Back to Journals » Clinical Ophthalmology » Volume 11
Refractive and visual outcomes after Keraring intrastromal corneal ring segment implantation for keratoconus assisted by femtosecond laser at 6 months follow-up
Authors Heikal MA ![]() , Abdelshafy M
, Abdelshafy M ![]() , Soliman TT
, Soliman TT ![]() , Hamed AM
, Hamed AM
Received 20 August 2016
Accepted for publication 29 October 2016
Published 23 December 2016 Volume 2017:11 Pages 81—86
DOI https://doi.org/10.2147/OPTH.S120267
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mohamed A Heikal, Marwa Abdelshafy, Tarek T Soliman, Abdelmonem M Hamed
Department of Ophthalmology, Benha University, Banha, Egypt
Purpose: We attempted to evaluate the efficacy of femtosecond laser-assisted intrastromal corneal ring segment implantation in patients with keratoconus (KC).
Patients and methods: A retrospective interventional consecutive clinical study was conducted on patients with KC who were treated with femtosecond laser Keraring implantation. All procedures were performed at Ebsar Eye Center in the period from January 5, 2015, to February 28, 2016.
Results: Thirty eyes of 20 patients were included in this study. The mean age of patients was 27.43±3.57 years. Eleven patients (55%) were female and nine patients (45%) were male. Keraring segments were successfully implanted in all eyes. There were no complications or need for ring repositioning. The follow-up period was 6 months postoperatively. There was a significant improvement in the mean logarithm of the minimum angle of resolution (LogMAR) of uncorrected visual acuity (UCVA) after Keraring segment implantation from 1.5±0.23 preoperatively to 0.54±0.16 at 6 months postoperatively (P=0.001). The preoperative mean LogMAR of best-corrected visual acuity (BCVA) was 0.85±0.17. At 1 month postoperatively, it was 0.35±0.15; at 3 months postoperatively, it was 0.26±0.11, and at 6 months postoperatively, it was 0.14±0.07 (P=0.001). The mean preoperative maximum keratometric value for 3 mm pupil in diopters (K max) significantly decreased from 55.85±5.44 preoperatively (N=30) to 44.05±1.64 D at 6 months postoperatively (P=0.001). There was a statistically significant reduction in the mean preoperative spherical equivalent from –5.43±1.76 D preoperatively to –2.43±0.95 D at 6 months postoperatively. No statistically significant differences were detected between 1 and 3 months of follow-up regarding the visual and refractive outcomes.
Conclusion: Analysis of the outcomes after Keraring ICRS implantation showed a significant postoperative corneal flattening with a subsequent increase in UCVA and BCVA. Using the femtosecond laser for tunnel creation made the procedure easy and fast with an accurate precise depth of implantation and reduced the risk of operative and postoperative complications.
Keywords: femtosecond laser, K astigmatism Keraring, spherical error
Introduction
Keratoconus (KC) is a noninflammatory ectatic corneal disease characterized by progressive paracentral corneal thinning and inferior corneal steepening that causes irregular astigmatism, protrusion and decreased visual acuity.1,2 It usually starts in early adulthood and progresses until the third decade of life and then becomes stable.3,4 Different methods of increasing visual acuity in KC, including spectacles, contact lenses and corneal grafting, have been introduced.3,5
In the early stages of the disease, the decreased visual acuity can be improved with rigid permeable contact lenses or spectacles. However, as the condition progresses, the patients may require corneal grafting. KC is the leading cause for keratoplasty in the developed world.3,5
Intrastromal corneal ring segment (ICRS) implantation is considered as a minimally invasive surgical procedure in the management of KC. ICRS implantation minimizes the spherocylindrical error by reducing the steepness of the curvature of the central cornea with promising changes in the topographic analysis, uncorrected visual acuity (UCVA) and best-corrected visual acuity (BCVA).6,7
The construction of intrastromal tunnel for ring implantation with mechanical dissection has many complications such as epithelial defects, depth asymmetry and corneal perforation.8–10
Femtosecond laser has been introduced to create the tunnel for ring implantation with an accurately precise depth in a programmed way with a safe and effective procedure for creating tunnels for segment placement at predetermined depths. The tunnel creation using femtosecond laser is easier, more precise and more predictable than the conventional mechanical technique.11
There are different types of intracorneal rings that have variable curvatures, widths and zones of implantation. The Keraring (Mediphacos, Belo Horizonte, Brazil) is used to treat KC. It is made of polymethyl methacrylate (PMMA). It is characterized by a triangular cross-section in contrast to other ICRSs, such as Ferrara rings. The SI-5 design is available in a 600 μm base with an optical diameter of 5 mm with different thicknesses, such as 0.15, 0.20, 0.25, 0.30 and 0.35 mm.12 The SI-6 is designed with an 800 μm base with an optical zone of 6 mm.13
Patients and methods
This is a retrospective interventional consecutive clinical study. All procedures were performed at Ebsar Eye Center in the period from January 5, 2015, to February 28, 2016. This study was carried out on 30 eyes of 20 patients who had been diagnosed and graded with KC according to standard criteria based on slit-lamp observation and corneal topography.
