Back to Journals » International Journal of Women's Health » Volume 18
Recognition and Management of Transfusion-Associated Immune Hemolytic Crisis in Pregnant Patients with Thalassemia: Analysis of Three Cases and Construction of a Clinical Pathway
Received 21 October 2025
Accepted for publication 6 March 2026
Published 5 June 2026 Volume 2026:18 574613
DOI https://doi.org/10.2147/IJWH.S574613
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Haijuan Li,1,* Lingling Huang,1,* Lijun Li2
1Department of Obstetrics, Wuming Hospital of Guangxi Medical University, Nanning, Guangxi, People’s Republic of China; 2Department of Blood Transfusion, Wuming Hospital of Guangxi Medical University, Nanning, Guangxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lijun Li, Department of Blood Transfusion, Wuming Hospital of Guangxi Medical University, No. 26, Yongning Road, Wuming District, Nanning, Guangxi, 530000, People’s Republic of China, Email [email protected]
Abstract: Pregnancy complicated by thalassemia, especially in transfusion-dependent thalassemia (TDT) patients, poses major obstetric challenges. Due to physiological hemodilution and a shortened red blood cell (RBC) lifespan, these patients require regular transfusions to maintain stable hemoglobin levels. Long-term transfusions increase the risks of alloimmunization and autoimmune hemolytic anemia (AIHA). These conditions can be misdiagnosed as primary thalassemia or normal pregnancy-related physiological changes due to their non-specific manifestations, thus delaying critical intervention. This raises risks of maternal mortality, thrombosis, heart failure, fetal growth restriction (FGR), and preterm birth. While guidelines recommend multidisciplinary management for pregnant women with thalassemia, there’s no standardized clinical pathway for rapid differentiation between alloimmune and autoimmune hemolysis and initiating targeted intervention after transfusion refractoriness. This study analyzed three cases of pregnancy complicated by thalassemia and immune hemolysis with clinical significance. Based on these cases and guidelines, a management pathway was established emphasizing immediate antibody screening and direct antiglobulin test (DAT, Coombs test) upon signs of transfusion refractoriness to differentiate alloimmunity from AIHA and guide targeted treatment.
Keywords: pregnancy, thalassemia, autoimmune hemolytic anemia, alloimmunity, transfusion refractoriness, clinical pathway
Introduction
Thalassemia is a hereditary blood disorder that affects hemoglobin production and contributes to significant public health challenges. The rising incidence among women of childbearing age in certain regions, such as in Southeast Asia, the Mediterranean region, India, the Middle East, Africa, and southern China has been on the rise.1,2 Thalassemia-complicated pregnancy increases the risk of fetal growth restriction (FGR), premature birth, low birth weight, and stillbirth by causing maternal anemia-induced placental dysfunction.3 It also leads to the need for careful monitoring of patients because the physiological increase in blood volume and hemodilution during pregnancy can further exacerbate maternal anemia. This situation may lead to some non-transfusion-dependent thalassemia (NTDT) patients becoming transfusion-dependent, thereby requiring an adjustment in treatment strategies.4 While blood transfusions improve pregnancy outcomes, they also introduce significant complications. One such complication is transfusion-associated immune hemolytic crisis (TAIHC); this is a severe adverse reaction and presents a significant threat to the safety of both mothers and infants.5,6 Pregnant patients with thalassemia have a significantly higher risk of immune hemolysis due to repeated blood transfusions, which can lead to both alloimmune and autoimmune hemolytic anemia (AIHA). This risk is heightened compared to patients with conventional types of anemia because thalassemia is a genetic disorder that often requires frequent, lifelong transfusions to correct severe anemia.7,8 Hemolytic crises are life-threatening in both occasional transfusion and when a thalassemic woman is transfused. Furthermore, the clinical signs of hemolytic crises are not specific. These signs include persistent anemia that is challenging to correct and a suboptimal increase in hemoglobin levels following transfusion. Clinicians frequently attribute these symptoms to the progression of thalassemia or to physiological changes occurring during pregnancy. This misattribution can lead to delayed diagnosis and significantly increasing the risks for both the mother and the fetus.9,10 Currently, clinical practice primarily uses passive checks to identify hemolytic crises after typical symptoms like hemoglobinuria and chills with a high fever appear. This lack of early active screening and awareness of emergency intervention poses serious risks to patient safety.11
The management of transfusion-related adverse reactions has emerged as a pivotal area of research in recent years, particularly in the fields of hematology and obstetrics and gynecology. However, studies on the clinical characteristics and treatment guidelines for immune hemolytic crisis in pregnant women with thalassemia remain scattered and lack systematic evidence support. Consequently, we conducted a retrospective analysis of three representative cases of pregnant patients with thalassemia, encompassing one fatal case, one case with delayed diagnosis, and one case with successful clinical management. The study systematically elaborated on the disease spectrum, diagnostic challenges, and key clinical insights for the effective management of this condition. By adhering to the 2024 Guidelines for Pregnancy Management issued by the British Society for Hematology (BSH)4 and integrating relevant domestic and international clinical consensus statements,12–15 a standardized clinical pathway for early identification and proactive intervention was formulated.
