Back to Archived Journals » International Journal of Clinical Transfusion Medicine » Volume 2
Red blood cell transfusion in preterm neonates: current perspectives
Authors Chirico G
Received 29 December 2013
Accepted for publication 17 February 2014
Published 16 June 2014 Volume 2014:2 Pages 21—28
DOI https://doi.org/10.2147/IJCTM.S40026
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Video abstract presented by Gaetano Chirico.
Views: 2463
Gaetano Chirico
Neonatology and Neonatal Intensive Care Unit, Children Hospital, Spedali Civili, Brescia, Italy
Abstract: Preterm neonates, especially very low birth weight infants, remain a category of patients with high transfusion needs; about 90% of those with <1,000 g birth weight may be transfused several times during their hospital stay. However, neonatal red blood cells (RBC) transfusion is not without risks. In addition to well-known adverse events, several severe side effects have been observed unique to preterm infants, such as transfusion-related acute gut injury, intraventricular hemorrhage, and increased mortality risk. It is therefore important to reduce the frequency of RBC transfusion in critically ill neonates, by delayed clamping or milking the umbilical cord, using residual cord blood for initial laboratory investigations, reducing phlebotomy losses, determining transfusion guidelines, and ensuring the most appropriate nutrition, with the optimal supplementation of iron, folic acid, and vitamins. Ideally, RBC transfusion should be tailored to the individual requirements of the single infant. However, many controversies still remain, and the decision on whether to transfuse or not is often made on an empirical basis. Recently, a few clinical trials have been performed with the aim to compare the risk/benefit ratio of restrictive versus liberal transfusion criteria. No significant differences in short-term outcomes were observed, suggesting that the restrictive criteria may reduce the need for transfusion and the related side effects. Neurodevelopmental long-term outcome seemed more favorable in the liberal group at first evaluation, especially for boys, and significantly better in the restrictive group at a later clinical investigation. Magnetic resonance imaging scans, performed at an average age of 12 years, showed that intracranial volume was substantially smaller in the liberal group compared with controls. When sex effects were evaluated, the girls in the liberal group had the most significant abnormalities. In conclusion, it would seem preferable to adopt restrictive criteria. Current recommendation on transfusion therapy should be revised to take into account this suggestion.
Keywords: preterm neonates, red blood cells, transfusion, anemia
Introduction
Packed red blood cell (pRBC) transfusion is a common practice in preterm infants admitted to neonatal intensive care units (NICUs). Very low birth weight (VLBW, <1,500 g) and extremely low birth weight (ELBW, <1,000 g) infants remain a category of patients with high transfusional needs, notwithstanding the continuing efforts to prevent anemia in these small patients. Indeed, about 40%of neonates at 1,000–1,500 g birth weight and 90%of those at <1,000 g birth weight may be transfused, with the extremely preterm patients receiving a mean of five RBC transfusions during their hospital stay.1
Other frequent causes of anemia, such as acute bleeding, hemolysis, or impaired red cell production following acquired or inherited diseases, will not be discussed in this review.
Despite the recent studies on the risk-to-benefit ratio of neonatal transfusion, many controversies about how to identify preterm neonates likely to benefit from a RBC transfusion still remain.2
The paucity of clear scientific evidence makes it difficult to formulate accurate recommendations. The transfusion need is traditionally related to hemoglobin (Hb)/hematocrit (Ht) values in relation to the reference ranges of Hb or Ht at different postnatal ages. In preterm neonates “normal values” for blood parameters are generally unavailable, because blood is usually drawn on patients with minimal pathology. Therefore, “reference ranges” are used, consisting of the 5th to the 95th percentile values, under the premise that such ranges approximate normal values.3 Ht and Hb values during the first hours after delivery correlate positively with gestational age, while erythrocyte mean corpuscular volume, which is high in neonates, tends to fall steadily as gestational age advances.3
Markers of transfusion needs in preterm neonates
The clinical status of the newborn is considered an important indication, particularly in the presence of severe cardiopulmonary diseases or of symptoms of anemia suggesting inadequate tissue oxygenation, such as increase in oxygen requirement, tachycardia, apnea, and poor weight gain. A recent international survey of transfusion practices for extremely premature infants showed that factors considered “very important” regarding the need to administer blood transfusions included degree of oxygen requirement (44.7%of respondents) and need for respiratory support (44.1%of respondents).4
In addition, it is particularly important to evaluate the degree of reticulocyte response, considering that a reticulocyte count >100,000 per μL is usually an indicator of efficient bone marrow compensation.
