Back to Journals » Clinical Interventions in Aging » Volume 20
Relationship Between Cognitive Ability and Phase Angle in Older Adults with Cardiovascular Disease: A Cross-Sectional Study
Authors Peng H ![]() , Huang J, Qiu Y, Fang H
, Huang J, Qiu Y, Fang H ![]() , Ye Q
, Ye Q
Received 8 March 2025
Accepted for publication 2 December 2025
Published 10 December 2025 Volume 2025:20 Pages 2505—2513
DOI https://doi.org/10.2147/CIA.S518961
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Huan Peng,1 Jie Huang,2 Yinwei Qiu,3 Han Fang,1 Qiang Ye1
1The Second School of Clinical Medicine, Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Geriatrics, The Second Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China; 3Zhejiang Provincial Center for Disease Control and Prevention, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Jie Huang, Department of Geriatrics, The Second Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, Zhejiang, 310005, People’s Republic of China, Email [email protected]
Background: Cognitive decline in older adults with Cardiovascular Disease (CVD) is frequently mediated by chronic inflammation, oxidative stress, and cellular dysfunction. However, reliable biomarkers for early detection are still lacking. Phase angle (PhA), a sensitive bioelectrical impedance analysis (BIA) parameter reflecting cellular health and nutritional status, may serve as a novel tool for detecting cognitive impairment in this population.
Methods: In this cross-sectional study, 340 CVD patients (mean age: 80.8 ± 8.0 years; 36.5% male) were recruited from the Zhejiang Elderly Health Monitoring Cohort. PhA was measured using the InBody S10. Participants were stratified into cognitive impairment (n = 138) and cognitively normal (n = 202) groups based on Mini-Mental State Examination (MMSE) scores adjusted for education level. Group differences were analyzed via independent t-tests, Mann–Whitney U-tests, and chi-square tests. Binary logistic regression evaluated the association between PhA and cognitive ability.
Results: The cognitive impairment group exhibited significantly lower PhA (P < 0.001), older age, reduced grip strength, smaller calf circumference, slower gait speed (all P < 0.001), along with lower education levels and poorer physical activity intensity (both P< 0.01). Additionally, they demonstrated worse performance in activities of daily living, nutritional status, balance, and swallowing function, along with greater frailty severity (all P < 0.001). Multivariate analysis confirmed PhA as an independent predictor of cognitive ability after adjusting for age, education, physical activity, grip strength, gait speed, and calf circumference (β = − 0.474, OR = 0.62, 95% CI: 0.43– 0.89, P = 0.01). ROC curve analysis revealed an optimal PhA threshold of 4.75° for cognitive impairment detection (specificity: 70.3%).
Conclusion: Reduced PhA is independently associated with cognitive impairment risk in older CVD patients. Its noninvasive, cost-effective measurement supports its potential as a community screening tool and may provide a critical target for early intervention.
Keywords: cardiovascular disease, phase angle, cognitive impairment
Introduction
With the intensification of global population aging, the number of older cardiovascular disease (CVD) patients continues to rise. CVD remains one of the leading causes of global mortality and disability.1 Older CVD patients face elevated risks of cognitive impairment, driven by multidimensional pathological interactions.2–4 First, atherosclerosis and chronic heart failure lead to cerebral hypoperfusion, accelerating white matter lesions and hippocampal atrophy.5 Second, elevated levels of circulating pro-inflammatory factors such as C-reactive protein (CRP) and interleukin-6 (IL-6) in CVD patients promote β-amyloid deposition by disrupting the blood-brain barrier and inducing neuronal apoptosis.6 Furthermore, insulin resistance, dyslipidemia, and cerebrovascular endothelial dysfunction synergistically exacerbate cerebral energy metabolism imbalance.5,7 These mechanisms not only independently impair cognitive function but also exhibit pathological overlap with neurodegenerative diseases,8 forming a vicious cycle of “heart-brain comorbidity”. Consequently, older CVD patients frequently experience cognitive decline, significantly compromising their quality of life and social independence. Early identification of CVD patients at risk of cognitive impairment is therefore critically important.
