Back to Journals » Clinical Ophthalmology » Volume 15
Relationship Between Central Corneal Thickness and Ganglionic-Inner Plexiform Cell Layer and Retinal Nerve Fibre Layer Thickness in Normal Subjects
Authors Al Saad M ![]() , Shehadeh A
, Shehadeh A ![]() , Meqbil J
, Meqbil J ![]() , Elubous K
, Elubous K ![]() , Qablawi M, Abu-Yaghi NY
, Qablawi M, Abu-Yaghi NY ![]()
Received 26 February 2021
Accepted for publication 1 April 2021
Published 28 April 2021 Volume 2021:15 Pages 1809—1812
DOI https://doi.org/10.2147/OPTH.S308585
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mouna Al Saad, Amin Shehadeh, Jehad Meqbil, Khaled Elubous, Mohammed Qablawi, Nakhleh Abu-Yaghi
Department of Special Surgery/Ophthalmology Division, School of Medicine, The University of Jordan, Amman, Jordan
Correspondence: Mouna Al Saad
Department of Special Surgery/Ophthalmology Division, School of Medicine, The University of Jordan, Queen Rania Street, P.O Box 113301, Amman, 11942, Jordan
Tel +962 797793018
Email [email protected]
Purpose: To determine the relationship between central corneal thickness (CCT), ganglionic cell-inner plexiform layer thickness and macular nerve fibre layer (RNFL) thickness as measured by optical coherence tomography in a cohort of healthy subjects.
Methods: Sixty healthy eyes from 60 subjects were included in this study. All subjects had a standard slit-lamp examination and optical coherence tomography. Central corneal thickness was measured using the Optopol spectral domain optical coherence tomography (SD OCT) machine (version 7.2.0). A linear mixed effects model was used to assess the relationship between central corneal thickness (CCT) and ganglionic cell-inner plexiform layer thickness and macular retinal nerve fibre layer thickness (RNFL).
Results: Sixty healthy eyes from 60 subjects were included in this study. The average age was 41.8 years (± 20.6 years). There were 22 males (37%) and 38 females (63%). The average central corneal thickness was 525.2 ± 35.1 μm (451– 601) μm. The average macular retinal nerve fiber layer thickness was 28.9 ± 2.5 μm (23– 38μm), and the average ganglionic cell-inner plexiform layer thickness was 88.6 ± 6.3 μm (75– 110 μm). We found no statistically significant relationship between central corneal thickness and ganglionic cell-inner plexiform layer thickness (p=0.983) nor with macular RNFL (p =0.285).
Conclusion: In this cohort of healthy subjects, there was no statistically significant relationship between central corneal thickness and ganglionic cell-inner plexiform layer thickness or with macular retinal nerve fibre layer thickness.
Keywords: central corneal thickness, ganglion cell layer, inner plexiform layer, optical coherence tomography
Introduction
Central corneal thickness (CCT) detection is an important tool in the diagnosis and follow-up of glaucoma and refractive surgical interventional procedures.1 In addition, measurement of CCT serves as an indirect method to evaluate whether the corneal endothelium is healthy and is used to follow up certain ocular diseases such as corneal dystrophies.2 Moreover, it is important for correct measurement of the intraocular pressure.2,3 The retinal nerve fibre layer represents the quality of axons while the ganglionic cell-inner plexiform layer thickness represents the quantity of cell bodies and dendrites of retinal ganglionic cell. Both of which may be negatively affected by glaucoma. The optical coherence tomography (OCT) has emerged as an accurate noncontact method to measure CCT with the advantage of demonstrating the thinnest parts of the cornea.4 Data concerning the relationship between CCT and ganglionic cell-inner plexiform (GC-IPL) and macular retinal nerve fibre layer (RNFL) thickness in healthy subjects is scarce especially in the Middle Eastern population. The relationship between CCT and glaucoma was evaluated by many studies and CCT was found to be thinner in patients with glaucoma compared to controls.5 Additionally, thinner CCT has been associated with progression of glaucoma. Additionally, tonometry artefacts can result from variations in CCT.6 Many biological and genetic associations between corneal thickness and glaucoma exist along with demographic and environmental factors. The measuring instrument playing a significant role on CCT measurement and should be kept in mind when evaluating the impact of corneal thickness on patients with glaucoma. Early glaucomatous damage affects the macula and this can be demonstrated by thinning of the macular RNFL and thinning of the GC-IPL. The macular GC-IPL is of particular importance as 50% of the retinal ganglionic cells are located in the macula.3
The aim of this study is to evaluate the relationship between CCT and GC-IPL thickness and macular RNFL thickness in a cohort of normal Jordanian subjects.
