Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Rehabilitation Combined with Coagulation Tests for the Prevention of DVT in Patients After Hypertensive Intracerebral Hemorrhage Surgery
Received 9 September 2025
Accepted for publication 29 November 2025
Published 19 December 2025 Volume 2025:21 Pages 1761—1771
DOI https://doi.org/10.2147/TCRM.S566486
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sandeep Ajoy Saha
Lingwen Kong,1 Shan Yao2
1Neurosurgical Intensive Care Unit, The Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China; 2Department of Rehabilitation, Xuzhou Central Hospital, Southeast University, Xuzhou, Jiangsu, People’s Republic of China
Correspondence: Shan Yao, Department of Rehabilitation, Xuzhou Central Hospital, Southeast University, Room 603, Unit 4, Building 4, Qingnian Community, Yunlong District, Xuzhou, Jiangsu, 221000, People’s Republic of China, Tel +86-15862186026, Email [email protected]
Objective: To evaluate the efficacy of ultra-early rehabilitation combined with coagulation monitoring in preventing deep vein thrombosis (DVT) in patients following surgical intervention for hypertensive intracerebral hemorrhage (HICH).
Methods: A retrospective cohort study was conducted involving 126 HICH patients treated at the Neurosurgery ICU of The Affiliated Hospital of Xuzhou Medical University and the Rehabilitation Department of Xuzhou Central Hospital between January 2023 and December 2024. Participants were stratified into an experimental group (ultra-early rehabilitation with daily coagulation testing, n=63) and a control group (conventional care, n=63) based on the management protocol they received during their hospitalization. Hemodynamic parameters, muscle strength, and coagulation markers were assessed at baseline (T0: pre-intervention), T1 (postoperative day 1), T7 (postoperative day 7), and T14 (postoperative day 14).
Results: Baseline characteristics demonstrated comparability between groups (P> 0.05). The experimental group exhibited superior muscle strength recovery in both upper and lower extremities, with statistically significant differences emerging at T14 (P< 0.05). Coagulation parameters including fibrinogen (FIB), fibrinogen degradation products (FDP), D-dimer, thrombin-antithrombin III complex (TAT), plasmin-antiplasmin complex (PIC), and thrombomodulin (TM) demonstrated progressive decline in the experimental cohort. At T7, FIB, FDP, and D-dimer levels were significantly lower in the experimental group compared to controls (P< 0.05), with more pronounced reductions observed at T14. TAT, PIC, and TM similarly demonstrated substantial decreases at T14 (P< 0.01). DVT incidence was significantly reduced in the experimental group (12.70% vs 31.75%, P< 0.05).
Conclusion: Ultra-early rehabilitation guided by systematic coagulation monitoring appears to be associated with favorable modulation of hemostatic markers (FIB, FDP, D-dimer, TAT, PIC, TM) and enhanced muscle strength recovery following HICH surgery. This integrated approach may effectively reduce postoperative DVT incidence, offering a promising strategy for thromboprophylaxis management.
Keywords: early ambulation, blood coagulation tests, hypertension, cerebral hemorrhage, postoperative complications, venous thrombosis
Introduction
Hypertension refers to a condition where the pressure exerted by blood on the vessel walls remains consistently higher than normal (systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg). Hypertensive intracerebral hemorrhage (HICH) represents one of the most devastating complications of hypertension, characterized by sudden onset, rapid progression, and severe neurological deficits.1 The disease predominantly affects individuals aged 50 to 70 years, with approximately 10–20% of all strokes attributed to spontaneous intracerebral hemorrhage in China.2,3 Despite advances in minimally invasive surgical techniques, postoperative mortality remains high, and survivors frequently experience substantial functional impairments that significantly impact long-term quality of life.4,5
Patients undergoing HICH surgery face elevated risks of postoperative complications, particularly deep vein thrombosis (DVT).6 The reported incidence of DVT following neurosurgical procedures ranges from 4% to 10%, with substantially higher rates observed in patients with intracerebral hemorrhage.7 Surgical trauma, prolonged bed rest, and restricted limb mobility contribute to venous stasis, creating conditions favorable for thrombosis formation.7 Because venous systems possess extensive collateral circulation, early thrombus formation may not immediately impede venous return. Clinical symptoms, such as lower limb swelling, only appear when thrombi extend sufficiently to obstruct both proximal and distal collateral pathways. DVT can extend proximally to the inferior vena cava and may block the renal vein, leading to renal failure and posing life-threatening.8,9 Therefore, preventing DVT in patients after HICH surgery represents a pressing clinical priority.
Early mobilization has emerged as a potential strategy to reduce DVT risk through enhanced venous return and reduced blood stasis.10 Recent evidence from surgical populations demonstrates that early mobilization within the initial 24 hours postoperatively significantly reduces DVT incidence compared to prolonged bed rest.11 However, in HICH patients, initiating early rehabilitation poses unique challenges due to concerns about provoking hemorrhagic complications. Coagulation function after HICH surgery demonstrates substantial individual variability, with some patients exhibiting prolonged activated partial thromboplastin time (APTT) associated with increased rebleeding risk, while others rapidly develop hypercoagulable states predisposing to thrombosis.12 Traditional DVT prophylaxis strategies rely on fixed protocols without real-time adjustment for individual coagulation status, potentially exposing patients to either bleeding or thrombotic complications. Despite recognition of both early mobilization benefits and the importance of coagulation monitoring, few studies have evaluated whether integrating these approaches can safely reduce DVT while maintaining hemorrhagic safety in HICH patients. The optimal timing for initiating rehabilitation, appropriate coagulation parameters to guide mobilization, and the effectiveness of such a combined strategy remain unclear.
This study aimed to evaluate whether ultra-early rehabilitation guided by daily coagulation monitoring can effectively reduce DVT incidence compared to conventional care in patients following HICH surgery, while maintaining acceptable hemorrhagic safety.
Materials and Methods
Study Design
This was a retrospective cohort study conducted at Neurosurgery ICU of The Affiliated Hospital of Xuzhou Medical University and Rehabilitation Department of Southeast University Affiliated Xuzhou Central Hospital (Xuzhou Central Hospital) from January 2023 to December 2024. The study protocol was reviewed and approved by the Ethics Committee of Xuzhou Medical Center (Ethics Approval No.: XZXY-LK-20230626-091) and conducted in accordance with the Declaration of Helsinki. Due to the retrospective nature of this study, the requirement for informed consent was waived by the ethics committee. Patient data were anonymized prior to analysis to protect confidentiality. As a retrospective study, formal sample size calculation was not performed. All patients meeting the eligibility criteria during the study period were included to maximize statistical power and generalizability of findings.
