2021 Volume 2021:14 Pages 97—107
DOI https://doi.org/10.2147/RMHP.S287767
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Marco Carotenuto
Ewa Kupcewicz,1 Małgorzata Drężek–Skrzeszewska,2 Wioletta Roszuk1 ,† Marcin Jóźwik3
1Department of Nursing, Collegium Medicum University of Warmia and Mazury in Olsztyn, Olsztyn, Poland; 2Department of Obstetrics, Collegium Medicum, University of Warmia and Mazury in Olsztyn, Olsztyn 10-719, Poland; 3Department of Gynecology and Obstetrics, Collegium Medicum, University of Warmia and Mazury in Olsztyn, Olsztyn, Poland
†Mrs Wioletta Roszuk passed away on September 9 2020
Correspondence: Ewa Kupcewicz Email [email protected]
Purpose: The study aims to compare the quality of life of nurses in the somatic, mental, social and environmental dimensions in the full reproductive and perimenopausal period and to determine the relationship between the frequency and intensity of menopausal symptoms and the quality of life of nurses aged 45– 55.
Patients and Methods: The study involved 334 nurses, of which: 158 (47.31%) were aged 25– 35 and 176 (52.69%) aged 45– 55, included in the perimenopausal group. A diagnostic survey was used as the research method and the WHOQoL-Bref Questionnaire and the Menopause Symptom List were used to collect data.
Results: Nurses aged 25– 35 achieved a significantly (p < 0.02) higher level of satisfaction with overall health quality (M = 3.9; SD = ± 0.7) than nurses in the 45– 55 age group (M = 3.7; SD = ± 0.7). A variation in the frequency (F = 62.64; p < 0.0001) and intensity (F = 130.18; p < 0.0001) of menopausal symptoms was identified. It was found that the frequency and intensity of psychological symptoms were significantly higher than vasomotor (p < 0.0001) and somatic (p < 0.0001) symptoms. Additionally, negative relations between the frequency and intensity of menopausal symptoms and the quality of life of nurses in the 45– 55 age group in the somatic, mental, social and environmental domains were demonstrated, with their value ranging from r = − 0.19 to r = − 0.48.
Conclusion: The quality of life of the examined nurses varies. In the perimenopausal period, the frequency and intensity of psychological, vasomotor and somatic symptoms have a significant negative impact on the quality of life of nurses.
Keywords: quality of life, nursing, menopausal symptoms
Introduction
Interest in the quality of life can be traced back to ancient times. Hippocrates and Aristotle, based on philosophy and medicine, tried to define the foundation of a happy and satisfying life.1 Over the centuries, the concept of quality of life evolved and became an ambiguous and multidimensional construct, reflecting numerous aspects of human life and activities.2,3
In the literature, the concept of quality of life is defined in several ways.1 The World Health Organization (WHO) defines quality of life as the subjective assessment by an individual of their life situation in relation to the culture in which they live, and their system of values, goals, expectations and interests.4 From the perspective of medical science, the definitions of quality of life are largely focused on the phenomena of health and disease. Another definition is the “health-related quality of life” (HRQoL) definition provided by Schipper et al.1,5 The HRQoL definition takes into account four basic aspects of the patient’s functioning - physical condition and motor fitness, mental state, social and economic situation and somatic experience.1 The quality of life determined by health is primarily related to functional variables, which is the reason why it has been given the status of an objective measure.1
Quality of life is closely linked to health, the most important asset, value, wealth and resource. A particular type of health is procreative health, which is an important part of the definition of health as one’s entire physical, mental and social wellbeing. Taking into account these definitions of quality of life, researchers try to identify factors related to the quality of life at different stages of human development. In a period of full procreation in a woman’s life, pregnancy and childbirth have a significant impact on their quality of life, because the birth of a child is a breakthrough event, changing values, priorities and creating a new kind of bond and responsibility between partners. Changes are taking place in the roles of both parents and new tasks related to motherhood are emerging.6
On the other hand, developmental processes typical for middle-aged women form an individual concept of menopause. As the literature indicates, menopause is a complex physiological process during which the ovarian function and sex hormone production gradually decrease.7 The reduction in the production of estrogens, which are involved in numerous biological processes, is particularly strongly experienced. Their deficiency may cause cardiovascular, cerebral, skin, genitourinary, bone and vascular changes in women, as well as changes in mood and appetite.8 Researchers typically indicate three groups of menopausal symptoms. These are groups of psychological, vasomotor and somatic nature.9 The most frequent symptoms include night sweats, hot flashes, vaginal dryness, weakening of pelvic floor muscles, dyspareunia and insomnia.8,10 The physical changes occurring in a woman are linked to the ageing process. They can lead to changes in a woman’s self-image.8,11 In turn, scientific reports on the occurrence of anxiety and depression during menopause indicate changes in the activity of neurotransmitters, attributable to sex hormones.8,12 Some studies suggest no direct link between depression and menopause, but hormonal changes occurring during and after the menopause in most women cause mental changes or intensify other menopausal symptoms.13
Menopause-related symptoms, such as anxiety, stress and depressive symptoms, extend, on average, over about 4.5 years after the last menstrual period date.14 According to the WHO, the perimenopausal period covers from 2 to 8 years preceding the last menstrual period date and one year after it.4 In individual life, menopause can occur between the age of 45 and 55. The average age at which Polish women reach menopause is between 48 and 52, while the median age of menopause is 51.25 years.15–17 In a study conducted by Zamaniyan et al in the group of Iranian women, the average age of natural menopause was 49.2 ± 4.7 years.16 Forecasts indicate that by 2030 there will be 1.2 billion women aged 50 and over in the world; 76% of these will live in developing countries.7,18,19 Over 50% of middle-aged women experience frequent menopause-related symptoms.14 The research conducted by Kaczmarek showed that early first menstruation, short menstrual cycle, smoking, low level of education and negative perception of health were significantly related to the occurrence of menopause at an earlier age. In contrast, the use of oral contraceptives and childbirth were both associated with the occurrence of menopause at a later age.15
The working environment of nurses presents several risk factors for reproductive disorders. Reproductive disorders include menstrual disorders, prolonged or absent menstrual periods, painful anovulatory cycles, spontaneous miscarriages and premature menopause.20 Risk factors for reproductive disorders are primarily related to occupational stress, heavy physical effort, shift work, radiation and chemicals.20 A nurse, as a person responsible for the professional care of a healthy or sick person, may herself have health problems that may be related to the quality of life. Numerous researchers indicate that the quality of nurses’ professional life varies greatly and requires intervention.21 Viselita et al carried out a systematic review and, based on reliable publications regarding the results of primary research in the area of quality of professional life, found that in eight countries, 28.6% of the examined nurses identified their life quality level as low, 52.4% as moderate and only 19% high.21
This paper aims to compare the quality of life of nurses in the somatic, mental, social and environmental dimensions in the full reproductive period and in the perimenopausal period, and to determine the relationship between the frequency and intensity of menopausal symptoms and the quality of life of nurses aged 45–55 years.
