Back to Journals » Research Reports in Clinical Cardiology » Volume 7
Recurrent pericarditis: current challenges and future prospects
Authors Dauphin C, Merlin E, Chalard A, Trésorier R, Lusson J, Soubrier M
Received 18 January 2016
Accepted for publication 5 May 2016
Published 18 July 2016 Volume 2016:7 Pages 99—108
DOI https://doi.org/10.2147/RRCC.S87827
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Richard Kones
Claire Dauphin,1 Etienne Merlin,2 Aurélie Chalard,1 Romain Trésorier,1 Jean-René Lusson,1 Martin Soubrier3
1Department of Cardiology and Cardiovascular Diseases, 2Department of Pediatrics, 3Department of Rheumatology, Clermont-Ferrand Hospital, Clermont-Ferrand, France
Abstract: Recurrent pericarditis, usually idiopathic, is difficult to treat. Previous etiological studies can eliminate potentially serious causes that require specific treatment. The pathophysiology of “idiopathic” pericarditis involves autoimmunity and autoinflammation in various degrees and is usually caused by a microbacteriological or postinjury trigger. It requires multidisciplinary care to provide individualized treatment to each patient: treatment escalation by increments, then weaning should be guided by clinical examination but also CRP and potential magnetic resonance imaging. The role of immunomodulators, especially anakinra, should be revisited. Their efficacy is remarkable, and they could be considered for second-line treatment, preferably with corticosteroids (at least among certain selected patients), especially after the failure of prolonged and high-dose standard therapy with aspirin/nonsteroidal anti-inflammatory drugs and colchicine.
Keywords: recurrent pericarditis, review, pathophysiology, individualized treatment, multidisciplinary care, treatment options
Introduction
Recurrence is the main complication of acute pericarditis. It occurs in about one-third of cases, and after the first recurrence in half of all cases.1–3 While the prognosis of this disease is ultimately good,4 its functional and social impact is significant. The 2015 European recommendations on the treatment of pericardium diseases5 provide the definition, risk factors, and some therapeutic principles: it is referred to as “recurrent” pericarditis when symptoms reappear after a disease-free period of 4–6 weeks following a first episode of acute pericarditis. A diagnosis of “incessant” pericarditis can be made when symptoms persist for more than 4 weeks after an acute episode without a free interval and “chronic” pericarditis after 3 months of disease progression. These three entities present similar diagnostic and therapeutic difficulties, although their pathophysiology remains unclear and their treatment is not standardized (ie, several therapeutic options exist including personalized treatment, where the duration of treatment is dependent on progression). The diagnostic criteria of recurrent pericarditis are as follows: 1) a documented initial episode of acute pericarditis; 2) the reemergence of pericarditis type pain; and 3) it is associated with at least one of the following signs: pericardial friction, evocative electrical modifications, new or increased pericardial effusion, elevated CRP, evidence of pericardial inflammation by cross-sectional imaging (magnetic resonance imaging [MRI] or computed tomography [CT] scan).5–7 This confirmation is important in cases of recurrence where symptoms are sometimes worn and limited to pain.3,8 It is not uncommon after several episodes of pericarditis that patients complain of suggestive pain without objective signs of recurrence. This pain must of course be treated while avoiding therapeutic escalation.9,10 Resistance to treatment or recurrence in the absence of a clearly demonstrated etiology is more common in the group of patients defined as “high risk”.5 That is, women (63.6% vs 41.8%) with subacute beginning, abundant pericardial effusion, or tamponade (16.4% vs. 2.5%),11 fever over 38°C and major inflammatory syndrome,1,2 showing lack of improvement after 1 week of treatment with nonsteroidal anti-inflammatory drugs (NSAIDs) or aspirin, no colchicine treatment, but especially prescription of corticosteroids during the first episode that could promote a possible viral replication. Most often, however, the recurrence is secondary to the use of insufficient doses of NSAIDs and/or a therapeutic weaning that is too early and too fast. Resistance to treatment or recurrence is more common in patients with autoimmune disease (30.9% vs. 5%).
The objective of this article is to review the etiology, workup, and treatment for this disease, especially new, emerging therapeutic options.
Etiology
The cause of pericarditis is very often investigated in the acute phase, and among the different publications, it is difficult to distinguish etiological research between acute and recurrent pericarditis.12 A recent prospective study on 933 patients hospitalized with acute pericarditis, who underwent an etiological assessment, led to a new diagnosis in 6.7% of patients only (among these, 53% were infectious). Approximately 55% of these cases of pericarditis remained “idiopathic”, 21% were “postinjury”, and 16% had complications from an already known pathology.13
Although a comprehensive etiological investigation is not of interest in the absence of specific treatment during the first episode of acute pericarditis,5 it is recommended in patients with high risk of pericarditis escalating to chronic, recurrent, or incessant to investigate the causes requiring specific treatment (Table 1). However, in the case of so-called idiopathic pericarditis, it is common that an investigation is not renewed with each occurrence. The diagnosis should remain a diagnosis of exclusion, but accounts for 70%–90% of cases in different published series,10,14–16 with the exception of a small pediatric series (6.7%).17 The typical causes are infectious (bacterial or viral), neoplastic, autoimmune, postcardiac injury, or drug-induced.