Case Presentation
This case series has been approved by the Ethical Review Committee of Wuming Hospital of Guangxi Medical University [Approval No. WM-2025(160)], including approval of the study protocol and permission to publish the case details. For the three cases presented in this manuscript, written consent for the publication of any potentially identifiable images or data has been properly obtained as follows: for the deceased patient, written consent was acquired from the patient prior to death; for the remaining two living patients, written consent was obtained directly from the patients themselves.
Case 1: Death Due to Sepsis-Induced AIHA and Poor Treatment Compliance
Basic Information
A 23-year-old Zhuang ethnic primigravida (gravida 1, para 0) with a previous diagnosis of β-thalassemia carrier (genotype: β17/βN) was admitted to our hospital. During pregnancy before admission, her Hb levels fluctuated between 76 and 131 g/L, and she had no prior history of blood transfusion.
Diagnosis and Treatment Process
She was admitted on June 13, 2024, at 38+1 weeks of gestation due to FGR indicated by ultrasound. On admission, she presented with obvious symptomatic anemia, manifested as persistent dizziness, fatigue and pale complexion. The complete blood count (CBC) analysis showed that Hb levels were 68 g/L, neutrophil percentage (NEUT%) was 80.7%, and white blood cell count (WBC) was 19.77×109/L. Both the direct antiglobulin test (DAT, Coombs test) and the indirect antiglobulin test were negative. Her serum ferritin level was 818.1 ng/mL, and despite her serum folate level being 1.2 ng/mL, she had received continuous folic acid supplementation throughout pregnancy. Furthermore, no signs of acute infection were detected during pregnancy, and there were no clinical manifestations of infection during the prenatal examinations that were conducted irregularly. Considering her symptomatic anemia and third-trimester status approaching labor, blood transfusion therapy was implemented. On June 14, she received a transfusion of 2 units of leukocyte-depleted suspended RBCs. A recheck of CBC after transfusion showed that the Hb level increased to 77 g/L. On June 16, she delivered a live infant vaginally. Meconium-stained amniotic fluid was noted during delivery, which was identified as a potential risk factor for perinatal infection. Therefore, oral cefaclor sustained-release tablets (375 mg per tablet) were administered at a dose of 1 tablet twice daily for routine infection prophylaxis. The newborn weighed 2260 g and had an Apgar score of 10–10-10 (at 1, 5, and 10 min, respectively). She then developed recurrent fever on the 2nd day after delivery, with the highest body temperature reaching 39.0°C. Re-examination showed further elevation of WBC (31.45×109/L), which, combined with persistent high fever, suggested the progression of infection. She was initially administered cefaclor dispersible tablets (375 mg per tablet, 1 tablet twice daily) for infection control from June 18 to 19. However, due to persistent high fever up to 39.0°C and no improvement in infection-related indicators, the antibiotic regimen was switched to piperacillin-sulbactam sodium (4.5 g, intravenously, every 8 hours) for enhanced anti-infective therapy from June 20 to 23. A BC recheck on June 22 showed Hb levels of 61 g/L, WBC of 27.7×109/L, absolute neutrophil count (ANC) of 18.40×109/L, high-sensitivity C-reactive protein (hsCRP) levels of 34.07 mg/L, and procalcitonin (PCT) levels of 0.33 ng/mL. On June 24, her body temperature returned to normal for half a day. Although continued hospitalization was recommended, she and her family signed the informed consent for discharge against medical advice. She was readmitted to another hospital on June 29 due to recurrent fever. A CBC performed upon admission revealed Hb levels of 53 g/L, WBC of 27.7×109/L, ANC of 18.40×109/L, RBCs of 2.42×1012/L, hematocrit levels of 17.2%, and hsCRP levels of 50.34 mg/L. Sepsis was suspected, and she was administered moxifloxacin combined with meropenem for anti-infective therapy and fluconazole sodium chloride injection for antifungal treatment. On July 2, she received a transfusion of 2 units (U) of leukocyte-depleted suspended RBCs. Laboratory testing showed a DAT (IgG+C3d) titer of 2+ and positive irregular antibody screening; thus, secondary wAIHA was considered.13,16 In the early morning of July 3, she was treated with prednisone followed by a transfusion of 2 U of suspended RBCs. A post-transfusion CBC review showed that Hb levels were 57 g/L, WBC was 21×109/L, and ANC was 18.65×109/L, with a slight improvement in fever symptoms. Nevertheless, she and her family insisted on discharge and completed the necessary paperwork at noon on that same day. That night, she developed a fever again and was re-hospitalized. A repeat of CBC analysis showed that Hb levels were 40 g/L, NEUT% was 80.7%, WBC was 30.79×109/L, and PCT levels were 11.27 ng/mL. Given her unstable condition, she was transferred to the intensive care unit (ICU). Unfortunately, she succumbed to the critical illness on the 42nd day after delivery despite rescue efforts.
