Back to Journals » Clinical and Experimental Gastroenterology » Volume 17
Refractory Crohn’s Disease: Perspectives, Unmet Needs and Innovations
Authors Bertin L ![]() , Crepaldi M, Zanconato M
, Crepaldi M, Zanconato M ![]() , Lorenzon G
, Lorenzon G ![]() , Maniero D, De Barba C
, Maniero D, De Barba C ![]() , Bonazzi E, Facchin S, Scarpa M, Ruffolo C, Angriman I
, Bonazzi E, Facchin S, Scarpa M, Ruffolo C, Angriman I ![]() , Buda A, Zingone F, Savarino EV
, Buda A, Zingone F, Savarino EV ![]() , Barberio B
, Barberio B ![]()
Received 3 June 2024
Accepted for publication 4 October 2024
Published 10 October 2024 Volume 2024:17 Pages 261—315
DOI https://doi.org/10.2147/CEG.S434014
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Andreas M. Kaiser
Luisa Bertin,1 Martina Crepaldi,1 Miriana Zanconato,1 Greta Lorenzon,1 Daria Maniero,1 Caterina De Barba,1 Erica Bonazzi,1 Sonia Facchin,1 Marco Scarpa,2 Cesare Ruffolo,2 Imerio Angriman,2 Andrea Buda,3 Fabiana Zingone,1 Edoardo Vincenzo Savarino,1 Brigida Barberio1
1Gastroenterology Unit, Department of Surgery, Oncology and Gastroenterology, University of Padova, Padova, Italy; 2Chirurgia Generale 3 Unit, Azienda Ospedale Università di Padova, Padua, Italy; 3Gastroenterology Unit, Department of Oncological Gastrointestinal Surgery, Feltre, Italy
Correspondence: Edoardo Vincenzo Savarino, Gastroenterology Unit, Department of Surgery, Oncology and Gastroenterology, University of Padova, Padova, Italy, Tel +39-049-8217749, Fax +39-049-8760820, Email [email protected]
Abstract: Crohn’s disease (CD) is a complex, chronic inflammatory bowel disease characterized by unpredictable flare-ups and periods of remission. Despite advances in treatment, CD remains a significant health burden, leading to substantial direct healthcare costs and out-of-pocket expenses for patients, especially in the first-year post-diagnosis. The impact of CD on patients’ quality of life is profound, with significant reductions in physical, emotional, and social well-being. Despite advancements in therapeutic options, including biologics, immunomodulators, and small molecules, many patients struggle to achieve or maintain remission, leading to a considerable therapeutic ceiling. This has led to an increased focus on novel and emerging treatments. This context underscores the importance of exploring advanced and innovative treatment options for managing refractory CD. By examining the latest approaches, including immunomodulators, combination therapies, stem cell therapies, and emerging treatments like fecal microbiota transplantation and dietary interventions, there is an opportunity to gain a comprehensive understanding of how best to address and manage refractory cases of CD.
Keywords: refractory Crohn’s disease, mesenchymal stem cell therapy, medical therapy, combination therapy, fecal microbiota transplantation, biologic drugs, perianal Crohn’s disease, small molecules, hyperbaric oxygen therapy
Graphical Abstract:

Introduction
Crohn’s disease (CD) is a chronic idiopathic inflammatory bowel disease (IBD) affecting individuals across all age groups. Nonetheless, most diagnoses occur in young adults, with an observed increase in diagnoses aged between 20 and 60.1–3 The reported prevalence of CD varies, with the highest rates observed in Germany, where it reaches 322 cases per 100.000 people.4 However, CD incidence has increased in Asia, Africa, and Latin America due to industrialization and adopting Westernized diets and lifestyles.5,6
Around 1 in 5 patients with CD develop perianal disease within 10 years of their diagnosis, with 11.5% presenting with it at the time of diagnosis.7 Complications such as strictures, fistulas, and abscesses occur in approximately 50% of patients with CD.8 An IBD diagnosis leads to more than triple the direct healthcare costs compared to non-IBD patients, along with significantly higher out-of-pocket expenses and productivity losses, particularly in the first year after diagnosis.9 To understand the impact of this disease, a systematic review published in 2013, calculated the total annual economic burden of CD in Europe and the USA which was estimated to be nearly €30 billion, with indirect costs (such as lost productivity and absenteeism) comprising more than half of these costs.10 The primary drivers of CD-related costs include disease severity, hospitalizations, surgeries, and the use of biologic therapies. Moreover, CD significantly impairs HRQoL, with patients reporting lower physical, emotional, and social well-being compared to the general population. HRQoL declines are more pronounced during active disease phases and improve during remission, but rarely reach levels comparable to the general population.10 The impact of this condition on quality of life and bowel disability remains high despite the progress in therapeutic management.11–13
The therapeutic armamentarium of CD evolved from early 20th-century dietary changes to the introduction of corticosteroids in the 1940s. Immunomodulators emerged in the 1970s-80s. The late 1990s saw a breakthrough with biologics, and recent years have brought small molecule drugs.14–17 However, despite the numerous therapies available to treat the disease, disease remission is not always reached or maintained with these therapies, shaping the concept of a “therapeutic ceiling”.18 About 50% of patients experience secondary loss of response, and 30% experience primary non-response after biologic treatment.19,20 The main goal of the available therapies is to target chronic inflammation, primarily driven by an imbalance between pro-inflammatory and anti-inflammatory cytokines, as well as dysregulated immune cells. However, in refractory cases, where the disease does not respond to standard treatments, the underlying mechanisms may involve more complex immune dysregulation, microbial imbalances, or genetic factors, necessitating more advanced or personalized therapeutic approaches.
In this context, efforts to define refractory IBD have been made. Refractory IBD has been described as a disease that does not respond or loses response to all classes of licensed immunosuppressive and biologic agents or a disease not amenable to surgery by the 2021 European Crohn’s and Colitis Organization (ECCO) topical review consensus.21 This evolving definition encompasses newer therapeutic agents introduced into the landscape of CD treatment. However, it currently excludes small molecules, including those that target specific Janus kinases or modulators of the sphingosine-1 phosphate receptor (S1PR). Refractory perianal fistulizing CD was defined by the same consensus as a failure of at least one surgical intervention and anti-tumor necrosis factor therapy (anti-TNF).21 However, the size of the problem has not yet been defined since the global prevalence of refractory CD is unknown.22 Classically, risk factors for severe disease include early onset disease, perianal disease, ileocolic and upper GI tract location. However, lack of treatment optimization, non-adherence to therapy, delayed diagnosis, and disparities in care can also negatively affect prognoses of these patients.23
Despite numerous studies defining risk factors for aggressive disease, there remains a scarcity of predictors or biomarkers indicating refractory disease behavior or a scoring system incorporating these variables. This shortfall may be attributed to the heterogeneous nature and course variability of the disease. From a molecular perspective, a recent study has explored the underlying mechanisms of refractory disease in IBD, observing increased mucosal transcription of IL-17 and IL-23 in patients with non-response to biologic therapy.23 The diagnosis and treatment of refractory CD continue to be areas of active debate. This review aims to explore optimal management strategies and available therapies, with the goal of guiding future research and improving clinical practice.
Diagnosis and Challenges of Refractory CD
Diagnosing refractory CD involves ruling out other potential causes of symptoms, evaluating disease activity, assessing the adherence of patients to treatment and, in some cases, using therapeutic drug monitoring (TDM). Therefore, its diagnosis requires accuracy and attention.
The complexity of the scenario is also enhanced by the fact that clinical symptoms may be present even though the disease is in remission, with clinical scores like the Harvard-Bradshaw Index (HBI) correlating poorly with endoscopic activity.24 For this reason, treatment targets have evolved from symptomatic improvement to clinical remission and endoscopic healing, normalization of biomarkers, absence of disability, restoration of quality of life, as defined by STRIDE-II consensus.25 The disease activity assessment should therefore include using serum or fecal biomarkers, conducting endoscopy. Clinical response was defined as a reduction of at least 50% in patient-reported outcomes related to abdominal pain and stool frequency, while clinical remission for CD was defined by either score of abdominal pain at ≤1 and stool frequency ≤3, or a HBI score of less than 5. Endoscopic healing was defined as a Simple Endoscopic Score for Crohn’s Disease (SES-CD) of less than 3 points or the absence of ulcerations, with SES-CD ulceration subscores of 0. Although endoscopic healing is a treatment goal, patients still favor non-invasive monitoring methods, as intestinal ultrasound.26 The presence of clinical symptoms despite treatment optimization necessitates the exclusion of another potential that could mimic active IBD symptoms. Disorders of Gut-Brain Interaction (DGBI) are more common among individuals with IBD compared to the general population, with approximately 40% experiencing symptoms compatible with irritable bowel syndrome (IBS).27 Organic conditions that may contribute to the differential diagnosis are bacterial infections (including Clostridium difficile, Salmonella, Yersinia, and Campylobacter), viral infections (such as CMV), sexually transmitted infections (like Chlamydia trachomatis and syphilis), bowel enteropathy linked to medication use (such as NSAIDs, mycophenolate, or cocaine). Additionally, exposure to cell cycle checkpoint inhibitors, radiotherapy, and ischemic changes due to vascular insufficiency or vasculitis should be considered. Other potential causes include sarcoidosis, coeliac disease, intestinal lymphoma, bile acid malabsorption, and small bowel overgrowth.21
Adherence to treatment poses a frequent challenge in chronic conditions, potentially worsening disease severity and increasing the risk of relapse, reduced effectiveness of anti-TNFs and heightened morbidity.28 It is estimated that between 53% to 75% of individuals with IBD fail to adhere to prescribed medication regimens as directed.28,29 Jackson et al in their systematic review noted significant associations between demographic, clinical, and psychosocial factors and non-adherence in IBD.30 However, they found inconsistencies due to heterogeneity of inclusion criteria across studies. Notably, younger age, employment status, unmarried status, and shorter disease duration were linked to non-adherence to oral medication. Moreover, prescription of concomitant medications was associated with lower adherence. Psychological distress and doctor-patient discordance were also cited as contributors to non-adherence, although findings regarding depression and anxiety varied across studies. There are two main approaches for assessing adherence: direct methods, such as biochemical analysis, and indirect methods, like pill counts, pharmacy refills, self-reporting, or electronic monitoring devices.28
Therapeutic drug monitoring entails assessing drug concentrations and detecting the emergence of antidrug antibodies (ADA).31 It proves particularly valuable in patients receiving therapy with anti-TNFs or thiopurines. It may also be considered for those undergoing treatment with vedolizumab or ustekinumab.32 TDM serves two primary purposes: addressing the loss of response (reactive TDM) or optimizing treatment during remission (proactive TDM), offering potential benefits under specific circumstances. A proactive TDM approach facilitates the identification of poor adherence, which becomes increasingly relevant with subcutaneous infliximab and vedolizumab formulations.33 However, challenges persist in TDM implementation. Inter-assay variability challenges translating findings to clinical practice.34 The turnaround time for results may lead to delays in dose adjustments.35 Various patient-related and disease-related factors, such as inflammatory burden or disease phenotype, influence pharmacokinetics, and in this context, fistulizing disease may necessitate a tailored TDM approach.36
Optimizing Current Medical Treatments for Refractory Luminal CD
Biologic medications are fundamental in managing moderate-to-severe CD. The available agents include anti-TNFs (such as infliximab, adalimumab, and certolizumab pegol), antibodies targeting the p40 subunit of interleukins (IL)-12 and −23 (ustekinumab), and α4β7 integrins on leukocytes (vedolizumab).37–39 Recently, the FDA has approved a specific interleukin-23 inhibitor (risankizumab) and an oral selective Janus kinase (upadacitinib) for adults with moderate-to-severe CD who have had an inadequate response to one or more TNF blockers.40 Further strategies have been explored in refractory patients with CD, such as altering drug sequencing (ascending/descending ladder) and employing switching and sequential therapy, all geared towards improving treatment outcomes in IBD in clinical settings. Nevertheless, the long-term response rate remains inadequate.41 A significant proportion of patients, up to one-third, may experience a primary non-response. For these patients, switching to a biologic with a different mechanism of action is often more effective. In clinical practice, when patients exhibit reduced responsiveness to medications, healthcare providers often consider TDM. Other strategies include reinduction, increasing dose frequency or drug dosage. However, there is no clear evidence on the best strategy for optimizing anti-TNF therapies, though options include either doubling the dose or shortening the intervals between doses.42
Regarding ustekinumab, a multicenter study led by Fumery et al enrolled 100 patients with active CD who needed to escalate their ustekinumab dosage to 90 mg every four weeks due to either a loss of response or an incomplete response to the standard dose of 90 mg every eight weeks. The study discovered that two-thirds of the patients achieved a clinical response after the treatment was intensified to 90 mg every four weeks.43 A systematic review evaluating the effectiveness of reinduction and/or shortening the dose interval of ustekinumab found that shortening the interval to every 4 to 6 weeks was the most common escalation strategy, leading to endoscopic response in patients with CD with inadequate response or loss of response to induction or maintenance therapy.44
Recent studies have also demonstrated that increasing the dosing frequency of vedolizumab to every four weeks is associated with improved endoscopic outcomes.45,46
Currently, there is minimal to no data available to guide the optimization of risankizumab and upadacitinib beyond the approved doses to enhance clinical outcomes.47
In cases where drug optimization fails to yield results, medical therapeutic approaches may involve combining two drugs with distinct mechanisms, considering bowel bone marrow autotransplantation, hematopoietic stem cell therapy, fecal microbiota transplantation or immunomodulators. Dietary treatments may represent an adjunctive measure in these patients.
Combination Therapy
Combination therapies encompass two scenarios: 1) pairing a biologic or small molecule with an immunosuppressor such as thiopurine, methotrexate, or calcineurin inhibitor, and 2) dual-targeted therapy (DTT), which involves using two biologic agents and/or small molecules concurrently. These approaches may be considered for patients with concurrent IBD and extraintestinal manifestations or those with medically refractory IBD lacking viable alternatives. However, cost, logistics, and safety concerns have hindered research progress.
The seminal study in this area was the SONIC trial (Study Of Biologic and Immunomodulator Naive Patients In Crohn’s Disease), published in 2010, where Colombel et al conducted a randomized controlled trial (RCT) in patients with CD, revealing that the combination of infliximab and azathioprine was more effective than either treatment alone.48 Patients who underwent combination therapy experienced notably greater rates of achieving corticosteroid-free clinical remission and mucosal healing at week 26 and lower instances of immunogenicity. At week 30, antibodies to infliximab were identified in only 0.9% patients undergoing combination therapy, compared to 14.6% receiving infliximab alone. Interestingly, the combination therapy group was also determined to be the safest course of action. The investigation into the enhanced efficacy of combination therapy was extended through a subsequent post hoc analysis of SONIC. This analysis revealed that the elevated efficacy rates were attributed to increased drug levels rather than solely to the utilization of combination therapy.49 The results of the COMMIT trial, unveiled in 2014, investigated the efficacy of combining infliximab with parenteral methotrexate in contrast to infliximab alone. Although it showed that patients receiving the combination had higher levels of infliximab and lower occurrences of anti-drug antibodies compared to those on monotherapy, no clear benefit was evident in clinical outcomes.50
The more recent PROFILE (PRedicting Outcomes For CD using a moLecular biomarker) study recently validated this finding. Indeed, it demonstrated that initiating treatment with a combination of infliximab and an immunomodulator in patients with newly diagnosed active CD led to significantly superior outcomes at one year compared to the accelerated step-up approach.51 Colombel et al also published the EXPLORER trial in 2023, a Phase IV, single-arm, open-label study evaluating triple combination therapy with vedolizumab, adalimumab, and methotrexate in biologic-naïve patients with newly diagnosed CD.52 This combination therapy led to endoscopic and clinical remission at week 26 in 34.5% and 54.5% of patients, respectively, without any safety concerns related to the treatment regimen.
Apart from RCTs, much of the data on combination drugs in IBD stems from lower-quality sources such as cohort studies, case series, and reports. Recent meta-analyses and comprehensive reviews have explored the efficacy and safety of this treatment approach.53,54 Ribaldone et al in their systematic review focused on dual biologic therapy with anti-TNFs, vedolizumab, or ustekinumab, included seven studies involving 18 patients (56% with CD). Patients received a combination of anti-TNFs and vedolizumab or vedolizumab and ustekinumab, resulting in clinical improvement in 100% and 93% of patients, respectively.53 Another recent meta-analysis of 30 studies, including 279 patients receiving dual biologic therapy in combination or with tofacitinib (79% patients with CD), found that pooled clinical and endoscopic remission rates were 59% and 34%, respectively.54 Surgical intervention was required in 12% of cases, with 31% experiencing adverse effects, including 7% categorized as life-threatening, over a median follow-up of 32 weeks. A retrospective multicenter European observational study of 98 IBD patients undergoing combination therapy with biologics and small molecules, along with accompanying extraintestinal manifestations or other immune-mediated inflammatory diseases, found that the most common combination was anti-TNFs and vedolizumab, with 80% of patients being treatment-naïve to the second drug.55 Dual therapy with ustekinumab and vedolizumab led to an endoscopic response in 11 out of 13 patients with CD after an 11-month follow-up.55 Moreover, in a recent systematic review with meta-analysis conducted by Alayo et al, comprising 13 studies and 273 patients, the safety and efficacy of biologics and small molecules in IBD were analyzed. The review revealed that 77.9% of patients treated with anti-TNFs and vedolizumab achieved clinical response, while 55.1% attained clinical remission.56 The pooled rates of clinical remission and response among patients on vedolizumab plus ustekinumab were 47.0% and 83.9%, respectively. However, the combination of vedolizumab and tofacitinib was associated with lower rates of clinical response (59.9%) and clinical remission (55.1%). Regarding adverse events, a study examining DTT in IBD patients revealed varying rates, ranging from 13% to 30%, with infections being the most prevalent adverse effect.57 Research into combination therapy involving ustekinumab and vedolizumab typically indicated minimal adverse effects.58–61 At the same time, slightly higher rates were observed with anti-TNFs and vedolizumab, ranging from 15% to 37.5%, primarily due to an increased risk of infections.41,56,61 Conversely, limited data on patients receiving anti-TNFs and ustekinumab showed clinical response without adverse effects.59–63 Further studies comparing the efficacy and safety of combination therapies are warranted due to the limited data on infection risk and long-term effects.
For a comprehensive overview of the studies examining combined therapy for refractory luminal CD, please refer to Tables 1 and 2.