The phase angle (PhA), a key parameter derived from bioelectrical impedance analysis (BIA), reflects cellular health, nutritional status, and overall bodily function.9 Lower PhA values typically indicate compromised cell membrane integrity and abnormal fluid balance, whereas higher values correlate with better cellular function and health status.10 In recent years, PhA has been widely applied in assessing body composition, nutritional status, and prognosis in chronic disease populations.11–13 A meta-analysis indicates that PhA, as a sensitive biomarker of cellular health and metabolic status, is inversely correlated with inflammatory markers in individuals with CVDs.14 Systemic inflammation and sodium-water retention commonly observed in CVD patients can alter cellular membrane impedance, significantly reducing PhA values.15 Chronic inflammation and oxidative stress play pivotal roles in both cardiovascular and neurodegenerative diseases.16,17 Reactive oxygen species (ROS) generated through oxidative stress can not only damage cell membranes and reduce PhA,10,18 but also promote β-amyloid and tau protein deposition—hallmark pathological features of Alzheimer’s disease.19 Additionally, cardiac cachexia and medication side effects contribute to muscle mass loss and malnutrition, both associated with lower PhA values.20 These factors may further impact cerebral structure and function, thereby influencing cognitive capacity.21
Therefore, PhA not only reflects the systemic metabolic status of CVD patients but may also exhibit specific associations with cognitive ability through these mechanisms, positioning it as an ideal biomarker for cognitive risk screening in this population. However, the relationship between PhA and cognitive ability in older CVD patients remains insufficiently investigated. This study aims to explore the association, providing new insights for early identification of cognitive impairment risk in this population and informing targeted prevention and intervention strategies.
Materials and Methods
Study Design and Participants
This cross-sectional study enrolled 340 older patients with CVD from the Zhejiang Elderly Health Monitoring Cohort between August 2022 and June 2024. Inclusion criteria: (1) age ≥60 years; (2) diagnosed with hypertension, coronary heart disease, heart failure, arrhythmia, or valvular heart disease according to World Health Organization (WHO) criteria; (3) ability to complete questionnaires and physical function assessments. Exclusion criteria: (1) severe psychiatric disorders or acute illnesses within the past 3 months; (2) implanted metal devices or pacemakers; (3) severe visual or auditory impairments; (4) refusal to participate. The study protocol was approved by the Medical Ethics Committee of the Second Affiliated Hospital of Zhejiang Chinese Medical University (Approval No. LGF21H250001), Written informed consent was obtained from all participants, and the study design and conduct strictly adhered to the principles of the Declaration of Helsinki and its subsequent amendments.
Demographic and Anthropometric Indicators
Demographic data, including age, sex, education level, marital status, living arrangement, and physical activity intensity, were collected through structured questionnaires. Anthropometric measurements were performed as follows: (1) Height: Measured using a wall-mounted stadiometer (RGZ-120), with participants standing barefoot and aligning their heads, shoulders, and heels with the measurement rod. Values were recorded to the nearest 0.1 cm. (2) Weight: Measured using a calibrated electronic scale with participants fasting, wearing light clothing, and barefoot, recorded to the nearest 0.1 kg. (3) BMI: Calculated as weight (kg) divided by height squared (m2), rounded to one decimal place. (4) Physical activity intensity was categorized into four levels according to the International Physical Activity Questionnaire guidelines as follows: sedentary activities, such as sitting or watching television; low-intensity activities, such as walking or household chores; moderate-intensity activities, such as brisk walking or dancing; and high-intensity activities, such as running or swimming.
Grip Strength, Gait Speed, and Calf Circumference
Trained researchers performed the following measurements: (1) Grip Strength: Measured using a calibrated dynamometer (CAMRY-EH101) with participants seated or standing, elbow flexed at 90°, forearm in neutral position, and wrist extended. Two consecutive measurements per side (1-minute interval), with the maximum value recorded. (2) Gait Speed: Calculated as 4-meter habitual walking speed (m/s), with 1-meter acceleration/deceleration zones. The average of two trials was recorded to two decimal places. (3) Calf Circumference: Measured at the maximal calf girth using a non-elastic tape (0.1 cm precision). Both sides were measured once, with the dominant side recorded to the nearest 0.1 cm.
