Back to Journals » Clinical Ophthalmology » Volume 19
Reduced Ocular Surface Inflammation in SMILE Patients: The Beneficial Outcome of 0.1% Ciclosporin Cationic Emulsion Treatment
Received 5 June 2025
Accepted for publication 25 July 2025
Published 4 August 2025 Volume 2025:19 Pages 2565—2573
DOI https://doi.org/10.2147/OPTH.S536742
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Alex LK Ng,1,2 Douglas KT Lam1,2
1Hong Kong Ophthalmic Associates, Hong Kong SAR, People’s Republic of China; 2Hong Kong Eye Day Surgery Centre, Hong Kong SAR, People’s Republic of China
Correspondence: Alex LK Ng, Hong Kong Ophthalmic Associates, 26/F, New World Tower I, 18 Queen’s Road, Central, Hong Kong SAR, People’s Republic of China, Tel +852 2526 6198, Fax +852 2810 9477, Email [email protected]
Background: After laser refractive surgery, dry eye disease is a common issue, primarily caused by inflammation. In a cohort of patients undergoing small incision lenticule extraction (SMILE), we examined the impact of anti-inflammatory drug ciclosporin (0.1% in cationic emulsion; CsA-CE) on the corneal fluorescein staining (CFS) score and other indicators of dry eye disease.
Methods: This non-randomized, interventional, comparative study enrolled 30 patients undergoing SMILE, who received a once-daily, preservative-free, single-dose formulation of CsA-CE for one month following surgery. Tear osmolarity, ocular surface disease index (OSDI) scores, and CFS scores were measured after one- and three-months following surgery and compared to a control group (n=30). In the CsA-CE group, 26 patients completed the follow-up at Month 1, compared to 28 patients in the control group. At three-months follow-up, 22 patients in the CsA-CE group and 23 in the control group remained.
Results: At Month 1 and Month 3 postoperative follow-up, the CsA CE group’s CFS scores were significantly lower compared to controls: 0.31 ± 0.74 vs 0.75 ± 0.89 (P = 0.02) and 0.05 ± 0.21 vs 0.43 ± 0.84 (P = 0.04), respectively. Mean CFS scores of CsA-CE group were 0.44 (Month 1) and 0.38 (Month 3) lower postoperatively, compared to the control group. Tear osmolarity and OSDI scores, however, did not significantly differ between the two groups and stayed within normal bounds. With 57.7% of patients reporting no instillation site pain and no other side effects, the treatment was well-tolerated.
Conclusion: The anti-inflammatory effect of CsA-CE application in the early postoperative period after SMILE resulted in significantly lower CFS scores at Months 1 and 3 in comparison to the control group. These results suggest that 0.1% CsA-CE treatment lowers ocular surface damage and might thus benefit the recovery process of patients treated with this form of laser refractive surgery.
Keywords: SMILE, refractive surgery, dry eye disease, ciclosporin, ocular surface
Background
Hong Kong has a very high prevalence of myopia, and the demand for laser refractive surgery remains high. Recently, small incision lenticule extraction (SMILE) has gained popularity, and multiple studies have consistently shown comparable results to that of laser in situ keratomileusis (LASIK).1,2 Although both procedures have a very high patient satisfaction rate with a good safety and efficacy profile, post-laser refractive surgery dry eye disease (DED) continues to be a prevalent clinical issue that can affect patients’ recovery and quality of life.3
The pathogenesis of DED after laser refractive surgery is multifactorial.3–5 In LASIK and SMILE procedures, the creation of the flap or the incision involves vertical cutting of the sub-basal nerve plexus, causing corneal denervation that may lead to neurotrophic dry eye and a reduced cornea-blink reflex. During the corneal wound healing process, associated inflammatory responses may result in an up-regulation of pro-inflammatory cytokines, such as interleukin-6, on the ocular surface. This in turn may increase tear osmolarity and further aggravate ocular surface inflammation.6
Although post-refractive surgery DED is usually temporary, patients can experience blurring of vision and fluctuations in refractive error, as well as significant corneal punctate epithelial damage in the early postoperative period. This can reduce overall satisfaction with treatment and prolong the time necessary for full visual recovery.7 To improve patient outcomes, it is common for post-refractive surgery DED to be treated with artificial tears, gels, anti-inflammatory agents, punctal plugs or autologous serum tears.5 In particular, the control of ocular surface inflammation is now recognized as having a pivotal role in the management of DED.