Apart from Hb or Ht concentration, there are several different factors that influence the oxygen transport and delivery system, such as regulation of the stroke volume and cardiac output, Hb affinity for oxygen, arterial oxygen tension, oxygen extraction fraction, and consumption of oxygen. Once oxygen availability is reduced by either diminished transport or delivery, oxygen consumption is maintained by compensatory adaptive responses such as increased blood flow by vasodilatation, increased cardiac output, or improved oxygen drop off (eg, substituting adult Hb and shifting of the Hb saturation curve), and/or via increased fractional oxygen extraction from Hb to meet metabolic demands. The critical oxygen point when the patients exceed their ability to cope with the restriction cannot be accurately defined to determine when transfusion is required, due to the difficulty of obtaining reliable clinical or laboratory indicators.5
Direct measurement of tissue oxygenation is not possible. There is no single accurate clinical sign or biochemical marker for detecting insufficient tissue oxygenation in order to guide the transfusion need.6
In a recent study, Kasat et al7 evaluated patient clinical status as a potential marker for neonatal RBC transfusion need. He observed that tachycardia was the most sensitive predictor of a benefit from pRBC transfusion. He also observed no significant clinical improvement after transfusion in critically ill ventilator-dependent neonates, probably due to the complex physiology of neonatal respiratory pathology. On the contrary, he found an increase in oxygen requirement after transfusion in a cohort of critically ill premature neonates in the first week of life, likely caused by the volume overload. For these reasons, he recommended more restrictive RBC transfusion guidelines for critically ill neonates.
To date, no conclusive data about blood lactate levels are available, especially in asymptomatic neonates.
Hemodynamic changes detected by echocardiography suggest that there is a chronic adaptation to anemia,8 although the usefulness of measures of cardiac function to identify neonates in need of pRBC transfusion remains to be assessed.
A pilot randomized controlled trial (RCT)9 to evaluate peripheral fractional oxygen extraction, measured by near infrared spectroscopy as a marker to guide blood transfusions in preterm infants, failed to identify patients who needed a blood transfusion according to clinical assessment. van Hoften et al10 used regional cerebral oximetry as a possible method for determining when a blood transfusion is indicated; premature infants had improved cerebral oxygen saturation when transfused at a restrictive threshold Hb of 6 mmol/L (97 g/L).
The splanchnic-cerebral oxygenation ratio (SCOR) provides insight into overall tissue oxygen sufficiency and can be determined using near-infrared spectroscopy. A recent study showed that infants with a low baseline SCOR (<0.73) were more likely to improve after transfusion; therefore, SCOR may help identify premature infants who will benefit from RBC transfusion.11 A previous similar study reported the significant post-transfusion improvement of cerebral, splanchnic, and renal oxygenation in anemic preterm infants.12
A prospective clinical study13 has recently shown that high concentrations (>140 pg/mL) of vascular endothelial growth factor (VEGF) may indicate insufficient oxygen delivery to tissues and may be a marker for transfusion need. Only 23 of 75 infants who required a transfusion according to local guidelines had elevated VEGF concentrations. Interestingly, VEGF concentrations did not correlate with Ht, suggesting that infants with an Ht level as low as 20%can have sufficient tissue oxygenation, whereas a higher Ht level could be observed in infants with tissue hypoxia (Table 1).
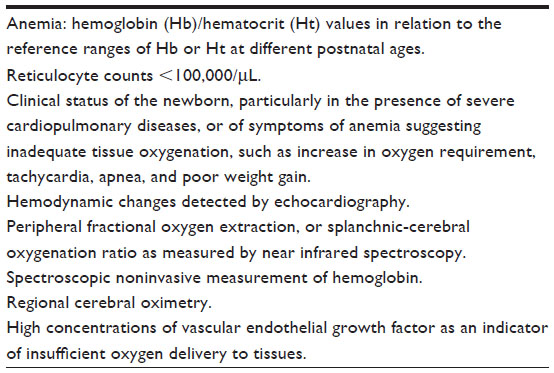 | Table 1 Markers of transfusion needs in neonates |
Adverse outcomes of RBC transfusion
Neonatal RBC transfusion is not without risks. In the last Serious Hazards of Transfusion (SHOT) report,7 the incidence of an adverse outcome of RBC transfusion was estimated to be 12.3 per 10,000 components in UK in 2012. Of the 3,545 side effects reported, 110 were observed in children less than 18 years, and 21 in newborns.14
In addition to well-known adverse events such as incorrect blood component transfusion, transfusion-transmitted infections, potassium and preservatives toxicity, transfusion-related acute lung injury, transfusion-associated circulatory overload, transfusion-related immunomodulation, and transfusion-associated graft versus host disease, several severe side effects have been observed that are unique to preterm infants.15–18
A recent study showed that RBC transfusions are independently associated with intra-hospital mortality in VLBW preterm infants. More than 50%infants received a mean number of 3.3 RBC transfusions during their hospital stay. After adjusting for confounders, the relative risk of death in infants who received at least one RBC transfusion in the first 28 days of life was 1.49, compared with infants who did not receive a transfusion. The risk of death was even higher if patients received more than two RBC transfusions after 28 days of life.15