Comprehensive Geriatric Assessment
Standardized assessments were conducted by geriatricians trained in protocol adherence: (1) Cognitive ability: Evaluated using the Mini-Mental State Examination (MMSE; total score 0–30). Cutoffs: >17 for illiteracy, >20 for primary education, >24 for junior high or above; scores below these thresholds indicated cognitive impairment. (2) Activities of Daily Living: Assessed via the Instrumental Activities of Daily Living (IADL) scale (total score 0–8): Independence (8 points), Mild dependence (5–7 points), Moderate dependence (2–4 points), Severe dependence (0–1 points). (3) Nutritional Status: Classified using the Mini Nutritional Assessment-Short Form (MNA-SF): 12–14 (normal), 8–11 (at risk), 0–7 (malnourished). (4) Balance Ability: Evaluated via the Berg Balance Scale (total score 0–56): 0–20 (severe impairment), 21–40 (moderate impairment), 41–56 (good-to-normal balance). (5) Frailty Status: Assessed using the Fried Frailty Phenotype (score 0–5): 0 (non-frail), 1–2 (pre-frail), ≥3 (frail). (6) Swallowing Function: Tested via the Kubota Water Swallowing Test (30 mL water): normal (swallowed within 5s without coughing), suspected impairment (>5s or split swallows without coughing), Abnormal (coughing or inability to swallow).
Body Composition Analysis
A multi-frequency bioelectrical impedance analyzer (InBody S10) was used to measure phase angle (PhA) and skeletal muscle index (SMI). PhA values were derived from whole-body impedance at 50 kHz.
Statistical Analysis
Data were analyzed using SPSS 27.0. Normality of continuous variables was assessed via the Kolmogorov–Smirnov test. Normally distributed data are presented as mean ± standard deviation (SD), compared using independent t-tests; non-normally distributed data as median (interquartile range) [M (Q1, Q3)], compared via Mann–Whitney U-tests. Categorical data are expressed as frequencies (percentages) and analyzed using chi-square (χ2) tests. Variables with P<0.1 in univariate analysis were included in binary logistic regression (forward stepwise method) to calculate odds ratios (ORs) and 95% confidence intervals (CIs). Predictive performance of independent factors was evaluated via receiver operating characteristic (ROC) curve analysis (area under the curve, AUC).
Results
Baseline Characteristics of the Study Population
A total of 340 CVD patients were included, with a mean age of 80.80 ± 8.02 years, of whom 36.5% (124/340) were male. Based on MMSE scores, participants were categorized into a cognitive impairment group (n = 138) and a cognitively normal group (n = 202). The analysis revealed significant differences between the two groups in age, education level, marital status, living environment, physical activity intensity, grip strength, gait speed, calf circumference, and PhA. Patients in the cognitive impairment group were significantly older (83.3 ± 6.8 vs 79.1 ± 8.3 years, P < 0.01) and had fewer years of education (P < 0.01). They exhibited a higher prevalence of widowhood (55.1% vs 33.2%, P<0.01) and institutionalized living arrangements (37.0% vs 13.9%, P<0.01). Sedentary behavior was more prevalent in the cognitive impairment group (6.5% vs 2.0%), while moderate-to-high-intensity physical activity was less frequent (P < 0.001). Additionally, the cognitive impairment group demonstrated significantly lower grip strength, slower gait speed, and smaller calf circumference (all P < 0.001). PhA values were markedly reduced in the cognitive impairment group [median (IQR): 4.3 (3.8, 4.9) vs 4.7 (4.2, 5.4), P < 0.001]. However, no statistically significant differences were observed between the two groups in sex, body mass index (BMI), or skeletal muscle index (SMI) (all P > 0.05). Details are presented in Table 1.
