Back to Journals » Therapeutics and Clinical Risk Management » Volume 16
Refractory Sarcoidosis: A Review
Authors El Jammal T, Jamilloux Y ![]() , Gerfaud-Valentin M, Valeyre D, Sève P
, Gerfaud-Valentin M, Valeyre D, Sève P
Received 29 November 2019
Accepted for publication 22 March 2020
Published 17 April 2020 Volume 2020:16 Pages 323—345
DOI https://doi.org/10.2147/TCRM.S192922
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Thomas El Jammal,1 Yvan Jamilloux,1 Mathieu Gerfaud-Valentin,1 Dominique Valeyre,2 Pascal Sève1,3
1Department of Internal Medicine, Lyon University Hospital, Lyon, France; 2Department of Pneumology, Assistance Publique - Hôpitaux de Paris, Hôpital Avicenne et Université Paris 13, Sorbonne Paris Cité, Bobigny, France; 3Hospices Civils de Lyon, Pôle IMER, Lyon, F-69003, France, University Claude Bernard Lyon 1, HESPER EA 7425, Lyon F-69008, France
Correspondence: Pascal Sève
Service de Médecine Interne, Groupement Hospitalier Nord, 103 Grande rue de la Croix-Rousse, Lyon F-69004, France
Tel +33 426 732 636
Fax +33 426 732 637
Email [email protected]
Abstract: Sarcoidosis is a multi-system disease of unknown etiology characterized by granuloma formation in various organs (especially lung and mediastinohilar lymph nodes). In more than half of patients, the disease resolves spontaneously. When indicated, it usually responds to corticosteroids, the first-line treatment, but some patients may not respond or tolerate them. An absence of treatment response is rare and urges for verifying the absence of a diagnosis error, the good adherence of the treatment, the presence of active lesions susceptible to respond since fibrotic lesions are irreversible. That is when second-line treatments, immunosuppressants (methotrexate, leflunomide, azathioprine, mycophenolate mofetil, hydroxychloroquine), should be considered. Methotrexate is the only first-line immunosuppressant validated by a randomized controlled trial. Refractory sarcoidosis is not yet a well-defined condition, but it remains a real challenge for the physicians. Herein, we considered refractory sarcoidosis as a disease in which second-line treatments are not sufficient to achieve satisfying disease control or satisfying corticosteroids tapering. Tumor necrosis alpha inhibitors, third-line treatments, have been validated through randomized controlled trials. There are currently no guidelines or recommendations regarding refractory sarcoidosis. Moreover, criteria defining non-response to treatment need to be clearly specified. The delay to achieve response to organ involvement and drugs also should be defined. In the past ten years, the efficacy of several immunosuppressants beforehand used in other autoimmune or inflammatory diseases was reported in refractory cases series. Among them, anti-CD20 antibodies (rituximab), repository corticotrophin injection, and anti-JAK therapy anti-interleukin-6 receptor monoclonal antibody (tocilizumab) were the main reported. Unfortunately, no clinical trial is available to validate their use in the case of sarcoidosis. Currently, other immunosuppressants such as JAK inhibitors are on trial to assess their efficacy in sarcoidosis. In this review, we propose to summarize the state of the art regarding the use of immunosuppressants and their management in the case of refractory or multidrug-resistant sarcoidosis.
Keywords: refractory sarcoidosis, JAK inhibitors, anti-TNF
Introduction
Sarcoidosis was first described by Besnier et al in 1889.1 It is a multi-systemic disease of unknown etiology characterized by the infiltration of various tissues by non-caseating granulomas. Even if sarcoidosis remains a disease of unknown etiology, the mechanisms underlying granuloma formation are well understood.2 Sarcoidosis can affect people from any ethnicity and occurs at any time of life although more often in young adults with onset occurring later in females than males. About 70% of cases involve 25- to 40-year-old patients at presentation and a second peak of incidence is observed in women over 50 years old.3 Its incidence is estimated between 2.3 and 11 per 100000 individuals/year.4 The estimated prevalence varies from 2.17 to 160 cases per 100,000 individuals (this large variability could be explained by the diagnostic tools used to define sarcoidosis in older series, plus the ethnicity of each cohort). Sarcoidosis’ course can be divided into two distinct groups: a time-limited course (two-thirds of patients evolve through a self-remitting disease within 12 to 36 months),3–5 and a chronic course (10% to 30% of patients requiring prolonged treatment). Not all sarcoidosis patients require a systemic treatment, which is often reserved for life-threatening organ involvement (advanced pulmonary fibrosis and pulmonary hypertension, central nervous system (CNS), heart, renal sarcoidosis, etc.) or functional threat (severe or defacing skin disease, larynx involvement, and/or posterior uveitis).6 Functional symptoms and impaired quality of life also represent an indication for treatments. Ethnicity (especially African-American and Afro-Caribbean origins), age above 40 at presentation, lupus pernio, chronic uveitis, sinonasal and osseous localizations, CNS involvement, cardiac involvement, severe hypercalcemia, nephrocalcinosis, and radiographic stages III and IV have been associated with a poorer prognosis.7
Corticosteroids (CS) are the cornerstone of treatment for sarcoidosis but, in some patients, may not result in satisfactory clinical response or else lead to clinical response with unacceptable side effects. In such cases, additional treatments must be considered, either to achieve disease control or CS sparing.
Pathophysiology of Sarcoidosis and Granuloma Formation
Granuloma is a defense mechanism of the immune system to contain various antigens.8 Sarcoidosis is currently considered as an exuberant immune response against unknown antigens. Many antigens may trigger granuloma formation (bacteria, fungi, viruses,9,10 or nanoparticles10). Circulating monocytes recognize a specific antigen which interacts with monocytes pattern recognition receptors (Toll-like receptors (TLR) and especially TLR2 which is known to transduce signals mediated by bacterial lipoproteins)11 and then differentiate into specific antigen-presenting cells (macrophages or dendritic cells (DCs)).12 Macrophages then aggregate into epithelioid cells to form immature granuloma. The fusion of monocytes-macrophages generates multinucleated giant cells (MGC) then surrounded by T and B lymphocytes. Th1 lymphocytes (induced under cytokine secretion by MGC and macrophages) generate Th1-specific cytokines (interferon-gamma (IFN-γ), IL-2, tumor necrosis factor-α (TNF-α)), which promote inflammation at granuloma sites13 and help the granuloma to maintain its structure.14 Secretion by DCs of interleukin (IL)-6, IL-23 and IL-12 promotes another type of polarized T cells, which are Th17 cells also promoting inflammation. Of note, a particular type of Th17 cells was found to be relevant in sarcoidosis, a subtype of IFN-γ producing Th17 cells called Th17.1 cells.15
Autophagic process disruption could promote granuloma formation. Indeed, several polymorphisms in genes implicated in autophagy were also shown to be linked with sarcoidosis.16 The lack of clearance of certain antigens may represent one possible explanation for the granulomatous reaction linked to autophagy failure.
A better understanding of granuloma formation pathophysiology may help explain why various treatments, especially antimalarial drugs (which are known to modulate autophagy), targeted therapies such as TNF inhibitors (TNFi) and biodrugs targeting cytokines (tocilizumab (TCZ) against interleukin 6 receptor (IL-6R)) or their pathway (Janus kinase (JAK) inhibitors), can be effective in the course of sarcoidosis.
What is Refractory Sarcoidosis?
No consensual definition of refractory sarcoidosis is available in guidelines and medical literature; accordingly, the rate of refractory sarcoidosis patients is unknown.
In the STAT cohort (sarcoidosis treated with TNFi), refractory sarcoidosis was defined as a condition in which second-line immunosuppressants were not sufficient to achieve satisfactory control of the disease.17 In 2017, Korsten et al defined refractory pulmonary sarcoidosis as a condition in which CS cannot be tapered under the dose of 10 mg/day or was responsible for worrying side-effects.18 In a prospective trial, Sweiss et al defined refractory pulmonary sarcoidosis as patients with symptomatic sarcoidosis under CS over 10 mg/day or symptomatic sarcoidosis with a CS-sparing agent (CSA).19 We chose to define refractory sarcoidosis as a situation in which CS and second-line treatment(s) (methotrexate, azathioprine, leflunomide, antimalarials, or mycophenolate mofetil) are not sufficient to achieve clinical remission with a CS dosage under 10 mg/d.
Is Sarcoidosis Refractory?
The diagnosis of sarcoidosis is based on an evocative clinico-radiological presentation and evidence of noncaseating granulomas on biopsy specimens after exclusion of other granulomatous disorders. The sarcoidosis organ assessment instrument of the World Association of Sarcoidosis and Other Granulomatous Diseases is used to classify the diagnosis of sarcoidosis organ involvement is highly probable, probable, or possible20 while Bickett et al recently proposed a Sarcoidosis Diagnosis Score to help sarcoidosis diagnostic evaluation.21 Many diseases or pathological conditions may mimic sarcoidosis (Table 1). Atypical manifestations which may challenge the diagnosis of sarcoidosis are hemoptysis, crackles, digital clubbing, unilateral hilar lymphadenopathy or isolated mediastinal lymphadenopathy without hilar lymph node enlargement, compressive lymphadenopathy, non-lymphatic diffuse lung micronodules, cavitary mass on chest X-ray, and hypogammaglobulinemia.22,23 After the initial diagnosis, new organ involvement by sarcoidosis is rare and even more so once the disease remits.24 Accordingly, such unusual circumstances should question the assertion of sarcoidosis and lead the clinician to verify occupational and environmental exposures susceptible of inducing granulomatosis as well as links to infections (contact with tuberculosis, endemic risk for histoplasmosis or leprae). In such cases, clinicians are encouraged to repeat histologic samples and microbiologic analyses, including standard staining and cultures, as well as 16S-RNA and specific polymerase chain reaction analysis (PCR). Accurate pathological diagnosis is also crucial since neoplastic disorders and especially lymphoma can mimic sarcoidosis.25
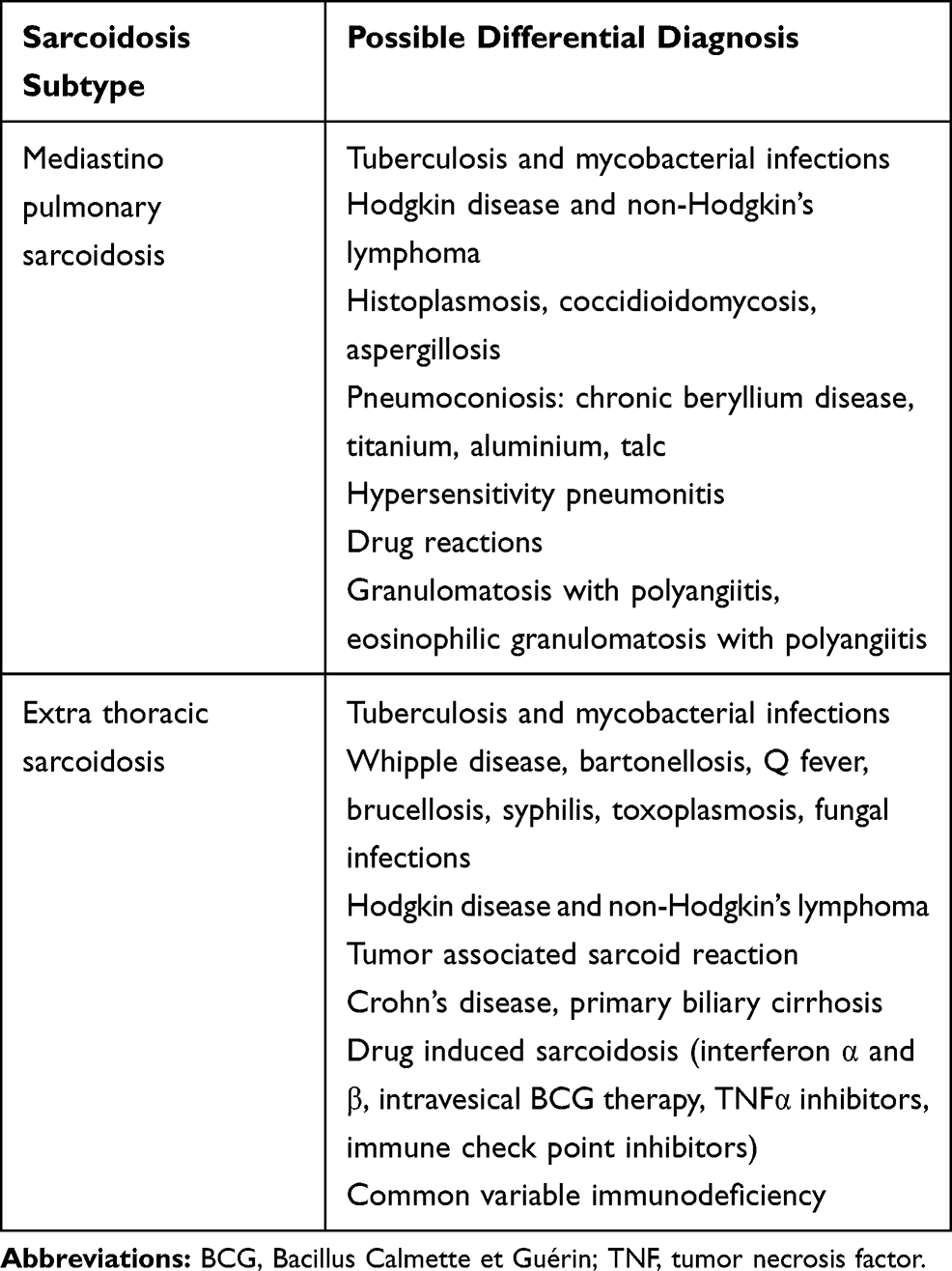 |
Table 1 Main Differential Diagnoses to Exclude in Sarcoidosis |
Infectious Granulomatosis
Tuberculosis remains the main differential diagnosis of sarcoidosis26 but some biological and histological elements can help to distinguish one from the other. Interferon-γ release assays (IGRA) have the same sensitivity as in the general population and are not affected by sarcoidosis activity as opposed to classic tuberculin skin testing (i.e., anergy).27 Mycobacterium-specific PCR despite its low sensitivity may be useful to differentiate tuberculosis and atypical mycobacterial infections28,29 from sarcoidosis. Caseating granuloma is atypical in sarcoidosis. It is evocative but not pathognomonic of tuberculosis. Atypical mycobacteria and histoplasmosis are also classical infectious differential diagnoses. Tropheryma whipplei infection is sometimes mistaken as sarcoidosis since granuloma formation within lymph nodes is not uncommon.30
Other Inflammatory Diseases
Among inflammatory diseases with granulomatous manifestations, granulomatosis with polyangiitis (GPA) and eosinophilic granulomatosis with polyangiitis (EGPA) may be differential diagnoses when the lung is involved. In inflammatory bowel diseases and more specifically Crohn’s disease, non-caseating granulomas are also possible features.31
Drug-Induced Granulomatosis
Drug-induced sarcoid-like reactions (SLRs) are common with IFN therapy (especially interferon alpha), which was known to induce granulomatous reactions with lung involvement in up to 76% of patients with hepatitis C and granulomatosis.32 Cutaneous granulomas were also noticed in 60% of cases. Drug-induced SLRs have also been described with TNFi and especially with etanercept (ETN).33 Among new therapies, immune checkpoint inhibitors, such as anti-cytotoxic T-lymphocyte-associated protein 4 (CTLA4) antibodies (ipilimumab) and anti-programmed cell death protein 1 (PD1) (nivolumab, pembrolizumab) or anti-PDL1 (ligand) antibodies (atezolizumab, durvalumab, avelumab) may trigger drug-induced SLRs.33 BRAF and MEK inhibitors (dabrafenib, vemurafenib, trametinib, cobimetinib) were also associated with SLRs in 37 patients in medical literature.34 SLRs occurring during cancer immunotherapy are generally characterized by paucisymptomatic lung, skin, and mediastinal hilar lymph nodes involvement. The onset of such manifestations varies between 1 and 22 months with a mean time of onset at 6 months after initiation of treatment.35,36
Common Variable Immunodeficiency
Systemic granulomatosis can occur in the course of common variable immunodeficiency (CVID).37 Bouvry et al observed several differences in biological and clinical findings comparing CVID related granulomatous disease (CVID-RGD) and sarcoidosis. Patients with CVID-RGD were more likely to present with hepato- and splenomegaly compared to sarcoidosis patients. CVID-RGD patients had also more frequently history of recurrent infections and autoimmune diseases (especially autoimmune cytopenia). CD4/CD8 ration in bronchoalveolar fluid was slightly more elevated in sarcoidosis than CVID-RGD. Chest computed tomography patterns were also different. Nodules and peribronchovascular micronodules were more frequent in sarcoidosis whereas nodules with halo signs were more frequently seen in CVID-RGD patients. For the clinician, the distinction between sarcoidosis and CVID can be made on the basis of the gammaglobulin levels on electrophoresis.
