Back to Journals » Clinical Ophthalmology » Volume 19
Refractive Predictability After Keratorefractive Lenticule Extraction Using a New Nomogram Creation Software Tool Compared to a Matched Control
Authors Wan Q ![]() , Wei R, Tang J, Deng YP, Ma K
, Wei R, Tang J, Deng YP, Ma K ![]()
Received 1 June 2025
Accepted for publication 24 July 2025
Published 1 August 2025 Volume 2025:19 Pages 2541—2548
DOI https://doi.org/10.2147/OPTH.S544117
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Qi Wan, Ran Wei, Jing Tang, Ying-ping Deng, Ke Ma
Department of Ophthalmology, West China Hospital of Sichuan University, Chengdu, People’s Republic of China
Correspondence: Ying-ping Deng, Department of Ophthalmology, West China Hospital of Sichuan University, #37, Guo Xue Lane, Chengdu, Sichuan, 610041, People’s Republic of China, Email [email protected] Ke Ma, Department of Ophthalmology, West China Hospital of Sichuan University, #37, Guo Xue Lane, Chengdu, Sichuan, 610041, People’s Republic of China, Email [email protected]
Purpose: The study aimed to assess the impact of VISULYZE nomogram software on refractive outcomes after lenticule extraction for myopia and myopic astigmatism correction.
Methods: This ambispective, single-site, matched case–control study was conducted at West China Hospital in Chengdu, China. Treatments using the VISULYZE nomogram were compared to a control group without it. The main outcome was refractive accuracy at 3 months, measured by the proportion of eyes achieving a spherical equivalent (SEQ) within ± 0.50 D of the target and astigmatism ≤ 0.50 D.
Results: The study involved 180 eyes, with 90 treated using VISULYZE and 90 matched controls analyzed retrospectively. In the VISULYZE group, 98.9% achieved SEQ within ± 0.50 D versus 85.6% in the control group (P< 0.001). Astigmatism ≤ 0.50 D was achieved in 100% of VISULYZE-treated eyes compared to 93.3% in controls (P=0.006). Both groups had similar safety indices. VISULYZE showed higher correlations between attempted and achieved SEQ (R²=0.9799) and astigmatism (R²=0.8996) compared to the control group (SEQ: R²=0.9590; Astig: R²=0.5992). Standard efficacy and safety measures showed no difference between groups.
Conclusion: The VISULYZE-generated nomogram demonstrated improved predictability and accuracy in refractive outcomes. It may enhance results for surgeons compared to those using no nomogram or a standard offset nomogram.
Keywords: lenticule extraction, outcomes, nomogram, VISULYZE, SMILE
Introduction
Refractive surgery holds a significant position in contemporary ophthalmology, particularly with the advent of keratorefractive lenticule extraction (KLEx) procedures such small-incision lenticule extraction (SMILE). KLEx has become a mainstream procedure for correcting myopia and myopic astigmatism due to its reported advantages over laser in-situ keratomileusis (LASIK).1,2 However, just as with LASIK, it is essential that surgeons used personalized treatment parameters to achieve optimal visual outcomes.3,4
Nomograms can be created empirically based on a surgeon’s experience. However, nomogram development and subsequent outcomes analysis can be time-consuming and require both an understanding of the necessary data to gather as well as the knowledge of how to formulate and implement the nomogram. There are a number of options, depending on the region, such as software programs that are available to help corneal refractive surgeons develop a nomogram and/or monitor patient outcomes including IBRA® (Zubisoft GmbH), Datagraph-med® (Datagraph-med), and SurgiVision® Datalink (SurgiVision Consultants Inc). However, there are minor downsides to each of the available programs such as needing a subscription to access your own data or poor visualization of results.
