Back to Journals » Journal of Blood Medicine » Volume 16
Red Cell Alloimmunization Among Transfused Chronic Kidney Disease Patients: A Hospital-Based Study in Southwestern Uganda
Authors John EA ![]() , Muwanguzi E, Wagubi R
, Muwanguzi E, Wagubi R ![]() , Rugera SP
, Rugera SP ![]() , Bagenda CN
, Bagenda CN ![]() , Muhindo R
, Muhindo R ![]() , Okongo B
, Okongo B ![]()
Received 5 August 2025
Accepted for publication 3 November 2025
Published 11 November 2025 Volume 2025:16 Pages 537—549
DOI https://doi.org/10.2147/JBM.S558414
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Martin H Bluth
Elizabeth A John,1 Enoch Muwanguzi,1 Robert Wagubi,1 Simon Peter Rugera,1 Charles Nkubi Bagenda,1 Rose Muhindo,2 Benson Okongo1
1Department of Medical Laboratory Science, Mbarara University of Science and Technology, Mbarara City, Uganda; 2Department of Internal Medicine, Mbarara University of Science and Technology, Mbarara City, Uganda
Correspondence: Benson Okongo, Department of Medical Laboratory Science, Mbarara University of Science and Technology, P.O. BOX 1410, Mbarara City, Uganda, Tel +256 778 557 867, Fax +256-485-20782, Email [email protected]
Purpose: This study determined the prevalence, types of red cell alloantibodies and factors associated with red cell alloimmunization among transfused patients with CKD at Mbarara Regional Referral Hospital.
Patients and Methods: A cross-sectional study was conducted among 141 consented, transfused patients with CKD from March to May 2025. Sociodemographic characteristics and clinical data were collected using a structured questionnaire. Four millilitres of EDTA anticoagulated blood were collected and tested for ABO/Rh blood group, direct antihuman globulin test, and red cell alloantibodies screening and identification by using the Echo Lumena machine (Immucor USA). Data were analyzed using STATA version 17. Logistic regression was used to determine factors associated with alloimmunization, and a p-value of ≤ 0.05 was considered statistically significant.
Results: Out of 141 patients with CKD, 97 (67.8%) were male, and the mean age was 54.4 ± 17.12. The overall prevalence of red cell alloimmunization was 10 (7.1%). A total of 4 study patients were alloimmunized with a single type of antibody; 2 had multiple antibodies, while 4 had undetermined types. Anti-K was the commonest identified alloantibody. Blood group A had significantly lower odds of alloimmunization (aOR 0.01, 95% CI: 0.0005– 0.229, p = 0.004), similar to blood group O (aOR 0.01, 95% CI: 0.0007– 0.163, p = 0.001).
Conclusion: The study reveals a slightly higher prevalence of red cell alloimmunization compared to global prevalence, with Anti-K being the most frequent antibody. Only ABO blood group was significantly associated with red cell alloimmunization. Therefore, more studies are needed to evaluate the complex nature of this phenomenon.
Keywords: alloimmunization, associated factors, chronic kidney disease, transfusion
Introduction
Chronic Kidney Disease (CKD) is characterized by lasting structural or functional abnormalities in the kidneys for a period exceeding three months.1 Anemia frequently develops in CKD patients due to various underlying factors, one of the most prominent being a reduction in erythropoietin, a hormone essential for the production of red blood cells.2 Inflammation, which is common in CKD, can lead to iron being trapped within the mononuclear phagocytic system, thereby reducing its availability for red blood cell formation.3 Effective management of CKD-related anemia often involves the use of iron supplements, erythropoiesis-stimulating agents (ESAs), and blood transfusions.4 However, due to ESA resistance and risks associated with prolonged iron therapy, including iron overload, blood transfusions are frequently used.5,6
While transfusions are beneficial, they also present immunological challenges. Red blood cells have more than 300 surface antigens, many of which can provoke an immune response.7 Each transfusion introduces numerous foreign antigens into the patient’s system, potentially stimulating the immune system to form alloantibodies against these non-self-cells.8 This immune reaction, known as red cell alloimmunization, involves the production of antibodies targeting foreign red cell antigens.9 CKD patients undergoing repeated transfusions are particularly at risk for alloimmunization, which can lead to complications such as delayed transfusion reactions, difficulty in matching future blood products, delays in kidney transplantation, increased rejection risk, and even death.10–12
Globally, red cell alloimmunization is reported in approximately 2% to 6% of transfused patients.13 However, prevalence differs by region. In Malaysia, the rate among CKD patients is 12.4%, while in Indonesia it is 6%.14,15 African studies reveal a broader range, from 5.2% up to 47.82%, depending on the study.16,17 These variations are likely influenced by the methods used to detect alloantibodies, patient demographics, and inconsistent transfusion protocols across settings.18,19
Among the various blood group systems, the Rhesus (Rh) antigens—particularly Rh D are known to cause strong immune responses. The Rh system’s antigens have decreasing immunogenicity in the order: D > E > e > C > c.17 Anti-Kell (anti-K) is another commonly identified alloantibody, while antibodies from less prevalent systems, such as Lewis and Diego, can also be involved, albeit less frequently, in African populations.16 In contrast, anti-Mia is the most frequently reported alloantibody in Malaysia.14 Other potent antibodies, such as anti-Kidd (anti-Jk) and anti-Duffy (anti-Fy ab-), are rare among individuals of African descent.20
Several factors have been linked with higher chances of alloimmunization among CKD patients. Advanced kidney disease, particularly stage five, significantly increases the risk.16 Additionally, the likelihood of alloimmunization rises with the number of transfused red blood cell units10 Women are more likely to develop alloantibodies than men.21
In Uganda, access to ESAs is often limited due to financial constraints, making repeated blood transfusions the primary treatment for CKD-related anemia.6 However, data are scarce on the burden and patterns of red cell alloimmunization in this population, hindering the development of effective guidelines and interventions.