RBC transfusion of preterm neonates with a Grade 1 intraventricular hemorrhage is associated with extension to a Grade 3 or 4 hemorrhage.16
Transfusion-related acute gut injury was recently reported. A significant temporal association (<48 hours) between pRBC transfusion and necrotizing enterocolitis (NEC) was observed in VLBW newborns.17 An analogous pathogenesis than transfusion-related acute lung injury was hypothesized. Christensen et al also found that approximately one-third of surgical NEC cases were temporally associated with pRBC transfusion.18 The pathogenetic links between transfusion and these adverse outcomes remains to be discovered. Moreover, further studies are required to clarify whether transfusions are causatively associated or are covariables.18
T activation, or the Hübener–Thomsen–Friedenreich phenomenon, is due to the enzymatic modification of the red cell membrane to expose the T antigen that is present on the surface of all red cells. The T antigen remains masked until N-acetyl-neuraminic acid (sialic acid) residues are removed by neuraminidase, an enzyme produced by a wide variety of microorganisms, such as those in the Clostridia class. Ubiquitous IgM antibodies in donor plasma directed against the T antigen and related epitopes may provoke hemolysis in patients with T-activated red cells. Several reports have shown the association of T activation during sepsis with an increased incidence of NEC and death in preterm infants following RBC transfusions.19–22
How to reduce transfusion needs
It is important to reduce the frequency of RBC transfusion in critically ill neonates, particularly considering the high risk of adverse outcomes. It has been demonstrated that the implementation of transfusional guidelines in NICUs limits the number of transfusions.23
Furthermore, improvements in NICU transfusion practice after the introduction of national recommendations for transfusion of blood products to neonates was observed in a recent multicenter study. In particular, prophylaxis for transfusion-transmitted cytomegalovirus infection, mainly through filter leukoreduction of RBC donor units rather than cytomegalovirus antibody testing to obtain cytomegalovirus-safe blood components, reached nearly total adherence to national recommendations, and both prophylaxis for graft-versus-host disease and usage of dedicated RBC donor units (pedipack system), permitting multiple transfusions from the same unit and reducing donor exposure, suggested a trend of improvement of adherence rates.24
Delivery room prevention by using delayed cord clamping for at least 30 seconds from birth can reduce the need for transfusions and facilitate early hemodynamic stabilization of VLBW infants.25
Several reports have demonstrated the short- and long-term favorable effects of delaying umbilical cord clamping. The most consistent result is represented by the increase of circulating RBC volume, Hb, and Ht in the neonate, and the consequential reduced need of RBC transfusions, as confirmed by several trials.26
However, the most important favorable effect reported in preterm infants may be considered the better hemodynamic stabilization soon after birth, with the improvement of mean systemic blood pressure, urine output, improved superior vena cava blood flow and cardiac function, and the reduced need for vasopressors. This may contribute to the reported reduction of the prevalence of intraventricular hemorrhage,27 NEC, and sepsis,28 as well as to long-term protection against motor disability.29
The need to rush when resuscitation is required, may be overcome by the use of cord milking. This fast method has been shown to achieve a similar amount of blood transfusion, as compared with delaying clamping the cord for 30 seconds.30–32
The superiority of delaying clamping or milking the cord in preterm infants is unanimously acknowledged, due to the highly favorable cost-to-benefit ratio. Indeed, the only side effect reported so far is the possible increased requirement of phototherapy.26
An additional utilization of the residual cord blood after delayed clamping or milking may be for the initial blood tests, such as blood culture, complete blood count with differential and platelet count, blood gas, typing of the ABO/Rh blood groups, and the direct antiglobulin test, in order to reduce the amount of blood initially drawn from VLBW neonates.33
Finally, the possible role for autologous RBC transfusions by collection, processing, and storage of umbilical cord blood is under evaluation.1,34
Phlebotomy losses are considered the first mechanism leading to neonatal anemia.35 The reduction of the required amount of blood for investigation by the use of microsampling, and the judicious utilization of laboratory evaluations helps to reduce transfusions in the smallest, sickest infants.
