Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Recurrent Primary Cutaneous Mucinous Carcinoma of the Lower Eyelid: A Case Initially Misdiagnosed as Metastatic Carcinoma
Received 6 November 2025
Accepted for publication 30 December 2025
Published 7 January 2026 Volume 2026:19 579570
DOI https://doi.org/10.2147/CCID.S579570
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Monica K. Li
Wen Xu,1 Qi Gao,1 Yuxin Wang2
1Department of Dermatology, Zhejiang Provincial People’s Hospital, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Dermatology, Peking University People’s Hospital, Beijing, People’s Republic of China
Correspondence: Yuxin Wang, Department of Dermatology, Peking University People’s Hospital, No. 11, Xizhimen South Street, Xicheng District, Beijing, 100044, People’s Republic of China, Tel +86 010-88325472, Email [email protected]
Abstract: Primary cutaneous mucinous carcinoma (PCMC) is a rare, low-grade adnexal tumor with a propensity for local recurrence despite a low metastatic potential. It typically presents as an asymptomatic, solitary red-to-gray-blue nodule on the head and neck. We report a case of recurrent PCMC on the lower eyelid that was initially misdiagnosed as metastatic carcinoma. The lesion was successfully and definitively managed with Mohs micrographic surgery (MMS) following multiple recurrences after standard excision.
Keywords: mucinous carcinoma, primary, mohs surgery, immunochemistry
Introduction
Primary cutaneous mucinous carcinoma (PCMC) is a rare low-grade malignant adnexal tumor originating from eccrine sweat glands and their primordial structures,1 with an estimated incidence of approximately 0.04 per 100,000.2 It typically affects middle-aged and elderly individuals, with no clear gender predilection. Clinically, PCMC most often presents as a solitary, red or bluish-gray nodule, predominantly located on the head and neck, particularly the face and scalp.3
The clinical features of PCMC are often non-specific, so a histopathological examination is required to confirm the diagnosis. Characteristic histopathological features include abundant mucin pools separated by fibrous septa, containing islands of floating tumor cells.4 The immunohistochemical (IHC) profile of PCMC is typically positive for CK7, EMA, ER, PR, and E-cadherin, with variable expression of MUC1 and MUC2.5
Recommended treatment options include standard excision, wide local excision, Mohs micrographic surgery (MMS) and regional lymph node dissection if nodal metastasis is suspected.1 Surgery is the primary treatment modality. Radiotherapy and chemotherapy have shown limited efficacy, particularly for recurrent PCMC.6 For recurrent eyelid PCMC, modified local extended resection is an option.7
We report a challenging case of recurrent PCMC of the lower eyelid that was initially misdiagnosed as metastatic carcinoma. This case shows the diagnostic steps and highlights the role of MMS in its final management.
Case Report
An 81-year-old man with well-controlled hypertension and hyperlipidemia presented with a 2-year history of a recurrent, asymptomatic nodule on his left lower eyelid. The lesion first appeared as a firm, reddish papule (Figure 1A) and was initially excised 18 months prior. The lesion recurred at the same site and grew rapidly into a larger nodule (Figure 1B). A second biopsy performed two months before the current admission. Despite this, the lesion recurred again, prompting our evaluation. At this time, a firm, reddish, hemispherical nodule of approximately 1 cm in diameter with surface telangiectasia was observed (Figure 1C). The initial excision 18 months prior revealed a poorly differentiated mucinous adenocarcinoma on histopathology, raising the possibility of metastasis, with clear margins (Figure 2A–C). However, the patient was lost to follow-up, and no further oncological workup was pursued at that time.