Case Characteristics
This case highlights that infection (especially sepsis) is an important risk factor for inducing or exacerbating AIHA,13,17 and it also emphasizes the extreme importance of patient education, treatment compliance, and continuous follow-up by a multidisciplinary team (MDT) in the management of critical cases.4
Case 2: Persistent Transfusion Refractoriness During Pregnancy with Postpartum Diagnosis of AIHA
Basic Information
A 23-year-old Zhuang ethnic pregnant woman (gravida 2, para 1) had a vaginal delivery of a female infant at 35 weeks of gestation in 2020. The infant, with a birth weight of 1990 g, is currently alive and healthy. During that pregnancy, she had a history of receiving blood transfusion and subsequently developed puerperal infection after delivery. She reported a history of chronic gastritis and denied any history of drug allergy. She had previously been diagnosed with HbH disease (genotype: --SEA/αCSα). During the current pregnancy, her Hb levels fluctuated between 48 g/L and 78 g/L. Blood transfusion was initiated at 9 weeks of gestation, and a total of 33 U of leukocyte-depleted suspended RBCs were transfused. However, the transfusion efficacy remained unsatisfactory, and transfusion refractoriness was suspected.15,18 No in-depth immunological evaluation was performed for this persistent warning sign during the aforementioned period.
Diagnosis and Treatment Process
She was admitted on November 22, 2024, at 36+5 weeks of gestation due to upper abdominal pain. She was diagnosed with gastritis and received fluid replacement for symptomatic relief. Upon admission, CBC analysis revealed that Hb levels were 67 g/L, total bilirubin was 61.10 μmol/L (with indirect bilirubin at 46.10 μmol/L), and Bishop score was 4. From November 23 to 24, misoprostol was administered for cervical ripening until the Bishop score reached 6, followed by an oxytocin challenge test (OCT) + and planned delivery; however, labor induction failed. On November 24, she received a transfusion of 2 U of leukocyte-depleted suspended RBCs; post-transfusion recheck showed Hb levels of 72 g/L. On November 25, she had a body temperature of 37.5°C. Due to intrauterine infection, she underwent a cesarean section on November 25 and delivered a healthy, mature live infant. The newborn had a birth weight of 2300 g and an Apgar score of 10–10-10. Postoperatively, intravenous meropenem was administered for anti-infection treatment. Subsequently, she developed symptoms including hemoglobinuria and fever, with the maximum body temperature reaching 39°C. Placental pathological examination indicated moderate acute amnionitis and chorioamnionitis, confirming