Back to Journals » OncoTargets and Therapy » Volume 11
Reformulating acute myeloid leukemia: liposomal cytarabine and daunorubicin (CPX-351) as an emerging therapy for secondary AML
Authors Chen EC, Fathi AT, Brunner AM
Received 1 February 2018
Accepted for publication 8 April 2018
Published 12 June 2018 Volume 2018:11 Pages 3425—3434
DOI https://doi.org/10.2147/OTT.S141212
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Samir Farghaly
Evan C Chen,1 Amir T Fathi,2 Andrew M Brunner2
1Department of Medicine, Massachusetts General Hospital, Boston, MA, USA; 2Department of Hematology/Oncology, Massachusetts General Hospital, Boston, MA, USA
Abstract: Despite increasing understanding of the pathobiology of acute myeloid leukemia (AML), outcomes remain dismal particularly for patients over the age of 60 years, a population enriched for therapy-related AML (tAML) and secondary AML (sAML). For decades, the standard of care for AML has been the combination of cytarabine and daunorubicin, typically delivered in combination as “7 + 3” induction. In 2017, a liposomal-encapsulated combination of daunorubicin and cytarabine (CPX-351, Vyxeos) was approved by the US Food and Drug Administration (FDA) for use in the treatment of newly diagnosed tAML or AML with myelodysplasia-related changes (AML-MRCs). CPX-351 was designed to deliver a fixed 5:1 molar ratio of cytarabine and daunorubicin, respectively, based on the hypothesis that ratiometric dosing may be more effective than the delivery of either drug at their maximum tolerated dose. In a Phase III trial of older patients with sAML aged 60–75 years, CPX-351 was compared to “7 + 3” and was associated with a higher overall survival, event-free survival, and higher rates of complete remission (CR) and CR with incomplete hematologic recovery (CRi). These data were the basis for the approval of this new drug for use in the treatment of AML, but questions remain regarding how to best administer this agent across AML subgroups. Future directions include evaluating dose intensification with CPX-351, combining this agent with targeted therapies, and better understanding the mechanism of improved responses in tAML and AML-MRC, two entities that are historically less responsive to cytotoxic agents. In summary, CPX-351 offers an exciting new change to the landscape of AML therapy.
Keywords: acute myeloid leukemia, AML, liposome, liposomal, Vyxeos, CPX-351, cytarabine, daunorubicin
Introduction
Acute myeloid leukemia (AML) is a cancer of hematopoietic progenitor cells, which is characterized by a proliferation of blast cells and loss of normal hematopoiesis. It predominantly impacts older adults with a median age of diagnosis of 68 years.1 In spite of substantial gains in the pathobiology of AML, outcomes remain poor at the population level. In particular, survival is dismal among patients diagnosed with AML over the age of 60 years, who also represent the majority of AML cases. This may be, in part, because this older group of patients is enriched for AML developing out of preceding myeloid malignancies (secondary AML, sAML) and AML arising after prior radiation or chemotherapy (therapy-related AML, tAML). The poor outcomes seen in older patients may also reflect excess toxicity of existing cytotoxic regimens among these patients as well as less frequent and shorter treatment responses. CPX-351 (Vyxeos, Jazz Pharmaceuticals), a liposomal formulation of cytarabine and daunorubicin in a 5:1 molar ratio, has emerged as a new treatment option for AML.2 The current review discusses the current treatment landscape of AML, specific challenges related to the subgroup of patients with sAML, and then focuses on the preclinical and clinical data supporting the use of CPX-351.
Current treatment landscape of AML
Induction chemotherapy for AML
For decades, the standard of care for treating AML has been the combination of the nucleoside analog, cytarabine, with an anthracycline, typically daunorubicin or idarubicin.3 Most often, these agents are administered using a 7-day continuous infusion of cytarabine with idarubicin or daunorubicin administered on days 1, 2, and 3, a combination typically referred to as “7 + 3.” Dosing schedules of “7 + 3” underwent a number of adjustments through trials run by the Cancer and Leukemia Group B (CALGB), eventually resulting in a dose of daunorubicin of 45 mg/m2 per day for 3 days and cytarabine at a dose of 100 mg/m2 per day via continuous infusion for 7 days. This was superior to 2 and 5 days of each respective drug and superior to 10 days of daunorubicin.4,5 The “7 + 3” resulted in remission rates of 60%–80% of younger adults (those under the age of 60 years) and 40%–60% of older adults (typically defined as patients over the age of 60 years).6
Many attempts to improve upon “7 + 3” have failed to conclusively supplant this regimen. The Southeastern Cancer Study Group compared idarubicin at 12 mg/m2 to daunorubicin for induction among younger patients, suggesting that idarubicin is similarly active in AML induction.7 Dose intensification of daunorubicin, at 90 mg/m2 compared to 45 mg/m2, results in higher remission rates and improved survival among younger patients but not older patients with AML.8,9 Variations on the administration of cytarabine and anthracycline, including substituting the continuous infusion of cytarabine with high-dose cytarabine, have been explored.9 Although some studies suggested a possible improvement in disease-free survival with high-dose cytarabine, there was no significant benefit in complete remission (CR) rate and overall survival (OS) and at a cost of more significant hematologic side effects.10,11 Thioguanine with a double induction protocol, or the addition of etoposide to induction, also failed to show significant improvements in CR rates or disease-free survival.12,13 More recently, encouraging responses were reported with the histone deacetylase (HDAC) inhibitor, vorinostat, added to the idarubicin and Ara-C (IA) backbone;14 however, this also failed to improve upon “7 + 3” in a Phase III study.15
Advances in targeting specific AML subgroups
Recent advancements in AML induction chemotherapy have largely been within specific, well-defined AML subpopulations, often characterized by recurrent, targetable genetic mutations. The clinical development of targeted therapies in AML is most advanced for agents targeting FLT3- or IDH-mutated proteins. For patients whose AML harbors mutations in FLT3, either an internal tandem duplication (ITD) or a tyrosine kinase domain (TKD) mutation, a Phase III trial of midostaurin added to standard “7 + 3” resulted in improved OS (HR for death, 0.78; one-sided p = 0.009) and event-free survival (EFS; HR for event or death, 0.78; one-sided p = 0.002).16 These findings led to the approval of this agent during induction and the first targeted therapy to alter induction therapy in decades. For IDH2-mutated AML, enasidenib, a selective IDH2 inhibitor, has also shown impressive responses in relapsed and refractory IDH2-mutated AML.17 Of the patients receiving enasidenib, 19% of those with relapsed/refractory AML achieved CR, while the overall response rate was 40%. Median OS was 9.3 months, and for those patients who had received at least 2 treatment regimens for AML prior to enasidenib, the median survival was 8.0 months. While these agents are shaping the standard of care for the subsets of patients with these mutations, the vast majority of AML patients do not harbor such mutations, and new, more effective therapies are desperately needed.