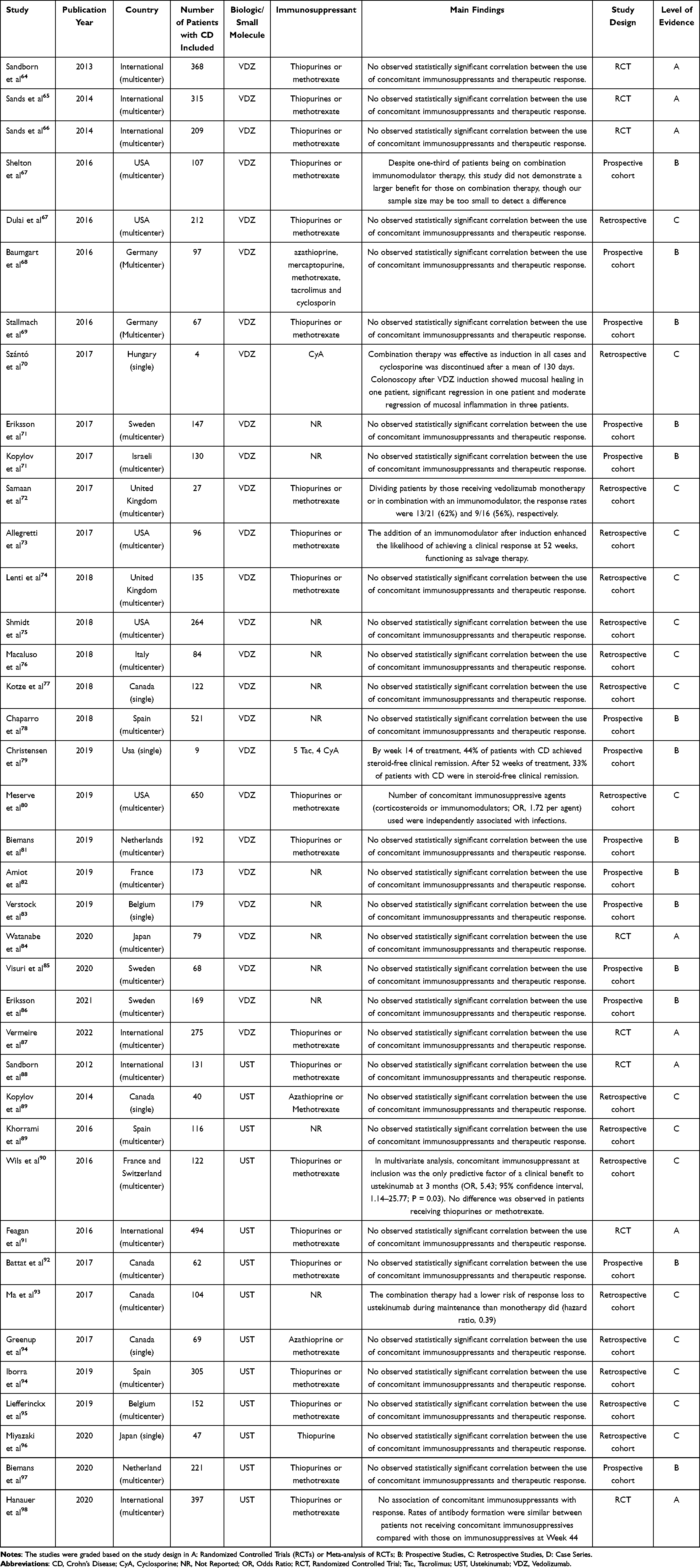 |
Table 1 Description of Selected Studies for Combined Therapy of Refractory Luminal Crohn’s Disease |
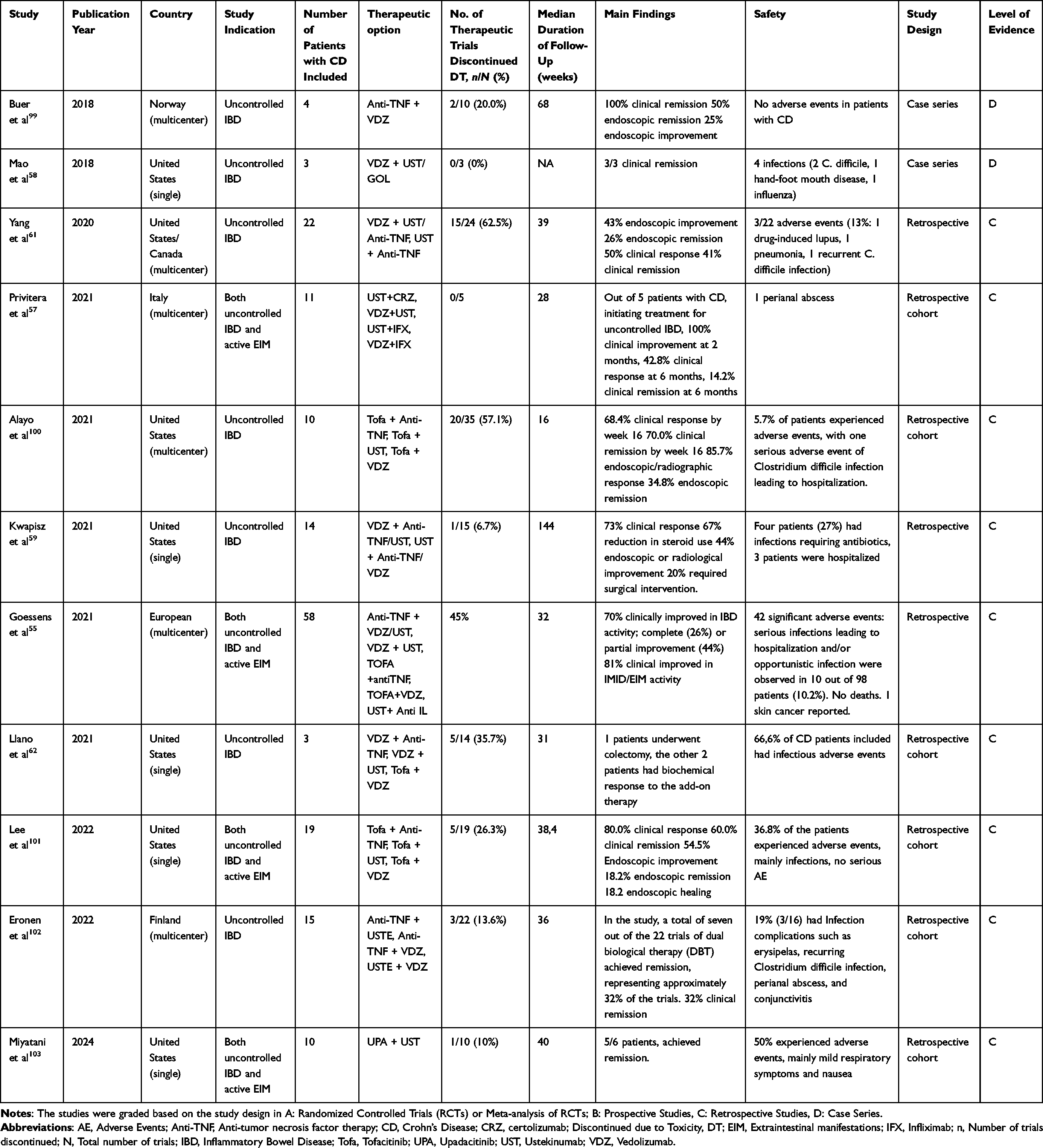 |
Table 2 Description of Selected Studies for Double Target Therapy of Refractory Luminal Crohn’s Disease |
Dual therapy could be an attractive opportunity for refractory patients with CD. In the future, identifying the most effective and safest combinations and exploring combinations with non-immunosuppressive treatments, such as those targeting environmental factors like diet or the microbiome, will be essential.
Hematopoietic Stem Cell Transplantation
Hematopoietic stem cell transplantation (HSCT) is widely used in benign and malignant hematological diseases.104 Stem cells are retrievable from peripheral blood, bone marrow, or umbilical cord units. Hematopoietic stem-cell transplantation can take two forms: autologous, where the stem cells originate from the recipient, or allogeneic, where they are sourced from another individual or one or more umbilical cord blood units. During the last decade, mainly autologous HSCT gained increasing attention in treating refractory autoimmune diseases. Indeed, HSCT aims to regenerate the immune system and establish immune tolerance, offering a viable treatment option for refractory CD by addressing the immune dysregulation that is thought to be a key factor in IBD pathophysiology.
Autologous HSCT was used in patients with CD affected by malignant hematological disease during the 1990s. An improvement or a disease remission was reported after HSCT.105–107 In 2003, a retrospective analysis that included 7 patients with CD and 4 with UC diagnosis treated with allogeneic HSCT for acute/chronic myeloid leukemia or myelodysplastic syndrome observed a clinical remission during a follow-up that could range from 3 months to 10 years. Currently, evidence on HSCT in CD is still limited to phase I/II studies, small prospective single-arm retrospective studies or case reports. According to data from the European Bone Marrow Transplantation registry, between January 1997 and July 2023, 232 patients underwent HSCT for CD. Out of them, 210 (91%) were adults and 22 (10%) were children under 18 years old at the time of transplantation. Among the procedures, 223 (96%) were performed in the autologous setting and nine (4%) in the allogeneic setting. The ASTIC trial, conducted between July 2007 and September 2011, involved 11 European transplant units. The primary endpoint of the trial was achieving clinical remission for a minimum of 3 months within the year following HSCT, without the use of immunosuppressives or biological treatments, and demonstrating a normal gastrointestinal tract according to endoscopic and radiologic assessments. Patients with CD younger than 50 years who had at least three unsuccessful treatment attempts with immunomodulators or biologics and were not suitable for surgery were included. All patients received mobilization with cyclophosphamide and G-CSF. Consequently, 23 patients underwent HSCT, and 22 were controls. ASTIC trial showed that HSCT was associated with a high burden of adverse events, particularly infections linked to pancytopenia induced by the conditioning regimen, resulting in one patient fatality.108 The stringent primary endpoint criteria were met by only two patients who underwent immediate HSCT and one patient who underwent delayed HSCT. Complete endoscopic healing was noted in half of the patients, and the combined primary endpoint of clinical remission with a CDAI < 150 and no corticosteroids for at least three months was achieved by 38% of patients after one year. It was also observed that an inflammatory phenotype, colonic disease location, and a high endoscopic disease score were associated with treatment response. In contrast, smoking and perianal disease were identified as risk factors for adverse effects.109 A single-center cohort assessed 37 patients with CD for HSCT in Barcelona. Relapse occurred in most patients within five years after transplant; these patients retreated, and 80% gained clinical remission.110 In 2020, Burt et al conducted a pilot study of non-myeloablative allogeneic HSCT in patients with CD. Three patients received unselected matched sibling peripheral blood stem cells, and six received umbilical cord blood when a matched sibling donor was not available. During 5-year follow-up, there was not clinical, imaging, endoscopic, or histologic evidence of disease.111
A breaking point is the safety of HSCT because this procedure is associated with febrile neutropenia, bacteremia, septic shocks, and acute Graft Versus Host Disease. Due to the risk of HSCT-related mortality and morbidity in CD, the risks and benefits of performing such a high-risk therapeutic procedure have to be carefully weighed.108,111,112 The hematopoietic cell transplantation comorbidity index (HCT-CI) could estimate pre-transplant comorbidities that predict non-relapse mortality and survival.113 Besides, mortality occurred in one of the 23 transplanted patients of the ASTIC trial (sinusoidal obstructive syndrome), the Barcelona cohort (due to CMV infection) and a multicenter trial in Brazil (due to disseminated adenovirus infection). The ASTIClite trial implemented a reduced-intensity conditioning regimen to mitigate toxicity. Its primary goal, achievable within a 48-week follow-up, centered on the absence of endoscopic ulceration without necessitating surgery or resulting in mortality. The trial compared the safety and efficacy of autologous HSCT with a lower dose of cyclophosphamide during stem-cell mobilization and conditioning against the standard of care. However, due to a significant occurrence of serious adverse events and two fatalities, the trial was prematurely halted.114
Stem cell therapy holds promise for patients with CD by modulating immune responses and inducing remission. More investigation is required to define uniform dosing schedules and stems cell quantities protocols. Stem cell mobilization reduces patient immunity, heightening infection susceptibility.115 Due to its associated morbidity and mortality, HSTC should be reserved for highly selected patients or within clinical trials.21 Currently, three ongoing trials in the United States are actively enrolling patients for autologous HSCT in CD (NCT04224558, NCT00692939, NCT03219359), with the third trial investigating vedolizumab post-autologous HSCT as maintenance therapy.
Mesenchymal Stem Cell Therapy
Stem cell transplantation is a valuable adjunctive therapy for CD, with mesenchymal stem cells (MSCs) demonstrating lower immunogenicity and more excellent immunomodulatory effects than HSCs.116 MSCs are multipotent stem cells capable of both self-renewal and differentiation into diverse cell lineages.117 MSCs exhibit differentiation potential into adipocytes, osteocytes, and chondrocytes in vitro. Various sources contribute to the availability of MSCs, including bone marrow, adipose tissue, muscle, peripheral blood, umbilical cord, placenta, fetal tissue, and amniotic fluid. MSC has been used intravenously to treat luminal CD, locally to treat perianal CD fistulas and CD strictures, even though its exact mechanism in this condition is yet to be understood.118,119
RCTs have demonstrated that administering intravenous MSCs can enhance CD-related immune tolerance and alleviate CD symptoms.120–125 A meta-analysis conducted in 2019 identified 13 RCTs of MSCs, indicating both efficacy and safety.126 Regarding luminal refractory CD, Phase I trials have confirmed the safety and feasibility of MSC therapy.120,121 Moreover, Phase II studies and case reports have shown promising results in reducing disease activity scores with allogeneic bone marrow and cord blood-derived MSCs.122,124 In phase IIa double-blind study, 50 patients with moderate to severe CD were randomly assigned to placebo or placenta-derived MSC (PDA-001).127 Clinical improvement in patients treated with PDA-001 compared to placebo. Only one treatment-related serious adverse event occurred (systematic hypersensitivity reaction). A recent systematic review and meta-analysis examined 28 animal studies and 18 human trials on CD and stem cells.128 In the MSC treatment group, disease activity decreased compared to the control group. Animals that received MSC treatment exhibited lower histopathological scores and reduced myeloperoxidase levels. Similarly, clinical trials showed reduced CD activity and endoscopic severity indices in patients. Patients with CD maintained high remission rates for 3–24 months after transplantation. Interestingly, subgroup analysis by the source of stem cells revealed that autologous stem cells had a more favorable effect on the CDAI than allogeneic stem cells.
More recently, a study evaluated MSC injection in CD strictures. In a Phase I–II clinical study, allogeneic bone marrow-derived MSCs injected into non-passable strictures of patients with CD showed partial or complete resolution in some cases, with good tolerability but no statistically significant evolution in clinical scores over time.118 For an overview of the selected studies in this review focusing on hematopoietic stem cell transplantation for refractory luminal CD, please refer to Table 3.
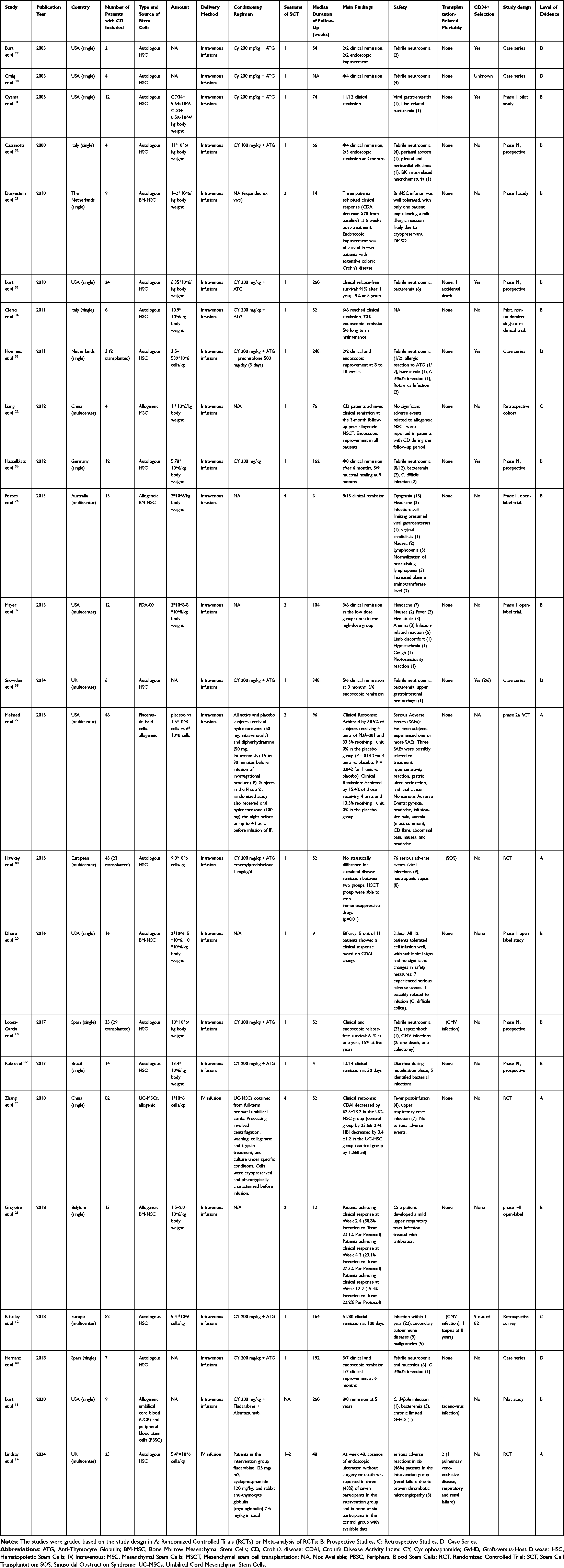 |
Table 3 Description of Selected Studies for Hematopoietic Stem Cell Transplantation of Refractory Luminal Crohn’s Disease |
A Cochrane review published in 2022 examined the efficacy and safety of stem cell transplantation (SCT) for refractory CD and found that SCT showed uncertain effects on achieving clinical remission and CDAI <150 at 24 weeks, with low to very low certainty evidence.141 However, it was likely to achieve fistula closure both in short and long-term follow-up, albeit with low-certainty evidence. There was no significant difference in total adverse events between SCT and control, but SCT increased serious adverse events with low-certainty evidence. Withdrawal due to adverse events was slightly higher in the control group. Limitations include small sample sizes and varying blinding methods across studies.
Despite the short-term safety and feasibility of MSC therapy, challenges such as long-term side effects and poor engraftment need to be addressed for wider clinical adoption. Strategies like cell priming and genetic modification could enhance engraftment, while exosome therapy offers a promising alternative with its better engraftment potential, albeit hindered by low yield.142 Ultimately, preconditioned MSC-derived exosomes warrant further investigation and development.
Fecal Microbiota Transplantation
Several pilot studies have evaluated the safety, feasibility, and efficacy of fecal microbiota transplantation (FMT) in patients with refractory CD. However, the safety data for FMT in CD are limited due to the absence of long-term follow-up studies. Furthermore, the lack of RCTs hinders confirmation of these findings, and data on maintenance therapy are also scarce.143 Additionally, the ideal donor characteristics of stool and the optimal route of administration as well as engraftment remain unclear.144–146 A recent systematic review and meta-analysis investigating the efficacy of FMT in inducing remission among patients with CD encompassed 11 non-comparative cohort studies and 1 non-placebo controlled randomized trial, involving a total of 228 patients.147 The results revealed that FMT led to a reduction in CDAI scores within 4 to 8 weeks post-treatment, with consistent decreases also observed in biochemical outcomes in studies reporting them. A Cochrane review published in 2023 assessed the effectiveness and safety of FMT for inducing and maintaining remission in CD.143 However, none of the included studies reported data on the use of FMT for inducing remission in CD. For the maintenance of remission, only one study was available, which reported very uncertain evidence regarding the use of FMT.148 Additionally, serious adverse events were reported, but the data lacked specificity in terms of event breakdown between the FMT and control groups. Therefore, no definitive conclusion could be drawn about the risk of serious adverse events associated with FMT in CD patients. In terms of safety, FMT for indications such as recurrent Clostridioides difficile infection is generally considered safe and well-tolerated, with most short-term adverse effects being mild.149 However, although rare, serious adverse events have been reported, including the transmission of infections like multi-drug-resistant organisms from donor stool. These risks can be mitigated through careful and rigorous donor screening. Table 4 provides a comprehensive summary of selected studies investigating FMT in the management of refractory luminal CD.
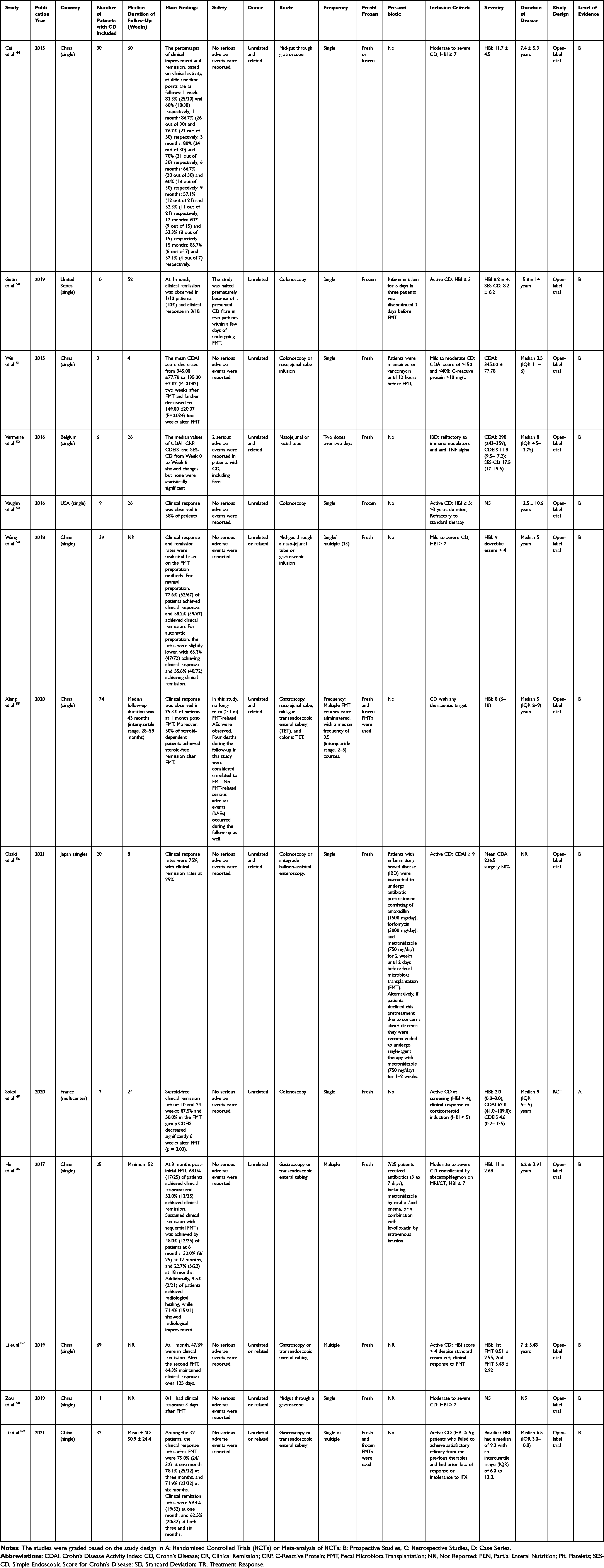 |
Table 4 Description of Selected Studies for FMT of Refractory Luminal Crohn’s Disease |
In conclusion, FMT holds promise as a potential treatment for refractory CD, yet further placebo-controlled trials are imperative to substantiate its efficacy, especially focusing on endoscopic parameters. Additionally, uncertainties persist regarding optimal donor characteristics, administration routes, and engraftment, highlighting the need for comprehensive research to elucidate these aspects and optimize FMT’s therapeutic potential in CD management.