Low levels of erythropoietin (EPO), a substance in the blood that stimulates RBC production, in preterm infants provide a rationale for the use of EPO to prevent or treat anemia. A recent RCT demonstrated that the combined treatment of high-dose erythropoietin (300 U/kg/day intravenously or 700 U/kg/3 times/week subcutaneously), iron (1.5 mg/kg/day intravenously or 9 mg/kg/day orally), folate (100 mg/kg/day orally), and vitamin E and B12 during the first weeks of life significantly reduced the transfusion need of ELBW infants.36 Ohls et al showed that infants treated with darbepoetin or EPO received fewer transfusions and were exposed to fewer donors.37 In addition, recent data seems to suggest a relationship between elevated serum EPO concentrations and improved neurodevelopmental outcomes in ELBW infants.38
However, a recent meta-analysis that included almost 2,300 preterm infants enrolled in 27 studies, reached the conclusion that early administration of EPO (before the infant reaches 8 days of age) reduces the use of RBC transfusions and the volume of RBCs transfused. These small reductions are of limited clinical importance. Donor exposure is probably not avoided since most studies included infants who had received RBC transfusions prior to trial entry. Treatment with early EPO did not have any important effects on mortality or common complications of preterm birth with the exception that EPO increased the risk for retinopathy of prematurity (stage ≥3), a serious complication that may cause blindness in babies born before term. Due to the limited benefits and the increased risk of retinopathy of prematurity, early administration of EPO is not recommended. Evidence is lacking for the possible neuroprotective role of EPO in preterm infants,39 although a few studies have suggested the hypothesis of a favorable effect of human recombinant EPO on outcome in VLBW infants.40–43
As for late administration, a meta-analysis on 28 studies enrolling 1,361 preterm infants reported that administration of EPO reduces the use of one or more RBC transfusions, the number of RBC transfusions per infant but not the total volume of RBCs transfused per infant. Any donor exposure is likely not avoided as most studies included infants who had received RBC transfusions prior to trial entry. Late EPO does not significantly reduce or increase any clinically important adverse outcomes. Further research of the use of late EPO treatment to prevent donor exposure is not indicated.44
Similar conclusions emerged from a meta-analysis comparing early versus late EPO for preventing RBC transfusion in preterm and/or low birth weight infants.45
Therefore, although the association between retinopathy of prematurity and EPO administration is yet to be confirmed, the use of either early or late EPO to reduce RBC transfusions in preterm infants remains controversial.
Finally, particular attention should be directed to ensure the most favorable nutrition with an adequate protein intake, which is an important factor in stimulating erythropoiesis,35 and the optimal supplementation of iron, folic acid, and vitamins (Table 2).
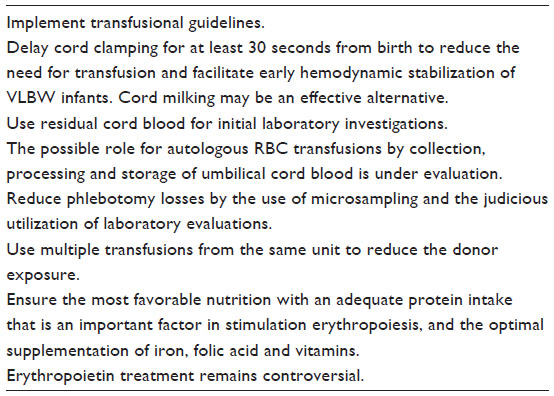 | Table 2 How to reduce neonatal transfusion needs |
Recommendations on transfusion therapy
Ideally, RBC transfusion should be tailored to the individual needs of the infant. However, due to the lack of reliable indications, the decision on whether to transfuse or not is often made on empirical basis, with large variation in transfusion practices among neonatologists.
Several guidelines on who, when, and how to transfuse preterm babies have been issued and are frequently updated. Recommendations may be mainly based on Hb or Ht levels. A recent report suggested an Hb threshold of 12 g/dl in the first 24 hours or in neonates receiving intensive care, or of 11 g/dl in case of chronic oxygen dependency, or of 7 g/dl in stable patients with late anemia.58 The suggested Ht threshold may vary from 0.40 in VLBW neonates on mechanical ventilation and oxygen therapy, to 0.35, 0.30, or 0.25 depending on the post-natal age <15 days, 15–28 days, or >28 days, respectively.59 The threshold may be lowered to 20%Ht for asymptomatic anemia, in the absence of any degree of cardiopulmonary disease.60 Major surgery, symptomatic anemia, or low reticulocyte counts are considered as factors indicating higher Ht thresholds for transfusion.59,60
A few clinical trials have been performed with the aim to compare the risk/benefit ratio of restrictive versus liberal transfusion criteria.46
Bell et al randomized 100 preterm infants with birth weights of 500–1,300 g to two levels of Ht threshold for RBC transfusion. An algorithm was developed where the highest Hb threshold was 153 g/L or Ht 46%, and the lowest Hb threshold was 73 g/L or Ht 22%. At the time of the first RBC transfusion after 6 weeks of age, mean Hb concentration was 11.0 versus 8.3 g/dL in the liberal and restrictive groups, respectively. Pretransfusion Ht, arterial oxygen content, and systemic oxygen transport values were significantly higher in the liberal transfusion group, while plasma erythropoietin concentration was higher in the restrictive transfusion group. Infants in the liberal transfusion group received more RBC transfusions (mean 5.2) as compared to the restrictive transfusion group (mean 3.3).47 Cardiac output, measured by echocardiography, and fractional oxygen extraction fell after transfusion in the low Ht group only, suggesting increased cardiac output to maintain adequate tissue oxygen delivery in response to anemia. The fall in cardiac output suggested that this group may have benefitted from transfusion.48
On the other hand, infants in the restrictive transfusion group showed a trend for increased intraparenchymal brain hemorrhage or periventricular leukomalacia (6 versus 0; P<0.012), and they had more frequent mild and severe episodes of apnea.
