Back to Journals » International Medical Case Reports Journal » Volume 19
Recurrent Pediatric Upper Tracheal Stenosis Stabilized with a Montgomery Airway Stent: A Case Report
Authors Aldakak MA ![]() , Al Jabban Y, Saleh A, Aldalati A, Darwish B
, Al Jabban Y, Saleh A, Aldalati A, Darwish B
Received 6 February 2026
Accepted for publication 14 May 2026
Published 20 May 2026 Volume 2026:19 601744
DOI https://doi.org/10.2147/IMCRJ.S601744
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Thomas E Hutson
Mohammad Alaa Aldakak,1 Yousef Al Jabban,2 Ahmed Saleh,2 Ahmad Aldalati,2 Bassam Darwish2
1Faculty of Medicine, Damascus University, Damascus, Syrian Arab Republic; 2Department of Thoracic Surgery, Al-Mouwasat University Hospital, Faculty of Medicine, Damascus University, Damascus, Syrian Arab Republic
Correspondence: Mohammad Alaa Aldakak, Email [email protected]
Background: Pediatric post-intubation upper tracheal stenosis is uncommon but clinically important. High cervical lesions near the vocal cords are especially challenging because of recurrence risk and poor tolerance of airway stents.
Case Presentation: A 10-year-old boy developed progressive dyspnea and inspiratory stridor over four months after a motor vehicle accident requiring endotracheal intubation for seven days. On presentation, respiratory rate was 26 breaths/min, oxygen saturation was 92– 93% on room air, and stridor was present at rest. Rigid bronchoscopy demonstrated a 2-cm Myer–Cotton grade II upper tracheal stenosis approximately 2 cm below the vocal cords. Endoscopic dilation provided only transient improvement, with recurrence within three weeks. He underwent cervical tracheal resection with end-to-end anastomosis. Early postoperative restenosis developed, with bronchoscopic granulation-like tissue and exposed anastomotic sutures requiring repeat dilation, debridement, and suture removal. A silicone stent placed immediately below the vocal cords was poorly tolerated, causing severe stridor and laryngeal edema requiring emergency tracheostomy and later stent removal. A Montgomery airway stent was subsequently placed. Respiratory rate improved to 16 breaths/min, oxygen saturation increased to 96%, and stridor resolved. At two-week follow-up, he was breathing comfortably without a tracheostomy cannula.
Conclusion: Montgomery airway stenting may provide effective short-term stabilization for recurrent high cervical pediatric tracheal stenosis complicated by anastomotic granulation, suture exposure, and silicone stent intolerance.
Keywords: post-intubation tracheal stenosis, pediatric airway obstruction, tracheal resection and anastomosis, montgomery T-tube / airway stent, case report
Introduction
Pediatric laryngotracheal stenosis (LTS) leads to impaired airflow, mucociliary clearance, phonation, and sometimes swallowing, and it therefore requires careful preoperative assessment and classification supported by clinical history, endoscopy, and radiological evaluation.1 Among children with acquired LTS, post-intubation injury accounts for the majority of cases (reported as 90%), while less frequent causes include iatrogenic endoscopic injury, benign tumors, caustic or thermal injury, external blunt trauma, chronic inflammatory disorders, and idiopathic disease.1 During endotracheal intubation, maintaining tracheal mucosal capillary pressure around 20–40 mmHg is highlighted, because excessive cuff pressures may cause ischemic necrosis and ulceration that heal with fibrous stenosis.2 Clinically, the delayed presentation with progressive wheezing and respiratory difficulty can lead to misdiagnosis as asthma.3 Severity description commonly incorporates the Myer–Cotton grading system (grade I: 0–50% lumen reduction; grade II: 51–70%; grade III: 71–99%; grade IV: no detectable lumen).1 To standardize evaluation and reporting, the European Laryngological Society describes a five-step endoscopic airway assessment designed to define stenosis type, involved subsites, extension, laryngeal motility, and airway lumen, while integrating relevant comorbidities.1 Radiologic assessment complements endoscopy, and radiological investigation is described as mandatory for Cotton–Meyer grade III–IV stenosis unless immediate tracheotomy is required, with ultrafast CT acquisition noted as a means to obtain good-quality imaging without sedation.1 The therapeutic armamentarium includes endoscopic dilation, laser or electro-knife techniques, stent placement, cryotherapy, intralesional steroid injection, and mitomycin application, alongside open procedures such as surgical resection, tracheoplasty, and tracheostomy.4 Treatment selection is reported to depend on available resources and expertise, patient condition, and stenosis severity and length, and resection with anastomosis is described as the gold-standard treatment.4
As an endoscopic adjunct, dilation with topical mitomycin C achieved ≥12-month symptom-free intervals in 14/22 patients, including 6/8 treated for postoperative anastomotic restenosis.5 Here, we present a case of recurrent upper tracheal stenosis in a child after prolonged endotracheal intubation, complicated by postoperative granulation and intolerance to silicone stenting, ultimately managed with a Montgomery airway stent.