Immunomodulators
Calcineurin-Inhibitors
Tacrolimus and cyclosporine are calcineurin inhibitors, constituting the cornerstone of immunosuppressive therapy in organ transplantation.160,161 They exert their effect by binding to intracellular proteins, primarily cyclophilin in the case of cyclosporine and FKBP12 in the case of tacrolimus. This complex formation inhibits calcineurin, a phosphatase enzyme crucial for T-lymphocyte activation. By blocking calcineurin, these medications downregulate the IL-2 pathway, thereby suppressing T-cell proliferation and cytokine production, leading to overall immune system inhibition.
RCTs assessing the effectiveness of oral or intravenous tacrolimus in luminal CD are currently unavailable. A systematic review conducted in 2011 summarized six studies investigating the role of tacrolimus in luminal refractory CD. Among these studies, complete remission was achieved in 31 patients (44.3%, range 7–69%), while partial response was observed in 26 patients (37.1%, range 14–57%).162 However, several important questions regarding the long-term efficacy of tacrolimus remain unanswered due to the absence of RCTs. More studies are needed in this regard.
A Cochrane review published in 2005 assessed the efficacy of oral cyclosporine for inducing remission in active CD.163 While a study by Brynskov in 1989 found statistically significant clinical improvement with high-dose cyclosporine (7.6 mg/kg/day) at 12 weeks compared to placebo, other trials using low-dose cyclosporine (5 mg/kg/day) alone or in combination with corticosteroids did not demonstrate significant benefits. Cyclosporine treatment was associated with a higher incidence of adverse events and withdrawals due to adverse events compared to placebo. Overall, low-dose oral cyclosporine was not found to be effective for inducing remission in CD and was instead found to lead to adverse effects, including renal dysfunction. Higher doses or parenteral administration have not been sufficiently evaluated in controlled trials.
As such, while calcineurin inhibitors offer a therapeutic avenue, their use in CD warrants careful consideration, with a preference for alternative interventions supported by stronger evidence and a better safety profile. Further research, particularly RCTs assessing long-term efficacy and safety, is essential for establishing their role in the management of CD.
Thalidomide
Thalidomide, originally introduced for its sedative properties, was withdrawn from the market in 1961 due to severe teratogenic effects, notably phocomelia.164,165 However, in recent years, it has been repurposed as a potent anti-inflammatory and immunosuppressive agent, demonstrating efficacy in conditions like erythema nodosum leprosum, sarcoidosis, Behcet syndrome as well as recurrent bleeding due to small-intestinal angiodysplasia.166–170 Thalidomide’s mechanism involves shifting the immune response from Th1 to Th2, inhibiting TNF-α, IFN-γ, and IL-12 while stimulating IL-4 and IL-5, and blocking NF-κB activation.171
Prior research, including a RCT in children and adolescents, has supported thalidomide’s ability to induce clinical remission in refractory CD.172 Although mainly documented in open-label trials and retrospective studies, thalidomide’s efficacy has been noted in refractory CD cases where biological agents failed or were unsuitable.173–176
Despite its potential, thalidomide is known for its adverse effects, including peripheral neuropathy.177,178 However, a recent double-blind RCTs has demonstrated promising results: patients treated with thalidomide showed significantly higher clinical remission rates, as described by the CDAI index at 8th week of treatment, compared to placebo recipients, with subsequent treatment extension for responders.179 Adverse events, though prevalent, were predominantly mild and tolerable.
Similarly, a retrospective study evaluated the combination of thalidomide with azathioprine in CD patients unresponsive to azathioprine alone.180 The combination therapy resulted in positive clinical outcomes, with 70.5% of patients (86 individuals) achieving clinical remission by week 24. However, during follow-up, 22.4% (22 out of 98) of the patients who continued with the combination therapy experienced a clinical relapse. Notably, adverse events were reported but rarely led to therapy discontinuation.
Conclusively, although thalidomide offers a potential solution for refractory CD, clinicians must carefully balance its benefits with its well-documented adverse effects, necessitating vigilant patient monitoring and thoughtful consideration of alternative therapies. While current guidelines do not endorse its widespread use due to the limited quality of available data, it may be a viable option, especially in regions with limited access to biologic therapies and resources.
Dietary Treatments
Exclusive Enteral Nutrition
Exclusive enteral nutrition (EEN) represents an intensive dietary intervention wherein individuals rely solely on commercially available oral liquid meal replacements for their entire caloric intake, typically over a 6- to 8-week period.181–184 EEN is predominantly administered orally and is commonly initiated in pediatric patients with CD as a first-line, steroid-sparing therapy, demonstrating clinical remission rates comparable to corticosteroids (approximately 60% to 80%).183 While less frequently prescribed for adult patients with CD, several studies suggest that EEN, when tolerated, may effectively induce clinical and biochemical remission and provide an effective bridge to safer interval elective surgery.185 However, challenges in trial recruitment and poor adherence to the EEN regimen contribute to the scarcity of definitive data in adults. Efficacy of EEN is influenced by product fatigue, which adults may find particularly challenging in group settings where food consumption occurs. Although the exact therapeutic mechanism of EEN success remains undefined, hypothesized factors include its potential modulatory effect on the microbiome.186
A Cochrane review published in 2019 included 27 studies involving 1011 participants to assess the efficacy of enteral nutritional therapy for induction of remission in CD.187 Overall, the evidence suggested that corticosteroid therapy was more effective than EEN for inducing clinical remission in adults with active CD, even though the data was rated as very low quality. Protein composition did not seem to influence the effectiveness of EEN. However, treatment failures in EEN trials were often due to poor compliance, with common adverse events including nausea, vomiting, diarrhea, and bloating. Recently a real-world, multicenter retrospective study was published regarding the effectiveness of combining biologic treatment with 16 weeks of EEN compared to that of biologics alone in patients with ileum-dominant CD.188 Of the patients included, approximately 70% of patients exhibited either structuring or fistulizing disease and 40% had previously undergone anti-TNF treatment. The results indicated that the treatment combination led to significantly higher rates of clinical response, clinical remission, endoscopic response, and mucosal healing at both week 16 and week 52 compared to biologics alone.
EEN has shown promise in the treatment of CD. However, compliance remains a significant challenge with EN, with many patients withdrawing due to poor palatability and side effects. Future research should focus on improving the palatability of EN formulations and increasing adherence to therapy. Additionally, the optimal route of administration and composition of EN formulations warrant further investigation. For further insight into the various approaches to dietetic therapy in refractory luminal CD, please refer to Table 5.
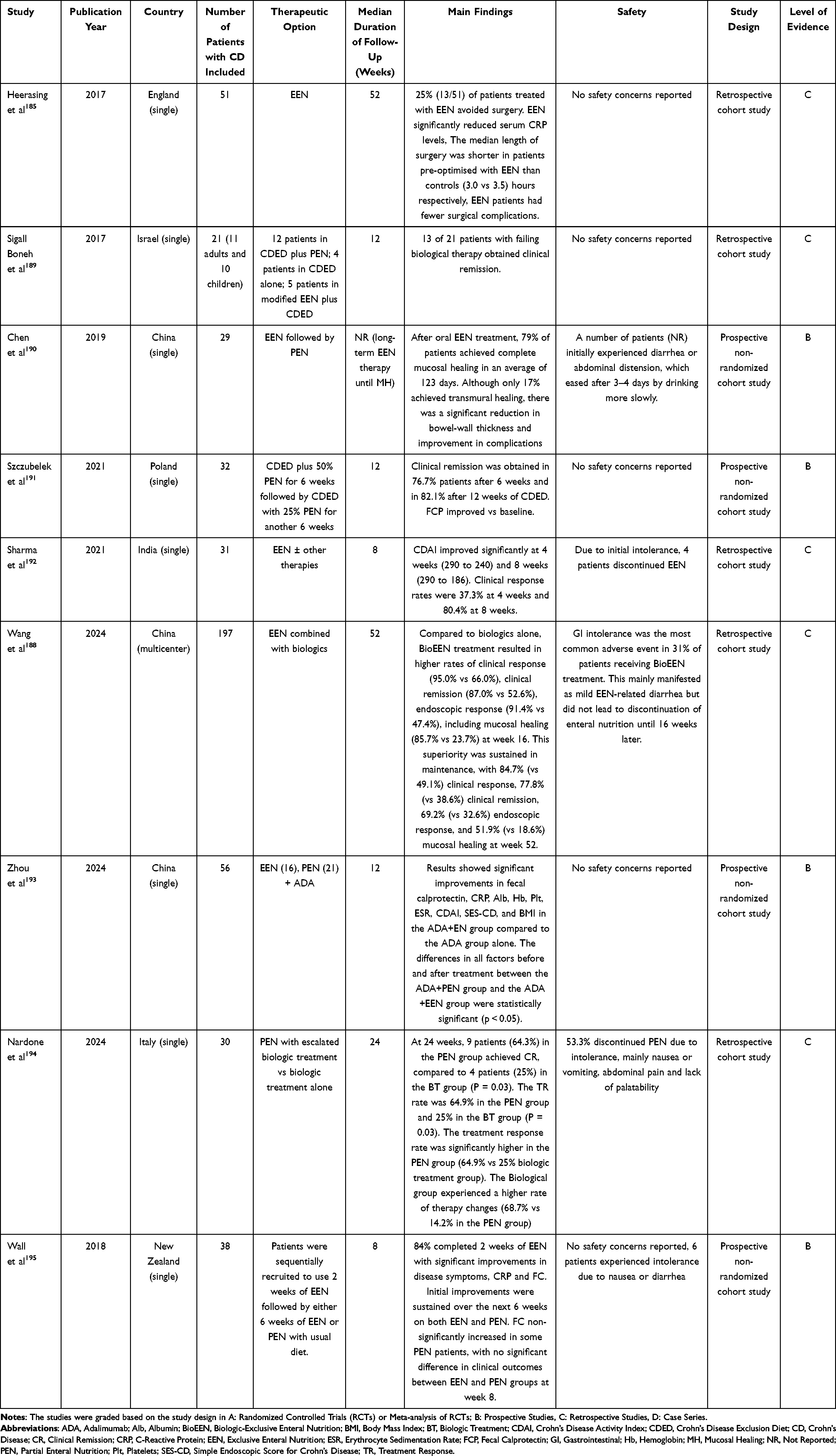 |
Table 5 Description of Selected Studies for Dietetic Therapy of Refractory Luminal Crohn’s Disease |
Crohn’s Disease Exclusion Diet
The CDED is a dietary approach combining partial enteral nutrition (PEN) with specific food components, initially developed for children and later explored in adults with mild to moderate CD.196 It involves three phases, gradually introducing select foods while maintaining PEN supplementation. A recent pilot study demonstrated that CDED, with or without PEN, induced clinical remission in 63% of adult patients at week six, with 50% maintaining remission at week 24.197 Endoscopic remission was achieved in 35% of patients by week 24, with better sustained remission and weight gain observed in the CDED + PEN group compared to CDED alone. Although not adequately powered, the combination of CDED + PEN has shown effectiveness in adult CD patients, including those unresponsive to biologic therapy. Additional studies support its efficacy, with one study reporting clinical remission rates of 76.7% after 12 weeks of therapy.191 The combination of CDED + PEN has shown effectiveness in a small cohort of adult patients with CD who did not respond to biologic therapy with anti-TNFs despite dose adjustments: 13 out of 21 (61.9%) achieved clinical remission within six weeks of treatment.189 In a prospective study in Poland involving 32 adult patients with CD with active disease, clinical remission was achieved in 76.7% after six weeks and 82.1% after 12 weeks of therapy, with significant improvement in fecal calprotectin levels by week 12 compared to baseline.191 Additionally, a case report documented the successful use of CDED + PEN as the sole therapy in a pregnant woman diagnosed with CD from week 14 of gestation until after delivery.198
Despite promising results, caution is warranted in employing restrictive diets, particularly in pregnant women, necessitating close medical monitoring.
Further research is needed to validate these findings and elucidate the optimal use of CDED in adult CD management.
Partial Enteral Nutrition
The limitations of conventional therapies could potentially be addressed by PEN, which allows patients to consume a portion of selected foods daily, potentially enhancing both therapeutic tolerance and overall quality of life. However, research on the efficacy of PEN for inducing remission in CD is limited, with sparse evidence available, mainly recommending it for maintenance therapy. Nevertheless, systematic reviews comparing PEN with EEN show comparable results, with both therapies demonstrating high response rates and clinical remission.199 These findings contrast with earlier randomized clinical trials, such as that conducted by Jonhson et al in 2011 which reported lower remission rates in the PEN group compared to EEN.200 Several factors, including concurrent corticosteroid use or dietary variations, may have influenced these results. Conversely, Nardone et al published a pilot study investigating the efficacy of PEN as an adjunct to escalated biological therapy in adults with refractory CD.194 Results showed that PEN combined with escalated biologics led to higher rates of clinical remission and response compared to escalated therapy alone. Additionally, PEN was associated with improved nutritional status.
Additional research is required to establish the role of dietary interventions as a supplementary treatment in individuals with refractory CD.
Optimizing Current Medical Treatments for Refractory Perianal Fistulizing CD
In CD, the progression of transmural inflammation can lead to the development of adhesions, transmural fissures, intra-abdominal abscesses, and fistula tracts. The risk of fistula formation in patients with CD ranges from 14% to 38%, with a high likelihood of abscesses and fistulae in the anus, particularly in those with proctitis, in which this percentage reaches 90%.201,202 Up to 40% of cases have already developed fistulae by the time of diagnosis, causing significant morbidity and impacting quality of life.203–205 Perianal fistulae are an aggressive disease phenotype and need a multidisciplinary approach.206 Despite advances in treatment, the recurrent disease affects up to two-thirds of patients, sometimes necessitating fecal diversion when medical and local surgical management fails, and approximately 20% of patients may require proctectomy with a permanent colostomy.207–210 Refractory perianal fistulizing CD was defined by the 2021 ECCO topic review on refractory IBD as the lack of response to at least one surgical intervention and anti-TNF therapy.21
As CD follows a chronic course, addressing this complication becomes progressively more complex over time, especially following unsuccessful surgical interventions. While various treatments have been evaluated, only immunomodulators and anti-TNFs have demonstrated apparent efficacy. Traditional anti-inflammatory drugs such as aminosalicylates or corticosteroids have shown low effectiveness and high recurrence rates in perianal fistulizing CD. Corticosteroids alone are associated with a high recurrence rate post-treatment. Immunomodulators often require combination therapy, while infliximab stands out as the only TNF inhibitor proven effective for treating fistulizing CD.211 A recent meta-analysis by Shehab demonstrated the efficacy of TNF antagonists in inducing response and remission in fistulizing disease, with infliximab showing superiority over adalimumab in response induction.212 Adalimumab has demonstrated superiority over placebo in a post-hoc analysis for fistula healing after 56 weeks of treatment.213 As for certolizumab pegol, in the PRECiSE 3 study investigating fistulizing CD, clinical advancements were noted in a restricted subset of patients with perianal fistulas. By the 26th week, 36% of individuals who had previously drained fistulas in the certolizumab pegol group achieved complete fistula closure, contrasting with 17% of those on placebo. However, subsequent trials have not consistently reproduced these findings concerning certolizumab pegol, especially in perianal fistulizing disease.214 Additionally, while some small uncontrolled trials in the 2010s reported promising results with local injections of infliximab and adalimumab in refractory complex perianal fistulae in CD, with reported healing rates around 70–80%, subsequent studies have not consistently replicated these findings.215 Guidelines recommend considering alternative anti-TNF therapies or optimizing current ones if there is a loss of response in refractory CD.37
This section will describe potential medical treatments for refractory perianal CD. Refer to Table 6 for an overview of selected studies examining medical therapy for refractory perianal CD. It is essential to evaluate and consider these options in collaboration with surgeons, as the management of this complication requires multidisciplinary care.
 |
Table 6 Description of Selected Studies for Medical Therapy of Refractory Perianal Crohn’s Disease |
Antibiotics
Antibiotics lack robust clinical support from high-quality evidence. Indeed, in a single RCT with three arms, 25 patients with active draining perianal fistula were assigned to receive ciprofloxacin, metronidazole, or placebo for ten weeks.299 Neither ciprofloxacin nor metronidazole demonstrated superior efficacy compared to placebo in achieving complete fistula closure. However, cohort studies report that antibiotics could help improve clinical symptoms in this patient category.211,299 Further studies are necessary to draw any conclusion on the effectiveness of antibiotics in this setting.
Biologic Drugs
Ustekinumab
Ustekinumab, an IL12/23 inhibitor, is currently undergoing an RCT to evaluate its’ efficacy in this patient’s population. The Ustekinumab in Fistulizing Perianal CD (USTAP) trial, sponsored by GETAID (NCT04496063) is now active.
Induction outcomes for fistulizing CD were evaluated in a post-hoc analysis of the UNITI-1 and UNITI-2 trials.300 24% of patients treated with ustekinumab achieved a fistula response compared to 15.6% of those on placebo, with no statistically significant difference observed. Similarly, ustekinumab did not demonstrate superiority over placebo for inducing fistula remission. Regarding maintenance of fistula response, a subgroup analysis from the IM-UNITI and CERTIFI-M studies revealed that ustekinumab was associated with a significantly higher fistula response rate (58.8%) compared to placebo (26.8%). Within a subset of patients presenting fistulas in the SEAVUE trial, which compared ustekinumab and adalimumab for initiating and maintaining in biologic-naïve individuals with moderately to severely active CD, no statistically notable distinction was observed between the two treatments in preserving fistula remission.301 Moreover, in a subset investigation derived from the STARDUST trial, patients with moderate-to-severe CD who were biologic-naïve or had previously failed biologic therapy been administered ustekinumab intravenously at approximately 6mg/kg at baseline followed by subcutaneous ustekinumab at 90mg at week 8. By week 16, patients were randomized to receive maintenance therapy following either standard care or a treat-to-target approach, with dosage being modulated according to SES-CD scores. Approximately 47.4% of patients, encompassing both treatment groups, attained complete resolution of fistulas by week 48.301 On the other hand, the majority of the data is derived from retrospective studies.302 Attauabi et al conducted a meta-analysis encompassing nine studies involving 396 patients with perianal CD treated with ustekinumab. The combined proportions of patients achieving a fistula response were 41%, 40%, and 55% at weeks 8, 24, and 52, respectively. Correspondingly, the pooled proportions for fistula remission were 17%, 18%, and 16.7% at these time points.303
While observational data suggest the potential benefits of ustekinumab in patients unresponsive to anti-TNF agents, the evidence level remains relatively low, emphasizing the anticipation for the results of the USTAP study.