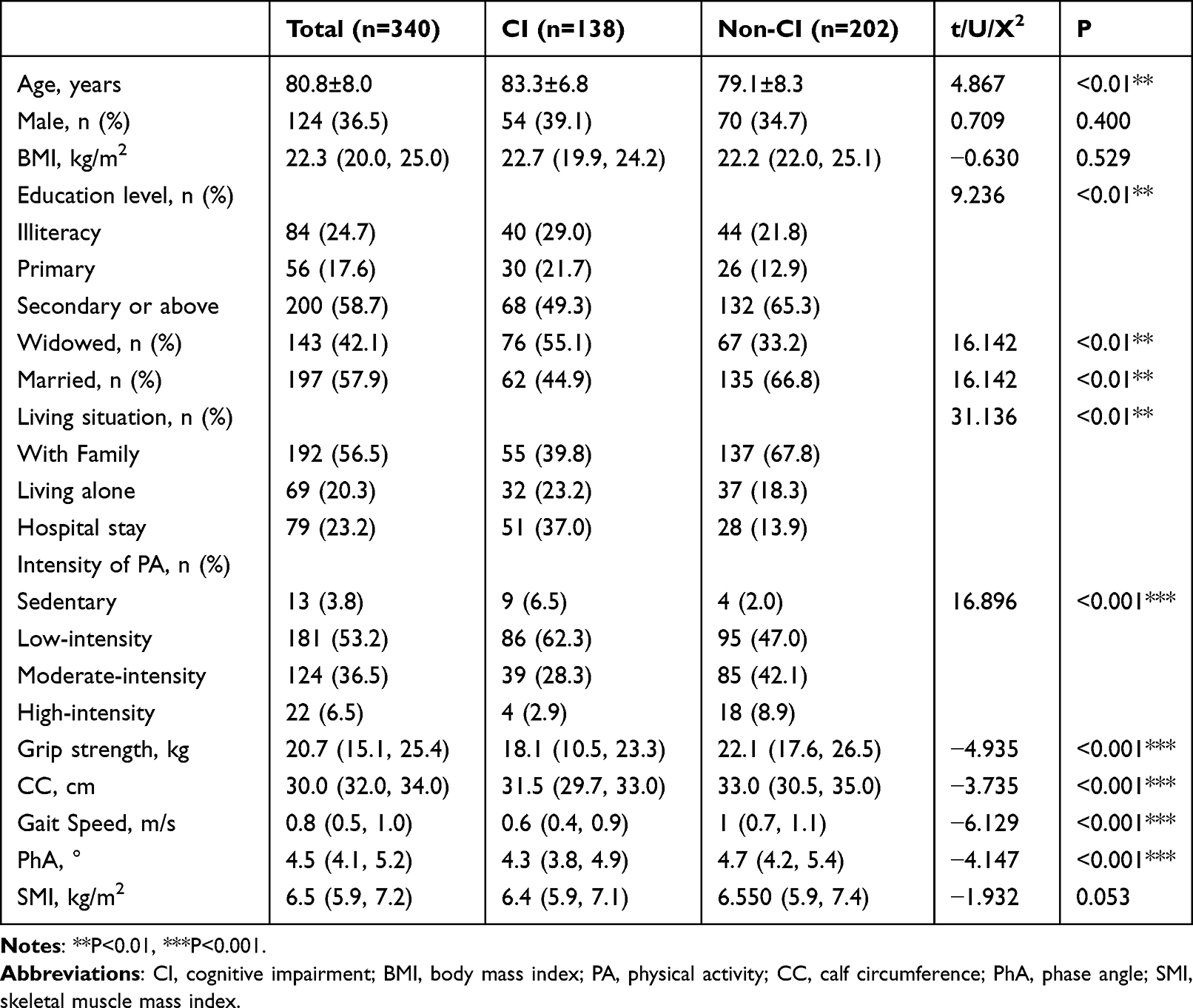 |
Table 1 Baseline Characteristics |
Cross-Sectional Analysis of Comprehensive Geriatric Assessments
Patients in the cognitive impairment group exhibited significantly worse performance in activities of daily living, swallowing function, balance ability, and nutritional status, along with more severe frailty (all P < 0.001). Detailed data are presented in Table 2.