Case Presentation
A 10-year-old male child presented with progressive dyspnea and inspiratory stridor that had been worsening over approximately four months. The symptoms developed after a prior motor vehicle accident that required endotracheal intubation for seven days (Figure 1). On presentation, he had stridor at rest, respiratory rate of 26 breaths/min, and oxygen saturation of 92–93% on room air, requiring supplemental oxygen. Chest examination was otherwise unremarkable.
 |
Figure 1 Anteroposterior chest radiograph obtained on admission after prior endotracheal intubation, used as part of the initial airway assessment. No chest CT was performed because urgent management was guided by rigid bronchoscopy. |
Rigid bronchoscopy using a 4.5 rigid scope demonstrated an upper tracheal stenosis (Myer–Cotton grade II) located approximately 2 cm below the vocal cords and extending for approximately 2 cm (Figure 2). Chest CT was not performed because the child required urgent airway assessment and management, and rigid bronchoscopy provided direct visualization of the stenosis, including its location, length, and severity. Endoscopic dilation was performed up to size 6 with transient improvement. Approximately three weeks later, symptoms recurred; repeat rigid bronchoscopy confirmed the same stenotic segment, and an attempt at stent placement was unsuccessful.
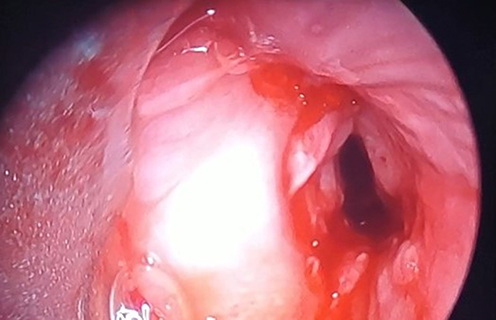 |
Figure 2 Rigid bronchoscopy view demonstrating an upper tracheal stenosis (Myer–Cotton grade II) approximately 2 cm below the vocal cords, showing a narrowed tracheal lumen consistent with post-intubation cicatricial stenosis. |
The patient subsequently underwent cervical tracheal resection via a Kocher neck incision. The mature fibrotic stenotic segment, measuring approximately 2 cm, was excised, followed by end-to-end anastomosis using interrupted 3–0 Vicryl round-body sutures with extraluminal knots. Postoperative neck flexion was maintained using chin-to-chest approximation sutures to reduce anastomotic tension.
Roughly two weeks after surgery, recurrent airway symptoms prompted repeat rigid bronchoscopy, which revealed reddish, friable proliferative tissue at the anastomotic site, interpreted bronchoscopically as granulation tissue; histopathologic confirmation was not obtained. Dilation was performed up to size 5. Two days later, bronchoscopy showed exposed anastomotic sutures with persistent granulation-like tissue; the sutures were removed, the tissue was debrided, and the airway was dilated again to size 5.