This study was conducted to determine the prevalence, types of red cell alloantibodies, and associated factors among transfused CKD patients at Mbarara Regional Referral Hospital (MRRH) in southwestern Uganda.
Materials and Methods
Study Site
This study was conducted in the Renal Unit of Mbarara Regional Referral Hospital (MRRH), located in Mbarara City, approximately 260 kilometers southwest of Kampala, the capital of Uganda. MRRH serves as a major referral center for the southwestern region of Uganda. It provides healthcare services to patients from Mbarara City and surrounding districts as well as cross-border patients from Rwanda, Burundi, the Democratic Republic of Congo, and Tanzania.
Mbarara Regional Referral Hospital (MRRH) consists of multiple departments, including internal medicine and the Renal clinic. Renal Clinic is one of the specialized clinics that operates every Monday. On average, it receives approximately 10 to 15 patients per day who are seen and treated by resident doctors, medical officers, and intern doctors. Patients with kidney disease usually visit the clinic and get admitted to the general medical ward when necessary. Those with kidney failure get hemodialysis while patients with anemia receive blood transfusions. On average around 350 anemic patients with chronic kidney disease (CKD) visit or get admitted and undergo blood transfusion each year.
The hospital laboratory includes a blood bank section. Safe blood issued to CKD patients from this section is collected from Mbarara Regional Blood Bank and stored at 2–8°C. The blood units are then verified for ABO/Rh blood grouping and cross-matched. The immediate saline technique is commonly used in emergencies. Alloantibody detection is performed by the indirect antihuman globulin test or using Echo-Lumena (Immucor, USA).
Study Design
This was a cross-sectional study which was conducted from March 2025 to May 2025 among patients with CKD receiving care at MRRH.
Study Population
This study involved adult patients with chronic kidney disease with a history of blood transfusion.
Inclusion Criteria
- Consented patients with chronic kidney disease.
- All patients with CKD with a history of blood transfusion.
Exclusion Criteria
- Patients who have undergone kidney transplantation within less than a year.
- Patients with CKD with a confirmed diagnosis of autoimmune diseases.
- Patients with CKD who had transfusions due to other chronic illness rather than chronic kidney disease.
- Patients who were transfused at the time of sample collection.
Sample Size Determination
The sample size was determined before data collection for statistically meaningful deduction by using Kish Leslie’s (1965) formula.

Where;
z was the probability value corresponding to 95% level of significance (1.96)
p was 16.9%; proportion of red cell alloimmunization among transfused kidney patients in central Sudan.10
d = margin of error allowed in this study = 5%
n = estimated sample size

n = 215 patients
The finite population correction was used to get the minimum sample size, which is proportional to the population size. Kidney patients attending the Renal Unit at MRRH are approximately 350 per year (population size = 350).
no = initial sample size
N = population of CKD patients at MRRH per year


n = 133 patients
Therefore, a minimum of 133 patients were estimated to participate in this study.
Sampling Procedures
Participants were selected by a consecutive sampling technique, which involved choosing patients who were accessible and willing to participate. Data were collected from the dialysis unit and renal clinic, which is conducted every Monday, as well as from the general medical ward. Consented, adult patients with CKD were selected on the day of visit for clinic or dialysis.
Data Collection
The study procedures and objectives were clearly explained to each participant before obtaining written informed consent, which was provided in a translated format. Data collection involved the use of pre-tested, structured questionnaires to obtain socio-demographic information such as age, sex, place of residence, marital, and employment status. Additional information on transfusion history, including the frequency and number of blood units received within a given month, was also gathered using the same questionnaire. Furthermore, data on indications for transfusion, the specific type of blood product administered, and any history of hemolytic transfusion reactions were collected through the questionnaire and cross-checked against the patients’ medical records.
Data on comorbidities and current health conditions such as sickle cell disease, pregnancy, hematologic malignancies, hemodialysis, hypertension, and diabetes mellitus were collected using a structured questionnaire. Information regarding hemoglobin levels, use of erythropoietin-stimulating agents (ESA), and the stage of kidney disease was also obtained through the questionnaire and verified against the patients’ medical records.
In cases where information on the stage of kidney disease was unavailable, the recorded serum creatinine levels were used to estimate GFR and then stage using the 2012 Kidney Disease: Improving Global Outcomes (KDIGO) guidelines.22 Patients were classified as having received multiple transfusions if they had been given more than one unit of blood within a single month.
The alloimmunization status of the patient was assessed from the laboratory and reported in the corresponding structured questionnaire.
Blood Sample Collection and Preparation
The patient was prepared for blood collection after providing consent. The site for venipuncture was disinfected with 70% alcohol before sampling. The principal investigator, together with a trained nurse or clinician responsible for blood collection, used personal protective equipment and adhered to aseptic techniques. Privacy was maintained during sample collection. Four milliliters of venous blood were drawn into ethylene diamine tetra-acetic acid (EDTA) vacutainer tubes. The samples were transported to the MRRH laboratory blood bank for ABO/Rh D blood grouping, Direct Antihuman Globulin test (DAT), alloantibody detection, and identification were performed using solid phase techniques with the Echo Lumena machine (Immucor, USA). Plasma from samples not tested immediately was separated from the red blood cells within 24 hours of collection and stored at 1–10°C.
Laboratory Procedures
ABO blood grouping was performed using both forward and reverse typing, based on the principle of direct hemagglutination. Forward grouping employed monoclonal antisera A, B, and AB, while reverse grouping used pooled reagent red cells (A1 and B cells). The testing was conducted using the fully automated Echo Lumena system (Immucor, USA).