The authors concluded that their finding of more frequent major adverse short-term neurologic events in the restrictive RBC-transfusion group, presumably due to lower systemic oxygen transport and lower oxygen delivery to the brain, suggests that the practice of restrictive transfusions may be harmful to preterm infants.47
However, the same group from Iowa City, recently reported the results of long-term neurocognitive outcomes at school age for 33 and 23 of the preterm infants randomly assigned to the liberal or restrictive transfusion strategy, respectively. Those in the liberal transfusion group performed more poorly than those in the restrictive group on measures of associative verbal fluency, visual memory, and reading. The authors concluded that these findings highlight possible long-term neurodevelopmental consequences of maintaining higher Ht levels.49
In addition, 44 of the original 100 subjects, who were included in the liberal versus restricted RBC transfusions trial, were compared with a group of full-term healthy control children to assess the long-term outcome of brain structure, at an average age of 12 years. Magnetic resonance imaging scans showed that intracranial volume was substantially smaller in the liberal group compared with controls. Cerebral white matter was reduced in both preterm groups, more so for the liberal group. When sex effects were evaluated, the girls in the liberal group had the most significant abnormalities. These data suggest that RBC transfusions affected the long-term outcome of premature infants as indicated by reduced brain volumes at 12 years of age for neonates who received transfusions using liberal guidelines. One possible etiology for such findings was that the restrictive group fared better because endogenous erythropoietin production, a factor with possible neuroprotective properties, was suppressed in the liberal transfusion group.50
In the Premature Infants in Need of Transfusion (PINT) trial,51 a multicenter RCT of low versus high Hg transfusion thresholds, 451 ELBW infants, with birth weight <1,000 g and gestational age <31 weeks, were enrolled and transfused following an algorithm where the highest Hb threshold was 135 g/L or Ht 40.5%, and the lowest Hb threshold was 77 g/L or Ht 23%. The mean Hb difference before transfusion was 1.1 g/dL (11.2 and 10.1 g/dL in the liberal and restrictive groups, respectively), as compared to 2.7 g/dL in the study of Bell et al.47 Short-term outcomes showed no difference in death or major morbidity with restrictive or liberal transfusion regimens. By discharge from the hospital, fewer infants (89%) in the low threshold group had received a transfusion either by algorithm or clinical decision, compared with the high threshold group (95%). It was concluded that in ELBW infants, maintaining a higher Ht level resulted in more infants receiving transfusions without evidence of benefit.51
The study groups were followed up at 18–21 months’ corrected age to evaluate neurodevelopmental outcomes. The primary composite outcome was death or the presence of cerebral palsy, cognitive delay, or severe visual or hearing impairment. There was no statistically significant difference in the primary outcome, found in 45%in the restrictive group and 38%in the liberal group. At 18 months, measures of length, weight, and head circumference were strikingly similar. However, the difference in cognitive delay (Mental Development Index score <70) approached statistical significance. A post hoc analysis with cognitive delay redefined (Mental Development Index score <85) showed a significant difference favoring the liberal threshold group. Although the study provided some weak evidence of benefit from a higher Ht threshold for transfusion, the authors advocated caution in the interpretation of these results, and called for additional investigation of the effects of transfusion regimes in the prevention of neurodevelopmental impairment in ELBW infants.52
von Lindern et al recently reported the long-term outcome at 24 months’ corrected age in relation to neonatal transfusion volume. In this observational follow-up study of a cohort of extremely prematurely born infants, treated in two NICUs using different transfusion volumes (15 mL/kg in Unit A and 20 mL/kg in Unit B), no relationship was found between the composite outcome and transfusion volume received during the postnatal hospital stay. It was concluded that as there was no clinical advantage of the higher transfusion volume, a more restrictive volume will reduce total transfusion volume and donor exposure.53
Chen et al randomized 36 VLBW preterm babies to restrictive or liberal criteria for pRBC transfusion. Infants in the liberal group received a larger pRBC transfusion volume compared with the restrictive group over 30 days (41.7±20.1 versus 27.2±15.9 mL). There were no significant differences in the proportion of patients with respiratory distress syndrome, patent ductus arteriosus, severe intraventricular hemorrhage, retinopathy of prematurity, or chronic lung disease between the two groups. However, a total transfused blood volume greater than 30 mL over 30 days was a risk factor for developing chronic lung disease in VLBW infants. The authors suggested that restrictive criteria for minimizing the overall amount of transfusion to <30 mL may be a better way of preventing chronic lung disease in VLBW infants.54
Conclusion
In conclusion, reports comparing liberal and restrictive transfusion strategies yielded controversial results. Most of the studies failed to demonstrate significant differences in short-term outcomes, suggesting that the restrictive criteria may reduce the need for transfusion and the related side effects.