the diagnosis of intrauterine infection. Laboratory tests showed a positive DAT (IgG+C3d) and positive plasma antibody screening, though the specificity of the antibody was not identified. She was finally diagnosed with secondary wAIHA. Fever resolution was achieved on November 29. On December 2, re-examination showed Hb levels of 62 g/L, WBC of 8.03×109/L, and hsCRP levels of 6.46 mg/L. Following a conservative treatment of glucocorticoid therapy and hematopoietic raw material supplementation, she recovered and was discharged.
Case Characteristics
This case is a typical example of diagnostic delay. The prolonged history of transfusion refractoriness during pregnancy already served as a strong indicator of AIHA; however, it failed to trigger a timely diagnostic process, resulting in the missed opportunity for early intervention during pregnancy.4,13
Case 3: Successful Identification of Alloimmunization in Early Pregnancy
Basic Information
A 40-year-old advanced-age Zhuang ethnic pregnant woman (gravida 1, para 0) with a history of 1 artificial abortion, 2 failed in vitro fertilization-embryo transfer (IVF-ET) cycles, and a pre-admission history of congenital heart disease was presented. She was previously diagnosed with Hb H disease, with the genotype of --SEA/αCSα).
Diagnosis and Treatment Process
At 8 weeks of gestation (July 4, 2025), the patient was admitted to the Department of Gynecology due to severe anemia (Hb 67 g/L). During hospitalization, she received 3 transfusions of leukocyte-depleted suspended RBCs totaling 6 U. Subsequent follow-up tests showed sequential Hb levels of 63 g/L, 73 g/L, and 83 g/L. At 13 weeks of gestation (August 19), the patient was readmitted to the Department of Obstetrics with recurrent anemia (Hb 62 g/L). After transfusion of 2 U of leukocyte-depleted suspended RBCs, her Hb level showed an unsatisfactory increase (only rising to 65 g/L). Clinically, transfusion refractoriness was immediately suspected. Further testing of the patient’s blood sample, including irregular antibody screening under special conditions (4°C), identified the presence of anti-M alloantibodies, while the DAT (Coombs test) yielded negative results. The patient then received 2 U of M antigen-negative leukocyte-reduced suspended RBCs, with follow-up confirming an increase in Hb to 77 g/L, which remained stable for 2 months. At 26 weeks of gestation (November 5), anemia relapsed, and the patient received another 2 U of M antigen-negative leukocyte-reduced suspended RBCs. Post-transfusion Hb rose to 72 g/L and was maintained stably for 1 month. At 30+3 weeks of gestation, routine antenatal screening revealed a blood