The following research problems were formulated:
- To what extent do differences exist in the quality of life of nurses in the somatic, mental, social and environmental dimensions in the full reproductive period (25–35 years) and in the perimenopausal period (45–55 years)?
- To what extent does the frequency and intensity of psychological, vasomotor and somatic menopausal symptoms vary among nurses aged 45–55?
- Is there a correlation between the frequency and intensity of menopausal symptoms and the quality of life of nurses in the somatic, mental, social and environmental dimensions of 45–55 years old and if so, what is this correlation?
Patients and Methods
Settings and Design
A survey study was conducted among nurses between June 2013 and January 2015 in seven hospitals located in Olsztyn in the Warmia and Mazury Province (Poland). The inclusion criterion for group A was the age of the nurses between 25 and 35, in their full reproductive period, and their consent to participate in the study. Nurses who did not express their consent to participate were excluded from the study. Group B included nurses aged 45–55 years who had not used hormone replacement therapy in the last six months and expressed their consent to participate in the study. Nurses in whom menopause was caused by surgical intervention, chemical, radiological or other external causes or who did not consent to participate in the study were excluded from the study. After obtaining permission from the hospital management to conduct the research, one of the researchers (E.K.) personally delivered ready-made sets of questionnaires. Respondents were informed about the purpose of the survey and provided with instructions on how to fill in the questionnaires and they had the opportunity to ask questions and receive comprehensive explanations. The survey was voluntary and anonymous and the respondents could opt-out at any time. After expressing their informed consent to participate in the study, the respondents received sets of questionnaires. The women from the perimenopausal group were additionally provided with the “My wellbeing” questionnaire included in the set. The time for filling in the questionnaires was about 20 minutes. A total of 405 sets of questionnaires were distributed. After collecting the data and eliminating defective questionnaires, 334 questionnaires (ie 82.47%) were included in the analysis. Empirical data were collected in a database and encrypted using the Excel package.
The study was carried out in accordance with the ethical standards for scientific research included in the Declaration of Helsinki. The study design was approved by the Senate Research Ethics Committee of Olsztyn University College J. Rusiecki (No. 11/2016), Poland. The research meets the criteria for a cross-sectional study and is part of a larger research project carried out among Polish nurses.22
Participants
The study involved 334 women practising as nurses, including 158 (47.31%) women aged 25–35 years in the full reproductive period and 176 (52.69%) women aged 45–55 years classified into the perimenopausal group. The distribution of the education level in the studied groups was significantly different (χ2 = 126.61; p < 0.0001). Nurses aged 25–35 more often declared higher education (96.84%) than nurses in the older age group (44.32%). Most respondents in both age groups were married or in partnership (n = 143; 81.25% vs n = 103; 65.19%) and lived in the town (n = 153; 86.93% vs n = 123; 77.85%). Nurses from the perimenopausal group significantly more often (40.34%) declared a good or very good financial situation as compared to younger women (16.46%) (Table 1).
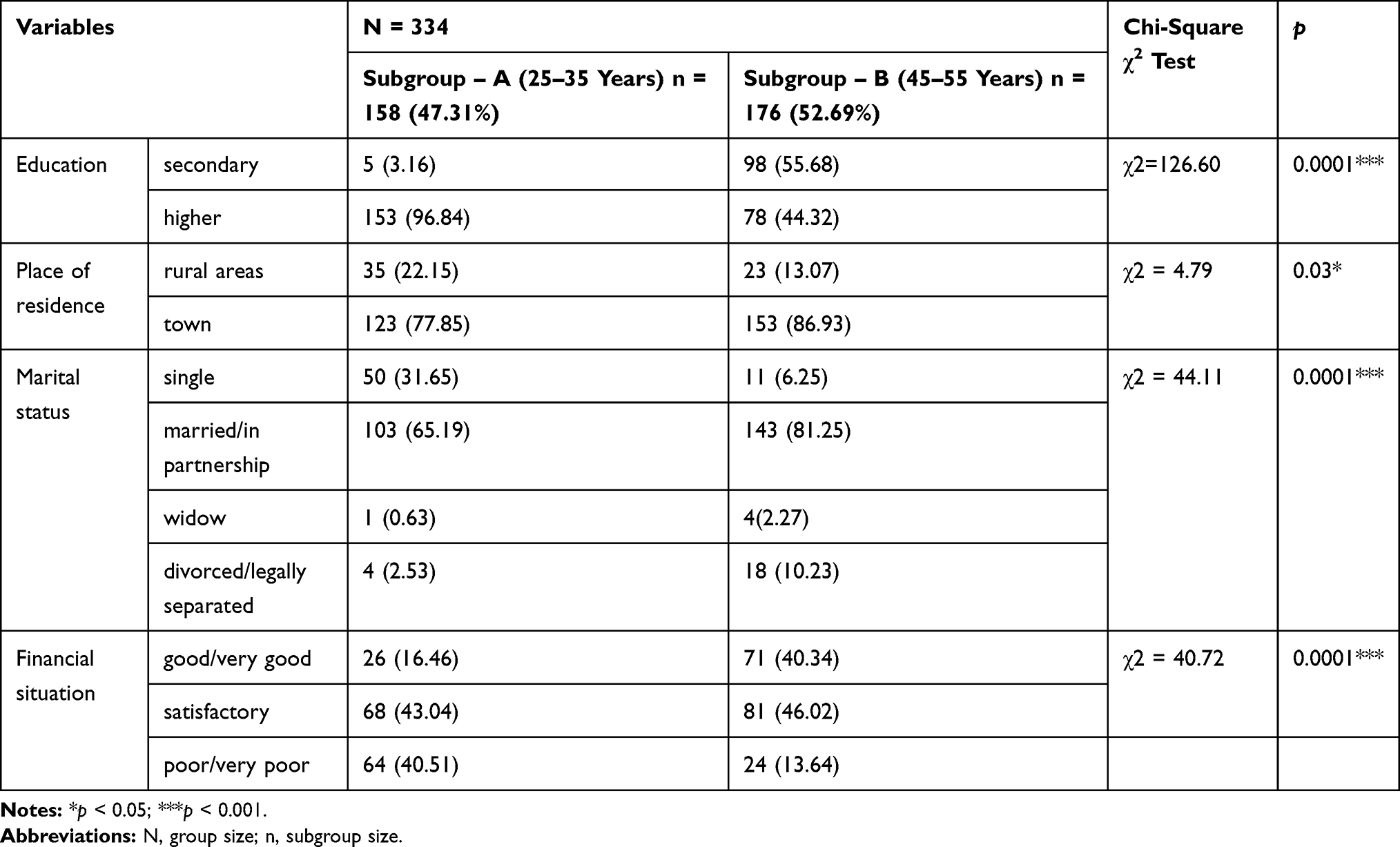 |
Table 1 Characteristics of the Examined Group |
Research Instruments
A diagnostic survey was used as a research method and two research tools, validated in the Polish language version, were used to collect data.