Patient Selection
A total of 126 patients diagnosed with HICH identified and allocated to either the experimental group (ultra-early rehabilitation combined with coagulation testing, n=63) or the control group (conventional care, n=63) based on the treatment protocol implemented during their hospitalization period.
Inclusion Criteria: (1) Age 18–75 years; (2) Neuroimaging confirming the diagnosis of HICH; (3) undergone surgical treatment for HICH; (4) Normal preoperative and postoperative coagulation function test results, including D-Dimer, FIB, and FDP; (5) Patients were in stable without active bleeding or hemorrhage expansion on CT within 24 hours; (6) Glasgow Coma Scale (GCS) score ≥8 after surgery; (7) Hemodynamically stable (systolic blood pressure 100–180 mmHg without escalating vasopressor support).
Exclusion Criteria: (1) Serious problems with their heart, lungs, liver, kidneys, or other vital parts that would preclude safe rehabilitation; (2) History of thrombosis or venous clotting disorders prior to the study; (3) Were taking therapeutic anticoagulation within 7 days before surgery; (4) Had contraindications to rehabilitation; (5) Incomplete medical records.
Management Methods
Patients were categorized into two groups based on the management protocol they received during their hospitalization: the ultra-early rehabilitation combined with coagulation testing group (experimental group, n=63) and the conventional care group (control group, n=63). Clinical data and outcomes were collected from medical records for 14 days post-surgery, with observations recorded at four time points: T0 (before intervention), T1 (1 day after intervention), T7 (7 days after intervention), and T14 (14 days after intervention).
Control Group
The control group received standard postoperative care. Patients underwent bed rest for 7–10 days post-surgery with gradual mobilization initiated only after day 10 if neurologically stable Passive range-of-motion exercises were performed by nurses twice daily (15 min per session), including gentle limb movements without active patient participation, starting from postoperative day 3. The mobilization schedule progressed as follows: sitting at bedside on day 10–11, standing with assistance on day 12–13, and walking with assistance from day 14 onwards. Standard DVT prophylaxis measures included: (1) pneumatic compression devices applied to both lower limbs continuously (removed only during physical examination or transfers); (2) graduated compression stockings (18–20 mmHg); and (3) adequate hydration to prevent blood viscosity increase. Anticoagulant therapy consisted of subcutaneous injection of LMWH at a dose of 20–40 U/kg once daily, initiated 1 to 4 days postoperatively after confirming stable hemostasis.13 Additional standard postoperative care included vital signs monitoring, pain management, nutritional support, and prevention of other postoperative complications according to institutional protocols.
Experimental Group
Patients in the experimental group received ultra-early rehabilitation training initiated within 24 h post-surgery, guided by daily coagulation monitoring. Anticoagulant therapy was administered using the same LMWH protocol as the control group. Coagulation parameters were measured daily from postoperative day 1 to day 14. According to the protocol, rehabilitation proceeded if INR ≤1.5, PT ≤15 s, and no signs of rebleeding were present on neurological examination. Rehabilitation was temporarily held if INR >1.8, new neurological deterioration occurred, or hemorrhage expansion was detected, and resumed when parameters stabilized. Rehabilitation training consisted of passive joint exercises performed by professional therapists twice daily (30 min per session), including upper limb movements from shoulder to fingers and lower limb exercises (hip rotation, flexion, ankle movements), with each movement repeated 100 times (3 s per repetition). Shoulder movements were restricted to 50% of normal range to prevent excessive strain. Progressive mobilization followed this schedule based on coagulation safety: (1) day 1–2: passive exercises in bed; (2) day 3–4: active-assisted exercises; (3) day 5–7: sitting with support; (4) day 8–10: standing and weight-bearing; and (5) day 11–14: walking with assistance.
Observational Indicators
After patient selection, the following data were collected from medical records: demographics, medical history including comorbidities, hemorrhage characteristics, vital signs, and laboratory parameters.
Primary Outcome
DVT incidence at 14 days post-surgery. DVT diagnosis was confirmed by bilateral lower limb compression Doppler ultrasound examination performed at postoperative day 7 and day 14. Ultrasound reports were reviewed to extract the following DVT-related data: presence or absence of thrombus, thrombus characteristics (diameter >7 mm vs ≤7 mm, proximal vs distal location, single vs multiple thrombi).
Secondary Outcomes
- Muscle Strength: Muscle strength assessments were retrospectively obtained from physical therapy and nursing records at T0, T1, T7, and T14. Muscle strength was assessed using the modified Ashworth Scale Muscle strength grades: −1, reduced strength (sEMG amplitude <2 μV); 0, no increase in muscle tone; 1, slight increase in muscle tone with minimal resistance; 1+, slight increase with catch followed by minimal resistance; 2, marked increase in muscle tone with easy passive movement; 3, considerable increase in muscle tone with difficult passive movement; 4, rigid limb.
- Coagulation Parameters: Laboratory results for coagulation markers were extracted from the laboratory information system at T0, T1, T7, and T14, including: fibrinogen (FIB), fibrinogen degradation products (FDP), D-dimer (D-D), thrombin-antithrombin III complex (TAT), plasmin-antiplasmin complex (PIC), and thrombomodulin (TM).
Safety Outcomes
Safety-related data were collected from medical records, imaging reports, and adverse event documentation, including: (1) hemorrhagic complications: intracranial hemorrhage expansion, surgical site bleeding requiring re-intervention, gastrointestinal bleeding, or other major bleeding events; (2) falls or injuries during rehabilitation documented in nursing records or incident reports; and (3) mortality at 14 days.
Statistical Analysis
All figures in this study were created using Excel and further processed with SPSS 22.0 statistical software. The Shapiro–Wilk test was applied to evaluate the normality of the data. For continuous variables, those following a normal distribution were described as mean ± standard deviation (SD), while those with a non-normal distribution were presented as median (interquartile range, IQR). Categorical variables were expressed as frequencies and percentages. For between-group comparisons, the independent samples t-test was used for normally distributed continuous variables, while the Mann–Whitney U-test was adopted for non-normally distributed continuous variables. For categorical variables, between-group comparisons were performed using either the chi-square (χ2) test or Fisher’s exact test, with the specific choice depending on the data characteristics. All statistical analyses were conducted with a two-tailed test, and a P-value < 0.05 was considered statistically significant.