sAML: an unmet need for new therapies
Many of the gains seen in AML have been in younger patients,18 while patients over the age of 60 years at diagnosis have had minimal improvement in overall dismal survival outcomes.18,19 One reason may be the underlying genetic features of AML in older adults: sequencing of the disease of older patients with AML shows an increased frequency of complex mutation patterns and a greater proportion of unfavorable mutations than are seen in younger patients. Many of these mutations are similar to those seen in secondary AML (sAML), which develop from a preexisting hematologic neoplasm such as myelodysplastic syndrome (MDS) or a myeloproliferative neoplasm (MPN), or therapy-related AML (tAML), which arise following chemotherapy or radiation.20 Patients with “secondary-like” AML according to the mutational profile have worse outcomes than patients with de novo AML lacking such mutations.21 Regardless of mutation profile, the overall outcomes of patients with sAML, accounting for cytogenetics and age, are worse than the de novo AML population.22
New approaches are, therefore, critically needed for patients with AML that have poor outcomes with standard intensive induction, including sAML, tAML, and AML in older patients, in whom these conditions are enriched. Increasingly, trials are turning to less intensive therapeutic backbones, typically using one of the hypomethylating agents, azacitidine or decitabine. Such studies seek to minimize the toxicities that are associated with standard “7 + 3,” particularly for patients with less chemosensitive disease, by using a hypomethylating agent (HMA) as the treatment backbone. A recent multicenter, randomized trial comparing azacitidine to conventional care regimens, including standard induction chemotherapy, low-dose Ara-c, or supportive care only, suggested a trend toward improved OS for those treated with azacitidine compared to conventional care (10.4 vs 6.5 months, respectively, p = 0.1009).23 Whether certain older AML patients may benefit from intensive therapy over HMA therapies, or those with multiple medical comorbidities, remains controversial.24 As such, intensive chemotherapy remains the standard of care for younger patients and is a reasonable first-line treatment for a select group of older “fit” patients.
CPX-351, liposomal cytarabine and daunorubicin, for AML
Preclinical studies
CPX-351 (brand name Vyxeos) is a liposomal-encapsulated combination of cytarabine and daunorubicin, approved by the Food and Drug Administration (FDA) in August 2017 for use in the treatment of newly diagnosed tAML or AML with myelodysplasia-related changes (AML-MRCs), two AML subtypes with poor prognosis. CPX-351 was developed in part using preclinical models that predicted that chemotherapeutics may act antagonistically or synergistically depending on the proportional ratio of each agent as seen by tumor cells during administration. Historically, many chemotherapy regimens have been developed based on a maximum tolerated dose (MTD) identified in dose-finding studies; such an approach is grounded in an assumption that this dose is also associated with maximum efficacy. Standard practice when developing a multiagent chemotherapy regimen has been to first add one agent followed by maximization of its dose then adding a second agent and so forth to identify the maximum tolerated combination dose. Whether this also corresponds to the maximal efficacious combination may not always be known.
Another approach to chemotherapy dosing utilizes ratiometric dosing, whereby a certain dose ratio of two agents is evaluated to identify the maximal efficacy. This ratio may or may not represent the MTD of these agents. Mayer et al25 tested the approach of ratiometric dosing for chemotherapy in colorectal cancer, small cell lung cancer, and AML by using nanoscaled liposomes for drug delivery in vivo at a fixed molar ratio. For the combination of cytarabine and daunorubicin, the authors noted that a ratio of 5:1, respectively, yielded synergistic effects when used to treat the P388 leukemic cell line in vitro. To test this in vivo, CPX-351 was designed, a formulation of cytarabine and daunorubicin packaged within 100-nm diameter liposomes at the fixed molar ratio of 5:1. CPX-351 led to a higher response rate against P388 tumors compared to matched doses of the individual drugs packaged in liposomes as well as improved responses compared to a free drug cocktail of cytarabine and daunorubicin administered at their respective MTDs. Serologic studies revealed that CPX-351 maintained a 5:1 ratio of plasma levels of cytarabine and daunorubicin, as intended.
