Back to Journals » International Medical Case Reports Journal » Volume 19
Recurrent Pacemaker Lead Infection in A Patient with Opioid Induced Bradycardia: A Case Report
Authors Vadher A ![]() , Achuta KM, Devireddy R, Kambhatla S, Kondur A
, Achuta KM, Devireddy R, Kambhatla S, Kondur A
Received 16 March 2026
Accepted for publication 14 May 2026
Published 20 May 2026 Volume 2026:19 609537
DOI https://doi.org/10.2147/IMCRJ.S609537
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Thomas E Hutson
Abhishek Vadher,1 Kesava Manikanta Achuta,1 Rakesh Devireddy,2 Sujata Kambhatla,1 Ashok Kondur2
1Department of Internal Medicine, Garden City Hospital, Michigan State University, East Lansing, MI, USA; 2Department of Cardiology, Garden City Hospital, Michigan State University, East Lansing, MI, USA
Correspondence: Abhishek Vadher, Email [email protected]
Abstract: Pacemaker lead infections are complications of pacemakers that occur infrequently (0.13– 2.11 per 1,000 device recipients) but cause significant morbidity and mortality, especially in high-risk cohorts such as intravenous drug users (IVDUs). We report a 36-year-old male with pacemaker lead infection with methicillin-sensitive Staphylococcus aureus (MSSA). Despite the extraction of the entire pacemaker system and medical therapy based on the latest guidelines, reimplantation of a pacemaker in the setting of ongoing intravenous (IV) heroin abuse led to recurrent infection and 2.2 cm right atrial vegetation. This case highlights the unresolved tension between guideline-directed extraction for definite CIED infection and the difficult decision of reimplantation in a patient with ongoing intravenous drug use, recurrent bacteremia risk, and suspected opioid-associated conduction disease.
Keywords: pacemaker lead endocarditis, pacemaker lead infection, opioid induced bradycardia, infective endocarditis
Introduction
Cardiac implantable electronic devices, crucial in the management of bradyarrhythmias and conduction disorders, are plagued by an increased risk of infection. In the past two decades, infection rates have surged by 124%, from 1.53% to 3.43%, primarily due to the expanded indications, aging populations, and their rising comorbidities.1 Staphylococcal species (60–80%) predominate owing to their ability to form biofilms on surfaces of these devices, including leads, which can resist eradication. IVDUs, with recurrent bacteremia, delayed care-seeking behavior, and immune dysregulation, have the highest relative risk. Mortality exceeds 30% in recipients with device explantation, rising significantly in recurrent cases. Simultaneously, the opioid epidemic has led to an emerging and an unprecedented situation for cardiologists. Chronic use of opioids inhibits the HCN4 channel, leading to sick sinus syndrome in 1.2% of long-term users.2 These patients are unique; they present with dual vulnerabilities: a heightened risk of device infection due to repeated bacteremia and device presence (in ICDs) and intrinsic conduction disease. This paradoxical clinical situation is a testament to the interplay between device safety, conduction disorders, and the opioid epidemic.
Management requires a strict regimen of device removal, extended antimicrobial therapy, and deferred re-implantation, yet there are inevitable ethical considerations in high-risk populations, such as IVDUs, where non-adherence and recurring bacteremia are likely. Newer devices, such as leadless pacemakers that reduce infection risk with the elimination of hardware and removal of the transvenous lead, are promising, but due to technological and behavioral barriers, they remain underutilized in this population.3
Case Report
Initial Evaluation and Diagnosis
A 36-year-old male presented with complaints of progressive lower limb weakness, impaired ambulation, and bilateral cellulitis of the legs. On arrival, his vital signs were stable—temperature 98°F, respiratory rate 18/min, pulse 65/min, and blood pressure 105/70 mmHg. Physical examination revealed 2+ pitting edema extending to the mid-shin bilaterally. Cardiac, respiratory, and neurological examinations were unremarkable. The patient’s history was significant for a prior pacemaker implantation a decade earlier for suspected sick sinus syndrome, complicated by a pacemaker lead infection with a documented 1.6 cm vegetation and MSSA bacteremia six years prior. His history of intravenous heroin use further compounded his clinical risk.