Neoplastic Disorders
Differentiating malignancies from sarcoidosis is of the utmost importance, since a wrong diagnosis, and the ensuing delay in properly treating the underlying malignancy, especially lymphomas, can be deleterious.38 Of note, sarcoidosis may precede, follow, or occur concurrently with a number of cancers, especially lymphomas, thus representing a diagnostic challenge.25,36,39 Both cancer and sarcoidosis are 18-fluorodeoxyglucose (18-FDG) avid; therefore 18-FDG positron emission tomography (PET) may be useful in selecting possible biopsy sites (in priority, sites with the greatest 18-FDG uptake), but not in distinguishing between the two entities.24 If uncertainty remains, multiple biopsies may be needed to determine whether all FDG-avid sites are involved with sarcoidosis or whether they harbor cancer cells as well.
Poor Treatment Adherence
Only very rare cases of sarcoidosis fail to respond to combined CS and second-line immunosuppressants, a situation which may suggest either poor treatment adherence or, as seen above, another granulomatous disease. Hydroxychloroquine (HCQ) levels as well as azathioprine (AZA) metabolites and mycophenolate mofetil (MMF) concentrations can be easily determined to assess patient adherence. However, currently there are no recommendations regarding therapeutic target values for these drugs in sarcoidosis.
Inherent Immunosuppression
Inherent immunosuppression is a consideration the physician must pay careful attention to when managing active sarcoidosis. Even if this condition is not well understood, several cases of opportunistic infections (cryptococcosis,40 progressive multifocal leukoencephalopathy)41 have been described in sarcoidosis even in patients with no immunosuppressants and with no human immunodeficiency virus (HIV) coinfection. Of note, several patients in those series had normal CD4 blood levels. Currently, inherent suppression in sarcoidosis is not a well-known condition but serious infectious risk should be considered when treating severe and refractory sarcoidosis to limit the side-effects of immunosuppressants, especially if the latter not strictly necessary.
What are Sarcoidosis First-Line Treatments?
There is no cure for chronic sarcoidosis, and treatment only changes the granulomatous process and its clinical consequences. The general indications for systemic therapy are shown in Table 2. In most cases, sarcoidosis is a self-remitting disease which does not require any treatment. Martusewicz-Boros et al reported only 16% of the patients requiring systemic treatment within a cohort of 1810 sarcoidosis.42
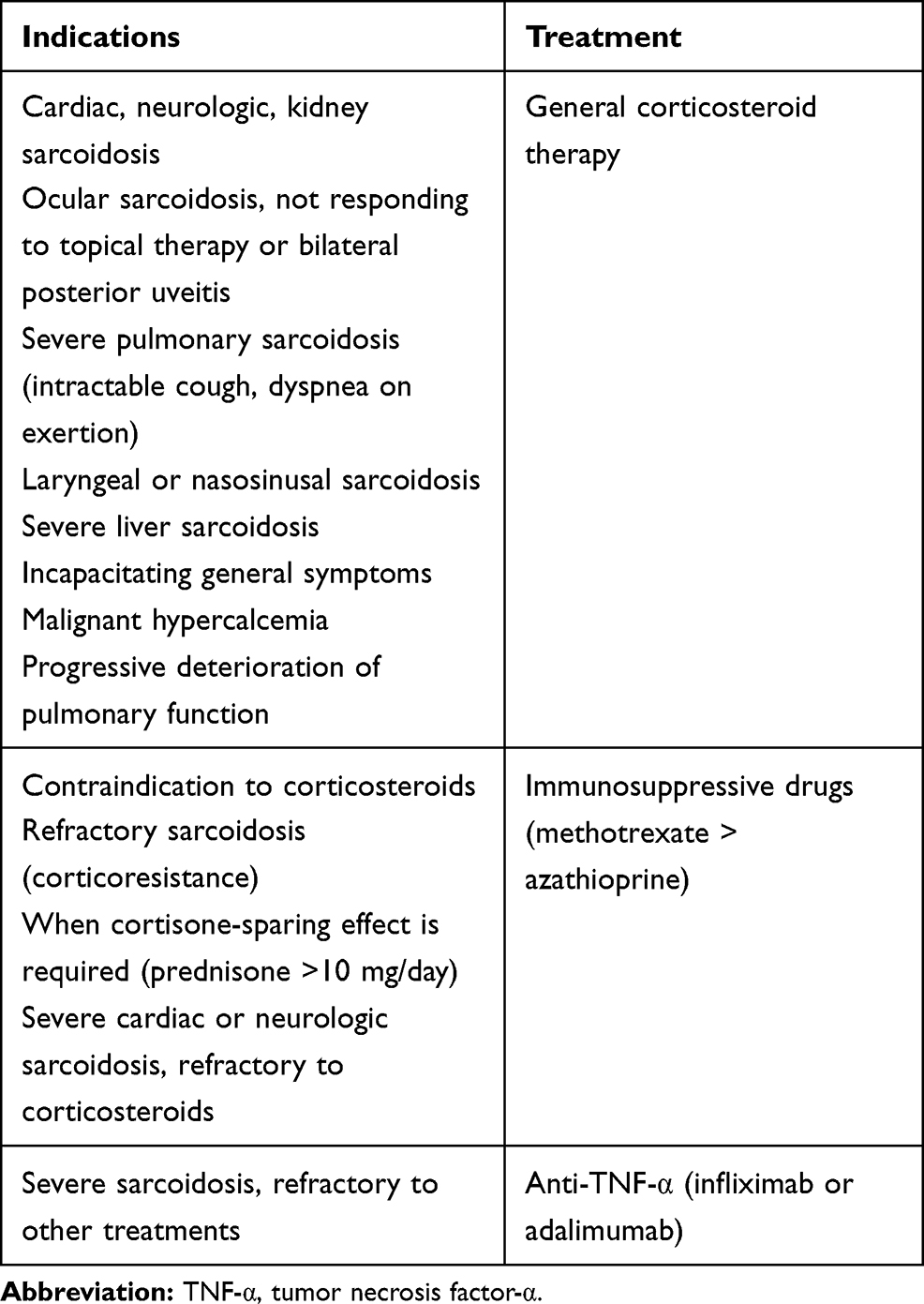 |
Table 2 Indications for the Treatment of Sarcoidosis |
CS remain the cornerstone of sarcoidosis treatment.6,7 Their efficacy has been shown in randomized controlled trials, particularly on pulmonary sarcoidosis.43 Overall, a response to CS is obtained in 80% to 90% of patients, from a few weeks (3 to 4 weeks in case of lung involvement,44 4 weeks in case of renal involvement)45 to 3 months with a complete response often obtained at 6 weeks.46 Therefore, CS are the preferred first-line treatment since second-line immunosuppressants offer lower response rates and require more time, often 2 to 6 months for a clinical response. Due to multiple side effects (osteoporosis, weight gain, mood and behavioral changes, irritability, diabetes, infections, etc.), CS should be tapered to the lowest effective dose as soon as possible since CS must be maintained for at least 1 year. Alternative or additional options to CS are discussed under various circumstances: involvement of specific organs, contraindication for CS, a need for an unacceptably high dose (CS-dependency) and CS-resistant disease. Among the CSA, AZA, methotrexate (MTX), MMF and antimalarial drugs are considered as second-line agents while other immunosuppressive drugs are third-line therapies. The main anti-inflammatory drugs used in sarcoidosis are shown in Table 3.