- The WHOQoL-Bref questionnaire, in the Polish adaptation by L. Wołowicka and K. Jaracz23
- The Menopause Symptom List (MSL) by J.M Perz, in the Polish version known as “Moje samopoczucie” (“My wellbeing”), by E. Bielawska-Batorowicz.9
A self-constructed questionnaire, which referred to age, education, place of residence, marital status and financial situation, was used to collect sociodemographic data.
WHOQoL-Bref Questionnaire
The WHOQoL-Bref (World Health Organization Quality of LifeTest-Bref) questionnaire was prepared based on the WHOQoL-100 questionnaire from the World Health Organization. It can be used to assess the quality of life of healthy and sick persons. It contains 26 questions analyzing four domains of life: somatic (7 questions), psychological (6 questions), social relations (3 questions), environmental (8 questions) and two questions aimed at determining satisfaction with the overall quality of life and satisfaction with the overall quality of health. In the somatic domain, an assessment was made of: everyday activities, dependence on drugs and treatments, energy and fatigue, mobility, pain and discomfort, rest and sleep, ability to work; in the psychological domain: appearance, negative feelings, positive feelings, self-esteem, spirituality, religion, personal faith, thinking, learning, memory, concentration; in the social relationships domain: personal relationships, social support, sexual activity; in the environmental field: financial resources, freedom, physical and mental safety, health and health care (accessibility and quality), home environment, opportunities to acquire new information and skills, opportunities and participation in recreation and leisure, physical environment (pollution, noise, traffic, climate), transport. The respondents were asked to mark their answer for each question on a five-point Likert scale (from 1 to 5). The direction of the score for the questions is positive – the higher the score, the better the quality of life.24 The WHOQoL-Bref questionnaire has good psychometric properties and the reliability of the Polish version is similar to the original. Cronbach’s alpha coefficient for individual domains ranged from 0.69 to 0.81, while for the entire questionnaire it was 0.90.23
Menopause Symptom List (MSL) – “My Wellbeing”
The “My wellbeing” questionnaire is used to measure the frequency and intensity of menopausal symptoms in women aged 45–55. It contains 25 statements which describe the menopausal symptoms, forming three subscales: I - psychological symptoms (9 statements), II–vasomotor symptoms (9 statements), III - somatic symptoms (7 statements). In the psychological symptoms sub-scale, the following are assessed: irritability, depressive feelings, excitability, feeling of tension, mood swings, outbursts of crying, worrying for no reason, bad concentration, tension or pressure in the head or other parts of the body; in the vasomotor symptoms sub-scale: numbness and tingling, lack of feeling in the hands and feet, hot flashes, sweating, lack of appetite, lack of breath, palpitations, burning eyes, cold hands and feet; the somatic symptoms subscale: gaining weight, dyspareunia, insomnia, loss of sexual interest, early waking up in the morning, constipation and headaches. The questions refer to the existing symptoms, and the respondents were asked to mark one answer that was most appropriate for them on each line on a six-point Likert scale, choosing a number from 0 to 5. The larger the number, the more intense the experience of the symptom. For frequency assessment, the following meanings were assigned to the specific points of the scale: (0) never - not once in the last 3 months; (1) rarely - once or twice in the last 3 months; (2) sometimes - about 5 times; (3) often – between 5 and 10 times; (4) very often – more than 10 times in the last 3 months; (5) almost always – almost daily in the last 3 months. In the assessment of intensity, the meaning of the scale points was as follows: (0) not applicable - the sensation did not occur; (1) slight - barely noticeable change or sensation; (2) small - minor change, sensation of low intensity; (3) moderate - a clear change/sensation; (4) large - very significant change, an intense sensation; (5) very large, radical change, it is difficult to get a more intense sensation. Statements forming subscales were also assigned weights: if the factor loads of the given statement were greater than 0.7, weight = 2 was assigned, if they were less than 0.7, weight = 1. The score in the subscales was calculated by multiplying the points assigned to each statement by its weight and then added up. The reliability rate of the Polish version, which was titled “Moje samopoczucie” (“My wellbeing”), is high. The values of Cronbach’s alphas in all three subscales range from 0.70 to 0.87 and indicate satisfactory internal consistency.9
Statistical Analysis
The statistical analysis of the data was conducted using the Polish version of STATISTICA 13 (TIBCO, Palo Alto, CA, USA).
Descriptive statistics (arithmetic mean, standard deviation, median, minimum, maximum) were used in statistical analyses. A confidence interval of ±95% was assumed for the mean value and the chi-square (χ2) test for independence was used to examine the distribution of characteristics between nominal (categorical) variables. Student’s t-test (t) for independent samples was used to compare the quality of life of women in the 25–35 and 45–55 age groups. The ANOVA (F) test was used to assess the variation in the values of the investigated characteristics, including the frequency and intensity of menopausal symptoms in women aged 45–55 years. A Bonferroni post hoc test was applied to examine the differences between groups of menopausal symptoms and the Pearson correlation coefficient was used to analyze the linear relationship of quantitative variables. The strength of the relationship between the variables was interpreted based on Guilford’s classification assuming the following values: |r| = 0 - no correlation; 0.0 < |r| ≤ 0.1 - slight correlation; 0.1 < |r| ≤ 0.3 - low correlation; 0.3 < |r| ≤ 0.5 - average correlation; 0.5 < |r| ≤ 0.7 - high correlation; 0.7 < |r| ≤ 0.9 - very high correlation; 0.9 < |r| < 1.0 - almost full correlation; |r| = 1 - full correlation.25 A significance level of p < 0.05 was assumed.