Materials and Methods
Study Design
This study was approved by the Institutional Review Board at Jordan University Hospital. All participants provided written informed consent. Sixty eyes of 60 healthy subjects, who visited the ophthalmology clinic from March 2018 to March 2020, were included. Exclusion criteria were any patient who had an ocular condition that may affect CCT or GC-IPL thickness, including myopia more than 3 diopters, retinal detachment, history of vitrectomy, glaucoma, abnormal peripapillary nerve fiber layer or central laser, corneal scar, cataract, glaucoma and/or keratoconus. In addition, pseudophakic patients and any patient with evidence of endothelial dystrophy on slit-lamp bio- microscopy as well as contact lens wearers and patients suffering from ocular surface disease were also excluded.
All included subjects had a detailed ophthalmic examination including best corrected visual acuity using the Snellen chart, slit-lamp biomicroscopy as well as intraocular pressure measurement and a dilated fundus exam. Macular OCT in which the central and the para central macular area as well as the GC-IPL thickness and macular RNFL thickness measurement and the anterior segment OCT showing the central corneal thickness were performed for each patient using the Optopol SD OCT machine (version 7.2.0 Sp.z.o.o. Poland). Regarding the macular thickness, 8×8mm macular area centered on the fovea was imaged and recorded. Foveal thickness was segmented by a single retina specialist (MAS). The OCT machine differentiates and records GC-IPL thickness as well as macular RNFL thickness (diameter 3.5 mm, 768 A-scans). In addition, CCT thickness measurements (radial 4×4 mm) and a pachymetry map were obtained showing the anterior CCT. The device’s eye tracking system compensated for eye movement.
Statistical Analysis
We used SPSS version 21.0 (Chicago, USA) in our analysis. We used mean (± standard deviation) to describe continuous variables (age and sex). We used count (frequency) to describe other nominal variables (ie, gender). Pearson correlation was used to analyze if the correlation between the difference in CCT measurements and either GL-IPL or RNFL. All underlying assumptions were met, unless otherwise indicated. We adopted a p value of 0.05 as a significant threshold.
Results
A total of 60 eyes from 60 subjects were included in this study. The mean age was 41.7 (±20.6) years. They were 22 (37%) males and 38 (63%) females. The mean central corneal thickness was 525.2±35.1µm (range: 451–601µm). The mean macular retinal nerve fiber layer (RNFL) thickness was 28.9±2.5µm (range: 23–38µm) while the mean retinal ganglionic cell-inner plexiform layer (RGC-IPL) thickness was 88.6 ± 6.3 µm (75–110µm). Demographic and clinical characteristics of the studied subjects are shown in Table 1.