All patients underwent Keraring ICRS implantation assisted with the femtosecond laser (VisuMax® femtosecond system; Zeiss, Jena, Germany) for tunnel creation.
Inclusion criteria were as follows: clear corneal center with corneal thickness >500 μm at the site of tunnel creation, no improvement in visual acuity with spectacles correction or intolerance to contact lenses, and patients with a mean keratometry between 42 and 65 D.
Patients were excluded if they had corneal scarring, history of previous corneal surgeries or ocular pathology, history of systemic medications that affect corneal wound healing, collagen vascular diseases, corneal dystrophies, were pregnant or lactating, or patients with follow-up <6 months.
All the patients had preoperative evaluations including manifest UCVA, BCVA (logarithm of the minimum angle of resolution [LogMAR]), spherical equivalent (SE), slit-lamp biomicroscopy, fundus examination and corneal topographic analysis (maximum keratometric value for 3 mm pupil in diopters [K max] and K astigmatism) with oculus pentacam.
Preoperative informed consent was obtained from the patients. Written informed consent to publish this paper and accompanying images was obtained from the patients. This research has been approved by the Ebsar Eye Center institutional review board.
The procedure was performed under topical anesthesia. We used femtosecond laser delivery system (VisuMax) to create the tunnels. The incision axis was planned on the axis of the steepest keratometric reading, with an 80% depth of the thinnest location at an optical zone 5 mm of inner diameter and an outer diameter of 5.8 mm. The pockets were opened using a blunt sinskey. The Kerarings were implanted according to the Keraring nomogram rules.
Postoperative visits were scheduled at the first postoperative day and then at 1, 3 and 6 months after surgery. On each visit, manifest UCVA, BCVA (LogMAR), SE, slit-lamp biomicroscopy (Keraring position and corneal integrity) and corneal topographic analysis were observed. Postoperative treatment of tobramycin 0.3% and dexamethasone 0.1% eye drops was applied five times daily for 2 weeks with tapering of dexamethasone 0.1% for 2 weeks.
Statistical analysis
Statistical tests used are mean, standard deviation, analysis of variance and P-value. P-value was considered significant if <0.05. Statistical analysis was performed using the commercially available statistical software package (Statistical Package for Social Sciences for windows, Version 20).
Results
Thirty eyes of the 20 patients were included in this study. The mean age of patients was 27.43±3.57 years. Eleven patients (55%) were female and nine patients (45%) were male. Grading of KC in patients was as follows: grade II in 19 eyes (63.33%) and grade III in 11 eyes (36.66%) (Figures 1–3 and Table 1).