Results
Differentiation of the Quality of Life in the Examined Groups – A Comparative Analysis
Student’s t-test was used to compare the quality of life of nurses from subgroups A and B. The obtained results indicate significant differences in the general quality of health of the examined nurses, as well as in the quality of life in the somatic health and environmental domain. Nurses aged 25–35 in the full reproductive period achieved a significantly (p < 0.02) higher level of satisfaction with the overall health quality (M = 3.9; SD = ±0.7) than nurses from the menopausal group, aged 45–55 years (M = 3.7; SD = ±0.7).
However, further analyses showed that nurses in the younger age group obtained lower scores in the assessment of the quality of life in the somatic health domain (M = 12.5; SD = ±1.6 vs M = 13.2; SD = ±1.7) at significance level of p < 0.0003 and environmental domain (M = 13.4; SD = ±2.3 vs M = 14.1; SD = ±2.0) at a significance level of p < 0.003 than nurses in the menopausal group (Table 2). This means that, despite their young age, nurses perceive their physical condition and being in their environment worse than nurses experiencing menopausal symptoms. Interestingly, no significant differences were found between the groups studied in terms of the quality of life in the psychological and social relations’ domains. However, the results obtained prompt researchers to continue further scientific exploration in this area.
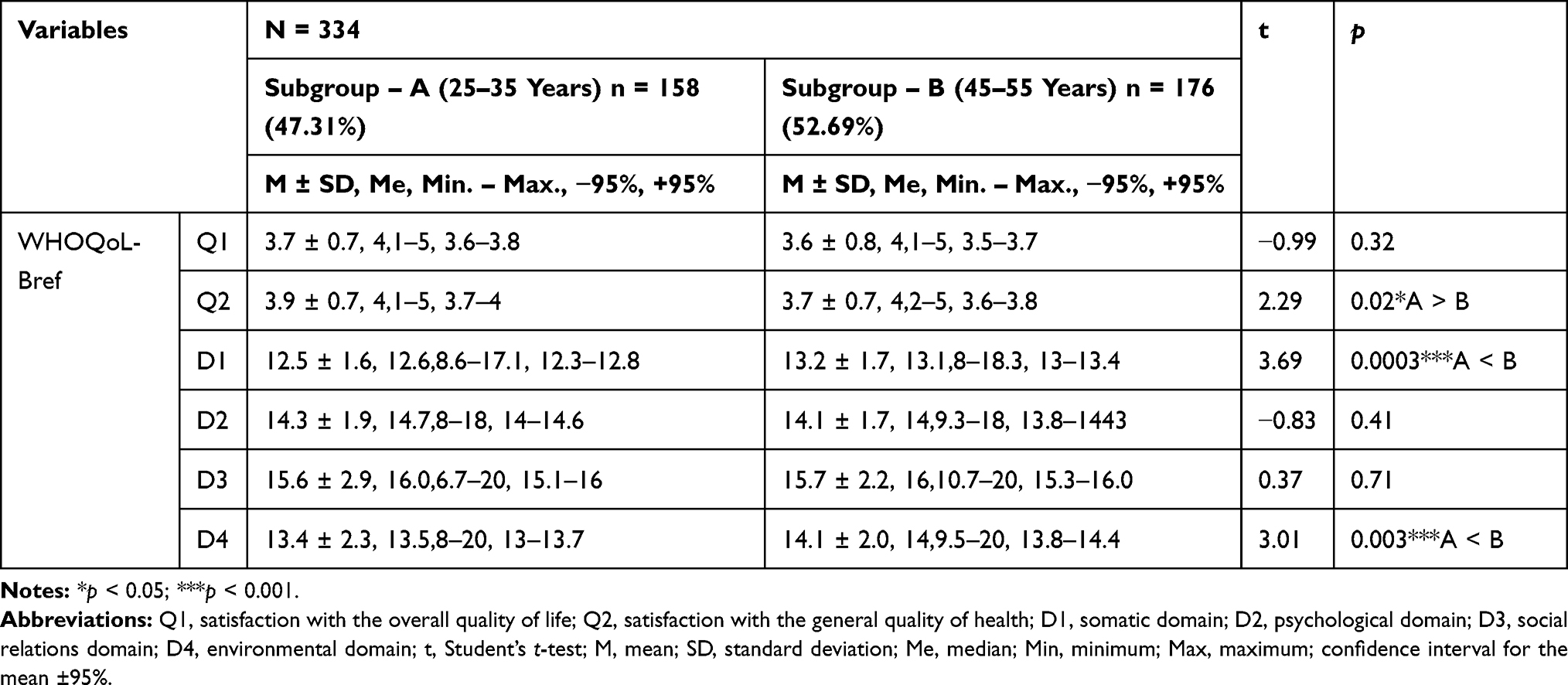 |
Table 2 Quality of Life of Nurses – Results of the Significance Test for Differences Taking into Account the Grouping Variable – the Age of Respondents |
Analysis of the Frequency and Intensity of Menopausal Symptoms in Nurses Aged 45–55 Years
In subsequent analyses, the ANOVA test with repeated measurements was used to determine the variety of menopausal symptoms in nurses aged 45–55 years who did not use hormone replacement therapy, taking into account the frequency and intensity of symptoms. The analysis of variance indicates significant variation (F = 62.64; p < 0.0001) in the frequency of psychological, vasomotor and somatic symptoms (Table 3). As a result of the analyses conducted with the post hoc test, it was found that the frequency of psychological symptoms in the studied group was significantly higher than that of vasomotor (p < 0.0001) or somatic symptoms (p < 0.0001) (Table 3; Figure 1).