In recent years, 0.1% ciclosporin A in cationic emulsion (CsA-CE; Ikervis, Santen Pharmaceutical) has gained popularity as a once-daily, topical anti-inflammatory agent for treating DED. It was found to be able to significantly improve the clinical manifestations seen in patients affected by moderate-to-severe DED, most notably when assessed via corneal fluorescein staining (CFS).8–12 CFS is one of the key parameters examined in pivotal trials involving CsA.11,13 Importantly, studies using conjunctival epithelial biopsies have shown that decreased corneal staining can reflect a reduction in inflammatory markers on the ocular surface.13 CsA-CE is thought to act mainly not only by inhibition of T-cell activation but also via lowering inflammatory cytokines in the conjunctiva, leading to reduced inflammation on the ocular surface. While previous studies have shown success with CsA in managing DED after LASIK,14,15 evidence supporting its use in the context of SMILE remains limited. It has also been demonstrated during the early postoperative period after SMILE that both dry eye symptoms and CFS can worsen.16 In the current study, we examined the hypothesis that 0.1% CsA-CE treatment immediately after SMILE surgery may down-regulate the surgery-induced inflammatory response on the ocular surface, thereby reducing ocular surface damage (assessed via CFS) and DED symptoms (assessed via OSDI) in the early postoperative period.
Materials and Methods
Study Design
This was a non-randomized, interventional, comparative study evaluating the effects of 0.1% CsA-CE one-month treatment on induced inflammatory response on the ocular surface after SMILE, compared with an age-matched, untreated control group. Briefly, the control group consisted of 30 consecutive patients, undergoing SMILE surgery, and selected based solely on appointment time. The next 30 consecutive patients undergoing SMILE were treated with 0.1% CsA-CE immediately after surgery (CsA-CE group). All patients were of Chinese ethnicity.
From August to December 2019, all procedures were carried out at the Hong Kong Eye Day Surgery Centre. Prior to SMILE, every patient had a thorough ophthalmic evaluation and was free of ocular comorbidities except myopia and myopic astigmatism. Each had a corrected distance visual acuity (CDVA) of 20/20 or higher prior to surgery. Unstable refraction, topographic evidence of forme fruste keratoconus, serious eye conditions, prior corneal surgery, autoimmune diseases, or drugs known to impair wound healing or worsen DED were among the exclusion criteria for SMILE. Pregnant and lactating women were also excluded from our study.17 In addition, patients with any symptomatic DED, corneal staining before surgery (confirmed with fluorescein in all cases), abnormal tear break-up time (TBUT) or tear meniscus height, or patients who received any steroids or CsA treatment prior to surgery, were also excluded. Patients were followed up at postoperative Month 1 and Month 3; those who missed one or more follow-up consultations were excluded from the analysis.
The Declaration of Helsinki’s guiding principles were followed when conducting the study. Prior to surgery, each patient signed an informed consent form. Before the study started, the Hong Kong Eye Day Surgery Centre ethics committee (DSC2019-001) examined and approved the study protocol.
Surgical Technique and 0.1% CsA-CE Treatment
A previously described surgical technique was used to perform the SMILE procedures using the 500 kHz VisuMax femtosecond laser (ZEISS).17 Two experienced SMILE surgeons (the authors) alternatively carried out each surgery. The following parameters were used: cap thickness, 100 μm; cap diameter, 7.6 mm; lenticule diameter, 6.5 mm with a transition zone of 0.1 mm; cut energy, 1.4 μJ; spot and tracking distance, 2.0–3.0 μm and peripheral incision, 2.5 mm. Postoperatively, the following drug regimen was prescribed for both control and CsA-CE groups: 0.3% tobramycin + 0.1% dexamethasone (TobraDex, Novartis) QID for 1 week; and hyaluronic acid-containing artificial tears QID for 1 month (OptiveFusion, AbbVie). Patients were instructed to start using these eye drops on the day of surgery. In addition, for the CsA-CE group, an unpreserved single-dose of 0.1% CsA-CE (Ikervis, Santen Pharmaceutical) was prescribed once daily before bedtime for 1 month, starting on the day of surgery.
Data Collection and Statistical Analysis
Patient demographics and ocular parameters [refractive error (spherical equivalence, SEQ), Ocular Surface Disease Index (OSDI) score, tear osmolarity] were recorded at baseline. OSDI score and tear osmolarity were assessed at postoperative Month 1 and Month 3 visits, and corneal fluorescein staining (CFS) was assessed by operating surgeon at postoperative Week 1, Month 1 and Month 3.
The TearLab osmometer (TearLab Corporation) was used to measure the tear osmolarity of both eyes, and the OSDI questionnaire18 was utilized to assess the symptoms of DED. As recommended by the manufacturer, the value for the patient’s eye with the highest reading was used to determine their tear osmolarity.19 Prior to the tear osmolarity measurement, none of the patients received any artificial tears or other eye drops. To determine the CFS score, a slit lamp examination was conducted. The conjunctival sac was instilled with sodium fluorescein, and the staining was evaluated using the Oxford scoring system (0–5).20 The mean score from both eyes was used for analysis.