Results
Baseline Characteristics
A total of 126 patients were included in this study, with 63 patients in each group. Baseline characteristics are presented in Table 1. The two groups were well-balanced with no significant differences in demographic characteristics, DVT risk factors, hemorrhage characteristics, or baseline coagulation parameters (all P>0.05), indicating successful comparability between groups.
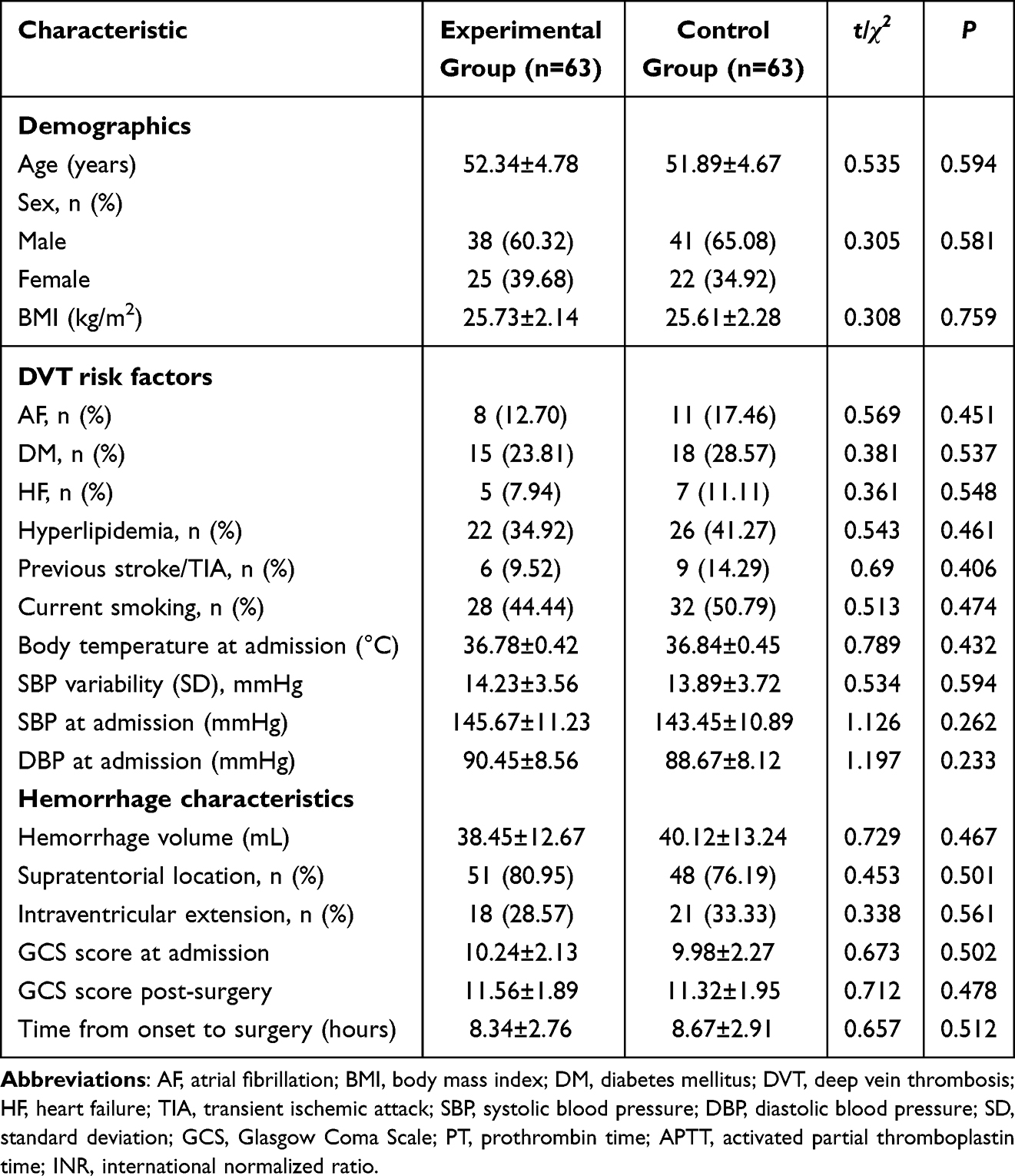 |
Table 1 Baseline Characteristics and DVT Risk Factors of Study Participants |
Muscle Strength Recovery
Muscle strength assessments for both upper and lower limbs are summarized in Table 2. At T0, muscle strength distribution was comparable between groups (P>0.05). Both groups demonstrated progressive improvement in muscle strength over time; however, the experimental group showed significantly greater recovery compared to the control group. The between-group difference became statistically significant at T7 for both upper limbs (U=2.456, P=0.014) and lower limbs (U=2.103, P=0.035), with the disparity widening further by T14 (upper limbs: U=3.124, P=0.002; lower limbs: U=2.876, P=0.004). These findings indicated that ultra-early rehabilitation combined with coagulation monitoring accelerated functional recovery in postoperative HICH patients.