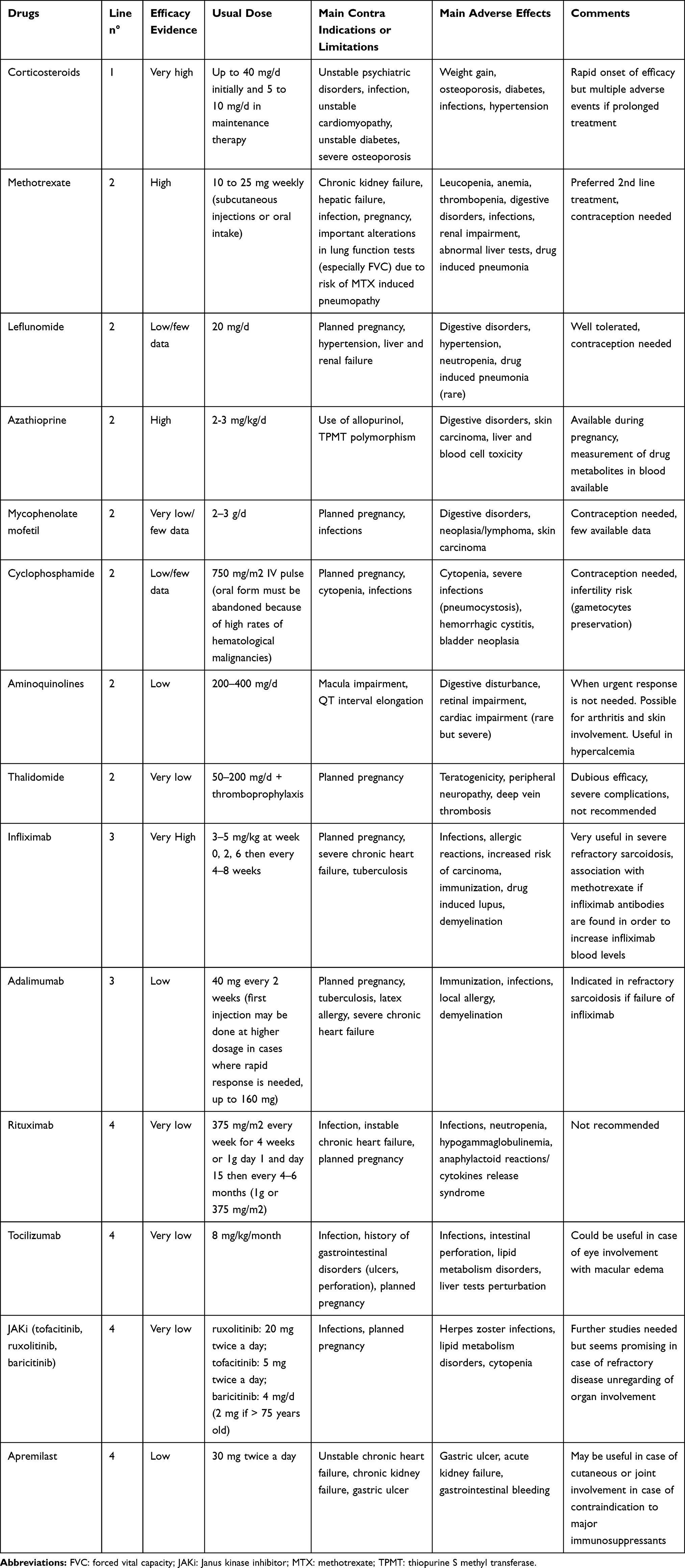 |
Table 3 Main Anti-Inflammatory Drugs in Sarcoidosis |
Efficacy of sarcoidosis treatments must be assessed with objective criteria. Such criteria vary according to the organ involved. In trials, improvement of forced vital capacity (FVC) is the most commonly used criterion to assess respiratory outcomes. A threshold of 10% is generally used to establish lung function improvement.47 For skin and eye improvement, clinical assessment is generally sufficient to judge treatment efficacy (visual acuity improvement, reduced skin lesions size, reduced steroid use, reduced flares).48,49 In cardiac sarcoidosis, left ventricular ejection fraction improvement and suppression or lowering of 18-fluorodeoxyglucose uptake in positron emission tomography help to assess treatment efficacy.50,51 In neurosarcoidosis trials, the ePOST or extrapulmonary physician organ severity tool is the most commonly used efficacy assessment tool52,53 even if clinical improvement, resolution of gadolinium uptake on magnetic resonance imaging, and improvement in cerebrospinal fluid inflammation are also used and may represent easier ways to ensure correct evaluation of treatment efficacy.54,55 In the case of renal sarcoidosis, improvement of serum creatinine levels, and the tapering of CS are the most commonly used criteria for assessing treatment efficacy.56
Corticosteroids
CS are indicated for most organ damage except Lofgren syndrome or asymptomatic lung involvement. Initial treatment for most cases is 20 to 40 mg a day of prednisone equivalent.57 After 4 weeks of treatment and obtention of a response, steroids must be tapered to 5–10 mg/d for 1–6 months representing the maintenance regimen. This maintenance regimen is continued 1–3 months then tapered off until treatment discontinuation.58,59 Judson et al proposed a 6-step scheme for managing of CS in sarcoidosis: 1) initial high dose to control inflammation, 2) maintenance dose to maintain inflammation control and lower toxic CS side effects, 3) continuing maintenance dosage until the decision taper off CS, 4) tapering off CS, 5) observation time to relapse, 6) initiate treatment again in case of relapse.58 Higher dosages (1 mg/kg/d equivalent prednisone) may be required in cases of CNS involvement due to more frequent relapses at lower CS doses.59
In life-threatening situations like severe CNS and heart involvement, or optic neuritis, the use of methylprednisolone pulses are usually weighed but no evidence in the literature supports this effect.60 A current trend is to start an early treatment with a CSA in order to avoid the occurrence of CS side effects, particularly when the threshold dose for keeping the disease inactive is over 7–10 mg/d of prednisone.57
Other types of CS administrations were studied in the context of localized sarcoidosis. Local CS may be useful for limited cutaneous involvement as well as anterior uveitis.61 Subconjunctival injections of dexamethasone, triamcinolone acetate, or betamethasone may be used in case of persistence of uveitis despite topical CS therapy.62 Posterior sub-tenon and peribulbar injections of triamcinolone acetate permit direct administration of steroids. Alternatively, intravitreal injections of steroids can be suggested to treat unilateral macular edema or when it resists systemic therapy and periocular injections.63 Inhaled CS are not effective on lung disease but may help in reducing or stopping cough when there is no indication for a general treatment.43
Second-Line Treatment (i.e., CS-Sparing Agents)
Corticoresistance in sarcoidosis is unusual (except for neurosarcoidosis). CS-dependency is more common and a Delphi consensus study concluded that a maintenance dose regimen of over 10 mg of prednisone equivalent a day is unacceptable.57 If the clinician fears CS side effects or if the maintenance dose of CS is unacceptable, CSA must be discussed.
Methotrexate
Among CSA options, MTX is the only one to have been assessed in a randomized controlled trial.64 This randomized controlled trial is the only one concerning the use of MTX in the case of pulmonary sarcoidosis. MTX remains the preferred second-line CSA in sarcoidosis.65 In 1995, Lower et al showed a benefit with MTX therapy both in symptomatic pulmonary and extra-pulmonary sarcoidosis: 66% of the treated patients (33/50) experienced disease improvement. In 17 remaining patients, total elimination of CS was possible, and among them, 6 individuals had no relapse.66 However, particular attention should be paid to the risk of hepatotoxicity, especially in patients with initially abnormal liver tests. The most frequently used weekly dose is 10–15 mg (or 0.3 mg/kg/week).6 In the case of oral administration failure or intolerance in rheumatoid arthritis patients, a switch to subcutaneous administration may lead to better tolerance and efficacy outcomes, especially in extreme-range body mass index patients.67 Of note, concomitant folic acid administration may prevent gastrointestinal and hepatic side effects.68
Antimalarial Drugs
Hydroxychloroquine and chloroquine (CQ) may be useful in non-life-threatening organ involvement (symptomatic persistent pulmonary sarcoidosis69 such as mild hypercalcemia,56 moderate cutaneous sarcoidosis,70 and mild cranial neuropathies71)
Sarcoidosis-related joint involvement may also improve under treatment.72 The advantage of antimalarial drug use is based on its excellent safety profile (especially for HCQ). Nevertheless, some rare but severe complications may occur such as anti-malarial myopathy or cardiomyopathy and antimalarial maculopathy.73 Among the two available anti-malarial drugs, HCQ is the one with the lowest retinal toxicity.74
Azathioprine
AZA is a prodrug converted in vivo into its active metabolite, 6-mercaptopurine. Its immunosuppressive effects are linked to cytotoxicity against T lymphocytes.75 There is currently no prospective clinical trial on the effectiveness of AZA in the case of sarcoidosis. In a large nonrandomized retrospective comparative study evaluating AZA and MTX in thoracic sarcoidosis, a similar corticosteroid-sparing benefit was observed with a similar gain in vital capacity, 1 second forced expiratory volume, and carbon monoxide diffusing capacity (DLCO).76 Adverse events may also be very similar except for infections which might be more frequent with AZA.76 In cases of refractory sarcoidosis treated with AZA, dosage of metabolite blood level dosages can be performed in order to rule out lack of adherence. However, no data regarding target ranges of blood metabolites are available in the literature for sarcoidosis.
Leflunomide
Leflunomide is an immunomodulating agent active via its metabolite (A771726) for selective dihydroorotate dehydrogenase inhibition. Only a limited number of patients with sarcoidosis have been investigated in two open studies and reported cases.77–79 In a retrospective study, potential beneficial effects on skin, eyes, and lung sarcoidosis were observed when given at 20 mg/day, but with a mild response as to lung involvement.79 Leflunomide has been shown to be effective in refractory sarcoid uveitis, either alone or in combination with MTX.78
Mycophenolate Mofetil
MMF is a prodrug of mycophenolic acid, an inhibitor of inosine monophosphate dehydrogenase (IMDH). Scant data regarding the efficacy of MMF in sarcoidosis are available in the medical literature. Reported experiences mainly concern extrapulmonary sarcoidosis (e.g., neurologic, cutaneous, and ophthalmologic involvement).80,81 Data obtained in neurologic sarcoidosis with CNS involvement do not suggest any advantage of MMF over MTX.52 Benefits of MMF therapy rely on rapid onset of action and limited toxicity in hematological and infectious complications.6 The usual dose range varies from 2 to 3 g a day in maintenance therapy (Table 3).
Third-Line Treatments
If disease activity is not controlled through CS at an acceptable dose and CSA, a third-line treatment should be considered.
Cyclophosphamide
Cyclophosphamide (CYC) has been successfully used for both refractory or severe cardiac50,82 and CNS sarcoidosis83 in retrospective series. However, treatment modalities and indications remain non-specific since data on these extrapulmonary manifestations are limited. CYC is usually administered intravenously as pulses varying from 500 to 1200 mg every 3 to 4 weeks.6 For oncogenic, hematologic, urologic, and infectious cumulative side effects, which seem to be more frequent in sarcoidosis,84 CYC should be reserved for severe and refractory sarcoidosis when no other acceptable therapeutic alternative is available, including TNFi.
TNF-α Inhibitors
Because some patients may be refractory to conventional immunosuppressants or develop side effects, biological agents which target TNF-α have been proposed as a third-line option.85 Whereas one randomized clinical trial on ETN reported no improvement in refractory ocular sarcoidosis,86 several studies on infliximab (IFX) showed efficacy in refractory sarcoidosis.17,85,87 In a randomized trial on IFX in pulmonary sarcoidosis, Baughman et al reported a modest but significant improvement of pulmonary vital capacity at 24 weeks.88 Nevertheless, the pulmonary function test improvement canceled out during the subsequent 24-week washout. Furthermore, in the post-hoc analysis of this trial, IFX was also effective in extrapulmonary sarcoidosis.88 Judson et al observed the same results in a trial dedicated to extrapulmonary sarcoidosis assessing its activity via the ePOST scoring system, a scoring system assessing 17 organs and the severity of their involvement on a scale from 0 (not affected) to 6 (severely affected).87 In another controlled trial, among chronic active pulmonary sarcoidosis patients, Rossman et al found no significant difference between the IFX group and the placebo group although the study was underpowered and failed to reach its target number of enrolled patients.89 The improvement in FVC in the IFX group of this study was higher than in any other study on IFX.
The STAT study, reporting on 132 sarcoidosis patients treated with TNFi (IFX in 91% of cases) in a large French nationwide multicentric retrospective study, found that TNF antagonists were efficient in about two-thirds of the patients and permitted a substantial reduction in prednisone dosages (from 23 to 11 mg/day).17
The efficacy of adalimumab (ADA) has been reported in a randomized controlled clinical trial of 16 patients with skin sarcoidosis (ADA, n=10 vs placebo, n=6)90 and in a prospective case series of 26 patients with refractory sarcoid uveitis,91 and other disabling sarcoidosis-related symptoms such as dyspnea.
Finally, in a recent systematic review of the efficacy and safety of TNFi in sarcoidosis from inception to November 2017, Adler et al looked at non-randomized studies of cutaneous, ocular, neurologic, and multisystemic sarcoidosis and reported an improvement in 89%, 69%, 77%, and 71% of cases, respectively.92
Schimmelpennink et al recently reported in a retrospective study of 29 patients that the IFX biosimilar (i.e., Inflectra®) appears to be effective in the treatment of refractory sarcoidosis with a profile comparable to the reference.93
In contrast to randomized controlled trials versus placebo, in retrospective and open-labeled studies TNFi had more overall and serious adverse events and more severe infections. These adverse events seemed to be more frequent during sarcoidosis treatment than during other inflammatory diseases.17,94,95
The use of high-dose TNFi has been reported to adversely affect the clinical condition of patients with moderate-to-severe chronic heart failure.96 In a multicentric retrospective series of 20 patients with definite cardiac sarcoidosis refractory to CS plus immunosuppressive therapy, TNFi showed a complete/partial response in 75% of patients, with a significant CS-sparing effect.97 Harper et al described another retrospective series of 36 patients with cardiac sarcoidosis refractory to conventional CS therapy. Twenty-four patients out of 36 (67%) were categorized as responders, meaning they had at least an improvement on CS dose, ejection fraction, or dysrhythmia burden. Steroids dose, dysrhythmia control, and ejection fraction were improved, respectively, in 20, 12, and 8 patients among responders.98
Overall, current data suggest the efficacy of IFX in pulmonary, cutaneous, ocular, and multisystemic sarcoidosis and of ADA in cutaneous and ocular sarcoidosis. To date, no available data support the use of other TNFi, such as golimumab 99 in sarcoidosis.
The recommended IFX dosage is usually 5 mg/kg intravenously but 3 mg/kg may be enough to treat lung involvement.17 The induction protocol often includes intravenous administration at weeks 0, 2, and 6. Then, a four-week maintenance interval may be recommended in sarcoidosis in view of establishing better responses and fewer flares. For ADA, a weekly administration using low doses is preferred, with a loading dosage of 80 to 120 mg at week 0, and at least 40 mg at weeks 1 and 2. Then, maintenance therapy is based on 40 mg every other week.
Some studies evidenced frequent relapses when treatment lasted only 4 to 8 months.100,101 Thus, before considering withdrawal, the duration of TNFi treatment should be 6 to 12 months after obtention of the clinical response. Before discontinuing IFX or ADA, the treatment should be gradually spaced apart.102 In 2014, Vorselaars et al showed that patients who experienced high levels of soluble IL-2 receptor (≥4000 pg/mL) and high mediastinal standardized uptake value (SUV) (-≥6.0) on initial FDG-PET-CT before initiation of IFX therapy had a higher risk of disease relapse after IFX discontinuation.101
Primary and secondary non-responders to TNFi should be distinguished. Primary TNFi failure may necessitate a change in therapeutic class. Secondary failure occurring in the course of TNFi therapy should raise an alert about patient treatment adherence or immunization against TNFi.103 Recommendations incite the clinician to prescribe a TNFi in combination with another anti-inflammatory drug (either MTX, AZA, or CS).102
As shown in patients with rheumatoid arthritis (RA) and inflammatory bowel diseases, serum assays with bio drug titers and TNFi antibodies can be performed before concluding to failure in patients receiving TNFi.104 The use of low-dose MTX might increase TNFi efficacy with re-increased IFX or ADA serum levels linked to antidrug antibody elimination. Moreover, one TNFi can be changed to another in cases of lack of response and immunization, if TNFi blood levels are in the normal range105 In non-immunized patients with low drug concentrations, reducing the intervals between two injections should be considered.102
Fourth-Line Agents
We proposed defining refractory sarcoidosis here as a situation in which CS and second-line treatment are not sufficient to achieve clinical remission with a CS dosage under 10 mg/day. Among the 132 patients from the Sarcoidosis Treated with Anti TNF (STAT) registry, we recently reported on nine who were considered to be TNFi non-responders.106 Among them, seven experienced a clinical response (complete or partial) with additional immunosuppressive therapy which had previously been used in all but one case. The disease only progressed in 2 patients CS treated with no adjunctive immunosuppressants.
