Back to Journals » International Medical Case Reports Journal » Volume 19
Recurrent Post-Abortion Gestational Trophoblastic Neoplasia Successfully Treated with TP/TE: A Case Report
Authors Afriansyah D, Pribadi A ![]() , Handono B, Salima S
, Handono B, Salima S ![]() , Nisa AS
, Nisa AS ![]() , Rinaldi M
, Rinaldi M
Received 10 October 2025
Accepted for publication 29 December 2025
Published 13 January 2026 Volume 2026:19 566927
DOI https://doi.org/10.2147/IMCRJ.S566927
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Thomas E Hutson
Denis Afriansyah, Adhi Pribadi, Budi Handono, Siti Salima, Aisyah Shofiatun Nisa, Muhamad Rinaldi
Department of Obstetrics and Gynecology, Hasan Sadikin General Hospital-Padjadjaran University, Bandung, Indonesia
Correspondence: Denis Afriansyah, Department of Obstetrics and Gynecology, Hasan Sadikin General Hospital-Padjadjaran University, Jl. Pasteur No. 38, Kel. Pasteur, Kec. Sukajadi, Bandung, 40161, Indonesia, Tel +62 822 3984 4705, Email [email protected]
Introduction: Gestational trophoblastic neoplasia (GTN) is a highly curable malignancy, but cases arising after abortion are uncommon and often diagnosed late. We report a recurrent high-risk GTN following abortion that relapsed multiple times despite etoposide–methotrexate–actinomycin D/cyclophosphamide–vincristine (EMA/CO).
Case Report: A 26-year-old woman achieved initial remission with six cycles of EMA/CO but experienced several recurrences from 2021 to 2023. She presented again with rising β-hCG (16,925.8 mIU/mL) and an intrauterine mass. Paclitaxel/cisplatin alternating with paclitaxel/etoposide (TP/TE) was given for six cycles plus two consolidation cycles, resulting in complete remission. β-hCG normalized by January 2024 and remained undetectable for 12 months.
Conclusion: This case highlights diagnostic challenges of post-abortion GTN and shows that TP/TE is an effective and well-tolerated salvage option for recurrent or EMA/CO-resistant GTN. Long-term β-hCG surveillance is essential to ensure durable remission and assess fertility outcomes.
Keywords: gestational trophoblastic neoplasia, abortion, β-hCG, recurrence, salvage chemotherapy
Introduction
Gestational trophoblastic neoplasia (GTN) represents a malignant continuum of trophoblastic diseases, including invasive mole, choriocarcinoma, placental site trophoblastic tumor (PSTT), and epithelioid trophoblastic tumor (ETT).1,2 It is highly responsive to chemotherapy, with survival exceeding 90% even in high-risk disease.3 Serum β-hCG is the most reliable biomarker for diagnosis, monitoring treatment response, and detecting persistence or recurrence, and rising or plateauing levels after uterine evacuation or chemotherapy define treatment failure.4–6
Although approximately half of GTN cases arise after molar pregnancy, about 25% develop following nonmolar gestations such as miscarriage or abortion.7 Women with a history of spontaneous abortion have a two- to threefold increased risk of subsequent trophoblastic disease.7,8 However, GTN following abortion remains uncommon, with an estimated incidence of 2–200 per 100,000 pregnancies, and often presents with nonspecific symptoms such as persistent bleeding, contributing to diagnostic delay.7,9 As a result, patients may present with higher-risk disease or face an increased likelihood of recurrence after treatment.
For high-risk GTN (FIGO score ≥7), etoposide–methotrexate–actinomycin D/cyclophosphamide–vincristine (EMA/CO) remains the standard first-line regimen, achieving survival rates of approximately 90%.6,10 Around 10% of patients, however, develop drug resistance or experience relapse and require salvage therapy.10,11 Etoposide–cisplatin alternating with EMA (EP/EMA) is an established salvage option but is associated with substantial toxicity, including high rates of neutropenia, thrombocytopenia, anemia, and renal impairment.10–12 Because of these limitations, paclitaxel-based regimens have gained interest. Emerging evidence from small case series and early clinical experiences suggests that paclitaxel/cisplatin alternating with paclitaxel/etoposide (TP/TE) demonstrates meaningful activity and improved tolerability in relapsed or refractory GTN.12–14
This case report describes a rare post-abortion GTN with multiple relapses following EMA/CO, ultimately achieving sustained remission with TP/TE. It underscores the diagnostic challenges of GTN after nonmolar pregnancy, the need for vigilant β-hCG surveillance even after remission, and the potential role of TP/TE as an effective and better-tolerated salvage option for recurrent high-risk GTN.