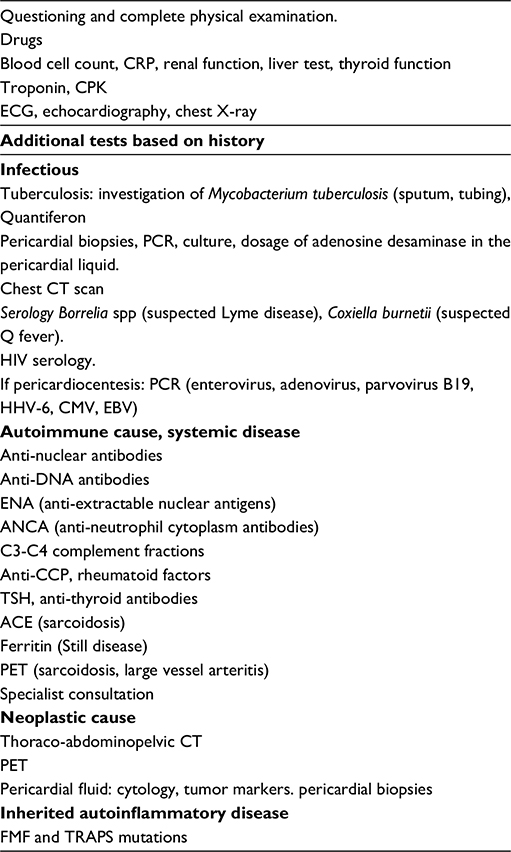 | Table 1 Proposed etiological workup Abbreviations: CT, computed tomography; ECG, electrocardiogram; HIV, human immunodeficiency virus; CCP, cyclic citrullinated peptide; CMV, cytomegalovirus; CPK, creatine phosphokinase; EBV, Epstein-Barr virus; HHV-6, human herpes virus-6; PCR, polymerase chain reaction; PET, positron emission tomography; TSH, thyroid-stimulating hormone; FMF, familial Mediterranean fever. |
In a review of recent literature, pericarditis was often found to be neoplastic (5%–10%), secondary to a systemic disease or postinjury (2%–7%), tuberculosis (4%), and purulent (<1%).10
Bacterial infections
Tuberculosis is the predominant cause of pericarditis from bacterial infection. Although tuberculosis represents <4% of pericarditis cases in developed countries, it is the primary etiology in developing countries where it is responsible for 50%–70% of pericarditis cases in nonhuman immunodeficiency virus-infected patients, and up to 90% of patients infected with human immunodeficiency virus. The diagnosis is confirmed by the analysis of the pericardial fluid or pericardial biopsy, but in the case of known tuberculosis, an unexplained lymphocytic pericarditis is likely with the elevation of unstimulated interferon-gamma adenosine desaminase or lysozyme in the pericardial fluid and/or a treatment response test.5
Viral etiology
A viral cause is found in around 20% of cases, when an analysis of the pericardial fluid or pericardium is carried out.18,19 The persistence of viral RNA in the pericardium can maintain inflammation by triggering mimicry of autoimmunity against cardiac-specific proteins. Little correlation is found between throat swabs, serology, and isolation of viral fragments from the pericardium or pericardial fluid. However, this invasive research is performed rarely because of the absence of a known specific treatment and the impossibility of preventing the persistence of viral particles in the pericardium.19
Neoplastic pericarditis
The diagnosis of neoplastic pericarditis is usually made by imaging, fluid analysis, or pericardial biopsies.5 In the presence of an underlying neoplasia, malignancy of the effusion is confirmed by the infiltration of the pericardium. Indeed, in two-thirds of cases, pericardial involvement is secondary to other causes: radiation, infections, and so on. Primary malignant pericardial neoplasm is a rare cause of recurrent pericarditis: 0% in published series,14–17 although it is documented in some clinical cases.20
Systemic diseases
Systemic diseases are responsible for 5%–15% of recurrent pericarditis. Pericarditis is a well-known clinical manifestation of lupus erythematosus, Sjögren syndrome, rheumatic arthritis, scleroderma, and also systemic vasculitis, sarcoidosis, and inflammatory colitis. Pericardial disease is rarely identified first, but rather complicates an already known disease and falls under the latter’s treatment.21 Autoimmune inflammatory diseases will be considered in the pathogenesis of idiopathic recurrent pericarditis.
Postcardiac injury syndromes
This group includes postinfarction pericarditis (Dressler syndrome), posttraumatic pericarditis, postpericardiotomy pericarditis, and postinterventional pericarditis (pacemaker, coronary dilation, rhythm disorder ablation by radiofrequency, atrial septal defect closure, closure of the atrial appendage, etc).22 It is secondary to an “attack” of pericardial mesothelial cells and/or bleeding, however small in the pericardial cavity, which would trigger an autoimmunity reaction in susceptible patients, as evidenced by the presence of antiheart antibodies. Its frequency increases with the development of invasive techniques. It could be promoted by a viral infection as evidenced by a seasonal recrudescence. Clinical signs are usually “noisy” due to their association with a marked inflammatory syndrome and pericardial effusion of average abundance that is often associated with pleural effusion. The history of cardiac surgery in recurrent pericarditis is 13%–25% in adults, but 47% in children.17 It is possible that this difference is due to the higher frequency of postpericardiotomy syndrome in children. However, these data are based on a single-center series of 15 cases of recurrent pericarditis in children.17 Postcardiac injury syndromes are more frequent in women and after pleural opening, and colchicine given postoperatively showed a preventive effect.23 The progression is usually benign, but with an initial risk of tamponade and abundant pleural effusion, and a risk of progression to constriction of 2%–5%.
Drug-induced pericarditis
Cases of drug-induced pericarditis are rare, but may be due to different mechanisms: drug-induced lupus erythematosus (procainamide, hydralazine, methyldopa, isoniazid, and phenytoin), hypersensitivity or idiosyncratic reaction (penicillins, amiodarone, methisergide, mesalazine, clozapine, minoxidil, dantrolene, practolol, phenylbutazone, thiazides, streptomycin, thiouracil, streptokinase, p-aminosalicylic acid, sulfa drugs, cyclosporine, bromocriptine, several vaccines, and anti-tumor necrosis factor [TNF] agents) secondary to chemotherapy (anthracycline derivatives, 5-fluorouracil, and cyclophosphamide), scorpion venom, and so on.5–24
Pathophysiology of idiopathic recurrent acute pericarditis
The pathophysiology of idiopathic recurrent acute pericarditis (IRAP) remains controversial and may involve both an infectious cause (usually viral or bacterial) as a trigger or an autoimmune and autoinflammatory cause in susceptible patients.8–25 The role of autoimmunity is suggested by several elements: 1) the presence of antinuclear antibodies is more common in patients suffering from IRAP (43.4%) than among controls (9.8%),8 but rarely at a rate higher than 1/160 (5%)26; 2) the presence of antiheart and anti-intercalated disk antibodies in 67.5% of patients with IRAP probably induced by overexposure to self-antigens secondary to myocardial or pericardial disease: pericardiotomy, myocardial infarction, pacemaker implant, and so on11–27; 3) the presence of proinflammatory cytokines (interleukin [IL]-6, IL-8, and interferon-γ) in the pericardial fluid, but not in the plasma, indicating a local inflammation28; and 4) the incidence of pericardial disease in connective tissue disease and vasculitis.