Vedolizumab
Vedolizumab, a fully humanized monoclonal antibody that selectively targets α4β7 integrin, has shown promise as a second or third therapy-line option. A post-hoc analysis of the GEMINI-2 trial evaluated the effectiveness of vedolizumab versus placebo in patients with fistulizing CD.295 28% of vedolizumab-treated patients achieved fistula remission compared to 11% of placebo patients, but this difference was not statistically significant. Similarly, there was no considerable contrast in maintaining fistula remission compared to placebo. In a phase IV, double-blind, RCT called ENTERPRISE trial, a standard dose of vedolizumab was compared with the standard dose plus an additional intravenous infusion at week 10. At week 30, the two dosing regimens had no statistically significant disparity in fistula response or remission.297 A recent meta-analysis of four studies, including two RCTs, two retrospective cohort studies, and almost 200 patients affected by perianal fistulizing CD, found that vedolizumab resulted in complete healing in 27.6% of patients and partial healing in 35%.304 In a comparative study examining the efficacy of biologic therapies in fistulizing CD, Shehab et al analyzed data from 10 RCTs.212 Their findings revealed that ustekinumab was more effective than placebo in inducing response (Odds ratio, 0.48; 95% CI, 0.26–0.860) but not in inducing remission (Odds ratio, 0.50; 95% CI, 0.13–1.93) and vedolizumab did not demonstrate superiority over placebo in inducing remission (Odds ratio, 0.32; 95% CI, 0.04–2.29). Moreover, no significant difference was observed in inducing remission when comparing different biologic therapies. Firm recommendations cannot be made due to limited published data and lack of head-to-head trials comparing different biologic drugs in IBD patients.
Immunosuppressants
In the past, immunomodulators and immunosuppressants were commonly utilized for treating fistulizing CD. Azathioprine and 6-mercaptopurine have been employed in fistula treatment, but data supporting their efficacy are limited. A meta-analysis of five RCTs suggested that thiopurines could effectively induce fistula closure.305 Nevertheless, many patients had to discontinue the therapy due to side effects like allergy, leukopenia, pancreatitis, and nausea. Due to insufficient evidence, ECCO guidelines do not advocate using thiopurines in monotherapy.305
In a 1998 study by Egan et al, seven out of nine patients with fistulizing CD partially responded to intravenous cyclosporine, with four of six maintaining or improving the response during subsequent oral therapy. However, all patients experienced a relapse within 1 to 17 weeks after discontinuing the treatment.306 In a 2002 Spanish study, these findings were not replicated, as the response to intravenous cyclosporine was observed in refractory CD but not in fistulizing/perianal disease.307
Tacrolimus has been utilized as an oral and topical rescue therapy for fistulizing CD. However, give its safety profile and limited tolerability, long-term studies to assess its efficacy and safety are scarce.308–311 A RCT was undertaken to evaluate the effectiveness of topical tacrolimus treatment to address potential systemic adverse effects. Nineteen patients were stratified according to whether they presented with ulcerating (7 patients) or fistulizing (12 patients) CD. Subsequently, they were randomly allocated to receive topical tacrolimus or a placebo for 12 weeks. For individuals with fistulizing disease, topical tacrolimus showed no efficacy.275 In 2011, a systematic review examined eight studies involving 49 patients with perineal CD treated with oral or intravenous tacrolimus. Among patients who received oral tacrolimus, there was a reported partial or complete response rate of 67.4%.162
A study conducted by Plamondon and Kamm and published in 2007 proposed that thalidomide might be effective as a short-to-medium-term treatment for specific patients with refractory luminal and fistulizing CD.276 Out of 11 patients with active fistulizing disease included in this study, nine responded positively to thalidomide treatment, with six experiencing improvements and three achieving remission. Despite its potential efficacy, long-term use of thalidomide was limited due to toxicity issues, including sedation, abdominal pain, leukopenia, and neuropathy.276 A subsequent systematic review conducted in 2016 aimed to describe the efficacy of thalidomide in luminal and fistulizing CD. It included ten studies and 81 patients with fistulizing CD. Despite varying definitions used by different authors, improvement in perianal fistulas was documented in 49 out of 81 patients (60.5%), with closure achieved in 28 out of 81 patients (34.6%).312 A recent systematic review and meta-analysis analyzed pharmacological therapies for fistulizing CD and found that on pooled analysis fistula response but not fistula remission was achieved with immunosuppressants against placebo.313
In conclusion, while immunosuppressants have historically been used in the treatment of fistulizing CD, their efficacy remains uncertain, and their use is often limited by adverse effects.
Combined Medical Therapy
Combined Anti-TNF and Antibiotics
The most common combination includes anti-TNF drugs (such as infliximab and adalimumab) paired with antibiotics (typically ciprofloxacin), outperforming anti-TNF monotherapy. The ADAFI trial demonstrated that combining adalimumab with ciprofloxacin was more effective than adalimumab alone in achieving fistula closure in perianal fistulizing CD.272 After 12 weeks of treatment, the combination therapy resulted in significantly higher rates of clinical response and remission compared to adalimumab monotherapy.272 However, this beneficial effect was not sustained after discontinuation of antibiotic therapy. Similarly, an RCT investigated the efficacy of combining ciprofloxacin with infliximab in treating perianal fistulae in CD.314 In a double-blind placebo-controlled trial, patients received either ciprofloxacin or a placebo for 12 weeks alongside infliximab. The primary endpoint, clinical response defined by fistula reduction, showed a trend favoring the ciprofloxacin group (73% vs 39% in the placebo group), although not statistically significant. However, secondary endpoints such as the Perianal Disease Activity Index score showed significant improvement in the ciprofloxacin group. However, the improvement in fistulas was restricted to the duration of antibiotic use.272
Combining anti-TNF drugs like infliximab and adalimumab with antibiotics, particularly ciprofloxacin, has emerged as a promising approach for treating perianal fistulizing CD. However, the sustained benefit may be limited to the duration of antibiotic therapy.
Combined Anti-TNFs and Immunomodulators
Contrary to previous assumptions, introducing thiopurines after anti-TNF therapies does not seem beneficial. A 2015 meta-analysis based on 11 RCTs found no clear advantage with combined therapy concerning partial or complete fistula closure compared to anti-TNF monotherapy.315 Presently, ECCO guidelines stress the need for further research due to insufficient evidence supporting a definitive recommendation for or against using immunomodulators in this context.37
Dual-Targeted Therapy
Specific clinical trials suggest the potential of utilizing a combined medical approach to address this condition. A small retrospective cohort study examined 22 patients who received treatment with dual biologics, finding that 33% of patients with perianal fistulas experienced fistula healing post-treatment.61 These findings imply that combining two biologics could be an alternative for managing refractory fistulizing CD. Nevertheless, additional research is necessary to validate the efficacy and safety of this approach.
Small Molecules
Utilizing small molecules in treating fistulizing CD remains a topic of debate. A study by Colombel et al explored the efficacy of upadacitinib in patients with CD complicated by fistulas. The group receiving treatment exhibited higher rates of external closure and fistula drainage resolution than the placebo group. Interestingly, the incidence of adverse events was comparable between the upadacitinib and placebo groups.263 Nevertheless, current data is very limited.
Local Mesenchymal Stem Cell Injection
As previously mentioned, there is clear evidence that combining medical and surgical treatments is superior to single medication therapy in achieving fistula closure (53% vs 43%, P < 0.05).316 Additionally, autologous MSC transplantation has emerged as a potential therapy for perianal fistulas in CD alongside traditional methods like fistula drainage and ligation. Administering a MSC preparation into a carefully prepared fistula tract has shown increased rates of fistula healing compared to surgery alone.233,234 The rationale behind these therapies resides in the unique properties of mesenchymal cells, including their potential to differentiate into various mesodermal cell lineages and their ability to modulate immune cell activation, proliferation, differentiation, and maturation, making them promising candidates for therapeutic use.317 These cells can be sourced from adipose tissue or bone marrow or be allogeneic or autologous. A recent meta-analysis incorporating five RCTs reaffirmed the safety and efficacy of MSC treatment in this patient population.211 Patients treated with MSCs exhibited a significant likelihood of remission (odds ratio of 2.06), with consistent findings across studies. Regarding treatment-emergent adverse events, perianal abscesses and proctalgia were commonly reported in trials, with no notable difference compared to the control group. However, in the clinical application of MSCs, determining the optimal dose or injection site remains challenging. Interestingly, in the review, as mentioned earlier, the group receiving 3×107 MSCs demonstrated superior fistula healing compared to the 9×107 MSCs group, possibly due to a lower cell survival rate.
Darvadstrocel consists of 120 million expanded human allogeneic adipose-derived MSCs, which showed great promise in perianal CD. Two Phase III studies analyzing the efficacy and safety of Darvadstrocel have been recently published. In the phase III multi-center ADMIRE-CD study, 212 patients diagnosed with treatment-refractory perianal CD underwent examination under anesthesia with curettage of fistula tracts and surgical closure of their internal openings.233 These patients received two operations, which included the closure of the internal opening and were randomly assigned to receive either a placebo or a single injection of darvadstrocel. The study found that 56% of patients treated with stem cells achieved combined radiological and clinical remission at 52 weeks, defined as closure of external openings and absence of fistula drainage, compared to 39% of those in the control group. Furthermore, extended follow-up indicated that remission rates persisted beyond 104 weeks, with no observed safety concerns.243 The global ADMIRE-CD II phase III study aimed to assess the efficacy and safety of treating complex perianal fistulas in CD.318 Patients were randomized to receive either darvadstrocel or a placebo. The primary endpoint was combined remission at 24 weeks, with secondary endpoints including combined remission at 52 weeks, clinical remission at 24 and 52 weeks, and time to clinical remission at 24 weeks. Overall, darvadstrocel was well tolerated, with a safety profile consistent with previous studies. Although there were no statistically significant differences in remission rates between darvadstrocel and placebo at 24 weeks, a post hoc analysis suggested lower placebo response rates in patients randomized before COVID-19.
Given the limited available data, further trials are warranted to establish optimal dosing and injection sites for MSC therapy in this patient subset. Therefore, more research is needed to define these individuals’ most appropriate treatment approaches.
Hyperbaric Oxygen Therapy
Hyperbaric oxygen therapy (HBOT) shows promising effectiveness in treating perianal CD and enterocutaneous fistulas, as indicated by uncontrolled observational studies and prospective case series. A recent systematic review and metanalysis found that HBOT in luminal and perianal CD resulted in an overall clinical response rate of 75% and a clinical remission rate of 55%, with no major differences observed in sensitivity analyses.319 For rectovaginal fistulas, clinical response occurred in 62.5% of patients and clinical remission in 37.5%. Radiographic assessment revealed significant improvements in fistula tracts, with some studies reporting complete resolution in up to 75% of cases. In enterocutaneous fistulas, the clinical response rate was 85%, with partial closure achieved in 50% of cases. These findings suggest that HBOT may be a valuable adjunctive therapy for fistulizing CD.
Regarding safety, a total of 15% of patients experienced an adverse event to HBOT, none of which were serious, and the majority of which did not impact treatment. Ear barotrauma was the most frequently reported adverse event, occurring in 3% of patients, and was less common than what has been reported in prior studies, possibly as a result of fewer predisposing risk factors (intubation, concomitant cardiovascular disease, head and neck cancers, diabetes, and sinus infections) in patients with IBD compared with non-IBD patients with chronic wounds.320,321
In a study involving 20 patients, treatment with 40 hyperbaric oxygen sessions resulted in marked improvements in clinical outcomes, including decreased scores of perianal disease activity and modified van Assche index.262 Additionally, a substantial proportion of patients achieved clinical response and remission, with many showing inactive perianal disease by week 16. Furthermore, reductions in inflammatory markers such as C-reactive protein and fecal calprotectin levels were observed.
These findings suggest that hyperbaric oxygen therapy holds promise as a therapeutic option for managing perianal fistulas in patients with CD.
Conclusion
Despite advancements in treatment and the biologic era, some patients with CD exhibit inadequate responses to medical therapy. Refractory CD, although rare, poses a formidable challenge in treatment. Despite efforts over the past two decades to discover new drugs, data remain limited, albeit preliminary findings may seem promising. We reviewed the evidence on various treatments for both luminal and perianal CD, including combined therapies, HSCT, FMT, immunomodulators, HBOT and dietary approaches. While the evidence is promising, it remains limited. Further research is imperative to comprehend refractoriness mechanisms and innovate new medicines.
Disclosure
Edoardo Vincenzo Savarino has served as speaker for Abbvie, Agave, AGPharma, Alfasigma, Aurora Pharma, CaDiGroup, Celltrion, Dr Falk, EG Stada Group, Fenix Pharma, Fresenius Kabi, Galapagos, Janssen, JB Pharmaceuticals, Innovamedica/Adacyte, Malesci, MayolyBiohealth, Omega Pharma, Pfizer, Reckitt Benckiser, Sandoz, SILA, Sofar, Takeda, Tillots, Unifarco; has served as a consultant for Abbvie, Agave, Alfasigma, Biogen, Bristol-Myers Squibb, Celltrion, DiademaFarmaceutici, Dr. Falk, Fenix Pharma, Fresenius Kabi, Janssen, JB Pharmaceuticals, Merck & Co, Nestlè, Reckitt Benckiser, Regeneron, Sanofi, SILA, Sofar, Synformulas GmbH, Takeda, Unifarco; he received research support from Pfizer, Reckitt Benckiser, SILA, Sofar, Unifarco, Zeta Farmaceutici. Fabiana Zingone has served as a speaker for EG Stada Group, Fresenius Kabi, Janssen, Pfizer, Takeda, Unifarco, Malesci, and Kedrion and has served as a consultant for Galapagos. Brigida Barberio has served as a speaker for Abbvie, Agave, Alfasigma, AGpharma, Janssen, Lilly, MSD, Pfizer, Sofar, Takeda, and Unifarco. Edoardo Vincenzo Savarino and Brigida Barberio are co-senior authors. The other authors declare no conflict of interest.
References
1. Kaplan GG, Windsor JW. The four epidemiological stages in the global evolution of inflammatory bowel disease. Nat Rev Gastroenterol Hepatol. 2021;18(1):56–66. doi:10.1038/s41575-020-00360-x
2. da Silva Júnior RT, Apolonio JS, de Souza Nascimento JO, et al. Crohn’s disease and clinical management today: how it does? World J Methodol. 2023;13(5):399–413. doi:10.5662/wjm.v13.i5.399
3. Cassol OS, Zabot GP, Saad-Hossne R, Padoin A. Epidemiology of inflammatory bowel diseases in the state of Rio Grande do Sul, Brazil. World J Gastroenterol. 2022;28(30):4174–4181. doi:10.3748/wjg.v28.i30.4174
4. Ng SC, Shi HY, Hamidi N, et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet. 2017;390(10114):2769–2778. doi:10.1016/S0140-6736(17)32448-0
5. Kaplan GG, Bernstein CN, Coward S, et al. The impact of inflammatory bowel disease in Canada 2018: epidemiology. J Can Assoc Gastroenterol. 2019;2(Suppl 1):S6–S16. doi:10.1093/jcag/gwy054
6. Shivashankar R, Tremaine WJ, Harmsen WS, Loftus EV. Incidence and prevalence of Crohn’s disease and ulcerative colitis in Olmsted County, Minnesota from 1970 through 2010. Clin Gastroenterol Hepatol. 2017;15(6):857–863. doi:10.1016/j.cgh.2016.10.039
7. Tsai L, McCurdy JD, Ma C, Jairath V, Singh S. Epidemiology and natural history of perianal Crohn’s disease: a systematic review and meta-analysis of population-based cohorts. Inflamm Bowel Dis. 2021;28(10):1477–1484. doi:10.1093/ibd/izab287
8. Thia KT, Sandborn WJ, Harmsen WS, Zinsmeister AR, Loftus EV. Risk factors associated with progression to intestinal complications of Crohn’s disease in a population-based cohort. Gastroenterology. 2010;139(4):1147–1155. doi:10.1053/j.gastro.2010.06.070
9. Park KT, Ehrlich OG, Allen JI, et al. The cost of inflammatory bowel disease: an initiative from the crohn’s & colitis foundation. Inflamm Bowel Dis. 2020;26(1):1–10. doi:10.1093/ibd/izz104
10. Floyd DN, Langham S, Séverac HC, Levesque BG. The economic and quality-of-life burden of crohn’s disease in Europe and the United States, 2000 to 2013: a systematic review. Dig Dis Sci. 2015;60(2):299–312. doi:10.1007/s10620-014-3368-z
11. Barberio B, Zamani M, Black CJ, Savarino EV, Ford AC. Prevalence of symptoms of anxiety and depression in patients with inflammatory bowel disease: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2021;6(5):359–370. doi:10.1016/S2468-1253(21)00014-5
12. Marinelli C, Savarino E, Inferrera M, et al. Factors Influencing Disability and Quality of Life during Treatment: a Cross-Sectional Study on IBD Patients. Gastroenterol Res Pract. 2019;2019:5354320. doi:10.1155/2019/5354320
13. Bodini G, Giannini EG, De Maria C, et al. Anti-TNF therapy is able to stabilize bowel damage progression in patients with Crohn’s disease. A study performed using the Lémann Index. Dig Liver Dis. 2017;49(2):175–180. doi:10.1016/j.dld.2016.10.014