Case Report
A 26-year-old woman was diagnosed with recurrent gestational trophoblastic neoplasia (GTN) following abortion. Her clinical course began in June 2020 with an abortion managed by uterine evacuation, with histopathology confirming retained products of conception. Despite curettage, she continued to experience vaginal bleeding with a persistently positive urine pregnancy test (qualitative β-hCG). In September 2020, serum β-hCG was 73,870 mIU/mL and rose to >1,000,000 mIU/mL in October, the following month, leading to referral to a tertiary center.
On assessment in November 2020, she complained vaginal bleeding without abdominal pain. Physical examination revealed a uterine fundal height midway between the symphysis and umbilicus. Transvaginal ultrasound demonstrated a uterus measuring 8.50×4.02 × 6.62 cm with two intrauterine masses infiltrating the myometrium (1.27 × 2.35 cm and 2.26×2.17 cm, Doppler +4). She was diagnosed with stage I GTN, FIGO score 8 (high risk), and received EMA/CO chemotherapy (4 cycles plus 2 consolidation cycles, December 2020–May 2021), achieving β-hCG <5 mIU/mL.
During surveillance, β-hCG rose again to 40.7 mIU/mL in December 2021, then she received another 2 cycles of EMA/CO plus 1 consolidation cycle (January–June 2022). By June 2022, β-hCG had declined to 1.75 mIU/mL. In July 2022, β-hCG increased again to 128.7 mIU/mL, and she was given 3 EMA/CO cycles plus 2 consolidation cycles, achieving remission (<5 mIU/mL, December 2022). However, in January 2023, levels rose again to 7 mIU/mL. Chest X-ray, head CT scan, and repeat β-hCG testing were performed, but the patient was lost to follow-up until August 2023.
When she returned in August 2023, she presented with vaginal spotting and provided imaging results from August 2023 showing a normal chest X-ray, a head CT scan without evidence of intracranial metastasis, neoplasm, or vascular malformation. The level β-hCG had increased to 16,925.8 mIU/mL in august 2023. Repeat evaluation revealed an abdominal ultrasound showing a mixed-echogenic uterine mass without calcification, suggestive of recurrent gestational trophoblastic neoplasia, with no evidence of metastasis (Figure 1A). The patient was then scheduled to receive TP/TE chemotherapy (Paclitaxel 135 mg/m2 / Cisplatin 60 mg/m2 alternating with Paclitaxel 135 mg/m2 / Etoposide 150 mg/m2). The timeline of the disease is illustrated in Figure 1B.
 |
Figure 1 (A) Transverse pelvic ultrasonography showing a heterogeneous intrauterine mass with cystic spaces, measuring approximately 7.04×5.23 cm. (B) Sagittal Doppler pelvic ultrasonography showing a hypervascular intrauterine mass with prominent peripheral and intralesional blood flow signals. |
The patient received six cycles of TP/TE followed by two consolidation cycles, resulting in a decline of β-hCG from 75,367.6 mIU/mL (September 2023) to 2.8 mIU/mL (January 2024). Twelve months of surveillance showed persistently normal β-hCG. At the latest follow-up, the patient had regular menstrual cycles and normal ovarian function. No markers of diminished ovarian reserve were noted; however, anti-Müllerian hormone (AMH) levels were not assessed due to limited availability at the time. Timeline of the patient’s clinical course, including initial presentation, serial β-hCG trends, periods of loss to follow-up, and chemotherapeutic regimens administered from 2020 to 2024 was shown in Figure 2.