This inflammatory stimulation could be triggered in the absence of systemic disease or myocardial damage by a misdirected immune reaction against microorganisms, usually viral, even when serologies are negative. The microorganism would act as a trigger in predisposed patients, stimulating both the innate and adaptive immune system.8,29,30
Monogenic autoinflammatory diseases – inborn anomalies of inflammation of genetic origin – are complicated with pericardial disease in nearly one-third of cases, but this involvement is rarely isolated and often begins in childhood. However, due to a low penetrance of mutations, they may develop into recurrent pericarditis in adulthood. In these diseases, a faulty inflammasome regulation leads to an overproduction of inflammatory cytokines (IL-1 and TNF-α). The monogenic autoinflammatory diseases most frequently involved in recurrent pericarditis are the Mediterranean fever family (caused by the mutation of the Mediterranean fever gene-encoding pyrin, mostly autosomal recessive transmission, and pericardial disease in 0.7%–1.4% of cases) and TNF receptor-associated periodic syndrome (TRAPS; caused by the mutation of the TNRFRSF1A gene encoding the 55-kD receptor for TNF-α, dominant autosomal transmission). A systematic search for these mutations in patients with IRAP did not find any familial Mediterranean fever mutation31 but did find a TRAPS mutation in 6% of cases32,33: family nature, resistance to colchicine for TRAPS, an early onset, and recurrence after 1 year are suggestive of such pathologies. However, these are rare pathologies, with only three cases of diagnosed familial Mediterranean fever reported in the literature at the time of an isolated recurrent pericarditis.34 The identification of these patients means that their treatment can be adapted specifically: anakinra, a recombinant IL-1 receptor antagonist, is very effective due to the increased secretion of IL-1, secondary to hyperactivity of the inflammasome. The concept of autoinflammatory disease has more recently extended to other multifactorial pathologies, such as Still’s disease or gout, similar in terms of the existence of inflammatory attacks that can affect specific organs and are recurrent, noninfectious, and without autoantibodies or T cells.
IRAP could be “classified” into this type of pathology, with the presence of IL-1 and IL-6 in the pericardial fluid. The presence of IL-8 in plasma could be a predictive factor of recurrence during acute pericarditis.35
There is a link between an innate and adaptive immune response and, therefore, a continuum between autoimmune and autoinflammatory diseases, which are found for example in inflammatory bowel disease. These complex conditions could be due to the assembly of several inflammasomes, secondary to both genetic and environmental factors.8–36 A genetic character is suggested by the existence of familial forms in 10% of cases.37 Systematic human leucocyte antigen (HLA) typing of 55 patients with recurrent pericarditis showed the existence of “predisposing” HLA alleles (HLA-A*02, - Cw*07, and -DQB1*0202), or “protective” HLA alleles (HLA-DRB1*04 and -DQB1*0302).35 Similarly, these patients have a lower rate of CD4+/CD45RA+ naïve T cells and a higher rate of CD8+DR+ activated T cells than patients who do not recur or controls.38
Treatment
Therapeutic methods
NSAIDs/aspirin
Aspirin (2–4 g/day in three intakes), indomethacin (75–150 mg/day in three intakes), and ibuprofen (1,600–3,200 mg/day in three intakes) are the most studied therapeutic methods. However, no study has compared the drugs with one another, and the choice is made individually based on tolerance, route of administration, and comorbidities.39 In the acute phase, intravenous administration may be beneficial. We usually use either aspirin IV orally or as the second-line, in the case of an incomplete improvement, IV ketoprofen (100 mg/three times a day) and then naproxen orally (550 mg/two times a day). Table 2 provides the pericarditis treatment plan that has been adopted in our hospital.
 | Table 2 Recurrent pericarditis treatment Abbreviation: NSAID, nonsteroidal anti-inflammatory drug. |
Colchicine
Colchicine’s action, although not yet completely understood, is based on its association with the tubulin protein, which by inhibiting the microtubule assembly process modifies cellular function, decreases the mobility of leukocytes and phagocytosis, and thus limits the inflammatory response.40,41 It is lipophilic by nature and is 16 times more concentrated in leukocytes than in plasma. Essential side effects are gastrointestinal: diarrhea, nausea, and vomiting. However, the following are more rarely observed: hematological toxicity, liver, muscle, or alopecia. Colchicine is metabolized by liver through the P450 cytochrome 3A4 isoenzyme. The combination with CYP3A4 product inhibitors (macrolides and ketoconazole) is therefore contraindicated. Large quantities of grapefruit juice can increase the concentration of colchicine. It is important that both the practitioner and the patient need to know all these data, because the prescription is usually prolonged, ≥3 months. The starting dose is 1 mg/twice a day for 1–2 days, then 0.5 mg/twice a day, reduced by half for patients <70 kg. The dose should be reduced by half after 70 years, and its use should be cautious or avoided in patients with hepatic or renal impairment. The colchicine for acute pericarditis study1 showed that the addition of colchicine to conventional treatment of acute pericarditis reduced the persistence of symptoms after 72 hours (11.7% vs 36.7%, P=0.003) as well as the risk of recurrence (10.7% vs 32.3%, P=0.004). After the first recurrent episode of pericarditis, the CORE study3 (randomized and open-labeled), then the CORP study42 (randomized and double-blind), applying the same doses of colchicine as conventional therapy, showed a decrease in recurrence of 50% to 24% (P=0.02 and P<0.001, respectively). This effect was confirmed in the investigation on colchicine for acute pericarditis study2 (randomized and double-blind), which combined colchicine or placebo with conventional treatment of acute pericarditis without a loading dose for 3 months. The primary endpoint combining constant or recurrent pericarditis with colchicine decreased by 37.5% to 16.7% (P<0.001). In multiple recurrent pericarditis (two recurrences or more), the randomized, double-blind CORP-2 study, with colchicine combined with NSAID treatment or aspirin for 6 months, reduced the risk of further recurrence by 42% to 21% (P=0.0009) compared with the placebo.6 The optimal treatment duration is unknown and may be 3, 6, or indeed 12 months.