In addition to maintaining a specific ratio of cytarabine and daunorubicin, part of the rationale for CPX-351 was whether the pharmacokinetics of using a liposomally packaged agent may also improve treatment outcomes. Lim et al26 utilized Rag2 mice engrafted with the CCRF-CEM leukemia cell line to compare the effects of CPX-351 and the equivalent free drug cocktail. CPX-351 led to a more durable remission (77 days) than the free drug cocktail (49 days) and a higher and longer-lasting accumulation of cytarabine and daunorubicin in the bone marrow (BM), suggesting a longer drug elimination half-life with the liposomal formulation. Notably, CPX-351 selectively accumulated in leukemic CCRF-CEM cells than normal BM cells from the same mice based on the observation that CCRF-CEM cells had two times as much liposomal lipid than normal BM cells. A later study by Kim et al27 also showed the preferential accumulation of CPX-351 in leukemic cells vs normal BM cells. Although AML blasts showed similar sensitivity to both the liposomal and free drug formulations, normal BM showed five-fold more sensitivity to the free drug formulation than it did to CPX-351, suggesting perhaps that CPX-351 would have a relatively lessened impact on otherwise healthy hematopoietic progenitors. In addition, CPX-351 may alter the interactions between leukemic blasts and the BM niche. The BM microenvironment may play a role in supporting leukemogenesis;28 the efficacy seen with CPX-351, relative to the independent cytarabine and daunorubicin components, may be in part related to preferential uptake of liposomes into the BM.29
Clinical studies of CPX-351
Given this encouraging preclinical data, a Phase I dose escalation study was performed by Feldman et al30 for all patients with advanced AML or acute lymphoblastic leukemia (ALL). A total of 48 patients with advanced AML or ALL and high-risk MDS (defined as IPSS intermediate-2 or higher) were included in the study. CPX-351 was administered on days 1, 3, and 5, and the MTD was found to be 101 units/m2 (where each unit of CPX-351 contained 1 mg cytarabine and 0.44 mg daunorubicin). Overall, CPX-351 appeared to be tolerable; the most common side effects included hypertensive crisis (one patient), heart failure (defined as a decrease in left ventricular ejection fraction (LVEF) to <50%, one patient), and prolonged cytopenias leading to infection and bleeding (one patient). Nausea and vomiting were controllable with antiemetics, and a distinct maculopapular rash was seen in 71% patients which resolved with corticosteroids. Interestingly, of the 48 patients, only six patients exhibited alopecia. Notably, out of the 43 AML patients, the study resulted in CR for nine patients (21%) and CR with incomplete hematologic recovery (CRi) in one patient (2%). Eight of the nine patients achieving CR had previously received cytarabine- and daunorubicin-based treatment. Responses were seen at doses as low as 32 units/m2.
A follow-up report in 2012 expounded upon the adverse effects of CPX-351.31 Hematologic effects such as cytopenias were seen in doses as low as 12 units/m2 with a gradual dose-related increase in frequency and severity. At the highest tested dose of 134 units/m2, cytopenia-related adverse events (AEs) were common with febrile neutropenia (83%), infections of grade ≥3 severity (67%), bacteremia (33%), epistaxis (17%), and petechiae seen (17%). Non-hematologic effects were noted starting at 24 units/m2 with a shallower dose–response curve thereafter. Of the non-hematologic effects, stomatitis (83%), nausea (67%), rash (50%), vomiting (50%), cough (33%), and alopecia (33%, notably less alopecia than is seen with standard “7 + 3”) were most commonly observed. Dose-limiting adverse effects were seen at 134 units/m2 and included hypertensive crisis (one patient), possible anthracycline-associated cardiomyopathy in the setting of sepsis (one patient) and grade 4 (>56 days) neutropenia and thrombocytopenia (one patient).
A Phase II trial was subsequently completed in 2014, in which the efficacy of CPX-351 was compared to the traditional “7 + 3” treatment in newly diagnosed AML patients.32 This study enrolled patients who historically have poor responses to standard “7 + 3:” older patients with AML aged 60–75 years and all patients with sAML. Some investigator discretion was allowed for the control arm treatment, as patients could also receive 5 + 2 or intermediate-dose cytarabine following “7 + 3.” The dose of daunorubicin utilized in this study for the control arm was 60 mg/m2, but could be decreased to 45 mg/m2 in patients with advanced age, poor performance status, or reduced kidney or liver function. The consolidation regimen allowed for either “5 + 2” chemotherapy or for intermediate doses of cytarabine. Patients aged 60–69 years with de novo AML were classified as the “standard-risk” group, while patients aged 70–75 years, those with sAML, or those with complex karyotype (defined as ≥3 clonal abnormalities) were stratified into a predetermined “high-risk” group. Response was defined as a combined end point of CR and CRi.
This Phase II study showed that CPX-351 was associated with a trend toward higher response rates (CR and CRi) compared to “7 + 3,” although not statistically significant (66.7% vs 52.1%, p = 0.07; Figure 1). CPX-351 had a longer median time to response (48 vs 42 days), and a similar duration of response (8.9 vs 8.6 months). Higher CR rates were reported specifically in CPX-351 patients with adverse cytogenetics (as defined by National Comprehensive Cancer Network criteria; 77.3% vs 38.5%, p = 0.03) and sAML (57.6% vs 31.6%, p = 0.06). In the 24 months of follow-up, median OS was 14.7 vs 12.9 months, and median EFS was 6.5 vs 2.0 months between the CPX-351 and “7 + 3” groups. These outcomes were not significantly different between the groups, but favored CPX-351. Within a planned analysis of the sAML subgroup, CPX-351 was associated with a trend to improved OS (HR, 0.46; p = 0.1). Notably, CPX-351 was associated with prolonged cytopenias and an increased risk of infection; however, there was no difference in death from infections or 60-day mortality compared to “7 + 3” patients. There was in fact a trend toward lower 60-day mortality in the CPX-351 arm (4.7% vs 14.6%, p = 0.053). There was also some suggestion, in these studies, that CPX-351 may be associated with a slightly more tolerable toxicity profile than “7 + 3,” in part reflecting the differences in early mortality.