EDTA blood samples were centrifuged at 4000 RPM for 10 minutes before being loaded into the analyzer. The red blood cells were then suspended in a diluent and dispensed onto microplates along with specific reagents (either known antisera or red cells). The presence of agglutination in reaction with a specific antiserum was used to determine the patient’s ABO blood group.
Rh blood grouping was carried out using the principle of direct agglutination on the Echo Lumena system (Immucor, USA). Monoclonal anti-D reagents, including a blend of IgG and IgM (Novaclone) and rapid IgM anti-D (ImmuClone), were used in conjunction with Rh D positive control cells. The patient’s red blood cells were incubated with anti-D at room temperature, and the presence of the Rh D antigen was indicated by agglutination at the bottom of the microplate following centrifugation. To detect weak D antigens, the blended Novaclone anti-D reagent was used after incubating the samples at 37°C for 15 minutes. A negative result was indicated by the absence of visible agglutination.
The internal camera of the analyzer captured images of the reactions, and the results were interpreted automatically by the system. Both tests were conducted in accordance with the standard ABO/Rh D blood grouping protocol.
The Direct Antiglobulin Test (DAT) was performed using the automated Echo Lumena analyzer (Immucor, USA) employing a solid-phase microplate technique, following the protocol for automatic antibody screening on the device. In this method, in vivo sensitized red blood cells are immobilized on polystyrene microwells, allowing their surface antigens to capture red cell-specific IgG antibodies present in the patient’s sample. After incubation to facilitate antibody-antigen binding, unbound antibodies are washed away. Capture-R ready indicator red cells, which carry IgG antibodies, are then added and centrifuged to bring them into proximity with the antibodies bound to the immobilized red cells. A positive result is indicated by the formation of IgG-anti-IgG complexes, causing the indicator red cells to adhere to the microplate wells. In contrast, if no antibody–antigen interaction is detected (negative test), the indicator red cells settle at the bottom of the wells.
Alloantibody Detection
Alloantibody screening for unexpected red cell IgG antibodies was performed using a modified solid-phase technique on the automated Echo Lumena analyzer (Immucor, USA). EDTA samples were centrifuged at 4000 RPM for 10 minutes to separate plasma from red blood cells before being loaded into the analyzer. Three pooled donor red cell panels (Capture-R Ready Screen) were used, each containing a specific set of red cell antigens: Panel 1 included Rh antigens (R1wR1 B7205; D, C, e, Cw), K, Kpb, Jsb, Fyb, Jkb, Lea, P1, M, N, S, s, Lub, and Xga; Panel 2 comprised Rh (R2R2 C7072; D, c, E), K, k, Kpb, Jsb, Fya, Fyb, Jka, Leb, P1, M, S, Lub, and Xga; Panel 3 contained Rh (rrH1049; c, e), k, Kpa, Kpb, Jsb, Fya, Jkb, Leb, P1, M, N, s, Lua, Lub, and Xga. These panels were used alongside Capture-R Ready Indicator Red Cells as part of the screening process.
The system utilized strips containing microwells coated with dried red blood cell membranes, whose antigens serve to capture red cell-specific antibodies present in the patient’s plasma. Patient plasma was added to the microwells and incubated at 37°C and 24°C for four minutes. After incubation, unbound immunoglobulins were washed away, and indicator red blood cells were introduced. The mixture was then centrifuged to bring the indicator red cells into contact with any antibodies attached to the red cell membranes. In cases where IgG antibodies were present in the patient’s serum (positive result), the indicator red cells adhered to the IgG antibodies bound on the microwell membranes, preventing the formation of a pellet at the bottom. Conversely, a negative test was indicated by the formation of a pellet as the indicator cells settled at the well’s base. A low ionic strength solution (Capture LISS) was included to enhance the antibody–antigen interactions. Each batch of samples was tested alongside Capture-R ready positive and negative control sera to ensure accuracy.
Alloantibodies Identification
All samples that tested positive for alloantibody screening and DAT but negative for auto-control were forwarded for alloantibody identification. This was carried out using the automated Echo Lumena analyzer (Immucor, USA) with a solid-phase system designed to detect unexpected IgG antibodies against red blood cells (Lot No: ID490). The system utilized a panel of fourteen donor red cells expressing various antigens from blood group systems including Rh, Kell, Duffy, Kidd, Lewis, P, MN, Lutheran, and Xg. Identification was guided by the Capture-R ID master list. A low ionic strength solution was employed to enhance antigen–antibody reactions, and positive and negative controls were included in wells 15 and 16 of each identification strip. Quality assurance was ensured through the use of the automated WBc or QC system, which served as an integrated run control during blood testing. This quality control system was applied alongside blood grouping antisera, reagent red cells, and antibody screening reagents. Alloantibody identification strips contained sixteen microwells, with wells 15 and 16 reserved for positive and negative controls, respectively.
These controls were included in every centrifugation run, regardless of the number of strips processed, to identify any reagent failures or technical issues such as inadequate washing or centrifugation errors. Furthermore, 10% of the samples were sent to the Mbarara Regional Blood Bank for parallel testing using the Galileo Neo platform to confirm the accuracy of results and ensure procedural consistency. The study investigators received practical training on sample processing, quality control, and result interpretation from the senior laboratory technician experienced with both the Echo Lumena and Galileo Neo systems (Immucor, USA). Additionally, all research assistants involved were comprehensively trained in the standard operating procedures for proper sample handling and analysis.
Autologous Control
Auto-control was performed on all samples, which turned out to be DAT and screening positive to detect the presence of red cell autoantibodies. The test was performed on Echo Lumena (Immucor USA) using coated micro-typing plates.