A 3-cm silicone stent was then placed immediately below the vocal cords to bypass the stenotic segment, and adjunct therapy with intravenous and inhaled corticosteroids plus nebulized epinephrine was administered. Despite this, the patient developed severe respiratory distress and stridor the following day, necessitating emergency tracheostomy with the cannula positioned below the stent. Silicone stent intolerance was attributed mainly to secretion retention and its very proximal position near the vocal cords. Several days later, repeat rigid bronchoscopy demonstrated laryngeal edema with the silicone stent in situ; the stent was removed during bronchoscopy because of intolerance and insufficient clinical efficacy, and subglottic granulation-like tissue was excised again. Corticosteroid therapy had not produced sufficient clinical improvement.
A Montgomery airway stent was subsequently placed. After Montgomery stent placement, respiratory rate improved to 16 breaths/min, oxygen saturation increased to 96%, and stridor resolved. At two-week follow-up, the patient remained on the Montgomery stent, was breathing comfortably without a tracheostomy cannula, and had no stridor or obstructive respiratory symptoms. Follow-up was limited to two weeks because the patient subsequently returned to his home region in another governorate far from the treating hospital.
Discussion
Post-intubation tracheal stenosis (PITS) is a clinically important late complication of airway instrumentation and should be considered in any child who develops progressive obstructive respiratory symptoms following endotracheal intubation.1,4 The pathophysiology is closely related to mechanical mucosal injury and pressure-related ischemia; maintaining tracheal mucosal capillary perfusion pressure around 20–40 mmHg is emphasized, as exceeding cuff pressures can lead to ischemic necrosis and ulceration followed by fibrotic healing and fixed stenosis.2 In addition, pediatric reports highlight contributory factors such as tube size relative to the child’s airway, repetitive tube motion, and repeated intubations or extubation failures, supporting a structured review of potentially modifiable iatrogenic risks when counseling families and anticipating recurrence.3
Symptoms typically evolve gradually and may present within 1–6 weeks after extubation, but clinical trajectories are variable, and diagnostic delay is common due to overlap with prevalent pediatric conditions.4 Misclassification as asthma is a well-described pitfall; a 10-year-old boy with tracheal stenosis was repeatedly treated as asthma, reflecting how wheeze and exertional dyspnea can obscure a fixed central airway obstruction.3 Importantly, by the time symptoms become prominent, the stenosis may already involve 30–50% of the lumen, underscoring the need for early definitive airway assessment when stridor or refractory symptoms persist.3 Our patient’s progressive dyspnea and inspiratory stridor evolving over several months after a motor vehicle accident with a 7-day intubation history fit this delayed-presenting spectrum and reinforced the need for timely endoscopic evaluation.4
Contemporary diagnostic frameworks emphasize stepwise assessment integrating detailed clinical history with endoscopic examination to define lesion location, length, involved subsites, and whether the stenosis is incipient (edema/ulceration/granulation) versus mature cicatricial disease because staging directly informs endoscopic versus open surgical decision-making.1 In addition to endoscopy, combined bronchoscopy and CT are described as key to characterizing stenosis severity, segment length, and precise location.4 In our case, chest CT was not performed because the child required urgent airway assessment and management, and rigid bronchoscopy provided direct visualization of the stenosis, including its location, length, and severity. Rigid bronchoscopy identified an upper tracheal stenosis approximately 2 cm below the vocal cords, extending for approximately 2 cm and classified as Myer–Cotton grade II, a high cervical location that can be technically challenging and prone to restenosis.1,4
Management options for nonmalignant tracheal stenosis include bronchoscopic dilation and other endoscopic modalities, such as incision techniques, stenting, intralesional steroids, and topical mitomycin, as well as open procedures such as segmental resection with end-to-end anastomosis and tracheostomy, with selection influenced by lesion complexity and institutional expertise.4,6 Endoscopic balloon dilation is commonly used as a minimally invasive strategy in pediatric subglottic/tracheal stenosis and has been associated with favorable clinical outcomes and long-term quality-of-life measures in pediatric series.7 However, restenosis during wound healing remains a central limitation of dilation-based approaches, and endoscopic therapy is frequently positioned as definitive treatment only in selected cases or as a bridge to surgery when recurrence occurs.5 Our patient experienced transient improvement after dilation followed by recurrence within weeks, mirroring reports in which repeat dilations may be required; for example, early bronchoscopic balloon dilation successfully treated multilevel post-traumatic stenosis in a child but still required re-intervention for mild restenosis during follow-up.8