Recently, new therapeutic approaches have been proposed in refractory sarcoidosis with targeted synthetic drugs, such as JAK inhibitors, or biologics, such as rituximab (RTX) and tocilizumab (TCZ), and additional trials are currently underway (Table 4). Other immunosuppressive agents targeting the NFκb pathway have been assessed in sarcoid patients including ciclosporin and mammalian target of rapamycin (mTOR) inhibitors.
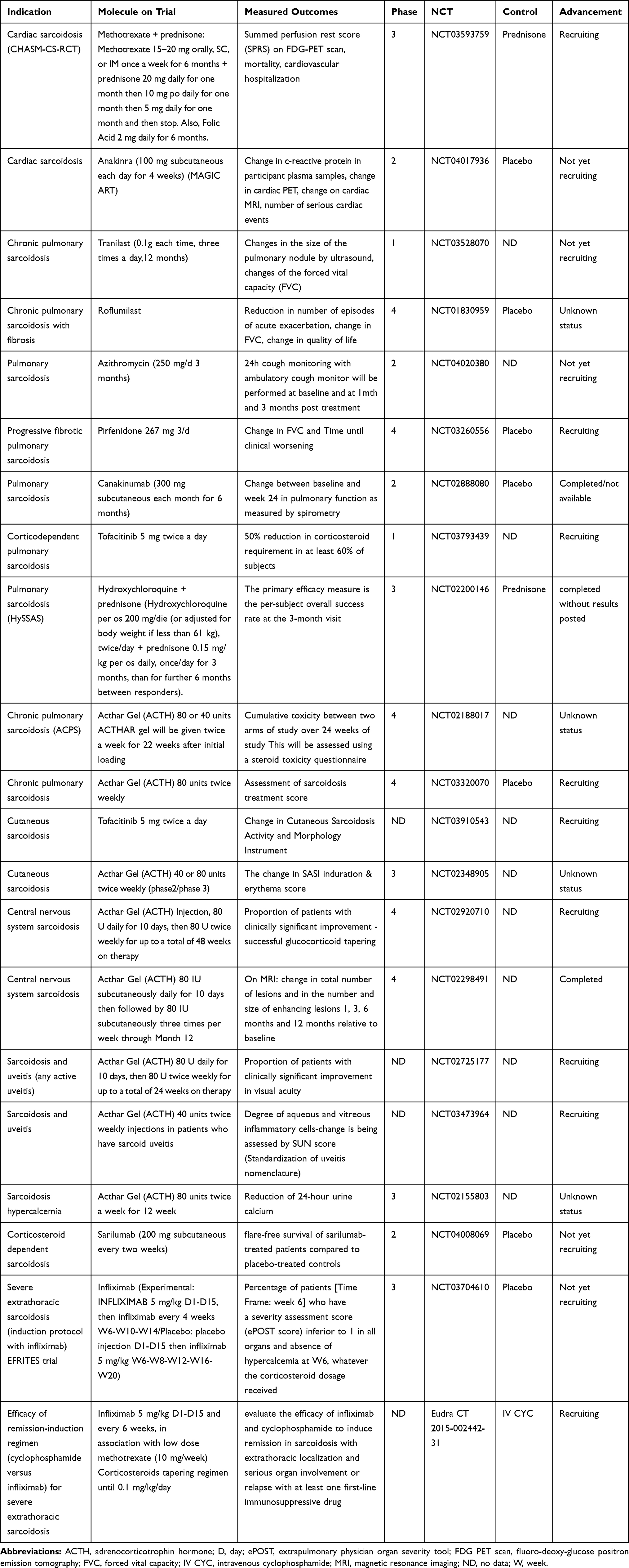 |
Table 4 Ongoing Trials for Sarcoidosis |
 | 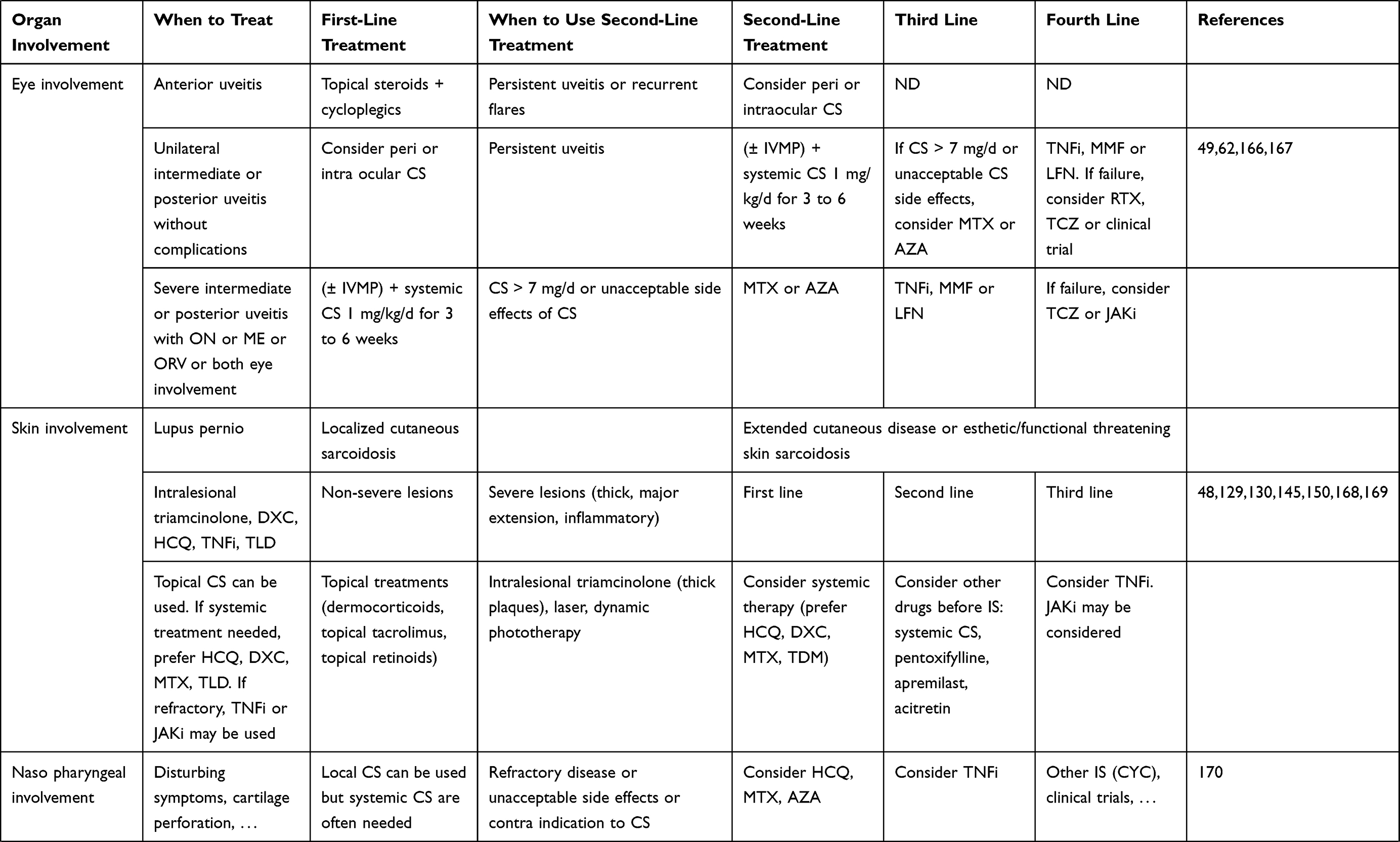 | 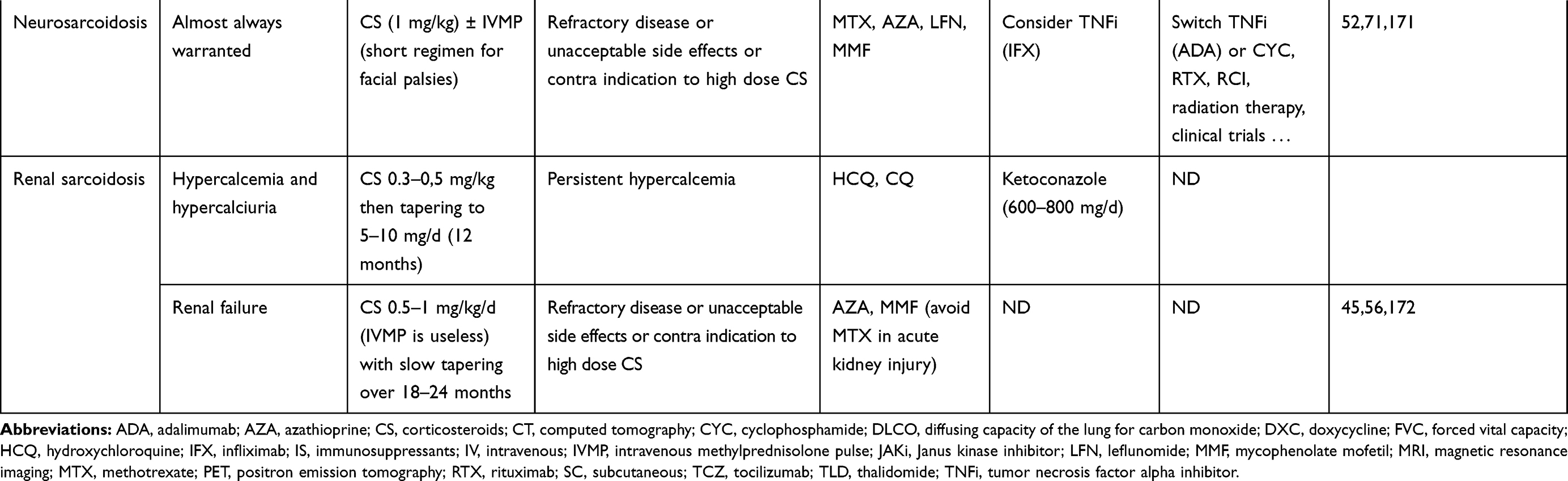 |
Table 5 Therapeutic Management of Sarcoidosis Depending on Organ Involvement |
Rituximab
B-cells were suspected of participating in the pathophysiology of sarcoidosis since hypergammaglobulinemia and B cell accumulation in granuloma are frequently observed. In 2012, Saussine et al found that patients with an active chronic form of sarcoidosis had significantly fewer circulating memory B cells, more transitional B cells, and increased number of IL-10 producing B-cells. Thus, B-cell targeting therapies could theoretically be efficient in sarcoidosis.107 RTX is a monoclonal chimeric antibody targeting CD20, which is preferentially expressed on B cells.
In 2014, Sweiss et al conducted a Phase I/II open-label clinical trial to assess the safety and tolerance of RTX in 10 patients with pulmonary sarcoidosis.19 Unfortunately, the efficacy of RTX was inconstant on objective criteria regarding pulmonary involvement. About half the patient improved their forced vital capacity while only 3 patients out of 10 improved their 6-minute walk test. The two major adverse events which occurred during the study were deaths linked to sarcoidosis progression.
Apart from this study, medical literature evidence on the use of RTX in sarcoidosis concerns case reports establishing response for some patients with refractory pulmonary, CNS, eye, or heart manifestations.108,109–114 Severe infections may represent a limit to the use of rituximab although no large series are available on sarcoidosis, so this risk is presupposed on the basis of rheumatoid arthritis trials.115
Tocilizumab
As previously described, sarcoidosis is a granulomatous disease with a Th1, Th17 and Th17.1 cytokine signature associated with high levels of interleukin-6 (IL-6) in active sarcoidosis.15,116
Few cases in the medical literature report the use of antiIL-6 or IL-6R agents in sarcoidosis. In 2012, Awano et al reported a case of Castleman’s disease occurring in the case of chronic sarcoidosis which dramatically improved upon TCZ, a recombinant, humanized, anti-human IL-6 receptor monoclonal antibody.117 In 2017, Semiz et al described an association of adult-onset Still’s disease and sarcoidosis and both diseases dramatically improved under TCZ.118
Recently, Sharp et al reported four patients with multidrug-resistant sarcoidosis treated with TCZ (one case of pulmonary sarcoidosis, one of cutaneous sarcoidosis, one of sarcoidosis with arthritis and fatigue, and one of upper respiratory tract involvement).119 Three patients were treated with TCZ infusion and one patient was treated with subcutaneous TCZ. One patient developed breast cancer under TCZ.
In ocular involvement, TCZ may be helpful in patient with uveitis refractory to TNFi. In 2016, Silpa-Archa et al reported improvement of inflammatory ocular disease in a case series of 17 patients.120 Among the 17 patients, one had ocular multidrug-resistant sarcoidosis, which improved under TCZ therapy with no major side effects. TCZ is also known to be effective in refractory inflammatory cystoid macular edema (CME) no matter its etiology.121
Currently, few data support the use of TCZ in sarcoidosis. Preliminary data indicate that anti-IL-6 therapy could be an interesting therapeutic approach to treat multidrug-resistant sarcoidosis, but further studies must be carried out.
Paradoxically, new-onset sarcoidosis during TCZ treatment has been described in four case-reports.122–125 In three cases, there was what was presumed to be TCZ-induced sarcoidosis, observed during treatment for RA, at least 1 year after the start of the treatment. Del Giorno et al recently reported TCZ-induced sarcoidosis in a 74-year-old woman treated for giant cell arteritis, which occurred 8 months after TCZ initiation. In all these cases, there was skin involvement, associated with bilateral hilar lymphadenopathy in 3 patients.124 No clinical trial is underway to evaluate TCZ in this indication.