During the study, all adverse events (AEs) were recorded. In the CsA-CE group, patients’ subjective tolerability to transient instillation site pain, a common mild side effect when applying the medication, was graded and scored (Grade 0, no pain; Grade 1, mild instillation site pain but well tolerated; Grade 2, moderate instillation site pain but still tolerable; Grade 3: intolerable instillation site pain).
Patient characteristics and ocular parameters were summarized using descriptive statistics. Fisher’s exact test was used for categorical variables, and the non-parametric Mann–Whitney U-test was used for continuous variables to assess the statistical significance of differences between the CsA-CE and control groups. Statistical significance was defined as a P value of less than 0.05. SPSS Version 21.0 (IBM Corporation) was used for statistical analysis.
Results
Thirty patients (30) were enrolled in each group. Of these, 26 patients in the CsA-CE group and 28 patients in the control group completed one month of follow-up; at Month 3, there were 22 patients in the CsA-CE group and 23 patients in the control group. Patients’ reasons for missing follow-up visits were related to disruptions associated with the social movement in Hong Kong in late 2019 and the COVID-19 outbreak since early 2020. There were no discernible patterns in the dropout patients.
Baseline characteristics of patients are summarized in Table 1. The average age (mean ± SD) was 31.9 ± 6.2 years in the CsA-CE group and 31.6 ± 7.9 years in the control group. In both groups, most patients were female. At baseline, both groups had normal OSDI scores (<12) and normal tear osmolarity (<308 mOsm/L). There were no statistically significant differences between the groups in OSDI scores, tear osmolarity or SEQ at baseline. All eyes aimed for a plano correction and had a preoperative CDVA of 20/20 or better. Postoperatively, no eyes had a reduction in CDVA at either Month 1 or Month 3. At Month 3, the mean ± SD SEQ in the CsA-CE group was −0.07 ± 0.34 diopters (D) in the right eye and −0.04 ± 0.41 diopters (D) in the left eye. In the control group, mean ± SD SEQ at Month 3 was −0.07 ± 0.31 D in the right eye and −0.03 ± 0.32 D in the left eye. There were no significant differences between groups (right eye: P = 0.67, left eye: P = 0.95).
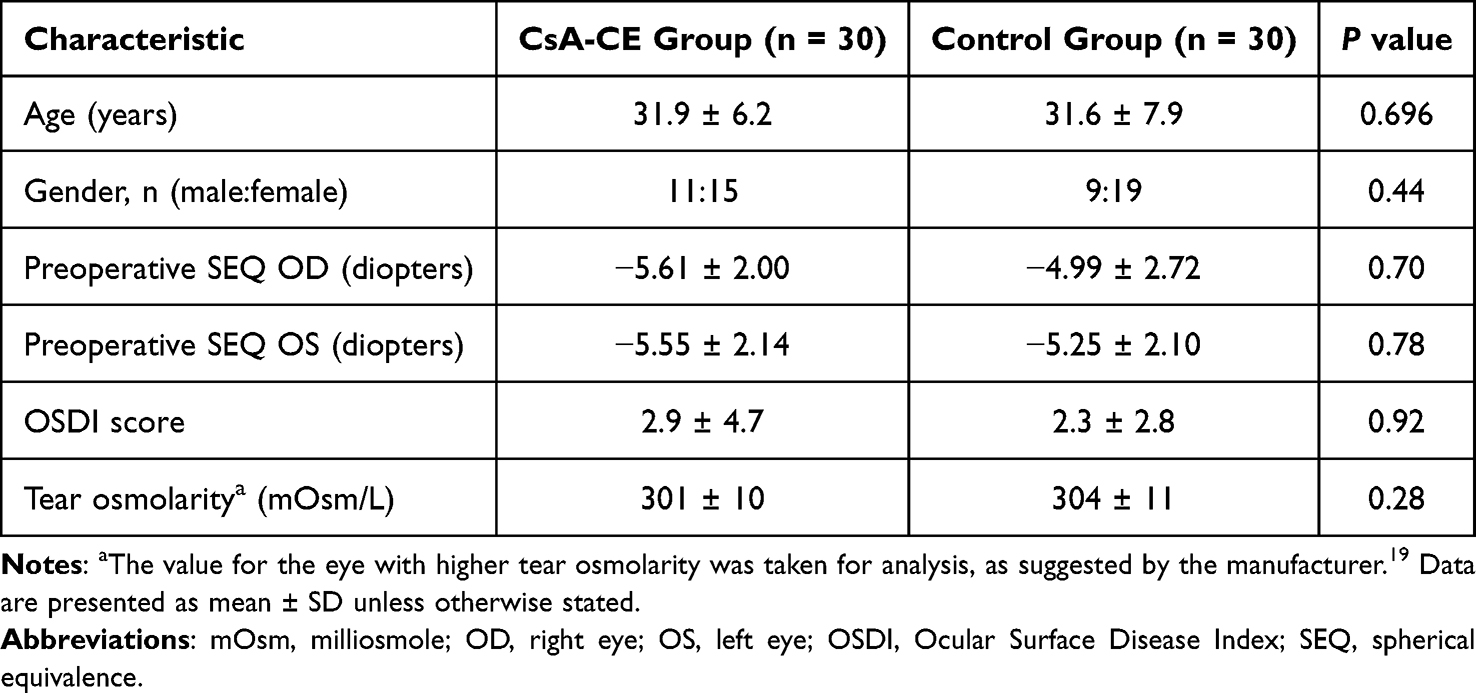 |