Corticosteroids
Corticosteroids exhibit numerous side effects, in particular, an increase in recurrence and therefore corticosteroid dependency, especially since they are used in high doses. A retrospective study of 100 patients showed a recurrence rate that was two times higher (64.7% vs 32.6%, P=0.002), and severe adverse reaction rates that were ten times higher (23.5% vs 2%) in the case of using higher doses (1 mg/kg/day) compared with lower doses (0.2–0.5 mg/kg/day), independent of sex, autoimmune or idiopathic etiology, or age.4 However, this retrospective study does not take into account the “seriousness” evaluated by the physician during the patient’s care, often leading to the use of high intravenous doses. Nevertheless, it is currently preferable to use small quantities (0.2–0.5 mg/kg/day) and to wean very gradually, as indicated in the European Society of Cardiology guidelines5: if the dose is >50 mg/day, decrease 10 mg/day every 1–2 weeks; if the dose is between 25 and 50 mg/day, decrease 5–10 mg/day every 1–2 weeks; when the dose is between 15 and 25 mg/day, decrease by 2.5 mg/day every 2–4 weeks followed by a decrease of 1.25–2.5 mg per day every 2–6 weeks.5–43 We speak of corticosteroid dependency after two relapses during tapering. Because of the importance of the side effects of corticosteroids, a local, intrapericardial treatment was proposed. Maish et al44 report the same efficacy as oral corticosteroids but with reduced side effects from 29.6% to 13.3%. However, clinical data from this treatment are currently limited.
Immunosuppressors
Immunosuppressors are mainly suggested before colchicine (actually systematic), in corticosteroid-dependent IRAPs. Pericarditis is a functionally disabling disease but usually has a good prognosis; therefore, the risk–benefit ratio of these treatments, which often have many side effects, should be well assessed, and immunosuppressors should only be used as a last resort, after the new immunotherapy treatment.5 Marcolongo45 proposed a treatment regimen -involving the use of high-dose corticosteroids (1–1.5 mg/kg/day) for 4 weeks, followed by a tapering over 3 months with a bridge using aspirin, and in the case of recurrence, the use of azathioprine or cyclophosphamide is ultimately required only in three patients.45 Methotrexate was ineffective in preventing recurrence.17
Azathioprine
The largest series of patients with IRAP treated with azathioprine was reported by Vianello et al and concerned 46 corticosteroid-dependent patients.46 Azathioprine treatment at a dose of 1.5–2.5 mg/kg/day allowed weaning without recurrence in 63% of cases. It was ineffective in 15.2% of cases, which presented more than three recurrences upon decreasing corticosteroids. Treatment with azathioprine was finally stopped after an average of 14 months of treatment in 58.6% of patients.
Immunomodulators
Intravenous immunoglobulin
The use of intravenous immunoglobulin depends on its action in immune-mediated disease such as Kawasaki disease, the idiopathic thrombocytopenic purpura, or Guillain–Barre syndrome. Moretti et al47 reported their efficacy in eight out of nine patients resistant or intolerant to conventional NSAIDs, corticosteroids, and colchicine, at a dose of 500 mg/kg/day for 5 days, in combination with conventional treatment, and in one, two (two patients), or three (one patient) spaced treatment courses of 4 weeks. Del Fresno et al48 report the postoperative use in two children – at a high dose (2 g/kg), administered monthly, two to five times – which made it possible to control the disease. The mechanism of action of intravenous immunoglobulin is complex and is not yet fully understood: the Fc region of the immunoglobulins interacts with the Fc receptors of the phagocyte, lymphocytes, and the Fc-binding plasma proteins. They decrease phagocytosis, modulate the expression of Fc receptors, decrease the activation and deposition of complement, inhibit cytokine cascade, modulate activation and differentiation of T and B cells, and neutralize circulating autoantibodies. Although minimal in the Moretti series,45 side effects can be serious (ie, renal failure) and administration should be cautious.
Anakinra
Anakinra is an IL-1 receptor antagonist. IL-1 plays an important role in the inflammation cascade – whether sterile inflammation (IL-1α) or triggered by a microbiological agent or other chemokine (IL-1β). It is involved in many autoinflammatory (ie, TRAPS) or autoimmune (ie, rheumatoid arthritis) diseases.49 The use of anakinra follows its remarkable efficiency in autoinflammatory diseases, especially Still’s disease.50 It was first used in children, allowing weaning from corticosteroids whose side effects on growth inhibit their long-term use, and then it was used with the same efficacy in adults. Because of its immunosuppressive effect, anakinra should not be prescribed in the acute phase of infection, and the presence of tuberculosis should be investigated before prescribing. However, due to its short half-life, full recovery of normal immune function occurs within a few hours after the cessation of anakinra treatment. This pharmacokinetic profile restrains the incidence of damaging severe infections.
The side effects reported in different series are local reactions at the injection site, usually transient and not requiring discontinuation of treatment, and a usually moderate and transient elevation of transaminases, which may however rarely require discontinuation of treatment. Its first use was reported by Picco et al51 in three corticosteroid-dependent children with IRAP. The authors describe a rapid efficacy, comparable to that of high-dose corticosteroids, the possibility of weaning corticosteroids, but a recurrence during weaning of anakinra, quickly controlled by its reintroduction.