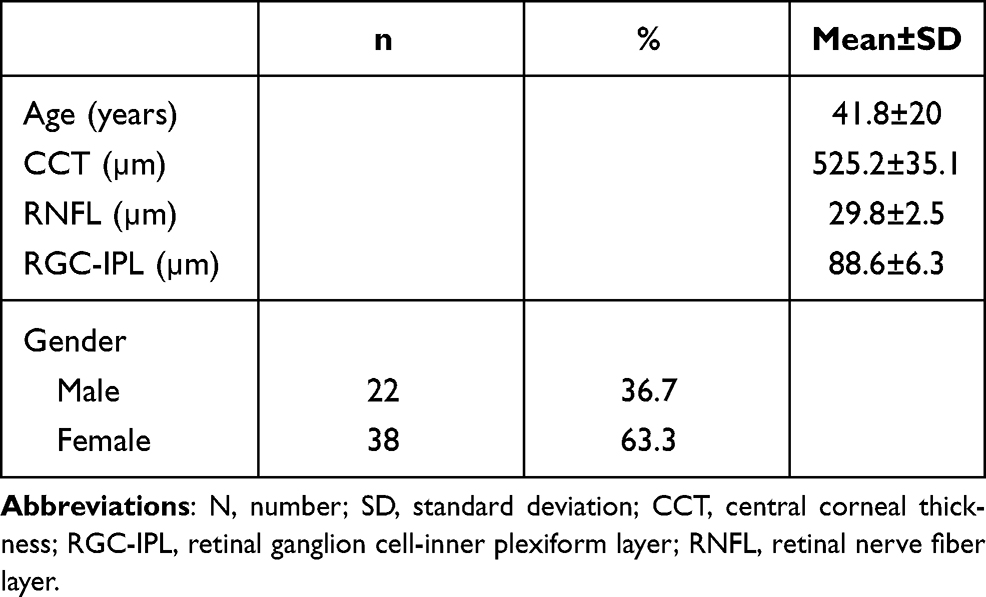 |
Table 1 Demographic and Clinical Characteristics of Participants |
The correlation between SD-OCT measurements (average RGC-IPL and RNFL) and central corneal thickness (CCT) is shown in Table 2. There was no statistically significant correlation between the average CCT and average RGC-IPL (p=0.938) as well as RNFL (p=0.285).
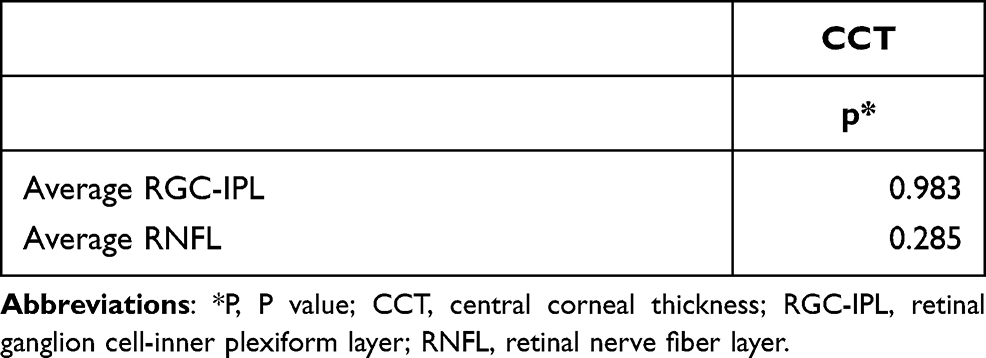 |
Table 2 Correlation Between Measured Central Corneal Thickness and Average Retinal Ganglionic Cell-Inner Plexiform Layer and Retinal Nerve Fiber Layer |
Table 3 shows the correlation between the average RGC-IPL thickness and the average RNFL thickness with age. There was a statistically significant negative relationship with age and the average RGC-IPL thickness (p=0.033). Additionally, the relationship with the average RNFL thickness was statistically significant (p=0.045) as given in Table 3.
