Back to Journals » Vascular Health and Risk Management » Volume 21
Relationship Between Cardio-Ankle Vascular Index (CAVI) and the Severity of Coronary Artery Lesions: A Case-Control Study
Authors Dung LV ![]() , Son PN
, Son PN ![]() , Nguyen KLT, Pho DC
, Nguyen KLT, Pho DC ![]() , Thang NM, Thang DC
, Thang NM, Thang DC ![]() , Son PT
, Son PT
Received 24 May 2025
Accepted for publication 2 August 2025
Published 11 August 2025 Volume 2025:21 Pages 607—615
DOI https://doi.org/10.2147/VHRM.S542595
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Harry Struijker-Boudier
Le Van Dung,1 Pham Nguyen Son,2 Kieu Ly Thi Nguyen,2 Dinh Cong Pho,2 Nguyen Manh Thang,1 Dao Chien Thang,1 Pham Truong Son2
1Department of Cardiology, Duc Giang General Hospital, Hanoi, Vietnam; 2Department of Cardiology, Heart Institute, 108 Military Central Hospital, Hanoi, Vietnam
Correspondence: Pham Truong Son, Department of Cardiology, Heart Institute, 108 Military Central Hospital, Hanoi, Vietnam, Email [email protected]
Introduction: The cardio-ankle vascular index (CAVI) is an important metric for evaluating arterial stiffness (AS). In this study, we used cardio-ankle vascular index (CAVI) to predict CAD severity of coronary artery lesions.
Methods: This case-control study was conducted between October 2019 and December 2022. There were 222 patients divided into two groups: those with chronic coronary artery disease (CAD group), with 160 patients and a control group (non–CAD group) with 62 patients. The CAVI measurement and severity of coronary artery lesion parameters were evaluated (severity of stenosis, number of coronary artery diseases, syntax scores, and Gensini scores).
Results: The CAVI in the CAD group (9.21 ± 0.79) was significantly higher than that in the non-CAD group (8.48 ± 0.62) (p < 0.001). CAVI, with a cut-off point ≥ 8.83, was a significant predictor of chronic CAD (OR = 9.6; 95% CI: 4.0– 18.8) with an area under the curve (AUC) of 0.796 (95% CI: 0.736– 0.856; p < 0.001). CAVI was significantly higher in severe stenosis (≥ 75%) compared to moderate stenosis (9.41 ± 0.81 vs 9.02 ± 0.75, p = 0.002). CAVI was higher in multivessel disease compared to single-vessel disease (9.43 ± 0.80 vs 8.90 ± 0.70, p < 0.001). CAVI increased with higher SYNTAX scores (mild, moderate, and severe: 9.09 ± 0.65, 9.80 ± 1.05, and 9.45 ± 0.46, respectively; p < 0.001) and Gensini scores (mild, moderate, and severe: 8.90 ± 0.65, 9.37 ± 0.95, and 9.43 ± 0.59, respectively; p < 0.001).
Conclusion: CAVI is higher in chronic CAD and can predict chronic CAD with a cut-off point of ≥ 8.83. The CAVI is higher in patients with severe stenosis, multivessel coronary artery disease, higher syntax scores, and higher Gensini scores.
Keywords: CAVI, CAD, syntax scores, gensini scores
Introduction
Atherosclerosis is the leading underlying pathology of cardiovascular disease. As reported by the World Health Organization in 2018, cardiovascular conditions accounted for 17.8 million deaths globally, representing 44% of non-communicable disease mortality and 31% of all-cause mortality.1 The incidence of atherosclerosis-related mortality has markedly declined in high-income countries owing to improvements in prevention and treatment strategies; however, it continues to increase in low- and middle-income regions.1
Assessment of atherosclerosis using non-invasive methods plays a critical role in the diagnosis, treatment, monitoring, and prediction of cardiovascular disease events. A few methods for evaluating atherosclerosis include pulse wave velocity (PWV),2,3 carotid intima-media thickness (IMT), augmentation index (AI), β-parameter,4,5 and ambulatory arterial stiffness index (AASI). However, these indices have certain limitations, such as the dependence of PWV on blood pressure at the time of measurement,6 and the β parameter, while independent of blood pressure, only provides an assessment of a localized arterial segment.7 The Cardio-Ankle Vascular Index (CAVI), which was introduced in Japan in 2004, addresses the key limitations of earlier vascular stiffness indices. According to previous studies, CAVI is an index associated with atherosclerosis from the aorta to the lower limb arteries,7 demonstrating a stronger correlation with the severity of atherosclerosis than IMT,8 PWV,9,10 and β.11
Several studies have indicated that the CAVI is significantly higher in patients with CAD than in those without CAD12,13 even in the absence of symptoms.14 Furthermore, elevated CAVI is associated with the progression of CAD severity,15,16 the degree of coronary artery stenosis,17,18 and the number of stenosed coronary arteries.13,19 CAVI is strongly correlated with coronary artery lesions12,20 and is valuable in predicting atherosclerotic CAD.13,21 Consequently, several studies have proposed CAVI as an effective tool for screening CAD, predicting the extent of coronary artery damage, and forecasting cardiovascular events (CVE) associated with CAD.12,22 It offers multiple advantages over other atherosclerosis assessment indices. 23,24
Recent studies have shown the significant association between the cardio-ankle vascular index (CAVI) and the progression of coronary artery disease (CAD) severity, highlighting its role as a predictor of cardiovascular (CV) events and coronary artery stenosis extent. Elevated CAVI values, particularly at or above 9.0, have been established as an optimal cutoff for predicting CV disease,25 with psychological stress-induced increases in CAVI further emphasizing its prognostic value.26 Beyond its predictive capacity, CAVI serves as a critical structural stiffness parameter, and its inclusion in risk assessment models has been shown to enhance predictive accuracy for CV events in patients without prior CVD history, opening new avenues for vascular function research.27
However, variability remains in determining the CAVI cut-off point and establishing the sensitivity and specificity of the method for assessing CAD. Therefore, this study aimed to determine the cutoff point and use the CAVI to predict the severity of coronary artery lesions.