Finetti et al52 reported the efficacy of anakinra (1–2 mg/kg/day) in 15 corticosteroid-resistant or colchicine-resistant patients (twelve children and three adults). All the patients had a rapid response to anakinra and could be quickly weaned from colchicine and corticosteroids in 2 months. NSAIDs were gradually weaned. Anakinra was left as single therapy daily for a median duration of 12 months, which was then gradually decreased. Six patients recurred during treatment reduction and were controlled by reintroducing treatment at the initial dose. Seven patients were weaned at an average of 25.1 months. Two of them recurred, after 1 week and 1 month, respectively, and were controlled by reintroducing the treatment. Five patients showed a transient local reaction at the puncture site.52 Jain et al53 reported the use of anakinra (100 mg/day) in 13 adult patients with recurrent pericarditis taking NSAIDs, colchicines, and corticosteroids. Anakinra was used because of the persistence of symptoms on corticosteroids or because tapering was impossible. Treatment was effective in all cases, with a complete response in twelve of 13 cases. Side effects were minimal: a transient local reaction at the puncture site. After a follow-up of 23±6 months, eleven patients remained on anakinra, and five (38%) of them recommenced after weaning failure. Only two patients were weaned.53 Lazaros et al7 reported the use of anakinra in ten adults at a dose of 100 mg/day for 6 months and then 100 mg every other day for 6 months. Colchicine and corticosteroids were stopped progressively after the introduction of anakinra. This small study supports the rapid efficacy of anakinra on symptoms (48 hours) and inflammation (CRP normalization in 5.9 days) but shows a recurrence rate of 70% upon dose reduction, reacting well to the resumption of initial doses.7 We reported the use of this treatment to replace corticosteroids as second-line treatment, in a diabetic patient and in a patient with stable rheumatoid polyarthritis.54
The randomized study against placebo reported at the last American Congress of Rheumatology undoubtedly confirms the efficacy of anakinra55: 21 patients with IRAP on corticosteroids were treated with anakinra (eleven) or placebo (ten) in combination with their treatment for 6 months. After the disappearance of pain and normalization of CRP, they were weaned from all other treatment. Flare-ups of pericarditis occurred in all ten patients randomized to placebo and none of the eleven patients were randomized to anakinra during the double-blind treatment (P<0.0001). Two serious adverse events were reported, both in the anakinra-treated patients (P=0.47): one skin herpes zoster and one ischemic optic neuropathy in the fifth month of the double-blind period, but the exact mechanism of the optic neuropathy is debatable.
Anti-TNF
Nieto Gonzalez et al56 have successfully treated three children with IRAP using anti-TNF-α. The efficacy of anti-TNF was also reported in adults.57,58 However, anti-TNF agents may also be responsible for pericarditis.59–62
Statins
Because of their immunomodulatory effects, the statins were evaluated in a randomized study: combined with indomethacin, they have not shown greater efficacy compared with the placebo.63
Pericardiectomy
Pericardiectomy was proposed as a last resort in patients with multiple relapses despite treatment: its effect was positive in a retrospective study of 184 patients (58 operated and 126 medically treated), but not found in another series (only two out of nine patients improved).64,65
Indications
Treatment should be tailored specifically to the patient, taking into account the patient’s history, risk factors, history of pericarditis, and response to different treatments used. The duration of treatment must also be adapted to the clinical and biological responses, as well as the withdrawal, by steps of 1–2 weeks, molecule by molecule, only in the absence of recurrent pain and while controlling the negativity of CRP. The course of treatment is often long, lasting from several weeks to several months.10
First-line therapy5: 1) resumption of aspirin or NSAIDs in combination with colchicine, which speeds up the response to treatment and reduces the rate of recurrence2,3,6,42 and 2) depending on the response to treatment, a change in molecule or IV administration may be proposed.
Second-line therapy: it is usually based on corticosteroids; in the case of failure of aspirin and NSAIDs, or contraindication to their prescription. However, in patients at high risk of complications on corticosteroids (children, diabetes, etc), the use of anakinra at this stage can be discussed.
Third-line therapy: traditionally, immunosuppressive drugs were recommended as third-line treatment after failure of corticosteroids. Azathioprine was the most used, its efficacy having been shown in small series, and having an acceptable tolerance.46 Currently, immunosuppressive drugs are usually replaced by an immunomodulator, in particular anakinra.
Fourth-line therapy: only in the case of failure of these therapies, we can propose a pericardiectomy.
General measures5: exercise restriction should be recommended until symptoms and inflammation resolve and for a period of 3 months in athletes. Influenza vaccination during the treatment of recurrent pericarditis is not recommended, as it can induce recurrences by stimulating the immune system.17
Monitoring of treatment – additional examinations
CRP
CRP increases from the sixth hour, with a peak at 48 hours from the onset of pain. A study of 200 patients with pericarditis found a normal CRP in 22% of patients at presentation, in 60% after 1 week of treatment, in 85% after 2 weeks, and in 100% of patients after 4 weeks. In this series, the loading dose of NSAIDs/aspirin was continued until normalization of the CRP. An incomplete clinical response after 1 week, corticosteroid treatment, and a high CRP after 1 week were independent risk factors of recurrence.66