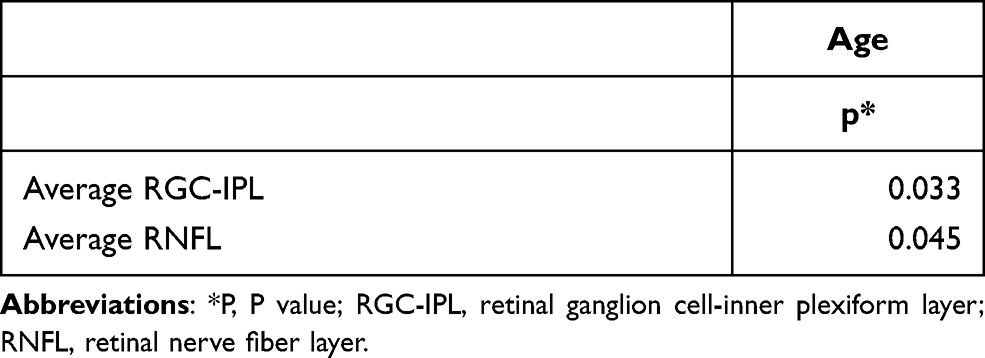 |
Table 3 Correlation Between Age and Average Retinal Ganglionic Cell-Inner Plexiform Layer and Retinal Nerve Fiber Layer |
Discussion
Up to our knowledge, this is the first study to evaluate the relationship between CCT and macular GC-IPL and RNFL thicknesses in healthy eyes. We found that ganglionic cell layer thickness and macular RNFL negatively correlate with age; however, no statistically significant relationship was detected between CCT and macular GC-IPL or RNFL thickness. Evaluating this relationship in healthy eyes will eliminate the inevitable confounder when evaluating glaucomatous eyes, due to the inherent effect of the disease on the GC-IPL and RNFL thickness.
Although CCT, GC-IPL and RNFL were important biological parameters for glaucoma, it is not surprising to find the negative result since they were independent anatomically and physiologically. However, it is well known that corneal thickness is an important indicator for the overall structure and biochemical characteristics of the eye.2 CCT is a major risk factor for the development of glaucoma.3,8,11,13 Furthermore, detection of CCT may serve as an early indicator for the development of glaucoma, especially if associated with macular ganglionic cell layer loss.1 In addition, macular ganglionic cell layer is particularly important as 50% of retinal ganglionic cells are in the macula.3 Limited studies evaluated the relationship between the macular ganglionic cell layer thickness and other ocular structures. Ou Tan et al evaluated the macular ganglionic cell loss using Fourier Domain OCT and concluded that the average measurement had significant diagnostic power in differentiating between primary glaucoma and normal subjects.3 However, Barua et al concluded that only inferior ganglionic cell thickness had diagnostic value for detecting glaucoma. In addition, a strong structure–function correlation of macular ganglion and retinal nerve fiber layer values with visual fields were found.3 On the other hand, limited studies evaluated the relationship between CCT and the RNFL layer with variable results.9,10,12,14 Most investigators found significant correlations between CCT and average RNFL in glaucomatous eyes.2 Other investigators studied the relationship between the CCT and the average RNFL in healthy subjects,10,13 Henderson et al examined the relationship between CCT and RNFL thickness and found no correlation between the CCT and the RNFL in healthy eyes which is consistent with this current work.4
Age was negatively associated with macular ganglionic cell layer thickness and CCT in our work, a finding mirrored by other reports.2,5–7,11
This study is limited by its rather small number of subjects and that the sample is hospital based. Further studies with larger sample size and from different societies are needed to confirm these findings. However, the study adds important information regarding the correlation between CCT and GC-IPL and macular RNFL in healthy subjects.
In conclusion, we did not find a significant correlation between CCT and macular GC-IPL or RNFL thickness in our cohort of normal Jordanian subjects. A significant difference was detected between age, GC-IPL thickness and macular RNFL, which may indicate that loss of the RNFL and the ganglionic cells are the result of glaucoma rather than a causative factor.
Studying the correlation in healthy eyes will eliminate an important risk factor when evaluating glaucomatous eyes, due to the effect of glaucoma on the GC-IPL and RNFL thickness and signify that glaucomatous damage may be responsible for thinning of the GC-IPL and macular RNFL in eyes with thin corneas as no correlation exists in normal subjects.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethical Approval
Institutional ethical approval was obtained from the IRB committee at Jordan University Hospital. This research complies with the tenants of the Declaration of Helsinki. All enrolled participants provided written informed consent.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors reported no conflicts of interest for this work.