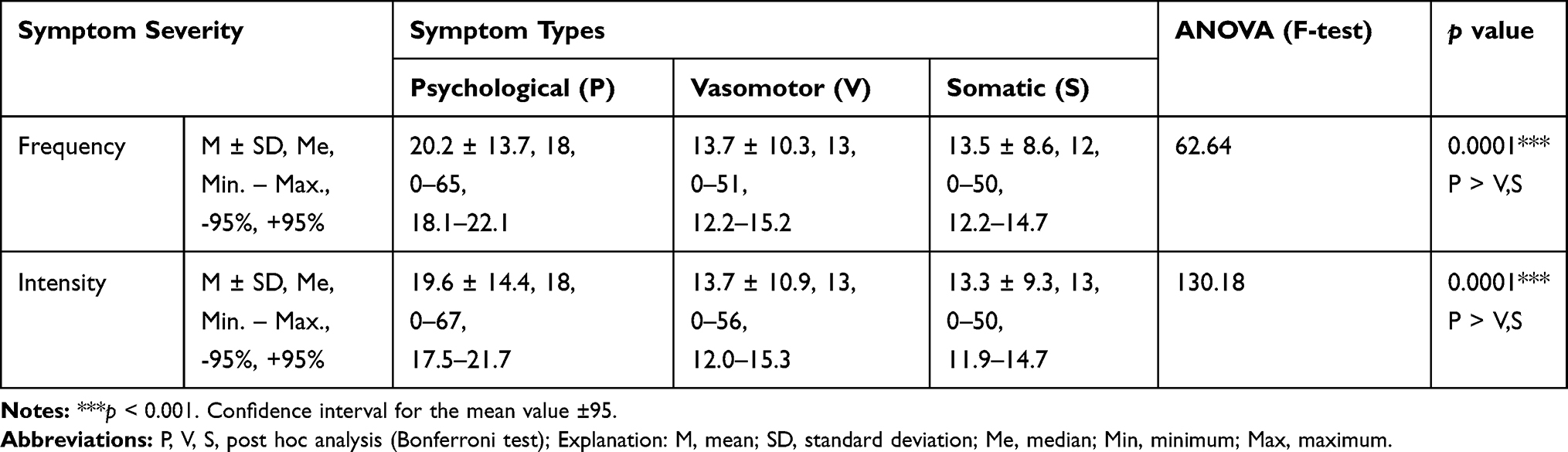 |
Table 3 Frequency and Intensity of Menopausal Symptoms in Nurses Aged 45–55 Years |
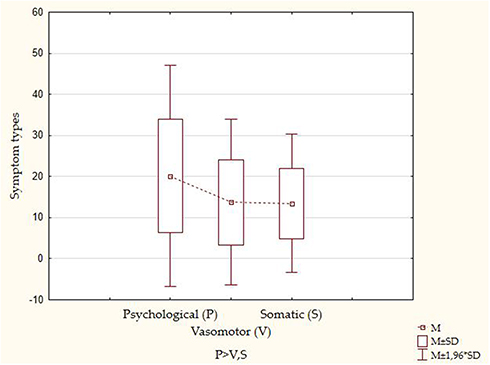 |
Figure 1 Comparison of the mean results of menopausal symptoms frequency in nurses aged 45–55 years. |
For the intensity of menopausal symptoms, the analysis of variance also revealed significant differences (F = 130.18; p < 0.0001) between psychological, vasomotor and somatic symptoms (Table 3). The post hoc test proved that the intensity of psychological symptoms in nurses aged 45–55 years was significantly higher than vasomotor (p < 0.0001) and somatic (p < 0.0001) symptoms (Table 3; Figure 2). No statistically significant differences were found, however, in the intensity of menopausal symptoms of a vasomotor or somatic nature.
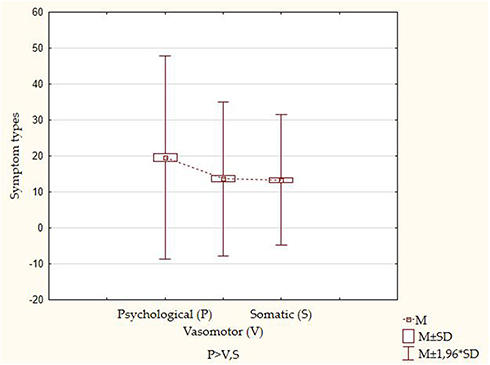 |
Figure 2 Comparison of the mean results of menopausal symptoms intensity in nurses aged 45–55 years. |
Relationships Between the Frequency and the Intensity of Menopausal Symptoms and the Quality of Life of Nurses Aged 45–55 Years
The Pearson correlation coefficient was used to search for the existence or absence of a relationship between the intensity and frequency of menopausal symptoms experienced and the quality of life of nurses aged 45–55 years, while determining the strength and the direction of the relationship. The correlation coefficients presented in Figures 3 and 4 indicate that the frequency and intensity of psychological, vasomotor and somatic symptoms are significantly related to the overall quality of life and health of the examined nurses and significantly related to the four quality of life domains, ie somatic, psychological, social and environmental relations. The interpretation of the strength of the relationship between variables is based on Guilford’s classification. All observed relationships (Figures 3 and 4) are negative and range from r = −0.19 to r = −0.48, which means that the higher the frequency and intensity of menopausal symptoms, the lower the quality of life of nurses and vice versa.
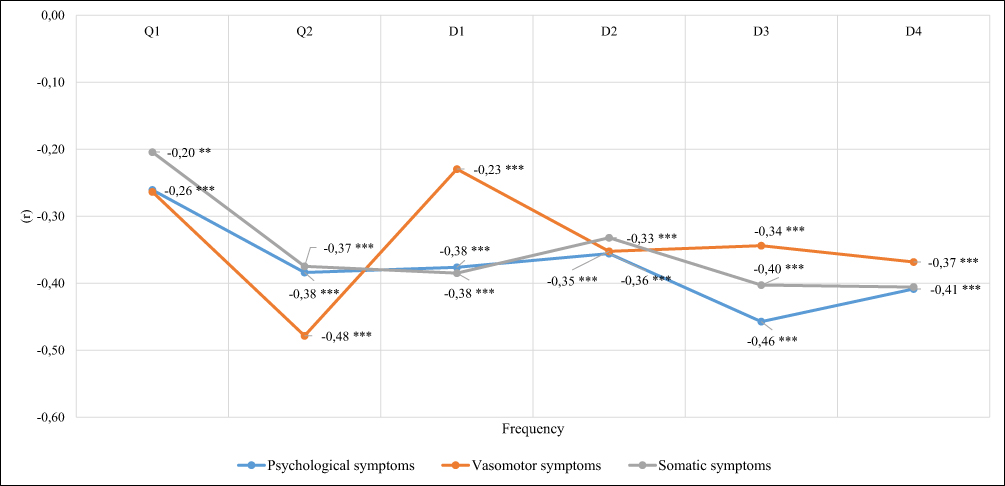 |
Figure 3 The frequency of menopausal symptoms and the quality of life of the examined nurses – Pearson correlation coefficients. Abbreviations: Q1, satisfaction with the overall quality of life; Q2, satisfaction with the overall quality of health; D1, somatic domain; D2, psychological domain; D3, social relations domain; D4, environmental domain. Notes: *p < 0.05; **p < 0.01; ***p < 0.001. |
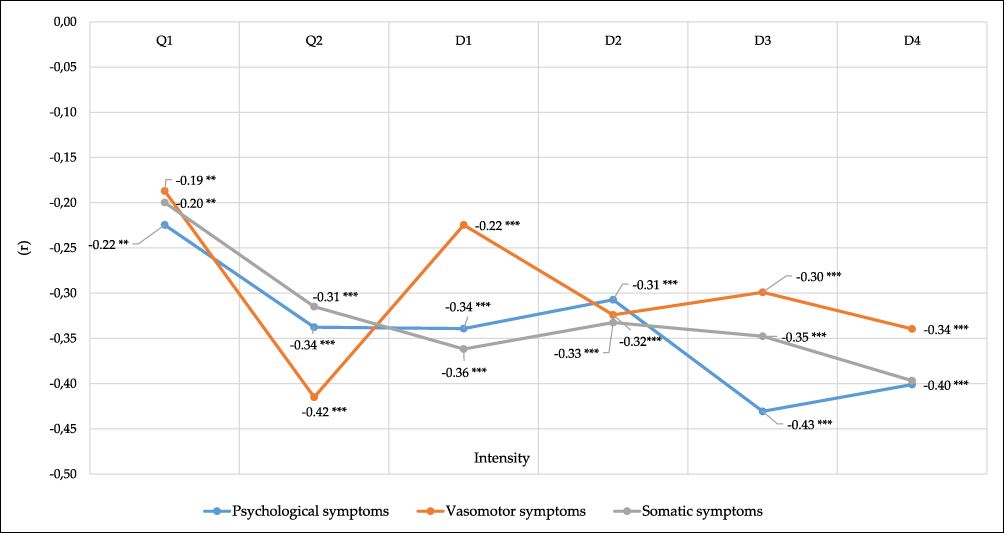 |
Figure 4 The intensity of menopausal symptoms and the quality of life of the examined nurses – Pearson correlation coefficients. Abbreviations: Q1, satisfaction with the overall quality of life; Q2, satisfaction with the overall quality of health; D1, somatic domain; D2, psychological domain; D3, social relations domain; D4, environmental domain. Notes: *p < 0.05; **p < 0.01; ***p < 0.001. |
In analyzing the correlations between the discussed variables, negative relationships of average strength were observed between the frequency of vasomotor symptoms and satisfaction with the general quality of health (r = −0.48), psychological symptoms and quality of life in the social (r = −46) and environmental (r = −0.41) domains, as well as somatic symptoms and quality of life in the environmental (r = −0.41) domain (Figure 3). Subsequent analyses revealed correlations between the intensity of menopausal symptoms and the quality of life of the nurses studied. These are also negative relationships, with average strength, between vasomotor symptoms and satisfaction with general health (r = −0.42), psychological symptoms and the quality of life in the environmental domain (r = −0.40) and somatic symptoms and the quality of life in the environmental domain (r = −0.40) (Figure 4). The details are presented in Figures 3 and 4.