pressure (BP) reading of 145/89 mmHg, leading to a diagnosis of gestational hypertension. At 31 weeks of gestation (December 26), laboratory tests showed the following results: Hb 71 g/L, hematocrit (HCT) 27.7%, WBC count 9.66×109/L, serum albumin (ALB) 31.5 g/L, and 24-hour urinary protein excretion 244.2 mg/24h. Labetalol was administered on the same day for antihypertensive therapy. On December 30, tocolytic therapy was initiated for the management of gestational hypertension. On December 31, dexamethasone was given to promote fetal lung maturation. At 32 weeks of gestation, repeat testing indicated worsening anemia (Hb: 66 g/L). The patient thus received 2 U of M antigen-negative leukocyte-reduced suspended RBCs on January 1, 2026, with an additional 2 U M antigen-negative leukocyte-reduced suspended RBCs administered on January 2. A follow-up test on January 9 showed an increase in Hb to 85 g/L. On January 3, a BP measurement of 152/98 mmHg prompted the initiation of combined tocolytic and antihypertensive treatment. Near 34 weeks of gestation, antenatal assessment documented a BP of 162/102 mmHg. Given the history of gestational hypertension and disease progression, a diagnosis of severe preeclampsia was made. On January 12, nifedipine was added for enhanced BP control. Preoperative laboratory tests on the same day (at 34 weeks of gestation, prior to cesarean section) revealed: Hb 81 g/L, N-terminal pro-B-type natriuretic peptide (NT-proBNP) 205 pg/mL, and serum uric acid (UA) 593 μmol/L. Following a MDT consultation, the patient was deemed to have indications for cesarean section due to poorly controlled hypertension and concurrent pulmonary hypertension. She underwent low-segment cesarean section on January 13 (at 34+1 weeks of gestation), resulting in the uneventful delivery of a premature live infant with a birth weight of 2000 g and Apgar scores of 10/10/10. Placenta accreta was identified intraoperatively and managed promptly. The estimated intraoperative blood loss was 400 mL. On the first postoperative day (January 13), the patient continued to receive supportive care, including transfusion of 2 U of M antigen-negative leukocyte-reduced suspended RBCs to correct anemia secondary to surgical blood loss, along with anti-infective agents and uterotonic medications. On the second postoperative day (January 14), a repeat Hb test showed a level of 77 g/L, and enoxaparin was initiated for anticoagulant therapy. Subsequently, the patient’s condition remained stable, with satisfactory healing of the abdominal surgical incision and well-controlled blood pressure. No additional complications occurred, and she was discharged from the hospital as scheduled.