Data Analysis
Data were cleaned, coded, and analyzed using STATA version 17. Continuous variables were checked for normality and summarized accordingly, while categorical variables were reported as frequencies and percentages. Alloimmunization prevalence was calculated with 95% confidence intervals and model fit was assessed using the Hosmer–Lemeshow test. Odds ratios together with their 95% confidence interval and P value were used as a measure of association between the independent variable and the outcome variable. Logistic regression was used to identify factors associated with alloimmunization. Statistical significance was set at p ≤ 0.05.
Ethical Approval
The study was conducted in accordance with the principles of the declaration of Helsinki. Ethical approval for this study was obtained from the Research Ethics Committee (REC) of Mbarara University of Science and Technology (MUST), with reference number MUST–2025–2042. Administrative permission was also secured from the Director of Mbarara Regional Referral Hospital. Before enrolment, the study’s procedures, potential benefits, and risks were thoroughly explained to each participant in a language they understood, and written informed consent was obtained.
Participation was voluntary, with individuals free to withdraw without affecting their medical care. To ensure confidentiality, participants were assigned unique identification codes instead of using their names. All patient information was handled confidentially and stored securely, with dataset access limited through password protection and security measures.
Results
Patients’ Socio-Demographic and Transfusion Characteristics
A total of 141 participants were enrolled, with a mean age of 54.4 ± 17.23 years; the majority, 56 (39.7%), were aged 41–60 years. Males constituted the majority, 96 (68.1%) of the participants. Most participants had blood group O, 70 (49.6%) Rh D positive 137 (97.2%), notably; 105 (74.5%) had received transfusions within the past month, yet 128 (90.8%) reported no transfusion reaction. Advanced kidney disease was prevalent, with 111 (79.3%) in stage 5 and 47 (33.3%) on hemodialysis. Anemia was common; the mean hemoglobin concentration was 8.1g/dL (±2.1) with 65 (46.1%) having severe anemia. Additionally, 50 (35.5%) had a history of multiple transfusions, and 134 (95.0%) had received packed red blood cells within the past three months (Table 1).
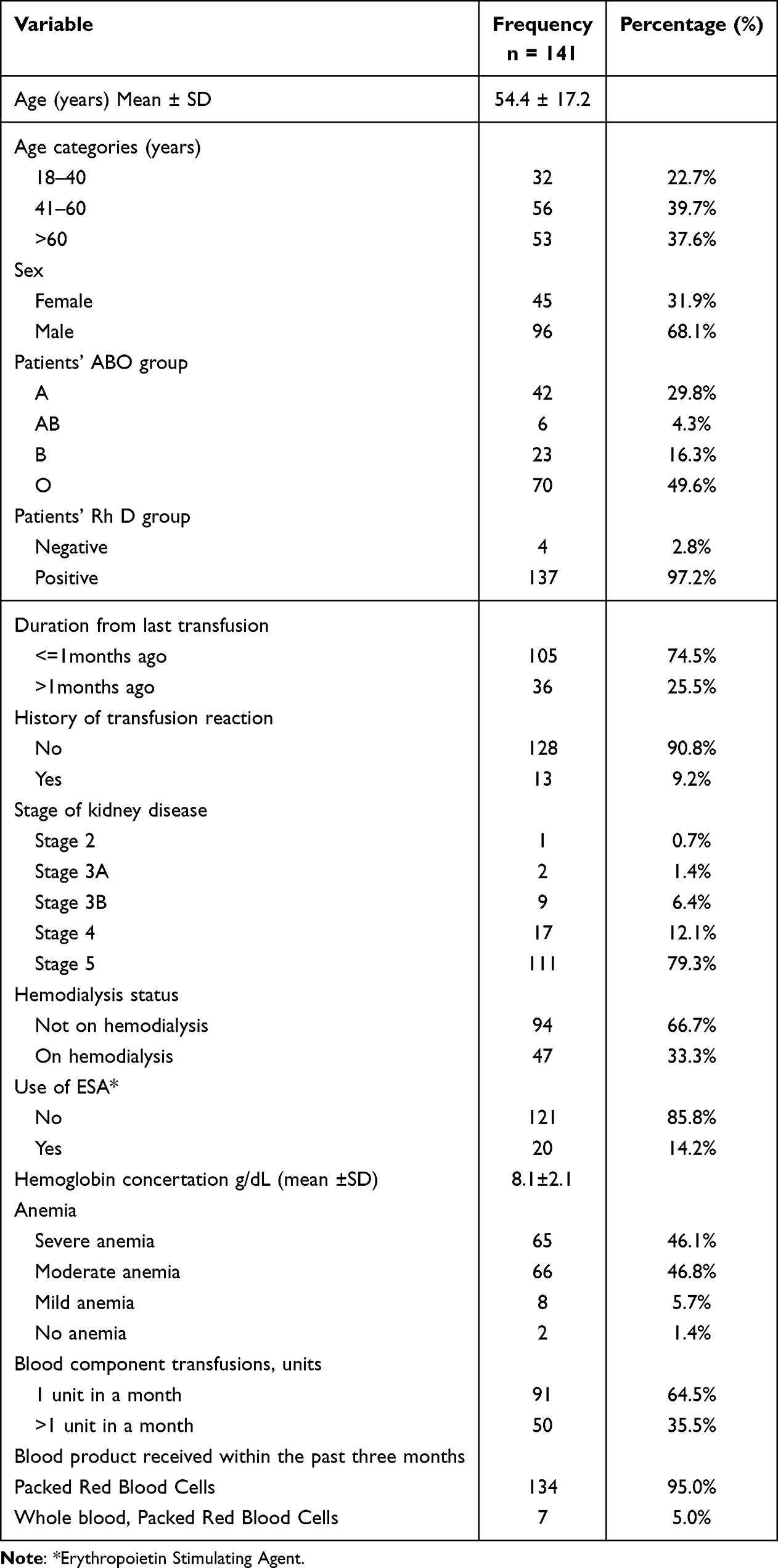 |
Table 1 Patients Sociodemographic and Transfusion Characteristics |
Prevalence of Red Cell Alloimmunization Among Transfused Patients with CKD
Out of 141 participants, 10 were found to have alloantibodies, giving an overall prevalence of alloimmunization of 7.1% (95% CI: 3.8–12.7%).