Discussion
The quality of life of nurses in the study varies. Nurses from the 25–35 age group achieved a significantly higher level of satisfaction with their overall quality of health than nurses from the 45–55 age group experiencing menopause symptoms. As the literature review shows, the results of numerous studies confirm that menopause is one of the most important problems for women’s reproductive health and that menopausal symptoms have a negative impact on women’s quality of life.26,27 Makara-Studzińska et al in an intercontinental review indicate that women worldwide suffer from menopausal problems regardless of their ethnic origin, skin color or socio-demographic factors.28 Gracia and Freeman showed that it is important to determine whether the symptoms are mainly related to the menopause temporarily and therefore likely to be limited in time or whether the symptoms are a continuum of medical or mental illness.29 To support this thesis, it is worth referring to the work of Italian researchers who focused on examining the potential role of the post-menopausal period in sleep-related respiratory disorders. By analyzing gender differences in prevalence, pathogenesis and clinical features of sleep apnea, the authors indicate, inter alia, the role of sex hormones in this condition.30
In the authors’ own research presented in this paper, quite surprising results were obtained concerning the quality of life of nurses in the somatic and environmental domains. It was found that nurses from the younger age group (25–35 years) achieved significantly lower quality of life results in the somatic and environmental domain than the nurses from the perimenopausal group (45–55 years). A reduction in the quality of life of women aged 25–35 may be associated with performing multiple life roles (starting a family, bringing up children, building a career, etc.). Mishra and Kuh presented interesting research results in a group of British women. The researchers observed that women who were in the perimenopausal period for only one year experienced a significant decline in their quality of life, particularly in the physical and psychosomatic spheres, as compared to pre-menopausal women.31
In the authors’ own research, nurses from the 45–55 age group described the frequency and intensity of psychological menopause symptoms to be higher than those of a vasomotor and somatic nature. It can be concluded that for nurses, in view of the nature of their work associated with caring for people in health and illness, this represents an additional burden, particularly in the mental sphere, which nurses have to face. According to Castiglione et al, women in menopause are more afraid of future changes in their body and have more negative expectations regarding their own body image than those not yet in the menopausal period.32
The authors of the current study did not find statistically significant differences between the frequency and intensity of vasomotor and somatic symptoms in the examined group.