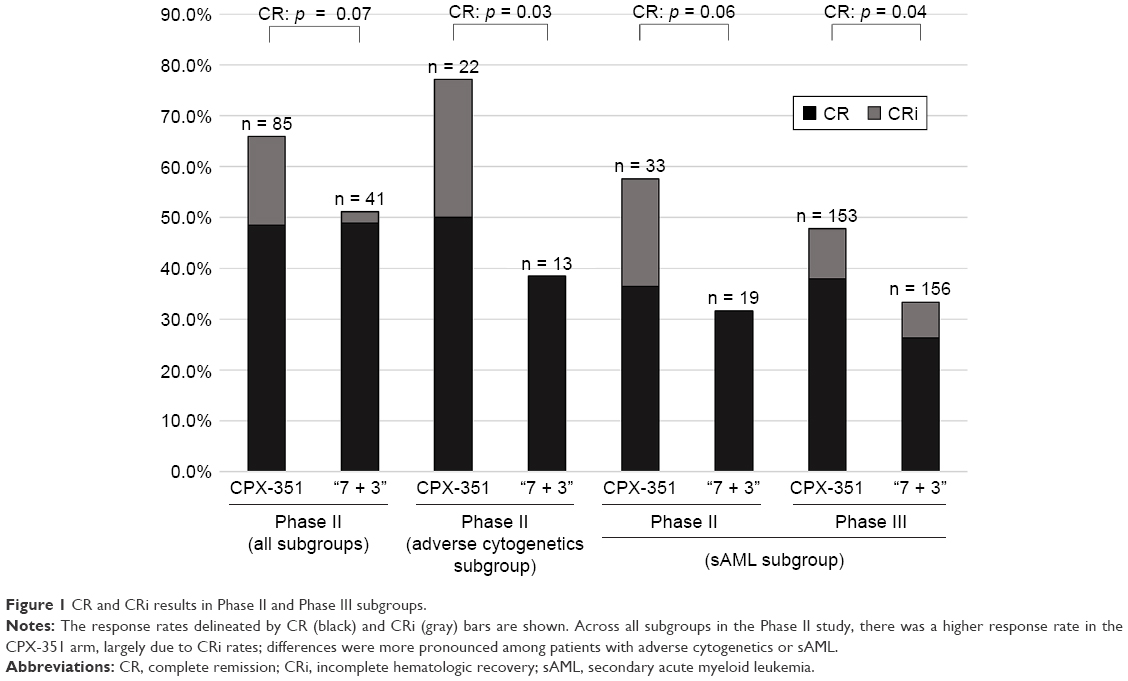 | Figure 1 CR and CRi results in Phase II and Phase III subgroups. |
Interestingly, this study allowed for patient in the “7 + 3” arm with refractory disease after induction to “cross over” and receive CPX-351 as salvage therapy. A total of 10 patients who had persistent disease after “7 + 3” received CPX-351 salvage, and four of these patients achieved clinical response, three a CR, and one a CRi.33 CPX-351 patients had higher response rates than their corresponding controls in the “7 + 3” group regardless of prior hypomethylating agent therapy. Older patients (age >70 years) also exhibited higher response rates with CPX-351.
Given the signal for possible benefit of CPX-351 in patients with refractory AML, a second Phase II trial was performed by Cortes et al34 to assess the efficacy of CPX-351 in patients aged 18–65 years with AML in the first relapse compared to the provider’s choice of conventional intensive salvage therapy. In this study, salvage therapies consisted of cytarabine (97.7% of the control group) and anthracycline (77.3%) with other agents such as etoposide (54.5%) or gemtuzumab ozogamicin (18.2%). CPX-351 was associated with a higher rate of CR (37% vs 32%) and CRi (12% vs 9%), but this did not result in a significant increase in the 1-year EFS or OS. However, for the subset of patients deemed to be poor risk per the European Prognostic Index, higher response rates were seen in the CPX-351 group (39.3% vs 27.6%, no formal analysis performed given small subgroup sizes) with a trend toward improved EFS (HR, 0.63; p = 0.08) and a significant improvement in OS (HR, 0.55; p = 0.02). Sixty-day mortality was also lower for poor-risk patients (16.1% vs 24.1%), again speaking to an encouraging signal relative to “7 + 3.”
More importantly, CPX-351 was studied in a pivotal Phase III trial comparing CPX-351 induction to standard “7 + 3,” using a daunorubicin dose of 60 mg/m2 in this arm.2 Patients could get two cycles of chemotherapy consolidation on trial, and in this study consolidation on the “7 + 3” arm was “5 + 2.” In this study, patients aged 60–75 years with untreated sAML (defined as a history of prior cytotoxic treatment, preceding MDS or chronic myelomonocytic leukemia (CMML) or having World Health Organization (WHO)-defined MDS-associated cytogenetic changes) were randomized to receive CPX-351 on days 1, 3, and 5, or to receive “7 + 3” induction. This AML subgroup was selected based upon the signals seen in the Phase II studies. Outcomes of interest included OS, EFS, CR + CRi, and 60-day mortality. Results showed that those patients treated with CPX-351 had a higher OS (HR, 0.69; p = 0.005; median OS 9.56 vs 5.95 months), EFS (HR, 0.74; p = 0.021), CR + CRi response (47.7% vs 33.3%; p = 0.016; Figure 1), and an improved 60-day mortality (13.7% vs 21.2%). Although previous experience had hypothesized that CPX-351 may yield a better toxicity profile, the rates of grade 3 or higher AEs were similar in frequency and severity in both arms (92% in CPX-351, 91% in “7 + 3”). In a planned subgroup analysis of tAML patients in this study, CPX-351 was associated with an improvement in outcomes similar to the overall treatment group with higher OS compared to standard “7 + 3” (HR, 0.49; median 12.17 vs 6.64 months), EFS (HR, 0.66; median 2.5 vs 1.64 months), and longer remission duration in the CPX-351-treated arm (HR, 0.50; 10.87 vs 6.11 months).38 Based on this study, in large part, the FDA approved CPX-351 for patients with newly diagnosed tAML or AML-MRC. The label interestingly extends to some populations outside the scope of the Phase III study, notably including adult AML patients regardless of age at diagnosis.