Materials and Methods
This case-control study was conducted between October 2019 and December 2022. Based on coronary angiography findings, the patients were divided into two groups: patients with chronic coronary artery disease (CAD group) and control group (Non – CAD group).
The study Group (CAD group) had percutaneous coronary angiography results showing ≥50% stenosis of vessel diameter (significant stenosis). The control Group had percutaneous coronary angiography results showing <50% stenosis of the vessel diameter (no stenosis or nonsignificant stenosis). The exclusion criteria for both the CAD and non-CAD groups included acute coronary syndrome, history of revascularization or coronary artery bypass grafting, comorbidities affecting CAVI measurement (bilateral peripheral artery disease, acute venous thrombosis of the limbs, Raynaud’s syndrome, or limb amputation), and patients who did not consent to participate in the study.
Study Procedures
The study was conducted following these sequential steps:
Patient Recruitment
Patients with suspected chronic coronary artery disease (CCAD), as defined by the 2019 ESC guidelines, were screened for eligibility and subjected to the following assessments:
+ Medical History: Documentation of cardiovascular risk factors and comorbidities.
+ Clinical Examination: Comprehensive physical assessment of patients.
+ Laboratory and Diagnostic Evaluations: Analysis of blood biochemistry, complete blood count, electrocardiogram, and echocardiogram.
+ Indication for Coronary Angiography: Eligibility for percutaneous coronary angiography was determined based on predefined inclusion and exclusion criteria.
Cardio-Ankle Vascular Index (CAVI) Measurement Procedure
CAVI measurements were performed using the Vasera vs-1500N device (Fukuda-Denshi).
+ Measurement Environment: Measurements were conducted in a room shielded from electronic devices to prevent interference, with an ambient temperature maintained at 20–25°C to ensure patient comfort and muscle relaxation.
+ Patient Preparation: Patients were informed about the procedure to facilitate cooperation. They rested for ≥10 minutes in a supine position with arms and legs extended, muscles relaxed, and were instructed to remain still and silent.
+ Device Setup: Blood pressure cuffs, electrocardiogram electrodes, and a phonocardiogram microphone were attached to the patient.
+ Measurement Process: The device automatically (1) measured blood pressure in all four limbs simultaneously and (2) recorded pulse wave transit time from the aortic arch to the ankle. CAVI was calculated automatically using a pre-installed algorithm incorporating blood pressure and pulse wave transit time.
Percutaneous Coronary Angiography
Coronary angiography was performed according to standard protocols. Based on the results, patients were categorized into two groups: CAD (+) (study group) and CAD (-) (control group).
Statistical Analysis
Data were entered and managed using the Epidata software. Statistical processing and analysis were performed using SPSS version 20.0. Descriptive statistics included mean, median, and standard deviation for quantitative variables and frequency and percentage for qualitative variables. Pearson’s, Fisher’s exact, Kolmogorov–Smirnov, unpaired t-tests, and Mann–Whitney U-test were used, as appropriate. Receiver operating characteristic (ROC) curves were used to determine the area under the curve. Statistical significance was set at P < 0.05.
Ethics
This study was approved by the Ethics Committee of 108 Military Central Hospital (No.232/QĐ-VNC dated on 17th May, 2017) and adhered to the principles of the Helsinki Declaration. Written informed consent was obtained from all the patients.
Results
The results in Table 1 showed that there was no significant difference in the number of females and males and the mean age between the patients and controls. Hypertension was the most prevalent risk factor, whereas smoking had the lowest, with no significant differences between the two groups.