In 2021, VISULYZE® was released by Carl Zeiss Meditec. VISULYZE is a data analysis and nomogram creation software tool that is available for surgeons performing treatments using the MEL 80 and MEL 90 excimer lasers (Carl Zeiss Meditec) as well as VisuMax and VISUMAX 800 femtosecond lasers (Carl Zeiss Meditec). As with all nomograms, VISULYZE software intends to optimize predictability, but also provide easy visualization of the results to allow surgeons to effectively and efficiently monitor outcomes.
To date, there have been no reports in the literature evaluating outcomes using VISULYZE or comparing outcomes without using the program. The current study investigates the impact that a VISULYZE generated nomogram has on refractive predictability following SMILE surgery with the VisuMax femtosecond laser.
Methods
This was an ambispective, matched, case–control study evaluating outcomes in patients undergoing routine SMILE surgery at the Refractive Center of West China Hospital, Sichuan University. The study received approval from the ethics committee of West China Hospital, Sichuan University and complied with the principles of the Declaration of Helsinki. Informed consent was obtained from all patients prior to treatment. Inclusion criteria were age 18 years or older, spherical equivalent (SEQ) ranging from −0.50 to −8.00 D and cylinder up to 2.00 D. Exclusion criteria were active inflammation-related eye diseases, intraoperative or postoperative surgical complications, and a preoperative corrected distance visual acuity (CDVA) less than 20/20. Patients treated using a VISULYZE generated nomogram (VISULYZE group) were treated prospectively. The nomogram used for the VISULYZE group was generated through entering 339 eyes that underwent routine SMILE between 2022 and 2023 into the VISULYZE nomogram generation software. A matched group of eyes, treated using a standard “surgeon experience” nomogram (control group), were retrospectively analyzed.
Settings of VISULYZE Group and Control Group
The VISULYZE group was constructed using the ZEISS VISULYZE software (version 1.1). By performing a linear regression analysis, a functional relationship was established between the actual corrected spherical equivalent (SE) and the intended machine-corrected SE (model formula: Y = 0.9436*x; goodness-of-fit R² = 0.996). This was used to generate a personalized nomogram chart to guide the laser input settings for new cases. In contrast, the control group setting scheme adjusted the laser input value by adding a 10% increment of the actual sphere.
Surgical Procedure and Postoperative Care
All procedures (for both groups) were performed by a single experienced surgeon (K.M). A standard operative procedure was followed for all subjects. The lenticule diameter ranged from 6.0 to 6.5 mm with a cap thickness of 110 to 120 μm and a cap diameter 1 mm larger than the lenticule. A single 2mm small-incision was created in each eye; 12 o’clock position in the left eye and 11 o’clock position in the right eye. The lenticule was separated using a dissector (Suzhou Heart Lamp Medical Equipment, China) and removed using micro-forceps. Postoperatively, patients were prescribed 0.5% levofloxacin eye drops (Santen, Japan) four times daily for one week, 0.1% tobramycin dexamethasone eye drops (Alcon, China) four times daily for one week, and preservative-free artificial tears (0.1% sodium hyaluronate) four times daily, with dosage adjustments based on patient symptoms.
Statistical Analysis
Propensity score matching was performed using the “MatchIt” package in R software (version 4.2.2) to match groups (VISULYZE vs control) based on the patients’ baseline characteristics in a 1:1 ratio, considering factors such as age, spherical equivalent, UDVA, and CDVA. The matched groups’ data were analyzed in R. The Shapiro–Wilk test was used to confirm whether the data followed a normal distribution. Continuous variables were described using Mean ± SD or Median [IQR] and compared using the Paired t-test or Mann–Whitney U-test. Categorical variables were described using frequencies and compared using the Chi-square test. Correlation data and R² values are compared using Fisher’s z-transformation test. Postoperative refractive outcomes were statistically analyzed using VISULYZE software (V1.1) and presented according to the standard graphs for reporting refractive surgery outcomes.5 The primary outcome measures were refractive accuracy at three months postoperatively, defined as the proportion of eyes achieving postoperative spherical equivalent (SEQ) within ±0.50 D and ±1.00 D target ranges. Astigmatism was assessed for proportion of eyes with ≤0.50 D and ≤1.00 D of residual refractive astigmatism. Secondary outcome measures included proportion of eyes achieving uncorrected distance visual acuity (UDVA) of 20/20 or better postoperatively, proportion of eyes with unchanged or improved UDVA compared to preoperative CDVA, proportion of eyes with unchanged or improved CDVA postoperatively, and predictability between attempted and achieved spherical equivalent and astigmatism. The proportion of eyes with postoperative refractive astigmatism axis deviation within ±15° was also assessed.