References
1. Tan O, Chopra V, Lu ATH, et al. Detection of macular ganglion cell loss in glaucoma by Fourier-domain optical coherence tomography. Ophthalmology. 2009;116(12):2305–14e2. doi:10.1016/j.ophtha.2009.05.025
2. Mohamed E, Basiony A, Ibrahim A. Correlation between central corneal thickness and retinal nerve fiber layer thickness in open-angle glaucoma. Delta J Ophthalmol. 2019;20(2):55.
3. Barua N, Sitaraman C, Goel S, Chakraborti C, Mukherjee S, Parashar H. Comparison of diagnostic capability of macular ganglion cell complex and retinal nerve fiber layer among primary open angle glaucoma, ocular hypertension, and normal population using Fourier-domain optical coherence tomography and determining their functional correlation in Indian population. Indian J Ophthalmol. 2016;64(4):296–302. doi:10.4103/0301-4738.182941
4. Henderson PA, Medeiros FA, Zangwill LM, Weinreb RN. Relationship between central corneal thickness and retinal nerve fiber layer thickness in ocular hypertensive patients. Ophthalmology. 2005;112(2):251–256. doi:10.1016/j.ophtha.2004.09.016
5. Gaspar R, Pinto LA, Sousa DC. Corneal properties and glaucoma: a review of the literature and meta- analysis. Arq Bras Oftalmol. 2017;80(3):202–206. doi:10.5935/0004-2749.20170050
6. Chelvin CA, Ang M, Barton K. Central corneal thickness in glaucoma. Curr Opin Ophthalmol. 2017;28(2):120–126. doi:10.1097/ICU.0000000000000335
7. Hood DC, Raza AS, de Moraes CG, Liebmann JM, Ritch R. Glaugomatous damage of the macula. Prog Retin Eye Res. 2013;32:1–21. doi:10.1016/j.preteyeyeres.2012.08.003
8. Aditya M, Nath JK, Srikanth K, Ezhumalai G. Correlation between retinal nerve fiber layer thickness and central corneal thickness in ocular hypertension. J Ophthalmic Sci Res. 2019;57(4):285–288. doi:10.4103/tjosr.tjosr_68_18
9. Romero OJ, Zapata PA, Candelaria YP, García LI, Carcasé YA, Legró KM. Corneal biomechanical properties and glaucoma. Rev Cuba Oftalmol. 2017;30(3):1–11.
10. Mumcuoglu T, Townsend KA, Wollstein G, et al. Assessing the relationship between central corneal thickness and retinal nerve fiber layer thickness in healthy subjects. Am J Ophthalmol. 2008;146(4):561–566. doi:10.1016/j.ajo.2008.05.038
11. Jacob S, Kumar D, Agarwal AT, Agarwal AM. Application of OCT in ophthalmology in optical coherence tomography in macular diseases and glaucoma, Jaypee − Highlights Medical Publishers Inc. Curr Opin Ophthalmol. 2012;1:1–19.
12. Wangsupadilok B, Orapiriyakul L. Correlation between central corneal thickness and visual field defect, cup to disc ratio and retinal nerve fiber layer thickness in primary open-angle glaucoma patients. J Med Assoc Thai. 2014;97(7):1.
13. Thatsnarong D. Correlation between retinal nerve fiber layer thickness and central corneal thickness in healthy subjects. J Med Assoc Thai. 2015;98(7):693–697.
14. Sarfraz MH, Mehboob MA, Haq R. Correlation between central corneal thickness and visual field defects, cup to disc ratio and retinal nerve fiber layer thickness in primary open angle glaucoma patients. Pak J Med Sci. 2017;33(1):132–136. doi:10.12669/pjms.331.11623
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.