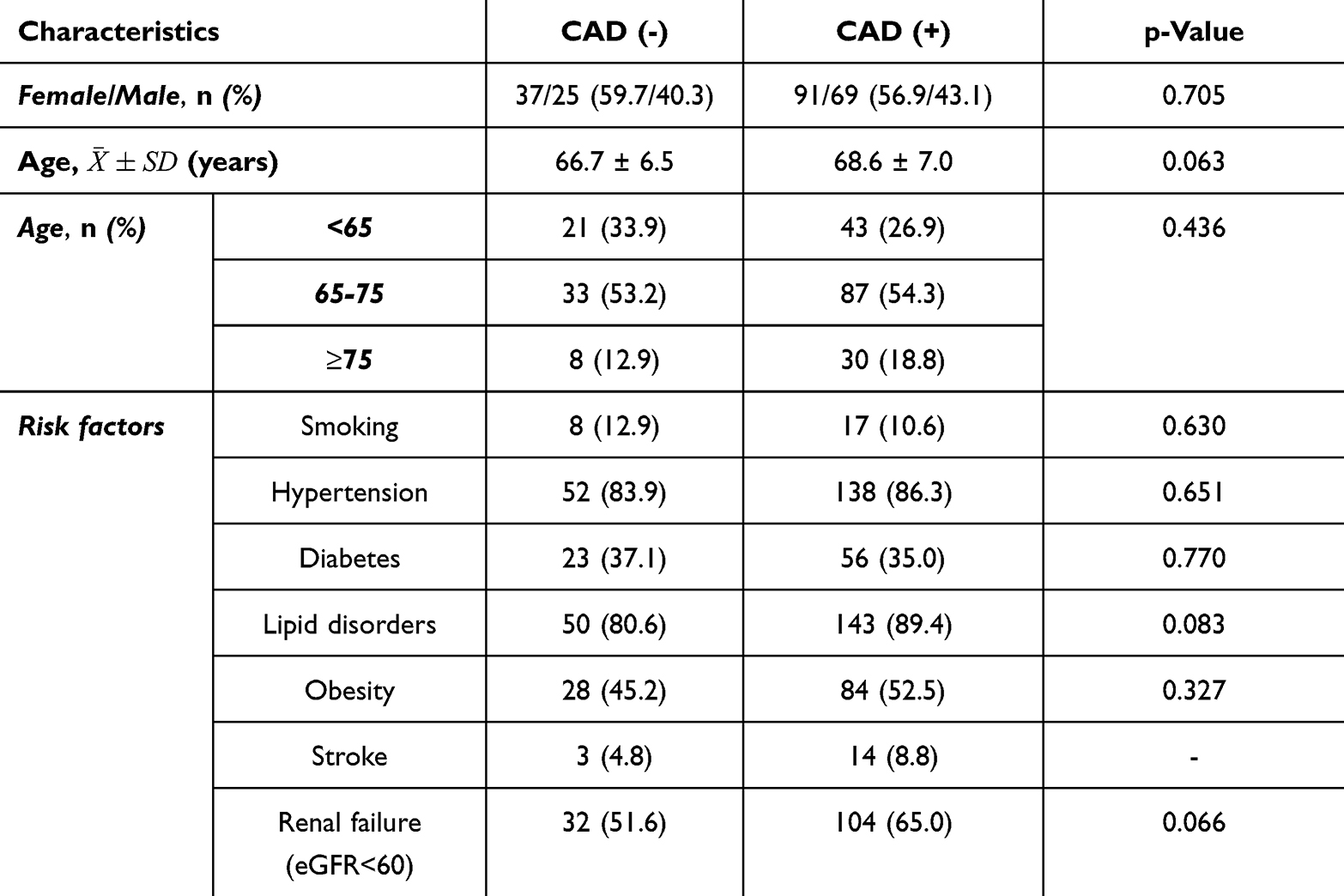 |
Table 1 Patients Characteristics |
Table 2 showed the cardio-ankle vascular index measurement. The mean CAVI in the CAD (+) group was 9.20 ± 0.80, which was significantly higher than that in the CAD (-) group (8.44 ± 0.0.63, p < 0.001). The maximum CAVI in the CAD (+) group was 9.30 ± 0.81, which was significantly higher than that in the CAD (-) group (8.54 ± 0.62, p < 0.001).