Table 1 Patient Demographics and Ocular Characteristics |
Results for CFS scores at three follow-up time points are shown in Figure 1. Other ocular surface parameters at postoperative time points are summarized in Table 2. At Week 1, mean CFS scores were 0.81 ± 0.94 in the CsA-CE group and 0.67 ± 1.00 in the control group, with no statistically significant difference between groups (P = 0.398). However, at both Month 1 and Month 3, the mean CFS score in the CsA-CE group was significantly reduced in comparison to the control group [Month 1: 0.31 ± 0.74 versus 0.75 ± 0.89 (P = 0.02); Month 3: 0.05 ± 0.21 versus 0.43 ± 0.84 (P = 0.04)]. When compared with the control group, the mean CFS score in the CsA-CE group was 0.44 and 0.38 lower at Months 1 and 3, respectively.
 |
Table 2 Ocular Surface Parameters (CFS Scores, OSDI Score, and Tear Osmolarity) at Postoperative Time Points |
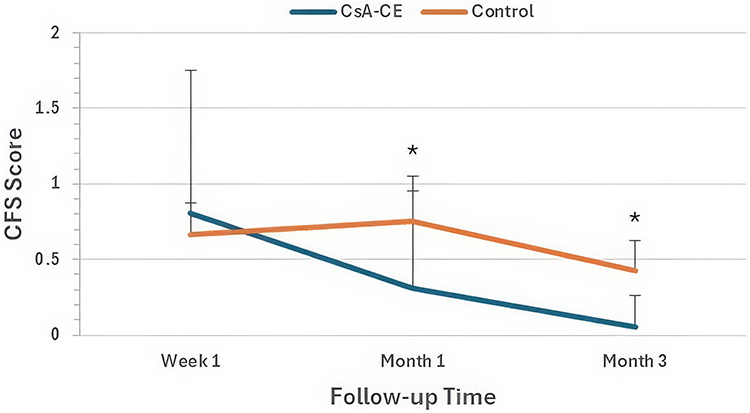 |
Figure 1 Comparison of CFS scores between CsA-CE and control groups. Data are presented as mean ± SD. (*) indicates statistically significant changes with P < 0.05 between groups. |
Notably, OSDI scores between the groups at either time points were not statistically different. OSDI scores improved from Month 1 to Month 3 in 59.1% of patients in the CsA-CE group (13 out of 22), and similarly in 56.5% of the control group (13 out of 23). Tear osmolarity remained normal in both groups at both Month 1 and Month 3, with no statistically significant differences between groups.
Among the 26 patients in the CsA-CE group who completed the one-month treatment with 0.1% CsA-CE, subjective tolerability scores were as follows: Grade 0 (no instillation site pain): 15 patients (57.7%); Grade 1 (mild but brief instillation site pain): 7 patients (26.9%); Grade 2 (moderate instillation site pain but tolerable): 4 patients (15.0%); Grade 3 (intolerable instillation site pain): no patients. No other adverse effects (AEs), such as accumulation of emulsified solution in the incision wound or interface, were reported in the CsA-CE group.
Discussion
In this study, we evaluated the effect of 0.1% CsA-CE on CFS score, OSDI score and tear osmolarity after SMILE. Our clinical data indicate that the use of 0.1% CsA-CE in the first month post-SMILE resulted in significantly lower CFS scores in the CsA-CE group than in the control group, indicative of reduced ocular surface damage.