Case Characteristics
This case presents a complicated pregnancy with HbH disease complicated by multiple high-risk factors, including CHD, severe PE, and severe anemia. It demonstrates a successful management model characterized by active monitoring and rapid response. In clinical practice, transfusion refractoriness was treated as emergency. Through comprehensive interventions involving multidisciplinary collaboration, active anemia correction (via targeted transfusion), and timely pregnancy termination, favorable maternal and neonatal outcomes were ultimately achieved.10,18,19
Comparison of Clinical Characteristics Among Three Cases
As summarized in Tables 1–3, the three cases demonstrated distinct disparities in hemolysis-related indicator levels, transfusion reactions, concurrent complications [including preeclampsia (PE), congenital heart disease (CHD), and gestational diabetes mellitus (GDM)], comorbidities, interventions, and pregnancy outcomes. Notably, these differences not only accounted for the variations in transfusion dosages and clinical intervention strategies implemented during the diagnostic and therapeutic course but also underscoring the clinical relevance of obstetric complications (eg., PE) in modulating AIHA via hemolytic pathways.20
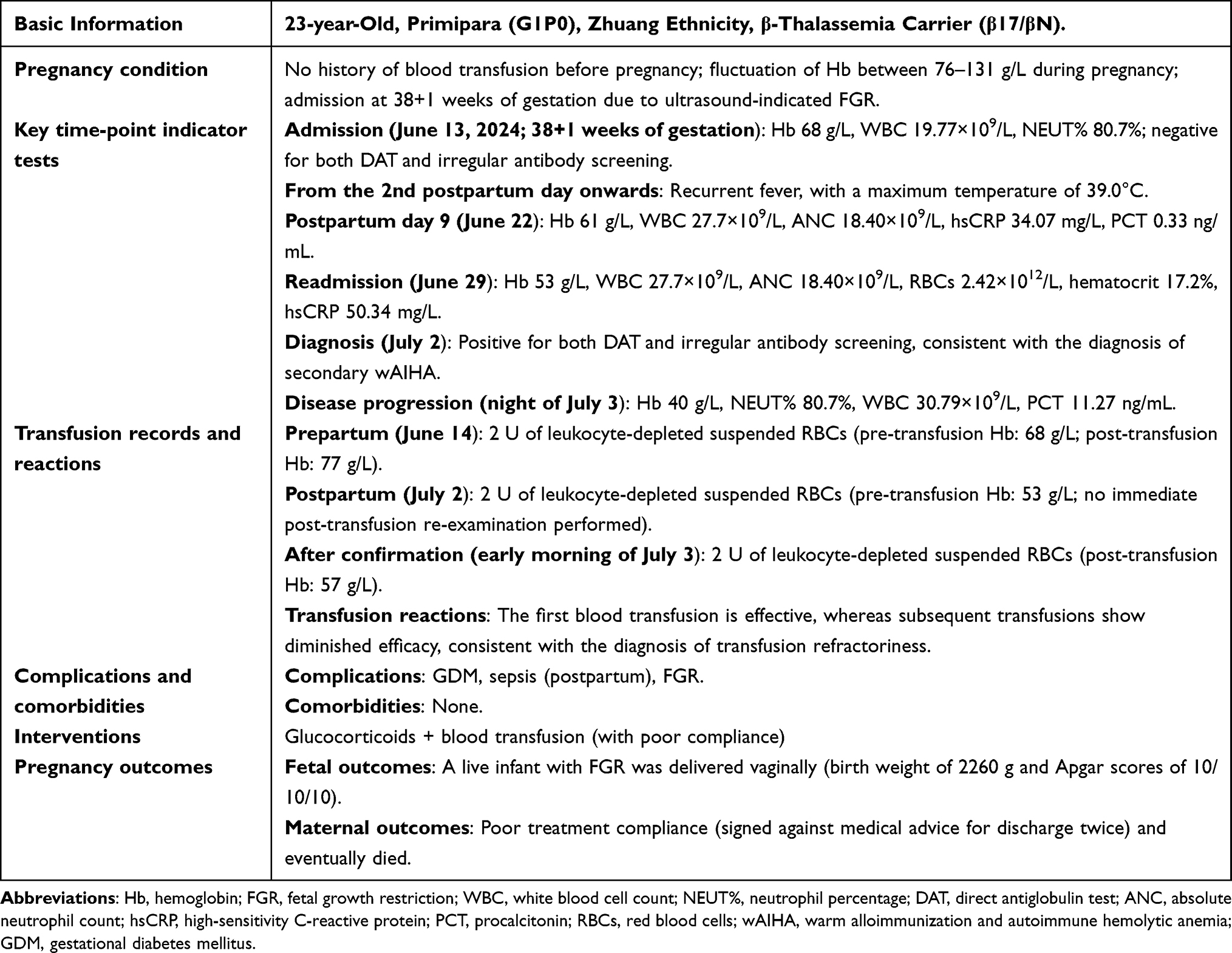 |
Table 1 Clinical Characteristics, Laboratory Examinations, and Diagnosis-Treatment Process of Case 1 |
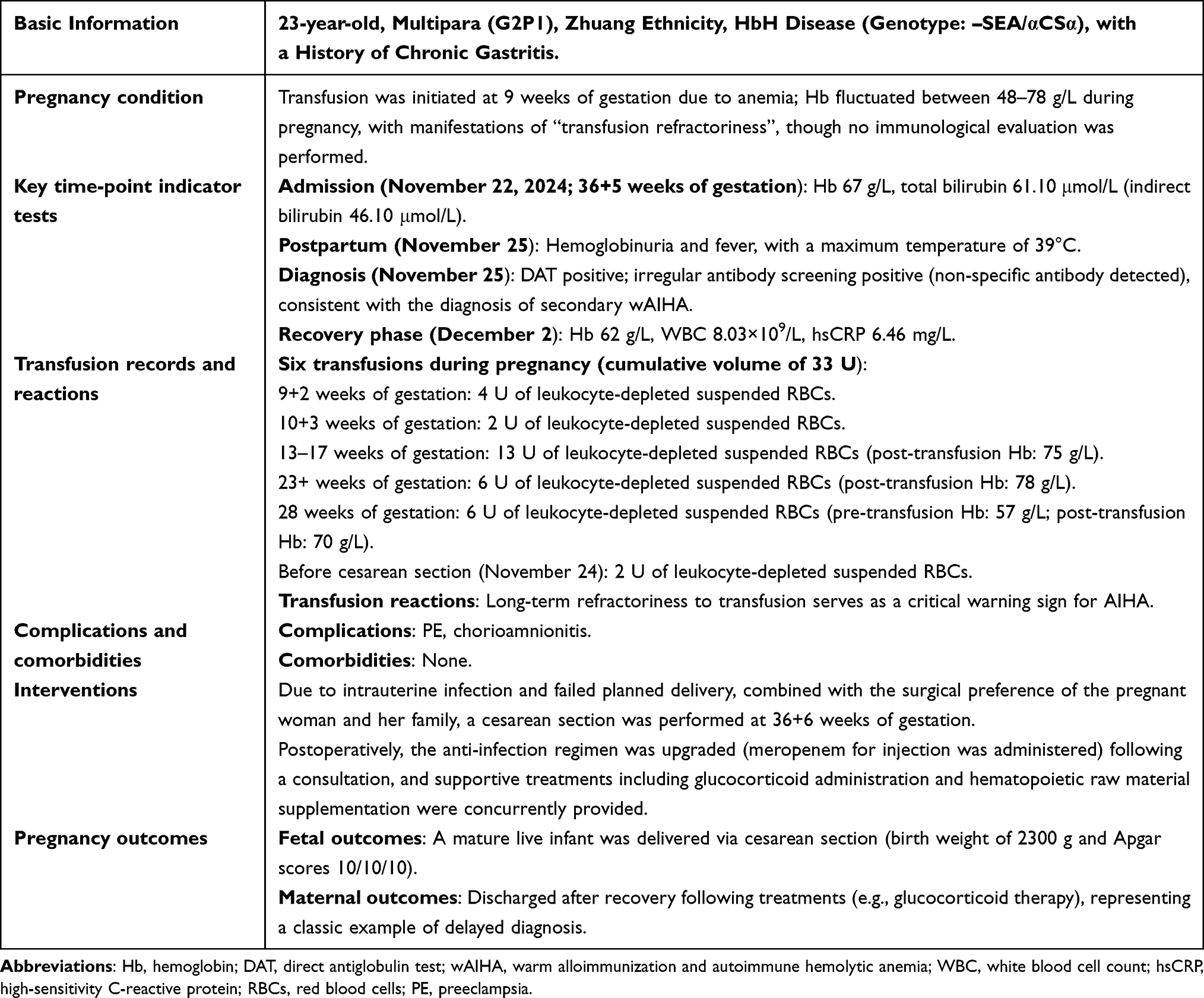 |
Table 2 Clinical Characteristics, Laboratory Examinations, and Diagnosis-Treatment Process of Case 2 |
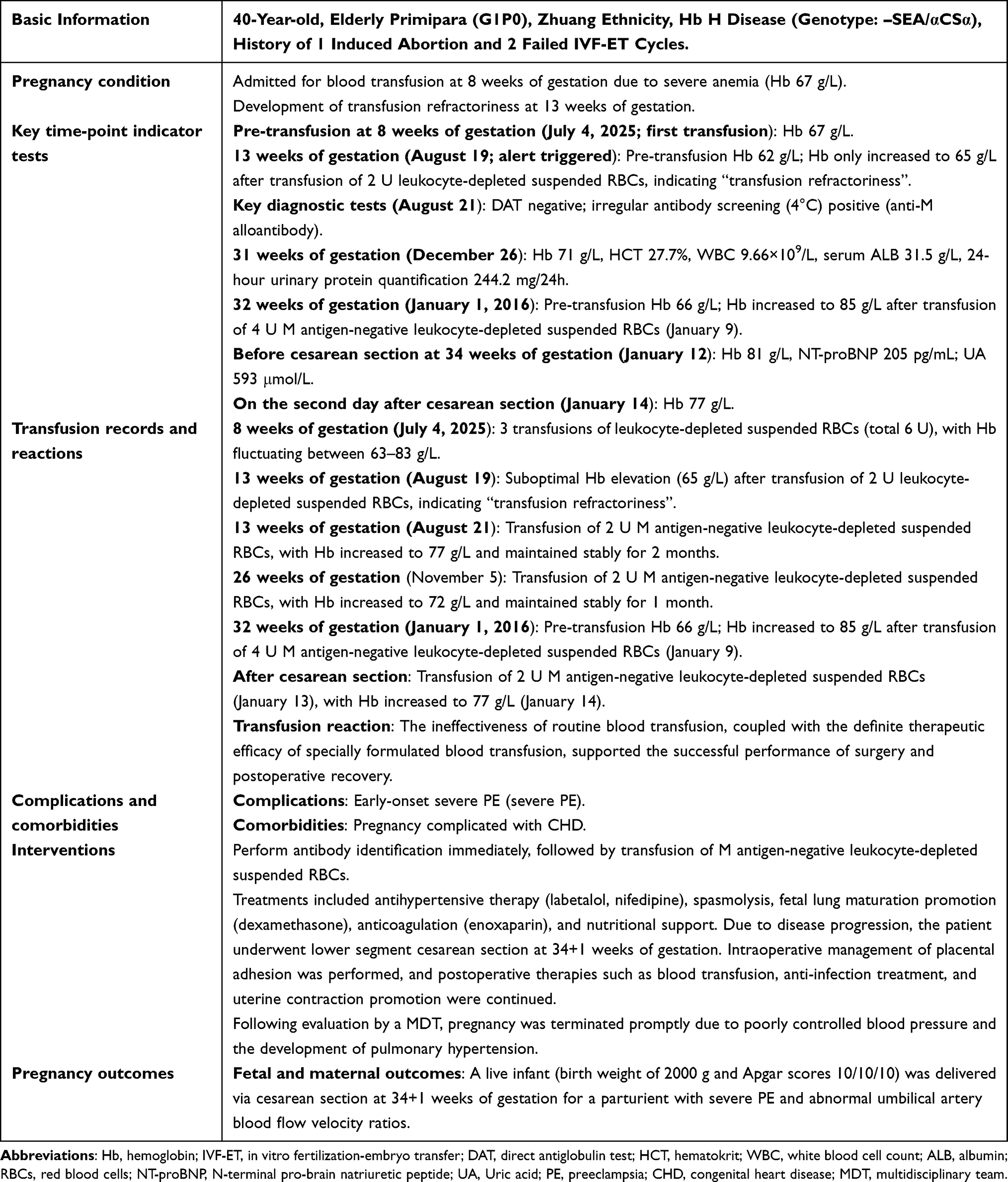 |
Table 3 Clinical Characteristics, Laboratory Examinations, and Diagnosis-Treatment Process of Case 3 |
Discussion
This study conducted an in-depth analysis of 3 cases of pregnancy complicated by thalassemia and immune hemolysis. Based on the latest domestic and international clinical guidelines and evidence-based data, we focused on transfusion refractoriness as the core early warning indicator, and presented the clinical spectrum of immune hemolysis in pregnant patients with thalassemia. It ranges from catastrophic outcomes (eg., Case 1 with death, mainly attributed to AIHA caused by infection and pregnancy-induced hypoimmunity, uncontrolled postpartum sepsis, and poor patient compliance) to successful management (eg., complete recovery in Case 2 and a successful example of “active monitoring and rapid response” in Case 3). On this basis, a standardized diagnostic and triage pathway was further established, providing actionable practical references for clinically reducing the risk of adverse maternal and fetal outcomes.