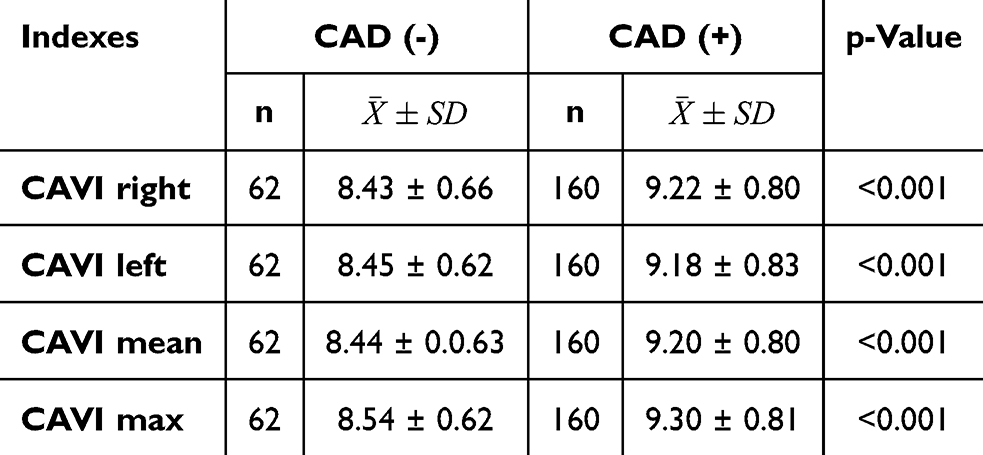 |
Table 2 Cardio-Ankle Vascular Index Measurement |
Table 3 and Figure 1 show the CAVI as a Predictor of CCAD Risk. The area under the curve (AUC) for the mean CAVI was 0.796 (95% CI: 0.736–0.856, p < 0.001), and the maximum CAVI was 0.798 (95% CI: 0.738–0.857, p < 0.001). The cutoff point for predicting CCAD risk was ≥8.83 for mean CAVI, with an odds ratio (OR) of 9.6 (95% CI: 4.0–18.8), and ≥8.95 for maximum CAVI, with an OR of 9.9 (95% CI: 5.0–19.5).
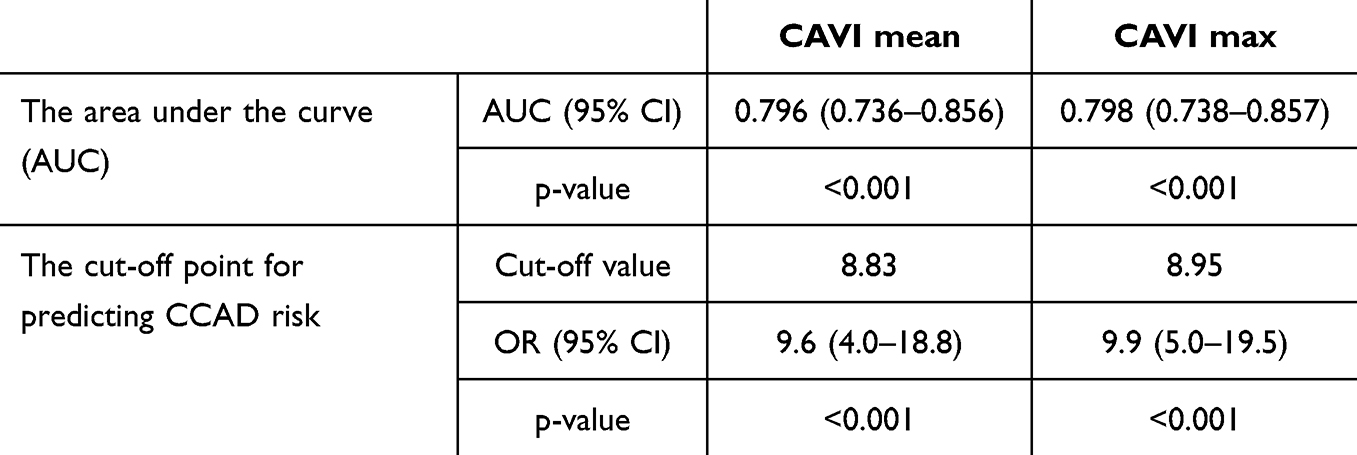 |
Table 3 CAVI as a Predictor of CCAD Risk |
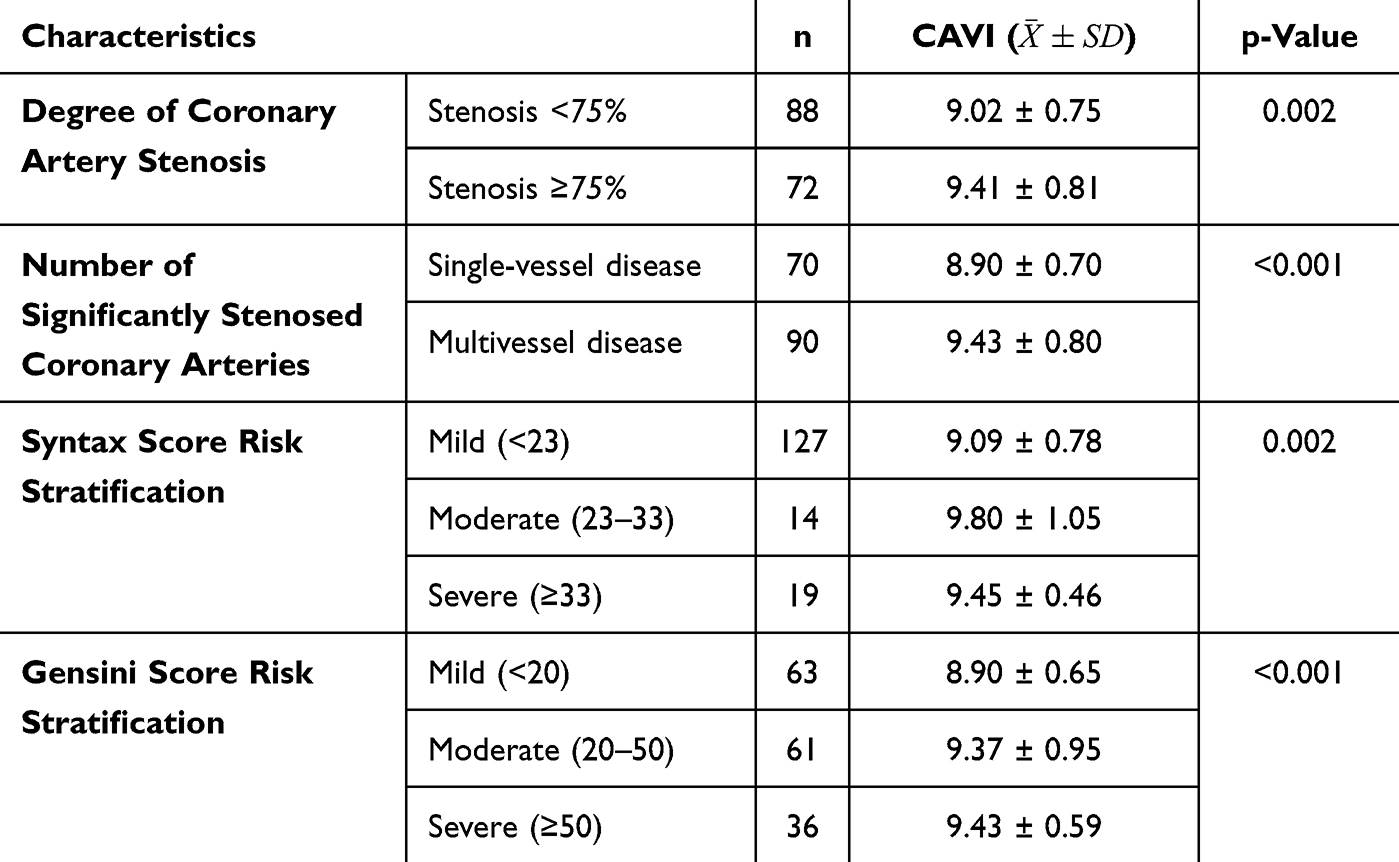 |
Table 4 The Relationship Between Cardio-Ankle Vascular Index (CAVI) and the Severity of Coronary Artery Lesions |