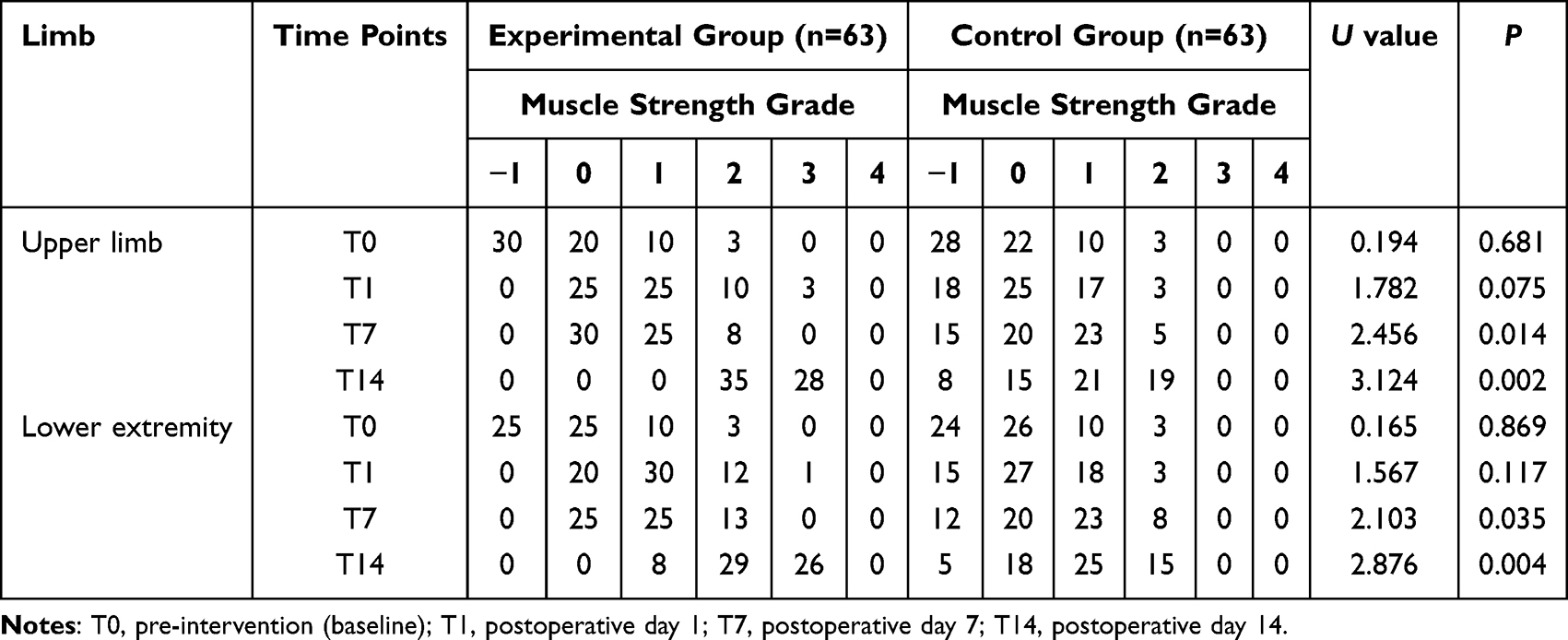 |
Table 2 Comparison of Upper and Lower Limb Muscle Strength Between Groups at Different Time Points |
DVT Incidence and Characteristics
DVT occurrence and characteristics are presented in Table 3. The experimental group demonstrated a significantly lower DVT incidence compared to the control group (12.70% vs 31.75%, P=0.010), representing a relative risk reduction of 60%. Furthermore, patients in the experimental group had significantly fewer large thrombi (diameter >7 mm: 7.94% vs 23.81%, P=0.015), proximal thrombi (4.76% vs 15.87%, P=0.040), and multiple thrombi (6.35% vs 19.05%, P=0.030). These findings suggest that the combined intervention not only reduced DVT incidence but also appeared to prevent more severe thrombotic complications.
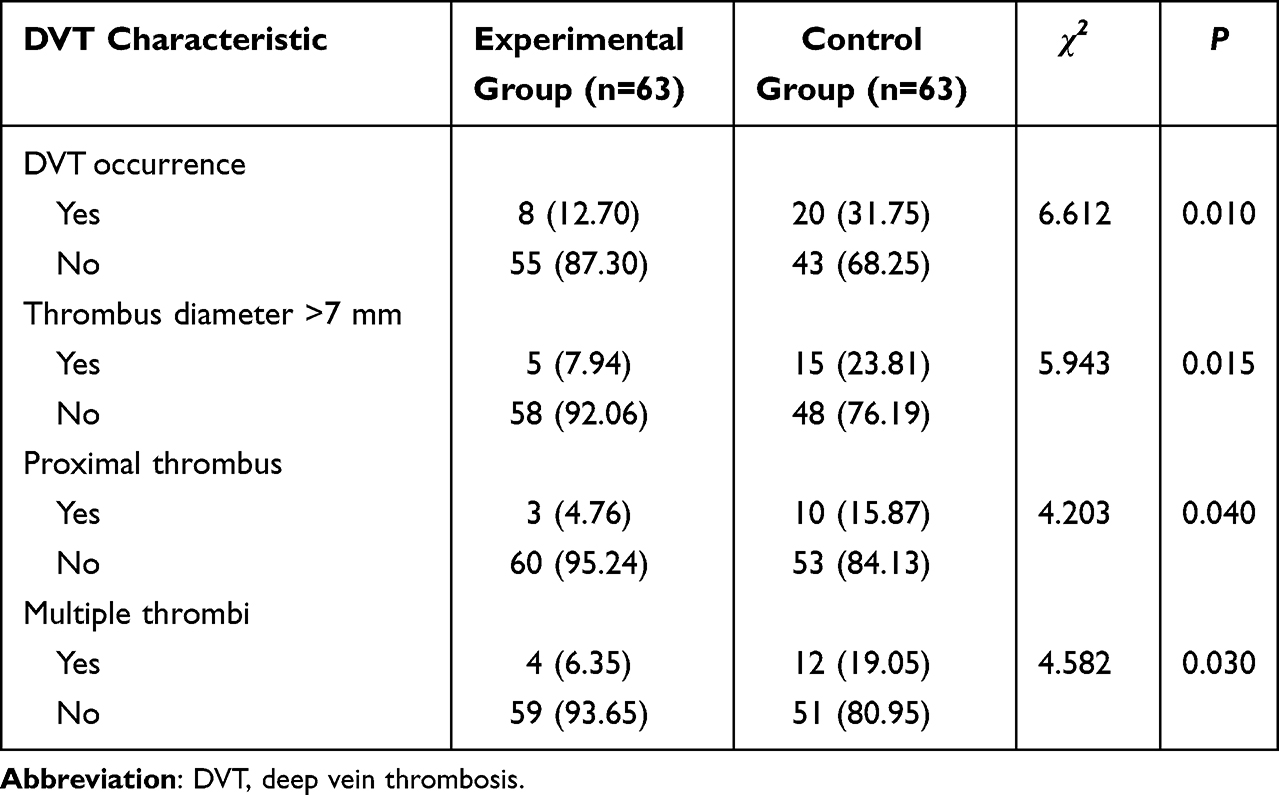 |
Table 3 Incidence and Characteristics of DVT in Two Groups |
Serial Changes in Coagulation Parameters
Temporal changes in coagulation parameters throughout the 14-day observation period are illustrated in Figure 1.