When endoscopic control is insufficient or disease is recurrent and functionally significant, surgical approaches including tracheal resection and reconstruction are widely described as definitive options in appropriate candidates.4,9 In our patient, despite grade II classification, open resection was selected because the lesion was mature and fibrotic, approximately 2 cm long, highly symptomatic, located in the high cervical trachea, and recurred shortly after dilation. Cervical tracheal resection with end-to-end anastomosis was performed using interrupted 3–0 Vicryl round-body sutures with extraluminal knots, and postoperative neck flexion was maintained with chin-to-chest approximation sutures to reduce anastomotic tension. Early postoperative recurrence was driven by bronchoscopically identified granulation-like tissue at the anastomosis and exposed sutures, requiring repeat bronchoscopies with dilation, debridement, and suture removal. Histopathologic confirmation was not obtained; therefore, the term granulation tissue was used based on its bronchoscopic appearance as reddish, friable, proliferative tissue at the anastomotic site. This trajectory aligns with broader experience that postoperative restenosis may occur and often necessitates structured endoscopic surveillance and targeted management.1,5 In this setting, topical mitomycin C has been investigated as an adjunct to reduce restenosis; in a prospective cohort, 6/8 (75%) of postoperative anastomotic stenosis cases responded to dilation plus topical mitomycin, supporting its role as a potential option if cicatricial restenosis recurs during longer follow-up.5 In our patient, topical mitomycin C was not used because the clinical course required urgent airway stabilization and repeated bronchoscopic interventions; corticosteroids were used but did not provide sufficient clinical improvement.
Our subsequent attempt at silicone stenting immediately below the vocal cords was complicated by intolerance and marked laryngeal edema, necessitating emergent tracheostomy and eventual stent removal. Silicone stent failure was attributed mainly to secretion retention and the very proximal position of the stent near the vocal cords. This is consistent with pediatric data showing that severe glottic and subglottic edema can be associated with worse prognosis in post-intubation laryngeal injury cohorts, highlighting the vulnerability of the proximal airway to inflammatory compromise after instrumentation and foreign-body presence.10 Stenting remains a recognized strategy in complex post-intubation airway injury, but it can be accompanied by ongoing inflammation and the need for repeated interventions, emphasizing the importance of individualized selection and close follow-up.2
After removal of the silicone stent, a Montgomery airway stent was placed, achieving stable short-term airway patency and comfortable breathing without a tracheostomy cannula at two-week follow-up. Evidence from surgical series indicates that T-tube strategies can enable successful decannulation in a substantial proportion of patients, for example 82% in one cohort, while also underscoring the need for vigilance regarding granulation and infectious colonization as drivers of complications.9 The short follow-up period represents an important limitation. Longer surveillance would be required to assess long-term airway patency, restenosis, granulation formation, decannulation status, and the need for further interventions; however, extended follow-up was not available because the patient returned to a distant home region after early clinical stabilization. Given our limited follow-up duration, continued surveillance remains necessary to evaluate durability, monitor for restenosis, and address stent-related granulation should it arise.1,5,9,11
Conclusion
This case highlights the diagnostic and therapeutic complexity of high cervical post-intubation tracheal stenosis in children, particularly when the lesion is close to the vocal cords and prone to recurrence. Despite initial endoscopic dilation and definitive cervical tracheal resection with end-to-end anastomosis, early restenosis developed due to granulation tissue and exposed anastomotic sutures, requiring repeat bronchoscopic interventions. Silicone stenting immediately below the vocal cords was poorly tolerated and complicated by significant laryngeal edema, necessitating emergent tracheostomy. Placement of a Montgomery airway stent ultimately achieved satisfactory airway patency with resolution of stridor and successful breathing without a tracheostomy cannula at short-term follow-up. Early recognition of post-intubation stenosis, careful endoscopic reassessment of the anastomosis, and individualized escalation between endoscopic, surgical, and stenting strategies are essential to optimize outcomes in pediatric patients.