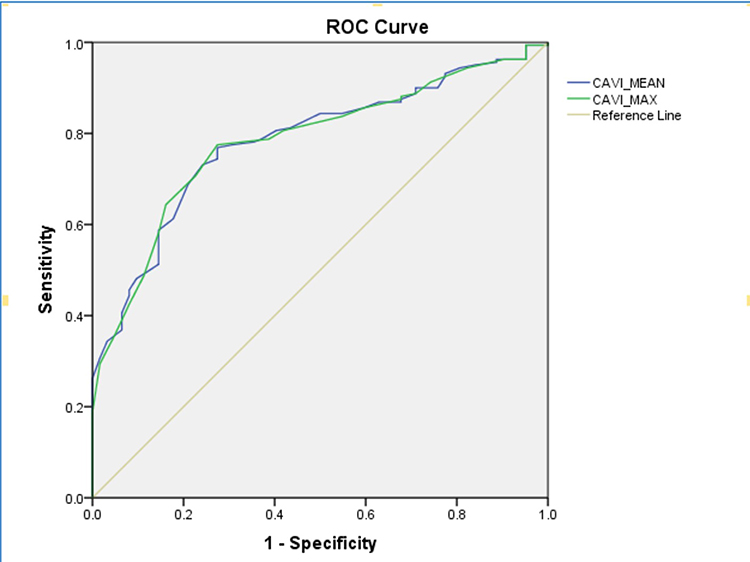 |
Figure 1 ROC for CAVI as a Predictor of CCAD Risk. |
Table 4 and Table 5 showed cardio-ankle vascular index (CAVI) to predict the severity of coronary artery lesions. CAVI was significantly higher in severe stenosis (≥75%) compared to moderate stenosis (9.41 ± 0.81 vs 9.02 ± 0.75, p = 0.002). CAVI was higher in multivessel disease compared to single-vessel disease (9.43 ± 0.80 vs 8.90 ± 0.70, p < 0.001). CAVI increased with higher SYNTAX scores (mild, moderate, and severe: 9.09 ± 0.65, 9.80 ± 1.05, and 9.45 ± 0.46, respectively; p < 0.001) and Gensini scores (mild, moderate, and severe: 8.90 ± 0.65, 9.37 ± 0.95, and 9.43 ± 0.59, respectively; p < 0.001).