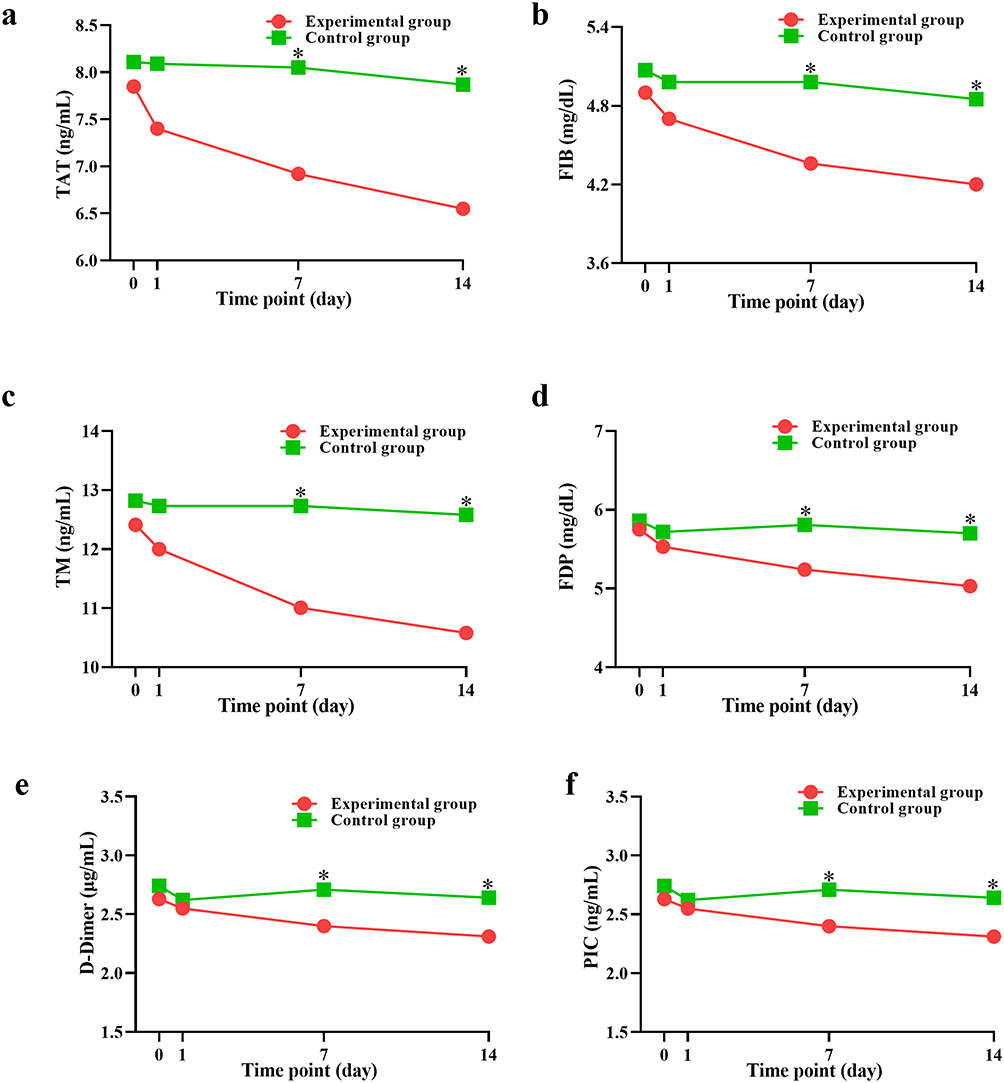 |
Figure 1 Serial changes in coagulation parameters between groups. The figure shows the time-dependent changes in coagulation markers in both the experimental and control groups over 14 days. (a) TAT (ng/mL), (b) FIB (mg/dL), (c) TML (ng/mL), (d) FDP (mg/dL), (e) D-dimer (μg/mL), and (f) PIC (ng/mL). *P < 0.05, comparing the experimental group and the control group at each time point. |
At T1, both groups exhibited elevated coagulation markers consistent with surgical stress and postoperative hypercoagulability, with no significant between-group differences at this time point. However, by T7, the experimental group exhibited lower levels of FIB, FDP, D-dimer, TAT, and PIC compared to the control group (all P<0.05). By T14, these between-group differences became more pronounced, with the experimental group maintaining significantly reduced levels across all monitored coagulation markers (all P<0.05). Within-group comparisons revealed significant decreases in FIB, TAT, and TM from baseline by T14 in the experimental group, indicating favorable modulation of hemostatic balance.
Coagulation Parameters in Patients with and without DVT
Table 4 and Figure 2 compare coagulation parameters between patients who developed DVT (n=28) and those who remained DVT-free (n=98) during the 14-day observation period, irrespective of treatment group allocation. Patients with DVT exhibited significantly elevated levels of all monitored coagulation markers compared to those without DVT, including FIB, FDP, D-dimer, TAT, PIC, and TM (all P<0.01). The magnitude of these differences was substantial, with particularly marked elevations in TAT and FDP levels in the DVT group.
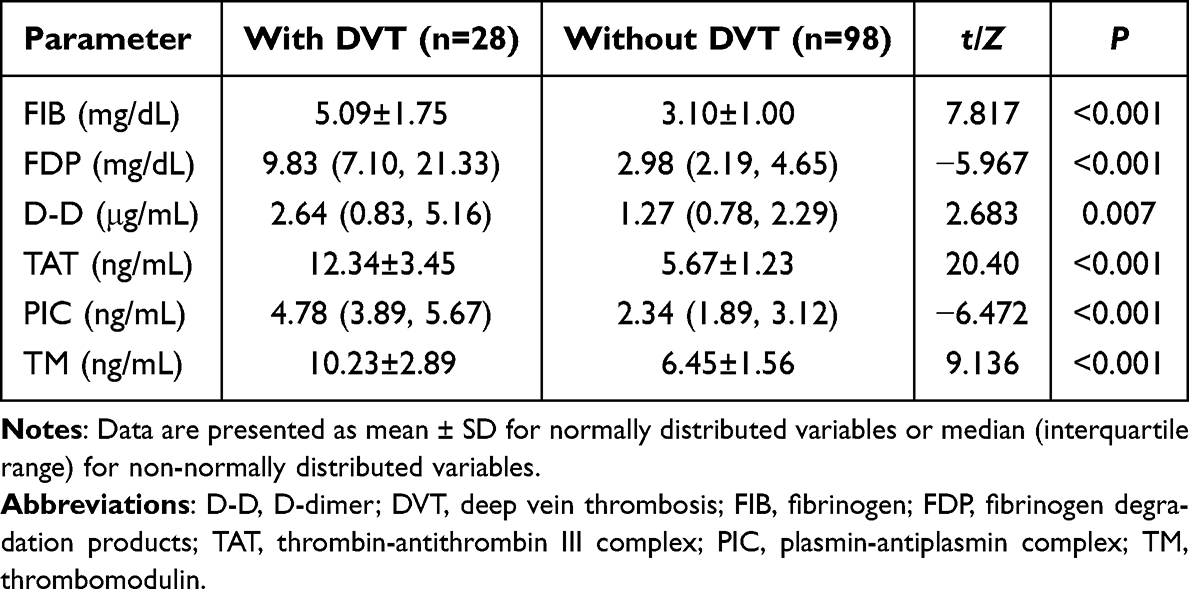 |
Table 4 Comparison of Coagulation Parameters Between Patients with and without DVT |
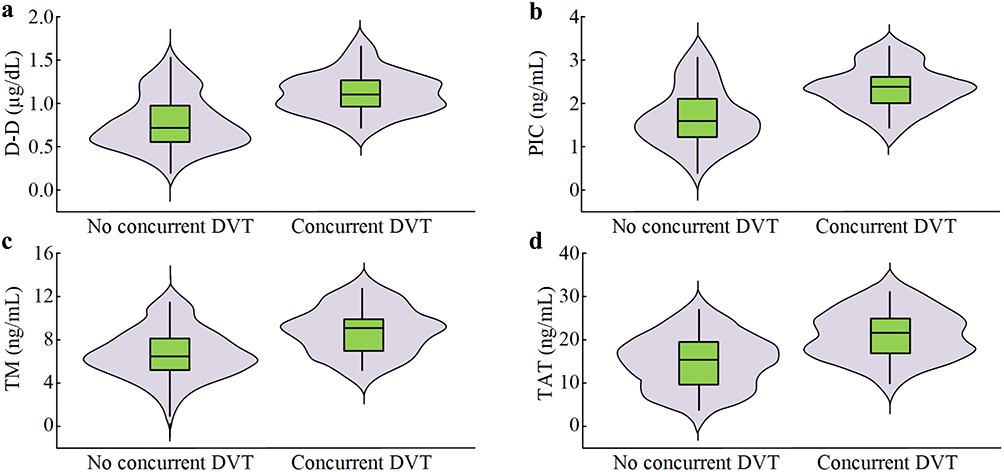 |