Data Sharing Statement
All data generated or analyzed during this case report are included in this published article.
Ethics Approval and Consent to Participate
Not applicable. As this is a single case report, ethical approval was not required in accordance with institutional policies.
Consent for Publication
Written informed consent was obtained from the parents for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Filauro M, Mazzola F, Missale F, Canevari FR, Peretti G. Endoscopic preoperative assessment, classification of stenosis, decision-making. Front Pediatr. 2020;7:532. doi:10.3389/fped.2019.00532
2. Gaspar MTDC, Maximiano LF, Minamoto H, Otoch JP. Tracheal stenosis due to endotracheal tube cuff hyperinflation: a preventable complication. Autops Case Rep. 2019;9(1):e2018072. doi:10.4322/acr.2018.072
3. Siddiqui NUR, Rehman AU, Sultan A, Abbas A, Siddiqui MIU, Abbas Q. Tracheal stenosis misdiagnosed as asthma: a case report. J Med Case Rep. 2024;18(1):588. doi:10.1186/s13256-024-04915-3
4. Gulilat D, Genetu A, Kejela S, Kassa S, Bekele A, Tizazu A. Nonmalignant tracheal stenosis: presentation, management and outcome in limited resources setting. J Cardiothorac Surg. 2024;19(1):21. doi:10.1186/s13019-024-02480-w
5. Cataneo DC, Ximenes AMG, Cataneo AJM. Mitomycin C in the endoscopic treatment of tracheal stenosis: a prospective cohort study. J Bras Pneumol. 2018;44(6):486–6. doi:10.1590/S1806-37562017000000423
6. Caruselli M, Amici M, Galante D, Paut O, De Francisci G, Carboni L. Post intubation tracheal stenosis in children. Pediatr Rep. 2014;6(3):5491. doi:10.4081/pr.2014.5491
7. Ghasempour Alamdari M, Modaresi MR, Shirzadi R, Kazemi S, Mirlohi SH. Long-term quality of life in children after balloon dilatation for subglottic and tracheal stenosis: eight years’ experience. Medicine. 2025;104(36):e44428. doi:10.1097/MD.0000000000044428
8. Al Dhouyani B, AbdulWahab A, Maarafiya M, Kabbara B, Abu-Hasan M. Successful treatment of multilevel tracheal stenosis post blunt chest trauma in a child by early bronchoscopic balloon dilatation: a case report. Pediatr Rep. 2025;17(6):117. doi:10.3390/pediatric17060117
9. Tsai SC, Lin FC. Surgical treatments for post-intubation laryngotracheal stenosis in patients with central nervous system injuries. Medicine. 2020;99(3):e18628. doi:10.1097/MD.0000000000018628
10. Lira NE, Kuhl LP, Maróstica PJC, Schweiger C. Post-intubation acute laryngeal injuries: analysis of predictive factors of poor prognosis. Laryngoscope. 2025;135(10):3535–3541. doi:10.1002/lary.32256
11. Aldakak MA, Fallouh N, Ibrahim B, Ahmad R, Abbas Y, Al Kateb K. Delayed diagnosis of post-traumatic bronchial transection in a pediatric patient: a case report. Int J Surg Case Rep. 2025;135:111892. doi:10.1016/j.ijscr.2025.111892
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.