14. Barberio B, Gracie DJ, Black CJ, Ford AC. Efficacy of biological therapies and small molecules in induction and maintenance of remission in luminal Crohn’s disease: systematic review and network meta-analysis. Gut. 2023;72(2):264–274. doi:10.1136/gutjnl-2022-328052
15. Macaluso FS, Papi C, Orlando A, et al. Use of biologics for the management of Crohn’s disease: IG-IBD clinical guidelines based on the GRADE methodology. Dig Liver Dis. 2023;55(4):442–453. doi:10.1016/j.dld.2023.01.155
16. Degli Esposti L, Daperno M, Dovizio M, et al. A retrospective analysis of treatment patterns, drug discontinuation and healthcare costs in Crohn’s disease patients treated with biologics. Dig Liver Dis. 2023;55(9):1214–1220. doi:10.1016/j.dld.2023.04.010
17. Ardizzone S, Armuzzi A, Caprioli F, et al. Timing of proper introduction, optimization and maintenance of anti-TNF therapy in IBD: results from a Delphi consensus. Dig Liver Dis. 2024;56(1):98–105. doi:10.1016/j.dld.2023.09.003
18. Raine T, Danese S. Breaking through the therapeutic ceiling: what will it take? Gastroenterology. 2022;162(5):1507–1511. doi:10.1053/j.gastro.2021.09.078
19. Sparrow MP, Papamichael K, Ward MG, et al. Therapeutic drug monitoring of biologics during induction to prevent primary non-response. J Crohns Colitis. 2020;14(4):542–556. doi:10.1093/ecco-jcc/jjz162
20. Yanai H, Lichtenstein L, Assa A, et al. Levels of drug and antidrug antibodies are associated with outcome of interventions after loss of response to infliximab or Adalimumab. Clin Gastroenterol Hepatol. 2015;13(3):522–530.e2. doi:10.1016/j.cgh.2014.07.029
21. Raine T, Verstockt B, Kopylov U, et al. ECCO topical review: refractory inflammatory bowel disease. J Crohn’s Colitis. 2021;15(10):1605–1620. doi:10.1093/ecco-jcc/jjab112
22. He Y, Xu P, Zeng Z, et al. P319 the prevalence and clinical characteristics of refractory crohn’s disease in South China. J Crohn’s Colitis. 2014;8(Supplement_1):S197–S198. doi:10.1016/S1873-9946(14)60440-2
23. Goll R, Moe ØK, Johnsen KM, et al. Pharmacodynamic mechanisms behind a refractory state in inflammatory bowel disease. BMC Gastroenterol. 2022;22(1):464. doi:10.1186/s12876-022-02559-5
24. Z E, K B, Ob K, et al. Development of the Harvey-Bradshaw Index-pro (HBI-PRO) score to assess endoscopic disease activity in crohn’s disease. J Crohn’s Colitis. 2017;11(5). doi:10.1093/ecco-jcc/jjw200
25. Shah SC, Colombel JF, Sands BE, Narula N. Systematic review with meta-analysis: mucosal healing is associated with improved long-term outcomes in Crohn’s disease. Aliment Pharmacol Ther. 2016;43(3):317–333. doi:10.1111/apt.13475
26. Rohatinsky N, Zelinsky S, Dolinger M, et al. Crohn’s disease patient experiences and preferences with disease monitoring: an international qualitative study. Crohn’s & Colitis. 2023;5(2):otad012. doi:10.1093/crocol/otad012
27. Halpin SJ, Ford AC. Prevalence of symptoms meeting criteria for irritable bowel syndrome in inflammatory bowel disease: systematic review and meta-analysis. Am J Gastroenterol. 2012;107(10):1474–1482. doi:10.1038/ajg.2012.260
28. Chan W, Chen A, Tiao D, Selinger C, Leong R. Medication adherence in inflammatory bowel disease. Intest Res. 2017;15(4):434–445. doi:10.5217/ir.2017.15.4.434
29. Chapman S, Sibelli A, St-Clair Jones A, Forbes A, Chater A, Horne R. Personalised adherence support for maintenance treatment of inflammatory bowel disease: a tailored digital intervention to change adherence-related beliefs and barriers. J Crohns Colitis. 2020;14(10):1394–1404. doi:10.1093/ecco-jcc/jjz034
30. Jackson CA, Clatworthy J, Robinson A, Horne R. Factors associated with non-adherence to oral medication for inflammatory bowel disease: a systematic review. Am J Gastroenterol. 2010;105(3):525–539. doi:10.1038/ajg.2009.685
31. Papamichael K, Afif W, Drobne D, et al. Therapeutic drug monitoring of biologics in inflammatory bowel disease: unmet needs and future perspectives. Lancet Gastroenterol Hepatol. 2022;7(2):171–185. doi:10.1016/S2468-1253(21)00223-5
32. Irving PM, Gecse KB. Optimizing therapies using therapeutic drug monitoring: current strategies and future perspectives. Gastroenterology. 2022;162(5):1512–1524. doi:10.1053/j.gastro.2022.02.014
33. Lopez A, Billioud V, Peyrin-Biroulet C, Peyrin-Biroulet L. Adherence to anti-TNF therapy in inflammatory bowel diseases: a systematic review. Inflamm Bowel Dis. 2013;19(7):1528–1533. doi:10.1097/MIB.0b013e31828132cb
34. Papamichael K, Clarke WT, Vande Casteele N, et al. Comparison of assays for therapeutic monitoring of infliximab and adalimumab in patients with inflammatory bowel diseases. Clin Gastroenterol Hepatol. 2021;19(4):839–841.e2. doi:10.1016/j.cgh.2020.03.002
35. Vermeire S, Dreesen E, Papamichael K, Dubinsky MC. How, when, and for whom should we perform therapeutic drug monitoring? Clin Gastroenterol Hepatol. 2020;18(6):1291–1299. doi:10.1016/j.cgh.2019.09.041
36. Hindryckx P, Novak G, Vande Casteele N, et al. Review article: dose optimisation of infliximab for acute severe ulcerative colitis. Aliment Pharmacol Ther. 2017;45(5):617–630. doi:10.1111/apt.13913
37. Torres J, Bonovas S, Doherty G, et al. ECCO guidelines on therapeutics in crohn’s disease: medical treatment. J Crohns Colitis. 2020;14(1):4–22. doi:10.1093/ecco-jcc/jjz180
38. Barberio B, Zingone F, D’Incà R, et al. Infliximab originator, infliximab biosimilar, and adalimumab are more effective in crohn’s disease than ulcerative colitis: a real-life cohort study. Clin Transl Gastroenterol. 2020;11(5):e00177. doi:10.14309/ctg.0000000000000177
39. Cingolani L, Barberio B, Zingone F, et al. Adalimumab biosimilars, ABP501 and SB5, are equally effective and safe as adalimumab originator. Sci Rep. 2021;11(1):10368. doi:10.1038/s41598-021-89790-4
40. Loftus EV, Panés J, Lacerda AP, et al. Upadacitinib Induction and Maintenance Therapy for Crohn’s Disease. N Engl J Med. 2023;388(21):1966–1980. doi:10.1056/NEJMoa2212728
41. Privitera G, Pugliese D, Lopetuso LR, et al. Novel trends with biologics in inflammatory bowel disease: sequential and combined approaches. Therap Adv Gastroenterol. 2021;14:17562848211006669. doi:10.1177/17562848211006669
42. Turner D, Ricciuto A, Lewis A, et al. STRIDE-II: an update on the selecting therapeutic targets in inflammatory bowel disease (STRIDE) initiative of the international organization for the study of IBD (IOIBD): determining therapeutic goals for treat-to-target strategies in IBD. Gastroenterology. 2021;160(5):1570–1583. doi:10.1053/j.gastro.2020.12.031
43. Fumery M, Peyrin-Biroulet L, Nancey S, et al. Effectiveness and safety of ustekinumab intensification at 90 mg every four weeks in crohn’s disease: a multicenter study. J Crohns Colitis. 2020:jjaa177. doi:10.1093/ecco-jcc/jjaa177
44. Meserve J, Ma C, Dulai PS, Jairath V, Singh S. Effectiveness of reinduction and/or dose escalation of ustekinumab in crohn’s disease: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2022;20(12):2728–2740.e1. doi:10.1016/j.cgh.2021.10.002
45. Perry C, Fischer K, Elmoursi A, et al. Vedolizumab dose escalation improves therapeutic response in a subset of patients with ulcerative colitis. Dig Dis Sci. 2021;66(6):2051–2058. doi:10.1007/s10620-020-06486-x
46. Dal Buono A, Gabbiadini R, Migliorisi G, et al. P637 Targeting mucosal healing: dose optimization of Vedolizumab in IBD patients with inadequate endoscopic response to standard dosing. J Crohn’s Colitis. 2023;17(Supplement_1):i769–i770. doi:10.1093/ecco-jcc/jjac190.0767
47. Horst S, Cross RK. Clinical evaluation of risankizumab in the treatment of adults with moderately to severely active crohn’s disease: patient selection and reported outcomes. Drug Des Devel Ther. 2023;17:273–282. doi:10.2147/DDDT.S379446
48. Colombel JF, Sandborn WJ, Reinisch W, et al. Infliximab, azathioprine, or combination therapy for Crohn’s disease. N Engl J Med. 2010;362(15):1383–1395. doi:10.1056/NEJMoa0904492
49. Colombel JF, Adedokun OJ, Gasink C, et al. Combination therapy with infliximab and azathioprine improves infliximab pharmacokinetic features and efficacy: a post hoc analysis. Clin Gastroenterol Hepatol. 2019;17(8):1525–1532.e1. doi:10.1016/j.cgh.2018.09.033
50. Feagan BG, McDonald JWD, Panaccione R, et al. Methotrexate in combination with infliximab is no more effective than infliximab alone in patients with Crohn’s disease. Gastroenterology. 2014;146(3):681–688.e1. doi:10.1053/j.gastro.2013.11.024
51. Noor NM, Lee JC, Bond S, et al. A biomarker-stratified comparison of top-down versus accelerated step-up treatment strategies for patients with newly diagnosed Crohn’s disease (PROFILE): a multicentre, open-label randomised controlled trial. Lancet Gastroenterol Hepatol. 2024;9(5):415–427. doi:10.1016/S2468-1253(24)00034-7
52. Colombel JF, Ungaro RC, Sands BE, et al. Vedolizumab, adalimumab, and methotrexate combination therapy in crohn’s disease (EXPLORER). Clin Gastroenterol Hepatol. 2023. doi:10.1016/j.cgh.2023.09.010
53. Ribaldone DG, Pellicano R, Vernero M, et al. Dual biological therapy with anti-TNF, vedolizumab or ustekinumab in inflammatory bowel disease: a systematic review with pool analysis. Scand J Gastroenterol. 2019;54(4):407–413. doi:10.1080/00365521.2019.1597159
54. Ahmed W, Galati J, Kumar A, et al. Dual biologic or small molecule therapy for treatment of inflammatory bowel disease: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2022;20(3):e361–e379. doi:10.1016/j.cgh.2021.03.034
55. Goessens L, Colombel JF, Outtier A, et al. Safety and efficacy of combining biologics or small molecules for inflammatory bowel disease or immune-mediated inflammatory diseases: a European retrospective observational study. Unit Europ Gastroenterol J. 2021;9(10):1136–1147. doi:10.1002/ueg2.12170
56. Alayo QA, Fenster M, Altayar O, et al. Systematic review with meta-analysis: safety and effectiveness of combining biologics and small molecules in inflammatory bowel disease. Crohns Colitis 360. 2022;4(1):otac002. doi:10.1093/crocol/otac002
57. Privitera G, Onali S, Pugliese D, et al. Dual Targeted Therapy: a possible option for the management of refractory Inflammatory Bowel Disease. J Crohns Colitis. 2020:jjaa149. doi:10.1093/ecco-jcc/jjaa149
58. Mao EJ, Lewin S, Terdiman JP, Beck K. Safety of dual biological therapy in Crohn’s disease: a case series of vedolizumab in combination with other biologics. BMJ Open Gastroenterol. 2018;5(1):e000243. doi:10.1136/bmjgast-2018-000243
59. Kwapisz L, Raffals LE, Bruining DH, et al. Combination Biologic therapy in inflammatory bowel disease: experience from a tertiary care center. Clin Gastroenterol Hepatol. 2021;19(3):616–617. doi:10.1016/j.cgh.2020.02.017
60. Glassner K, Oglat A, Duran A, et al. The use of combination biological or small molecule therapy in inflammatory bowel disease: a retrospective cohort study. J Dig Dis. 2020;21(5):264–271. doi:10.1111/1751-2980.12867
61. Yang E, Panaccione N, Whitmire N, et al. Efficacy and safety of simultaneous treatment with two biologic medications in refractory Crohn’s disease. Aliment Pharmacol Ther. 2020;51(11):1031–1038. doi:10.1111/apt.15719
62. Llano EM, Shrestha S, Burstein E, Boktor M, Fudman DI. Favorable outcomes combining vedolizumab with other biologics or tofacitinib for treatment of inflammatory bowel disease. Crohns Colitis 360. 2021;3(3):otab030. doi:10.1093/crocol/otab030
63. Olbjørn C, Rove JB, Jahnsen J. Combination of biological agents in moderate to severe pediatric inflammatory bowel disease: a case series and review of the literature. Pediatr Drugs. 2020;22(4):409–416. doi:10.1007/s40272-020-00396-1
64. Sandborn WJ, Feagan BG, Rutgeerts P, et al. Vedolizumab as Induction and Maintenance Therapy for Crohn’s Disease. N Engl J Med. 2013;369(8):711–721. doi:10.1056/NEJMoa1215739
65. Sands BE, Kozarek R, Spainhour J, et al. Safety and tolerability of concurrent natalizumab treatment for patients with Crohn’s disease not in remission while receiving infliximab. Inflamm Bowel Dis. 2007;13(1):2–11. doi:10.1002/ibd.20014
66. Sands BE, Feagan BG, Rutgeerts P, et al. Effects of vedolizumab induction therapy for patients with Crohn’s disease in whom tumor necrosis factor antagonist treatment failed. Gastroenterology. 2014;147(3):618–627.e3. doi:10.1053/j.gastro.2014.05.008
67. Shelton E, Allegretti JR, Stevens B, et al. Efficacy of vedolizumab as induction therapy in refractory IBD patients: a multicenter cohort. Inflamm Bowel Dis. 2015;21(12):2879–2885. doi:10.1097/MIB.0000000000000561
68. Baumgart DC, Bokemeyer B, Drabik A, Stallmach A, Schreiber S. Vedolizumab Germany Consortium. Vedolizumab induction therapy for inflammatory bowel disease in clinical practice--a nationwide consecutive German cohort study. Aliment Pharmacol Ther. 2016;43(10):1090–1102. doi:10.1111/apt.13594
69. Stallmach A, Langbein C, Atreya R, et al. Vedolizumab provides clinical benefit over 1 year in patients with active inflammatory bowel disease - a prospective multicenter observational study. Aliment Pharmacol Ther. 2016;44(11–12):1199–1212. doi:10.1111/apt.13813
70. Szántó K, Molnár T, Farkas K. New promising combo therapy in inflammatory bowel diseases refractory to Anti-TNF agents: cyclosporine plus vedolizumab. J Crohn’s Colitis. 2018;12(5):629. doi:10.1093/ecco-jcc/jjx179
71. Eriksson C, Marsal J, Bergemalm D, et al. Long-term effectiveness of vedolizumab in inflammatory bowel disease: a national study based on the Swedish National Quality Registry for Inflammatory Bowel Disease (SWIBREG). Scand J Gastroenterol. 2017;52(6–7):722–729. doi:10.1080/00365521.2017.1304987
72. Samaan MA, Pavlidis P, Johnston E, et al. Vedolizumab: early experience and medium-term outcomes from two UK tertiary IBD centres. Front Gastroenterol. 2017;8(3):196–202. doi:10.1136/flgastro-2016-100720
73. Allegretti JR, Barnes EL, Stevens B, et al. Predictors of clinical response and remission at 1 year among a multicenter cohort of patients with inflammatory bowel disease treated with vedolizumab. Dig Dis Sci. 2017;62(6):1590–1596. doi:10.1007/s10620-017-4549-3
74. Lenti MV, Levison S, Eliadou E, et al. A real-world, long-term experience on effectiveness and safety of vedolizumab in adult patients with inflammatory bowel disease: the cross pennine study. Dig Liver Dis. 2018;50(12):1299–1304. doi:10.1016/j.dld.2018.07.007
75. Shmidt E, Kochhar G, Hartke J, et al. Predictors and management of loss of response to vedolizumab in inflammatory bowel disease. Inflamm Bowel Dis. 2018;24(11):2461–2467. doi:10.1093/ibd/izy171
76. Macaluso FS, Orlando R, Fries W, et al. The real-world effectiveness of vedolizumab on intestinal and articular outcomes in inflammatory bowel diseases. Dig Liver Dis. 2018;50(7):675–681. doi:10.1016/j.dld.2018.02.013
77. Kotze PG, Ma C, Almutairdi A, et al. Real-world clinical, endoscopic and radiographic efficacy of vedolizumab for the treatment of inflammatory bowel disease. Aliment Pharmacol Ther. 2018;48(6):626–637. doi:10.1111/apt.14919
78. Chaparro M, Garre A, Ricart E, et al. Short and long-term effectiveness and safety of vedolizumab in inflammatory bowel disease: results from the ENEIDA registry. Aliment Pharmacol Ther. 2018;48(8):839–851. doi:10.1111/apt.14930
79. Christensen B, Gibson P, Micic D, et al. Effective use of calcineurin inhibitors with vedolizumab in refractory inflammatory bowel disease. Clin Gastroenterol Hepatol. 2019;17(3):486–493. doi:10.1016/j.cgh.2018.04.060
80. Meserve J, Aniwan S, Koliani-Pace JL, et al. Retrospective analysis of safety of vedolizumab in patients with inflammatory bowel diseases. Clin Gastroenterol Hepatol. 2019;17(8):1533–1540.e2. doi:10.1016/j.cgh.2018.09.035
81. Biemans VBC, van der Woude CJ, Dijkstra G, et al. Vedolizumab for inflammatory bowel disease: two-year results of the initiative on crohn and colitis (ICC) Registry, A nationwide prospective observational cohort study: ICC registry - vedolizumab. Clin Pharmacol Ther. 2020;107(5):1189–1199. doi:10.1002/cpt.1712
82. Amiot A, Serrero M, Peyrin-Biroulet L, et al. Three-year effectiveness and safety of vedolizumab therapy for inflammatory bowel disease: a prospective multi-centre cohort study. Aliment Pharmacol Ther. 2019;50(1):40–53. doi:10.1111/apt.15294
83. Verstockt B, Mertens E, Dreesen E, et al. Influence of drug exposure on vedolizumab-induced endoscopic remission in anti-tumour necrosis factor [TNF] Naïve and Anti-TNF Exposed IBD Patients. J Crohn’s Colitis. 2020;14(3):332–341. doi:10.1093/ecco-jcc/jjz151
84. Watanabe K, Motoya S, Ogata H, et al. Effects of vedolizumab in Japanese patients with Crohn’s disease: a prospective, multicenter, randomized, placebo-controlled Phase 3 trial with exploratory analyses. J Gastroenterol. 2020;55(3):291–306. doi:10.1007/s00535-019-01647-w
85. Visuri I, Eriksson C, Karlqvist S, et al. Long-term outcomes of vedolizumab in inflammatory bowel disease: the Swedish prospective multicentre SVEAH extension study. Therap Adv Gastroenterol. 2023;16:175628482311749. doi:10.1177/17562848231174953
86. Eriksson C, Rundquist S, Lykiardopoulos V, et al. Real-world effectiveness of vedolizumab in inflammatory bowel disease: week 52 results from the Swedish prospective multicentre SVEAH study. Therap Adv Gastroenterol. 2021;14:175628482110233. doi:10.1177/17562848211023386
87. Vermeire S, D’Haens G, Baert F, et al. Efficacy and safety of subcutaneous vedolizumab in patients with moderately to severely active crohn’s disease: results from the VISIBLE 2 randomised trial. J Crohn’s Colitis. 2022;16(1):27–38. doi:10.1093/ecco-jcc/jjab133
88. Sandborn WJ, Gasink C, Gao LL, et al. Ustekinumab induction and maintenance therapy in refractory Crohn’s disease. N Engl J Med. 2012;367(16):1519–1528. doi:10.1056/NEJMoa1203572
89. Kopylov U, Afif W, Cohen A, et al. Subcutaneous ustekinumab for the treatment of anti-TNF resistant Crohn’s disease--the McGill experience. J Crohns Colitis. 2014;8(11):1516–1522. doi:10.1016/j.crohns.2014.06.005
90. Wils P, Bouhnik Y, Michetti P, et al. Subcutaneous ustekinumab provides clinical benefit for two-thirds of patients with crohn’s disease refractory to anti-tumor necrosis factor agents. Clin Gastroenterol Hepatol. 2016;14(2):
91. Feagan Brian G, Sandborn William J, Christopher G, et al. Ustekinumab as Induction and Maintenance Therapy for Crohn’s Disease. N Engl J Med. 2016;375(20):1946–1960. doi:10.1056/NEJMoa1602773
92. Battat R, Kopylov U, Bessissow T, et al. Association between ustekinumab trough concentrations and clinical, biomarker, and endoscopic outcomes in patients with crohn’s disease. Clin Gastroenterol Hepatol. 2017;15(9):1427–1434.e2. doi:10.1016/j.cgh.2017.03.032
93. Ma C, Fedorak RN, Kaplan GG, et al. Long-term maintenance of clinical, endoscopic, and radiographic response to ustekinumab in moderate-to-severe crohn’s disease: real-world experience from a multicenter cohort study. Inflamm Bowel Dis. 2017;23(5):833–839. doi:10.1097/MIB.0000000000001074