JAK Inhibitors
There are currently three JAK inhibitors approved by the FDA (Food and Drug Administration) and EMA (European Medicines Agency): ruxolitinib for the treatment of myeloproliferative disorders, tofacitinib in RA, psoriasis and ulcerative colitis, and baricitinib which is indicated for the treatment of RA.
Sarcoidosis pathophysiology involves several cytokines, such as IL12/23, IL-17, IL-6, and IFNγ, which signal through the JAK-STAT pathway. In a transcriptomic analysis, Rosenbaum et al showed that the STAT1 pathway is activated in granulomatous diseases.126
On Medline, 6 case reports are available.127–131 Among those patients, two were treated for concomitant polycythemia vera. Those 2 patients experienced improvement of lung involvement under ruxolitinib. Levraut et al recently reported a case of sarcoid-like systemic granulomatosis refractory to MTX, TNFi, anakinra, antimalarial drugs, AZA, MMF, and CYC that improved under ruxolitinib.127 Damsky et al reported a case of refractory cutaneous sarcoidosis previously unsuccessfully treated with topical steroids, hydroxychloroquine, MTX, tacrolimus, ADA, and apremilast.128 Once switched to tofacitinib, the patient improved her CSAMI score (Cutaneous Sarcoidosis Activity and Morphology Instrument). For skin biopsy samples, phosphoSTAT1 (Signal Transducer and Activators of Transcription) and phosphoSTAT3 immunostaining was done. During tofacitinib treatment, the entire phosphoSTAT1 and -3 staining vanished. During the treatment, downregulation of the mRNA of the JAK/STAT pathway (such as IL-6 and IFN-γ) was shown on skin samples, during the treatment.128
There are currently two trials recruiting for evaluating tofacitinib in sarcoidosis. NCT03793439 is a Phase 1 trial, which will evaluate the CS-sparing effect of tofacitinib in pulmonary sarcoidosis. NCT03910543 is an open-label trial assessing the efficacy of tofacitinib in granuloma annulare and cutaneous sarcoidosis.
Safety data are reassuring since severe adverse events with JAK inhibitors are rarely reported.132 An increased incidence of herpes zoster infection was noticed in RA trials.133 The FDA recently alerted on the increased risk of thromboembolic events under tofacitinib at higher dosages. Given the good safety profile of JAK inhibitors, they could represent an interesting alternative for refractory sarcoidosis in case of TNFi failure or contraindication. Further studies and randomized clinical trials are still needed to confirm this.
Ciclosporin A
Ciclosporin A (CisA) is an immunosuppressive agent targeting calcineurin, first used in organ transplants. Few data are available concerning the use of CisA in sarcoidosis. One randomized clinical trial was conducted in 1997 by Wyser et al to assess the efficacy of CisA in pulmonary sarcoidosis.134 Unfortunately, there were significantly more serious adverse events in the CisA group versus placebo (especially serum creatinine elevation). No statistically significant improvement was noted in the CisA group versus placebo. Bogabathina et al reported on a case of severe and refractory cardiac involvement that improved after CisA administration.135 Regarding T-cell involvement and potential efficacy of mTOR inhibition, CisA may theoretically be useful in sarcoidosis, although too little data are currently available to support its use.
mTOR Inhibitors
Some data are available on mTOR activity in sarcoidosis. Recently, Calender et al showed that mTOR signaling and autophagy signaling are overexpressed in sarcoidosis.16 This was consistent with previously published data in mice.136
In 2011, Manzia et al described a case of a liver transplant recipient with sarcoid-like granulomatosis which improved on introduction of rapamycin137 after CisA failure.
SAVE 1 and -2 studies were, respectively, phases I and II clinical trials assessing the safety and efficacy of intravitreal or subconjunctival sirolimus, administered either at 440 µg monthly or 880 µg every 2 months in patients with non-infectious uveitis. In those studies, the proportion of ocular sarcoidosis represented, respectively, 27% and 1% of the population.138 This treatment was well tolerated in both clinical trials. In SAVE 2, the 440-µg dosage seemed to be more efficient than 880-µg dosage. Both dosages were able to achieve vitreal haze resolution.139 The SAKURA study was a Phase III clinical trial reporting on the efficacy of intravitreal sirolimus for non-infectious uveitis. Twenty-nine patients out of 347 (8.4%) were treated for ocular sarcoidosis.140 Unfortunately, there are no available data for the sarcoidosis subgroup.
Further investigations must be carried out before recommending mTOR inhibition in sarcoidosis even though available data are encouraging.
IL-1 Blockade Therapy
No case reports are available concerning the use of IL-1 blockade therapy. On the contrary, cases of sarcoid-like side reactions are reported. Despite that, a Phase 2 clinical trial is ongoing to assess safety and efficacy of anakinra in adult cardiac sarcoidosis (ARAMIS trial NCT03018834). The MAGiC-ART trial (NCT04017936) is also an ongoing phase 2 study evaluating the IL-1 blockade in treating cardiac sarcoidosis.
Thalidomide
Thalidomide is an immunomodulating agent that is known to reduce IFNγ secretion and enhances IL-4 and IL-5 production, thus optimizing a Th1 to Th2 switch. This drug is usually prescribed for cutaneous sarcoidosis. In 2014, Droitcourt et al showed in a randomized controlled trial (RCT) that thalidomide was not superior to placebo in treating cutaneous sarcoidosis, to the contrary of a previous trial published in 2012.141,142 Some authors reported improved cutaneous and mucosal involvement under thalidomide.143 Available data are still not sufficient to recommend using thalidomide in treating sarcoidosis even though case reports may be encouraging. New molecules similar to thalidomide, such as lenalidomide, may represent a well-tolerated alternative to thalidomide.144
Apremilast
Apremilast is a specific phosphodiesterase 4 (PDE4) inhibitor. This specificity allows higher dosages with fewer side effects than pentoxifylline, a non-specific PDE4 inhibitor (cf infra). In 2012, Baughman et al described the efficacy of apremilast in treating chronic cutaneous sarcoidosis.145 Among the 15 patients treated with apremilast at 20 mg twice daily, 14 patients had improved induration scores after 4 and 12 weeks. Three months after apremilast discontinuation, 3 patients underwent a cutaneous relapse: the increase in CS dosage only moderately improved cutaneous induration.
Except for this publication, there are no case reports available today for recommending its use in sarcoidosis even if its safety profile may be of interest.
Ustekinumab
Ustekinumab is a human monoclonal antibody targeting the IL-12/23 pair. In a randomized double-blinded and controlled versus placebo trial in 2014, Judson et al showed that ustekinumab was neither associated with improved respiratory function tests nor improved organ involvement in the 60 patients studied.99
Abatacept
Abatacept is a fusion protein of CTLA4 (cytotoxic T-lymphocyte-associated protein 4) and immunoglobulin known as CTLA4-Ig. The mechanism of action is based on the downregulation of T lymphocyte-induced immune response by CTLA4.
Currently, there are no studies or case reports on abatacept use in sarcoidosis. A clinical trial (NCT00739960) was conducted to assess abatacept efficacy versus placebo but its results have not been published since its completion date.
Other Treatments and Adjunctive Therapies
Repository Corticotropin Injections
Except for CS, repository corticotropin injections (RCI; or ACTHAR® gel) are the only treatment approved by the US FDA for “sarcoidosis” indication whereas this therapeutic option is not used in Europe. RCI seems to represent a good alternative to CS in case of CS-resistant disease or CS side effects,146 but until recently, there were only a few retrospective studies supporting its use in sarcoidosis. Very recently Chopra et al published a large retrospective case series of 302 patients treated with RCI.147 A total of 288 (95%) patients improved their status at 3 months according to physicians' evaluations. A total of 116 (38%) improved lung function and reduction or discontinuation of CS was possible in 32% of the patients. At present, there is no completed prospective studies confirming its use in sarcoidosis even though such trials are underway (Table 4).
Pentoxifylline
Pentoxifylline is a non-specific phosphodiesterase 4 inhibitor used to reduce pro-inflammatory cytokine secretion, such as TNF-α. In 1997, Zabel et al treated 23 patients with pentoxifylline.148 Among them, 11 patients improved their lung function test. Three patients with CS-resistant disease were able to decrease their daily prednisone intake. In 2009, Park et al showed that adverse events of pentoxifylline at doses used to correctly treat thoracic sarcoidosis may limit its benefits.149 Pentoxifylline may possibly be useful in sarcoidosis-induced fatigue.
Antimycobacterial Therapy
In 2013, Drake et al showed in a phase 1 single masked study that oral concomitant antimycobacterial therapy (AMBT) with levofloxacin, ethambutol, azithromycin, and rifampicin in a population of 30 patients with chronic cutaneous sarcoidosis lesions resulted in a mean decrease in lesion diameter of −8.4 mm compared to an increase of 0.07 mm in the placebo group (p= 0.05) thereby suggesting objective efficacy for AMBT in chronic cutaneous sarcoidosis.150 In 2014, the same authors conducted a phase Ib clinical trial assessing the efficacy of specific AMBT in pulmonary sarcoidosis.151 Through it, AMBT was associated with significant improvement of FVC and an increase for the 6-minute walk test. These data, beyond the interesting pathophysiological considerations they highlight, need to be confirmed in larger trials.
Antifibrotic Agents
Pirfenidone and nintedanib are the two available and approved drugs for treating idiopathic pulmonary fibrosis when lung transplantation is contraindicated. There is no data in available medical literature recommending those drugs in fibrotic sarcoidosis. However, similar aspects of fibrotic process pathophysiology may indicate that pirfenidone and nintedanib could be used in fibrotic sarcoidosis152 as it was recently the case for systemic sclerosis.153 However, a recent RCT (INBUILD) that has evaluated the efficacy of nintedanib on various interstitial lung diseases-associated pulmonary fibrosis (including sarcoidosis) has demonstrated benefits on FVC decline.154 Of note, a clinical trial assessing the efficacy of pirfenidone in progressive fibrotic sarcoidosis is currently underway (NCT03260556).
Adjunctive Therapies
In addition to symptomatic treatment (e.g., antiepileptics, antiarrhythmics, prostacyclin for pulmonary hypertension, ursodeoxycholic acid for hepatic sarcoidosis, etc.), adjunctive therapy can be used in refractory sarcoidosis for specific localizations. Cardiac transplantation should be considered for patients with severe intractable heart failure refractory to medical therapy.82 In neurosarcoidosis, there have been rare reports of radiation therapy for CNS sarcoidosis but always in the context of other treatment failures.155
Beyond objective clinical symptoms, fatigue and parasarcoidosis syndrome can represent a therapeutic challenge. Nasopharyngeal obstruction and thus sleep apnea may increase fatigue. In most cases, anti-inflammatory drugs are ineffective. Other molecules (dexmethyl-, methylphenidate, armodafinil) can be useful.156 Small fiber neuropathy (SFN) may be a major concern for the patients and the clinicians in terms of pain management and quality of life. Several case series reported the efficacy of intravenous immunoglobulins (IVIg) in SFN.157,158 IVIg were also reported to be effective in other manifestations such as sarcoid myopathy159 or neuropathy.160
Conclusion
Refractory sarcoidosis and multidrug-resistant sarcoidosis are challenging conditions with no clear guidelines available. Even if no clear definition of refractory sarcoidosis can be found in medical literature, we chose to define it as a disease which does not respond to CS and conventional immunosuppressants. We considered this definition to fit the best with a situation many clinicians are facing. Checking for a differential diagnosis, assessing adherence, and testing for anti-drug antibodies should be done systematically before classifying patients as non-responders. At present, TNFi are the most commonly used immunosuppressants in severe or refractory sarcoidosis. Multidrug-refractory sarcoidosis should be referred to a clinician accustomed to refractory sarcoidosis management. In this context, switching from a TNFi to another or re-treating with a previously used immunosuppressant can sometimes be useful. New therapeutic approaches are on the horizon. Among them, JAK inhibitors appear promising although few clinical trials are currently carried out on this therapeutic approach to sarcoidosis. New tools to predict response and adverse events are required so as to optimize the risk/benefit ratio in a more personalized type of medicine.
Disclosure
Dr Yvan Jamilloux reports personal fees from Sobi, outside the submitted work. Professor Pascal Sève reports personal fees from Abbvie, Chugai, Pfizer, and Sobi, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Besnier EH. Lupus pernio de la face; synovites fongueuses (scrofulo-tuberculeuses) symétriques des extrémités supérieures. Ann Dermatol Syphil. 1889;333–336.