Types and Frequency of Alloantibodies Among Transfused Patients with CKD
Among those who developed alloantibodies, 4(40%) had single alloantibodies, 2(20%) had multiple, while the alloantibody specificities from four patients 4(40%) were undetermined. The most common alloantibody was anti-K 3(30.0%), while anti-S was found in 10.0% of the patients. Anti-Cw and Anti–Lewis constituted 1(10%) of the alloantibodies. Similarly, Anti-K and Anti-Cw also constituted 1(10%) of the alloantibodies (Table 2).
 |
Table 2 Types and Frequency of Alloantibodies Among Transfused Patients with CKD |
Factors Associated with Red Cell Alloimmunization Among Transfused Patients with CKD
To determine factors associated with red cell alloimmunization among CKD patients several factors were analyzed at bivariate analysis and only the patient’s ABO blood group showed a significant association with alloimmunization. Patients with blood group A (cOR: 0.024, 95% CI: 0.002–0.312, p=0.004) and blood group O (cOR: 0.029, 95% CI: 0.003–0.248, p=0.001) had significantly lower odds of developing red cell alloimmunization compared to those with blood group AB. No other factors were found to be statistically significant in the bivariate analysis (Table 3).
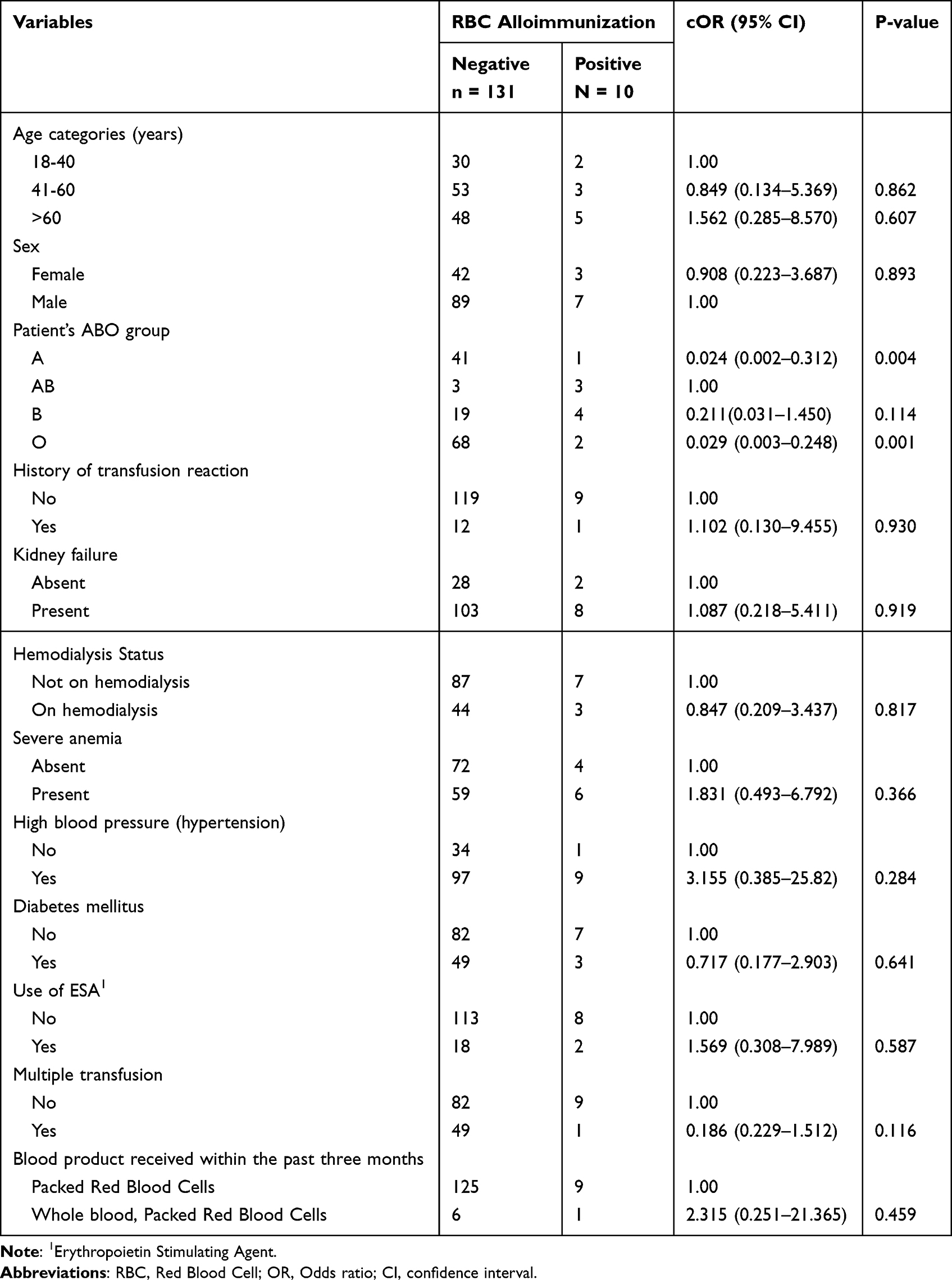 |
Table 3 Bivariate Analysis of Factors Associated with RBC Alloimmunization |
The following factors which were biologically plausible from bivariate analysis were analyzed at multivariate analysis: ABO blood group, multiple transfusion, and history of transfusion reaction. The model fitness was checked using Hosmer–Lemeshow test (p = 0.05).