94. Greenup AJ, Rosenfeld G, Bressler B. Ustekinumab use in Crohn’s disease: a Canadian tertiary care centre experience. Scand J Gastroenterol. 2017;52(12):1354–1359. doi:10.1080/00365521.2017.1373847
95. Liefferinckx C, Verstockt B, Gils A, et al. Long-term clinical effectiveness of ustekinumab in patients with crohn’s disease who failed biologic therapies: a national cohort study. J Crohns Colitis. 2019;13(11):1401–1409. doi:10.1093/ecco-jcc/jjz080
96. Miyazaki T, Watanabe K, Kojima K, et al. Efficacies and related issues of ustekinumab in Japanese patients with crohn’s disease: a preliminary study. Digestion. 2020;101(1):53–59. doi:10.1159/000503959
97. Biemans VBC, van der Meulen-de Jong AE, van der Woude CJ, et al. Ustekinumab for crohn’s disease: results of the ICC registry, a nationwide prospective observational cohort study. J Crohns Colitis. 2020;14(1):33–45. doi:10.1093/ecco-jcc/jjz119
98. Hanauer SB, Sandborn WJ, Feagan BG, et al. IM-UNITI: three-year efficacy, safety, and immunogenicity of ustekinumab treatment of crohn’s disease. J Crohn’s Colitis. 2020;14(1):23–32. doi:10.1093/ecco-jcc/jjz110
99. Buer LCT, Høivik ML, Warren DJ, Medhus AW, Moum BA. Combining Anti-TNF-α and vedolizumab in the treatment of inflammatory bowel disease: a case series. Inflamm Bowel Dis. 2018;24(5):997–1004. doi:10.1093/ibd/izx110
100. Alayo QA, Khatiwada A, Patel A, et al. Effectiveness and safety of combining tofacitinib with a biologic in patients with refractory inflammatory bowel diseases. Inflamm Bowel Dis. 2021;27(10):1698–1702. doi:10.1093/ibd/izab112
101. Lee SD, Singla A, Harper J, et al. Safety and efficacy of tofacitinib in combination with biologic therapy for refractory crohn’s disease. Inflamm Bowel Dis. 2022;28(2):309–313. doi:10.1093/ibd/izab176
102. Eronen H, Kolehmainen S, Koffert J, et al. Combining biological therapies in patients with inflammatory bowel disease: a Finnish multi-centre study. Scand J Gastroenterol. 2022;57(8):936–941. doi:10.1080/00365521.2022.2045350
103. Miyatani Y, Choi D, Choi NK, Rubin DT. Dual-targeted therapy with upadacitinib and ustekinumab in medically complex crohn’s disease. Dig Dis Sci. 2024;69(2):355–359. doi:10.1007/s10620-023-08182-y
104. Klein OR, Bonfim C, Abraham A, et al. Transplant for non-malignant disorders: an international society for cell & gene therapy stem cell engineering committee report on the role of alternative donors, stem cell sources and graft engineering. Cytotherapy. 2023;25(5):463–471. doi:10.1016/j.jcyt.2022.12.005
105. Drakos PE, Nagler A, Or R. Case of Crohn’s disease in bone marrow transplantation. Am J Hematol. 1993;43(2):157–158. doi:10.1002/ajh.2830430223
106. Kashyap A, Forman SJ. Autologous bone marrow transplantation for non-Hodgkin’s lymphoma resulting in long-term remission of coincidental Crohn’s disease. Br J Haematol. 1998;103(3):651–652. doi:10.1046/j.1365-2141.1998.01059.x
107. Ditschkowski M, Einsele H, Schwerdtfeger R, et al. Improvement of inflammatory bowel disease after allogeneic stem-cell transplantation. Transplantation. 2003;75(10):1745–1747. doi:10.1097/01.TP.0000062540.29757.E9
108. Hawkey CJ, Allez M, Clark MM, et al. Autologous hematopoetic stem cell transplantation for refractory crohn disease: a randomized clinical trial. JAMA. 2015;314(23):2524–2534. doi:10.1001/jama.2015.16700
109. Lindsay JO, Allez M, Clark M, et al. Autologous stem-cell transplantation in treatment-refractory Crohn’s disease: an analysis of pooled data from the ASTIC trial. Lancet Gastroenterol Hepatol. 2017;2(6):399–406. doi:10.1016/S2468-1253(17)30056-0
110. López-García A, Rovira M, Jauregui-Amezaga A, et al. Autologous haematopoietic stem cell transplantation for refractory crohn’s disease: efficacy in a single-centre cohort. J Crohns Colitis. 2017;11(10):1161–1168. doi:10.1093/ecco-jcc/jjx054
111. Burt RK, Craig R, Yun L, et al. A pilot feasibility study of non-myeloablative allogeneic hematopoietic stem cell transplantation for refractory Crohn Disease. Bone Marrow Transplant. 2020;55(12):2343–2346. doi:10.1038/s41409-020-0953-y
112. Brierley CK, Castilla-Llorente C, Labopin M, et al. Autologous haematopoietic stem cell transplantation for crohn’s disease: a retrospective survey of long-term outcomes from the European society for blood and marrow transplantation. J Crohns Colitis. 2018;12(9):1097–1103. doi:10.1093/ecco-jcc/jjy069
113. Berro M, Arbelbide JA, Rivas MM, et al. Hematopoietic cell transplantation-specific comorbidity index predicts morbidity and mortality in autologous stem cell transplantation. Biol Blood Marrow Transplant. 2017;23(10):1646–1650. doi:10.1016/j.bbmt.2017.06.014
114. Lindsay JO, Hind D, Swaby L, et al. Safety and efficacy of autologous haematopoietic stem-cell transplantation with low-dose cyclophosphamide mobilisation and reduced intensity conditioning versus standard of care in refractory Crohn’s disease (ASTIClite): an open-label, multicentre, randomised controlled trial. Lancet Gastroenterol Hepatol. 2024;9(4):333–345. doi:10.1016/S2468-1253(23)00460-0
115. Mohty B, Mohty M. Long-term complications and side effects after allogeneic hematopoietic stem cell transplantation: an update. Blood Cancer J. 2011;1(4):e16–e16. doi:10.1038/bcj.2011.14
116. Ko JZ, Johnson S, Dave M. Efficacy and safety of mesenchymal stem/stromal cell therapy for inflammatory bowel diseases: an up-to-date systematic review. Biomolecules. 2021;11(1):82. doi:10.3390/biom11010082
117. Jasim SA, Yumashev AV, Abdelbasset WK, et al. Shining the light on clinical application of mesenchymal stem cell therapy in autoimmune diseases. Stem Cell Res Ther. 2022;13(1):101. doi:10.1186/s13287-022-02782-7
118. Vieujean S, Loly JP, Boutaffala L, et al. Mesenchymal stem cell injection in crohn’s disease strictures: a phase I-II clinical study. J Crohns Colitis. 2022;16(3):506–510. doi:10.1093/ecco-jcc/jjab154
119. Dave M, Dev A, Somoza RA, et al. MSCs mediate long-term efficacy in a Crohn’s disease model by sustained anti-inflammatory macrophage programming via efferocytosis. npj Regen Med. 2024;9(1):1–16. doi:10.1038/s41536-024-00347-1
120. Dhere T, Copland I, Garcia M, et al. The safety of autologous and metabolically fit bone marrow mesenchymal stromal cells in medically refractory Crohn’s disease - a phase 1 trial with three doses. Aliment Pharmacol Ther. 2016;44(5):471–481. doi:10.1111/apt.13717
121. Duijvestein M, Vos ACW, Roelofs H, et al. Autologous bone marrow-derived mesenchymal stromal cell treatment for refractory luminal Crohn’s disease: results of a phase I study. Gut. 2010;59(12):1662–1669. doi:10.1136/gut.2010.215152
122. Liang J, Zhang H, Wang D, et al. Allogeneic mesenchymal stem cell transplantation in seven patients with refractory inflammatory bowel disease. Gut. 2012;61(3):468–469. doi:10.1136/gutjnl-2011-300083
123. Zhang J, Lv S, Liu X, Song B, Shi L. Umbilical cord mesenchymal stem cell treatment for crohn’s disease: a randomized controlled clinical trial. Gut Liver. 2018;12(1):73–78. doi:10.5009/gnl17035
124. Forbes GM, Sturm MJ, Leong RW, et al. A phase 2 study of allogeneic mesenchymal stromal cells for luminal Crohn’s disease refractory to biologic therapy. Clin Gastroenterol Hepatol. 2014;12(1):64–71. doi:10.1016/j.cgh.2013.06.021
125. Gregoire C, Briquet A, Pirenne C, Lechanteur C, Louis E, Beguin Y. Allogeneic mesenchymal stromal cells for refractory luminal Crohn’s disease: a phase I-II study. Dig Liver Dis. 2018;50(11):1251–1255. doi:10.1016/j.dld.2018.08.015
126. Cheng F, Huang Z, Li Z. Mesenchymal stem-cell therapy for perianal fistulas in Crohn’s disease: a systematic review and meta-analysis. Tech Coloproctol. 2019;23(7):613–623. doi:10.1007/s10151-019-02024-8
127. Melmed GY, Pandak WM, Casey K, et al. Human Placenta-derived Cells (PDA-001) for the treatment of moderate-to-severe crohn’s disease: a phase 1b/2a study. Inflamm Bowel Dis. 2015;21(8):1809–1816. doi:10.1097/MIB.0000000000000441
128. Wang R, Yao Q, Chen W, et al. Stem cell therapy for Crohn’s disease: systematic review and meta-analysis of preclinical and clinical studies. Stem Cell Res Ther. 2021;12(1):463. doi:10.1186/s13287-021-02533-0
129. Burt RK, Traynor A, Oyama Y, Craig R. High-dose immune suppression and autologous hematopoietic stem cell transplantation in refractory Crohn disease. Blood. 2003;101(5):2064–2066. doi:10.1182/blood-2002-07-2122
130. Craig RM, Traynor A, Oyama Y, Burt RK. Hematopoietic stem cell transplantation for severe Crohn’s disease. Bone Marrow Transplant. 2003;32(Suppl 1):S57–59. doi:10.1038/sj.bmt.1703945
131. Oyama Y, Craig RM, Traynor AE, et al. Autologous hematopoietic stem cell transplantation in patients with refractory Crohn’s disease. Gastroenterology. 2005;128(3):552–563. doi:10.1053/j.gastro.2004.11.051
132. Cassinotti A, Annaloro C, Ardizzone S, et al. Autologous haematopoietic stem cell transplantation without CD34+ cell selection in refractory Crohn’s disease. Gut. 2008;57(2):211–217. doi:10.1136/gut.2007.128694
133. Burt RK, Craig RM, Milanetti F, et al. Autologous nonmyeloablative hematopoietic stem cell transplantation in patients with severe anti-TNF refractory Crohn disease: long-term follow-up. Blood. 2010;116(26):6123–6132. doi:10.1182/blood-2010-06-292391
134. Clerici M, Cassinotti A, Onida F, et al. Immunomodulatory effects of unselected haematopoietic stem cells autotransplantation in refractory Crohn’s disease. Digestive Liver Dis. 2011;43(12):946–952. doi:10.1016/j.dld.2011.07.021
135. Hommes DW, Duijvestein M, Zelinkova Z, et al. Long-term follow-up of autologous hematopoietic stem cell transplantation for severe refractory Crohn’s disease. J Crohns Colitis. 2011;5(6):543–549. doi:10.1016/j.crohns.2011.05.004
136. Hasselblatt P, Drognitz K, Potthoff K, et al. Remission of refractory Crohn’s disease by high-dose cyclophosphamide and autologous peripheral blood stem cell transplantation. Aliment Pharmacol Ther. 2012;36(8):725–735. doi:10.1111/apt.12032
137. Mayer EA, Knight R, Mazmanian SK, Cryan JF, Tillisch K. Gut microbes and the brain: paradigm shift in neuroscience. J Neurosci. 2014;34(46):15490–15496. doi:10.1523/JNEUROSCI.3299-14.2014
138. Snowden JA, Ansari A, Sachchithanantham S, et al. Autologous stem cell transplantation in severe treatment-resistant Crohn’s disease: long-term follow-up of UK patients treated on compassionate basis. QJM. 2014;107(11):871–877. doi:10.1093/qjmed/hcu095
139. Ruiz MA, Kaiser RL, de Quadros LG, et al. Low toxicity and favorable clinical and quality of life impact after non-myeloablative autologous hematopoietic stem cell transplant in Crohn’s disease. BMC Res Notes. 2017;10(1):495. doi:10.1186/s13104-017-2824-1
140. Hernanz N, Sierra M, Volpato N, et al. Autologous haematopoietic stem cell transplantation in refractory Crohn’s disease: experience in our centre. Gastroenterol Hepatol. 2019;42(1):16–22. doi:10.1016/j.gastre.2019.01.013
141. El-Nakeep S, Shawky A, Abbas SF, Latif OA. Stem cell transplantation for induction of remission in medically refractory Crohn’s disease. Cochrane Database Syst Rev. 2022;(5). doi:10.1002/14651858.CD013070.pub2
142. Li X, Wang Q, Ding L, et al. Intercellular adhesion molecule-1 enhances the therapeutic effects of MSCs in a dextran sulfate sodium-induced colitis models by promoting MSCs homing to murine colons and spleens. Stem Cell Res Ther. 2019;10:267. doi:10.1186/s13287-019-1384-9
143. Imdad A, Pandit NG, Zaman M, et al. Fecal transplantation for treatment of inflammatory bowel disease. Cochrane Database Syst Rev. 2023;(4). doi:10.1002/14651858.CD012774.pub3
144. Cui B, Feng Q, Wang H, et al. Fecal microbiota transplantation through mid-gut for refractory Crohn’s disease: safety, feasibility, and efficacy trial results. J Gastroenterol Hepatol. 2015;30(1):51–58. doi:10.1111/jgh.12727
145. Suskind DL, Brittnacher MJ, Wahbeh G, et al. Fecal microbial transplant effect on clinical outcomes and fecal microbiome in active Crohn’s disease. Inflamm Bowel Dis. 2015;21(3):556–563. doi:10.1097/MIB.0000000000000307
146. He Z, Li P, Zhu J, et al. Multiple fresh fecal microbiota transplants induces and maintains clinical remission in Crohn’s disease complicated with inflammatory mass. Sci Rep. 2017;7(1):4753. doi:10.1038/s41598-017-04984-z
147. Zhou S, Cui Y, Zhang Y, Zhao T, Cong J. Fecal microbiota transplantation for induction of remission in Crohn’s disease: a systematic review and meta-analysis. Int J Colorectal Dis. 2023;38(1):62. doi:10.1007/s00384-023-04354-4
148. Sokol H, Landman C, Seksik P, et al. Fecal microbiota transplantation to maintain remission in Crohn’s disease: a pilot randomized controlled study. Microbiome. 2020;8(1):12. doi:10.1186/s40168-020-0792-5
149. Park SY, Seo GS. Fecal Microbiota Transplantation: is It Safe? Clin Endosc. 2021;54(2):157–160. doi:10.5946/ce.2021.072
150. Gutin L, Piceno Y, Fadrosh D, et al. Fecal microbiota transplant for Crohn disease: a study evaluating safety, efficacy, and microbiome profile. Unit Europ Gastroenterol J. 2019;7(6):807–814. doi:10.1177/2050640619845986
151. Wei Y, Zhu W, Gong J, et al. Fecal microbiota transplantation improves the quality of life in patients with inflammatory bowel disease. Gastroenterol Res Pract. 2015;2015:1–5. doi:10.1155/2015/517597
152. Vermeire S, Joossens M, Verbeke K, et al. Donor species richness determines faecal microbiota transplantation success in inflammatory bowel disease. J Crohns Colitis. 2016;10(4):387–394. doi:10.1093/ecco-jcc/jjv203
153. Vaughn BP, Vatanen T, Allegretti JR, et al. Increased intestinal microbial diversity following fecal microbiota transplant for active crohn’s disease. Inflamm Bowel Dis. 2016;22(9):2182–2190. doi:10.1097/MIB.0000000000000893
154. Wang H, Cui B, Li Q, et al. The safety of fecal microbiota transplantation for crohn’s disease: findings from a long-term study. Adv Ther. 2018;35(11):1935–1944. doi:10.1007/s12325-018-0800-3
155. Xiang L, Ding X, Li Q, et al. Efficacy of faecal microbiota transplantation in Crohn’s disease: a new target treatment? Microb Biotechnol. 2020;13(3):760–769. doi:10.1111/1751-7915.13536
156. Osaki H, Jodai Y, Koyama K, et al. Clinical response and changes in the fecal microbiota and metabolite levels after fecal microbiota transplantation in patients with inflammatory bowel disease and recurrent Clostridioides difficile infection. Fujita Med J. 2021;7(3):87–98. doi:10.20407/fmj.2020-021
157. Li P, Zhang T, Xiao Y, et al. Timing for the second fecal microbiota transplantation to maintain the long-term benefit from the first treatment for Crohn’s disease. Appl Microbiol Biotechnol. 2019;103(1):349–360. doi:10.1007/s00253-018-9447-x
158. Zou M, Jie Z, Cui B, et al. Fecal microbiota transplantation results in bacterial strain displacement in patients with inflammatory bowel diseases. FEBS Open Bio. 2020;10(1):41–55. doi:10.1002/2211-5463.12744
159. Li Q, Ding X, Liu Y, et al. Fecal microbiota transplantation is a promising switch therapy for patients with prior failure of infliximab in crohn’s disease. Front Pharmacol. 2021;12:658087. doi:10.3389/fphar.2021.658087
160. Schutte-Nutgen K, Tholking G, Suwelack B, Reuter S. Tacrolimus - Pharmacokinetic Considerations for Clinicians. Curr Drug Metab. 2018;19(4):342–350. doi:10.2174/1389200219666180101104159
161. Matsuda S, Koyasu S. Mechanisms of action of cyclosporine. Immunopharmacology. 2000;47(2–3):119–125. doi:10.1016/s0162-3109(00)00192-2
162. McSharry K, Dalzell AM, Leiper K, El-Matary W. Systematic review: the role of tacrolimus in the management of Crohn’s disease. Aliment Pharmacol Ther. 2011;34(11–12):1282–1294. doi:10.1111/j.1365-2036.2011.04873.x
163. McDonald JW, Feagan BG, Jewell DP, Brynskov J, Stange EF, MacDonald JK. Cyclosporine for induction of remission in Crohn’s disease. Cochrane Database Syst Rev. 2005;(2). doi:10.1002/14651858.CD000297.pub2
164. Ng SC. Thalidomide and refractory Crohn’s disease: what is in the future? J Clin Gastroenterol. 2014;48(6):476–477. doi:10.1097/MCG.0000000000000136
165. Bousvaros A. Thalidomide treatment of pediatric ulcerative colitis: a new use for an old drug. Inflamm Bowel Dis. 2015;21(8):1750–1751. doi:10.1097/MIB.0000000000000430
166. Wettstein AR, Meagher AP, Meagher AP. Thalidomide in Crohn’s disease. Lancet. 1997;350(9089):1445–1446. doi:10.1016/s0140-6736(05)64206-7
167. Jorizzo JL, Schmalstieg FC, Solomon AR, et al. Thalidomide effects in Behçet’s syndrome and pustular vasculitis. Arch Intern Med. 1986;146(5):878–881. doi:10.1001/archinte.1986.00360170074012
168. Rousseau L, Beylot-Barry M, Doutre MS, Beylot C. Cutaneous sarcoidosis successfully treated with low doses of thalidomide. Arch Dermatol. 1998;134(8):1045–1046. doi:10.1001/archderm.134.8.1045
169. Duong DJ, Spigel GT, Moxley RT, Gaspari AA. American experience with low-dose thalidomide therapy for severe cutaneous lupus erythematosus. Arch Dermatol. 1999;135(9):1079–1087. doi:10.1001/archderm.135.9.1079
170. Huimin C, Shan W, Mingyu T, et al. Thalidomide for recurrent bleeding due to small-intestinal angiodysplasia. N Engl J Med. 2023;389(18):1649–1659. doi:10.1056/NEJMoa2303706
171. Yang C, Singh P, Singh H, Le ML, El-Matary W. Systematic review: thalidomide and thalidomide analogues for treatment of inflammatory bowel disease. Aliment Pharmacol Ther. 2015;41(11):1079–1093. doi:10.1111/apt.13181
172. Lazzerini M, Martelossi S, Magazzù G, et al. Effect of thalidomide on clinical remission in children and adolescents with refractory Crohn disease: a randomized clinical trial. JAMA. 2013;310(20):2164–2173. doi:10.1001/jama.2013.280777
173. Vasiliauskas EA, Kam LY, Abreu-Martin MT, et al. An open-label pilot study of low-dose thalidomide in chronically active, steroid-dependent Crohn’s disease. Gastroenterology. 1999;117(6):1278–1287. doi:10.1016/s0016-5085(99)70277-5
174. Ehrenpreis ED, Kane SV, Cohen LB, Cohen RD, Hanauer SB. Thalidomide therapy for patients with refractory Crohn’s disease: an open-label trial. Gastroenterology. 1999;117(6):1271–1277. doi:10.1016/s0016-5085(99)70276-3
175. Gerich ME, Yoon JL, Targan SR, Ippoliti AF, Vasiliauskas EA. Long-term outcomes of thalidomide in refractory Crohn’s disease. Aliment Pharmacol Ther. 2015;41(5):429–437. doi:10.1111/apt.13057
176. Sabate JM, Villarejo J, Lemann M, Bonnet J, Allez M, Modigliani R. An open-label study of thalidomide for maintenance therapy in responders to infliximab in chronically active and fistulizing refractory Crohn’s disease. Aliment Pharmacol Ther. 2002;16(6):1117–1124. doi:10.1046/j.1365-2036.2002.01273.x
177. Ginsburg PM, Dassopoulos T, Ehrenpreis ED. Thalidomide treatment for refractory Crohn’s disease: a review of the history, pharmacological mechanisms and clinical literature. Ann Med. 2001;33(8):516–525. doi:10.3109/07853890108995961