 |
Table 2 Cross-Sectional Analysis of Comprehensive Geriatric Assessments |
Regression Analysis of Cognitive Ability Influencing Factors
In univariate regression analysis (Model1) incorporating variables with P<0.01 from correlation analyses, reduced PhA, advanced age, low education level, living alone, and impaired muscle function were significantly associated with cognitive impairment risk (all P<0.05). In the multivariate regression model (Model 2), after adjusting for confounders including age, living situation, marital status, physical activity intensity, grip strength, gait speed, and calf circumference, phase angle (OR = 0.622, 95% CI: 0.434–0.892, P=0.01) and education level above junior high school (OR = 0.241, 95% CI: 0.121–0.477, P<0.01) remained independent predictors. Notably, the association between muscle function metrics (such us, grip strength, gait speed, calf circumference) and cognitive impairment was attenuated to non-significance, suggesting their effects may be mediated through cellular energy homeostasis reflected by PhA. Detailed results are summarized in Table 3.
 |
Table 3 Regression Analysis of Factors Influencing Cognitive Ability |
ROC Curve Analysis of Phase Angle for Predicting Cognitive Impairment
As shown in Figure 1, the area under the curve (AUC) for phase angle (PhA) was 0.612, with an optimal cutoff value of 4.75°, demonstrating a sensitivity of 0.510 and specificity of 0.703. These findings suggest that PhA has moderate predictive value for cognitive impairment in older CVD patients.
 |
Figure 1 ROC curve of phase angle for predicting cognitive impairment. Abbreviation: PhA, phase angle. |
Discussion
Since the Lancet first proposed the concept of “cardiogenic dementia” in 1977, the interplay between cardiovascular disease and cognitive impairment has garnered significant attention. Current evidence suggests that CVD subtypes—including coronary heart disease, heart failure, abnormal blood pressure variability, orthostatic hypotension, and atrial fibrillation—accelerate cognitive decline,22–24 while cognitive impairment conversely worsens CVD prognosis by reducing treatment adherence and exacerbating autonomic dysfunction, forming a bidirectional vicious cycle.25 Thus, early identification of cognitive decline in CVD patients is critical for improving clinical outcomes.
This study revealed that reduced PhA is independently associated with cognitive impairment risk in older CVD patients, even after multivariate adjustment (β = −0.474, 95% CI: 0.434–0.892, P = 0.01). This finding offers a novel tool for early cognitive risk screening in this population. As a core parameter of BIA, PhA provides a noninvasive quantitative measure of cellular health by assessing cell membrane integrity, ion channel activity, and fluid distribution.9 Low PhA may indicate impaired membrane function, disrupting transmembrane nutrient transport and neuronal signaling, ultimately contributing to cognitive decline. Inflammation and oxidative stress likely underpin the association between PhA and cognitive ability. Chronic inflammation activates NADPH oxidase, driving excessive ROS production and mitochondrial dysfunction in neurons.17,26,27 Concurrently, cell membrane damage reflected by low PhA may impair the transmembrane transport capacity of antioxidants, forming a vicious cycle of oxidative stress.28,29 This bidirectional interaction is particularly pronounced in cardiometabolic diseases, suggesting that PhA-targeted interventions could concurrently improve cellular health and cognitive outcomes. Studies have shown that individuals with higher levels of oxidative stress perform worse on cognitive tests,30 so it is speculated that PhA may be associated with cognitive ability by reflecting oxidative stress levels. In addition, it has been found that PhA is inversely correlated with pro-inflammatory cytokines, such as IL-6, TNF-α, and CRP,31 which can cross the blood-brain barrier, trigger inflammation in the central nervous system, activate microglia, release neurotoxic substances, and promote Aβ deposition, while low PhA may exacerbate this process by upregulating IL-6, thereby exacerbating cognitive impairment.