Our study relied on CFS score as the primary outcome measure for evaluating ocular surface inflammation. As mentioned above, CFS is one of the key parameters examined in pivotal clinical trials involving CsA,11,13 and studies using conjunctival epithelial biopsies have shown that decreased corneal staining can reflect a reduction in inflammatory markers on the ocular surface.13 Furthermore, in one of the pivotal trials (the SANSIKA study), the expression of human leukocyte antigen-DR (HLA-DR) on conjunctival epithelial cells (a biomarker of ocular surface inflammation) was directly proportional to CFS scores. Of note, we did not evaluate other DED criteria, for instance tear break-up time (TBUT) and tear meniscus height (TMH) for several reasons. Firstly, in the SANSIKA and SICCANOVE clinical studies, the TBUT and TMH improved in both treatment and control groups without significant differences.8,9,11 The authors postulated that in the control group, the lubricating effect of the vehicle (an unpreserved cationic oil-in-water nano-emulsion) also improved DED on its own. This was similar in our control group, where all subjects were also routinely given artificial tears, following routine practice in all our SMILE surgeries. Secondly, TBUT or TMH may be less useful ocular parameters than the CFS, due to the low treatment severity and high recovery rates observed using these markers after SMILE. A meta-analysis demonstrated that there was only a non-significant reduction in tear production and TBUT after SMILE,21 and additional studies have shown that early recovery of TMH may be achieved as early as one month after SMILE.22 Thirdly, it is well known that such tear parameters are often poorly correlated with dry eye symptoms.23 Recently, another randomized control trial studied the effect of 0.05% ciclosporin on the OSDI, non-invasive tear break-up time (NIBUT), tear lipid layer thickness and TMH. The authors reported that 0.05% ciclosporin was effective in relieving these parameters in the early postoperative phase after SMILE, but only the lipid layer thickness (LLT) and TMH demonstrated a significant difference to the control group.24 This somehow echoed our previous discussion, and it is also worth noting that they did not report CFS findings.
CFS scores measured at postoperative time points are considered mild to minimal. Nonetheless, in comparison with the control group, the mean CFS score in the CsA-CE group was 0.44 lower at Month 1 and 0.38 lower at Month 3. As the modified Oxford scale we utilized for CFS grading is a logarithmic scale, a difference of one grade corresponds to a 3.16-fold increase or decrease in the number of dots. The statistically significant lower CFS scores in the CsA-CE versus control groups at Month 1 and Month 3 may therefore be interpreted as clinically significant.8,20
Our study did not show any statistically significant differences between the CsA-CE and control groups in either OSDI score or tear osmolarity. We suggest that this may be due to the routine post-SMILE drug regimen that both groups received (ie topical steroids for one week and an artificial tear for four weeks), which could have helped stabilize dry eye parameters at Month 1 and Month 3. Similar findings were observed in the CsA-CE pivotal studies SANSIKA and SICCANOVE, where both the CsA-CE-treated and vehicle-treated groups (with the vehicle itself being a cationic emulsion) showed improvements in OSDI score and other dry eye parameters.8,9 Nevertheless, we found significant between-group differences in CFS scores, which can likely be attributed to the additional study treatment received by the CsA-CE group. In addition, multiple comparative studies have found that SMILE is associated with less postoperative DED overall when compared with LASIK.25–27 In our control group, OSDI scores and tear osmolarity could thus have remained in the normal range even without CsA-CE treatment. It would therefore be worthwhile to study whether CsA-CE treatment could have significant effects on OSDI scores and tear osmolarity after LASIK surgery. With respect to long-term effects, Liu et al found that laser-induced corneal denervation was not fully healed even at five years after SMILE, indicating that SMILE patients could still be prone to developing DED due to neurotrophic factors and reduced corneal blink reflex.27 Therefore, CsA-CE treatment to control ocular surface inflammation in the early postoperative period could be considered as a way to further reduce the risk of developing DED in the future.
A commercially available, unpreserved, single-dose cationic emulsion containing 0.1% ciclosporin A was used in this investigation. By interacting electrostatically with the negatively charged tear film components, the cationic emulsion lengthens the duration of ocular retention and, consequently, the drug’s ocular bioavailability.28 In a recent animal study, a ciclosporin cationic emulsion preparation was found to have more potent anti-inflammatory and anti-apoptotic activity in an in-vitro dry eye model than a ciclosporin emulsion.29
Studies have shown that the corneal inflammatory response occurs as early as one hour after the laser procedure and peaks at seven days,30 and that dry eye symptoms, tear film instability and ocular surface damage are present in the early postoperative period.16 With this in mind, we adopted a “pre-emptive” approach to counteract ocular surface inflammation as soon as possible, by starting CsA-CE together with topical steroid treatment on the same day after the SMILE surgery. To prevent unwanted side effects from steroid treatment, we discontinued steroid use after Week 1, but continued CsA-CE treatment up to Month 1. Our findings demonstrate that early postoperative CsA-CE treatment soon after SMILE leads to significantly reduced corneal staining, indirectly indicating a reduction in ocular surface inflammation which we suggest is clinically significant. It is worth noting that CsA is known to peak in efficacy only after a few weeks of consistent usage. Hence, it cannot completely replace corticosteroids in the immediate postoperative period. In addition, it is generally recommended to use corticosteroids as a bridging therapeutic agent while waiting for the effects of CsA to kick in when initiating CsA treatment in treating ocular surface inflammation.