 |
Table 5 Correlation Between CAVI and Coronary Artery Lesions |
CAVI showed a weak but statistically significant positive correlation with the degree of coronary artery stenosis (r = 0.250, p = 0.001), syntax score (r = 0.275, p < 0.001), and Gensini score (r = 0.187, p = 0.018).
Discussion
Non-invasive assessments of the extent and progression of coronary artery atherosclerosis play a crucial role in screening, monitoring disease progression, guiding treatment, and preventing cardiovascular events in chronic coronary artery disease (CCAD). This study was designed to evaluate the characteristics of CAVI in patients with CCAD and its relationship with coronary artery lesions and cardiovascular events.
Our study results revealed that the mean CAVI in the CAD (+) group was 9.20 ± 0.80, which was significantly higher than that in the CAD (-) group (8.48 ± 0.63, p < 0.01). These findings are consistent with the analyses of case-control studies conducted by both international and domestic researchers in similar populations. Specifically, Miyoshi et al reported that the CAVI in the group with significant coronary artery stenosis (≥50% vessel diameter reduction on percutaneous coronary angiography) was higher than that in the group with non-significant stenosis (<50%) (9.1 ± 1.3 vs 8.7 ± 1.2; p = 0.02). A similar study by Izuhara et al also reported results that were consistent with the aforementioned findings. In their study, CAVI in the group with significant coronary artery stenosis was 8.7 ± 1.8, which was higher than that in the group without significant stenosis (8.3 ± 1.7, p = 0.027).8
Numerous studies have investigated the relationship between the CAVI and coronary artery disease (CAD). Patients with stable angina pectoris exhibited significantly higher CAVI values compared to the control group (9.71 ± 1.42 vs 9.10 ± 1.41; p = 0.0178). 16 In patients with acute myocardial infarction (AMI) undergoing emergency coronary artery reperfusion, Sairaku et al observed that CAVI was significantly higher than that in patients with stable angina pectoris undergoing elective coronary revascularization (9.3 ± 1.3 vs 10.0 ± 1.7; p = 0.0012). This difference persisted even after adjusting for clinical variables that differed between the two groups. Additionally, CAVI significantly decreased six months post-intervention (10.9 ± 1.6 vs 10.0 ± 1.5; p = 0.019). 15
Our study results demonstrated that CAVI varied across different syntax score risk levels and exhibited a weak but statistically significant positive correlation with the syntax score (r = 0.275, p < 0.001). In a study of 121 non-type 2 diabetes patients with suspected coronary artery disease (CAD) undergoing percutaneous coronary angiography, Gokdeniz et al found that CAVI was positively correlated with the SYNTAX score (r = 0.537, p < 0.001) and was an independent predictor of intermediate to high SYNTAX scores. With a cutoff value of 8.6, the CAVI had an AUC of 0.877 (95% CI: 0.805–0.929), with a sensitivity of 68.9% and specificity of 93.5%.28 Korkmaz et al, in a study of 172 patients with acute CAD, reported that CAVI was independently correlated with SYNTAX score (95% CI: 15–29, p = 0.021). The Syntax scores for normal, borderline, and abnormal CAVI levels were 4.0 ± 3.7, 11.1 ± 7.2, and 14.1 ± 9.1, respectively (p = 0.009).29 CAVI varied across different risk levels according to the Gensini score and showed a weak but statistically significant positive correlation with the Gensini score (r = 0.187, p = 0.018). Miyoshi et al reported that CAVI was positively correlated with the coronary artery stenosis index (modified Gensini score) in patients with acute coronary syndrome undergoing percutaneous coronary angiography (r = 0.32, p < 0.01).12 In a study of 548 subjects undergoing coronary angiography with optical coherence tomography to assess atherosclerotic plaque morphology, Sakaguchi et al found that CAVI correlated with the logarithm of the Gensini score and was higher in the group with coronary artery stenosis (p < 0.001). However, no correlation was observed between the CAVI and plaque morphology on optical coherence tomography. 30
The area under the curve (AUC) for the mean CAVI was 0.796 (95% CI: 0.736–0.856, p < 0.001), and the maximum CAVI was 0.798 (95% CI: 0.738–0.857, p < 0.001). In a study by Nakamura et al, the AUC was 0.775, with a cutoff point of 8.81, yielding a sensitivity of 83.9% and specificity of 70%.13
CAVI have consistently identified by numerous studies as an independent predictor of coronary artery disease (CAD). Analyses by Izuhara et al 8 and Miyoshi et al12 in patients with confirmed CAD using percutaneous coronary angiography demonstrated that CAVI was independently correlated with CAD. Additionally, a study by Park et al in asymptomatic CAD patients diagnosed using multidetector computed tomography showed that a CAVI ≥ 8.0 independently correlated with the degree of coronary artery stenosis, even after adjusting for age, sex, and cardiovascular risk factors such as hypertension, type 2 diabetes, and dyslipidemia (OR = 3.143, 95% CI: 1.004–9.842; p = 0.049).14 Based on research findings, the cutoff value for CAVI in detecting the presence of coronary artery disease (CAD) varies between 7.8 and 9.0 across different studies. Some studies have reported that a CAVI ≥ 8.0 correlates with coronary artery stenosis of ≥50%, 14,31 while a CAVI range of 8.91–9.0 correlates with stenosis of ≥75%.8,13
Our study on CAVI in coronary artery disease (CAD) among Vietnamese patients yielded results consistent with those of studies conducted in Japan and other countries worldwide, confirming that CAVI is associated with the severity of coronary artery lesions and has predictive value for CAD.25–27 Furthermore, the value of CAVI lies in its noninvasive nature, simple measurement process, and minimal technical requirements while providing relatively stable results, making it widely applicable.