Results
A total of 90 eyes were treated prospectively using a VISULYZE generated nomogram (VISULYZE group), and data was retrospectively collected from 90 eyes for the matched control (control group). Preoperative mean manifest sphere was −4.95±1.62 D in the VISULYZE group and −4.74±1.53 D in the control group. Population demographics for both groups are presented in Table 1.
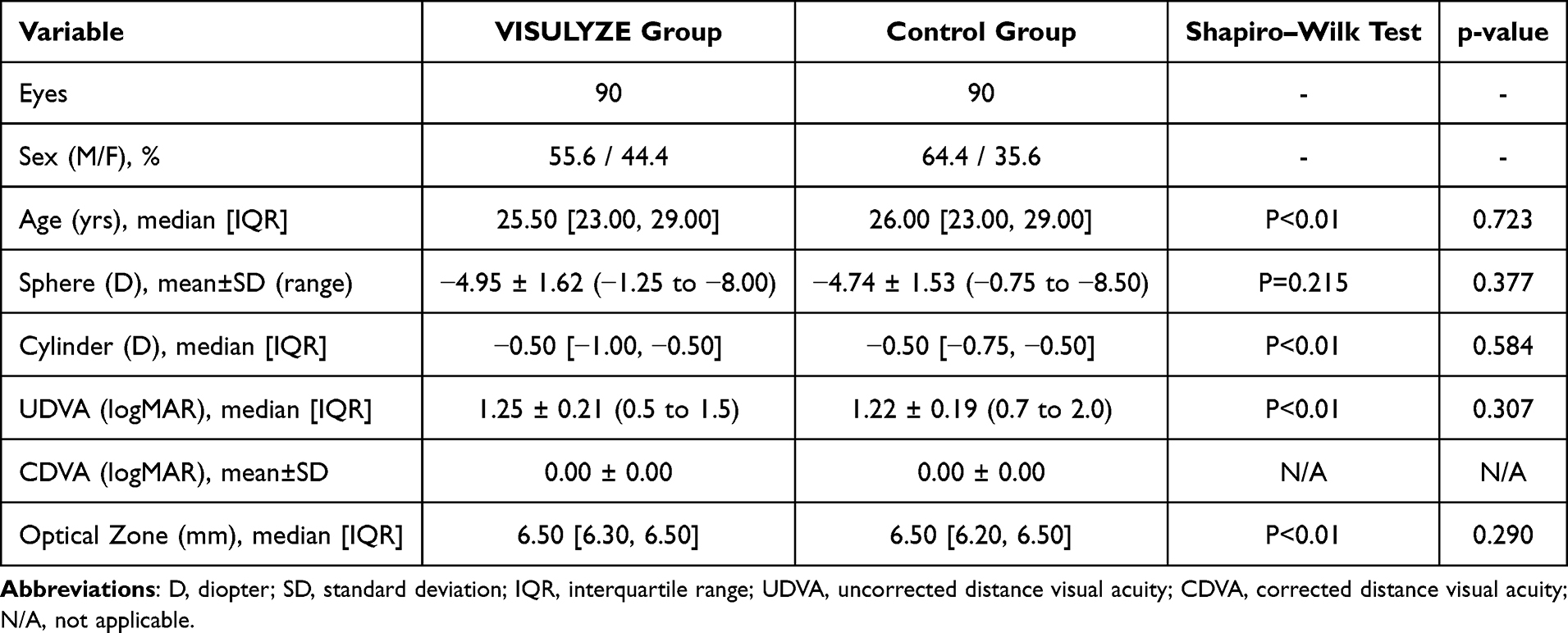 |
Table 1 Preoperative Demographics for the VISULYZE Group and Matched Control Group |
Efficacy and Predictability
Figures 1 and 2 show the standard graphs for reporting refractive outcomes for the VISULYZE group and control group, respectively. The specific statistical results of the two groups are shown in Table 2. In the VISULYZE group, 99% of eyes achieved an UDVA of 20/20 or better at the 3-month postoperative visit (Figure 1A). In the control group, 99% of eyes also achieved an UDVA of 20/20 or better (Figure 2A). The proportions maintaining or improving UDVA relative to preoperative CDVA were 100% for the VISULYZE group and 98.9% for the Control group (Figures 1B and 2B). When evaluating safety for the VISULYZE group, Figure 1C shows no change in 36.7% of eyes and 60.0% of eyes gained one or more lines compared to preoperative CDVA. In the control group (Figure 2C), there was no change in 52.2% of eyes and 44.4% gained one or more lines compared to preoperative CDVA. No eyes in either group lost one or more lines of CDVA compared to preoperative levels.