The study authors have subsequently further analyzed the Phase II and Phase III trial data to better understand the responses seen with CPX-351. Lancet et al35 pooled the sAML patients from both the combined Phase II and Phase III CPX-351 studies. They found that the CPX-351-treated cohort had higher OS (9.63 months) than the 7 + 3 cohort (5.59 months; HR, 0.64). OS at 1 year was 42% for CPX-351 and 27% for “7 + 3,” and rates of CR and CR + CRi were higher for CPX-351 than “7 + 3” (CR 36% vs 26%, respectively; CR + CRi 48% vs 33%, respectively). Overall, mortality rates were lower for CPX-351-treated patients at day 30 (5% vs 11%) and day 60 (12% vs 23%), and more CPX-351-treated patients went on to allogeneic transplant (34% vs 25% for “7 + 3”). An additional subgroup analysis was performed by Lin et al,41 who looked at the outcomes for the subset of patients from the Phase III trial with oligoblastic sAML, defined as BM blasts of 20%–29%, and previously classified as the MDS subgroup, refractory anemia with excess blasts in transformation (RAEB-T). They found a consistent improvement in median OS in the CPX-351 cohort compared to the “7 + 3” group (12.50 vs 5.95 months).32 From these studies, other factors associated with improved survival included lower Eastern Cooperative Oncology Group (ECOG) performance status (p = 0.034), non-adverse karyotype (p < 0.001), platelet count >50 (p < 0.001), white blood cell count (WBCs) <20 (p = 0.041) as well as treatment with CPX-351 (p = 0.008).36
While the overall number of AEs for patients treated with CPX-351 did not appear to differ from those receiving “7 + 3,” further study was performed to better characterize the toxicity profile in the Phase III trial. There was a greater proportion of patients treated with CPX-351 who received consolidation therapy compared to 7 + 3 (32% vs 21% received consolidation 1 and 15% vs 8% received consolidation 2).37 Evaluating the toxicity rates for patients for the duration of time on treatment, CPX-351 appeared to have a lower rate of AE events per person-time on trial. Patients on the CPX-351 arm had fewer AEs per person-year compared to those given “7 + 3” (75.68 vs 87.2 events/person-year and 12.2 vs 13.5 grade ≥3 AEs per person-year) although the confidence estimates were broad. Curiously, the percentage of patients experiencing common serious AEs were higher in the CPX-351 group, including febrile neutropenia (8% of CPX-351-treated patients vs 5% of patients receiving “7 + 3”), respiratory failure (7% vs 5%), systolic heart failure (6% vs 6%), sepsis (8% vs 3%), and pneumonia (7% vs 4%). Of note, this does not incorporate time at risk for events, which was longer for the CPX-351 patients as they had a longer duration of treatment. The higher number of serious AEs for CPX-351-treated patients was seen despite the observation that the cumulative doses of cytarabine and daunorubicin for patients alive in the CPX-351 group were lower than the cumulative doses for patients alive in the “7 + 3” group.38 Nonetheless, there was a lower mortality at 30 days (5.9% in the CPX-351 arm vs 10.6% in the “7 + 3” arm) and 60 days (13.8% vs 21.2%, respectively). It is possible that the higher remission rate drives this difference with more patients in the “7 + 3” arm dying related to refractory leukemia. Further study is needed to better understand these findings.
Incorporating CPX-351 into practice
The approval of CPX-351 has coincided with a rapidly changing AML landscape and added to an increasingly complicated up-front treatment decision-making process. A number of questions arise from the clinical trial leading to its approval, particularly as to the optimal patient populations to receive CPX-351 induction. It is not known whether CPX-351, at the doses employed in the Phase III study, would also be more efficacious than “7 + 3” with daunorubicin dosed at 90 mg/m2. It is for that reason as well that, for patients aged 65 years and younger who may be candidates for anthracycline intensification to 90 mg/m2 or to similarly high doses of idarubicin, CPX-351 may not be the agent of first choice, although one could argue that sAML is biologically similar irrespective of the age at diagnosis. Moreover, the anecdotal tolerability of CPX-351 has not been borne out in further analyses to date and may be further tempered if the anthracycline dose of CPX-351 is increased, as was seen in the dose escalation studies.