A limitation of this study was the exclusion of patients with a low ABI (<0.9), severe left ventricular dysfunction, and valvular heart disease, which restricts the generalizability of the findings. Nevertheless, the CAVI remains a valuable and effective tool for CAD screening, particularly in high-risk populations.
Conclusion
The CAVI is higher in chronic CAD and can predict chronic CAD with a cutoff point of ≥8.83. The CAVI is higher in patients with severe stenosis, multivessel coronary artery disease, higher syntax scores, and higher Gensini scores.
Data Sharing Statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Institutional Review Board of 108 Military Central Hospital (No.232/QĐ-VNC dated 17th May, 2017). This study adhered to the principles of the Declaration of Helsinki for Biomedical Research.
Consent for Publication
All the authors have read and agreed to the published version of the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas, took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Collaborators GBDCoD. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392(10159):1736–1788. doi:10.1016/S0140-6736(18)32203-7
2. Mattace-Raso FU, van der Cammen TJ, Hofman A, et al. Arterial stiffness and risk of coronary heart disease and stroke: the Rotterdam study. Circulation. 2006;113(5):657–663. doi:10.1161/CIRCULATIONAHA.105.555235
3. Roland A. Pulse Wave Velocity: Principles and Measurements. Arterial Stiffness and Pulse Wave Velocity–Clinical Applications. Paris: Elsevier SAS; 1999:25–53.
4. Hayashi K, Handa H, Nagasawa S, Okumura A, Moritake K. Stiffness and elastic behavior of human intracranial and extracranial arteries. J Biomech. 1980;13(2):175–184. doi:10.1016/0021-9290(80)90191-8
5. Kawasaki T, Sasayama S, Yagi S-I, Asakawa T, Hirai T. Non-invasive assessment of the age related changes in stiffness of major branches of the human arteries. Cardiovascul Res. 1987;21(9):678–687. doi:10.1093/cvr/21.9.678
6. Nye E. The effect of blood pressure alteration on the pulse wave velocity. British Heart J. 1964;26(2):261. doi:10.1136/hrt.26.2.261
7. Shirai K, Utino J, Otsuka K, Takata M. A novel blood pressure-independent arterial wall stiffness parameter; cardio-ankle vascular index (CAVI). J Atheroscler Thromb. 2006;13(2):101–107. doi:10.5551/jat.13.101
8. Izuhara M, Shioji K, Kadota S, et al. Relationship of cardio-ankle vascular index (CAVI) to carotid and coronary arteriosclerosis. Circ J. 2008;72(11):1762–1767. doi:10.1253/circj.CJ-08-0152
9. Horinaka S, Yabe A, Yagi H, et al. Comparison of atherosclerotic indicators between cardio ankle vascular index and brachial ankle pulse wave velocity. Angiology. 2009;60(4):468–476. doi:10.1177/0003319708325443
10. Yambe T, Yoshizawa M, Saijo Y, et al. Brachio-ankle pulse wave velocity and cardio-ankle vascular index (CAVI). Biomed Pharmacother. 2004;58(1):S95–8. doi:10.1016/S0753-3322(04)80015-5
11. Nakamura T, Nakahara Y, Matsumuro A, Hata H. Assessment of carotid arterial distensibility using beta stiffness index in the diagnosis of arteriosclerosis. Nihon Rinsho Japan J Clin Med. 2004;62(3):272–282.