Early Warning Value of Transfusion Refractoriness
A common clinical precursor in all 3 cases of this study was “transfusion refractoriness,” defined as failure of Hb to increase to the clinically expected level after RBC transfusion (it is generally accepted that Hb should increase by approximately 5–10 g/L per unit of RBC transfused).15,18 This manifestation is not an accidental result of primary thalassemia or physiological changes during pregnancy, but rather should be recognized as a clear clinical trigger for initiating the screening of immune hemolysis. Although the guidelines of the Thalassemia International Federation (TIF) emphasize that transfusion-dependent thalassemia (TDT) patients require dynamic monitoring of transfusion efficacy, they have not yet provided a specific definition or quantitative evaluation criteria for “transfusion refractoriness”, leading to delays or misjudgments in clinical practice.18 Based on the diagnosis and management of the cases in this study and clinical practice, we propose the following recommendations: Routine re-examination of CBC at 24–48 hours after transfusion should be included in the standard protocol for pregnant patients with TDT. Furthermore, transfusion refractoriness should be clearly defined as a scenario where, after excluding confounding factors such as acute blood loss and infection, the actual increase in Hb is lower than the expected or fails to remain stable following transfusion of an adequate volume of RBCs. The clarification of this definition can effectively reduce the subjectivity of clinical judgment and promote the standardized initiation of screening procedures after the occurrence of transfusion refractoriness.
In the differential diagnosis of immune hemolysis, irregular antibody screening and DAT (Coombs test) are two core detection items. Simultaneous implementation of these two tests can assist in distinguishing between alloimmune hemolysis and AIHA, laying a foundation for subsequent precise intervention.21 For example, in Case 3, based on the serological characteristics of positive irregular antibody screening (anti-M antibody) + negative direct Coombs test, combined with the manifestation of transfusion refractoriness, a rapid diagnosis of alloimmune hemolysis was made. Subsequent transfusion of specially matched blood lacking the M antigen resulted in a steady increase in the patient’s Hb level, with both maternal and fetal conditions remaining stable at 30 weeks of gestation. This validates the critical guiding significance of accurate antibody identification for treatment decision-making in alloimmune hemolysis.22 In Case 2, the patient was positive for direct Coombs test and irregular antibody screening, but no specific alloantibodies were detected. Combined with a history of repeated transfusions during pregnancy and the manifestation of “transfusion refractoriness”, the patient was finally diagnosed with wAIHA. Complete recovery was achieved after standardized treatment with glucocorticoids, indicating that the treatment of AIHA should focus on inhibiting autoimmune responses, and precise identification is a prerequisite for avoiding the erroneous transfusion of mismatched blood and exacerbation of hemolysis.23,24
Establishment of a Standardized Diagnostic and Triage Pathway
Based on the diagnosis and treatment experience of 3 cases in this study, combined with domestic and international guidelines,4,17,19,25 we have developed the “Diagnostic and Triage Pathway for Immune Hemolysis after Transfusion Refractoriness in Pregnant Women with Thalassemia” (Figure 1). With “transfusion refractoriness” as the trigger point, this pathway adopts a three-level process of “early warning-diagnosis-triage” to achieve rapid differentiation and precise management of immune hemolysis and other etiologies. The specific steps are as follows:
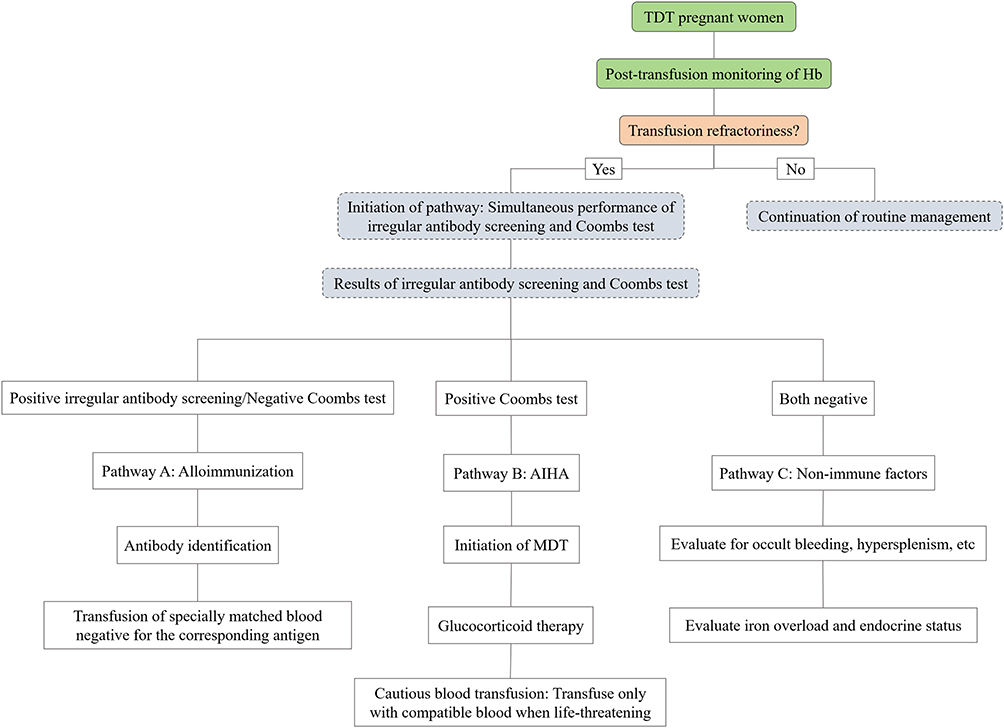 |
Figure 1 Clinical pathway. Abbreviations: TDT, transfusion-dependent thalassemia; Hb, hemoglobin; AIHA, autoimmune hemolytic anemia; MDT, multidisciplinary team. |
Early Warning and Triggering
For all transfusion-dependent pregnant women with thalassemia, a monitoring mechanism of CBC testing within 24–48 hours after each transfusion should be established, with a focus on the changing trend of Hb levels. Once manifestations of transfusion refractoriness appear, this pathway must be triggered immediately to initiate further investigation, so as to avoid diagnostic delay caused by waiting for typical hemolytic symptoms.