Other researchers also referred to the severity of psychological symptoms. They proved that as a result of hormonal changes, women experienced increased irritability, depressive moods and higher levels of anxiety. Depressive disorders were more common in women with a family history of affective or mental disorders, with previous mood disorders, at risk of stress, health and/or family problems, with early childhood trauma.19,33,34 Vasomotor symptoms are another group of troublesome symptoms for women in the perimenopausal period. According to Avis et al, vasomotor symptoms are one of the main menopause-related problems for which women in the United States seek medical treatment. The above-mentioned researchers showed that the majority of women assess the severity of vasomotor symptoms as moderate to severe.32 Risk factors for the occurrence of vasomotor symptoms include smoking, higher levels of anxiety and depression, lower levels of education and premenstrual syndrome.35 Krajewska-Ferishah et al in their international research identified certain differences between menopausal complaints reported by women from Belgium, Belarus, Greece and Poland. Belgian women demonstrated a lower quality of life due to a higher rate and severity of symptoms of the genitourinary and reproductive system.36
Makara-Studzińska et al indicate an alarmingly high incidence of menopausal symptoms in African women. Additionally, they report that women participating in the research in the United States complained most often about muscle and joint pain, while women from Australia suffered mainly from vasomotor symptoms and sexual dysfunctions. On the other hand, women from South America mainly reported symptoms of depression, sexual dysfunction and discomfort associated with muscle and joint pain. A worrying increase in the proportion of women reporting depressive disorders was observed in the examined group of Asian women. Similarly, in Europe, sleep disorders and depressive disorders were much more prevalent in the perimenopausal period in the examined women.28 Dasgupta and Ray tried to determine, in a group of 1400 Indian women, whether the post-menopausal condition is related to women’s attitudes towards menopause and ageing. It was demonstrated that post-menopausal women revealed a more positive attitude towards menopause and ageing than women in the perimenopausal period.37 In the research carried out by Kling et al on a group of 1884 women, a relationship was sought between the symptoms of menopause as measured by the Menopause Rating Scale and the stress in the relationship measured with the Kansas Marital Satisfaction Scale. It was discovered that women living in a harmonious relationship had less severe symptoms of menopause, especially in the psychological sphere, as compared to women reporting distress in their relationship.38 In the authors’ own studies, a statistically significant negative linear relationship of different strength (ranging from r = −0.19 to r = −0.48) was observed between the frequency and the intensity of menopausal symptoms in the group of psychological, vasomotor, somatic symptoms and the overall quality of life and health and the quality of life in the somatic, psychological, social and environmental domains. This means that when the frequency and the intensity of the menopausal symptoms in the examined nurses assume higher values, the quality of life of nurses in all domains of functioning deteriorates. Similarly, Bień et al and Wieder-Hulsza et al showed in their studies that the severity of menopausal symptoms significantly contributes to a decrease in women’s quality of life.39,40 Quiroga et al observed a moderating effect of the quality of sex life on the established correlation between depression and the intensity of menopausal symptoms.41 In turn, other Polish studies conducted by Bączek et al showed that women with menopausal symptoms were more often, and more severely, affected by a lower quality of life, lower self-esteem and a higher predisposition to depression.42 The examined women also showed the need for education on physiological changes during menopause, possible disorders and methods of dealing with them.42 Ambroziak and Bielawska-Batorowicz, carrying out a psycho-educational program for women aged 48–54 years, observed that it significantly changed the intensity of menopausal symptoms and attitudes of women towards menopause.43 Many researchers suggest that health-related behavior determines the quality of women’s health and life and also affects menopausal problems.35,36,44 Quinn and Cedars point out that positive health behaviors, ie stopping smoking, maintaining a healthy weight and reducing alcohol consumption, are important for optimizing fertility and overall health condition.36
Limitations and Implications for Professional Practice
The presented results of own research have certain limitations. The research focused only on one professional group (nurses) in two age groups. In an attempt to introduce the general issue of the quality of life of nurses in the reproductive and perimenopausal spheres, the authors limited the scope of the study, for example, they did not obtain data describing whether the nurses in the study group were treated for chronic diseases. The analysis of the own research results and their comparison with the results obtained by other researchers indicates the need to create conditions for the implementation of health-promoting interventions targeted at the health needs of professionally active nurses in the perimenopausal age group. Among the many possible ways of influencing the population, in addition to educational campaigns, it is important to implement programs on the promotion of physical activity, the creation of healthy employment conditions for nurses and the promotion of mental health.
Conclusions
- The quality of life of the examined nurses varies, and in the 45–55 age group, it is significantly negatively connected with the frequency and intensity of menopausal symptoms.
- A higher level of satisfaction with the overall quality of health is presented by nurses from the 25–35 age group in the full reproductive period than by nurses from the 45–55 age group, while nurses experiencing menopausal symptoms evaluate the quality of life in the somatic and environmental health domains much higher than nurses in the reproductive age group.
- Nurses in the perimenopausal period significantly more often and intensively experience menopausal symptoms of a psychological nature than vasomotor or somatic symptoms.
- Nurses in the 45–55 age group, with an increasing frequency and intensity of menopausal symptoms, report a significantly lower quality of life in the somatic, mental, social and environmental domains.
Funding
The following work is a part of a research project, financed by the University of Warmia and Mazury in Olsztyn (No 63-610-001), Poland.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Trzebiatowski J. Jakość życia w perspektywie nauk społecznych i medycznych – systematyzacja ujęć definicyjnych [Quality of life in the perspective of social and medical sciences – classification of definitions]. Hygeia Public Health. 2011;46(1):25–31.
2. Kupcewicz E, Grochans E, Kadučáková H, et al. Analysis of the relationship between stress intensity and coping strategy and the quality of life of nursing students in Poland, Spain and Slovakia. Int J Environ Res Public Health. 2020;17:4536. doi:10.3390/ijerph17124536
3. Kupcewicz E, Jóźwik M. Role of global self-esteem, professional burnout and selected socio-demographic variables in the prediction of polish nurses’ quality of life - a cross-sectional study. Risk Manag Healthc Policy. 2020;13:671–684. doi:10.2147/RMHP.S252270
4. The World Health Organization quality of life assessment (WHOQOL). Position paper from the world health organization. Soc Sci Med. 1995;41(10):1403–1409.
5. Schipper H. Quality of life: principles of the clinical paradigm. J Psychosocial Oncol. 1990;8(23):171–185. doi:10.1300/J077v08n02_09
6. Matusiak-Kita M, Zdrojewicz Z. Seksualność kobiet w ciąży, w okresie poporodowym i karmienia piersią. Prz Seksuol. 2010;6(1):12–16.
7. World Health Organization. Research on the Menopause in the 1990s: Report of a WHO Scientific Group. Geneva: World Health Organization; 1996.
8. Souza Guerra GE. Quality of life in climacteric women assisted by primary health care. PLoS One. 2019;14(2):e0211617. doi:10.1371/journal.pone.0211617
9. Bielawska-Batorowicz E. Moje samopoczucie – polska adaptacja kwestionariusza menopause symptom list Janette M. Perz. [My Wellbeing - Polish adaptation of the Menopause Symptom List by Janette M. Perz]. Acta Universitati Lodziensis Folia Psychologica. 2004;8:45–54.
10. Blümel JE, Chedraui P, Baron G, et al. Collaborative group for research of the climacteric in latin america (REDLINC). A large multinational study of vasomotor symptom prevalence, duration, and impact on quality of life in middle-aged women. Menopause. 2011;18(7):778–785. doi:10.1097/gme.0b013e318207851d
11. Medeiros de Morais MS, Andrade Do Nascimento R, Vieira MCA. Does body image perception relate to quality of life in middle-aged women? PLoS One. 2017;12(9):e0184031. doi:10.1371/journal.pone.0184031
12. Maheshwari PK, Agrawal P, Garg R, et al. Understanding climacteric depression and depression in other phases of women’s life. JSAFMS. 2015;3(1):20–23. doi:10.5005/jp-journals-10032-1064
13. Vesco KK, Haney EM, Humphrey L, et al. Influence of menopause on mood: A systematic review of cohort studies. Climacteric. 2007;10:448–465. doi:10.1080/13697130701611267
14. Avis NE, Crawford SL, Greendale G, et al. Study of Women’s Health Across the Nation. Duration of menopausal vasomotor symptoms over the menopause transition. JAMA Intern Med. 2015;175(4):531–539. doi:10.1001/jamainternmed.2014.8063
15. Kaczmarek M. The timing of natural menopause in Poland and associated factors. Maturitas. 2007;57:139–153. doi:10.1016/j.maturitas.2006.12.001
16. Zamaniyan M, Moosazadeh M, Peyvandi S, et al. Age of natural menopause and related factors among the tabari cohort. J Menopausal Med. 2020;26(1):18–23.