12. Miyoshi T, Doi M, Hirohata S, et al. Cardio-ankle vascular index is independently associated with the severity of coronary atherosclerosis and left ventricular function in patients with ischemic heart disease. J Atheroscler Thromb. 2010;17(3):249–258. doi:10.5551/jat.1636
13. Nakamura K, Tomaru T, Yamamura S, Miyashita Y, Shirai K, Noike H. Cardio-ankle vascular index is a candidate predictor of coronary atherosclerosis. Circ J. 2008;72(4):598–604. doi:10.1253/circj.72.598
14. Park HE, Choi SY, Kim MK, Oh BH. Cardio-ankle vascular index reflects coronary atherosclerosis in patients with abnormal glucose metabolism: assessment with 256 slice multi-detector computed tomography. J Cardiol. 2012;60(5):372–376. doi:10.1016/j.jjcc.2012.07.005
15. Sairaku A, Eno S, Hondo T, et al. Head-to-head comparison of the cardio-ankle vascular index between patients with acute coronary syndrome and stable angina pectoris. Hypertens Res. 2010;33(11):1162–1166. doi:10.1038/hr.2010.141
16. Takaki A, Ogawa H, Wakeyama T, et al. Cardio-ankle vascular index is superior to brachial-ankle pulse wave velocity as an index of arterial stiffness. Hypertens Res. 2008;31(7):1347–1355. doi:10.1291/hypres.31.1347
17. Choi SY. Clinical application of the cardio-ankle vascular index in asymptomatic healthy Koreans. Pulse. 2017;4(Suppl 1):17–20. doi:10.1159/000448462
18. Takata M, Shimakura A. Cardio-ankle vascular index (CAVI) and cardiovascular disease. Rinsho Byori. 2013;61(10):924–933.
19. Zhang W, Wei WL, Wang XB, et al. Evaluation of diagnosis and prediction of degree of coronary stenosis by CAVI. Zhonghua Yi Xue Za Zhi. 2009;89(32):2280–2282.
20. Horinaka S, Yabe A, Yagi H, et al. Cardio-ankle vascular index could reflect plaque burden in the coronary artery. Angiology. 2011;62(5):401–408. doi:10.1177/0003319710395561
21. Kadota K, Takamura N, Aoyagi K, et al. Availability of cardio-ankle vascular index (CAVI) as a screening tool for atherosclerosis. Circ J. 2008;72(2):304–308. doi:10.1253/circj.72.304
22. Sritara P. Cardio-ankle velocity index(CAVI) contributes to coronary artery disease risk prediction. J Atheroscler Thromb. 2014;21 Suppl 1:S18–9. doi:10.5551/jat.21_Sup.1-S18
23. Gohbara M, Iwahashi N, Sano Y, et al. Clinical impact of the cardio-ankle vascular index for predicting cardiovascular events after acute coronary syndrome. Circ J. 2016;80(6):1420–1426. doi:10.1253/circj.CJ-15-1257
24. Kirigaya J, Iwahashi N, Tahakashi H, et al. Impact of cardio-ankle vascular index on long-term outcome in patients with acute coronary syndrome. J Atheroscler Thromb. 2020;27(7):657–668. doi:10.5551/jat.51409
25. Nagayama D, Shirai K, Saiki A. Significance of CAVI as a functional stiffness parameter: beyond the prognostic value for cardiovascular events. Am College Cardiol Foundation Washington DC. 2024;101018.
26. Nagayama D. Psychological stress-induced increase in the cardio-ankle vascular index (CAVI) may be a predictor of cardiovascular events. Hypertens Res. 2022;45(10):1672–1674. doi:10.1038/s41440-022-00996-z
27. Miyoshi T, Shirai K, Horinaka S, et al. Cavi is a significant indicator in primary prevention of cardiovascular disease. J Hypertension. 2025;43(Suppl 1):e260. doi:10.1097/01.hjh.0001117916.07839.0f
28. Gokdeniz T, Turan T, Aykan AC, et al. Relation of epicardial fat thickness and cardio-ankle vascular index to complexity of coronary artery disease in nondiabetic patients. Cardiology. 2013;124(1):41–48. doi:10.1159/000345298
29. Korkmaz L, Adar A, Korkmaz AA, et al. Atherosclerosis burden and coronary artery lesion complexity in acute coronary syndrome patients. Cardiol J. 2012;19(3):295–300. doi:10.5603/CJ.2012.0052
30. Sakaguchi M, Hasegawa T, Ehara S, et al. Cardio-ankle vascular index associated with coronary plaque burden not plaque morphology. Osaka City Med J. 2016;62(2):47–57.
31. Yingchoncharoen T, Limpijankit T, Jongjirasiri S, Laothamatas J, Yamwong S, Sritara P. Arterial stiffness contributes to coronary artery disease risk prediction beyond the traditional risk score (RAMA-EGAT score). Heart Asia. 2012;4(1):77–82. doi:10.1136/heartasia-2011-010079
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.