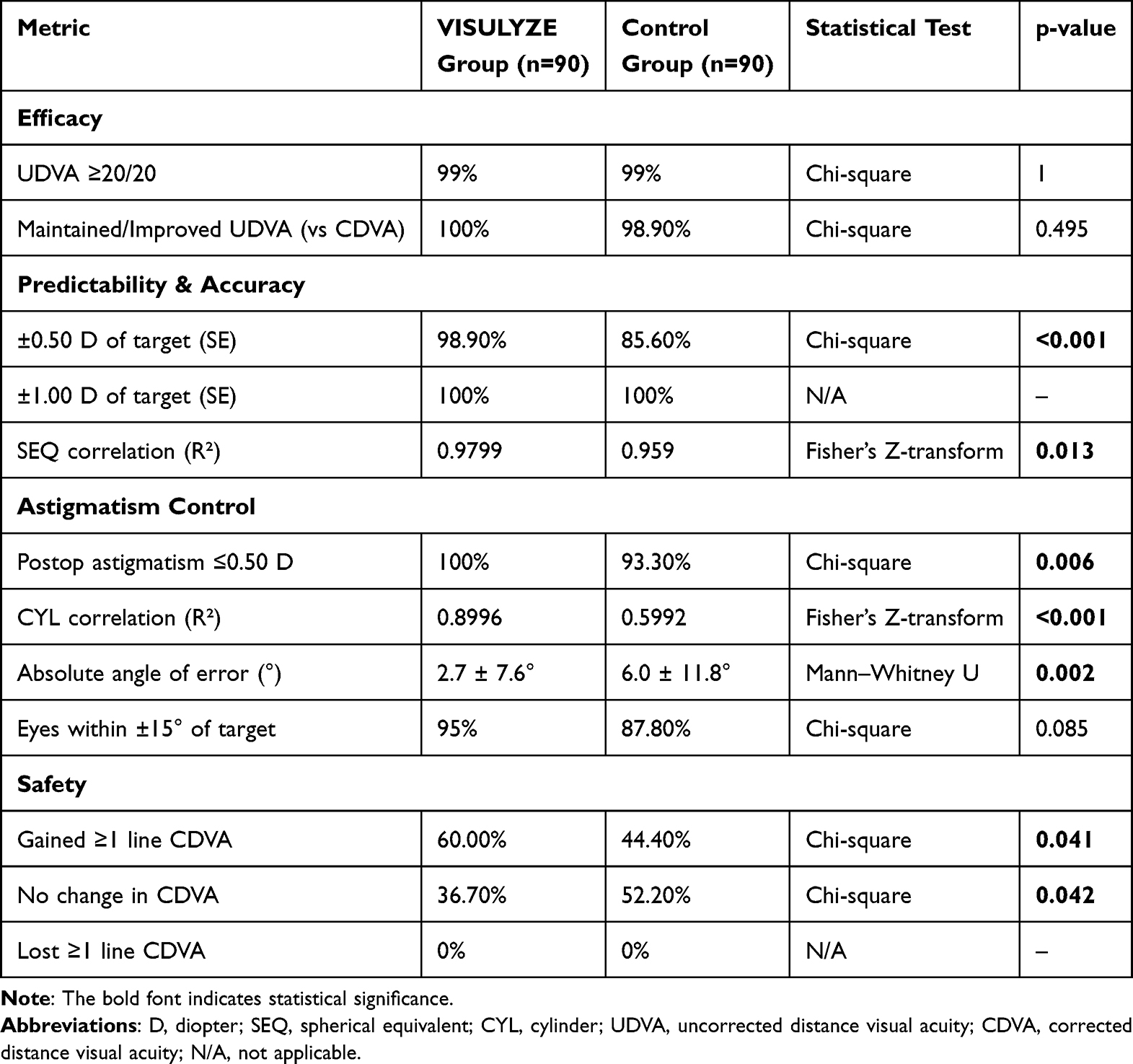 |
Table 2 Comparison of Efficacy, Predictability, and Safety Outcomes Between VISULYZE and Control Groups |
 |
Figure 1 Refractive outcomes of VISULYZE-nomogram-assisted SMILE surgery at 3 months: (A) Efficacy, represented by uncorrected distance visual acuity (UDVA); (B) Comparison of UDVA and corrected distance visual acuity (CDVA); (C) Safety, indicated by changes in CDVA; (D) Predictability, illustrated by the spherical equivalent (SEQ) of attempted versus achieved correction; (E) Accuracy, detailing the refractive SEQ outcomes; (F) Stability, showing changes in SEQ refraction tabover time; (G) Astigmatism, reflecting postoperative residual astigmatism on refraction; (H) Predictability, illustrated by the attempted versus achieved astigmatism correction; and (I) Angle of error for refractive astigmatism. |
 |
Figure 2 Refractive outcomes of the control group at 3 months: (A) Efficacy, represented by uncorrected distance visual acuity (UDVA); (B) Comparison of UDVA and corrected distance visual acuity (CDVA); (C) Safety, indicated by changes in CDVA; (D) Predictability, illustrated by the spherical equivalent (SEQ) of attempted versus achieved correction; (E) Accuracy, detailing the refractive SEQ outcomes; (F) Stability, showing changes in SEQ refraction over time; (G) Astigmatism, reflecting postoperative residual astigmatism on refraction; (H) Predictability, illustrated by the attempted versus achieved astigmatism correction; and (I) Angle or error for refractive astigmatism. |
Predictability, Accuracy, and Stability
The correlation R2 between Achieved and Attempted SEQ (D) was 0.9799 for the VISULYZE group and 0.9590 for the Control group (Figures 1D and 2D). In the VISULYZE group, 98.9% of eyes had a spherical equivalent refraction within ±0.50 D of target and 100% within 1.00 D of target (Figure 1E). In the control group, 85.6% of eyes were within ±0.50 D and 100% within 1.00 D of target (Figure 2E). The mean observed SEQs at 3-month follow-up were 0.05D (Figure 2F) and 0.22D (Figure 2F).
Astigmatism Analysis
In the VISULYZE group, 100% of eyes had ≤0.50 D of postoperative refractive astigmatism (Figure 1G). The correlation R2 between Achieved and Attempted CYL (D) was 0.8996 (Figure 1H). Angle of error analysis showed the absolute mean angle of error was 2.7±7.6° with 95% of eyes within ±15° (Figure 1I). In the control group, 93.3% of eyes had ≤0.50 D and 100% of eyes had ≤1.00 D of refractive astigmatism (Figure 2G). The correlation R2 between Achieved and Attempted CYL (D) was 0.5992 (Figure 2H). Angle of error analysis showed the absolute mean angle of error was 6.0±11.8° with 87.8% of eyes within ±15° (Figure 2I).