Previous studies have demonstrated that sarcopenia is associated with cognitive impairment. A cross-sectional study involving 5715 older individuals found that sarcopenia correlates with more severe cognitive impairment.32 Moreover, a recent meta-analysis further confirmed significant associations between sarcopenia and mild cognitive impairment (MCI), Alzheimer’s disease (AD), as well as other forms of dementia.32 However, this study found that cognitive performance was significantly associated with muscle function metrics (eg, grip strength and gait speed), but not with muscle mass as measured by SMI. Gait speed and grip strength serve as indicators of ADL and physical activity levels. Exercise may exert a positive impact on the rate of cognitive decline in AD.33 Furthermore, physical activity can prevent cognitive decline and dementia by mitigating cardiovascular risk factors such as hypertension, diabetes mellitus, hypercholesterolemia, and obesity.34 These findings align with the results of our current study, which demonstrated significant associations between cognitive function and both ADL performance and physical activity intensity. Compared to traditional muscle metrics, PhA not only reflects impaired muscle function but also evaluates cellular health status, potentially offering greater sensitivity in detecting early biological alterations associated with cognitive decline.35 Additionally, the cognitive impairment group showed sociodemographic characteristics such as advanced age, low education level, widowhood and high proportion of residents in medical institutions, which was consistent with a recent study.36
These disparities may influence PhA and cognitive function through mediating variables such as health literacy and nutritional status, creating a cascade effect of social deprivation-biological dysregulation-cognitive decline.
These findings suggest that PhA shows a modest association with cognitive decline in older CVD patients, but its clinical utility may be limited due to low sensitivity and a small AUC value. For hospitalized patients, PhA may guide personalized nutrition and rehabilitation programs, with antioxidant (eg, vitamin E) and anti-inflammatory dietary interventions prioritized for low-PhA individuals. Integrating PhA with metrics like grip strength and gait speed could further enhance multidimensional health assessments.
Strengths and Limitations
This study is the first to validate PhA’s independent predictive value for cognitive impairment in older CVD patients, offering novel cellular-level insights into heart-brain crosstalk. While prospective studies are required to confirm its clinical utility, PhA’s potential as a multidimensional health assessment tool is evident. However, we also acknowledge some limitations. First, its cross-sectional design precludes causal inferences; longitudinal studies are needed to determine whether low PhA is a risk factor or consequence of cognitive decline. Second, unmeasured confounders—such as mood disorders and medication use may introduce bias. Mood disorders could simultaneously reduce PhA values and impair hippocampal function through HPA axis activation. Anticholinergic drugs and benzodiazepines may lower PhA by altering membrane ion channels while directly contributing to cognitive symptoms. If not adjusted for, these factors may overestimate the effect size of PhA. Third, PhA measurements may be influenced by hydration status and device precision; future studies should validate reproducibility and technical robustness.
Conclusion
This study is the first to validate the independent predictive value of PhA in older CVD patients, providing novel cellular-level evidence for the “heart-brain comorbidity” mechanism. Although the clinical utility of PhA requires further validation in prospective studies, its potential as a multidimensional health assessment tool has already emerged.
Ethics Approval and Consent to Participate
This study was approved by the Medical Ethics Committee of The Second Affiliated Hospital of Zhejiang Chinese Medical University (2022-KL-092-01) and all the participants provided written informed consent to use their data.
Acknowledgments
An unauthorized version of the Chinese MMSE was used by the study team without permission, however this has now been rectified with PAR.
The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR (www.parinc.com).
Funding
This study was financially supported by Zhejiang Province Basic Public Welfare Research Program (LGF21H250001).
Disclosure
The authors declare no competing interests in this work.
References
1. Mensah GA, Fuster V, Murray CJL, et al. Global burden of cardiovascular diseases and risks, 1990–2022. J Am Coll Cardiol. 2023;82(25):2350–2473. doi:10.1016/j.jacc.2023.11.007
2. Gorelick PB, Scuteri A, Black SE, et al. Vascular Contributions to Cognitive Impairment and Dementia. Stroke. 2011;42(9):2672–2713. doi:10.1161/STR.0b013e3182299496
3. Snyder HM, Corriveau RA, Craft S, et al. Vascular contributions to cognitive impairment and dementia including Alzheimer’s disease. Alzheimer’s Dement. 2015;11(6):710–717. doi:10.1016/j.jalz.2014.10.008
4. Nash DT, Fillit H. Cardiovascular disease risk factors and cognitive impairment. Am J Cardiol. 2006;97(8):1262–1265. doi:10.1016/j.amjcard.2005.12.031
5. Iadecola C. The Neurovascular Unit Coming of Age: a Journey through Neurovascular Coupling in Health and Disease. Neuron. 2017;96(1):17–42. doi:10.1016/j.neuron.2017.07.030
6. Swardfager W, Lanctôt K, Rothenburg L, Wong A, Cappell J, Herrmann N. A meta-analysis of cytokines in Alzheimer’s disease. Biol Psychiatry. 2010;68(10):930–941. doi:10.1016/j.biopsych.2010.06.012
7. Arnold SE, Arvanitakis Z, Macauley-Rambach SL, et al. Brain insulin resistance in type 2 diabetes and Alzheimer disease: concepts and conundrums. Nat Rev Neurol. 2018;14(3):168–181. doi:10.1038/nrneurol.2017.185
8. Cousineau JP, Dawe AM, Alpaugh M. Investigating the interplay between cardiovascular and neurodegenerative disease. Biology. 2024;13(10):764. doi:10.3390/biology13100764
9. Kyle UG, Bosaeus I, De Lorenzo AD, et al. Bioelectrical impedance analysis—part I: review of principles and methods. Clin Nutr. 2004;23(5):1226–1243. doi:10.1016/j.clnu.2004.06.004
10. da Silva BR, Orsso CE, Gonzalez MC, et al. Phase angle and cellular health: inflammation and oxidative damage. Rev Endocr Metab Disord. 2023;24(3):543–562. doi:10.1007/s11154-022-09775-0
11. Do Amaral Paes TC, De Oliveira KCC, De Carvalho Padilha P, Peres WAF. Phase angle assessment in critically ill cancer patients: relationship with the nutritional status, prognostic factors and death. J Crit Care. 2018;44:430–435. doi:10.1016/j.jcrc.2018.01.006
12. Hirose S, Nakajima T, Nozawa N, et al. Phase Angle as an Indicator of Sarcopenia, Malnutrition, and Cachexia in Inpatients with Cardiovascular Diseases. JCM. 2020;9(8):2554. doi:10.3390/jcm9082554
13. Colín-Ramírez E, Castillo-Martínez L, Orea-Tejeda A, Vázquez-Durán M, Rodríguez AE, Keirns-Davis C. Bioelectrical impedance phase angle as a prognostic marker in chronic heart failure. Nutrition. 2012;28(9):901–905. doi:10.1016/j.nut.2011.11.033
14. Ceolin J, De Borba EL, Mundstock E, De Oliveira JR, Mattiello R, Bodanese LC. Phase angle of bioimpedance as a marker of inflammation in cardiovascular diseases: a systematic review. Nutrition. 2023;112:112064. doi:10.1016/j.nut.2023.112064
15. Alves FD, Souza GC, Clausell N, Biolo A. Prognostic role of phase angle in hospitalized patients with acute decompensated heart failure. Clin Nutr. 2016;35(6):1530–1534. doi:10.1016/j.clnu.2016.04.007
16. Shaito A, Aramouni K, Assaf R, et al. Oxidative stress-induced endothelial dysfunction in cardiovascular diseases. Front Biosci. 2022;27(3):105. doi:10.31083/j.fbl2703105
17. Dash UC, Bhol NK, Swain SK, et al. Oxidative stress and inflammation in the pathogenesis of neurological disorders: mechanisms and implications. Acta Pharm Sin B. 2024;2024:S2211383524004040. doi:10.1016/j.apsb.2024.10.004
18. da Silva BR, Gonzalez MC, Cereda E, Prado CM. Exploring the potential role of phase angle as a marker of oxidative stress: a narrative review. Nutrition. 2022;93:111493. doi:10.1016/j.nut.2021.111493
19. Gilbert MAG, Fatima N, Jenkins J, et al. CryoET of β-amyloid and tau within postmortem Alzheimer’s disease brain. Nature. 2024;631(8022):913–919. doi:10.1038/s41586-024-07680-x