Echocardiography
This is the first-line imaging examination of the pericardium.5,67,68 It investigates the existence of an effusion, a pericardial hyperechogenicity or thickening, signs of constrictive change, and a cause (eg, infarction and tumor). It describes the “inflammatory” nature of pericardial effusion: the presence of fibrinous strands. It can also describe the signs of “transient” constriction.5,69
Cross-sectional imaging
An MRI or CT can show an enhancement of the pericardium, inflammatory changes of the pericardial fat and pericardium, and the presence of blood in the pericardial cavity.67–70 Positron emission tomography scans and CT are mainly useful in eliminating a malignant pathology. However, MRI is the imaging technique of choice: it can eliminate the recurrence of pericarditis during atypical pain, where there is no thickening or inflammation of the pericardium. It also helps to guide treatment, late pericardial enhancement after an injection of gadolinium being a marker of disease activity. A recent retrospective study shows the importance of this treatment-guiding mode.70
Biopsy and pericardial drainage
These techniques are carried out therapeutically in the case of abundant effusion or tamponade. However, they are only indicated for diagnostic purposes if bacterial pericarditis, tuberculosis in nonendemic countries (if the investigation of noninvasive Mycobacterium tuberculosis is negative), or neoplastic disease is suspected.5,20
Evolution
A review of eight series involving a total of 230 patients with IRAP, followed up for an average of 61 months, found a tamponade rate of 3.5% and no progression toward constriction.4 This is not true for “secondary” pericarditis. In a series of 500 patients with acute pericarditis, Imazio et al71 reported 57% recurrence, 20.2% tamponade, and 8.3% progression toward constriction where there was a specific cause versus 25%, 1.2%, and 0.48%, respectively, for idiopathic or postviral pericarditis.71
Conclusion
Recurrent pericarditis is a difficult disease to treat, and is stressful for the patient. An etiological examination should be performed at the beginning of the treatment to eliminate the potentially serious causes requiring specific treatment. They are most often “idiopathic”, with a still incompletely understood pathophysiology, involving autoimmunity and autoinflammation of various degrees, and usually set off by microbacteriological or postinjury triggers. Multidisciplinary discussion is needed to provide individualized treatment to each patient. Treatment will generally be long and should be guided by the clinic, but also by the dosage of the CRP, and possibly by the appearance of the pericardium in MRI. These examinations are needed not only to assert control over the disease and the possibility of weaning the treatment but also to eliminate the diagnosis of recurrence in cases of atypical pain. Treatment of the patient includes reassurance: the disease as well as the length of the treatment should be explained, and that the possibility of recurrence, which does not worsen the prognosis, is usually good. The place of immunomodulators, and in particular anakinra, should be discussed again. Indeed, these treatments are currently used primarily in steroid-dependent patients and often lead to transforming a corticosteroid dependence to dependence on immunomodulators.72 Their remarkable efficacy could see them being used in second-line treatment in place of corticosteroids, at least in some patients, after the failure of standard therapy (treatment by aspirin/NSAIDs and colchicine, prolonged and at high doses). This will perhaps facilitate weaning. In the same way, use of these new treatments could, without doubt, replace the usual therapeutic escalation that leads to multiple therapeutic associations, which is not without risks with the most refractory forms of the disease.
Disclosure
The authors report no conflicts of interest in this work.
References
Imazio M, Bobbio M, Cecchi E, et al. Colchicine in addition to conventional therapy for acute pericarditis: results of the Colchicine for acute Pericarditis (COPE) trial. Circulation. 2005;112(13):2012–2016. | ||
Imazio M, Brucato A, Cemin R, et al. A randomized trial of colchicine for acute pericarditis. N Engl J Med. 2013;369(16):1522–1528. | ||
Imazio M, Bobbio M, Cecchi E, et al. Colchicine as first-choice therapy for recurrent pericarditis: results of the CORE (COlchicine for REcurrent pericarditis) trial. Arch Intern Med. 2005;165(17):1987–1991. | ||
Imazio M, Brucato A, Adler Y, et al. Prognosis of idiopathic recurrent pericarditis as determined from previously published reports. Am J Cardiol. 2007;100(6):1026–1028. | ||
Adler Y, Charron P, Imazio M, et al. 2015 ESC guidelines for the diagnosis and management of pericardial diseases: The task force for the diagnosis and management of pericardial diseases of the European Society of Cardiology (ESC) endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2015;36(42):2921–2964. | ||
ImazioM, Belli R, Brucato A, et al. Efficacy and safety of colchicine for treatment of multiple recurrences of pericarditis (CORP-2): a multicentre, double-blind, placebo-controlled, randomised trial. Lancet. 2014;383(9936):12232–12237. | ||
Lazaros G, Vasileiou P, Koutsianas C, et al. Anakinra for the management of resistant idiopathic recurrent pericarditis. Initial experience in 10 adult cases. Ann Rheum Dis. 2014;73(12):2215–2217. | ||
Cantarini L, Lopalco G, Selmi C, et al. Autoimmunity and autoinflammation as the yin and yang of idiopathic recurrent acute pericarditis. Autoimmun Rev. 2015;14(2):90–97. | ||
Imazio M, Demichelis B, Parrini I, et al. Recurrent pain without objective evidence of disease in patients with previous idiopathic or viral acute pericarditis. Am J Cardiol. 2004;94(7):973–975. | ||
Imazio M, Gaita F, LeWinter M. Evaluation and treatment of pericarditis: a systematic review. JAMA. 2015;314(14):1498–1506. | ||