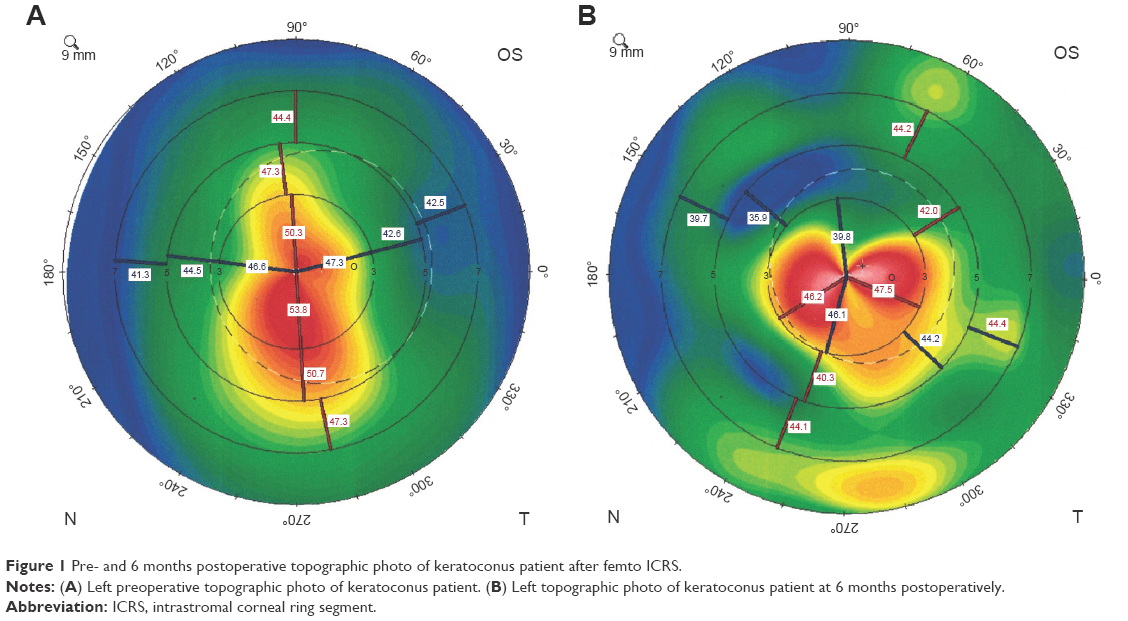 | Figure 1 Pre- and 6 months postoperative topographic photo of keratoconus patient after femto ICRS. |
 | Figure 2 Color photo showing intraoperative femtosecond laser Keraring implantation in keratoconus patient. |
 | Figure 3 Slit-lamp examination of keratoconus patient 6 months after femtosecond laser Keraring implantation. |
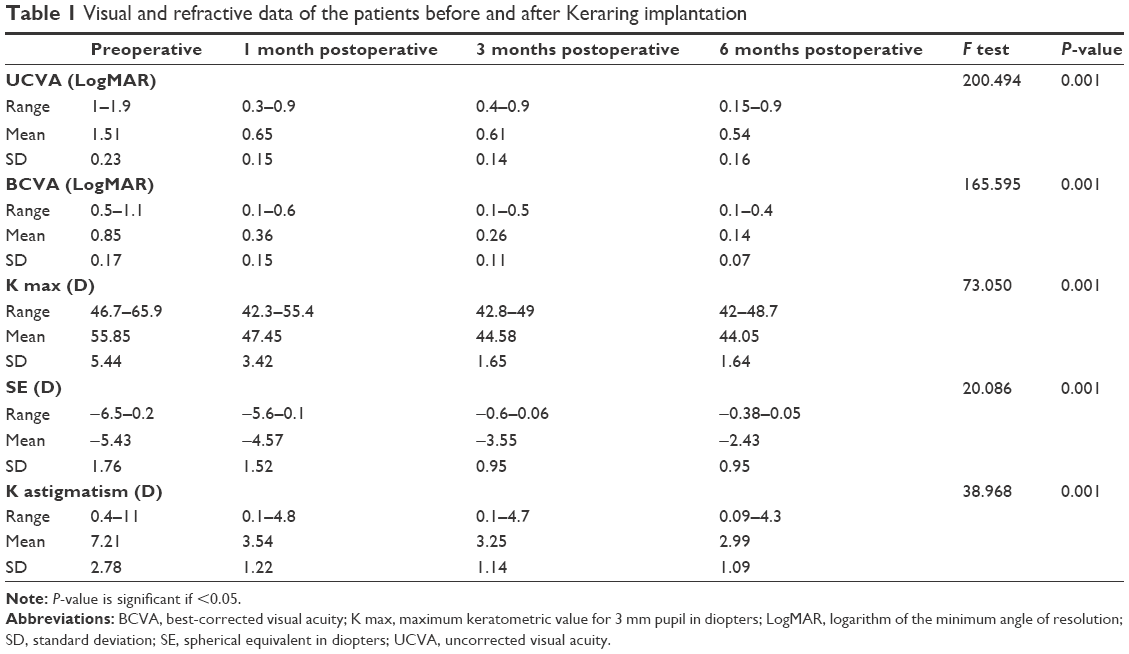 | Table 1 Visual and refractive data of the patients before and after Keraring implantation |
Ten patients had bilateral KC. The results were not affected in patients due to bilaterality or unilateralilty. Three eyes of two patients had follow-up <6 months postoperatively and were excluded from statistical analysis. No mutations were associated or identified in the patients.