Diagnostic Workup
Initial laboratory studies demonstrated marked leukocytosis (WBC 26,400/μL), anemia (hemoglobin 9.6 mg/dL), thrombocytopenia (platelet count 125,000/μL), and an elevated lactic acid level (2.02 mmol/L). Blood cultures were obtained promptly. A chest X-ray excluded pulmonary consolidation, while a 12-lead EKG—illustrated in Figure 1—revealed sinus tachycardia (HR 104/min), atrial tachycardia, occasional atrial premature complexes, intermittent atrial-sensed and ventricular-paced complexes, and an incomplete right bundle branch block without acute ST-T abnormalities. The patient’s previous history of device-related infections, corroborated by prior TEE findings of a 1.6×1.4 cm vegetation and CT evidence of septic emboli, prompted heightened vigilance during this evaluation.
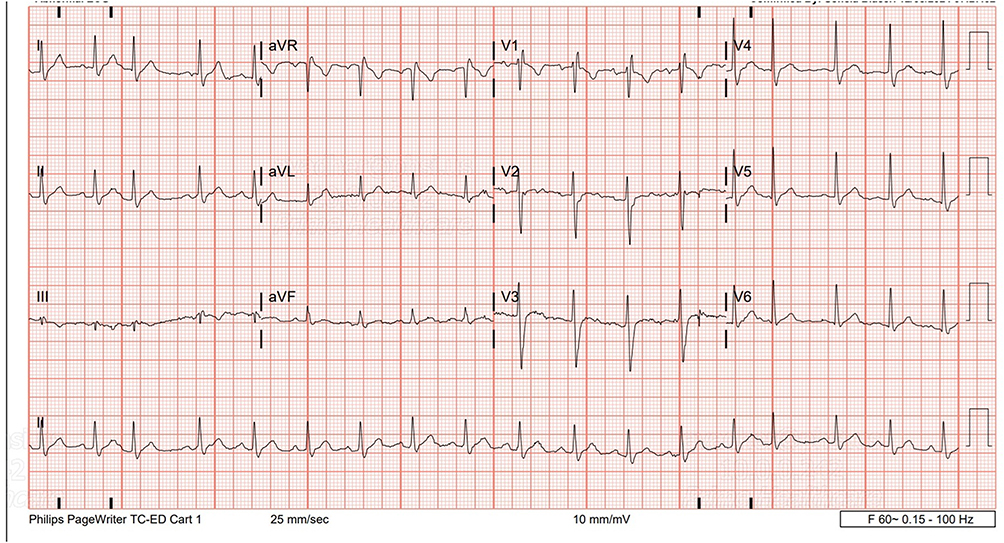 |
Figure 1 EKG on arrival showing normal sinus rhythm, normal PR, QRS, QTc and no acute ST-T Changed. |
Hospital Course and Complications
The patient’s initial hospitalization culminated in a course of intravenous oxacillin administered via a PICC line for 28 days, following complete pacemaker removal. Despite this, he returned one month later with persistent dizziness. Repeat evaluation revealed EKG changes suggestive of pericarditis, including episodes of 2–4 second pauses on cardiac monitoring, though thyroid and calcium levels were normal. With a working diagnosis of sinus bradycardia, chronic opioid use was considered a possible contributor, although a definitive causal relationship could not be established in this case. Treatment for pericarditis was initiated with high-dose NSAIDs, colchicine, and intermittent Toradol.
Given his high-risk profile, particularly his ongoing intravenous heroin use and recurrent device infections, the electrophysiology team faced a challenging decision. Despite the infection risk, a new DDD pacemaker (BIOTRONIK ELUNA 8 DR T 394969) was implanted to address his conduction abnormalities. Subsequent cardiac MRI revealed only a trace pericardial effusion with preserved biventricular function, while transthoracic echocardiography (TTE) identified a highly mobile 2.2×1.0 cm vegetation in the right atrium attached to the tricuspid valve and evidence of a vegetation on the RV pacemaker lead, accompanied by mild tricuspid regurgitation as illustrated in Figures 2 and 3. The patient was commenced on Ceftriaxone and Vancomycin, and plans were made for further evaluation with transesophageal echocardiography (TEE). TEE is central in the evaluation of suspected lead-associated infective endocarditis because it better characterizes lead and valvular vegetations and their embolic risk than transthoracic imaging alone. In this case, TTE demonstrated recurrent vegetation on the right atrium/tricuspid apparatus and pacemaker lead, but definitive TEE confirmation was not completed as the patient left against medical advise.