Importantly, although CsA-CE treatment was discontinued at Month 1, the lower levels of corneal staining in the CsA-CE group were sustained up to Month 3 post-SMILE treatment. The effects of CsA-CE on ocular surface inflammation were evaluated in the SANSIKA study using HLA-DR expression on the conjunctival cell surface as a biomarker. After one month, HLA-DR expression was significantly lower in the CsA-CE-treated group than in the control group.8
Taken together with our findings, this suggests that the “pre-emptive” one-month treatment in our study was sufficient to down-regulate pro-inflammatory markers on the ocular surface and reduce ocular surface inflammation. Importantly, the treatment effects (reduction in corneal staining) were sustained beyond CsA-CE discontinuation, suggesting a reduced potential for future DED development. This is further supported by results from Peyman et al, which demonstrated significantly improved corneal sensitivity with ciclosporin treatment after LASIK, suggesting that topical ciclosporin could promote enhanced corneal nerve regeneration.14 Thus, we suggest that 0.1% CsA-CE treatment could be considered for patients at higher risk of developing post-SMILE DED, such as those with pre-existing DED, those on DED-inducing systemic medications or those with significant meibomian gland dysfunction.31
The most common side effect of 0.1% CsA-CE is transient instillation site pain or stinging sensations. The pivotal studies reported stinging or pain from drop instillation in 29.2–54.5% of patients, with around 10% of patients eventually discontinuing treatment.9,10,12,32 In our study, CsA-CE treatment was well-tolerated, which may be partly attributed to the younger age of SMILE patients compared with our broader refractive surgery population, and better eye pain tolerance. Although some concerns have been raised about whether an emulsion-based eyedrop would accumulate within the corneal stromal interface, this did not prove to be an issue in our study.
This study had a number of limitations. First, the study was non-randomized and the sample size was rather small. It was logistically challenging to perform a randomized study in a refractive surgery center setting in Hong Kong, as all of the refractive practices in Hong Kong are in the private market and not affiliated to any academic institutions. Instead, we employed the consecutive sampling method to minimize selection bias. In addition, we have compared all the baseline parameters between the two groups and confirmed there were no significant differences. The consecutive sampling was purely based on appointment sequence, ie, the first 30 control cases were done in the more humid months (August – October) while treatment group cases were recruited in the drier months (October – December). This may have inadvertently created temporal bias, but since the treatment group was done in the drier months, the actual beneficial effect of CsA-CE might be more pronounced. The relatively high dropout rate contributed to the relatively small sample size. There were no discernible patterns in the dropout patients, except they tend to have better immediately postoperative visual acuity and expressed satisfaction with the SMILE refractive surgery. Given the social movement in Hong Kong in late 2019 (with frequent road blockades) and the COVID-19 outbreak since early 2020 (with frequent lockdowns), these patients defaulting to a “routine follow-up” is unavoidable especially in a private setting.
Second, the assessment of CFS was performed by the operating surgeon, as an independent masked observer was not available. This could have introduced a potential observer bias.
Third, the study did not include any biomarkers that directly quantified ocular surface inflammation. In recent years, the measurement of tear matrix-metalloproteinase-9 (MMP-9) levels has enabled quantitative assessment of ocular surface inflammation. However, MMP-9 testing was not yet available in Hong Kong at the time of our study. Instead, our study relied on commonly used parameters and tests without employing more sophisticated imaging systems or tools. As mentioned previously, the CFS score was found to be able to reflect ocular surface inflammation.
Fourth, the follow-up period was only three months with a few cases lost during follow-up. It would be worth investigating whether the effects of CsA-CE treatment on CFS score could be sustained beyond three months, for example, up to six months. However, since dry eye symptoms after SMILE tend to be mild and transient in nature,26 most signs and symptoms of DED should be resolved between three to six months after surgery. It is also known that the incidence and severity of dry eyes after LASIK is higher than that of SMILE.5 However, here we only studied SMILE patients because at the time of the study (when the CsA-CE became commercially available), SMILE was already much more popular than LASIK treatment in Hong Kong.
Conclusions
Our clinical investigation revealed that one-month of 0.1% CsA-CE treatment immediately after SMILE surgery was not only well-tolerated but also could reduce corneal staining, which is indicative of a reduction in ocular surface inflammation, in the early postoperative period. The “preemptive” approach of early, one-month CsA-CE treatment was another key aspect of this study.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon request.
Ethics Approval and Participant Consent
The study was carried out in compliance with the Declaration of Helsinki’s tenets. Prior to surgery, each patient signed an informed consent form. Before the study started, the Hong Kong Eye Day Surgery Centre ethics committee examined and approved the protocol. Every experiment was carried out in compliance with the applicable rules and regulations.