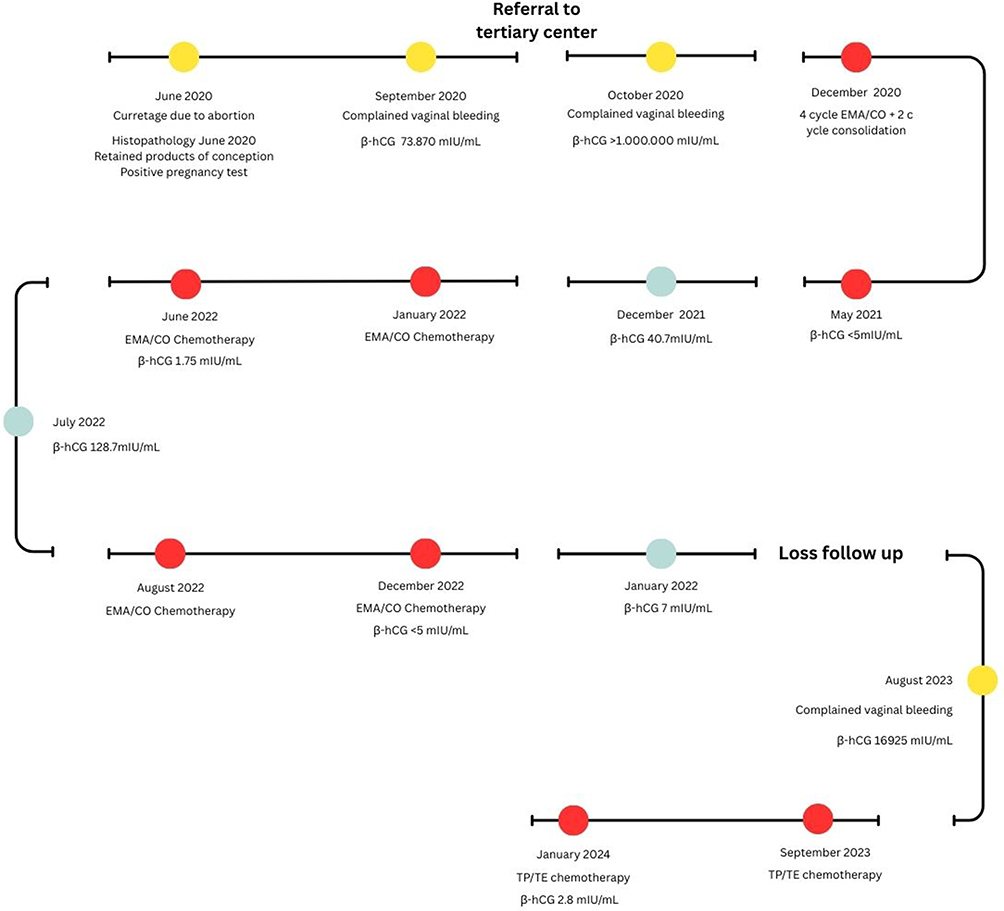 |
Figure 2 Timeline of the patient’s clinical course, including initial presentation, serial β-hCG trends, periods of loss to follow-up, and chemotherapeutic regimens administered from 2020 to 2024. Yellow markers indicate clinical presentations or diagnostic events; red markers represent chemotherapy treatments; blue markers represent follow-up evaluations and β-hCG monitoring. |
Discussion
GTN is a pregnancy‑associated malignancy characterized by placental origin and the presence of paternal genetic material, conferring unique biologic behavior and marked chemosensitivity. However, GTN is able to evade both maternal and placental immune surveillance, permitting unchecked proliferation, invasion, and metastatic spread. These immune escape mechanisms are thought to underlie the persistence and progression of GTN.15
The pathophysiology is closely related to alterations within the placental villi. The villous structure is composed of distinct cellular compartments: trophoblasts (including cytotrophoblasts and syncytiotrophoblasts), mesenchymal elements with Hofbauer cells, and extravillous trophoblasts (EVTs). Cytotrophoblasts generate syncytiotrophoblasts, which produce β-hCG and interact directly with maternal blood. Hofbauer cells, in turn, contribute to vasculogenesis through VEGF secretion, while also mediating maternal-fetal immune interactions.16,17 EVTs are of particular importance, as they share invasive, tumor-like behavior and are capable of infiltrating the decidua and maternal circulation.18 Normally, this invasion is tightly regulated by a balance of stimulatory and inhibitory signals in the myometrium. In GTN, disruption of this equilibrium drives uncontrolled trophoblast proliferation, invasion, and dissemination.16,19
GTN most commonly develops following a hydatidiform mole; however, this case illustrates the occurrence of GTN after an abortion. Persistent vaginal bleeding after curettage should always prompt careful evaluation for the possibility of GTN. In this case, the patient underwent curettage for abortion but continued to experience abnormal vaginal bleeding, leading the physician to perform a quantitative β-hCG test. The markedly elevated β-hCG level raised suspicion of GTN, and the patient was subsequently referred to a tertiary care center for further management. She was diagnosed with GTN with a FIGO score of 8, categorized as high risk, and was therefore treated with EMA/CO combination chemotherapy. Table 1 summarizes reported cases of GTN following abortion.