After controlling for confounding factors in the multivariate analysis, only the ABO blood group remained significantly linked to red cell alloimmunization. Compared to patients with blood group AB, those with blood group A (aOR: 0.024, 95% CI: 0.001–0.349, p=0.006) and blood group O (aOR: 0.022, 95% CI: 0.002–0.225, p=0.001) had significantly lower odds of alloimmunization. No other variables demonstrated statistically significant associations (p > 0.05) (Table 4).
 |
Table 4 Multivariate Analysis of Factors Associated with RBC Alloimmunization (n = 141) |
Discussion
Patients with chronic kidney disease (CKD) can benefit from blood transfusions for treating anemia, however, it imposes the risk of infection and red cell alloimmunization, particularly in settings where cross-matching is limited to ABO/Rh blood group systems only. In addition to making it more difficult to find a compatible blood unit for alloimmunized patients14 Red cell alloantibodies can also result in poor post-transfusion hemoglobin improvement8 or delayed hemolytic reaction.23
This study aimed at determining the proportion of patients with CKD who had red cell alloantibodies, identifying of detected alloantibodies and determining the factors associated with red cell alloimmunization.
Prevalence of Red Cell Alloimmunization Among Transfused Patients with CKD
The prevalence of red cell alloimmunization in this study was 7.1%. This is statistically comparable to that reported by Nebie et al, 5.9%,19 Hassan et al, 5.2%,16 and Krisnawati et al, 6.0%,15 but lower than the study conducted in South Sudan, which reported a prevalence of 16.9%10 and 12.4% in Malaysia.14 The finding in this study is higher than the 2.94% reported in India24 and Nigeria21 3.2%. Meanwhile, in study done by Handa et al25 none of the Patients with CKD had alloantibodies.
The existing difference in prevalence can be due to differences in sensitivity and specificity of the method used for detection. The current study reported a lower prevalence in comparison to the study done by Elmobark et al10 and Yussof et al14 this can be attributed to the difference in the testing method; the solid-phase technique used in this study has lower specificity than the gel card technique.18 The difference in study population may explain the higher prevalence that was reported in this study than in the study in India24 where it only considered Patients with CKD under hemodialysis. The antigenicity of red cells present among patients and the heterogeneity that exists between donors and recipients may also explain the difference10 while the duration of detection from the time of alloantibody detection can be another reason, some alloantibodies undergo evanescence so quickly.26
In general, the prevalence of red cell alloimmunization in Patients with CKD is lower than that reported among other groups which received multiple blood transfusions.8 A higher prevalence of up to 44% has been reported among sickle cell patients and patients with myelodysplastic syndrome (15–59%).13 Patients with CKD belong to a group with a lower alloimmunization rate.8 Age and inflammatory state of the patients affect the whole process of antibody formation and hence alloimmunization, and patients with CKD have lower chances of producing alloantibodies because of their compromised immune function.23
Types of Alloantibodies Identified in Alloimmunized Patients with CKD
In this study, 141 patients were screened for red cell alloimmunization, 7.1% of them were positive, and the majority of the patients were alloimmunized by a single alloantibody (40%) while only 20% had multiple alloantibodies. This is consistent with the findings of the study done by Yusoff et al,14 which found that 90.0% of participants had a single alloantibody and 10.0% had multiples, and Elmobarak et al,10 where 84.3% developed a single alloantibody and 15.7% had multiples.
The Anti-K was the commonest antibody in this study (30.0%), which is in agreement with findings from the meta-analysis study conducted in Iran (31.7%),27 but lower than that reported in India (40%). The study in Malaysia,14 Sudan.10 and Egypt16 reported anti-K prevalence of 3.3%, 14.8%, and 1.6%, respectively, but not as the most frequent antibody. Contrary findings were reported by Nebie et al19 and Obi et al,21 who did not identify anti-K. Antigen K (KEL1) is antithetical to k (KEL 2), whereby the former is less frequent in African populations; hence, a high level of alloimmunization is expected.28 Anti-K is highly immunogenic due to polymorphism and can cause fatal Hemolytic transfusion reactions. Also, when present, it can destroy the precursors of red blood cells.29
This study also found Anti-S in 10% of the patients. This finding is similar to various studies done in Brazil, 3.5%,30 India, 2.45%,31 and the Middle East 3.1%,32 Further, a study done in South Sudan by Elmobark et al reported 3.3%10 anti-S among Patients with CKD. However, the findings are in disagreement with Datta et al24 and Nebie et al19 who did not find Anti-S. Anti-S has been reported as a highly evanescent antibody, which can explain this variation.8
Although antibodies from the Rh blood group system are among the most common causes of alloimmunization in African populations17 Their prevalence was notably low in this study. Only two patients developed alloantibodies against anti-Cw, which occurred in combination with anti-Lea and anti-K antibodies. The Cw antigen, which is a weaker variant of the C antigen, is relatively rare, and its clinical significance in transfusion medicine remains underexplored.33 Similar findings were reported in studies conducted in India by Das et al31 and in Africa by Nebie et al,19 where the same type of alloantibody was identified.
One patient (10%) from this study had anti-Lea, which was found in combination with anti-Cw; similar findings were reported in studies conducted in Malaysia, 6.7%,14 India 5.7%,31 and South Sudan, 1.6%.10 Recent studies among Patients with CKD in Africa did not report the presence of anti-Lea antibodies.16 Antibodies from the Lewis blood group system, such as anti-Lea, are generally considered to have limited clinical significance, are not usually of clinical importance, as they are rarely associated with hemolytic disease of the fetus and newborn (HDFN) and hemolytic transfusion reactions.34
The alloantibodies in 20% of the patients were indeterminate, which is consistent with Nebie et al19 and Hassan et al16 studies. This may be attributed to the fact that the panel of donor cells used was sourced from the United States, where antigen profiles may differ from those commonly found in the African population.