17. Ding X, Tang R, Zhu J, et al. An appraisal of the role of previously reported risk factors in the age at menopause using mendelian randomization. Front Genet. 2020;11:507. doi:10.3389/fgene.2020.00507
18. Burger HG. Physiology and endocrinology of the menopause. J Steroid Biochem Mol Biol. 2006;34(1):27–30.
19. Czarnecka-Iwańczuk M, Stanisławska-Kubiak M, Mojs E, et al. Objawy menopauzy a satysfakcja z życia i samoocena wśród kobiet [Menopause symptoms versus life satisfaction and self-esteem among women]. Prz Menopauz. 2012;6:468–473. doi:10.5114/pm.2012.32539
20. Ksykiewicz-Dorota A. Zarządzanie w pielęgniarstwie [Nursing Management]. Wyd. Czelej, Lublin, 2005;421–463, Poland
21. Viselita F, Handiyani H, Pujasari H. Quality level of nursing work life and improvement interventions: systematic review. Enfermería Clínica. 2019;29(2):223–228. doi:10.1016/j.enfcli.2019.06.001
22. Vandenbroucke JP, von Elm E, Altman DG, et al. Strengthening the reporting of observational studies in epidemiology (strobe): explanation and elaboration. Int J Surg. 2014;12:1500–1524. doi:10.1016/j.ijsu.2014.07.014
23. Jaracz K, Kalfoss M, Górna K, et al. Quality of life in Polish respondents: psychometric properties of the Polish WHOQOL-Bref. Scand J Caring Sci. 2006;20(3):251–260. doi:10.1111/j.1471-6712.2006.00401.x
24. WHOQOL: measuring Quality of Life. Available from: https://www.who.int/toolkits/whoqol.
25. Szymczak W. Podstawy statystyki dla psychologów [Fundamentals of Statistics for Psychologists]. Wyd. Difin, Warszawa, 2018. Poland
26. Ghorbani R, Nassaji M, Shahbazi A, et al. Association between quality of life, menopausal status, and sociodemographic factors among middle-aged women in Iran. J Egypt Public Health Assoc. 2017;12(9):166–170. doi:10.1371/journal.pone.0184031
27. Namazi M, Sadeghi R, Behboodi Moghadam Z. Social determinants of health in menopause: an integrative review. Int J Womens Health. 2019;9(11):637–647. doi:10.2147/IJWH.S228594
28. Makara-Studzińśka MT, Kryś-Noszczyk KM, Jakiel G. Epidemiology of the symptoms of menopause - an intercontinental review. Prz Menopauz. 2014;13(3):203–211. doi:10.5114/pm.2014.43827
29. Gracia CR, Freeman EW. Onset of the menopause transition: the earliest signs and symptoms. Obstet Gynecol Clin N Am. 2018;45(40):585–597. doi:10.1016/j.ogc.2018.07.002
30. Perger E, Mattaliano P. Menopause and sleep apnea. Maturitas. 2019;124:35–38. doi:10.1016/j.maturitas.2019.02.011
31. Mishra G, Kuh D. Perceived change in quality of life during the menopause. Soc Sci Med. 2006;62(1):93–102. doi:10.1016/j.socscimed.2005.05.015
32. Castiglione C, Licciardello O, Rampullo A. Possible future changes in menopausal women. Life Span Disability. 2015;18(2):189–205.
33. Amore M, Di Donato P, Papalini A, et al. Psychological status at the menopausal transition: an Italian epidemiological study. Maturitas. 2004;48:115–124. doi:10.1016/j.maturitas.2003.08.010
34. Maartens LW, Knottnerus JA, Pop VJ. Menopausal transition and increased depressive symptomatology: a community based prospective study. Maturitas. 2002;42:195–200. doi:10.1016/S0378-5122(02)00038-5
35. Avis NE, Crawford SL, Green R. Vasomotor symptoms across the menopause transition: differences among women. Obstet Gynecol Clin N Am. 2018;45(4):629–640. doi:10.1016/j.ogc.2018.07.005
36. Krajewska-Ferishah K, Krajewska-Kułak E, Terlikowski S, et al. Analysis of quality of life of women in menopause period in poland, greece, belarus and belgium using mrs scale. A multicenter study. Adv Med Sci. 2010;55(2):191–195. doi:10.2478/v10039-010-0042-3
37. Dasgupta D, Ray S. Is menopausal status related to women’s attitudes toward menopause and aging? Women Health. 2017;57(3):311–328. doi:10.1080/03630242.2016.1160965
38. Kling JM, Kelly M, Rullo J, et al. Association between menopausal symptoms and relationship distress. Maturitas. 2019;130:1–5. doi:10.1016/j.maturitas.2019.09.006
39. Bień A, Rzońca E, Iwanowicz-Palus G, et al. The influence of climacteric symptoms on women’s lives and activities. Int J Environ Res Public Health. 2015;12:3835–3846. doi:10.3390/ijerph120403835
40. Wieder-Hulsza S, Szkup M, Jurczak A, et al. Effects of socio-demographic, personality and medical factors on quality of postmenopausal women. Int J Environ Res Public Health. 2014;11:6692–6708. doi:10.3390/ijerph110706692
41. Quiroga A, Larroy C, González-Castro P. Climacteric symptoms and their relation to feminine self-concept. Climacteric. 2017;20(3):274–279. doi:10.1080/13697137.2017.1310192
42. Bączek G, Wierzba W, Tataj-Puzyna U, et al. Jakość życia kobiet w okresie okołomenopauzalnym [Quality of life of women in perimenopausal]. Med Og Nauk Zdr. 2019;25(4):258–265. doi:10.26444/monz/114666
43. Ambroziak E, Bielawska Batorowicz E. Can the intensity of menopausal symptoms be modified? The pilot study of the effects of an intervention programme designed for 48–54 year old women. Prz Menopauz. 2011;10:58–62.
44. Pilewska-Kozak AB, Dobrowolska B, Stadnicka G, et al. Place of residence and age as variables differentiating health behaviors and perception of health by women past menopause. Ann Agric Environ Med. 2019;26(1):165–173. doi:10.26444/aaem/102496
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.