Figure 2 Distribution of Coagulation Markers in Patients With and Without DVT. Violin plots illustrating the distribution of key coagulation parameters stratified by DVT occurrence during the 14-day observation period. (a) D-D levels in patients without concurrent DVT compared with those with concurrent DVT. (b) PIC levels in patients without concurrent DVT compared with those with concurrent DVT. (c) TM levels in patients without concurrent DVT compared with those with concurrent DVT. (d) TAT levels in patients without concurrent DVT compared with those with concurrent DVT. |
Safety Outcomes
Safety outcomes throughout the 14-day observation period are presented in Table 5. Hemorrhagic complications were rare and comparable between groups, with no significant differences in ICH expansion, surgical site bleeding, gastrointestinal bleeding, or any major bleeding events (all P>0.05). Importantly, no falls or injuries during rehabilitation were documented in either group, indicating that the ultra-early mobilization protocol was safely implemented. The 14-day mortality rate was low and similar between groups (P=0.558). Notably, the experimental group demonstrated significantly shorter length of hospital stay compared to the control group (P<0.001).
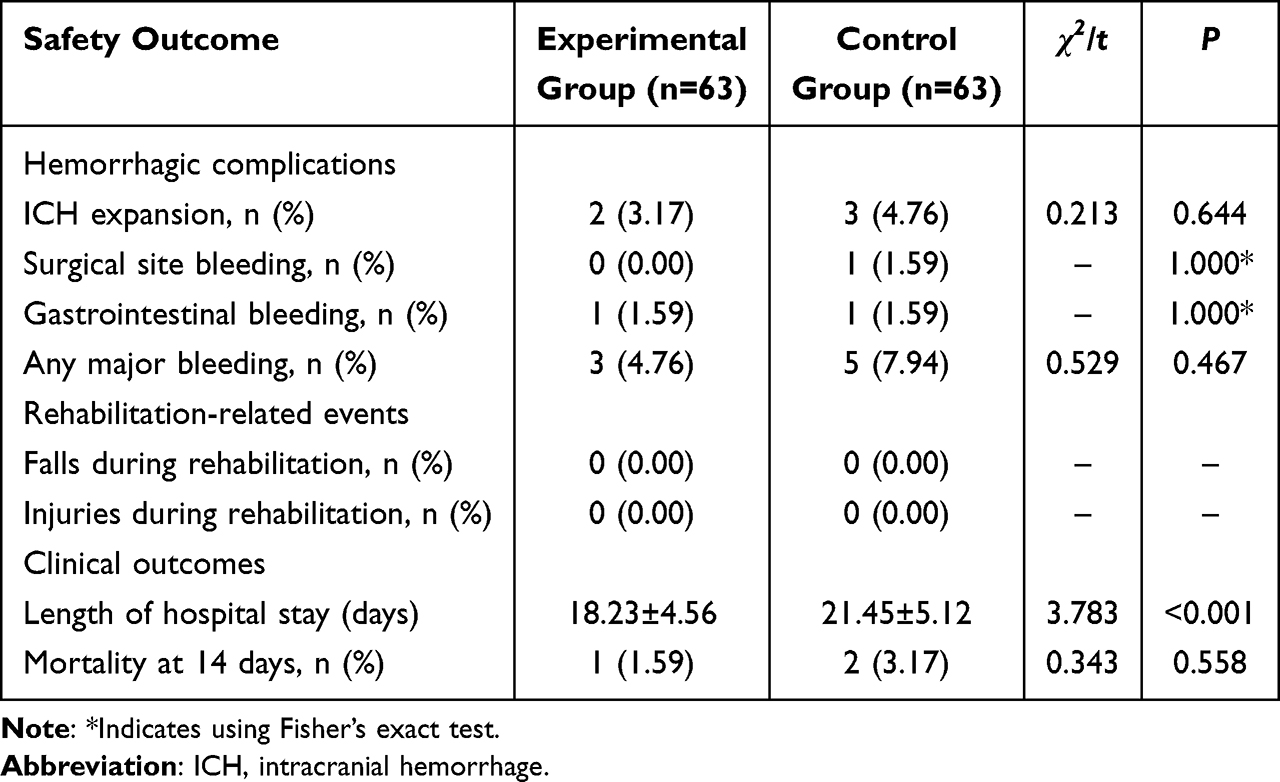 |
Table 5 Safety Outcomes During the 14-Day Observation Period |
Discussion
The present study observed that muscle strength recovery in both upper and lower limbs appeared more favorable in the experimental group compared to the control group, with differences becoming apparent by T14. The DVT incidence was notably lower in the experimental group compared to the control group, suggesting a potential association between ultra-early rehabilitation training and DVT prevention after HICH surgery. These findings are supported by recent evidence which suggest that ultra-early rehabilitation training can reduce the incidence of postoperative DVT.14–16 However, these studies primarily focused on single treatment approaches, lacking evaluation of combined therapies. This study further explores temporal changes in coagulation indicators, providing additional insights into assessing thrombotic activity.