2. Sakthivel P, Bruder D. Mechanism of granuloma formation in sarcoidosis. Curr Opin Hematol. 2017;24(1):59–65. doi:10.1097/MOH.0000000000000301
3. Hunninghake G, Costabel U. Statement on sarcoidosis. Am J Respir Crit Care Med. 1999;160:20. doi:10.1034/j.1399-3003.1999.14d02.x
4. Arkema EV, Cozier YC. Epidemiology of sarcoidosis: current findings and future directions. Ther Adv Chronic Dis. 2018;9(11):227–240. doi:10.1177/2040622318790197
5. Pereira CAC, Dornfeld MC, Baughman R, Judson MA. Clinical phenotypes in sarcoidosis. Curr Opin Pulm Med. 2014;20(5):496–502. doi:10.1097/MCP.0000000000000077
6. Valeyre D, Prasse A, Nunes H, Uzunhan Y, Brillet P-Y, Müller-Quernheim J. Sarcoidosis. The Lancet. 2014;383(9923):1155–1167. doi:10.1016/S0140-6736(13)60680-7
7. Nunes H, Bouvry D, Soler P, Valeyre D. Sarcoidosis. Orphanet J Rare Dis. 2007;2(1):46. doi:10.1186/1750-1172-2-46
8. Crouser ED. Lessons learned from the ABCs of granuloma formation. Am J Respir Cell Mol Biol. 2019;61(3):277–278. doi:10.1165/rcmb.2019-0076ED
9. Goto H, Usui Y, Umazume A, Uchida K, Eishi Y. Propionibacterium acnes as a possible pathogen of granuloma in patients with ocular sarcoidosis. Br J Ophthalmol. 2017;101(11):1510–1513. doi:10.1136/bjophthalmol-2016-309248
10. Pacheco Y, Ponchon M, Lebecque S, et al. Granulomatous lung inflammation is nanoparticle type dependent. Exp Lung Res. 2018;44(1):25–39. doi:10.1080/01902148.2017.1412541
11. Mortaz E, Adcock IM, Abedini A, et al. The role of pattern recognition receptors in lung sarcoidosis. Eur J Pharmacol. 2017;808:44–48. doi:10.1016/j.ejphar.2017.01.020
12. Rivera A, Siracusa MC, Yap GS, Gause WC. Innate cell communication kick-starts pathogen-specific immunity. Nat Immunol. 2016;17(4):356–363. doi:10.1038/ni.3375
13. Zissel G, Müller-Quernheim J. Cellular players in the immunopathogenesis of sarcoidosis. Clin Chest Med. 2015;36(4):549–560. doi:10.1016/j.ccm.2015.08.016
14. Roach DR, Bean AGD, Demangel C, France MP, Briscoe H, Britton WJ. TNF regulates chemokine induction essential for cell recruitment, granuloma formation, and clearance of mycobacterial infection. J Immunol. 2002;168(9):4620–4627. doi:10.4049/jimmunol.168.9.4620
15. Ramstein J, Broos CE, Simpson LJ, et al. IFN-γ–producing T-helper 17.1 cells are increased in sarcoidosis and are more prevalent than T-helper type 1 cells. Am J Respir Crit Care Med. 2016;193(11):1281–1291. doi:10.1164/rccm.201507-1499OC
16. Calender A, Lim CX, Weichhart T, et al. Exome sequencing and pathogenicity-network analysis of 5 French families implicate mTOR signalling and autophagy in familial sarcoidosis. Eur Respir J. 2019;54:2. doi:10.1183/13993003.00430-2019
17. Jamilloux Y, Cohen-Aubart F, Chapelon-Abric C, et al. Efficacy and safety of tumor necrosis factor antagonists in refractory sarcoidosis: A multicenter study of 132 patients. Semin Arthritis Rheum. 2017;47(2):288–294. doi:10.1016/j.semarthrit.2017.03.005
18. Korsten P, Strohmayer K, Baughman RP, Sweiss NJ. Refractory pulmonary sarcoidosis: proposal of a definition and recommendations for the diagnostic and therapeutic approach. Clin Pulm Med. 2016;23(2):67–75. doi:10.1097/CPM.0000000000000136
19. Sweiss NJ, Lower EE, Mirsaeidi M, et al. Rituximab in the treatment of refractory pulmonary sarcoidosis. Eur Respir J. 2014;43(5):1525–1528. doi:10.1183/09031936.00224513
20. Judson MA, Costabel U, Drent M, et al. The WASOG sarcoidosis organ assessment instrument: an update of a previous clinical tool. Sarcoidosis Vasc Diffuse Lung Dis. 31:19–27.
21. Bickett AN, Lower EE, Baughman RP. Sarcoidosis diagnostic score. Chest. 2018;154(5):1052–1060. doi:10.1016/j.chest.2018.05.003
22. Criado E, Sánchez M, Ramírez J, et al. Pulmonary sarcoidosis: typical and atypical manifestations at high-resolution CT with pathologic correlation. RadioGraphics. 2010;30(6):1567–1586. doi:10.1148/rg.306105512
23. Park HJ, Jung JI, Chung MH, et al. Typical and atypical manifestations of intrathoracic sarcoidosis. Korean J Radiol. 2009;10(6):623. doi:10.3348/kjr.2009.10.6.623
24. Spagnolo P, Luppi F, Roversi P, Cerri S, Fabbri LM, Richeldi L. Sarcoidosis: challenging diagnostic aspects of an old disease. Am J Med. 2012;125(2):118–125. doi:10.1016/j.amjmed.2011.06.003
25. Chalayer É, Bachy E, Occelli P, et al. Sarcoidosis and lymphoma: a comparative study. QJM. 2015;108(11):871–878. doi:10.1093/qjmed/hcv039
26. Gousseff M, Mechaï F, Lecuit M, Lortholary O. Les granulomatoses systémiques d’origine infectieuse. La Revue De Médecine Interne. 2008;29(1):15–27. doi:10.1016/j.revmed.2007.09.037
27. Piotrowski WJ, Żądło LJ, Górski W, et al. QuantiFERON-TB-GOLD In-Tube in patients with sarcoidosis. Advan Respir Med. 2018;86(5):234–239. doi:10.5603/ARM.2018.0037
28. O’Sullivan CE, Miller DR, Schneider PS, Roberts GD. Evaluation of gen-probe amplified mycobacterium tuberculosis direct test by using respiratory and nonrespiratory specimens in a tertiary care center laboratory. J Clin Microbiol. 2002;40(5):1723–1727. doi:10.1128/JCM.40.5.1723-1727.2002
29. Dhooria S, Gupta N, Bal A. Role of Xpert MTB/RIF in differentiating tuberculosis from sarcoidosis in patients with mediastinal lymphadenopathy undergoing EBUS-TBNA: a study of 147 patients. Sarcoidosis Vasc Diffuse Lung Dis. 2016;33(3):258–266.
30. James DG, Lipman MCI. Whipple’s disease: a granulomatous masquerader. Clin Chest Med. 2002;23(2):513–519. doi:10.1016/S0272-5231(02)00005-9
31. Ohshimo S, Guzman J, Costabel U, Bonella F. Differential diagnosis of granulomatous lung disease: clues and pitfalls: number 4 in the Series “Pathology for the clinician” Edited by Peter Dorfmüller and Alberto Cavazza. Eur Respir Rev. 2017;26(145):170012. doi:10.1183/16000617.0012-2017
32. Ramos-Casals M, Mañá J, Nardi N, et al. Sarcoidosis in patients with chronic hepatitis C virus infection: analysis of 68 cases. Medicine. 2005;84(2):69–80. doi:10.1097/01.md.0000157577.69729.e6
33. Chopra A, Nautiyal A, Kalkanis A, Judson MA. Drug-induced sarcoidosis-like reactions. Chest. 2018;154(3):664–677. doi:10.1016/j.chest.2018.03.056
34. Cohen Aubart F, Lhote R, Amoura A, et al. Drug‐induced sarcoidosis: an overview of the WHO pharmacovigilance database. J Intern Med. 2019. doi:10.1111/joim.12991
35. Le Burel S, Champiat S, Mateus C, et al. Prevalence of immune-related systemic adverse events in patients treated with anti-Programmed cell Death 1/anti-Programmed cell Death-Ligand 1 agents: a single-centre pharmacovigilance database analysis. Eur J Cancer. 2017;82:34–44. doi:10.1016/j.ejca.2017.05.032
36. Seve P, Jamilloux Y, Gerfaud-Valentin M, El-Jammal T, Pavic M. Faut-il rechercher un cancer après la découverte d’une granulomatose inexpliquée? La Revue de Médecine Interne. 2019;40(8):487–490. doi:10.1016/j.revmed.2019.05.006
37. Bouvry D, Mouthon L, Brillet P-Y, et al. Granulomatosis-associated common variable immunodeficiency disorder: a case-control study versus sarcoidosis. Eur Respir J. 2013;41(1):115–122. doi:10.1183/09031936.00189011
38. Wu C, Wang R, Chen B, et al. Granuloma with an underlying Lymphoma A diagnostic challenge and a wider histologic spectrum including adult T-cell leukemia/lymphoma. Appl Immunohistochem Mol Morphol. 2019:1. doi:10.1097/PAI.0000000000000731.
39. Brincker H. The sarcoidosis-lymphoma syndrome. Br J Cancer. 1986;54(3):467–473. doi:10.1038/bjc.1986.199
40. Bernard C, Maucort-Boulch D, Varron L, et al. Cryptococcosis in sarcoidosis: cryptOsarc, a comparative study of 18 cases. QJM. 2013;106(6):523–539. doi:10.1093/qjmed/hct052
41. Jamilloux Y, Néel A, Lecouffe-Desprets M, et al. Progressive multifocal leukoencephalopathy in patients with sarcoidosis. Neurology. 2014;82(15):1307–1313. doi:10.1212/WNL.0000000000000318
42. Martusewicz-Boros MM, Boros PW, Wiatr E, Fijołek J, Roszkowski-Śliż K. Systemic treatment for sarcoidosis was needed for 16% of 1810 Caucasian patients. Clin Respir J. 2018;12(4):1367–1371. doi:10.1111/crj.12664
43. Paramothayan NS, Lasserson TJ, Jones P. Corticosteroids for pulmonary sarcoidosis. Cochrane Airways Group, ed. Cochrane Database of Syst Rev. 2005. doi:10.1002/14651858.CD001114.pub2
44. Broos CE, Wapenaar M, Looman CWN, et al. Daily home spirometry to detect early steroid treatment effects in newly treated pulmonary sarcoidosis. Eur Respir J. 2018;51(1):1702089. doi:10.1183/13993003.02089-2017
45. Mahévas M, Lescure FX, Boffa -J-J, et al. Renal Sarcoidosis: clinical, Laboratory, and Histologic Presentation and Outcome in 47 Patients. Medicine. 2009;88(2):98–106. doi:10.1097/MD.0b013e31819de50f
46. McKinzie BP, Bullington WM, Mazur JE, Judson MA. Efficacy of Short-Course, Low-Dose Corticosteroid Therapy for Acute Pulmonary Sarcoidosis Exacerbations. Am J Med Sci. 2010;339(1):1–4. doi:10.1097/MAJ.0b013e3181b97635
47. Baughman RP, Lower EE. Treatment of Sarcoidosis. Clin Rev Allergy Immunol. 2015;49(1):79–92. doi:10.1007/s12016-015-8492-9
48. Noe MH, Rosenbach M. Cutaneous sarcoidosis. Curr Opin Pulm Med. 2017;23(5):482–486. doi:10.1097/MCP.0000000000000402
49. Yang SJ, Salek S, Rosenbaum JT. Ocular sarcoidosis: new diagnostic modalities and treatment. Curr Opin Pulm Med. 2017;23(5):458–467. doi:10.1097/MCP.0000000000000409
50. Ho JSY, Chilvers ER, Thillai M. Cardiac sarcoidosis – an expert review for the chest physician. Expert Rev Respir Med. 2019;13(6):507–520. doi:10.1080/17476348.2018.1511431
51. Shelke AB, Aurangabadkar HU, Bradfield JS, Ali Z, Kumar KS, Narasimhan C. Serial FDG-PET scans help to identify steroid resistance in cardiac sarcoidosis. Int J Cardiol. 2017;228:717–722. doi:10.1016/j.ijcard.2016.11.142
52. Bitoun S, Bouvry D, Borie R, et al. Treatment of neurosarcoidosis: a comparative study of methotrexate and mycophenolate mofetil. Neurology. 2016;87(24):2517–2521. doi:10.1212/WNL.0000000000003431
53. Cohen Aubart F, Bouvry D, Galanaud D, et al. Long-term outcomes of refractory neurosarcoidosis treated with infliximab. J Neurol. 2017;264(5):891–897. doi:10.1007/s00415-017-8444-9
54. Stern BJ, Royal W, Gelfand JM, et al. Definition and consensus diagnostic criteria for neurosarcoidosis: from the Neurosarcoidosis Consortium Consensus Group. JAMA Neurol. 2018;75(12):1546. doi:10.1001/jamaneurol.2018.2295
55. Wengert O, Rothenfusser-Korber E, Vollrath B, et al. Neurosarcoidosis: correlation of cerebrospinal fluid findings with diffuse leptomeningeal gadolinium enhancement on MRI and clinical disease activity. J Neurol Sci. 2013;335(1–2):124–130. doi:10.1016/j.jns.2013.09.008
56. Hilderson I, Van Laecke S, Wauters A, Donck J. Treatment of renal sarcoidosis: is there a guideline? Overview of the different treatment options. Nephrol Dialysis Transplant. 2014;29(10):1841–1847. doi:10.1093/ndt/gft442
57. Schutt AC, Bullington WM, Judson MA. Pharmacotherapy for pulmonary sarcoidosis: a delphi consensus study. Respir Med. 2010;104(5):717–723. doi:10.1016/j.rmed.2009.12.009
58. Judson MA. An approach to the treatment of pulmonary sarcoidosis with corticosteroids. Chest. 1999;115(4):1158–1165. doi:10.1378/chest.115.4.1158
59. Grutters JC, van den Bosch JMM. Corticosteroid treatment in sarcoidosis. Eur Respir J. 2006;28(3):627–636. doi:10.1183/09031936.06.00105805
60. Al-Kofahi K, Korsten P, Ascoli C, et al. Management of extrapulmonary sarcoidosis: challenges and solutions. Ther Clin Risk Manag. 2016;12:1623–1634. doi:10.2147/TCRM.S74476
61. Judson M. Extrapulmonary Sarcoidosis. Semin Respir Crit Care Med. 2007;28(1):083–101. doi:10.1055/s-2007-970335
62. Matsou A, Tsaousis KT. Management of chronic ocular sarcoidosis: challenges and solutions. OPTH. 2018;12:519–532. doi:10.2147/OPTH.S128949
63. Touhami S, Diwo E, Sève P, et al. Expert opinion on the use of biological therapy in non-infectious uveitis. Expert Opin Biol Ther. 2019;19(5):477–490. doi:10.1080/14712598.2019.1595578
64. Baughman RP. Methotrexate is steroid sparing in acute sarcoidosis: results of a double blind, randomized trial. Sarcoidosis Vasc Diffuse Lung Dis. 2000;60–66.