Acknowledgments
The 0.1% ciclosporin in cationic emulsion and tear osmolarity test cards were supplied by Santen Pharmaceutical (Hong Kong) Limited. Editorial assistance was provided by Media MICE Pte. Ltd. (Singapore) and supported by Santen Pharmaceutical (Hong Kong) Limited.
Author Contributions
ALKN: Idea and design of study, collection of data, analysis of data, writing of manuscript and final approval of manuscript. DKTL: Idea and design of study, collection of data, analysis of data, writing of manuscript and final approval of manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors did not receive any financial support for conducting the study.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Tülü Aygün B, Çankaya K, Ağca A, et al. Five-year outcomes of small-incision lenticule extraction vs femtosecond laser-assisted laser in situ keratomileusis: a contralateral eye study. J Cataract Refract Surg. 2020;46(3):403–409. doi:10.1097/j.jcrs.0000000000000067
2. Ang M, Farook M, Htoon HM, Mehta JS. Randomized clinical trial comparing femtosecond LASIK and small-incision lenticule extraction. Ophthalmology. 2020;127(6):724–730. doi:10.1016/j.ophtha.2019.09.006
3. Shen Z, Zhu Y, Song X, Yan J, Yao K. Dry eye after small incision lenticule extraction (SMILE) versus femtosecond laser-assisted in situ keratomileusis (FS-LASIK) for myopia: a meta-analysis. PLoS One. 2016;11(12):e0168081. doi:10.1371/journal.pone.0168081
4. Bandeira F, Yusoff NZ, Yam GH, Mehta JS. Corneal re-innervation following refractive surgery treatments. Neural Regen Res. 2019;14(4):557–565. doi:10.4103/1673-5374.247421
5. Wong AHY, Cheung RKY, Kua WN, Shih KC, Chan TCY, Wan KH. Dry eyes after SMILE. Asia Pac J Ophthalmol. 2019;8(5):397–405. doi:10.1097/01.APO.0000580136.80338.d0
6. Stern ME, Schaumburg CS, Pflugfelder SC. Dry eye as a mucosal autoimmune disease. Int Rev Immunol. 2013;32(1):19–41. doi:10.3109/08830185.2012.748052
7. Pietilä J, Huhtala A, Mäkinen P, et al. Uncorrected visual acuity, postoperative astigmatism, and dry eye symptoms are major determinants of patient satisfaction: a comparative, real-life study of femtosecond laser in situ keratomileusis and small incision lenticule extraction for myopia. Clin Ophthalmol. 2018;12:1741–1755. doi:10.2147/OPTH.S172894
8. Leonardi A, Van Setten G, Amrane M, et al. Efficacy and safety of 0.1% cyclosporine A cationic emulsion in the treatment of severe dry eye disease: a multicenter randomized trial. Eur J Ophthalmol. 2016;26(4):287–296. doi:10.5301/ejo.5000779
9. Baudouin C, Figueiredo FC, Messmer EM, et al. A randomized study of the efficacy and safety of 0.1% cyclosporine A cationic emulsion in treatment of moderate to severe dry eye. Eur J Ophthalmol. 2017;27(5):520–530. doi:10.5301/ejo.5000952
10. Baudouin C, de la Maza MS, Amrane M, et al. One-year efficacy and safety of 0.1% cyclosporine a cationic emulsion in the treatment of severe dry eye disease. Eur J Ophthalmol. 2017;27(6):678–685. doi:10.5301/ejo.5001002
11. Leonardi A, Messmer EM, Labetoulle M, et al. Efficacy and safety of 0.1% ciclosporin A cationic emulsion in dry eye disease: a pooled analysis of two double-masked, randomised, vehicle-controlled Phase III clinical studies. Br J Ophthalmol. 2019;103(1):125–131. doi:10.1136/bjophthalmol-2017-311801
12. Pisella PJ, Labetoulle M, Doan S, et al. Topical ocular 0.1% cyclosporine A cationic emulsion in dry eye disease patients with severe keratitis: experience through the French early-access program. Clin Ophthalmol. 2018;12:289–299. doi:10.2147/OPTH.S150957
13. Sall K, Stevenson OD, Mundorf TK, Reis BL. Two multicenter, randomized studies of the efficacy and safety of cyclosporine ophthalmic emulsion in moderate to severe dry eye disease. CsA Phase 3 Study Group. Ophthalmology. 2000;107(4):631–639. doi:10.1016/S0161-6420(99)00176-1
14. Peyman GA, Sanders DR, Batlle JF, Feliz R, Cabrera G. Cyclosporine 0.05% ophthalmic preparation to aid recovery from loss of corneal sensitivity after LASIK. J Refract Surg. 2008;24(4):337–343. doi:10.3928/1081597X-20080401-04