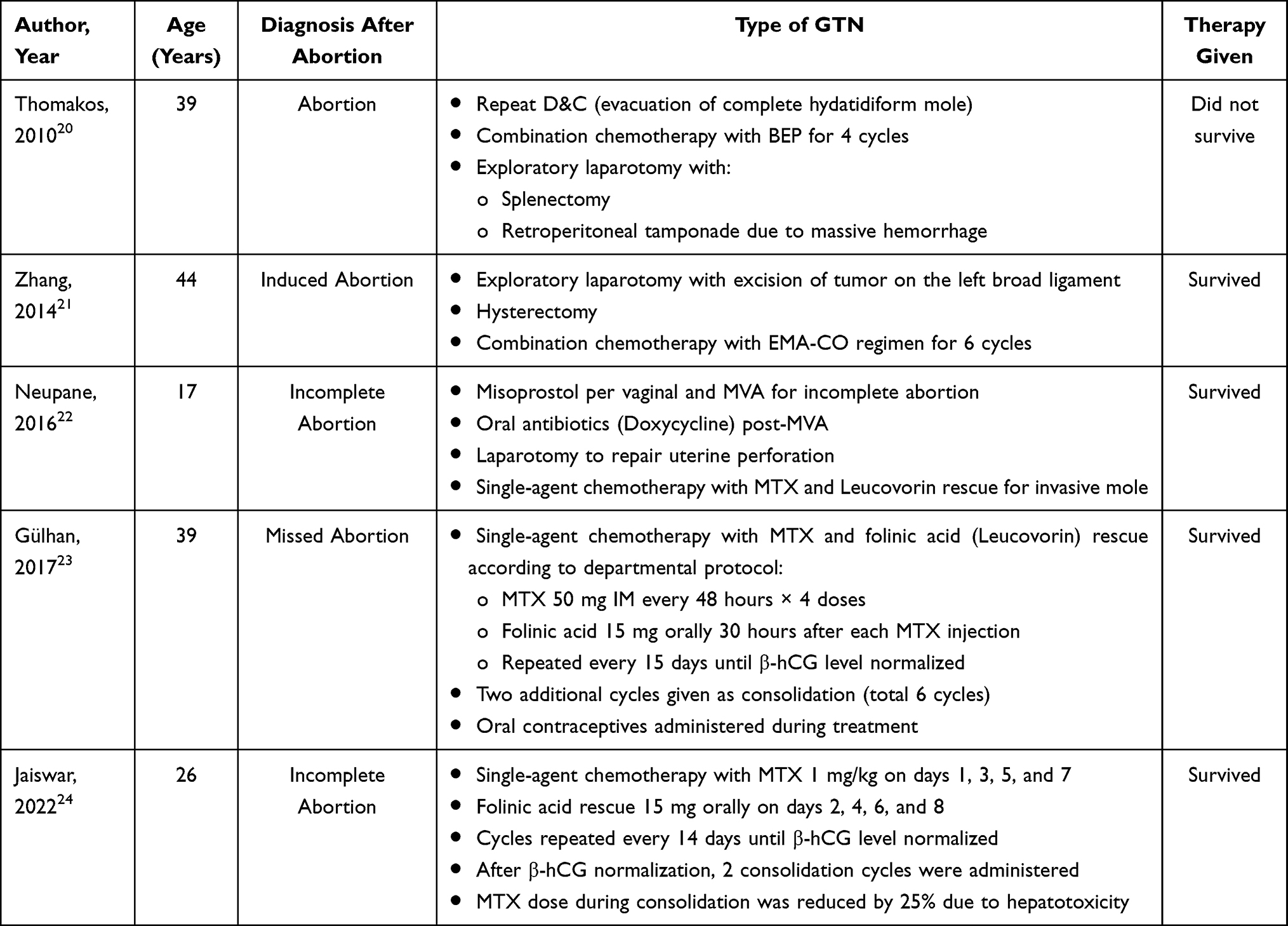 |
Table 1 Summarizes of Reported Cases of GTN Following Abortion |
Recurrent disease was evaluated using serial quantitative serum β-hCG measurements, clinical assessment, and imaging studies, including transvaginal and abdominal ultrasonography, chest radiography, and head CT when indicated. Importantly, alternative causes of β-hCG elevation—namely phantom hCG, quiescent GTN, and pituitary hCG—were considered during the evaluation of recurrence.
The marked rise in β-hCG to 16,925.8 mIU/mL occurring 7–8 months after completion of chemotherapy is inconsistent with phantom hCG, quiescent GTN, or pituitary hCG. Phantom hCG is characterized by low, non-progressive serum hCG levels without clinical or radiologic correlation and does not respond to chemotherapy. Quiescent GTN typically presents with persistently low and stable β-hCG levels (<200 mIU/mL), absence of symptoms, and no radiologic evidence of disease. Pituitary hCG occurs at very low levels in peri- or postmenopausal women. In contrast, this patient demonstrated progressive β-hCG elevation, clinical symptoms, radiologic evidence of uterine disease, and a prompt biochemical response to chemotherapy, confirming active recurrent GTN.