Moreover, the exact mechanism to explain an improvement in outcomes with CPX-351, especially in sAML or tAML, is unclear. It has long been recognized that these subgroups do not respond as well to standard induction, but why this liposomal formulation would improve outcomes in this group without any difference in outcomes in other AML subgroups is an area for further study. It is not known if this reflects the molar ratio of cytarabine and daunorubicin, although prior studies to explore different doses of cytarabine did not seem to have a marked dose effect.4,5,9 It may represent the longer exposure afforded by the liposomal formulation, selective uptake of this agent or concentration in the marrow, or another as-of-yet undetermined mechanism. Moreover, it is unclear how the survival difference in the trial relates to the initial induction therapy decision. In the pooled sAML analysis, there was approximately a 15% OS benefit at 1 year with CPX-351 compared to “7 + 3;” more patients on the CPX-351 arm also were able to proceed to allogeneic transplant, perhaps explaining, in part, this improvement. Prolonged cytopenias were more common among patients treated with CPX-351, and this is often a cause of induction-related mortality; the improved early mortality may therefore reflect higher rates of refractory disease in the “7 + 3” patients. Further understanding of the causes of death in each arm may thus be illustrative.
Nonetheless, the excitement around CPX-351, particularly in a traditionally refractory subset of AML, has led to a number of new studies of this agent in various settings. Given its activity in sAML and tAML, there is interest in exploring CPX-351 in other related settings, such as myelodysplasia, or as a maintenance or consolidation agent for high-risk disease (Table 1). Similarly, as the landscape of AML therapy evolves to incorporate therapies targeting specific mutations, strategies to add selective FLT3 or IDH inhibitors to CPX-351 may offer further advances to current AML treatment.
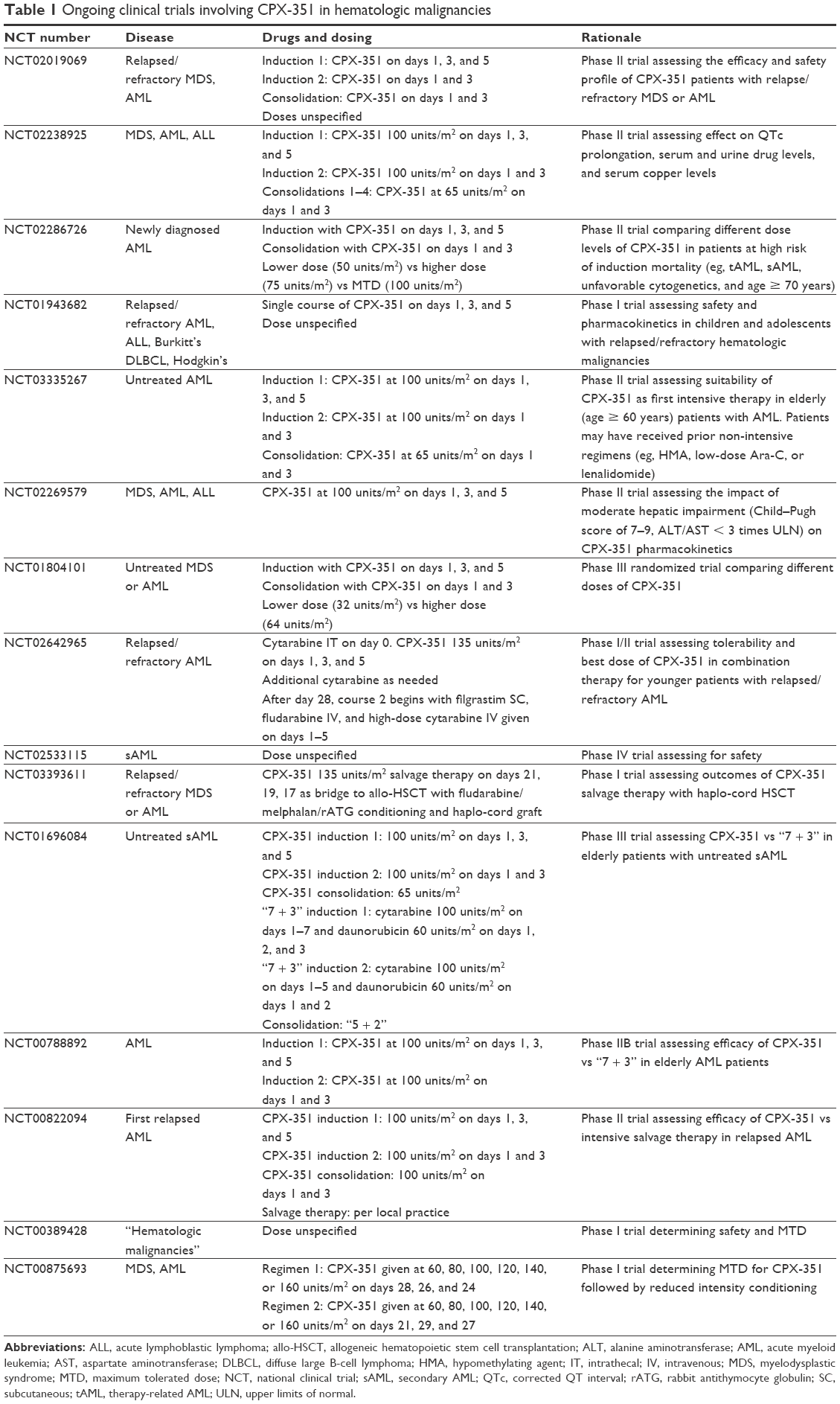 | Table 1 Ongoing clinical trials involving CPX-351 in hematologic malignancies |
Conclusion
CPX-351 offers a new active therapy in the treatment of AML. It appears to be more effective than standard “7 + 3” induction for patients with sAML, historically a group with dismal outcomes. In practice, it also affords some clinical benefits such as limited alopecia and shorter infusions (2 hours on days 1, 3, and 5, rather than a 7-day continuous infusion) as well as lower rates of early mortality, but is associated with prolonged cytopenias. Some caution should be taken in giving this to younger patients who would otherwise be candidates for anthracycline dose intensification as well as for other AML indications with favorable survival outcomes such as “7 + 3” + gemtuzumab ozogamicin for patients with favorable cytogenetic risk and select patients with intermediate-risk AML,39,40 or “7 + 3” + midostaurin for FLT3-mutated AML.16 As such, further study is needed to fully establish the role of CPX-351 in AML treatment.