Keraring segments were successfully implanted in all eyes. The follow-up period was 6 months postoperatively.
The preoperative mean LogMAR UCVA was 1.5±0.23. At 1 month postoperatively, it was 0.65±0.15; at 3 months postoperatively, it was 0.61±0.14, and at 6 months postoperatively, it was 0.54±0.16. There was a significant improvement in the mean LogMAR of UCVA after Keraring segment implantation at 6 months postoperatively (P=0.001).
The preoperative mean LogMAR BCVA was 0.85±0.17. At 1 month postoperatively, it was 0.35±0.15; at 3 months postoperatively, it was 0.26±0.11, and at 6 months postoperatively, it was 0.14±0.07.
There was a significant improvement in the mean LogMAR of BCVA after Keraring segment implantation at 6 months postoperatively (P=0.001).
The mean preoperative SE was −5.43±1.76 D. At 1 month postoperatively, it was −4.57±1.52 D. At 3 months postoperatively, it was −3.55±1.32 D. At 6 months postoperatively, it was −2.43±0.95 D. A significant reduction in SE was found (P=0.001).
The mean preoperative K astigmatism was 7.21±2.78 D. At 1 month postoperatively, it was 3.54±1.22 D. At 3 months postoperatively, it was 3.25±1.14 D. At 6 months postoperatively, it was 2.99±1.09 D. There was a significant reduction in the mean K astigmatism after Keraring segment implantation at 6 months postoperatively (P=0.001).
The mean preoperative K max was significantly decreased from 55.85±5.44 D preoperatively to 44.05±1.64 D at 6 months postoperatively (P=0.001).
No statistically significant differences were detected between 1 and 3 months of follow-up regarding the visual and the refractive outcomes.
No epithelial defects, white deposits in the segment tunnel, infections, segment migration to the incision site and corneal vascularization were observed postoperatively in the patients.
Discussion
ICRS (Keraring) implantation has been shown to be a minimally invasive, safe and effective procedure that may delay or even avoid the need for keratoplasty in patients with KC with a significant improvement in UCVA.14,15
Keraring implantation more centrally at a 5 mm diameter achieves a greater flattening of the central cornea and leads to more efficient correction of KC.16
Femtosecond laser and mechanical dissection are the two main techniques used for tunnel creation during ICRS implantation.11
In this retrospective clinical study, we attempted to evaluate the efficacy of femtosecond laser-assisted ICRS implantation (Keraring) in patients with KC.
Thirty eyes of 20 patients were included in this study. Grading of KC in patients was as follows: grade II in 19 eyes (63.33%) and grade III in 11 eyes (36.66%).
All eyes were followed up for 6 months postoperatively.
In our study, there was a significant improvement in the final LogMAR UCVA from 1.5±0.23 preoperatively to 0.54±0.16 at 6 months postoperatively (P=0.001). The final LogMAR BCVA was significantly improved from 0.85±0.17 preoperatively to 0.14±0.07 at 6 months postoperatively (P=0.001).
Kubaloglu et al17 compared the outcomes of Keraring ICRS implantation with mechanical and femtosecond laser tunnel creation. They reported an improvement in both UCVA and BCVA in 86% and 88% of eyes, respectively, with no statistically significant differences in the visual and refractive results between both groups.
Tunc et al18 reported that the mean LogMAR UCVA increased significantly from 1.36±0.64 preoperatively to 0.51±0.28 at 12 months after mechanical Keraring implantation (P=0.001). The mean preoperative LogMAR BCVA was significantly improved from 0.57±0.29 to 0.23±0.18 at 1 year postoperatively (P=0.001). Torquetti et al19 evaluated 10 years follow-up of intracorneal ring segments (Ferrara ring) in KC patients. They observed an improvement in both UCVA and BCVA in KC patients with a decrease in corneal thickness.