The treatment for GTN is chemotherapy, with the regimen selected based on stage and prognostic scoring. According to the 2000 FIGO system, patients with a score ≤6 are classified as low risk, while those with a score ≥7 are considered high risk. High-risk GTN, as in the present case, is primarily managed with combination chemotherapy such as EMA/CO, which is continued until β-hCG normalization. The EMA/CO regimen consists of etoposide, actinomycin D, and methotrexate on days 1–2, followed by cyclophosphamide and vincristine on day 8. An alternative protocol is EMA/EP, in which etoposide and cisplatin are administered on day 8 in place of cyclophosphamide and vincristine.25 According to the NCCN Clinical Practice Guidelines, once β-hCG levels have normalized, treatment should be continued with consolidation therapy. This consists of 2 cycles of single-agent chemotherapy for low-risk GTN, and 2–3 additional cycles of multi-agent chemotherapy, such as EMA/CO or EMA/EP, for high-risk disease.26
Although GTN is highly chemosensitive, approximately 25% of patients with high-risk disease may experience persistence or recurrence following first-line therapy, or relapse after initial remission, resulting in residual disease. This phenomenon is thought to be related to an imbalance between stimulatory and inhibitory mechanisms during the cellular phase, even after treatment. GTN employs several immune evasion strategies, such as: (1) imitating immune tolerance mechanisms by lacking HLA class II expression, thereby escaping T-cell recognition and cytolysis; (2) resisting natural killer (NK) cell–mediated cytotoxicity; (3) downregulating conventional activation markers—including CD69 (NK cells), CD71 (macrophages), CD134 (T cells), CD3/HLA-DR (T cells)—as well as the apoptosis marker CD95 (Fas) on lymphocytes; and (4) overexpressing hCG receptors and increasing hCG secretion, which enhances local immunosuppression at the uterine site and prevents malignant trophoblast detection by the maternal immune system. Several clinical risk factors contribute to this phenomenon.
Higher total FIGO scores are strongly associated with chemotherapy resistance, largely reflecting a greater tumor burden (eg, markedly elevated β-hCG levels, larger tumor size, multiple metastases) rather than independent prognostic factors. Inadequate primary therapy and poor treatment adherence also play critical roles in resistance development.27,28 Additionally, Doppler ultrasound studies have suggested that a low uterine artery pulsatility index before chemotherapy indicates increased tumor vascularization and a higher risk of methotrexate resistance.28 In the present case, the patient’s markedly high FIGO score, extremely elevated pretreatment β-hCG concentration (>1,000,000 mIU/mL), and treatment interruption contributed to the risk of relapse, necessitating salvage chemotherapy.27
Salvage chemotherapy options for recurrent GTN include Paclitaxel/Cisplatin–Paclitaxel/Etoposide (TP/TE), a regimen initially developed for germ cell tumors. More recently, case reports have described its benefit in two untreatment GTN patients. In a prior cohort of 24 patients receiving TP/TE, 16 had refractory or relapsed disease after earlier therapy. Within this subgroup, survival was relatively low (45%), reflecting the fact that most had undergone two or more previous regimens, including six patients who had failed platinum-based treatment (five after EP/EMA and one after BEP). Conversely, survival outcomes were more favorable (75%) in eight patients who were switched to TP/TE because of toxicity from their prior regimens, including six previously treated with EP/EMA. Notably, compared with EMA/CO, TP/TE was associated with a more tolerable toxicity profile, despite its use in patients who had generally received more intensive prior therapy. Severe neutropenia (grade 3–4) occurred in 42% and thrombocytopenia in 13% of TP/TE patients, compared with 68% and 40% among those receiving EP/EMA. Importantly, no TP/TE patients developed neutropenic sepsis or required treatment delays, whereas 88% of EP/EMA patients experienced delays, partly due to neutropenic sepsis.12,14
Nonetheless, two key uncertainties remain regarding TP/TE use: first, the long-term survival outcomes, given the relatively short follow-up in available series; and second, its potential impact on fertility. While animal studies and limited case reports indicate that pregnancy is possible after paclitaxel exposure, further data are required.12,14,29 Consequently, in cases of recurrent high-risk GTN, combination regimens such as TP/TE or EP/EMA may be considered.