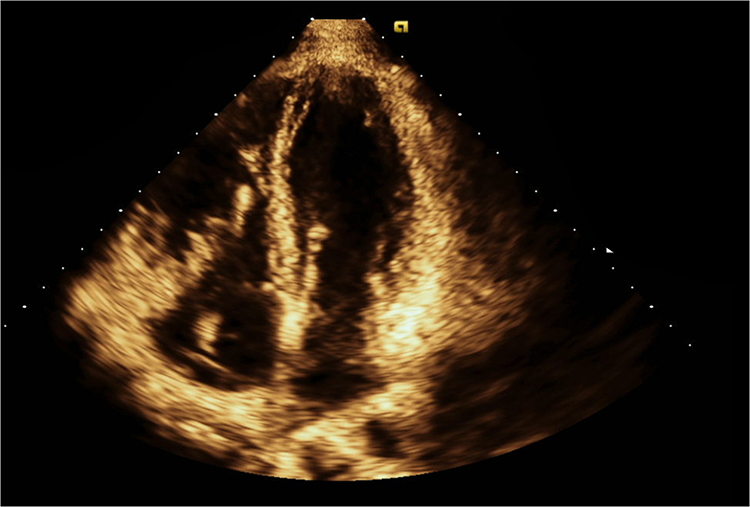 |
Figure 2 TTE Apical four chamber view showing RA vegetation. |
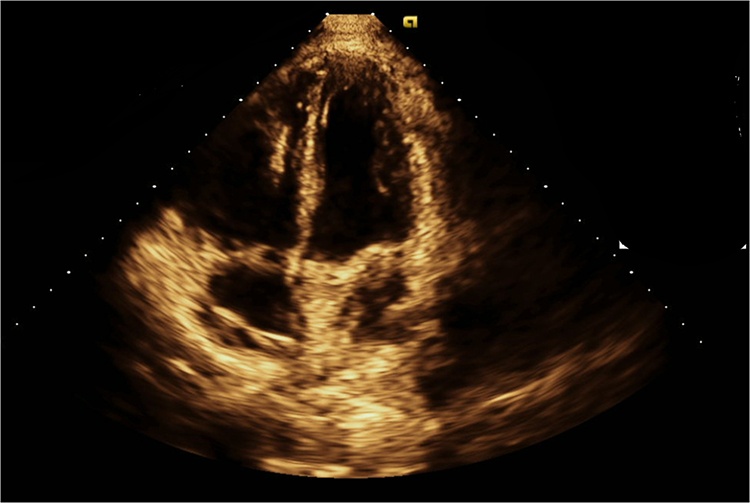 |
Figure 3 TTE Apical 4 Chamber view showing Pacemaker lead mass vegetation in Right ventricle. |
Timeline:
- Initial pacemaker implantation for suspected sick sinus syndrome 10 years ago
- First MSSA lead infection with 1.6 cm vegetation and extraction 6 years ago
- Completion of IV oxacillin after extraction of pacemaker 6 years ago
- Admission 2–3 years back with dizziness and pauses, reimplantation of DDD pacemaker
- Discovery of recurrent 2.2×1.0 cm right atrial/tricuspid/RV lead vegetation during this admission period
- Left against medical advice before definitive TEE/re-extraction
Final Diagnoses
- Recurrent pacemaker lead infection
- Pacemaker-associated vegetation (2.2x1.0 cm in the right atrium and additional mass on the RV lead)
- Pericarditis
- Sinus bradycardia potentially secondary to chronic opioid use
Management Challenges
This case epitomizes the clinical conundrum of managing recurrent Cardiovascular implantable electronic device (CIED) infections in a high-risk patient. The coexistence of opioid-induced conduction abnormalities and persistent bacteremia from ongoing intravenous drug use creates a dual vulnerability where the necessity for pacing support must be balanced against the risk of re-infection.