Neurodevelopmental long-term outcomes seemed more favorable in the liberal group at first evaluation, especially for boys, and significantly better in the restrictive group at a later clinical and brain RMN investigation, especially for girls.55
However, the effects of transfusion thresholds, transfusion frequency and timing, and Hb levels on neurodevelopmental outcome cannot be individually determined.56
When preventive measures (Table 2), such as favoring cord clamping delay or cord milking, ensuring optimal nutrition with adequate intake of proteins, iron,57 and other micronutrients, folic acid and vitamins, use of residual cord blood, and minimizing phlebotomy losses, fail to avoid the need for transfusion, it would seem preferable to adopt restrictive criteria. Current recommendation on transfusion therapy should be revised to take this suggestion into account.
Disclosure
The author reports no conflicts of interest in this work. The author declares that he has not received any funding source or payments for conducting or publicizing this article.
References
Strauss RG, Widness JA. Is there a role for autologous/placental red blood cell transfusions in the anemia of prematurity? Transfus Med Rev. 2010;24(2):125–129. | |
Christensen RD. Identifying neonates likely to benefit from a red blood cell transfusion. Transfusion. 2012;52(2):217–218. | |
Christensen RD, Henry E, Jopling J, Wiedmeier SE. The CBC: reference ranges for neonates. Semin Perinatol. 2009;33(1):3–11. | |
Guillén U, Cummings JJ, Bell EF, et al. International survey of transfusion practices for extremely premature infants. Semin Perinatol. 2012;36(4):244–247. | |
La Gamma EF. Introduction to transfusion practices in neonates: risks, benefits, and alternatives. Semin Perinatol. 2012;36(4):223–224. | |
Bishara N, Ohls RK. Current controversies in the management of the anemia of prematurity. Semin Perinatol. 2009;33(1):29–34. | |
Kasat K, Hendricks-Muñoz KD, Mally PV. Neonatal red blood cell transfusions: searching for better guidelines. Blood Transfus. 2011;9(1):86–94. | |
Alkalay AL, Galvis S, Ferry DA, Simmons CF, Krueger RC Jr. Hemodynamic changes in anemic premature infants: are we allowing the hematocrits to fall too low? Pediatrics. 2003;112(4):838–845. | |
Wardle SP, Garr R, Yoxall CW, Weindling AM. A pilot randomised controlled trial of peripheral fractional oxygen extraction to guide blood transfusions in preterm infants. Arch Dis Child Fetal Neonatal Ed. 2002;86(1):F22–F27. | |
van Hoften JC, Verhagen EA, Keating P, ter Horst HJ, Bos AF. Cerebral tissue oxygen saturation and extraction in preterm infants before and after blood transfusion. Arch Dis Child Fetal Neonatal Ed. 2010;95(5):F352–F358. | |
Bailey SM, Hendricks-Muñoz KD, Mally P. Splanchnic-cerebral oxygenation ratio as a marker of preterm infant blood transfusion needs. Transfusion. 2012;52(2):252–260. | |
Dani C, Pratesi S, Fontanelli G, Barp J, Bertini G. Blood transfusions increase cerebral, splanchnic, and renal oxygenation in anemic preterm infants. Transfusion. 2010;50(6):1220–1226. | |
Tschirch E, Weber B, Koehne P, et al. Vascular endothelial growth factor as marker for tissue hypoxia and transfusion need in anemic infants: a prospective clinical study. Pediatrics. 2009;123(3):784–790. | |
Bolton-Maggs PHB (editor), Poles D, Watt A, Thomas D; Cohen H; Serious Hazards of Transfusion (SHOT) Steering Group. The 2012 Annual SHOT Report (2013). Available from: http://www.shotuk.org/wp-content/uploads/2013/08/SHOT-Annual-Report-2012.pdf. Accessed December 23, 2013. | |
dos Santos AM, Guinsburg R, de Almeida MF, et al; Brazilian Network on Neonatal Research. Red blood cell transfusions are independently associated with intra-hospital mortality in very low birth weight preterm infants. J Pediatr. 2011;159(3):371–376. | |
Baer VL, Lambert DK, Henry E, Snow GL, Christensen RD. Red blood cell transfusion of preterm neonates with a Grade 1 intraventricular hemorrhage is associated with extension to a Grade 3 or 4 hemorrhage. Transfusion. 2011;51(9):1933–1939. | |