Factors Associated with Red Cell Alloimmunization Among Patients with CKD
A multivariate analysis was conducted to identify factors associated with red cell alloimmunization among patients with chronic kidney disease (CKD). Among the variables assessed, only ABO blood group was found to be significantly associated with alloimmunization. Other factors, including age, history of adverse transfusion reactions, severe anemia, hypertension, use of erythropoietin, multiple transfusions, and the type of blood product administered, were associated with higher odds of alloimmunization but did not reach statistical significance.
In this study, patients with blood group A and O had significantly lower odds of developing alloantibodies, with p-values of 0.004 and 0.001, respectively. These findings are in contrast to previous studies by Yusoff et al14 and Salarvand et al,32 which did not find any statistical significant association between ABO blood groups and red cell alloimmunization. Interestingly, despite the lack of statistical significance, Salarvand et al reported that a large proportion of alloimmunized individuals were blood group B, while fewer were group A or O,32 which is consistent with the current study’s observations.
However, other studies, such as those by Krisnawati et al15 and Louokdom et al17 reported that blood group O and A were more frequently observed among alloimmunized individuals, which contradicts the current study’s findings, where the majority of alloimmunized patients had blood group B.
The study by Yu et al35 demonstrated that ABO-matched transfusions reduce the likelihood of non-ABO alloimmunization. Therefore, the lower alloimmunization rate observed in this study could be attributed to the fact that most patients received ABO-matched blood transfusions, possibly mitigating the risk of alloantibody formation. There is scarcity of literature to support the current findings.
Strengths and Limitations of the Study
To the best of our knowledge, this is the first study assessing alloimmunization among patients with CKD in Uganda. The laboratory technique that was used for the detection and identification of alloantibodies is of high sensitivity and automated, therefore, reducing most errors related to misclassification. The study focused on patients with CKD, which is the group that receives multiple transfusions and are at high risk for alloimmunization.
Despite the strength, the evanescent nature of the antibodies might have negatively affected the prevalence of alloimmunization among CKD patients, the mismatch between donor panel and tested patients might have affected the study findings since the donors belong to American origin. The study was conducted at a single center, MRRH, which might have limited the generalizability of results among patients with CKD in Uganda. The study also faced challenges in obtaining patients’ transfusion information since they were disintegrated.
Conclusion
This study reveals a slightly higher prevalence (7.1%) of red cell alloimmunization in patients with CKD at MRRH compared to the global prevalence, with anti-K identified as the most common alloantibody. This suggests a heightened immunogenic response to the K antigen in this population. Most of the patients were alloimmunized by a single alloantibody (40.0%) while only 20.0% had multiple alloantibodies. Almost all factors were found not to be significantly associated with red cell alloimmunization except ABO blood group.
Acknowledgments
The authors express sincere gratitude to the study participants, the Director and staff of Mbarara Regional Referral Hospital, as well as the healthcare and laboratory personnel for their support during data collection. They also acknowledge the University of Dodoma for its financial support, which was crucial to the success of the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wilson S, Mone P, Jankauskas SS, Gambardella J, Santulli G. Chronic kidney disease: definition, updated epidemiology, staging, and mechanisms of increased cardiovascular risk. J Clin Hypertens. 2021;23(4):831–834. doi:10.1111/jch.14186
2. Salokhiddinovna X. Anemia of chronic diseases. Res J Trauma Disability Stud. 2023;2(12):364–372.
3. Macdougall IC, Bircher AJ, Eckardt K-U, et al. Iron management in chronic kidney disease: conclusions from a “Kidney disease: improving global outcomes”(KDIGO) controversies conference. Kidney Int. 2016;89(1):28–39. doi:10.1016/j.kint.2015.10.002
4. Ramatillah DL, Syarifah N. Mortality among chronic kidney failure patients who have died in last 2 years and got erythropoietin and/or blood transfusion as an Anemia Therapy in the Islamic Hospital Jakarta Cempaka Putih. Current Trends Biotechnol Pharm. 2020;2020:1.
5. Wu HH, Chinnadurai R. Erythropoietin-stimulating agent hyporesponsiveness in patients living with chronic kidney disease. Kidney Dis. 2022;8(2):103–114. doi:10.1159/000521162
6. Ameh OI, Ekrikpo U, Bello A, Okpechi I. Current management strategies of chronic kidney disease in resource-limited countries. Int J Nephrol Renovasc Dis. 2020;239–251. doi:10.2147/IJNRD.S242235
7. Far MAJ, Eftekhar Z, Far MAJ, Bahreiny SS, Mahdizade AH, Amirrajab N. Red blood cell alloimmunization: life-threatening response. Current Res Transl Med. 2024;72(4). doi:10.1016/j.retram.2024.103460
8. Tormey CA, Hendrickson JE. Transfusion-related red blood cell alloantibodies: induction and consequences. Blood. J Am Soc Hematol. 2019;133(17):1821–1830.
9. Dinardo CL. Red blood cell alloantibodies and autoantibodies: different presentation, same physiopathology. Hematology Transfusion Cell Ther. 2018;40(2):99–100. doi:10.1016/j.htct.2017.09.002
10. Elmobark ME, Abbass AA, Anwer E, Elsharief UA, Nour BYM. Red blood cell alloimmunization in multitransfused hemodialysis renal patients in central Sudan. Int J Blood Transfusion Immunohematol. 2019;9(2):1–7. doi:10.5348/100048Z02ME2019RA
11. Singh A, Kaur H, Garg P, et al. Antibody screening, identification and red cell alloimmunisation analysis in multi-transfused patients at a tertiary care hospital, Amritsar, India. J Clin Diagnostic Res. 2024;18(3):1.