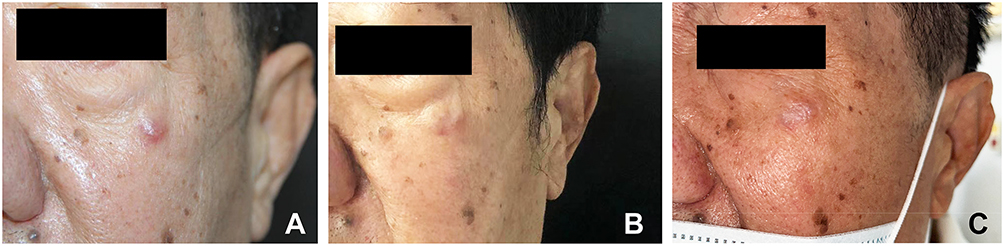 |
Figure 1 (A) Initial presentation: a firm, reddish papule present for 2 years; (B) First recurrence; (C) Second recurrence at the primary excision site prior to Mohs surgery, presenting as a firm, hemispherical nodule with telangiectasia. |
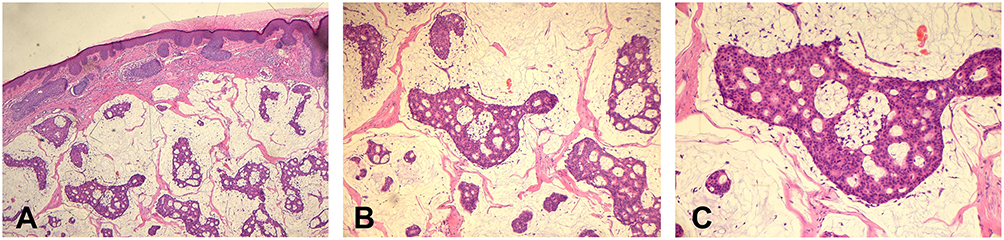 |
Figure 2 Histopathology at the first visit: the dermis showed mucus pools and tumor epithelial components were seen. (HE: (A)×40; (B)×200; (C)×400). |
Physical examination revealed a 1-cm, firm, non-tender, reddish nodule with telangiectasia on the left lower eyelid (Figure 1C). No lymphadenopathy was noted.
Extensive investigations to rule out a primary internal malignancy were undertaken: Tumor markers were largely unremarkable. Whole-body PET-CT and CT scans of the neck, chest, abdomen, and pelvis revealed no evidence of a primary tumor. Breast ultrasound was normal.
Histopathological examination of the completely excised specimen revealed mucin lakes within the dermis containing floating nests, cords, and glandular structures of tumor epithelial cells with moderate atypia. Combined with the clinical history, the findings were consistent with recurrent cutaneous mucinous carcinoma (moderately differentiated), measuring 0.8×0.5cm microscopically (Figure 3A–C). Immunohistochemical staining was positive for CK7, ER, PR, and GATA-3; showed focal weak positivity for CEA and Villin; and was negative for S-100, CK20, CK5/6, Tg, PSA, TTF-1, CDX-2, and SATB2 (Figure 4A–F).
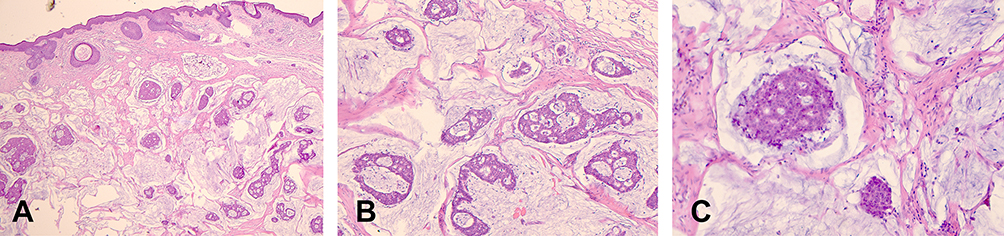 |
Figure 3 The epidermis was generally normal, and the dermis showed mucus pools. Floating nests and adenoid tumor epithelial components were seen, with moderate atypic cell. (HE: (A)×40; (B)×200; (C)×400). |
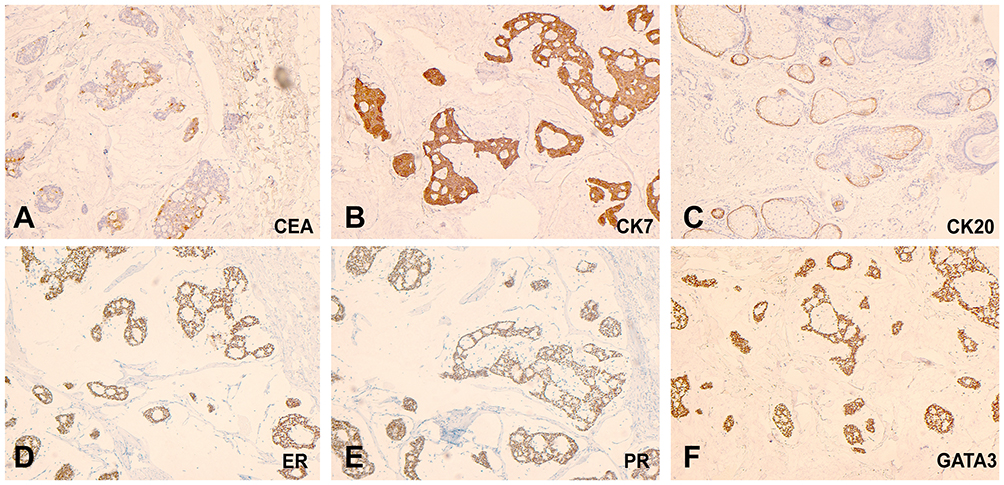 |
Figure 4 Immunochemistry: (A) CEA was partially positive in the tumor mass; (B) CK7 was positive in the tumor mass; (C) CK20 was negative in the tumor mass but positive in sebaceous glands; (D) ER was positive in the tumor mass; (E) PR was positive in the tumor mass; (F) GATA-3 was positive in the tumor mass. (magnification×100). |
A diagnosis of Primary Cutaneous Mucinous Carcinoma was established. The patient underwent MMS with stepwise excision until histologically clear margins were achieved. The resulting defect was repaired with a pedicled flap taken from the adjacent left cheek. The flap included skin and subcutaneous tissue only, without muscle. The postoperative course was uneventful. No adjuvant radiotherapy, chemotherapy, or targeted therapy was given. Follow-up showed good recovery without ischemia or necrosis (Figure 5).