Imazio M, Demichelis B, Parrini I, et al. Management, risk factors and outcomes in recurrent pericarditis. Am J Cardiol. 2005;96(5):736–739. | ||
Géri G, Cacoub P. Péricardites aigües récidivantes: mise au point et actualités 2011 [What’s new in recurrent pericarditis in 2011]. Rev Med Int. 2011;32(12):736–741. | ||
Gouriet F, Levy PY, Casalta JP, et al. Etiology of pericarditis in a prospective cohort of 1162 cases. Am J Med. 2015;128(7):784.e1–784.e8. | ||
Flower NO, Harbin AD 3rd. Recurrent acute pericarditis: follow-up study of 31 patients. J Am Coll Cardiol. 1986;7(2):300–305. | ||
Artom G, Koren-Morag N, Spodick DH, et al. Pretreatment with corticosteroids attenuates the efficacy of colchicine in preventing recurrent pericarditis: a multi-centre all-case analysis. Eur Heart J. 2005;26(7):723–727. | ||
Brucato A, Brambilla G, Moreo A, et al. Long term outcomes in difficult-to-treat patients with recurrent pericarditis. Am J Cardiol. 2006;98(2):267–271. | ||
Raatikka M, Pelkonen PM, Karjalainen J, Jokinen EV. Recurrent pericarditis in children and adolescents: reports of 15 cases. J Am Coll Cardiol. 2003;42(4):759–764. | ||
Pankuweit S, Stein A, Karatolios K, Richter A, Ruppert V, Maisch B. Viral genomes in the pericardial fluid and in peri- and epicardial biopsies from a German cohort of patients with large to moderate pericardial effusions. Heart Fail Rev. 2013;18(3):329–336. | ||
Maisch B, Rupp H, Ristic A, Pankuweit S. Pericardioscopy and epi- and pericardial biopsy – a new window to the heart improving etiological diagnoses and permitting targeted intrapericardial therapy. Heart Fail Rev. 2013;18(3):317–328. | ||
Smets P, Guettrot-Imbert G, Hermet M, et al. Péricardite récidivante: traquer le mésotheliome péricardique primitif [Recurrent pericarditis related to primary pericardial malignant mesothelioma]. Rev Med Int. 2013;34(9):573–576. | ||
Imazio M. Pericardial involvement in systemic inflammatory diseases. Heart. 2011;97(22):1882–1892. | ||
Imazio M, Hoit BD. Post-cardiac injury syndromes. An emerging cause of pericardial diseases. Int J Cardiol. 2013;168(2):648–652. | ||
Imazio M, Trinchero R, Brucato A, et al. Colchicine for the prevention of post-pericadiotomy syndrome (COPPS): a multicenter, randomized, double-blind placebo-controlled trial. Eur Heart J. 2010;31(22):2749–2754. | ||
Maisch B, Seferonic PM, Ristic AD, et al. Guidelines on the diagnosis and management of pericardial disease. Eur Heart J. 2004;25(7):587–610. | ||
Maestroni S1, Di Corato PR, Cumetti D, et al. Recurrent pericarditis: autoimmune or autoinflammatory? Autoimmun Rev. 2012;12(1):60–65. | ||
Brucato A, Maestroni S, Cumetti D, et al. Recurrent pericarditis: infectious or autoimmune? Autoimmun Rev. 2008;8(1):44–47. | ||
Caforio AL, Brucato A, Doria A, et al. Anti-heart and anti-intercalated disk autoantibodies: evidence for autoimmunity in idiopathic recurrent acute pericarditis. Heart. 2010;96(10):779–784. | ||
Pankuweit S, Wädlich A, Meyer E, Portig I, Hufnagel G, Maisch B. Cytokine activation in pericardial fluids in different forms of pericarditis. Herz. 2000;25(8):748–754. | ||
Bogdanos DP, Smyk DS, Invernizzi P, et al. Infectome: a platform to trace infectious triggers of autoimmunity. Autoimmun Rev. 2013;12(7):726–740. | ||
Selmi C, Leung PS, Sherr DH, et al. Mechanisms of environmental influence on human autoimmunity: a National Institute Environmental Health Sciences expert panel workshop. J Autoimmun. 2012;39(4):272–284. | ||
Brucato A, Shinar Y, Brambilla G, et al. Idiopathic recurrent acute pericarditis: familial Mediterranean fever mutations and disease evolution in a large cohort of Caucasian patients. Lupus. 2005;14(9):670–674. | ||
Cantarini L, Lucherini OM, Cimaz R, et al. Idiopathic recurrent pericarditis refractory to colchicine treatment can reveal tumor necrosis factor receptor-associated periodic syndrome. Int J Immunopathol Pharmacol. 2009;22(4):1051–1058. | ||
Cantarini L, Lucherini OM, Brucato A, et al. Clues to detect tumor necrosis factor receptor-associated periodic syndrome (TRAPS) among patients with idiopathic recurrent acute pericarditis: results of a multicentre study. Clin Res Cardiol. 2012;101(7):525–531. | ||
Yoshioka K, Furumitsu Y, SanonT, Miyamoto T, Agematsu K. Acute pericarditis as the first manifestation of familial Mediterranean fever: a possible relationship with idiopathic recurrent pericarditis. Int Med. 2014;53(15):1659–1663. | ||
Vasileiou P, Tsioufis C, Lazaros G, et al. Interleukin-8 as a predictor of acute idiopathic pericarditis recurrences. A pilot study. Int J Cardiol. 2014;172(3):e463–e464. | ||
Hedrich CM, Tsokos GC. Bridging the gap between autoinflammation and autoimmunity. Clin Immunol. 2013;147(3):151–154. | ||
Brucato A, Brambilla G. Recurrent idiopathic pericarditis familial occurrence. Int J Cardiol. 2005;102(3):529. | ||
Lazaros G, Karavidas A, Spyropoulou M, et al. The role of the immunogenetic background in the development and recurrence of acute idiopathic pericarditis. Cardiology. 2011;118(1):55–62. | ||
Schwier NC, Coons JC, Rao KS. Pharmacotherapy update of acute idiopathic pericarditis. Pharmacotherapy. 2015;35(1):99–111. | ||
Alabed S, Cabello JB, Irving GJ, Qintar M, Burls A. Colchicine for pericarditis. Cochrane Database Syst Rev. 2014;8:CD010652. | ||
Verma S, Eikelboom JW, Nidorf SM, et al. Colchicine in cardiac disease: a systematic review and meta-analysis of randomized controlled trials. BMC Cardiovasc Disord. 2015;15:96. | ||
Imazio M, Brucato A, Cemin R, et al. Colchicine for recurrent pericarditis (CORP): a randomised trial. Ann Intern Med. 2011;155(7):409–414. | ||
Imazio A, Brucato A, Cumetti D et al. Corticosteroids for recurrent pericarditis: high versus low doses: a nonrandomized observation. Circulation. 2008;118(6):667–671. | ||
Maish B, Ristic AD, Pankuweit S. Intrapericardial treatment of autoreactive pericardial effusion with triamcinolone: the way to avoid side effects of systemic corticosteroid therapy. Eur Heart J. 2002;23(19):1503–1508. | ||