Discussion
Our study demonstrated that SMILE, whether guided by a VISULYZE-generated nomogram or a traditional nomogram, resulted in excellent visual outcomes. As shown in Table 2, both groups achieved high efficacy and safety. There were no significant differences for UDVA ≥20/20 (p=1) or maintained/improved UDVA (p=0.495). However, the VISULYZE group demonstrated statistically significant improvements in predictability, with a greater proportion of eyes within ±0.50 D of target SE (98.9% vs 85.6%, p<0.001) and higher SEQ correlation (R²=0.9799 vs 0.959, p=0.013). Astigmatism control was also superior in the VISULYZE group, with more eyes achieving postoperative astigmatism ≤0.50 D (100% vs 93.3%, p=0.006) and better CYL correlation (R²=0.8996 vs 0.5992, p<0.001). Safety outcomes were comparable, with no eye in either group losing ≥1 line of CDVA.
Numerous studies have demonstrated the excellent safety, efficacy, and stability of SMILE surgery in both short-term and long-term observations.6–8 This surgical approach is favored for its minimally invasive nature and rapid recovery. However, to further enhance the precision of SMILE surgery, as with any type of corneal refractive surgery, optimization of preoperative parameters is key. One key to improving a patient’s outcome is to develop a personalized nomogram. Though some surgeons use nomograms, the quantitative standard is not yet unified and is primarily based on experience.4,9 Literature reports show that surgeons use varying nomogram adjustments or no nomogram,10 leading to possible refractive deviations after SMILE.
To the best of our knowledge, this study is the first to evaluate a nomogram generated by the VISULYZE nomogram generation software in a standardized manner to guide SMILE surgery, aiming to enhance refractive accuracy through scientific data analysis. In the current study, the primary outcome measures showed treatment using a VISULYZE generated nomogram demonstrated significantly greater refractive accuracy than a traditionally “experienced-based” nomogram. Specifically, the proportion of eyes achieving a postoperative SEQ within ±0.50 D was significantly higher in the VISULYZE group compared to the control group. This outcome suggests that a data-driven nomogram setting via VISULYZE software can effectively reduce occurrences of undercorrection or overcorrection. A previous study also demonstrated that the use of an astigmatic nomogram can enhance the accuracy and predictability of high myopic astigmatism correction in SMILE surgery.11
The proportion of eyes maintaining stable or improved uncorrected visual acuity (UDVA) and corrected distance visual acuity (CDVA) was not significantly different between the VISULYZE group and the control group. This indicates that while a personalized nomogram significantly improved refractive accuracy, the improvement in visual efficacy is comparable between the two approaches. This observation may be attributed to the inherently high efficacy of KLEx surgery with most recent studies showing that more than 90% of eyes typically see 20/20 or better without correction after treatment.12–14 While studies show that lenticule extraction is stable between 3 and 12 months, it would be important to re-evaluate the two groups at the 12-month postoperative visit to check for any additional changes to the UDVA results.
In terms of safety, both groups exhibited similar rates of stable or improved postoperative CDVA, with no significant declines observed. The safety results, while not necessarily directly related to the nomogram were also similar to previous studies where no eyes lost two or more lines of CDVA compared to preoperative.15–17 This reinforces the safety profile of SMILE surgery and shows that using a VISULYZE generated nomogram did not increase the risk of postoperative complications.