20. Murakami T, Kobayashi T, Ono H, et al. Phase angle as an indicator of sarcopenia and malnutrition in patients with chronic obstructive pulmonary disease. Respir Investig. 2024;62(4):651–656. doi:10.1016/j.resinv.2024.05.012
21. Robertson DA, Savva GM, Kenny RA. Frailty and cognitive impairment—a review of the evidence and causal mechanisms. Ageing Res Rev. 2013;12(4):840–851. doi:10.1016/j.arr.2013.06.004
22. Liang X, Huang Y, Han X. Associations between coronary heart disease and risk of cognitive impairment: a meta-analysis. Brain Behav. 2021;11(5):e02108. doi:10.1002/brb3.2108
23. Singh-Manoux A, Fayosse A, Sabia S, et al. Atrial fibrillation as a risk factor for cognitive decline and dementia. Eur Heart J. 2017;38(34):2612–2618. doi:10.1093/eurheartj/ehx208
24. Duan L, Xiao R, Liu S, Shi Y, Feng Y. Causality between cognitive performance and cardiovascular disease: a bidirectional Mendelian randomization study. Gene. 2024;891:147822. doi:10.1016/j.gene.2023.147822
25. Adams ML, Grandpre J, Katz DL, Shenson D. Cognitive impairment and cardiovascular disease: a comparison of risk factors, disability, quality of life, and access to health care. Public Health Rep. 2020;135(1):132–140. doi:10.1177/0033354919893030
26. Li J, Wang Y, Xiong K, Gao C. Editorial: neuroinflammation and cognitive impairment. Front Aging Neurosci. 2024;16:1453772. doi:10.3389/fnagi.2024.1453772
27. Heneka MT, Van der Flier WM, Jessen F, et al. Neuroinflammation in Alzheimer disease. Nat Rev Immunol. 2024;2024:1–32. doi:10.1038/s41577-024-01104-7
28. Itri R, Junqueira HC, Mertins O, Baptista MS. Membrane changes under oxidative stress: the impact of oxidized lipids. Biophys Rev. 2014;6(1):47–61. doi:10.1007/s12551-013-0128-9
29. Mahapatra C, Thakkar R, Kumar R. Modulatory impact of oxidative stress on action potentials in pathophysiological states: a comprehensive review. Antioxidants. 2024;13(10):1172. doi:10.3390/antiox13101172
30. Franzoni F, Scarfò G, Guidotti S, Fusi J, Asomov M, Pruneti C. Oxidative stress and cognitive decline: the neuroprotective role of natural antioxidants. Front Neurosci. 2021;15:729757. doi:10.3389/fnins.2021.729757
31. Tomeleri CM, Cavaglieri CR, de Souza MF, et al. Phase angle is related with inflammatory and oxidative stress biomarkers in older women. Exp Gerontol. 2018;102:12–18. doi:10.1016/j.exger.2017.11.019
32. Hu Y, Peng W, Ren R, Wang Y, Wang G. Sarcopenia and mild cognitive impairment among elderly adults: the first longitudinal evidence from CHARLS. J Cachexia, Sarcopenia Muscle. 2022;13(6):2944–2952. doi:10.1002/jcsm.13081
33. Farina N, Rusted J, Tabet N. The effect of exercise interventions on cognitive outcome in Alzheimer’s disease: a systematic review. Int Psychogeriatr. 2014;26(1):9–18. doi:10.1017/S1041610213001385
34. Iso-Markku P, Aaltonen S, Kujala UM, et al. Physical activity and cognitive decline among older adults: a systematic review and meta-analysis. JAMA Network Open. 2024;7(2):e2354285. doi:10.1001/jamanetworkopen.2023.54285
35. Di Vincenzo O, Marra M, Di Gregorio A, Pasanisi F, Scalfi L. Bioelectrical impedance analysis (BIA) -derived phase angle in sarcopenia: a systematic review. Clin Nutr. 2021;40(5):3052–3061. doi:10.1016/j.clnu.2020.10.048
36. Ruan X, Li H, Wang Z, et al. The influencing factors of cognitive impairment in elderly individuals in chengdu city: a cross-sectional study based on AD8. BMC Geriatr. 2025;25(1):19. doi:10.1186/s12877-024-05661-3
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Impact of Combined Cognitive and Physical Impairments on Long-Term Prognosis in Elderly Cardiovascular Disease Patients: A Prospective Cohort Study

Liu Y, Chai K, Wang T, Yang Z, Ji L, Guo D, Cui L, Luo Y, Sun N, Wang H
Clinical Interventions in Aging 2025, 20:1605-1617
Published Date: 15 September 2025