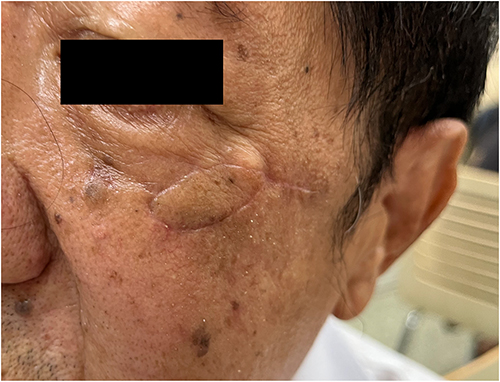 |
Figure 5 Postoperative view following Mohs micrographic surgery and pedicled flap reconstruction. |
Discussion
PCMC remains a diagnostic challenge because its histological features closely resemble those of metastatic mucinous carcinoma. We describe a case of recurrent PCMC of the lower eyelid in an 81-year-old man that was initially misdiagnosed as metastatic carcinoma. The diagnosis was ultimately confirmed through histopathological examination and a characteristic IHC profile. A normal whole-body PET-CT scan further supported the diagnosis. The tumor was successfully managed with MMS, resulting in good local recovery. This case highlights two key points. First, a full IHC panel is essential for differential diagnosis and for ruling out metastasis. Second, MMS is an effective treatment for recurrent PCMC in cosmetically sensitive areas.
Accurate diagnosis of PCMC depends on distinguishing it from metastatic mucinous carcinoma and other primary cutaneous tumors. Helpful discriminators include the thickness of fibrous septa, the epithelial-to-mucin ratio, the CK7/CK20 immunoprofile (PCMC is typically CK7+/CK20-), and the presence of an in-situ component, which favors a primary cutaneous origin.5 Among primary cutaneous tumors, primary cutaneous adenoid cystic carcinoma (PCACC) usually appears as a solitary mass in the head and neck region. Histologically, it is a biphasic tumor composed of ductal and myoepithelial cells.8 Positive MYB protein expression is an important diagnostic feature.8 While basal cell carcinoma (BCC) may mimic PCMC clinically, its diagnosis rests on distinct histopathological features, namely palisading basaloid cells and positive Ber-EP4 staining.9 In our patient, the diagnosis was based on characteristic histopathological findings of dermal mucin pools containing epithelial nests, supported by key IHC results (positive for CK7, ER, PR, and GATA-3; negative for CK20, TTF-1, and CDX-2). This profile helped confirm the tumor was of eccrine sweat glands origin and excluded other types of cancer.
Complete surgical excision remains the mainstay of PCMC treatment, but local recurrence rates are high, ranging from 19% to 45%.10 This emphasizes the importance of achieving histologically negative margins. Surgical options for PCMC include standard excision, wide local excision, and MMS.10 MMS offers advantages in reducing local recurrence rates and improving prognosis,10,11 and is particularly beneficial for areas where tissue preservation is critical, such as the eyelids.12 Given the complex periorbital anatomy in our patient, MMS was chosen for complete tumor removal, followed by pedicled flap reconstruction. The patient recovered well postoperatively.
Furthermore, given the frequent expression of ER and PR in PCMC, anti-estrogen receptor agents like tamoxifen have been proposed as potential therapeutic options.4 For tumors in anatomically challenging locations not amenable to wide excision, anti-estrogen/progesterone receptor therapy might be considered. Our patient has not received adjuvant therapy and remains under close follow-up.