178. Ghobrial IM, Rajkumar SV. Management of thalidomide toxicity. J Support Oncol. 2003;1(3):194–205.
179. Peng X, Lin ZW, Zhang M, et al. The efficacy and safety of thalidomide in the treatment of refractory Crohn’s disease in adults: a double-center, double-blind, randomized-controlled trial. Gastroenterol Rep. 2022;10:goac052. doi:10.1093/gastro/goac052
180. Li T, Qiu Y, Li X, et al. Thalidomide combined with azathioprine as induction and maintenance therapy for azathioprine-refractory crohn’s disease patients. Front M Ed. 2020;7:557986. doi:10.3389/fmed.2020.557986
181. Forbes A, Escher J, Hébuterne X, et al. ESPEN guideline: clinical nutrition in inflammatory bowel disease. Clin Nutr. 2017;36(2):321–347. doi:10.1016/j.clnu.2016.12.027
182. Lamb CA, Kennedy NA, Raine T, et al. British society of gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut. 2019;68(Suppl 3):s1–s106. doi:10.1136/gutjnl-2019-318484
183. Whitten KE, Rogers P, Ooi CY (Keith), Day AS. International survey of enteral nutrition protocols used in children with Crohn’s disease. J Digest Dis. 2012;13(2):107–112. doi:10.1111/j.1751-2980.2011.00558.x
184. Hashash JG, Elkins J, Lewis JD, Binion DG. AGA clinical practice update on diet and nutritional therapies in patients with inflammatory bowel disease: expert review. Gastroenterology. 2024;166(3):521–532. doi:10.1053/j.gastro.2023.11.303
185. Heerasing N, Thompson B, Hendy P, et al. Exclusive enteral nutrition provides an effective bridge to safer interval elective surgery for adults with Crohn’s disease. Aliment Pharmacol Ther. 2017;45(5):660–669. doi:10.1111/apt.13934
186. Geesala R, Recharla N, Zhang K, et al. Exclusive enteral nutrition beneficially modulates gut microbiome in a preclinical model of crohn’s-like colitis. Nutrients. 2024;16(3):363. doi:10.3390/nu16030363
187. Narula N, Dhillon A, Zhang D, Sherlock ME, Tondeur M, Zachos M. Enteral nutritional therapy for induction of remission in Crohn’s disease. Cochrane Database Syst Rev. 2018;2018(4). doi:10.1002/14651858.CD000542.pub3
188. Wang W, Yin A, Wang J, et al. Real-world evidence of combined treatment of biologics and exclusive enteral nutrition in patients with ileum-dominant Crohn’s disease: a multicenter study. Clin Nutr. 2024;43(6):1291–1298. doi:10.1016/j.clnu.2024.04.013
189. Sigall Boneh R, Sarbagili Shabat C, Yanai H, et al. Dietary therapy with the crohn’s disease exclusion diet is a successful strategy for induction of remission in children and adults failing biological therapy. J Crohn’s Colitis. 2017;11(10):1205–1212. doi:10.1093/ecco-jcc/jjx071
190. Chen JM, He LW, Yan T, et al. Oral exclusive enteral nutrition induces mucosal and transmural healing in patients with Crohn’s disease. Gastroenterol Rep. 2019;7(3):176–184. doi:10.1093/gastro/goy050
191. Szczubełek M, Pomorska K, Korólczyk-Kowalczyk M, Lewandowski K, Kaniewska M, Rydzewska G. Effectiveness of crohn’s disease exclusion diet for induction of remission in crohn’s disease adult patients. Nutrients. 2021;13(11):4112. doi:10.3390/nu13114112
192. Sharma S, Gupta A, Kedia S, et al. Efficacy and tolerability of exclusive enteral nutrition in adult patients with complicated Crohn’s disease. Intest Res. 2021;19(3):291–300. doi:10.5217/ir.2019.09172
193. Zhou S, Huang Z, Hou W, Lin Y, Yu J. Prospective study of an Adalimumab combined with partial enteral nutrition in the induction period of Crohn’s disease. Inflamm Res. 2024;73(2):199–209. doi:10.1007/s00011-023-01828-7
194. Nardone OM, Calabrese G, La Mantia A, et al. Effectiveness of partial enteral nutrition as add-on to biologics in patients with refractory and difficult-to-treat crohn’s disease: a pilot study. Crohn’s & Colitis. 2024;6(1):otae011. doi:10.1093/crocol/otae011
195. Wall CL, Gearry RB, Day AS. Treatment of active crohn’s disease with exclusive and partial enteral nutrition: a pilot study in adults. Inflamm Intest Dis. 2018;2(4):219–227. doi:10.1159/000489630
196. Yanai H, Levine A, Hirsch A, et al. The Crohn’s disease exclusion diet for induction and maintenance of remission in adults with mild-to-moderate Crohn’s disease (CDED-AD): an open-label, pilot, randomised trial. Lancet Gastroenterol Hepatol. 2022;7(1):49–59. doi:10.1016/S2468-1253(21)00299-5
197. Levine A, Wine E, Assa A, et al. Crohn’s Disease Exclusion Diet Plus Partial Enteral Nutrition Induces Sustained Remission in a Randomized Controlled Trial. Gastroenterology. 2019;157(2):440–450.e8. doi:10.1053/j.gastro.2019.04.021
198. Ukovic B, Chapman B, Schulberg J, De Cruz P, Choy MC. Novel use of the crohn’s disease exclusion diet plus partial enteral nutrition for the treatment of crohn’s disease during pregnancy. ACG Case Rep J. 2023;10(7):e01078. doi:10.14309/crj.0000000000001078
199. González-Torres L, Moreno-álvarez A, Fernández-Lorenzo AE, Leis R, Solar-Boga A. The role of partial enteral nutrition for induction of remission in crohn’s disease: a systematic review of controlled trials. Nutrients. 2022;14(24):5263. doi:10.3390/nu14245263
200. Johnson T, Macdonald S, Hill SM, Thomas A, Murphy MS. Treatment of active Crohn’s disease in children using partial enteral nutrition with liquid formula: a randomised controlled trial. Gut. 2006;55(3):356–361. doi:10.1136/gut.2004.062554
201. Wasmann KA, de Groof EJ, Stellingwerf ME, et al. Treatment of perianal fistulas in crohn’s disease, seton versus anti-TNF versus surgical closure following Anti-TNF [PISA]: a randomised controlled trial. J Crohns Colitis. 2020;14(8):1049–1056. doi:10.1093/ecco-jcc/jjaa004
202. Peyrin-Biroulet L, Loftus EV, Colombel JF, Sandborn WJ. The natural history of adult Crohn’s disease in population-based cohorts. Am J Gastroenterol. 2010;105(2):289–297. doi:10.1038/ajg.2009.579
203. Schwartz DA, Loftus EV, Tremaine WJ, et al. The natural history of fistulizing Crohn’s disease in Olmsted County, Minnesota. Gastroenterology. 2002;122(4):875–880. doi:10.1053/gast.2002.32362
204. Boudiaf R, Bouchard D, Rivière P, et al. Assessment of sexual dysfunction in patients with perianal Crohn’s disease. Colorectal Dis. 2021;23(1):114–122. doi:10.1111/codi.15375
205. Mahadev S, Young JM, Selby W, Solomon MJ. Self-reported depressive symptoms and suicidal feelings in perianal Crohn’s disease. Colorectal Dis. 2012;14(3):331–335. doi:10.1111/j.1463-1318.2011.02613.x
206. van Praag EMM, Becker MAJ, van Rijn KL, et al. Short-term anti-TNF therapy with surgical closure versus anti-TNF therapy alone for Crohn’s perianal fistulas (PISA-II): long-term outcomes of an international, multicentre patient preference, randomised controlled trial. eClinicalMedicine. 2023;61. doi:10.1016/j.eclinm.2023.102045
207. Wolff BG, Culp CE, Beart RW, Ilstrup DM, Roger MS, Ready L. Anorectal Crohn’s disease. Dis Colon Rectum. 1985;28(10):709–711. doi:10.1007/BF02560279
208. Steele SR, Kumar R, Feingold DL, Rafferty JL, Buie WD. Practice parameters for the management of perianal abscess and fistula-in-ano. Dis Colon Rectum. 2011;54(12):1465. doi:10.1097/DCR.0b013e31823122b3
209. Yamamoto T, Shimoyama T. Fecal diversion in complex perianal fistulizing crohn’s disease. Clin Colon Rectal Surg. 2022;35(1):5–9. doi:10.1055/s-0041-1740028
210. Molendijk I, Nuij VJ, van der Meulen-de Jong AE, van der Woude CJ. Disappointing durable remission rates in complex Crohn’s disease fistula. Inflamm Bowel Dis. 2014;20(11):2022–2028. doi:10.1097/MIB.0000000000000148
211. Li A, Liu S, Li L, Yu M. Mesenchymal stem cells versus placebo for perianal fistulizing crohn’s disease: a systemic review and meta-analysis. surgical Innovation. 2023;30(3):398–405. doi:10.1177/15533506231157167
212. Shehab M, Alrashed F, Heron V, Restellini S, Bessissow T. Comparative efficacy of biologic therapies for inducing response and remission in fistulizing crohn’s disease: systematic review and network meta-analysis of randomized controlled trials. Inflammat Bowel Dis. 2023;29(3):367–375. doi:10.1093/ibd/izac103
213. Colombel JF, Schwartz DA, Sandborn WJ, et al. Adalimumab for the treatment of fistulas in patients with Crohn’s disease. Gut. 2009;58(7):940–948. doi:10.1136/gut.2008.159251
214. Schreiber S. Certolizumab pegol for the treatment of Crohn’s disease. Therap Adv Gastroenterol. 2011;4(6):375–389. doi:10.1177/1756283X11413315
215. Alessandroni L, Kohn A, Cosintino R, et al. Local injection of infliximab in severe fistulating perianal Crohn’s disease: an open uncontrolled study. Tech Coloproctol. 2011;15(4):407–412. doi:10.1007/s10151-011-0759-4
216. García-Olmo D, García-Arranz M, Herreros D, Pascual I, Peiro C, Rodríguez-Montes JA. A phase I clinical trial of the treatment of Crohn’s fistula by adipose mesenchymal stem cell transplantation. Dis Colon Rectum. 2005;48(7):1416–1423. doi:10.1007/s10350-005-0052-6
217. Garcia-Olmo D, Herreros D, Pascual I, et al. Expanded adipose-derived stem cells for the treatment of complex perianal fistula: a phase II clinical trial. Dis Colon Rectum. 2009;52(1):79–86. doi:10.1007/DCR.0b013e3181973487
218. Ciccocioppo R, Bernardo ME, Sgarella A, et al. Autologous bone marrow-derived mesenchymal stromal cells in the treatment of fistulising Crohn’s disease. Gut. 2011;60(6):788–798. doi:10.1136/gut.2010.214841
219. Herreros MD, Garcia-Arranz M, Guadalajara H, De-La-Quintana P, Garcia-Olmo D; FATT Collaborative Group. Autologous expanded adipose-derived stem cells for the treatment of complex cryptoglandular perianal fistulas: a phase III randomized clinical trial (FATT 1: fistula Advanced Therapy Trial 1) and long-term evaluation. Dis Colon Rectum. 2012;55(7):762–772. doi:10.1097/DCR.0b013e318255364a
220. Guadalajara H, Herreros D, De-La-Quintana P, Trebol J, Garcia-Arranz M, Garcia-Olmo D. Long-term follow-up of patients undergoing adipose-derived adult stem cell administration to treat complex perianal fistulas. Int J Colorectal Dis. 2012;27(5):595–600. doi:10.1007/s00384-011-1350-1
221. Cho YB, Lee WY, Park KJ, Kim M, Yoo HW, Yu CS. Autologous adipose tissue-derived stem cells for the treatment of Crohn’s fistula: a phase I clinical study. Cell Transplant. 2013;22(2):279–285. doi:10.3727/096368912X656045
222. Lee WY, Park KJ, Cho YB, et al. Autologous adipose tissue-derived stem cells treatment demonstrated favorable and sustainable therapeutic effect for Crohn’s fistula. Stem Cells. 2013;31(11):2575–2581. doi:10.1002/stem.1357
223. Choi S, Ryoo SB, Park KJ, et al. Autologous adipose tissue-derived stem cells for the treatment of complex perianal fistulas not associated with Crohn’s disease: a phase II clinical trial for safety and efficacy. Tech Coloproctol. 2017;21(5):345–353. doi:10.1007/s10151-017-1630-z
224. de la Portilla F, Alba F, García-Olmo D, Herrerías JM, González FX, Galindo A. Expanded allogeneic adipose-derived stem cells (eASCs) for the treatment of complex perianal fistula in Crohn’s disease: results from a multicenter phase I/IIa clinical trial. Int J Colorectal Dis. 2013;28(3):313–323. doi:10.1007/s00384-012-1581-9
225. Molendijk I, Bonsing BA, Roelofs H, et al. Allogeneic bone marrow-derived mesenchymal stromal cells promote healing of refractory perianal fistulas in patients with crohn’s disease. Gastroenterology. 2015;149(4):918–927.e6. doi:10.1053/j.gastro.2015.06.014
226. Cho YB, Park KJ, Yoon SN, et al. Long-term results of adipose-derived stem cell therapy for the treatment of Crohn’s fistula. Stem Cells Transl Med. 2015;4(5):532–537. doi:10.5966/sctm.2014-0199
227. Park KJ, Ryoo SB, Kim JS, et al. Allogeneic adipose-derived stem cells for the treatment of perianal fistula in Crohn’s disease: a pilot clinical trial. Colorectal Dis. 2016;18(5):468–476. doi:10.1111/codi.13223
228. Ciccocioppo R, Gallia A, Sgarella A, Kruzliak P, Gobbi PG, Corazza GR. Long-term follow-up of crohn disease fistulas after local injections of bone marrow-derived mesenchymal stem cells. Mayo Clin Proc. 2015;90(6):747–755. doi:10.1016/j.mayocp.2015.03.023
229. Wainstein C, Quera R, Kronberg U, et al. Mesenchymal stem cells and platelet-rich plasma in the treatment of patients with perineal Crohn’s disease. Int J Colorectal Dis. 2016;31(3):725–726. doi:10.1007/s00384-015-2221-y
230. García-Arranz M, Herreros MD, González-Gómez C, et al. Treatment of crohn’s-related rectovaginal fistula with allogeneic expanded-adipose derived stem cells: a phase I-IIa clinical trial. Stem Cells Transl Med. 2016;5(11):1441–1446. doi:10.5966/sctm.2015-0356
231. Dietz AB, Dozois EJ, Fletcher JG, et al. Autologous mesenchymal stem cells, applied in a bioabsorbable matrix, for treatment of perianal fistulas in patients with crohn’s disease. Gastroenterology. 2017;153(1):59–62.e2. doi:10.1053/j.gastro.2017.04.001
232. Serrero M, Philandrianos C, Visee C, et al. OP008 An innovative treatment for refractory perianal fistulas in Crohn’s disease: local micro reinjection of autologous fat and adipose derived stromal vascular fraction. J Crohn’s Colitis. 2017;11(suppl_1):S5. doi:10.1093/ecco-jcc/jjx002.007
233. Panés J, García-Olmo D, Van Assche G, et al. Expanded allogeneic adipose-derived mesenchymal stem cells (Cx601) for complex perianal fistulas in Crohn’s disease: a phase 3 randomised, double-blind controlled trial. Lancet. 2016;388(10051):1281–1290. doi:10.1016/S0140-6736(16)31203-X
234. Panés J, García-Olmo D, Van Assche G, et al. Long-term efficacy and safety of stem cell therapy (Cx601) for complex perianal fistulas in patients with crohn’s disease. Gastroenterology. 2018;154(5):1334–1342.e4. doi:10.1053/j.gastro.2017.12.020
235. Dozois EJ, Lightner AL, Mathis KL, et al. Early results of a phase i trial using an adipose-derived mesenchymal stem cell-coated fistula plug for the treatment of transsphincteric cryptoglandular fistulas. Dis Colon Rectum. 2019;62(5):615–622. doi:10.1097/DCR.0000000000001333
236. Herreros MD, Garcia-Olmo D, Guadalajara H, Georgiev-Hristov T, Brandariz L, Garcia-Arranz M. Stem cell therapy: a compassionate use program in perianal fistula. Stem Cells Int. 2019;2019:6132340. doi:10.1155/2019/6132340
237. Dige A, Hougaard HT, Agnholt J, et al. Efficacy of injection of freshly collected autologous adipose tissue into perianal fistulas in patients with crohn’s disease. Gastroenterology. 2019;156(8):2208–2216.e1. doi:10.1053/j.gastro.2019.02.005
238. Barnhoorn MC, Wasser MNJM, Roelofs H, et al. Long-term evaluation of allogeneic bone marrow-derived mesenchymal stromal cell therapy for crohn’s disease perianal fistulas. J Crohns Colitis. 2020;14(1):64–70. doi:10.1093/ecco-jcc/jjz116
239. Zhou C, Li M, Zhang Y, et al. Autologous adipose-derived stem cells for the treatment of Crohn’s fistula-in-ano: an open-label, controlled trial. Stem Cell Res Ther. 2020;11(1):124. doi:10.1186/s13287-020-01636-4
240. Schwandner O. Stem cell injection for complex anal fistula in Crohn’s disease: a single-center experience. World J Gastroenterol. 2021;27(24):3643–3653. doi:10.3748/wjg.v27.i24.3643
241. Cabalzar-Wondberg D, Turina M, Biedermann L, Rogler G, Schreiner P. Allogeneic expanded adipose-derived mesenchymal stem cell therapy for perianal fistulas in Crohn’s disease: a case series. Colorectal Dis. 2021;23(6):1444–1450. doi:10.1111/codi.15587
242. Maciel Gutiérrez VM, Gutiérrez Guillen SG, Centeno Flores MW, et al. Safety of allogeneic adipose tissue-derived mesenchymal stem cells for the treatment of complex perianal fistulas not associated with crohn’s disease: a phase i clinical trial. Dis Colon Rectum. 2021;64(3):328–334. doi:10.1097/DCR.0000000000001863
243. Panés J, Bouma G, Ferrante M, et al. INSPECT: a retrospective study to evaluate long-term effectiveness and safety of darvadstrocel in patients with perianal fistulizing crohn’s disease treated in the ADMIRE-CD trial. Inflamm Bowel Dis. 2022;28(11):1737–1745. doi:10.1093/ibd/izab361
244. Colombo F, Cammarata F, Baldi C, et al. Stem cell injection for complex refractory perianal fistulas in crohn’s disease: a single center initial experience. Front Surg. 2022;9:834870. doi:10.3389/fsurg.2022.834870
245. Garcia-Olmo D, Gilaberte I, Binek M, et al. Follow-up study to evaluate the long-term safety and efficacy of darvadstrocel (mesenchymal stem cell treatment) in patients with perianal fistulizing crohn’s disease: ADMIRE-CD phase 3 randomized controlled trial. Dis Colon Rectum. 2022;65(5):713–720. doi:10.1097/DCR.0000000000002325
246. Guillo L, Grimaud F, Houser F, et al. Three-year outcome of local injection of autologous stromal vascular fraction cells and microfat in refractory perianal fistulas of Crohn’s disease. Stem Cell Res Ther. 2022;13(1):67. doi:10.1186/s13287-022-02738-x
247. Vosough M, Nikfam S, Torabi SH, et al. Mesenchymal stromal cell therapy improves refractory perianal fistula in crohn’s disease: case series clinical interventional study. Cell J. 2022;24(2):62–68. doi:10.22074/cellj.2022.7981
248. Furukawa S, Mizushima T, Nakaya R, et al. Darvadstrocel for complex perianal fistulas in japanese adults with crohn’s disease: a phase 3 study. J Crohns Colitis. 2023;17(3):369–378. doi:10.1093/ecco-jcc/jjac144
249. White I, Yanai H, Avni I, et al. Mesenchymal stem cell therapy for Crohn’s perianal fistula-a real-world experience. Colorectal Dis. 2024;26(1):102–109. doi:10.1111/codi.16830
250. Reenaers C, Gillard RP, Coimbra C, et al. Clinical and MRI evolution after local injection of bone marrow-derived mesenchymal stem cells in perianal fistulae in crohn’s disease: results from a prospective monocentric study. J Crohns Colitis. 2023;17(5):728–737. doi:10.1093/ecco-jcc/jjac192