Jadidi et al20 evaluated 15 eyes of 15 patients with KC that were treated by mechanical Keraring implantation. They observed a significant improvement in the mean LogMAR UCVA from 0.79±0.48 preoperatively to 0.28±0.15 at 6 months after implantation (P=0.001). The mean preoperative LogMAR BCVA was significantly improved from 0.36±0.21 to 0.18±0.9 at 6 months after implantation (P=0.009).20 In our study, the mean preoperative K max was significantly reduced from 55.85±5.44 D preoperatively to 44.05±1.64 D at 6 months postoperatively P<0.001.
The preoperative mean K astigmatism was significantly reduced from 7.21±2.78 D preoperatively to 2.99±1.09 D at 6 months postoperatively. The reduction in keratometry was accompanied with an improvement in both UCVA and BCVA.
Kubaloglu et al17 reported a decrease in the mean K max value from 53.5 to 48.9 D and an improvement in the mean SE from −5.05 to −1.87 D at 1 year postoperatively in the femtosecond laser group.
Our results are in agreement with previous studies that reported significant corneal flattening changes after Keraring implantation.18,20,21
In our study, there was a statistically significant reduction in the mean preoperative SE from −5.43±1.76 D preoperatively to −2.43±0.95 D at 6 months postoperatively.
Coskunseven et al22 implanted ICRS assisted by femtosecond laser in KC patients. They reported a statistically significant reduction in the SE refractive error compared to that observed at the examination before implantation. Tunc et al18 reported a significant reduction in SE refractive error from −6.42±4.69 D preoperatively to −1.26±1.45 D (P=0.001) at 1 year postoperatively.
Shabayek and Alió16 reported that ICRS (Keraring) implantation with femtosecond laser was a safe and effective method for KC with an improvement in BCVA and a reduction in corneal higher-order aberrations. No statistically significant differences were detected between 1 and 3 months follow-up regarding the visual and the refractive outcomes in our study.
No complications such as epithelial defects, white deposits in the segment tunnel, infections, segment migration to the incision site and corneal vascularization were observed in our study. Hellstedt et al23 reported segment movement, corneal melt and exposure in 35% of patients. Also Kwitko and Severo24 reported a higher rate of extrusion using mechanical dissection for Keraring implantation.
Shabayek and Alió16 reported a case with late localized infectious keratitis 1 month after the procedure that was treated well with no improvement in the visual outcome. Using the femtosecond laser for corneal tunnel creation in Keraring implantation made the procedure easier with an accurate precise depth of implantation, symmetry of the tunnels and little or no complication, and increased the experience of the surgeons.
Further studies should investigate the effect of ICRS (Keraring) implantation on corneal aberrations in patients with KC.
The drawbacks in our study were the short-term follow-up, the lack of analysis of corneal aberrations and the lack of comparison with mechanical ICRS (Keraring) implantation.
Conclusion
Analysis of the outcomes after Keraring ICRS implantation showed a significant postoperative corneal flattening with a subsequent increase in UCVA and BCVA. Using the femtosecond laser for tunnel creation made the procedure easy and fast with an accurate precise depth of implantation and reduced the risk of operative and postoperative complications.
Acknowledgments
This work was self-funded by the authors. This study was presented as a poster in ESCRS 2015.
Disclosure
The authors report no conflicts of interest in this work.