The prognosis for PCMC is generally favorable, with low metastatic potential. Lymph node metastasis occurs occasionally, but distant metastasis is rare.10 However, local recurrence rates are relatively high.1,2 Factors influencing prognosis include treatment modality, tumor diameter, and stage.1 Patients treated surgically have longer survival compared to those untreated, with those undergoing MMS achieving the longest survival, further underscoring its benefit. Future studies should involve multi-institutional cohorts to better define optimal surgical margins, evaluate the long-term effectiveness of MMS, and develop evidence-based management guidelines.
Conclusion
In conclusion, this case serves to reinforce several key principles in the management of PCMC. First, it must remain a prominent consideration in the differential diagnosis of cutaneous mucinous neoplasms. Second, a targeted IHC panel is indispensable for confirming the diagnosis and averting unnecessary and costly systemic investigations for a presumed metastasis. Finally, given the high recurrence rate of PCMC, particularly in critical facial locations, MMS should be strongly considered as the first-line surgical intervention to achieve optimal oncologic and cosmetic outcomes. Further research, including large cohort studies, systematic reviews, and prospective trials comparing treatment approaches, is needed to generate stronger evidence for evidence-based management of PCMC.
Data Sharing Statement
Data is available on request due to privacy/ethical restrictions. The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Consent
The patient has provided written informed consent for the publication of the case details and all accompanying images.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Behbahani S, Pinto JO, Wassef D, et al. Analysis of head and neck primary cutaneous mucinous carcinoma: an indolent tumor of the eccrine sweat glands. J Craniofac Surg. 2021;32(3):e244–5. doi:10.1097/SCS.0000000000006968
2. Rismiller KP, Crowe DR, Knackstedt TJ. Prognostic factors, treatment, and survival in primary cutaneous mucinous carcinoma: a SEER database analysis. Dermatol Surg. 2020;46:1141–1147. doi:10.1097/DSS.0000000000002263
3. Cheng CY, Huang YL, Kuo TT, et al. The histopathological and dermoscopic correlation of primary cutaneous mucinous carcinoma. Indian J Dermatol Venereol Leprol. 2019;85:215–220. doi:10.4103/ijdvl.IJDVL_286_18
4. Kwatra KS, Prabhakar BR, Jain S. Oestrogen and progesterone receptors in primary mucinous carcinoma of skin. Australas J Dermatol. 2005;46:246–249. doi:10.1111/j.1440-0960.2005.00193.x
5. Kazakov DV, Suster S, LeBoit PE, et al. Mucinous carcinoma of the skin, primary, and secondary: a clinicopathologic study of 63 cases with emphasis on the morphologic spectrum of primary cutaneous forms: homologies with mucinous lesions in the breast. Am J Surg Pathol. 2005;29:764–782. doi:10.1097/01.pas.0000159104.02985.6b
6. Breiting L, Christensen L, Dahlstrøm K, et al. Primary mucinous carcinoma of the skin: a population-based study. Int J Dermatol. 2008;47:242–245. doi:10.1111/j.1365-4632.2008.03558.x
7. Tillit SM, Iyer SSR, Grieser EJ, et al. Treatment of recurrent primary cutaneous mucinous carcinoma of the eyelid with modified wide local excision. Case Rep Ophthalmol Med. 2020;2020:6668640. doi:10.1155/2020/6668640
8. Lv JJ, Ren M, Cai X, et al. Primary cutaneous adenoid cystic carcinoma: a clinicopathologic, immunohistochemical, and fluorescence in-situ hybridisation study of 13 cases. Histopathology. 2022;80:407–419. doi:10.1111/his.14565
9. Cameron MC, Lee E, Hibler BP, et al. Basal cell carcinoma: epidemiology; pathophysiology; clinical and histological subtypes; and disease associations. J Am Acad Dermatol. 2019;80:303–317. doi:10.1016/j.jaad.2018.03.060
10. Freeman T, Russell AJ, Council ML. Primary cutaneous mucinous carcinoma: a review of the literature. Dermatol Surg. 2023;49:1091–1095. doi:10.1097/DSS.0000000000003921
11. Chavez A, Linos K, Samie FH. Primary cutaneous mucinous carcinoma of the eyelid treated with Mohs surgery. JAAD Case Rep. 2015;1:85–87. doi:10.1016/j.jdcr.2015.02.002
12. Tolkachjov SN. Adnexal carcinomas treated with mohs micrographic surgery: a comprehensive review. Dermatol Surg. 2017;43:1199–1207. doi:10.1097/DSS.0000000000001167
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.