The observed association between early rehabilitation and DVT reduction may involve several mechanisms. Enhanced venous return through active and passive limb movements could potentially reduce blood stasis in the lower extremities, a key component of Virchow’s triad. Recent evidence has suggested that early mobilization within 48 hours post-neurosurgery may improve venous flow velocity compared to delayed mobilization protocols.17 The improvement in muscle strength recovery observed in this study might contribute to venous pump function. A recent multi-center study exploring hemorrhagic transformation after thrombolysis in atrial fibrillation patients identified that early mobilization appeared to modify inflammatory responses, suggesting that rehabilitation interventions may exert effects beyond purely mechanical factors.18 The timing of rehabilitation initiation is crucial, as hypercoagulable states following neurosurgical procedures tend to peak within the initial postoperative week. Recent longitudinal data from patients with embolic stroke indicated that the risk window for thrombotic complications extended through the second postoperative week, which supports sustained intervention during this period.19 Compared to the findings previous investigations, this study shows that coagulation indicators began to decline at T7 after ultra-early rehabilitation intervention and decreased more notably at T14.20–22 The observed pattern raises the possibility that ultra-early rehabilitation may attributed to the earlier intervention in this study, indicating that ultra-early rehabilitation can initiate improvements in blood circulation and regulation of the coagulation system sooner, thereby accelerating DVT prevention.
The incorporation of daily coagulation monitoring to guide rehabilitation progression represents an approach that differs from conventional early mobilization protocols. The temporal pattern of coagulation marker decline observed in the experimental group suggests a possible relationship between appropriately timed physical activity and hemostatic balance. Evidence from orthopedic surgery populations has suggested that mechanical stimulation through rehabilitation exercises may influence endothelial function and thrombomodulin expression.23,24 The use of TAT, PIC, and TM measurements provided earlier detection of hypercoagulable states compared to conventional markers alone in this cohort. Previous validation studies in surgical populations have indicated that TAT may offer improved sensitivity compared to D-dimer in the early postoperative period for predicting venous thromboembolism.25,26
The experimental group also appeared to have fewer proximal and large-diameter thrombi, which are generally associated with higher risks of pulmonary embolism and post-thrombotic syndrome. Recent data from cancer-associated DVT populations have suggested that thrombus location and burden may independently influence long-term outcomes, emphasizing the clinical relevance of preventing more severe thrombotic presentations.27 Registry data have indicated that early intervention in proximal DVT may be associated with reduced post-thrombotic syndrome development, suggesting that preventing thrombus extension could be as important as preventing initial thrombus formation.8
The safety profile observed with ultra-early rehabilitation in this hemorrhagic population addresses a concern that has historically limited mobilization protocols. The comparable rates of hemorrhagic complications between groups, despite earlier and more intensive mobilization in the experimental group, suggests that coagulation-guided progression may provide adequate safety monitoring. A recent meta-analysis of heparin prophylaxis in spontaneous intracerebral hemorrhage found that timing and dosing adjustments based on coagulation parameters were associated with reduced bleeding complications without compromising thromboprophylaxis efficacy.13 The absence of falls or rehabilitation-related injuries in either group reflects the feasibility of implementing structured mobilization protocols in neurologically compromised patients.
This study still has several limitations. The retrospective design precluded randomization and may have introduced selection bias. The sample size limited the ability to perform subgroup analyses based on hemorrhage severity, location, or comorbidities. Individual variability in rehabilitation tolerance and compliance could not be fully quantified retrospectively and may have influenced outcomes. The stringent inclusion criteria requiring fully normal pre- and postoperative coagulation function may have excluded a substantial proportion of clinically relevant patients, thereby limiting the generalizability of findings to broader HICH populations with varying degrees of coagulation abnormalities. The 14-day observation period may have missed delayed thrombotic events occurring after hospital discharge. Additionally, unmeasured factors such as patients’ underlying conditions and rehabilitation compliance may have influenced the intervention outcomes. Future prospective randomized controlled trials with extended follow-up periods and larger sample sizes would strengthen the evidence base. Investigating specific coagulation thresholds for safe rehabilitation progression could enhance protocol standardization. Evaluating cost-effectiveness and long-term functional outcomes, including patient-reported measures and quality of life assessments, would provide important information for clinical decision-making beyond the clinical endpoints examined in this study.
Conclusion
This retrospective study suggests that ultra-early rehabilitation combined with coagulation-guided monitoring may be associated with reduced DVT incidence following HICH surgery. The observed improvements in muscle strength recovery and favorable modulation of hemostatic markers (FIB, FDP, D-dimer, TAT, PIC, TM) warrant further investigation. However, several limitations constrain interpretation, including the non-randomized design, relatively modest sample size, and potential unmeasured confounders such as rehabilitation adherence and underlying comorbidities. Prospective randomized controlled trials with larger cohorts and extended follow-up periods are needed to validate these preliminary findings and establish standardized coagulation thresholds for optimizing individualized thromboprophylaxis protocols in this vulnerable population.
Ethics Statement
This study was conducted in accordance with the Declaration of Helsinki. This study was approved by the Ethics Committee of Xuzhou Medical Center (Ethics Approval No.: XZXY-LK-20230626-091).
Funding
This work was supported by the 2022 Medical Scientific and Technological Innovation Project of Xuzhou Health Commission (Grant No.: XWKYHT20220109). The funder had no role in the design of the study, collection, analysis, and interpretation of data, or in the writing of the manuscript.