65. Cremers JP, Drent M, Bast A, et al. Multinational evidence-based world association of sarcoidosis and other granulomatous disorders recommendations for the use of methotrexate in sarcoidosis: integrating systematic literature research and expert opinion of sarcoidologists worldwide. Curr Opin Pulm Med. 2013;19(5):545–561. doi:10.1097/MCP.0b013e3283642a7a
66. Lower E. Prolonged use of methotrexate for sarcoidosis. Arch Intern Med. 1995;155(8):846–851. doi:10.1001/archinte.1995.00430080088011
67. Mainman H, McClaren E, Heycock C, Saravanan V, Hamilton J, Kelly C. When should we use parenteral methotrexate? Clin Rheumatol. 2010;29(10):1093–1098. doi:10.1007/s10067-010-1500-9
68. Shea B, Swinden MV, Ghogomu ET, et al. Folic acid and folinic acid for reducing side effects in patients receiving methotrexate for rheumatoid arthritis. J Rheumatol. 2014;41(6):1049–1060. doi:10.3899/jrheum.130738
69. Baltzan M, Mehta S, Kirkham TH, Cosio MG. Randomized trial of prolonged chloroquine therapy in advanced pulmonary sarcoidosis. Am J Respir Crit Care Med. 1999;160(1):192–197. doi:10.1164/ajrccm.160.1.9809024
70. Judson M, Barba, Beegle, Gobunsuy. Current and emerging pharmacological treatments for sarcoidosis: a review. Drug Des Devel Ther. 2013;325. doi:10.2147/DDDT.S31064
71. Fritz D, van de Beek D, Brouwer MC. Clinical features, treatment and outcome in neurosarcoidosis: systematic review and meta-analysis. BMC Neurol. 2016;16(1):220. doi:10.1186/s12883-016-0741-x
72. Arthritis in Sarcoidosis Group (ASG), Agarwal V, Agrawal V, et al. Arthritis in sarcoidosis: a multicentric study from India. Int J Rheum Dis. 2018;21(9):1728–1733. doi:10.1111/1756-185X.13349.
73. Tselios K, Deeb M, Gladman DD, Harvey P, Urowitz MB. Antimalarial-induced cardiomyopathy: a systematic review of the literature. Lupus. 2018;27(4):591–599. doi:10.1177/0961203317734922
74. Bernstein HN. Ophthalmologic considerations and testing in patients receiving long-term antimalarial therapy. Am J Med. 1983;75(1):25–34. doi:10.1016/0002-9343(83)91267-6
75. Maltzman JS, Koretzky GA. Azathioprine: old drug, new actions. J Clin Invest. 2003;111(8):3. doi:10.1172/JCI200318384
76. Vorselaars ADM, Wuyts WA, Vorselaars VMM, et al. Methotrexate vs azathioprine in second-line therapy of sarcoidosis. Chest. 2013;144(3):805–812. doi:10.1378/chest.12-1728
77. Emery P, Breedveld FC, Lemmel EM, et al. A comparison of the efficacy and safety of leflunomide and methotrexate for the treatment of rheumatoid arthritis. Rheumatology. 2000;39(6):655–665. doi:10.1093/rheumatology/39.6.655
78. Baughman RP. Leflunomide for chronic sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis. 2004;21(1):43–48. doi:10.1007/s11083-004-5178-y
79. Sahoo DH, Bandyopadhyay D, Xu M, et al. Effectiveness and safety of leflunomide for pulmonary and extrapulmonary sarcoidosis. Eur Respir J. 2011;38(5):1145–1150. doi:10.1183/09031936.00195010
80. Androdias G, Maillet D, Marignier R, et al. Mycophenolate mofetil may be effective in CNS sarcoidosis but not in sarcoid myopathy. Neurology. 2011;76(13):1168–1172. doi:10.1212/WNL.0b013e318212aafb
81. Bhat P, Cervantes-Castañeda RA, Doctor PP, Anzaar F, Foster CS. Mycophenolate mofetil therapy for sarcoidosis-associated uveitis. Ocul Immunol Inflamm. 2009;17(3):185–190. doi:10.1080/09273940902862992
82. Chapelon-Abric C, Sene D, Saadoun D, et al. Cardiac sarcoidosis: diagnosis, therapeutic management and prognostic factors. Arch Cardiovasc Dis. 2017;110(8–9):456–465. doi:10.1016/j.acvd.2016.12.014
83. Doty JD, Mazur JE, Judson MA. Treatment of corticosteroid-resistant neurosarcoidosis with a short-course cyclophosphamide regimen. Chest. 2003;124(5):2023–2026. doi:10.1378/chest.124.5.2023
84. Varron L, Broussolle C, Candessanche J-P, et al. Spinal cord sarcoidosis: report of seven cases. Eur J Neurol. 2009;16(3):289–296. doi:10.1111/j.1468-1331.2008.02409.x
85. Baughman RP. Infliximab for refractory sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis. 2001;18(3):310.
86. Baughman RP, Lower EE, Bradley DA, Raymond LA, Kaufman A. Etanercept for refractory ocular sarcoidosis. Chest. 2005;128(2):1062–1067. doi:10.1016/S0012-3692(15)50471-6
87. Judson MA, Baughman RP, Costabel U, et al. Efficacy of infliximab in extrapulmonary sarcoidosis: results from a randomised trial. Eur Respir J. 2008;31(6):1189–1196. doi:10.1183/09031936.00051907
88. Baughman RP, Drent M, Kavuru M, et al. Infliximab therapy in patients with chronic sarcoidosis and pulmonary involvement. Am J Respir Crit Care Med. 2006;174(7):795–802. doi:10.1164/rccm.200603-402OC
89. Rossman M. A double-blinded, randomized, placebo-controlled trial of infliximab in subjects with active pulmonary sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis. 2006;23(3):201–208.
90. Pariser RJ, Paul J, Hirano S, Torosky C, Smith M. A double-blind, randomized, placebo-controlled trial of adalimumab in the treatment of cutaneous sarcoidosis. J Am Acad Dermatol. 2013;68(5):765–773. doi:10.1016/j.jaad.2012.10.056
91. Erckens RJ, Mostard RLM, Wijnen PAHM, Schouten JS, Drent M. Adalimumab successful in sarcoidosis patients with refractory chronic non-infectious uveitis. Graefe’s Arch Clin Exp Ophthalmol. 2012;250(5):713–720. doi:10.1007/s00417-011-1844-0
92. Adler BL, Wang CJ, Bui T-L, Schilperoort HM, Armstrong AW. Anti-tumor necrosis factor agents in sarcoidosis: a systematic review of efficacy and safety. Semin Arthritis Rheum. 2019;48(6):1093–1104. doi:10.1016/j.semarthrit.2018.10.005
93. Schimmelpennink MC, Vorselaars ADM, van Beek FT, et al. Efficacy and safety of infliximab biosimilar Inflectra ® in severe sarcoidosis. Respir Med. 2018;138:S7–S13. doi:10.1016/j.rmed.2018.02.009
94. Barba T, Marquet A, Bouvry D, et al. Efficacy and safety of infliximab therapy in refractory upper respiratory tract sarcoidosis: experience from the STAT registry. Sarcoidosis Vasc Diffuse Lung Dis. 2018;34(4):343–351.
95. Marquet A, Chapelon-Abric C, Maucort-Boulch D, et al. Efficacy and safety of TNF antagonists in ocular sarcoidosis: data from the French registry STAT. Sarcoidosis Vasc Diffuse Lung Dis. 2017;34(1):74.
96. Chung ES, Packer M, Lo KH, Fasanmade AA, Willerson JT. Randomized, double-blind, placebo-controlled, pilot trial of infliximab, a chimeric monoclonal antibody to tumor necrosis factor-α, in patients with moderate-to-severe heart failure: results of the Anti-TNF Therapy Against Congestive Heart failure (ATTACH) Trial. Circulation. 2003;107(25):3133–3140. doi:10.1161/01.CIR.0000077913.60364.D2
97. Puyraimond-Zemmour D, Chapelon-Abric C, Bouvry D, Ruivard M, André M, Pérard L. Efficacy and tolerance of TNF alpha inhibitor treatment in cardiac sarcoidosis. Int J Exp Clin Res. 2018;2018:1.
98. Harper LJ, McCarthy M, Ribeiro Neto ML, et al. Infliximab for refractory cardiac sarcoidosis. Am J Cardiol. 2019:S0002914919309555. doi:10.1016/j.amjcard.2019.07.067.
99. Judson MA, Baughman RP, Costabel U, et al. Safety and efficacy of ustekinumab or golimumab in patients with chronic sarcoidosis. Eur Respir J. 2014;44(5):1296–1307. doi:10.1183/09031936.00000914
100. Panselinas E, Rodgers JK, Judson MA. Clinical outcomes in sarcoidosis after cessation of infliximab treatment. Respirology. 2009;14(4):522–528. doi:10.1111/j.1440-1843.2009.01518.x
101. Vorselaars ADM, Verwoerd A, van Moorsel CHM, Keijsers RGM, Rijkers GT, Grutters JC. Prediction of relapse after discontinuation of infliximab therapy in severe sarcoidosis. Eur Respir J. 2014;43(2):602–609. doi:10.1183/09031936.00055213
102. Drent M, Cremers JP, Jansen TL, Baughman RP. Practical eminence and experience-based recommendations for use of tnf-α inhibitors in sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis. 2014;31(2):91–107.
103. Vande Casteele N, Gils A, Singh S, et al. Antibody response to infliximab and its impact on pharmacokinetics can be transient. Am J Gastroenterol. 2013;108(6):962–971. doi:10.1038/ajg.2013.12
104. Bloem K, van Leeuwen A, Verbeek G, et al. Systematic comparison of drug-tolerant assays for anti-drug antibodies in a cohort of adalimumab-treated rheumatoid arthritis patients. J Immunol Methods. 2015;418:29–38. doi:10.1016/j.jim.2015.01.007
105. Crommelin HA, van der Burg LM, Vorselaars ADM, et al. Efficacy of adalimumab in sarcoidosis patients who developed intolerance to infliximab. Respir Med. 2016;115:72–77. doi:10.1016/j.rmed.2016.04.011
106. Thery-Casari C, Jamilloux Y, Bouvry D, et al. Outcome of patients with sarcoidosis refractory to TNF antagonists: a case series. Sarcoidosis Vasc Diffuse Lung Dis. 2018;35:371–375.
107. Saussine A, Tazi A, Feuillet S, et al. Active chronic sarcoidosis is characterized by increased transitional blood B cells, increased IL-10-producing regulatory B cells and high BAFF Levels. Hoshino Y, ed. PLoS One. 2012;7(8):e43588. doi:10.1371/journal.pone.0043588
108. Beccastrini E, Vannozzi L, Bacherini D, Squatrito D, Emmi L. Successful treatment of ocular sarcoidosis with rituximab. Ocul Immunol Inflamm. 2013;21(3):244–246. doi:10.3109/09273948.2012.762982
109. Cinetto F, Compagno N, Scarpa R, Malipiero G, Agostini C. Rituximab in refractory sarcoidosis: a single centre experience. Clin Mol Allergy. 2015;13:1. doi:10.1186/s12948-015-0025-9
110. Gottenberg J-E. Tolerance and short-term efficacy of rituximab in 43 patients with systemic autoimmune diseases. Ann Rheum Dis. 2005;64(6):913–920. doi:10.1136/ard.2004.029694
111. Zella S, Kneiphof J, Haghikia A, Gold R, Woitalla D, Thöne J. Successful therapy with rituximab in three patients with probable neurosarcoidosis. Ther Adv Neurol Disord. 2018;11:175628641880573. doi:10.1177/1756286418805732
112. Bomprezzi R, Pati S, Chansakul C, Vollmer T. A case of neurosarcoidosis successfully treated with rituximab. Neurology. 2010;75(6):568–570. doi:10.1212/WNL.0b013e3181ec7ff9
113. Sawaya R, Radwan W. Sarcoidosis associated with neuromyelitis optica. J Clin Neurosci. 2013;20(8):1156–1158. doi:10.1016/j.jocn.2012.09.030
114. Baughman R, Lower K. Rituximab for refractory granulomatous eye disease. Clin Ophthalmol. 2012;1613. doi:10.2147/OPTH.S35521
115. van Vollenhoven RF, Fleischmann RM, Furst DE, Lacey S, Lehane PB. Longterm safety of rituximab: final report of the rheumatoid arthritis global clinical trial program over 11 years. J Rheumatol. 2015;42(10):1761–1766. doi:10.3899/jrheum.150051
116. Girgis RE, Basha MA, Maliarik M, Popovich J, Iannuzzi MC. Cytokines in the bronchoalveolar lavage fluid of patients with active pulmonary sarcoidosis. Am J Respir Crit Care Med. 1995;152(1):71–75. doi:10.1164/ajrccm.152.1.7599865
117. Awano N, Inomata M, Kondoh K, et al. Mixed-type multicentric castleman’s disease developing during a 17-year follow-up of sarcoidosis. Internal Med. 2012;51(21):3061–3066. doi:10.2169/internalmedicine.51.8120
118. Semiz H, Kobak S. Coexistence of sarcoidosis and adult onset Still disease. Reumatología Clínica. 2017. doi:10.1016/j.reuma.2017.04.004
119. Sharp M, Donnelly SC, Moller DR. Tocilizumab in sarcoidosis patients failing steroid sparing therapies and anti-TNF agents. Respir Med. 2019;1:100004. doi:10.1016/j.yrmex.2019.100004
120. Silpa-archa S, Oray M, Preble JM, Foster CS. Outcome of tocilizumab treatment in refractory ocular inflammatory diseases. Acta Ophthalmol (Copenh). 2016;94(6):e400–e406. doi:10.1111/aos.13015
121. Vegas-Revenga N, Calvo-Río V, Mesquida M, et al. Anti-IL6-receptor tocilizumab in refractory and noninfectious uveitic cystoid macular edema: multicenter study of 25 patients. Am J Ophthalmol. 2019;200:85–94. doi:10.1016/j.ajo.2018.12.019
122. Nutz A, Pernet C, Combe B, Cohen J-D. Sarcoidosis induced by tocilizumab: a paradoxical event? J Rheumatol. 2013;40(10):1773–1774. doi:10.3899/jrheum.130278