12. Tsujimura K, Ota M, Chinen K, et al. Effect of perioperative blood transfusions in renal transplant patients.
13. Hendrickson JE. Recipient factors influencing red blood cell alloimmunization. ISBT Sci Series. 2020;15(1):194–200. doi:10.1111/voxs.12485
14. Yusoff SM, Bahar R, Hassan MN, Noor NHM, Ramli M, Shafii NF. Prevalence of red blood cell alloimmunization among transfused chronic kidney disease patients in hospital Universiti Sains Malaysia. Oman Med J. 2020;35(5):e177. doi:10.5001/omj.2020.95
15. Krisnawati NK, Herawati S, Mulyantari NK. Erythrocyte alloantibodies in chronic kidney disease patients receiving packed red cell transfusions in Sanglah General Hospital, Denpasar. Bali Med J. 2019;8(2):583–586. doi:10.15562/bmj.v8i2.1393
16. Hasan A, Am AE, Fouad TA. Screening and identification of red blood cell alloantibodies among hemodialysis patients in National Institute of Urology and Nephrology. J Med Scient Res. 2018;1(4):9.
17. Louokdom JS, Tuono RDM, Dedjo KN, et al. Anti-erythrocyte alloimmunisation in the RH system during chronic kidney disease: frequency in patients at the Yaoundé I University Teaching Hospital. Open Access Library J. 2023;10(3):1–10.
18. Yurtsever N, Carmichael G, Malonis R, et al. Evaluation of nonspecific reactivity rates across three immunohematology testing platforms with assessment of subsequent specific alloantibody development. Transfusion. 2025;65(5):978–984. doi:10.1111/trf.18256
19. Nebie K, Sawadogo S, Sawadogo S, et al. Red blood cell alloimmunisation in multi-transfused patients from an haemodialysis service in Burkina Faso. Afr J Lab Med. 2022;11(1):1–6. doi:10.4102/ajlm.v11i1.1625
20. Hariri D, Bordas J, Elkins M, Gallay B, Spektor Z, Hod-Dvorai R. The role of the duffy blood group antigens in renal transplantation and rejection. A mini review. Transplant Int. 2023;36:11725. doi:10.3389/ti.2023.11725
21. Obi EI, Pughikumo CO, Oko-Jaja RI. Red blood cell alloimmunization in multi-transfused patients with chronic kidney disease in Port Harcourt, South-South Nigeria. Afr Health Sci. 2018;18(4):979–987. doi:10.4314/ahs.v18i4.18
22. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group, Levin A, Stevens PE, Bilous RW, et al. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Supplements. 2013;3(1):1–150.
23. Arthur CM, Stowell SR. The development and consequences of red blood cell alloimmunization. Annual Rev Pathol. 2023;18(1):537–564. doi:10.1146/annurev-pathol-042320-110411
24. Datta SS. Red cell alloimmunization in chronic kidney disease. Asian J Transfusion Sci. 2024;18(2):371–372. doi:10.4103/ajts.ajts_121_22
25. Handa A, Kukar N, Maharishi RN, Syal N, Arora H. Analysis of red cell alloimmunization in multi transfused patients at a Tertiary care teaching hospital. J Fam Med Prim Care. 2020;9(6):2907–2911. doi:10.4103/jfmpc.jfmpc_351_20
26. Stack G. Post‐transfusion Detection of RBC Alloimmunization: Timing Is Everything. Wiley Online Library; 2021:2219–2222.
27. Hosseini MS, Jafari L, Heris RS, Gharehbaghian A. Red blood cell alloimmunization in Iran: a Comprehensive review of the literature. Asian J Transfusion Sci. 2020;14(1):4–8. doi:10.4103/ajts.AJTS_137_17
28. Shittu A, Olawumi H, Fawibe A, Biliaminu S, Yahya W. Anti-Kell allo-immunization in a Tertiary Care Hospital in North central Nigeria. East Afri Med J. 2021;98(3):3616–3624.
29. Maheshwari A, Killeen RB. Duffy blood group system. 2022.
30. Carlotto FM, Puhl BS, Beninca AA, Machado BA, de Araujo CR. Prevalence of red blood cell alloimmunization in multiply transfused patients. Clin Biomed Res. 2020;40(2):1.
31. Das SS, Biswas RN, Safi M, Zaman RU. Alloimmunization to erythrocyte antigens in patients receiving multiple blood transfusions: clinico-immunohematological and demographic risk factors and impact of extended red cell phenotyping. Global J Transfusion Med. 2021;6(2):171–177. doi:10.4103/GJTM.GJTM_68_21
32. Salarvand S, Nasab SM, Abdollahi A, Nozarian Z, Nazar E. Frequency and underlying causes of alloimmunization against red blood cell antigens in patients referred to the blood bank of the tertiary referral hospital of Tehran from 2018 to 2020. Arch Iranian Med. 2023;26(9):499. doi:10.34172/aim.2023.75
33. Rosenkrans D, Zubair M, Doyal A. Rh Blood Group System. StatPearls. 2023.
34. Liu J, Wang D. ABO (H) and Lewis blood group substances and disease treatment. Transfusion Med. 2022;32(3):187–192. doi:10.1111/tme.12820
35. Yu H, Karafin MS, Tormey CA, et al. Associations between blood donors, component modifications, and the alloimmunization of transfusion recipients. Transfusion. 2025;65(3):588–603. doi:10.1111/trf.18135
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.