Disclosure
AMB receives research funding to his institution from Celgene, Takeda, and Novartis and served on an advisory board for Celgene. ATF has consulted for and received clinical trial support from Celgene Corporation and Seattle Genetics, served on advisory boards for Agios, Celgene, and Jazz, and received clinical trial support from Takeda and Celgene. ECC reports no conflicts of interest in this work.
References
Howlader N, Noone A, Krapcho M, et al [webpage on the Internet]. SEER Cancer Statistics Review, 1975–2014. Bethesda, MD: National Cancer Institute; 2017. Available from: https://seer.cancer.gov/csr/1975_2014/. Accessed April 25, 2018. | ||
Lancet JE, Uy GL, Cortes JE, et al. Final results of a phase III randomized trial of CPX-351 versus 7+3 in older patients with newly diagnosed high risk (secondary) AML. J Clin Oncol. 2016;34(15_suppl):7000. | ||
Preisler HD, Anderson K, Rai K, et al. The frequency of long-term remission in patients with acute myelogenous leukaemia treated with conventional maintenance chemotherapy: a study of 760 patients with a minimal follow-up time of 6 years. Br J Haematol. 1989;71(2):189–194. | ||
Rai KR, Holland JF, Glidewell OJ, et al. Treatment of acute myelocytic leukemia: a study by cancer and leukemia group B. Blood. 1981;58(6):1203–1212. | ||
Preisler H, Davis RB, Kirshner J, et al. Comparison of three remission induction regimens and two postinduction strategies for the treatment of acute nonlymphocytic leukemia: a cancer and leukemia group B study. Blood. 1987;69(5):1441–1449. | ||
Estey E, Smith TL, Keating MJ, McCredie KB, Gehan EA, Freireich EJ. Prediction of survival during induction therapy in patients with newly diagnosed acute myeloblastic leukemia. Leukemia. 1989;3(4):257–263. | ||
Vogler WR, Velez-Garcia E, Weiner RS, et al. A phase III trial comparing idarubicin and daunorubicin in combination with cytarabine in acute myelogenous leukemia: a Southeastern Cancer Study Group Study. J Clin Oncol. 1992;10(7):1103–1111. | ||
Fernandez HF, Sun Z, Yao X, et al. Anthracycline dose intensification in acute myeloid leukemia. N Engl J Med. 2009;361(26):1249–1259. | ||
Lowenberg B, Ossenkoppele GJ, van Putten W, et al. High-dose daunorubicin in older patients with acute myeloid leukemia. N Engl J Med. 2009;361(13):1235–1248. | ||
Weick JK, Kopecky KJ, Appelbaum FR, et al. A randomized investigation of high-dose versus standard-dose cytosine arabinoside with daunorubicin in patients with previously untreated acute myeloid leukemia: a Southwest Oncology Group study. Blood. 1996;88(8):2841–2851. | ||
Bishop JF, Matthews JP, Young GA, et al. A randomized study of high-dose cytarabine in induction in acute myeloid leukemia. Blood. 1996;87(5):1710–1717. | ||
Bishop JF, Lowenthal RM, Joshua D, et al. Etoposide in acute nonlymphocytic leukemia. Australian Leukemia Study Group. Blood. 1990;75(1):27–32. | ||
Buchner T, Hiddemann W, Wormann B, et al. Double induction strategy for acute myeloid leukemia: the effect of high-dose cytarabine with mitoxantrone instead of standard-dose cytarabine with daunorubicin and 6-thioguanine: a randomized trial by the German AML Cooperative Group. Blood. 1999;93(12):4116–4124. | ||
Garcia-Manero G, Tambaro FP, Bekele NB, et al. Phase II trial of vorinostat with idarubicin and cytarabine for patients with newly diagnosed acute myelogenous leukemia or myelodysplastic syndrome. J Clin Oncol. 2012;30(18):2204–2210. | ||
Garcia-Manero G, Othus M, Pagel JM, et al. SWOG S1203: a randomized phase III study of standard cytarabine plus daunorubicin (“7+3”) therapy versus idarubicin with high dose cytarabine (IA) with or without vorinostat (IA+V) in younger patients with previously untreated acute myeloid leukemia (AML). Abstract #901. Presented at: The 2016 ASH Annual Meeting, San Diego, USA; 2016. | ||
Stone RM, Mandrekar SJ, Sanford BL, et al. Midostaurin plus chemotherapy for acute myeloid leukemia with a FLT3 mutation. N Engl J Med. 2017;377(5):454–464. | ||
Stein EM, DiNardo CD, Pollyea DA, et al. Enasidenib in mutant IDH2 relapsed or refractory acute myeloid leukemia. Blood. 2017;130:722–731. | ||
Burnett A, Wetzler M, Lowenberg B. Therapeutic advances in acute myeloid leukemia. J Clin Oncol. 2011;29(5):487–494. | ||
Bower H, Andersson TM, Bjorkholm M, Dickman PW, Lambert PC, Derolf AR. Continued improvement in survival of acute myeloid leukemia patients: an application of the loss in expectation of life. Blood Cancer J. 2016;6:e390. | ||
Appelbaum FR, Gundacker H, Head DR, et al. Age and acute myeloid leukemia. Blood. 2006;107(9):3481–3485. | ||
Lindsley RC, Mar BG, Mazzola E, et al. Acute myeloid leukemia ontogeny is defined by distinct somatic mutations. Blood. 2015;125(9):1367–1376. | ||