In predictability analysis, the correlation between postoperative SEQ and programmed SEQ was significantly better in the VISULYZE group, demonstrating higher refractive predictability. This indicates that VISULYZE-generated nomograms can more accurately predict postoperative refractive states, reducing refractive deviations. Previous SMILE studies have reported postoperative 3-month predictability within ±0.50 D in 85% to 95% of eyes. In comparison, the VISULYZE group achieved a higher predictability in the current study, further highlighting its benefits, while the control group results were consistent with previous findings.18–20 The slight increase in predictability may play a role in decreasing the need for surgical enhancements.
A key strength of this study is the systematic evaluation of the application of a VISULYZE generated nomograms in KLEx. Through rigorous propensity matching and systematic statistical analysis, there should be minimal impact of confounding factors, enhancing the scientific rigor and persuasiveness of the results. Additionally, the prospective design of the VISULYZE arm and strict follow-up protocol ensured data integrity and reliability. However, this study has several limitations. First, while the VISULYZE arm was prospective, the control arm consisted of retrospective data analysis. Nevertheless, as previously mentioned, the matching process was rigorous, and a standardized preoperative and postoperative evaluation and follow-up protocol was employed for all patients, ensuring high-quality data regardless of study enrollment status. Second, the follow-up period was limited to three months. Although short-term outcomes demonstrated significant advantages, long-term effects and potential differences in enhancement rates between groups require further validation. The study groups will continue to be followed to capture any changes in long-term outcomes. Third, both eyes of the same patient were included in each group. While this approach increases the available data, it may introduce inter-eye correlation, potentially inflating the effective sample size and reducing the true statistical power due to a lack of independence among observations. We acknowledge that this methodological decision may affect the interpretation of the results, and future studies could address this by including only one eye per patient. Finally, as with any nomogram, the accuracy of the VISULYZE-generated nomogram may further improve as additional data are incorporated into the database.
In conclusion, the current study demonstrated that using a VISULYZE generated nomogram yielded excellent results in terms of accuracy and predictability. In addition, there was an improvement in those measures when compared to not using the nomogram. This software provides another tool in a surgeon’s armamentarium for improving patient care. The ease of use of VISULYZE may also increase adoption amongst surgeons, especially those that have less experience when it comes to developing personalized nomograms or creating graphs to analyze and present outcomes. Future research should consider larger sample sizes and longer follow-up periods to further validate the durability and broad applicability of these findings.
Abbreviations
KLEx, Keratorefractive lenticule extraction; SMILE, Small-incision lenticule extraction; LASIK, Laser in-situ keratomileusis; SPH, Spherical lens; SEQ, Spherical equivalent; CYL, Sylinder; UDVA, Uncorrected distance visual acuity; CDVA, Corrected distance visual acuity.
Data Sharing Statement
The datasets generated and/or analysed during the current study are not publicly available due to restrictions from the West China Hospital data privacy policy, but may be available from the corresponding author on reasonable request.
Ethics Approval
The extended study was approved by the Ethics Committee of West China Hospital and performed in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
There are no competing interests among authors.