This patient initially presented with FIGO stage I disease but was categorized as high risk, with a FIGO score of 8. She was started on multi-agent chemotherapy with the EMA/CO regimen. Despite this, recurrence occurred, and salvage therapy with TP/TE was initiated in September 2023. The patient had complete response. Overall survival following chemotherapy in GTN is excellent, approaching 98%, but outcomes vary according to the risk of drug resistance determined by the FIGO score. Low-risk patients (scores 0–6) are treated with methotrexate and folinic acid, achieving nearly 100% survival, although up to one-third require second-line treatment with either intravenous actinomycin D alone or combination regimens such as EMA/CO.8 In contrast, patients with high-risk disease (score ≥7) are treated with EMA/CO as first-line therapy, with survival rates of approximately 90%.12,14,29,30 Nevertheless, more than 10% of these patients experience treatment failure. For women who relapse after EMA/CO, prior studies suggest that cisplatin can be incorporated with etoposide (EP) alternating weekly with EMA, sometimes alongside surgery, resulting in salvage rates of around 75%. However, this regimen is associated with substantial toxicity, as 40% of patients experience grade 3–4 adverse effects, including neutropenia (68%), thrombocytopenia (40%), anemia (21%), renal impairment (41%), and other complications. Consequently, there remains a need for salvage regimens with greater efficacy and a more favorable toxicity profile.12,14,29,30
If patients fail to respond to TP/TE, several studies have reported alternative salvage options, including gemcitabine-based regimens and high-dose chemotherapy (HDC) with stem cell rescue, which may be combined with surgical procedures such as hysterectomy. Patients who achieve a response to TP/TE generally show better outcomes with subsequent therapies.8,11,14 Because these patients are classified as high risk, the standard first-line treatment is EMA/CO. Serial quantitative β-hCG monitoring plays a central role in identifying drug resistance, recurrence, and therapeutic response.
All GTN patients require quantitative serum β-hCG surveillance for 12 months following treatment. The recommended schedule is every two weeks during the first three months, monthly for the next three months, and every two months over the final six months. In addition, chest radiography is suggested at 6 and 12 months if respiratory symptoms are present.25 In patients with stage IV disease, follow-up is extended to 24 months due to the higher risk of late recurrence.
Monitoring should continue until β-hCG levels remain undetectable for 12 consecutive months, during that, time effective contraception must be maintained. Patients should also be assessed for complications such as hemorrhage or metastatic disease involving the pelvis, abdomen, liver, or brain. Imaging modalities including pelvic and abdominal ultrasound, chest radiography, CT, or MRI may be employed as clinically indicated. During the surveillance phase, pregnancy is contraindicated, and only barrier methods or the calendar method are advised, whereas intrauterine devices and injectable contraceptives should be avoided.25
The incidence of secondary infertility following chemotherapy for GTN is relatively low, around 7%, indicating that most women who wish to conceive are able to achieve pregnancy.31,32 A large multicenter study involving 2,657 women demonstrated reassuring reproductive outcomes: the majority achieved live births, with rates of miscarriage, stillbirth, and congenital malformations comparable to the general population. Importantly, no significant differences were observed between single-agent and multi-agent regimens in terms of fertility or pregnancy outcomes. Current recommendations advise a 12-month follow-up period before attempting conception in stage I–III disease and 24 months in stage IV, to allow accurate β-hCG monitoring and reduce risks of adverse pregnancy outcomes. Pregnancies occurring within 6 months of treatment completion carry a higher risk of miscarriage, stillbirth, or recurrent molar pregnancy.31,32 In the present case, the patient achieved normal β-hCG levels during 12 months of surveillance post-chemotherapy; however, she has not yet conceived.
This case highlights several clinically important points. First, GTN can arise after abortion and should be considered in patients with persistent vaginal bleeding and elevated β-hCG following nonmolar pregnancy. Second, recurrent high-risk GTN may require alternative salvage chemotherapy strategies, particularly after failure of standard EMA/CO therapy. In this context, TP/TE demonstrated effective disease control with acceptable tolerability. Third, this case underscores the central role of serial quantitative β-hCG monitoring in detecting recurrence early and guiding timely therapeutic interventions.
This report has several limitations. First, as a single case report, the findings may not be generalizable to all patients with recurrent GTN. Second, the follow-up duration is insufficient to fully evaluate long-term survival and fertility outcomes following TP/TE therapy. Third, limited molecular profiling and imaging data precluded deeper exploration of the biological mechanisms underlying chemotherapy resistance and disease recurrence. Larger studies with longer follow-up are needed to better define the role of TP/TE in recurrent high-risk GTN.
Implications
This case highlights several important clinical implications. First, gestational trophoblastic neoplasia can occur after spontaneous abortion, emphasizing the need for early recognition and routine serial quantitative β-hCG monitoring to detect recurrence promptly. Second, in patients with recurrent high-risk GTN after standard EMA/CO therapy, TP/TE may serve as an effective and better-tolerated salvage regimen, supporting its consideration in treatment algorithms. Finally, long-term surveillance remains essential to ensure durable remission and to evaluate reproductive outcomes in women of reproductive age. This case supports vigilant post-abortion follow-up and individualized escalation of therapy in recurrent GTN.