References
Krachmer JH, Feder RS, Belin MW. Keratoconus and related non inflammatory corneal thinning disorders. Surv Ophthalmol. 1984;28(4):293–322. | ||
Fernández Meijide N. Keratoconus epidemiology. In: Albertazzi R, editor. Keratoconus: Guidelines for Diagnosis and Treatment. Buenos Aires, Argentina: Ediciones Cientificas Argentinas; 2010:11–15. | ||
Davidson AE, Hayes S, Hardcastle AJ, Tuft SJ. The pathogenesis of keratoconus. Eye (Lond). 2013;28(2):189–195. | ||
Rabinowitz YS. Keratoconus. Surv Ophthalmol. 1998;42(4):297–319. | ||
Gharaibeh AM, Muhsen SM, AbuKhader IB, Ababneh OH, Abu-Ameerh MA, Albdour MD. Keraring intrastromal corneal ring segments for correction of keratoconus. Cornea. 2012;31(2):115–120. | ||
Alió J, Salem TF, Artola A, Osman AA. Intracorneal rings to correct corneal ectasia after laser in situ keratomileusis. J Cataract Refract Surg. 2002;28(9):1568–1574. | ||
Lovisolo CF, Calossi A, Ottone AC. Intrastromal inserts in keratoconus and ectatic corneal conditions. In: Lovisolo CF, Fleming JF, Pesando PM, editors. Intrastromal Corneal Ring Segments. Canelli AT, Italy: Fabiano Editore; 2002:95–163. | ||
Kanellopoulos AJ, Pe LH, Perry HD, Donnenfeld ED. Modified intracorneal ring segment implantations (INTACS) for the management of moderate to advanced keratoconus: efficacy and complications. Cornea. 2006;25(1):29–33. | ||
Bourcier T, Borderie V, Laroche L. Late bacterial keratitis after implantation of intrastromal corneal ring segments. J Cataract Refract Surg. 2003;29(2):407–409. | ||
Ruckhofer J, Stoiber J, Alzner E, Grabner G; Multicenter European Corneal Correction Assessment Study Group. One-year results of European multicenter study of intrastromal corneal ring segments. Part 2: complications, visual symptoms, and patient satisfaction. J Cataract Refract Surg. 2001;27(2):287–296. | ||
Ertan A, Bahadir M. Topography-guided vertical implantation of Intacs using a femtosecond laser for the treatment of keratoconus. J Cataract Refract Surg. 2007;33(1):148–151. | ||
Burris TE. Intrastromal corneal ring technology: results and indications. Curr Opin Ophthalmol. 1998;9(4):9–14. | ||
Ganesh S, Shetty R, D’Souza S, Ramachandran S, Kurian M. Intrastromal corneal ring segments for management of keratoconus. Indian J Ophthalmol. 2013;61(8):451–455. | ||
Sansanayudh W, Bahar I, Kumar NL, et al. Intrastromal corneal ring segment SK implantation for moderate to severe keratoconus. J Cataract Refract Surg. 2010;36(1):110–113. | ||
Piñero DP, Alio JL, El Kady B, et al. Refractive and aberrometric outcomes of intracorneal ring segments for keratoconus: mechanical versus femtosecond-assisted procedures. Ophthalmology. 2009;116(9):1675–1687. | ||
Shabayek MH, Alió JL. Intrastromal corneal ring segment implantation by femtosecond laser for keratoconus correction. Ophthalmology. 2007;114(9):1643–1652. | ||
Kubaloglu A, Sari ES, Cinar Y, et al. Comparison of mechanical and femtosecond laser tunnel creation for intrastromal corneal ring segment implantation in keratoconus: prospective randomized clinical trial. J Cataract Refract Surg. 2010;36(9):1556–1561. | ||
Tunc Z, Helvacioglu F, Sencan S. Evaluation of intrastromal corneal ring segments for treatment of keratoconus with a mechanical implantation technique. Indian J Ophthalmol. 2013;61(5):218–225. | ||
Torquetti L, Ferrara G, Almeida F, et al. Intrastromal corneal ring segments implantation in patients with keratoconus: 10-year follow-up. J Refract Surg. 2014;30(1):22–26. | ||
Jadidi K, Mosavi SA, Nejat F, Naderi M, Janani L, Serahati S. Intrastromal corneal ring segment implantation (Keraring 355°) in patients with central keratoconus: 6-month follow-up. J Ophthalmol. 2015;2015:916385. | ||
Mirzaei M, Najafi A, Shahraki K, Taheri N, Mirzaei S. Clinical and topographical corneal changes after Keraring implantation in keratoconus patients. Adv Biosci Clin Med. 2014;3(1):40–45. | ||
Coskunseven E, Kymionis GD, Tsiklis NS, et al. One-year results of intrastromal corneal ring segment implantation (Keraring) using femtosecond laser in patients with keratoconus. Am J Ophthalmol. 2008;145(5):40–45. | ||
Hellstedt T, Mäkelä J, Uusitalo R, Emre S, Uusitalo R. Treating keratoconus with intacs corneal ring segments. J Refract Surg. 2005;21(3):236–246. | ||
Kwitko S, Severo NS. Ferrara intracorneal ring segments for keratoconus. J Cataract Refract Surg. 2004;30(4):812–820. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.