This case also raises an ethical dilemma. Reimplantation provides potentially life-saving pacing support, yet ongoing intravenous drug use increases the likelihood of recurrent bacteremia, repeat device infection, and incomplete treatment. These decisions should therefore be made through a multidisciplinary process involving electrophysiology, infectious diseases, and addiction medicine, with attention to patient autonomy, harm reduction, and post discharge follow-up barriers.
Discussion
The management of recurrent CIED infections in the background of opioid-induced conduction disturbances is a problem with a growing number of unknown and evolving factors. In this case, the effects of chronic opioid use alongside the recurrent device-related infections produced the interrelationship of several independent variables contributing to mutual exacerbation of the clinical picture.3 Chronic use of opioids not only affects the electrical activity of the heart by reducing the HCN4 channel function and, therefore, the development of conduction disturbances that require the implantation of CIEDs but also predisposes patients to permanent bacteremia and the formation of biofilm on the surfaces of the device.4 As a result, the patient is in a situation where the need for pacing, which is necessary to sustain life, must be balanced with a high risk of new infections.
Diagnostic evaluation has revealed the crucial importance of advanced diagnostic modalities, such as transesophageal echocardiography (TEE). Additionally, the use of newly developed techniques, such as 18F-FDG PET/CT, has been shown to be central for determining the entire spread of the infection.5 TEE remains important, but it cannot reliably distinguish infectious from noninfectious lead echodensities and when suspicion persists or echocardiography is equivocal, FDG PET/CT is complementary rather than universally definitive, and its sensitivity can be reduced in low-grade infection or after prior antibiotic exposure. Given the experience of the patient in terms of recurrent device infections, it is particularly vital that these imaging strategies allow for early detection of biofilm-associated vegetations and multifocal infectious processes.6 However, the management of this patient posed several challenges. First of all, the patient’s experience of recurrent infections with biofilm-associated pathogens requires their complete removal and prolonged antimicrobial therapy.7 Current consensus documents recommend complete device and lead removal for definite CIED infection, including lead-associated endocarditis, valvular infective endocarditis without definite device involvement, and persistent or relapsing bacteremia when no alternative source is identified. Reimplantation, when still indicated, should generally be delayed until signs of local and systemic infection have resolved and blood cultures have remained negative; recent guidance suggests at least 3 days of negative cultures after extraction, with longer delays in patients with valvular infective endocarditis or visible vegetations. In patients at particularly high risk of reinfection, alternative strategies such as leadless pacing or other nontransvenous approaches may be considered on a case-by-case basis. Secondly, there was also a need to factor in the patient’s active intravenous drug use and, therefore, to be prepared for his recurrent bacteremia and the associated difficulties with treatment compliance.8
The ethical and surgical dilemmas are considerable in such scenarios. The issue of reimplantation of the pacemaker in high-risk individuals continues to provoke fears about potential reinfection. Despite the fact that newer infection-resistant technologies (example: leadless pacemakers) may reduce this risk, these technologies are underused in high-risk populations due to technical and behavioral barriers.9 Observational data and a 2023 systematic review suggest that leadless reimplantation after infected CIED extraction is feasible and has low reinfection rates, but the evidence remains mostly nonrandomized and timing strategies vary across studies.