Conclusion
Spontaneous abortion may be followed by gestational trophoblastic neoplasia, underscoring the importance of serial β-hCG monitoring. In recurrent disease, timely modification or escalation of chemotherapy, including the use of alternative salvage regimens such as TP/TE, is crucial to achieve sustained remission.
Registration of Research Studies
Registration of research is not applicable in our case.
Abbreviations
BEP, Bleomycin–Etoposide–Cisplatin; β-hCG, Beta–human Chorionic Gonadotropin; D&C, Dilation and Curettage; EMA-CO, Etoposide–Methotrexate–Actinomycin D–Cyclophosphamide–Vincristine; IM, Intramuscular; MVA, Manual Vacuum Aspiration; MTX, Methotrexate; OCP, Oral Contraceptive Pills.
Ethical Approval
This study adhered to the principles of the Declaration of Helsinki and institutional guidelines for case reports. Written informed consent was obtained from the patient for publication of anonymized clinical details and accompanying images.
Informed Consent Patient Statement
The authors confirm that written informed consent has been obtained from the involved patient. The patient has been informed about the details of the case and has provided approval for the information to be published in this case report.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study did not receive external funding.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Höhn AK, Brambs CE, Hiller GGR, May D, Schmoeckel E, Horn LC. 2020 WHO classification of female genital tumors. Geburtshilfe Frauenheilkd. 2021;81(10):1145–9.
2. Kaur B, Short D, Fisher RA, Savage PM, Seckl MJ, Sebire NJ. Atypical placental site nodule (APSN) and association with malignant gestational trophoblastic disease; a clinicopathologic study of 21 cases. Int J Gynecol Pathol. 2015;34(2):152–158. doi:10.1097/PGP.0000000000000128
3. Fisher RA, Maher GJ. Genetics of gestational trophoblastic disease. Best Pract Res Clin Obstet Gynaecol. 2021;74:29–41. doi:10.1016/j.bpobgyn.2021.01.004
4. Lurain JR. Hydatidiform mole: recognition and management. Contemporary OB/GYN. 2019;64(3):12–17.
5. Thapa B, Maharjan M, Tuladhar H. Persistent gestational trophoblastic disease following ovarian molar pregnancy: a case report of a rare entity with review of the literature. Clin Case Rep. 2021;9(9):e04738. doi:10.1002/ccr3.4738
6. Alazzam M, Tidy J, Osborne R, Coleman R, Hancock BW, Lawrie TA. Chemotherapy for resistant or recurrent gestational trophoblastic neoplasia. Cochrane Database Syst Rev. 2016;2016(1):Cd008891. doi:10.1002/14651858.CD008891.pub3
7. Bruce S, Sorosky J. Gestational Trophoblastic Disease. Treasure Island (FL): StatPearls Publishing; 2025.
8. Ngan HYS, Seckl MJ, Berkowitz RS, et al. Diagnosis and management of gestational trophoblastic disease: 2021 update. Int J Gynaecol Obstet. 2021;155(Suppl 1):86–93. doi:10.1002/ijgo.13877
9. Eiriksson L, Wells T, Steed H, et al. Combined methotrexate-dactinomycin: an effective therapy for low-risk gestational trophoblastic neoplasia. Gynecol Oncol. 2012;124(3):553–557. doi:10.1016/j.ygyno.2011.10.036
10. Santaballa A, García Y, Herrero A, et al. SEOM clinical guidelines in gestational trophoblastic disease (2017). Clin Transl Oncol. 2018;20(1):38–46. doi:10.1007/s12094-017-1793-0
11. Alifrangis C, Agarwal R, Short D, et al. EMA/CO for high-risk gestational trophoblastic neoplasia: good outcomes with induction low-dose etoposide-cisplatin and genetic analysis. J Clin Oncol. 2013;31(2):280–286. doi:10.1200/JCO.2012.43.1817
12. Garcia-Sayre J, Castaneda AV, Roman LD, Matsuo K. Diagnosis and management of gestational trophoblastic disease. In: Shoupe D, editor. Handbook of Gynecology. Cham: Springer; 2023.