La Gamma EF, Blau J. Transfusion-related acute gut injury: feeding, flora, flow, and barrier defense. Semin Perinatol. 2012;36(4):294–305. | |
Christensen RD. Associations between “early” red blood cell transfusion and severe intraventricular hemorrhage, and between “late” red blood cell transfusion and necrotizing enterocolitis. Semin Perinatol. 2012;36(4):283–289. | |
Eder AF, Manno CS. Does red-cell T activation matter? Br J Haematol. 2001;114(1):25–30. | |
Ramasethu J, Luban N. T activation. Br J Haematol. 2001;112(2):259–263. | |
Boralessa H, Modi N, Cockburn H, et al. RBC T activation and hemolysis in a neonatal intensive care population: implications for transfusion practice. Transfusion. 2002;42(11):1428–1434. | |
Wang LY, Chan YS, Chang FC, Wang CL, Lin M. Thomsen-Friedenreich activation in infants with necrotizing enterocolitis in Taiwan. Transfusion. 2011;51(9):1972–1976. | |
Baer VL, Henry E, Lambert DK, et al. Implementing a program to improve compliance with neonatal intensive care unit transfusion guidelines was accompanied by a reduction in transfusion rate: a pre-post analysis within a multihospital health care system. Transfusion. 2011;51(2):264–269. | |
Motta M, Testa M, Tripodi G, Radicioni M. Changes in neonatal transfusion practice after dissemination of neonatal recommendations. Pediatrics. 2010;125(4):e810–e817. | |
Raju TN, Singhal N. Optimal timing for clamping the umbilical cord after birth. Clin Perinatol. 2012;39(4):889–900. | |
Rabe H, Diaz-Rossello JL, Duley L, Dowswell T. Effect of timing of umbilical cord clamping and other strategies to influence placental transfusion at preterm birth on maternal and infant outcomes. Cochrane Database Syst Rev. 2012;8:CD003248. | |
Sommers R, Stonestreet BS, Oh W, et al. Hemodynamic effects of delayed cord clamping in premature infants. Pediatrics. 2012;129(3):e667–e672. | |
Raju TN. Timing of umbilical cord clamping after birth for optimizing placental transfusion. Curr Opin Pediatr. 2013;25(2):180–187. | |
Mercer JS, Vohr BR, Erickson-Owens DA, Padbury JF, Oh W. Seven-month developmental outcomes of very low birth weight infants enrolled in a randomized controlled trial of delayed versus immediate cord clamping. J Perinatol. 2010;30(1):11–16. | |
Rabe H, Jewison A, Alvarez RF, et al; Brighton Perinatal Study Group. Milking compared with delayed cord clamping to increase placental transfusion in preterm neonates: a randomized controlled trial. Obstet Gynecol. 2011;117(2 Pt 1):205–211. | |
Hosono S, Mugishima H, Fujita H, et al. Umbilical cord milking reduces the need for red cell transfusions and improves neonatal adaptation in infants born at less than 29 weeks’ gestation: a randomised controlled trial. Arch Dis Child Fetal Neonatal Ed. 2008;93(1):F14–F19. | |
Hosono S, Mugishima H, Fujita H, et al. Blood pressure and urine output during the first 120 h of life in infants born at less than 29 weeks’ gestation related to umbilical cord milking. Arch Dis Child Fetal Neonatal Ed. 2009;94(5):F328–F331. | |
Baer VL, Lambert DK, Carroll PD, Gerday E, Christensen RD. Using umbilical cord blood for the initial blood tests of VLBW neonates results in higher hemoglobin and fewer RBC transfusions. J Perinatol. 2013;33(5):363–365. | |
Papacci P, Fioretti M, Giannantonio C, et al. Use of allogenic umbilical cord blood for red cells transfusion in premature infants: utopia or reality? Early Hum Dev. 2013;89(S4):S49–S51. | |
Carroll PD, Widness JA. Nonpharmacological, blood conservation techniques for preventing neonatal anemia – effective and promising strategies for reducing transfusion. Semin Perinatol. 2012;36(4):232–243. | |
Haiden N, Schwindt J, Cardona F, et al. Effects of a combined therapy of erythropoietin, iron, folate, and vitamin B12 on the transfusion requirements of extremely low birth weight infants. Pediatrics. 2006;118(5):2004–2013. | |
Ohls RK, Christensen RD, Kamath-Rayne BD, et al. A randomized, masked, placebo-controlled study of darbepoetin alfa in preterm infants. Pediatrics. 2013;132(1):e119–e127. | |
Xiong T, Qu Y, Mu D, Ferriero D. Erythropoietin for neonatal brain injury: opportunity and challenge. Int J Dev Neurosci. 2011;29(6):583–591. | |