Furthermore, the issue of economic burden also arises in the context of IV drug users since they are found to have higher rates of hospitalizations and premature cessation of treatment. Current guidelines from the 2017 Heart Rhythm Society (HRS) Expert Consensus Statement recommend complete device and lead removal for all patients with definite CIED system infection. This includes lead-associated endocarditis, valvular endocarditis, and persistent or recurrent bacteremia (Class I recommendation), as retained hardware serves as a nidus for relapse and significantly increases mortality. However, among IVDUs, high relapse rates and ethical concerns surrounding reimplantation mandate a more individualized and multidisciplinary management approach.9
This case also highlights the ethical tension between providing potentially life-sustaining pacing support and exposing a patient with ongoing injection drug use to a high probability of reinfection. Contemporary literature on infective endocarditis in people who inject drugs supports a multidisciplinary approach that includes electrophysiology, infectious diseases, addiction medicine, and social work, with early consideration of medications for opioid use disorder and discharge planning barriers. In selected patients who continue to require pacing after extraction, leadless pacemakers may reduce hardware burden and may be a reasonable alternative, although evidence remains observational and individualized decision-making is essential.10
Conclusion
This case illustrates the difficult balance between guideline-based management of definite CIED infection and the practical challenge of pacing reimplantation in a patient with ongoing intravenous drug use and suspected opioid-associated bradycardia. The report underscores the importance of complete device extraction, careful reassessment of pacing need, and multidisciplinary decision-making that includes infectious diseases and addiction services. Leadless pacing or other alternative strategies may be considered in selected high-risk patients, but the optimal approach in this setting remains individualized.
Ethical Compliance
Written consent was obtained from the patient for publication of this case report. All procedures followed were in accordance with the ethical standards. Institution approval is not required to publish the case details.
Funding
No external funding was received for this study.
Disclosure
The authors declare no conflicts of interest regarding the publication of this case report.
References
1. Han H, Hawkins NM, Pearman CM, Birnie DH, Krahn AD. Epidemiology of cardiac implantable electronic device infections: incidence and risk factors. EP Europace. 2021;23(Supplement_4):iv3–6. doi:10.1093/europace/euab042
2. Krantz MJ, Palmer RB, Haigney MCP. Cardiovascular complications of opioid use. J Ame College Cardiol. 2021;77(2):205–223. doi:10.1016/j.jacc.2020.11.002
3. El-Chami MF, Bonner M, Holbrook R, et al. Leadless pacemakers reduce risk of device-related infection: review of the potential mechanisms. Heart Rhythm. 2020;17(8):1393–1397. doi:10.1016/j.hrthm.2020.03.019
4. Mendhe S, Badge A, Ugemuge S, Chandi D. Impact of biofilms on chronic infections and medical challenges. Cureus. 2023. doi:10.7759/cureus.48204
5. Horgan SJ, Mediratta A, Gillam LD. Cardiovascular imaging in infective endocarditis. Circulation. 2020;13(7). doi:10.1161/circimaging.120.008956
6. Roy R, Tiwari M, Donelli G, Tiwari V. Strategies for combating bacterial biofilms: a focus on anti-biofilm agents and their mechanisms of action. Virulence. 2017;9(1):522–554. doi:10.1080/21505594.2017.1313372
7. Kusumoto FM, Schoenfeld MH, Wilkoff BL, et al. HRS expert consensus statement on cardiovascular implantable electronic device lead management and extraction. Heart Rhythm. 2017;14(12):e503–e551. doi:10.1016/j.hrthm.2017.09.001
8. Blomström-Lundqvist C, Traykov V, Erba PA, et al; ESC Scientific Document Group. European heart rhythm association (EHRA) international consensus document on how to prevent, diagnose, and treat cardiac implantable electronic device infections—endorsed by the heart rhythm society (HRS). the Asia Pacific Heart Rhythm Society (APHRS), the Latin American Heart Rhythm Society (LAHRS), International Society for Cardiovascular Infectious Diseases (ISCVID) and the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) in Collaboration With the European Association for Cardio-Thoracic Surgery (EACTS). Euro J Cardio Thoracic Surg. 2020;22(4):515–549.
9. Arcinas LA, Sheldon RS. Complications related to pacemakers and other cardiac implantable electronic devices: essentials for internists and emergency physicians. Intern Emerg Med. 2023;18(3):851–862. doi:10.1007/s11739-023-03227-6
10. Yucel E, Bearnot B, Paras ML, et al. Diagnosis and management of infective endocarditis in people who inject drugs: JACC state-of-the-art review. J Am Coll Cardiol. 2022;79(20):2037–2057. doi:10.1016/j.jacc.2022.03.349
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.