References
1. Cummings AB. Growing refractive surgery. Indian J Ophthalmol. 2020;68(12):2652–2653. doi:10.4103/ijo.IJO_1779_20
2. Kwak JJ, Jun I, Kim EK, et al. Clinical outcomes of small incision lenticule extraction in myopia: study of vector parameters and corneal aberrations. Korean J Ophthalmol. 2020;34(1):76–84. doi:10.3341/kjo.2019.0109
3. Arba Mosquera S, de Ortueta D, Verma S. The art of nomograms. Eye Vis. 2018;5(1):2. doi:10.1186/s40662-018-0096-z
4. Liang G, Chen X, Zha X, Zhang F. A nomogram to improve predictability of small-incision lenticule extraction surgery. Med Sci Monit. 2017;23:5168–5175. doi:10.12659/MSM.904598
5. Reinstein DZ, Archer TJ, Randleman JB. Jrs standard for reporting astigmatism outcomes of refractive surgery. J Refract Surg. 2014;30(10):654–659. doi:10.3928/1081597X-20140903-01
6. Blum M, Lauer AS, Kunert KS, Sekundo W. 10-year results of small incision lenticule extraction. J Refract Surg. 2019;35(10):618–623. doi:10.3928/1081597X-20190826-02
7. Blum M, Taubig K, Gruhn C, et al. Five-year results of small incision lenticule extraction (Relex Smile). Br J Ophthalmol. 2016;100(9):1192–1195. doi:10.1136/bjophthalmol-2015-306822
8. Reinstein DZ, Archer TJ, Vida RS, et al. Small incision lenticule extraction (Smile) for the correction of high myopia with astigmatism. J Refract Surg. 2022;38(5):262–271. doi:10.3928/1081597X-20220314-01
9. Zhang R, Yuan Y, Zhang Y, Chen Y. Subjective patient-reported visual quality after small-incision lenticule extraction and its correlation to the objective one. Int Ophthalmol. 2023;43(11):3935–3942. doi:10.1007/s10792-023-02794-z
10. Fu Y, Yin Y, Wu X, et al. Clinical outcomes after small-incision lenticule extraction versus femtosecond laser-assisted lasik for high myopia: a meta-analysis. PLoS One. 2021;16(2):e0242059. doi:10.1371/journal.pone.0242059
11. Yu N, Hou X, Liu C, et al. A nomogram to improve the predictability of high myopic astigmatism in small incision lenticule extraction surgery. J Refract Surg. 2025;41(1):e65–e72. doi:10.3928/1081597X-20241126-01
12. Reinstein DZ, Archer TJ, Potter JG, et al. Refractive and visual outcomes of smile for compound myopic astigmatism with the visumax 800. J Refract Surg. 2023;39(5):294–301. doi:10.3928/1081597X-20230301-02
13. Yoo TK, Kim D, Kim JS, et al. Comparison of early visual outcomes after smile using visumax 800 and visumax 500 for myopia: a retrospective matched case-control study. Sci Rep. 2024;14(1):11989. doi:10.1038/s41598-024-62354-y
14. Yoon H, Magnago T, Yeom DJ. Three-month clinical outcomes to correct myopia or myopic astigmatism using a femtosecond laser for lenticule creation with automated centration and cyclotorsion compensation. J Refract Surg. 2024;40(1):e30–e41. doi:10.3928/1081597X-20231212-03
15. Evangelista CB, Harris JP, Trinh TM, et al. Comparing visual outcomes of keratorefractive lenticule extraction, Prk, and lasik procedures in the military population. J Cataract Refract Surg. 2025;51(2):98–105. doi:10.1097/j.jcrs.0000000000001565
16. Sekundo W, Chang JSM, Ganesh S, et al. Keratorefractive lenticule extraction for myopia and myopic astigmatism with the visumax 800: 6-month outcomes of a prospective multi-center post-market clinical follow-up study. J Refract Surg. 2025;41(3):e264–e71. doi:10.3928/1081597X-20250204-03
17. Varman A, Varman A, Balakumar D. Comparison of visual and refractive outcomes of keratorefractive lenticule extraction for compound myopic astigmatism between visumax and visumax 800. Clin Ophthalmol. 2024;18:3557–3566. doi:10.2147/OPTH.S492552
18. Kim JR, Hwang HB, Mun SJ, et al. Efficacy, predictability, and safety of small incision lenticule extraction: 6-months prospective cohort study. BMC Ophthalmol. 2014;14(1):117. doi:10.1186/1471-2415-14-117
19. Reinstein DZ, Carp GI, Archer TJ, et al. Large population outcomes of small incision lenticule extraction in young myopic patients. J Refract Surg. 2022;38(8):488–496. doi:10.3928/1081597X-20220623-01
20. Tay E, Bajpai R. Visual recovery after small incision lenticule extraction (smile) in relation to pre-operative spherical equivalent. Graefes Arch Clin Exp Ophthalmol. 2021;259(4):1053–1060. doi:10.1007/s00417-020-04954-8
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.