Ohlsson A, Aher SM. Early erythropoietin for preventing red blood cell transfusion in preterm and/or low birth weight infants. Cochrane Database Syst Rev. 2012;9:CD004863. | |
Bierer R, Peceny MC, Hartenberger CH, Ohls RK. Erythropoietin concentrations and neurodevelopmental outcome in preterm infants. Pediatrics. 2006;118(3):e635–e640. | |
Brown MS, Eichorst D, Lala-Black B, Gonzalez R. Higher cumulative doses of erythropoietin and developmental outcomes in preterm infants. Pediatrics. 2009;124(4):e681–e687. | |
Neubauer AP, Voss W, Wachtendorf M, Jungmann T. Erythropoietin improves neurodevelopmental outcome of extremely preterm infants. Ann Neurol. 2010;67(5):657–666. | |
McAdams RM, McPherson RJ, Mayock DE, Juul SE. Outcomes of extremely low birth weight infants given early high-dose erythropoietin. J Perinatol. 2013;33(3):226–230. | |
Aher SM, Ohlsson A. Late erythropoietin for preventing red blood cell transfusion in preterm and/or low birth weight infants. Cochrane Database Syst Rev. 2012;9:CD004868. | |
Aher SM, Ohlsson A. Early versus late erythropoietin for preventing red blood cell transfusion in preterm and/or low birth weight infants. Cochrane Database Syst Rev. 2012;10:CD004865. | |
Chirico G, Beccagutti F, Sorlini A, Motta M, Perrone B. Red blood cell transfusion in preterm infants: restrictive versus liberal policy. J Matern Fetal Neonatal Med. 2011;24 Suppl 1:20–22. | |
Bell EF, Strauss RG, Widness JA, et al. Randomized trial of liberal versus restrictive guidelines for red blood cell transfusion in preterm infants. Pediatrics. 2005;115(6):1685–1691. | |
Fredrickson LK, Bell EF, Cress GA, et al. Acute physiological effects of packed red blood cell transfusion in preterm infants with different degrees of anaemia. Arch Dis Child Fetal Neonatal Ed. 2011;96(4):F249–F253. | |
McCoy TE, Conrad AL, Richman LC, Lindgren SD, Nopoulos PC, Bell EF. Neurocognitive profiles of preterm infants randomly assigned to lower or higher hematocrit thresholds for transfusion. Child Neuropsychol. 2011;17(4):347–367. | |
Nopoulos PC, Conrad AL, Bell EF, et al. Long-term outcome of brain structure in premature infants: effects of liberal vs restricted red blood cell transfusions. Arch Pediatr Adolesc Med. 2011;165(5):443–450. | |
Kirpalani H, Whyte RK, Andersen C, et al. The Premature Infants in Need of Transfusion (PINT) study: a randomized, controlled trial of a restrictive (low) versus liberal (high) transfusion threshold for extremely low birth weight infants. J Pediatr. 2006;149(3):301–307. | |
Whyte RK, Kirpalani H, Asztalos EV, et al; PINTOS Study Group. Neurodevelopmental outcome of extremely low birth weight infants randomly assigned to restrictive or liberal hemoglobin thresholds for blood transfusion. Pediatrics. 2009;123(1):207–213. | |
von Lindern JS, Khodabux CM, Hack KE, et al. Long-term outcome in relationship to neonatal transfusion volume in extremely premature infants: a comparative cohort study. BMC Pediatr. 2011;11:48. | |
Chen HL, Tseng HI, Lu CC, Yang SN, Fan HC, Yang RC. Effect of blood transfusions on the outcome of very low body weight preterm infants under two different transfusion criteria. Pediatr Neonatol. 2009;50(3):110–116. | |
Crowley M, Kirpalani H. A rational approach to red blood cell transfusion in the neonatal ICU. Curr Opin Pediatr. 2010;22(2):151–157. | |
Whyte RK. Neurodevelopmental outcome of extremely low-birth-weight infants randomly assigned to restrictive or liberal hemoglobin thresholds for blood transfusion. Semin Perinatol. 2012;36(4):290–293. | |
Ohls RK. Transfusions in the preterm infant. Neoreviews. 2007;8(9):e377. | |
Gibson BE, Todd A, Roberts I, et al; British Commitee for Standards in Haematology Transfusion Task Force: Writing group. Transfusion guidelines for neonates and older children. Br J Haematol. 2004;124(4):433–453. | |
Tripodi G, Antoncecchi S, Fanetti G, et al. Recommendations on transfusion therapy in neonatology. Blood Transfus. 2006;4:158–180. | |
Strauss RG. Anaemia of prematurity: pathophysiology and treatment. Blood Rev. 2010;24(6):221–225. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.