123. Bustamente L. Sarcoidosis and tocilizumab: is there a link? Clin Exp Rheumatol. 2017;35(4):716.
124. Del Giorno R, Iodice A, Mangas C, Gabutti L. New-onset cutaneous sarcoidosis under tocilizumab treatment for giant cell arteritis: a quasi-paradoxical adverse drug reaction. Case report and literature review. Ther Adv Musculoskelet Dis. 2019;11:1759720X1984179. doi:10.1177/1759720X19841796
125. Shono Y, Kamata M, Takeoka S, et al. Cutaneous sarcoidosis in a patient with rheumatoid arthritis receiving tocilizumab. J Dermatol. 2018;45(8):e217–e218. doi:10.1111/1346-8138.14268
126. Rosenbaum JT, Hessellund A, Phan I, Planck SR, Wilson DJ. The expression of STAT-1 and phosphorylated STAT-1 in conjunctival granulomas. Ocul Immunol Inflamm. 2010;18(4):261–264. doi:10.3109/09273941003797934
127. Levraut M, Martis N, Viau P, Suarez F, Queyrel V. Refractory sarcoidosis-like systemic granulomatosis responding to ruxolitinib. Ann Rheum Dis. 2019;
128. Damsky W, Thakral D, Emeagwali N, Galan A, King B. Tofacitinib treatment and molecular analysis of cutaneous sarcoidosis. N Engl J Med. 2018;379(26):2540–2546. doi:10.1056/NEJMoa1805958
129. Damsky W, Thakral D, McGeary MK, Leventhal J, Galan A, King B. Janus kinase inhibition induces disease remission in cutaneous sarcoidosis and granuloma annulare. J Am Acad Dermatol. 2019. doi:10.1016/j.jaad.2019.05.098
130. Wei JJ, Kallenbach LR, Kreider M, Leung TH, Rosenbach M. Resolution of cutaneous sarcoidosis after Janus kinase inhibitor therapy for concomitant polycythemia vera. JAAD Case Rep. 2019;5(4):360–361. doi:10.1016/j.jdcr.2019.02.006
131. Rotenberg C, Besnard V, Brillet P-Y, Giraudier S, Nunes H, Valeyre D. Dramatic response of refractory sarcoidosis under ruxolitinib in a patient with associated JAK2-mutated polycythemia. Eur Respir J. 2018;52(6):1801482. doi:10.1183/13993003.01482-2018
132. El Jammal T, Gerfaud-Valentin M, Sève P, Jamilloux Y. Inhibition of JAK/STAT signaling in rheumatologic disorders: the expanding spectrum. Joint Bone Spine. 2019;S1297319X19301265. doi:10.1016/j.jbspin.2019.09.005
133. Bechman K, Subesinghe S, Norton S, et al. A systematic review and meta-analysis of infection risk with small molecule JAK inhibitors in rheumatoid arthritis. Rheumatology. 2019;58(10):1755–1766. doi:10.1093/rheumatology/kez087
134. Wyser CP, van Schalkwyk EM, Alheit B, Bardin PG, Joubert JR. Treatment of progressive pulmonary sarcoidosis with cyclosporin A: a randomized controlled trial. Am J Respir Crit Care Med. 1997;156(5):1371–1376. doi:10.1164/ajrccm.156.5.9506031
135. Bogabathina H, Olson P, Rathi VK, Biederman RWW. Cardiac sarcoidosis or giant cell myocarditis? On treatment improvement of fulminant myocarditis as demonstrated by cardiovascular magnetic resonance imaging. Case Rep Cardiol. 2012;2012:1–5. doi:10.1155/2012/647041
136. Linke M, Pham HTT, Katholnig K, et al. Chronic signaling via the metabolic checkpoint kinase mTORC1 induces macrophage granuloma formation and marks sarcoidosis progression. Nat Immunol. 2017;18(3):293–302. doi:10.1038/ni.3655
137. Manzia TM, Bellini MI, Corona L, et al. Successful treatment of systemic de novo sarcoidosis with cyclosporine discontinuation and provision of rapamune after liver transplantation: letter to the editors. Transplant Int. 2011;24(8):e69–e70. doi:10.1111/j.1432-2277.2011.01256.x
138. Ibrahim MA, Sepah YJ, Watters A, et al. One-Year Outcomes of the SAVE Study: S irolimus as a therapeutic A pproach for U VE itis. Transl Vis Sci Technol. 2015;4(2):4. doi:10.1167/tvst.4.2.4
139. Nguyen QD, Sadiq MA, Agarwal A. The effect of different dosing schedules of intravitreal sirolimus, a mammalian target of rapamycin (mTOR) inhibitor, in the treatment of non-infectious uveitis (An american ophthalmological society thesis). Trans Am Ophthalmol Soc. 2016;14.
140. Nguyen QD, Merrill PT, Clark WL, et al. Intravitreal sirolimus for noninfectious uveitis: a phase III Sirolimus Study Assessing Double-masKed Uveitis TReAtment (SAKURA). Ophthalmology. 2016;123(11):2413–2423. doi:10.1016/j.ophtha.2016.07.029
141. Droitcourt C, Rybojad M, Porcher R, et al. A randomized, investigator-masked, double-blind, placebo-controlled trial on thalidomide in severe cutaneous sarcoidosis. Chest. 2014;146(4):1046–1054. doi:10.1378/chest.14-0015
142. Fazzi P, Manni E, Cristofani R, et al. Thalidomide for improving cutaneous and pulmonary sarcoidosis in patients resistant or with contraindications to corticosteroids. Biomed Pharmacother. 2012;66(4):300–307. doi:10.1016/j.biopha.2012.03.005
143. Huddleston SM, Houser KH, Walton RC. Thalidomide for recalcitrant nodular scleritis in sarcoidosis. JAMA Ophthalmol. 2014;132(11):1377. doi:10.1001/jamaophthalmol.2014.2420
144. Giv MJ, Yoosuff A, Bazargan A. Use of lenalidomide in 5q-myelodysplastic syndrome provides novel treatment prospects in management of pulmonary sarcoidosis. Chest. 2015;148(2):e35–e37. doi:10.1378/chest.14-2529
145. Baughman RP. Efficacy and safety of apremilast in chronic cutaneous sarcoidosis. Arch Dermatol. 2012;148(2):262. doi:10.1001/archdermatol.2011.301
146. Baughman RP, Grutters JC. New treatment strategies for pulmonary sarcoidosis: antimetabolites, biological drugs, and other treatment approaches. Lancet Respir Med. 2015;3(10):813–822. doi:10.1016/S2213-2600(15)00199-X
147. Chopra I, Qin Y, Kranyak J, et al. Repository corticotropin injection in patients with advanced symptomatic sarcoidosis: retrospective analysis of medical records. Ther Adv Respir Dis. 2019;13:175346661988812. doi:10.1177/1753466619888127
148. Zabel P, Entzian P, Dalhoff K, Schlaak M. Pentoxifylline in treatment of sarcoidosis. Am J Respir Crit Care Med. 1997;155(5):1665–1669. doi:10.1164/ajrccm.155.5.9154873
149. Park MK, Fontana JR, Babaali H, et al. Steroid-Sparing effects of pentoxifylline in pulmonary sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis. 2009;26(2):121–131.
150. Drake WP, Oswald-Richter K, Richmond BW, et al. Oral antimycobacterial therapy in chronic cutaneous sarcoidosis: a randomized, single-masked, placebo-controlled study. JAMA Dermatol. 2013;149(9):1040. doi:10.1001/jamadermatol.2013.4646
151. Drake WP, Richmond BW, Oswald-Richter K, et al. Effects of broad-spectrum antimycobacterial therapy on chronic pulmonary sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis. 2013;30(3):201–211.
152. Patterson KC, Strek ME. Pulmonary fibrosis in sarcoidosis. Clinical features and outcomes. Annals ATS. 2013;10(4):362–370. doi:10.1513/AnnalsATS.201303-069FR
153. Distler O, Highland KB, Gahlemann M, et al. Nintedanib for systemic sclerosis–associated interstitial lung disease. N Engl J Med. 2019;380(26):2518–2528. doi:10.1056/NEJMoa1903076
154. Flaherty KR, Wells AU, Cottin V, et al. Nintedanib in progressive fibrosing interstitial lung diseases. N Engl J Med. 2019;381(18):1718–1727. doi:10.1056/NEJMoa1908681
155. Kang S. Radiation therapy for neurosarcoidosis: report of three cases from a single institution. Radiat Oncol Investig. 1999;7(5):309–312. doi:10.1002/(SICI)1520-6823(1999)7:5<309::AID-ROI6>3.0.CO;2-W
156. Valeyre D, Jeny F, Nunes H. Current medical therapy for sarcoidosis. Semin Respir Crit Care Med. 2017;38(04):523–531. doi:10.1055/s-0037-1604032
157. Parambil JG, Tavee JO, Zhou L, Pearson KS, Culver DA. Efficacy of intravenous immunoglobulin for small fiber neuropathy associated with sarcoidosis. Respir Med. 2011;105(1):101–105. doi:10.1016/j.rmed.2010.09.015
158. Tavee JO, Karwa K, Ahmed Z, Thompson N, Parambil J, Culver DA. Sarcoidosis-associated small fiber neuropathy in a large cohort: clinical aspects and response to IVIG and anti-TNF alpha treatment. Respir Med. 2017;126:135–138. doi:10.1016/j.rmed.2017.03.011
159. Kono M, Kono M, Jodo S. A case of refractory acute sarcoid myopathy successfully treated with intravenous immunoglobulin. Scand J Rheumatol. 2018;47(2):168–169. doi:10.1080/03009742.2017.1393559
160. Kono Y, Omoto S, Sengoku R, et al. Multifocal conduction block in a patient with sarcoid neuropathy: successful treatment with intravenous immunoglobulin. Intern Med. 2013;52(9):999–1002. doi:10.2169/internalmedicine.52.7788
161. Spagnolo P, Rossi G, Trisolini R, Sverzellati N, Baughman RP, Wells AU. Pulmonary sarcoidosis. Lancet Respir Med. 2018;6(5):389–402. doi:10.1016/S2213-2600(18)30064-X
162. Nunes H, Soler P, Valeyre D. Pulmonary sarcoidosis. Allergy. 2005;60(5):565–582. doi:10.1111/j.1398-9995.2005.00778.x
163. Sweiss N, Patterson K, Sawaqed R, et al. Rheumatologic manifestations of sarcoidosis. Semin Respir Crit Care Med. 2010;31(04):463–473. doi:10.1055/s-0030-1262214
164. Cohen Aubart F, Nunes H, Mathian A, et al. Sarcoïdose cardiaque: avancées diagnostiques et thérapeutiques. La Revue de Médecine Interne. 2017;38(1):28–35. doi:10.1016/j.revmed.2016.03.003
165. Birnie D, Beanlands RSB, Nery P, et al. Cardiac Sarcoidosis multi-center randomized controlled trial (CHASM CS- RCT). Am Heart J. 2020;220:246–252. doi:10.1016/j.ahj.2019.10.003
166. Groen F, Rothova A. Ocular involvement in sarcoidosis. Semin Respir Crit Care Med. 2017;38(04):514–522. doi:10.1055/s-0037-1602382
167. Sève P, Jamilloux Y, Tilikete C, Gerfaud-Valentin M, Kodjikian L, El Jammal T. Ocular sarcoidosis. Semin Respir Crit Care Med. 2020.
168. Dai C, Shih S, Ansari A, Kwak Y, Sami N. Biologic therapy in the treatment of cutaneous sarcoidosis: a literature review. Am J Clin Dermatol. 2019;20(3):409–422. doi:10.1007/s40257-019-00428-8
169. Wanat KA, Rosenbach M. Cutaneous sarcoidosis. Clin Chest Med. 2015;36(4):685–702. doi:10.1016/j.ccm.2015.08.010
170. Edriss H, Kelley JS, Demke J, Nugent K. Sinonasal and laryngeal sarcoidosis—an uncommon presentation and management challenge. Am J Med Sci. 2019;357(2):93–102. doi:10.1016/j.amjms.2018.11.007
171. Voortman M, Drent M, Baughman RP. Management of neurosarcoidosis: a clinical challenge. Curr Opin Neurol. 2019;32(3):475–483. doi:10.1097/WCO.0000000000000684
172. Mahevas M, Simon T, Audard V, et al. Résultats de l’étude Corticoïdose. Étude prospective multicentrique randomisée comparant l’efficacité et la tolérance des bolus de méthylprednisolone dans la sarcoïdose rénale. La Revue de Médecine Interne. 2017;38:A43. doi:10.1016/j.revmed.2017.10.308
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.