15. Kanellopoulos AJ. Incidence and management of symptomatic dry eye related to LASIK for myopia, with topical cyclosporine A. Clin Ophthalmol. 2019;13:545–552. doi:10.2147/OPTH.S188521
16. Qiu PJ, Yang YB. Early changes to dry eye and ocular surface after small-incision lenticule extraction for myopia. Int J Ophthalmol. 2016;9(4):575–579. doi:10.18240/ijo.2016.04.17
17. Ng ALK, Cheng GPM, Woo VCP, Jhanji V, Chan TCY. Comparing a new hydroexpression technique with conventional forceps method for SMILE lenticule removal. Br J Ophthalmol. 2018;102(8):1122–1126. doi:10.1136/bjophthalmol-2017-310993
18. Schiffman RM, Christianson MD, Jacobsen G, Hirsch JD, Reis BL. Reliability and validity of the ocular surface disease index. Arch Ophthalmol. 2000;118(5):615–621. doi:10.1001/archopht.118.5.615
19. Lemp MA, Bron AJ, Baudouin C, et al. Tear osmolarity in the diagnosis and management of dry eye disease. Am J Ophthalmol. 2011;151(5):792–798.e791. doi:10.1016/j.ajo.2010.10.032
20. Bron AJ. The Doyne lecture. reflections on the tears. Eye. 1997;11(Pt 5):583–602. doi:10.1038/eye.1997.161
21. Sambhi RS, Sambhi GDS, Mather R, Malvankar-Mehta MS. Dry eye after refractive surgery: a meta-analysis. Can J Ophthalmol. 2020;55(2):99–106. doi:10.1016/j.jcjo.2019.07.005
22. Shaaban YM, Badran TAF. Tear meniscus evaluation after microkeratome laser in situ keratomileusis, femtosecond laser and femtosmile laser techniques using anterior segment optical coherence tomography. Clin Ophthalmol. 2018;12:1337–1345. doi:10.2147/OPTH.S169091
23. Schmidl D, Witkowska KJ, Kaya S, et al. The association between subjective and objective parameters for the assessment of dry-eye syndrome. Invest Ophthalmol Vis Sci. 2015;56(3):1467–1472. doi:10.1167/iovs.14-15814
24. Zhu X, Li S, Wang M, Yao W, Huang X, Zhao L. Effects of topical 0.05% cyclosporine A on dry eye symptoms and parameters following small incision lenticule extraction. J Refract Surg. 2024;40(4):e229–e238.
25. Denoyer A, Landman E, Trinh L, Faure JF, Auclin F, Baudouin C. Dry eye disease after refractive surgery: comparative outcomes of small incision lenticule extraction versus LASIK. Ophthalmology. 2015;122(4):669–676. doi:10.1016/j.ophtha.2014.10.004
26. Kobashi H, Kamiya K, Shimizu K. Dry eye after small incision lenticule extraction and femtosecond laser-assisted LASIK: meta-analysis. Cornea. 2017;36(1):85–91. doi:10.1097/ICO.0000000000000999
27. Liu YC, Jung ASJ, Chin JY, Yang LWY, Mehta JS. Cross-sectional study on corneal denervation in contralateral eyes following SMILE versus LASIK. J Refract Surg. 2020;36(10):653–660. doi:10.3928/1081597X-20200730-01
28. Lallemand F, Daull P, Benita S, Buggage R, Garrigue JS. Successfully improving ocular drug delivery using the cationic nanoemulsion, novasorb. J Drug Deliv. 2012;2012:604204. doi:10.1155/2012/604204
29. Hwang SB, Park JH, Kang SS, et al. Protective effects of cyclosporine a emulsion versus cyclosporine A cationic emulsion against desiccation stress in human corneal epithelial cells. Cornea. 2020;39(4):508–513. doi:10.1097/ICO.0000000000002244
30. Sun Y, Zhang T, Liu M, et al. Early corneal wound healing response after small incision lenticule extraction. Cornea. 2019;38(12):1582–1588. doi:10.1097/ICO.0000000000002105
31. Li Y, Li S, Zhou J, Liu C, Xu M. Relationship between lipid layer thickness, incomplete blinking rate and tear film instability in patients with different myopia degrees after small-incision lenticule extraction. PLoS One. 2020;15(3):e0230119. doi:10.1371/journal.pone.0230119
32. Hind J, Macdonald E, Lockington D. Real-world experience at a Scottish university teaching hospital regarding the tolerability and persistence with topical Ciclosporin 0.1% (Ikervis) treatment in patients with dry eye disease. Eye. 2019;33(4):685–686. doi:10.1038/s41433-018-0289-7
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.