Disclosure
The authors declare no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Yuan Z, Wang Q, Sun Q, Li C, Xiong F, Li Z. Hypertensive intracerebral hemorrhage: which one should we choose between laser navigation and 3D navigation mold? Front Surg. 2023;10:1040469. doi:10.3389/fsurg.2023.1040469
2. Puissant MM, Mayer SA, Goldstein JN. Emergency priorities in the treatment of cerebral hemorrhage: code-intracerebral hemorrhage. Neurol Clin. 2025;43(1):127–139. doi:10.1016/j.ncl.2024.07.007
3. Das AS, Mallick A, Mora SA, et al. Hypertension control after intracerebral hemorrhage among varying small vessel disease etiologies. Neurol Sci. 2024;45(10):4913–4921. doi:10.1007/s10072-024-07560-2
4. Lian M, Li X, Wang Y, Che H, Yan Z. Comparison of two minimally invasive surgical approaches for hypertensive intracerebral hemorrhage: a study based on postoperative intracranial pressure parameters. BMC Surg. 2024;24(1):10. doi:10.1186/s12893-023-02306-x
5. Abulhasan YB, Teitelbaum J, Al-Ramadhani K, Morrison KT, Angle MR. Functional outcomes and mortality in patients with intracerebral hemorrhage after intensive medical and surgical support. Neurology. 2023;100(19):e1985–e1995. doi:10.1212/WNL.0000000000207132
6. Germans MR, Rohr J, Globas C, et al. Challenges in coagulation management in neurosurgical diseases: a scoping review, development, and implementation of coagulation management strategies. J Clin Med. 2023;12(20):6637. doi:10.3390/jcm12206637
7. Zhang Z, Cai H, Vleggeert-Lankamp CLA. Thromboembolic prophylaxis in neurosurgical practice: a systematic review. Acta Neurochir. 2023;165(11):3119–3135. doi:10.1007/s00701-023-05792-3
8. Prandoni P, Haas S, Fluharty ME, et al. Incidence and predictors of post-thrombotic syndrome in patients with proximal DVT in a real-world setting: findings from the GARFIELD-VTE registry. J Thromb Thrombolysis. 2024;57(2):312–321. doi:10.1007/s11239-023-02895-7
9. Parmar CD, Felsenreich DM, Salminen P, Di Lorenzo N, Prager G. Guidelines for management of Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE) occurring after Metabolic Bariatric Surgery (MBS). Obes Surg. 2024;34(5):1964–1968. doi:10.1007/s11695-024-07187-4
10. Li L, Huang Y, He J, Zheng Q. Early rehabilitation nursing prevents postoperative DVT and promotes limb function recovery in patients with traumatic fracture. Am J Transl Res. 2025;17(4):2665–2677. doi:10.62347/WLTS7477
11. Liu F, Tan J, Pan Y. Prevention of deep vein thrombosis in postoperative orthopedic patients: a hybrid meta-analysis and clinical case study. Front Med. 2025;12:1603191. doi:10.3389/fmed.2025.1603191
12. Zhang H, Deng J, Sun N, et al. Effect of coagulation function on cerebral microbleeds in intracerebral hemorrhage. Brain Behav. 2020;10(6):e01634. doi:10.1002/brb3.1634
13. Zhou Y, Wang G, Xue C, et al. Effect of heparin for the prevention of venous thromboembolism in patients with spontaneous intracranial cerebral hemorrhage: a meta-analysis. Ther Adv Drug Saf. 2024;15:20420986241253469. doi:10.1177/20420986241253469
14. Wang Y, Zhu Y, Yang B. Effects of doctor-nurse integrated care combined with health education on hip function, incidence of deep vein thrombosis and nursing satisfaction in patients with hip arthroplasty. Altern Ther Health Med. 2023;29(6):254–259.
15. Zheng T, Zheng X. Outcome of preventive nursing intervention, prophylactic anticoagulation and the use of the Caprini score on venous thromboembolism after varicose vein surgery. Afr Health Sci. 2023;23(3):616–623. doi:10.4314/ahs.v23i3.72
16. Luo X, Huang X, Shi J, Xia L. The impacts of fast-track surgery on postoperative deep venous thrombosis among patients with lower limb fracture. Altern Ther Health Med. 2025;31(1):168–175.
17. Chen X, Wan L, Wang B. Early mobilization in postoperative glioma patients real world impact on recovery and long term prognosis. Sci Rep. 2025;15(1):18032. doi:10.1038/s41598-025-01871-w
18. Ahmed SR, Zeinhom MG, Ebied AAMK, et al. A multi-center study on the predictors of different subtypes of hemorrhagic transformation of brain infarction after thrombolysis in atrial fibrillation patients presented with embolic stroke. Sci Rep. 2025;15(1):15655. doi:10.1038/s41598-025-97968-3
19. Zeinhom MG, Khalil MFE, Elmesallami AG, et al. Predictors of post-alteplase long-term unfavorable outcome in atrial fibrillation patients presented with embolic stroke in the Middle East and North Africa Regions: a multi-center, longitudinal study. Neurol Ther. 2025;14:2359–2373. doi:10.1007/s40120-025-00814-x
20. Yamanaka S, Miyake R, Yamada Y, et al. Tissue factor pathway inhibitor 2: a novel biomarker for predicting asymptomatic venous thromboembolism in patients with epithelial ovarian cancer. Gynecol Obstet Invest. 2022;87(2):133–140. doi:10.1159/000524804
21. Shi LT, Kong FQ. Evaluation of preoperative coagulation function changes and deep vein thrombosis incidence in elderly patients with hip fractures. Clin Hemorheol Microcirc. 2024;87(3):375–382. doi:10.3233/CH-242122
22. Zheng J, Han M, Chen J, Deng MM, Luo G. Predictive value of D-dimer and fibrinogen degradation product for splanchnic vein thrombosis in patients with severe acute pancreatitis: a single-center retrospective study. Scand J Gastroenterol. 2023;58(10):1166–1172. doi:10.1080/00365521.2023.2215367
23. Yang Y, Feng G, Yan J, et al. Plasminogen activator inhibitor-1, thrombin-antithrombin, and prothrombin fragment F1+2 have higher diagnostic values than D-dimer for venous thromboembolism after TKA. Clin Appl Thromb Hemost. 2022;28:10760296221097383. doi:10.1177/10760296221097383
24. Cheng Y, Liu J, Su Y, et al. Clinical impact of coagulation and fibrinolysis markers for predicting postoperative venous thromboembolism in total joint arthroplasty patients. Clin Appl Thromb Hemost. 2019;25:1076029619877458. doi:10.1177/1076029619877458
25. Wu Z, Du Y, Cai X, Xu Q. Caprini score combined with thrombotic molecular markers for predicting DVT in patients with traumatic fractures. Sci Rep. 2025;15(1):1847. doi:10.1038/s41598-025-85941-z
26. Qiu Y, Han S, Ji Y, Lu Z, Huang X. Development of a thrombin-antithrombin complex detection kit and study in venous thromboembolism complicated by cervical cancer. BMC Biotech. 2024;24(1):103. doi:10.1186/s12896-024-00930-w
27. Galanaud JP, Trujillo-Santos J, Bikdeli B, et al. Clinical presentation and outcomes of patients with cancer-associated isolated distal deep vein thrombosis. J Clin Oncol. 2024;42(5):529–537. doi:10.1200/JCO.23.00429
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.