13. Lurain JR, Schink JC. Immunotherapy versus chemotherapy for methotrexate-resistant low-risk gestational trophoblastic neoplasia. J Clin Oncol. 2020;38(36):4349–4350. doi:10.1200/JCO.20.02613
14. Wang J, Short D, Sebire NJ, et al. Salvage chemotherapy of relapsed or high-risk gestational trophoblastic neoplasia (GTN) with paclitaxel/cisplatin alternating with paclitaxel/etoposide (TP/TE). Ann Oncol. 2008;19(9):1578–1583. doi:10.1093/annonc/mdn181
15. Huppertz B. Traditional and new routes of trophoblast invasion and their implications for pregnancy diseases. Int J Mol Sci. 2019;21(1):289. doi:10.3390/ijms21010289
16. Sharma N, Kundal R, Kaushal V. Immunobiology and immunotherapy of gestational trophoblastic disease. Gynecol Obstetrics Clinl Med. 2022;2(2):76–81. doi:10.1016/j.gocm.2022.04.008
17. Weiss G, Sundl M, Glasner A, Huppertz B, Moser G. The trophoblast plug during early pregnancy: a deeper insight. Histochem Cell Biol. 2016;146(6):749–756. doi:10.1007/s00418-016-1474-z
18. Allerkamp HH, Clark AR, Lee TC, Morgan TK, Burton GJ, James JL. Something old, something new: digital quantification of uterine vascular remodelling and trophoblast plugging in historical collections provides new insight into adaptation of the utero-placental circulation. Hum Reprod. 2021;36(3):571–586. doi:10.1093/humrep/deaa303
19. Roberts VHJ, Morgan TK, Bednarek P, et al. Early first trimester uteroplacental flow and the progressive disintegration of spiral artery plugs: new insights from contrast-enhanced ultrasound and tissue histopathology. Hum Reprod. 2017;32(12):2382–2393. doi:10.1093/humrep/dex301
20. Thomakos N, Rodolakis A, Belitsos P, et al. Gestational trophoblastic neoplasia with retroperitoneal metastases: a fatal complication. World J Surg Oncol. 2010;8:114. doi:10.1186/1477-7819-8-114
21. Zhang X, Shi H, Chen X. Epithelioid trophoblastic tumor after induced abortion with previous broad choriocarcinoma: a case report and review of literature. Int J Clin Exp Pathol. 2014;7(11):8245–8250.
22. Neupane S, Amatya A, Shrestha R. Gestational trophoblastic neoplasia following term pregnancy: a rare presentation. J Nepal Health Res Council. 2016;14(33):192–195.
23. Gülhan İ, Ibrahim Yıldız H, Inan H, Bağcı M, Erkılınç S, Sancı M. Gestational trophoblastic neoplasia after miscarriage with dilatation and curettage with normal histological findings. Curr Gynecol Oncol. 2017;15(2):146–148. doi:10.15557/CGO.2017.0015
24. Jaiswar SP, Agrawal M, Deo S, Saad S. Cervical gestational trophoblastic neoplasia: a rare form of gestational trophoblastic disease. J Cancer Res Ther. 2022;18(3):827–830. doi:10.4103/jcrt.JCRT_959_20
25. Hidayat YM. Mola Hidatidosa Dan Deteksi Keganasan Pasca Evakuasi Mola. Bandung: Pustaka Unpad; 2020.
26. N NCC. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®): Gestational Trophoblastic Neoplasia. Version 2.2025. Plymouth Meeting (PA): National Comprehensive Cancer Network, Inc.; 2025.
27. Hussain A, Aziz SA, Bhatt GM, et al. Gestational trophoblastic neoplasia: experience from a Tertiary Care Center of India. J Obstet Gynaecol India. 2016;66(6):404–408. doi:10.1007/s13224-015-0710-0
28. Weng Y, Liu Y, Benjoed C, et al. Evaluation and simplification of risk factors in FIGO 2000 scoring system for gestational trophoblastic neoplasia: a 19-year retrospective analysis. J Zhejiang Univ Sci B. 2022;23(3):218–229. doi:10.1631/jzus.B2100895
29. Ahamed E, Short D, North B, Savage PM, Seckl MJ. Survival of women with gestational trophoblastic neoplasia and liver metastases: is it improving? J Reprod Med. 2012;57(5–6):262–269.
30. Bolze PA, Mathe M, Hajri T, et al. First-line hysterectomy for women with low-risk non-metastatic gestational trophoblastic neoplasia no longer wishing to conceive. Gynecol Oncol. 2018;150(2):282–287. doi:10.1016/j.ygyno.2018.05.030
31. May T, Goldstein DP, Berkowitz RS. Current chemotherapeutic management of patients with gestational trophoblastic neoplasia. Chemother Res Pract. 2011;2011:806256. doi:10.1155/2011/806256
32. Garrett L, Garner E, Feltmate C, Goldstein D, Berkowitz R. Subsequent pregnancy outcomes in patients with molar pregnancy and persistent gestational trophoblastic neoplasia. J Reprod Med. 2008;53:481–486.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.