Granfeldt Ostgard LS, Medeiros BC, Sengelov H, et al. Epidemiology and clinical significance of secondary and therapy-related acute myeloid leukemia: a national population-based cohort study. J Clin Oncol. 2015;33(31):3641–3649. | ||
Dombret H, Seymour JF, Butrym A, et al. International phase 3 study of azacitidine vs conventional care regimens in older patients with newly diagnosed AML with >30% blasts. Blood. 2015;126(3):291–299. | ||
Sorror ML, Storer BE, Elsawy M, et al. Intensive versus non-intensive induction therapy for patients (Pts) with newly diagnosed acute myeloid leukemia (AML) using two different novel prognostic models. Blood. 2015;128:216. | ||
Mayer LD, Harasym TO, Tardi PG, et al. Ratiometric dosing of anticancer drug combinations: controlling drug ratios after systemic administration regulates therapeutic activity in tumor-bearing mice. Mol Cancer Ther. 2006;5(7):1854–1863. | ||
Lim WS, Tardi PG, Dos Santos N, et al. Leukemia-selective uptake and cytotoxicity of CPX-351, a synergistic fixed-ratio cytarabine:daunorubicin formulation, in bone marrow xenografts. Leuk Res. 2010;34(9):1214–1223. | ||
Kim HP, Gerhard B, Harasym TO, Mayer LD, Hogge DE. Liposomal encapsulation of a synergistic molar ratio of cytarabine and daunorubicin enhances selective toxicity for acute myeloid leukemia progenitors as compared to analogous normal hematopoietic cells. Exp Hematol. 2011;39(7):741–750. | ||
Ghobrial IM, Detappe A, Anderson KC, Steensma DP. The bone-marrow niche in MDS and MGUS: implications for AML and MM. Nat Rev Clin Oncol. 2018;15(4):219–233. | ||
Tardi P, Wan CP, Mayer L. Passive and semi-active targeting of bone marrow and leukemia cells using anionic low cholesterol liposomes. J Drug Target. 2016;24(9):797–804. | ||
Feldman EJ, Lancet JE, Kolitz JE, et al. First-in-man study of CPX-351: a liposomal carrier containing cytarabine and daunorubicin in a fixed 5:1 molar ratio for the treatment of relapsed and refractory acute myeloid leukemia. J Clin Oncol. 2011;29(8):979–985. | ||
Feldman EJ, Kolitz JE, Trang JM, et al. Pharmacokinetics of CPX-351; a nano-scale liposomal fixed molar ratio formulation of cytarabine:daunorubicin, in patients with advanced leukemia. Leuk Res. 2012;36(10):1283–1289. | ||
Lancet JE, Cortes JE, Hogge DE, et al. Phase 2 trial of CPX-351, a fixed 5:1 molar ratio of cytarabine/daunorubicin, vs cytarabine/daunorubicin in older adults with untreated AML. Blood. 2014;123(21):3239–3246. | ||
Lancet JE, Feldman EJ, Cortes JE, Hogge DE, Tallman MS. CPX-351 in AML after failed induction with cytarabine and daunorubicin. J Clin Oncol. 2016;28(no. 15_suppl):6572. | ||
Cortes JE, Goldberg SL, Feldman EJ, et al. Phase II, multicenter, randomized trial of CPX-351 (cytarabine:daunorubicin) liposome injection versus intensive salvage therapy in adults with first relapse AML. Cancer. 2015;121:234–242. | ||
Lancet JE, Ritchie EK, Uy GL, et al. Efficacy and safety of CPX-351 versus 7+3 in older adults with secondary acute myeloid leukemia: combined subgroup analysis of phase 2 and phase 3 studies. Blood. 2017;130:2657. | ||
Uy GL, Lancet JE, Cortes JE, et al. Multivariate efficacy analysis of a randomized, phase 3 study of CPX-351 versus 7+3 in older adults with treatment-related acute myeloid leukemia (AML) or AML with myelodysplasia-related changes. Blood. 2017;130:2647. | ||
Medeiros BC, Lancet JE, Cortes JE, et al. Rates of adverse events per patient-year in a randomized, phase 3 study of CPX-351 versus 7+3 in older adults with newly diagnosed, treatment-related acute myeloid leukemia (AML) or AML with myelodysplasia-related change. Blood. 2017;130:1366. | ||
Banerjee K, Wang Q, Wang J, Gibbons J. CPX-351 exposure-response based on cumulative dose of cytarabine and daunorubicin in patients with newly diagnosed, treatment-related acute myeloid leukemia (AML) or AML with myelodysplasia-related changes. Blood. 2017;130:1360. | ||
Rowe JM, Lowenberg B. Gemtuzumab ozogamicin in acute myeloid leukemia: a remarkable saga about an active drug. Blood. 2013;121(24):4838–4841. | ||
Castaigne S, Pautas C, Terre C, et al. Effect of gemtuzumab ozogamicin on survival of adult patients with de-novo acute myeloid leukaemia (ALFA-0701): a randomised, open-label, phase 3 study. Lancet. 2012;379(9825):1508–1516. | ||
Lin TL, Uy GL, Wieduwilt MJ, et al. Subanalysis of patients with secondary acute myeloid leukemia (sAML) with refractory anemia with excess of blasts in transformation (RAEB-t) enrolled in a phase 3 study of CPX-351 versus conventional 7+3 cytarabine and daunorubicin. Blood. 2017;130:1698. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.