Marcolongo R, Russo R, Laveder F, Noventa F, Agostini C. Immunosuppressive therapy prevents recurrent pericarditis. JACC. 1995;5(1):1276–1279. | ||
Vianello F, Cinetto F, Cavraro M, et al. Azathioprine in isolated recurrent pericarditis: a single centre experience. Int J Cardiol. 2011;147(3):477–478. | ||
Moretti M, Buiatti A, Merlo M, et al. Usefulness of high-dose intravenous human immunoglobulins treatment for refractory recurrent pericarditis. Am J Cardiol. 2013;112(9):1493–1498. | ||
Del Fresno MR, Peralta JE, Granados MA, Enriquez E, Pinilla ND, De Inocencio J. Intravenous immunoglobulin therapy for refractory recurrent pericarditis. Pediatrics. 2014;134(5):e1441–e1446. | ||
Baskar S, Klein AL, Zeft A. The use of IL-1 receptor antagonist (anakinra) in idiopathic recurrent pericarditis: a narrative review. Cardiol Res Pract. 2016;2016:7840724. | ||
Merlin E, Berthomieu L, Dauphin C, Stephan JL. Cardiac tamponade in a child with systemic onset juvenile idiopathic arthritis: dramatic improvement after interleukin-1 blockade by anakinra. Pediatr Cardiol. 2011;32(6):862–863. | ||
Picco P, Briscan G, Traverso F, Loy A, Gattorno M, Martini A. Successful treatment of idiopathic recurrent pericarditis in children with interleukin-1beta receptor antagonist (anakinra): an unrecognized autoinflammatory disease? Arthritis Rheum. 2009;60(1):264–268. | ||
Finetti M, Insalaco A, Cantarini L, et al. Long-term efficacy of interleukin-1 receptor antagonist (anakinra), in corticosteroid-dependent and colchicine-resistant recurrent pericarditis. J Pediatr. 2014;164(6):1425–1431. | ||
Jain S, Thongprayoon C, Espinosa RE, et al. Effectiveness and safety of anakinra for management of refractory pericarditis. Am J Cardiol. 2015;116(8):1277–1279. | ||
Massardier C, Dauphin C, Eschalier R, Lusson JR, Soubrier M. Resistant or recurrent acute pericarditis: a new therapeutic opportunity? Int J Cardiol. 2014;177(2):e75–e77. | ||
Brucato A, Imazio M, Maestroni S, et al. Anakinra in patients with cortico-dependent idiopathic recurrent pericarditis: A randomised double-blind placebo-controlled withdrawal trial [abstract]. Arthritis Rheumatol. 2015;67(suppl 10). Available from: http://acrabstracts.org/abstract/anakinra-in-patients-with-cortico-dependent-idiopathic-recurrent-pericarditis-a-randomised-double-blind-placebo-controlled-withdrawal-trial/. Accessed June 19, 2016. | ||
Nieto Gonzalez JC, Monteagudo Saez I, Lopez-Longo FJ, Serrano B, Mata Martinez C, Carreno Perez L. Idiopathic recurrent pericarditis treated successfully with tumour necrosis factor alpha blocking agents (anti-TNF-α). Clin Exp Rheumatol. 2013;31(5):776–778. | ||
Aslangul E, Perrot S, Durand E, Mousseaux E, Le Jeune C, Capron L. Successful etanercept treatment of constrictive pericarditis complicating rheumatoid arthritis. Rheumatology (Oxford). 2005;44(12):1581–1583. | ||
Esposito M, Giunta A, Babino G, Schipani C, Marchei M, Chimenti MS. Resolution of idiopathic recurrent pericarditis in a psoriatic arthritis patient treated with etanercept. Eur J Dermatol. 2012;22(1):151–152. | ||
Ozkan H, Cetinkaya AS, Yildiz T, Bozat T. A rare side effect due to TNF-alpha blocking agent: acute pleuropericarditis with adalimumab. Case Rep Rheumatol. 2013;2013(4):985914. | ||
Soh MC, Hart HH, Corkill M. Pericardial effusions with tamponade and visceral constriction in patients with rheumatoid arthritis on tumour necrosis factor (TNF)-inhibitor therapy. Int J Rheum Dis. 2009;12(1):74–77. | ||
Devasahayam J, Pillai U, Lacasse A. A rare case of pericarditis, complication of infliximab treatment for Crohn’s disease. J Crohns Colitis. 2012;6(6):730–731. | ||
Burke JP, Kelleher B, Ramadan S, Quinlan M, Sugrue D, O’Donovan MA. Pericarditis as a complication of infliximab therapy in Crohn’s disease. Inflamm Bowel Dis. 2008;14(3):428–429. | ||
Di Pasquale P, Cannizzaro S, Fasullo S, et al. Combination of indomethacin and statin compared with indomethacin and placebo in patients with a first episode of acute pericarditis: preliminary findings. Clin Sci (Lond). 2007;113(11):443–448. | ||
Khandaker MH, Schaff HV, Greason KL, et al. Pericardiectomy vs medical management in patients with relapsing pericarditis. Mayo Clinic Proc. 2012;87(11):1062–1070. | ||
Fowler NO, Harbin AD. Recurrent acute pericarditis. J Am Coll Cardiol. 1986;7(2):300–305. | ||
Imazio M, Brucato A, Maestroni S, et al. Prevalence of C-reactive protein elevation and time course of normalization in acute pericarditis: implications for the diagnosis, therapy, and prognosis of pericarditis. Circulation. 2011;123(10):1092–1097. | ||
Klein AL, Abbara S, Agler DA, et al. American Society of Echocardiography clinical recommendations for multimodality cardiovascular imaging of patients with pericardial disease: endorsed by the Society for Cardiovascular Magnetic Resonance and Society of Cardiovascular Computed Tomography. J Am Soc Echocardiogr. 2013;26(9):965–1012.e15. | ||
Cosyns B, Plein S, Nihoyanopoulos P, et al. European association of cardiovascular imaging (EACVI) position paper: multimodality imaging in pericardial disease. Eur Heart J Cardiovasc Imaging. 2015;16(1):12–31. | ||
Gentry J, Klein AL, Jellis CL. Transient constrictive pericarditis: current diagnosis and therapeutic strategies. Curr Cardiol Rep. 2016;18(5):41. | ||
Alraies MC, AlJaroudi WA, Yarmohammadi H, et al. Usefulness of cardiac magnetic resonance-guided management in patients with recurrent pericarditis. Am J Cardiol. 2015;115(4):542–547. | ||
Imazio M, Brucato A, Maestroni S, et al. Risk of constrictive pericarditis after acute pericarditis. Circulation. 2011;124(11):1270–1275. | ||
Lotan D, Wasserstrum Y, Fardman A, Kogan M, Adler Y. Usefulness of novel immunotherapeutic strategies for idiopathic recurrent pericarditis. Am J Cardiol. 2016;117(5):861–866. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.