251. Fathallah N, Akaffou M, Haouari MA, et al. Deep remission improves the quality of life of patients with Crohn’s disease and anoperineal fistula treated with darvadstrocel: results of a French pilot study. Tech Coloproctol. 2023;27(12):1201–1210. doi:10.1007/s10151-023-02765-7
252. Lightner AL, Reese J, Ream J, et al. A Phase IB/IIA study of ex vivo expanded allogeneic bone marrow-derived mesenchymal stem cells for the treatment of perianal fistulizing crohn’s disease. Dis Colon Rectum. 2023;66(10):1359–1372. doi:10.1097/DCR.0000000000002567
253. Fathallah N, Zmora O, Baumgart DC, et al. DOP66 INSPIRE: preliminary data from an observational post-marketing registry on the effectiveness and safety of darvadstrocel in patients with Crohn’s Disease and complex perianal fistulas. J Crohn’s Colitis. 2024;18(Supplement_1):i192–i194. doi:10.1093/ecco-jcc/jjad212.0106
254. Swaroop S, Vuyyuru SK, Kante B, et al. A phase I/II clinical trial of ex-vivo expanded human bone marrow derived allogeneic mesenchymal stromal cells in adult patients with perianal fistulizing Crohn’s Disease. Stem Cell Res Ther. 2024;15(1):140. doi:10.1186/s13287-024-03746-9
255. Pronk A, Beek KJ, Wildenberg ME, Bemelman WA, Stoker J, Buskens CJ. DOP77 Mesenchymal stem cell therapy for refractory Crohn’s perianal fistulas: a case series. J Crohn’s Colitis. 2024;18(Supplement_1):i216–i216. doi:10.1093/ecco-jcc/jjad212.0117
256. Herreros MD, Ramirez JM, Otero-Piñeiro AM, et al. Use of Darvadstrocel (Allogenic Stem Cell Therapy) for crohn’s fistulas in real clinical practice: the national project to implement mesenchymal stem cell for the treatment of perianal crohn’s fistula (the PRIME Study). Dis Colon Rectum. 2024. doi:10.1097/DCR.0000000000003216
257. Husman J, Wardenga M, Kirk SH, et al. P967 Allogeneic bone marrow-derived mesenchymal stromal cell therapy for complex perianal and rectovaginal fistulas in Crohn´s disease: a retrospective single-centre study. J Crohn’s Colitis. 2024;18(Supplement_1):i1755–i1756. doi:10.1093/ecco-jcc/jjad212.1097
258. Dawoud C, Widmann KM, Czipin S, et al. Efficacy of cx601 (darvadstrocel) for the treatment of perianal fistulizing Crohn’s disease-A prospective nationwide multicenter cohort study. Wien Klin Wochenschr. 2024;136(9–10):289–294. doi:10.1007/s00508-023-02283-4
259. Agrawal G, Borody T, Turner R, Leis S, Campbell J. Combining infliximab, anti-MAP and hyperbaric oxygen therapy for resistant fistulizing Crohn’s disease. Future Sci OA. 2015;1(4):FSO77. doi:10.4155/fso.15.77
260. Feitosa MR, Féres Filho O, Tamaki CM, et al. Adjunctive hyperbaric oxygen therapy promotes successful healing in patients with refractory crohn’s disease. Acta Cir Bras. 2016;31(Suppl 1):19–23. doi:10.1590/S0102-86502016001300005
261. Piotrowicz G, Kowerzanow J, Banaszkiewicz P, Babicki A, Kot J, Rydzewska G. P576 Could the hyperbaric oxygen therapy be an effective adjuvant therapy for fistulising Crohn’s disease? J Crohn’s Colitis. 2017;11(suppl_1):S373–S374. doi:10.1093/ecco-jcc/jjx002.700
262. Lansdorp CA, Gecse KB, Buskens CJ, et al. Hyperbaric oxygen therapy for the treatment of perianal fistulas in 20 patients with Crohn’s disease. Aliment Pharmacol Ther. 2021;53(5):587–597. doi:10.1111/apt.16228
263. Colombel JF, Irving P, Rieder F, et al. P491 Efficacy and safety of upadacitinib for the treatment of fistulas and fissures in patients with Crohn’s disease. Journal of Crohn’s and Colitis. 2023;17(Supplement_1):i620–i623. doi:10.1093/ecco-jcc/jjac190.0621
264. Reinisch W, Colombel JF, D’Haens GR, et al. Efficacy and safety of filgotinib for the treatment of perianal fistulising crohn’s disease [DIVERGENCE 2]: a phase 2, randomised, placebo-controlled trial. J Crohn’s Colitis. 2024:jjae003. doi:10.1093/ecco-jcc/jjae003
265. Present DH, Rutgeerts P, Targan S, et al. Infliximab for the treatment of fistulas in patients with Crohn’s disease. N Engl J Med. 1999;340(18):1398–1405. doi:10.1056/NEJM199905063401804
266. West RL, van der Woude CJ, Hansen BE, et al. Clinical and endosonographic effect of ciprofloxacin on the treatment of perianal fistulae in Crohn’s disease with infliximab: a double-blind placebo-controlled study. Aliment Pharmacol Ther. 2004;20(11–12):1329–1336. doi:10.1111/j.1365-2036.2004.02247.x
267. Sands BE, Anderson FH, Bernstein CN, et al. Infliximab maintenance therapy for fistulizing Crohn’s disease. N Engl J Med. 2004;350(9):876–885. doi:10.1056/NEJMoa030815
268. Fefferman DS, Lodhavia PJ, Alsahli M, et al. Smoking and immunomodulators do not influence the response or duration of response to infliximab in Crohn’s disease. Inflamm Bowel Dis. 2004;10(4):346–351. doi:10.1097/00054725-200407000-00004
269. Schwartz DA, White CM, Wise PE, Herline AJ. Use of endoscopic ultrasound to guide combination medical and surgical therapy for patients with Crohn’s perianal fistulas. Inflamm Bowel Dis. 2005;11(8):727–732. doi:10.1097/01.mib.0000172811.57242.18
270. Tozer P, Ng SC, Siddiqui MR, et al. Long-term MRI-guided combined anti-TNF-α and thiopurine therapy for Crohn’s perianal fistulas. Inflamm Bowel Dis. 2012;18(10):1825–1834. doi:10.1002/ibd.21940
271. Bouguen G, Siproudhis L, Gizard E, et al. Long-term outcome of perianal fistulizing Crohn’s disease treated with infliximab. Clin Gastroenterol Hepatol. 2013;11(8):
272. Dewint P, Hansen BE, Verhey E, et al. Adalimumab combined with ciprofloxacin is superior to adalimumab monotherapy in perianal fistula closure in Crohn’s disease: a randomised, double-blind, placebo controlled trial (ADAFI). Gut. 2014;63(2):292–299. doi:10.1136/gutjnl-2013-304488
273. Dejaco C, Harrer M, Waldhoer T, Miehsler W, Vogelsang H, Reinisch W. Antibiotics and azathioprine for the treatment of perianal fistulas in Crohn’s disease. Aliment Pharmacol Ther. 2003;18(11–12):1113–1120. doi:10.1046/j.1365-2036.2003.01793.x
274. González-Lama Y, Abreu L, Vera MI, et al. Long-term oral tacrolimus therapy in refractory to infliximab fistulizing Crohn’s disease: a pilot study. Inflamm Bowel Dis. 2005;11(1):8–15. doi:10.1097/00054725-200501000-00002
275. Hart AL, Plamondon S, Kamm MA. Topical tacrolimus in the treatment of perianal Crohn’s disease: exploratory randomized controlled trial. Inflamm Bowel Dis. 2007;13(3):245–253. doi:10.1002/ibd.20073
276. Plamondon S, Ng SC, Kamm MA. Thalidomide in luminal and fistulizing Crohn’s disease resistant to standard therapies. Aliment Pharmacol Ther. 2007;25(5):557–567. doi:10.1111/j.1365-2036.2006.03239.x
277. Khorrami S, Ginard D, Marín-Jiménez I, et al. Ustekinumab for the treatment of refractory crohn’s disease: the Spanish experience in a large multicentre open-label cohort. Inflamm Bowel Dis. 2016;22(7):1662–1669. doi:10.1097/MIB.0000000000000842
278. Battat R, Bessissow T, Strohl M, et al. P626 Ustekinumab for the treatment of perianal fistulas in patients with Crohn’s disease. J Crohn’s Colitis. 2017;11(suppl_1):S400–S401. doi:10.1093/ecco-jcc/jjx002.750
279. Ma C, Fedorak RN, Kaplan GG, et al. Clinical, endoscopic and radiographic outcomes with ustekinumab in medically-refractory Crohn’s disease: real world experience from a multicentre cohort. Aliment Pharmacol Ther. 2017;45(9):1232–1243. doi:10.1111/apt.14016
280. Sands BE, Gasink C, Jacobstein D, et al. Fistula healing in pivotal studies of ustekinumab in crohn’s disease. Gastroenterology. 2017;152(5):S185. doi:10.1016/S0016-5085(17)30930-7
281. Tsistrakis S, Oikonomou I. Real-life data on the use of ustekinumab for the treatment of fistulas in patients with crohnʼs disease. Am J Gastroenterol. 2017;112:S361. doi:10.14309/00000434-201710001-00651
282. Krugliak NC, Inessa N, Anthony B, et al. Ustekinumab provides steroid-sparing and perianal improvement in IBD patients: single center experience: p-031. Am J Gastroenterol. 2018;113:S8. doi:10.14309/00000434-201802001-00031
283. Satyam VR, Zullow S, Noronha A, Wasan SK, Farraye FA. Mo1875 - efficacy of ustekinumab in patients with refractory perianal crohn’s disease in a tertiary care IBD center. Gastroenterology. 2018;154(6):S–834. doi:10.1016/S0016-5085(18)32839-7
284. Shitrit A B-G, Ben-Ya’acov A, Siterman M, et al. Safety and effectiveness of ustekinumab for induction of remission in patients with Crohn’s disease: a multicenter Israeli study. United Eur Gastroenterol J. 2020;8(4):418–424. doi:10.1177/2050640620902956
285. Chapuis-Biron C, Kirchgesner J, Pariente B, et al. Ustekinumab for Perianal Crohn’s Disease: the BioLAP Multicenter Study From the GETAID. Am J Gastroenterol. 2020;115(11):1812–1820. doi:10.14309/ajg.0000000000000810
286. Harris RJ, McDonnell M, Young D, et al. Early real-world effectiveness of ustekinumab for Crohn’s disease. Frontline Gastroenterol. 2020;11(2):111–116. doi:10.1136/flgastro-2019-101237
287. Attauabi M, Burisch J, Seidelin JB. Efficacy of ustekinumab for active perianal fistulizing crohn disease: a double-center cohort study. Inflamm Bowel Dis. 2021;27(3):e37–e38. doi:10.1093/ibd/izaa297
288. Godoy Brewer GM, Salem G, Afzal MA, et al. Ustekinumab is effective for perianal fistulising Crohn’s disease: a real-world experience and systematic review with meta-analysis. BMJ Open Gastroenterol. 2021;8(1):e000702. doi:10.1136/bmjgast-2021-000702
289. Manlay L, Boschetti G, Pereira B, et al. Comparison of short- and long-term effectiveness between ustekinumab and vedolizumab in patients with Crohn’s disease refractory to anti-tumour necrosis factor therapy. Aliment Pharmacol Ther. 2021;53(12):1289–1299. doi:10.1111/apt.16377
290. Plevris N, Fulforth J, Siakavellas S, et al. Real-world effectiveness and safety of ustekinumab for the treatment of Crohn’s disease: the Scottish ustekinumab cohort. J Gastroenterol Hepatol. 2021;36(8):2067–2075. doi:10.1111/jgh.15390
291. Straatmijer T, Biemans VBC, Hoentjen F, et al. Ustekinuma b for crohn’s disease: two-year results of the initiative on crohn and colitis (ICC) registry, a nationwide prospective observational cohort study. J Crohns Colitis. 2021;15(11):1920–1930. doi:10.1093/ecco-jcc/jjab081
292. Yao J, Zhang H, Su T, et al. Ustekinumab promotes radiological fistula healing in perianal fistulizing crohn’s disease: a retrospective real-world analysis. J Clin Med. 2023;12(3):939. doi:10.3390/jcm12030939
293. Newman KL, Johnson LA, Stidham RW, Higgins PDR. Vedolizumab more likely to be discontinued than ustekinumab in anti-TNF-experienced patients with fistulizing Crohn’s disease. Therap Adv Gastroenterol. 2023;16:17562848221148254. doi:10.1177/17562848221148254
294. Peyrin-Biroulet L, Panaccione R, Gasink C, et al. P495 Perianal fistula closure in patients receiving ustekinumab: results from the SEAVUE and STARDUST trials. J Crohn’s Colitis. 2022;16(Supplement_1):i460–i460. doi:10.1093/ecco-jcc/jjab232.622
295. Feagan BG, Schwartz D, Danese S, et al. Efficacy of vedolizumab in fistulising crohn’s disease: exploratory analyses of data from GEMINI 2. J Crohns Colitis. 2018;12(5):621–626. doi:10.1093/ecco-jcc/jjy019
296. Chapuis-Biron C, Bourrier A, Nachury M, et al. Vedolizumab for perianal Crohn’s disease: a multicentre cohort study in 151 patients. Aliment Pharmacol Ther. 2020;51(7):719–727. doi:10.1111/apt.15665
297. Schwartz DA, Peyrin-Biroulet L, Lasch K, Adsul S, Danese S. Efficacy and safety of 2 vedolizumab intravenous regimens for perianal fistulizing crohn’s disease: ENTERPRISE study. Clin Gastroenterol Hepatol. 2022;20(5):1059–1067.e9. doi:10.1016/j.cgh.2021.09.028
298. Maeda Y, Ng SC, Durdey P, et al. Randomized clinical trial of metronidazole ointment versus placebo in perianal Crohn’s disease. Br J Surg. 2010;97(9):1340–1347. doi:10.1002/bjs.7121
299. Thia KT, Mahadevan U, Feagan BG, et al. Ciprofloxacin or metronidazole for the treatment of perianal fistulas in patients with Crohn’s disease: a randomized, double-blind, placebo-controlled pilot study. Inflamm Bowel Dis. 2009;15(1):17–24. doi:10.1002/ibd.20608
300. Fistula healing in pivotal studies of ustekinumab in crohn’s disease - clinicalKey. Available from: https://www.clinicalkey.com/#!/content/playContent/1-s2.0-S0016508517309307?returnurl=https:%2F%2Flinkinghub.elsevier.com%2Fretrieve%2Fpii%2FS0016508517309307%3Fshowall%3Dtrue&referrer=https:%2F%2Fwww.researchgate.net%2F.
301. Admin S. European crohn´s and colitis organisation - ECCO - P495 Perianal fistula closure in patients receiving ustekinumab: results from the SEAVUE and STARDUST trials. Available from: https://www.ecco-ibd.eu/publications/congress-abstracts/item/p495-perianal-fistula-closure-in-patients-receiving-ustekinumab-results-from-the-seavue-and-stardust-trials.html.
302. Yzet C, Brazier F, Sabbagh C, Fumery M. Managing complex perianal disease after anti-TNF failure: where to go next? Curr Res Pharmacol Drug Discovery. 2022;3:100081. doi:10.1016/j.crphar.2022.100081
303. Attauabi M, Burisch J, Seidelin JB. Efficacy of ustekinumab for active perianal fistulizing Crohn’s disease: a systematic review and meta-analysis of the current literature. Scand J Gastroenterol. 2021;56(1):53–58. doi:10.1080/00365521.2020.1854848
304. Ayoub F, Odenwald M, Micic D, et al. Vedolizumab for perianal fistulizing Crohn’s disease: systematic review and meta-analysis. Intest Res. 2022;20(2):240. doi:10.5217/ir.2021.00091
305. Pearson DC, May GR, Fick GH, Sutherland LR. Azathioprine and 6-mercaptopurine in Crohn disease. A meta-analysis. Ann Intern Med. 1995;123(2):132–142. doi:10.7326/0003-4819-123-2-199507150-00009
306. Egan LJ, Sandborn WJ, Tremaine WJ. Clinical outcome following treatment of refractory inflammatory and fistulizing crohn’s disease with intravenous cyclosporine. Off J Am Coll Gastroenterol. 1998;93(3):442. doi:10.1111/j.1572-0241.1998.00442.x
307. Ciclosporina A intravenosa en el tratamiento de la enfermedad de Crohn activa refractaria al tratamiento convencional | medicina Clínica. Available from: https://www.elsevier.es/es-revista-medicina-clinica-2-linkresolver-ciclosporina-a-intravenosa-el-tratamiento-13039507.
308. Dc B, Jp P, S A, W B, Au D. Tacrolimus is safe and effective in patients with severe steroid-refractory or steroid-dependent inflammatory bowel disease--a long-term follow-up. Am J Gastroenterol. 2006;101(5). doi:10.1111/j.1572-0241.2006.00524.x
309. I E, P M, F R, et al. Oral tacrolimus long-term therapy in patients with Crohn’s disease and steroid resistance. Aliment. Pharmacol. Ther. 2001;15(3). doi:10.1046/j.1365-2036.2001.00938.x
310. Benson A, Barrett T, Sparberg M, Buchman AL. Efficacy and safety of tacrolimus in refractory ulcerative colitis and Crohn’s disease: a single-center experience. Inflamm Bowel Dis. 2008;14(1):7–12. doi:10.1002/ibd.20263
311. Tamaki H, Nakase H, Matsuura M, et al. The effect of tacrolimus (FK-506) on Japanese patients with refractory Crohn’s disease. J Gastroenterol. 2008;43(10):774–779. doi:10.1007/s00535-008-2229-y
312. Bramuzzo M, Ventura A, Martelossi S, Lazzerini M. Thalidomide for inflammatory bowel disease: systematic review. Medicine. 2016;95(30):e4239. doi:10.1097/MD.0000000000004239
313. Vuyyuru SK, Solitano V, Narula N, et al. Pharmacological therapies for the management of fistulizing crohn’s disease: a systematic review and meta-analysis. J Crohn’s Colitis. 2024;18(4):589–603. doi:10.1093/ecco-jcc/jjad185
314. West RL, van der Woude CJ, Hansen BE, et al. Clinical and endosonographic effect of ciprofloxacin on the treatment of perianal fistulas in Crohn’s disease with infliximab: a double-blind placebo-controlled study. Eur J Gastroenterol Hepatol. 2005;17(1):A63.
315. Jones JL, Kaplan GG, Peyrin-Biroulet L, et al. Effects of concomitant immunomodulator therapy on efficacy and safety of anti-tumor necrosis factor therapy for crohn’s disease: a meta-analysis of placebo-controlled trials. Clin Gastroenterol Hepatol. 2015;13(13):
316. Lopez N, Ramamoorthy S, Sandborn WJ. Recent advances in the management of perianal fistulizing Crohn’s disease: lessons for the clinic. Expert Rev Gastroenterol Hepatol. 2019;13(6):563–577. doi:10.1080/17474124.2019.1608818
317. Panés J, Rimola J. Perianal fistulizing Crohn’s disease: pathogenesis, diagnosis and therapy. Nat Rev Gastroenterol Hepatol. 2017;14(11):652–664. doi:10.1038/nrgastro.2017.104
318. Serclova Z, Garcia-Olmo D, Chen ST, et al. OP18 Efficacy and safety of darvadstrocel treatment in patients with complex perianal fistulas and Crohn’s Disease: results from the global ADMIRE-CD II phase 3 study. J Crohn’s Colitis. 2024;18(Supplement_1):i34–i35. doi:10.1093/ecco-jcc/jjad212.0018
319. McCurdy J, Siw KCK, Kandel R, Larrigan S, Rosenfeld G, Boet S. The effectiveness and safety of hyperbaric oxygen therapy in various phenotypes of inflammatory bowel disease: systematic review with meta-analysis. Inflammat Bowel Dis. 2022;28(4):611–621. doi:10.1093/ibd/izab098
320. Heyboer M, Sharma D, Santiago W, McCulloch N. Hyperbaric Oxygen Therapy: side Effects Defined and Quantified. Adv Wound Care (New Rochelle). 2017;6(6):210–224. doi:10.1089/wound.2016.0718
321. Edinguele WF, Barberon B, Poussard J, Thomas E, Reynier JC, Coulange M. Middle-ear barotrauma after hyperbaric oxygen therapy: a five-year retrospective analysis on 2610 patients. Undersea Hyperb Med. 2020;47(2):217–228. doi:10.22462/04.06.2020.7
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.