Concurrent Diagnosis
After the pathway is activated, irregular antibody screening and DAT (Coombs test) should be conducted simultaneously. The parallel implementation of these two tests can minimize the differentiation time and gain a treatment window for patients with acute hemolysis.
Triage and Management
According to the results of concurrent diagnosis, patients are divided into three management pathways for hierarchical intervention. Pathway A (positive irregular antibody screening/negative or weakly positive Coombs test) is for the management of alloimmune hemolysis. This pathway is for the treatment of alloimmunity-related hemolysis. The blood transfusion department should immediately conduct antibody specificity identification and transfuse specially matched blood products negative for the corresponding antigens based on the antibody type.26
Pathway B (positive Coombs test) is for AIHA management. This pathway confirms the diagnosis of AIHA, requiring the immediate activation of MDT collaboration. First-line of treatment involves glucocorticoids (such as prednisone at a dose of 0.5–1.5 mg/kg/day).4,27 Blood transfusion support must be administered with extreme caution and only performed in life-threatening situations. Additionally, minimally incompatible RBCs with negative Coombs test results should be selected to avoid exacerbating hemolysis.28 Furthermore, active investigation of predisposing factors for AIHA (such as infection and medication) is necessary. In Case 1, the patient experienced aggravated AIHA induced by postpartum sepsis, which indicates that infection control exerts a crucial impact on the prognosis of AIHA.
Pathway C (negative irregular antibody screening and negative Coombs test) is used for investigation of non-immune factors. This pathway requires exclusion of non-immune causes of transfusion refractoriness, such as occult bleeding and aggravated hypersplenism, as well as the assessment of iron overload and endocrine status.4
The previously mentioned pathway not only elucidates the standardized evaluation and management process following transfusion refractoriness to prevent diagnostic delays or inappropriate treatments stemming from differences in clinicians’ experience, but it also highlights the necessity of multidisciplinary collaboration, thereby possessing considerable practical significance.
Paramount Importance of MDT Collaboration and Whole-Process Management
The fatal outcome of Case 1 (postpartum sepsis-induced aggravated AIHA, with sepsis as a key contributing factor to death, and poor treatment adherence also affecting prognosis) warns us that the lack of MDT collaboration and whole-process management is a key factor contributing to adverse outcomes. The BSH guidelines emphasize that pregnant women with thalassemia belong to the high-risk pregnancy group, and their management should rely on an MDT composed of obstetricians, hematologists, transfusion medicine specialists, cardiologists, endocrinologists, and neonatologists. Moreover, such collaboration should run through the entire course of pre-pregnancy, pregnancy, and postpartum periods.4 Consistent with this, the RCOG Green Top Guideline 66 specifically focuses on the management of β-thalassemia in pregnancy, highlighting that transfusion-dependent and non-transfusion-dependent thalassemia patients require individualized, whole-course management involving obstetric and hematological collaboration, with special attention to infection prevention and treatment as well as patient compliance enhancement.29 Additionally, the MDT should strengthen patient education and improve treatment adherence through regular follow-ups, popular science brochures, and other means. For instance, Case 1 experienced disease deterioration due to refusal of hormone therapy after delivery, which indicates that patient education is an indispensable part of MDT management.
Limitations
This study was a retrospective case series analysis, which only included 3 cases from a single center. The small sample size and inherent selection bias mean that the findings cannot fully represent the clinical characteristics of all patients with pregnancy complicated by thalassemia and concurrent immune hemolysis. Thus, the generalizability of the research conclusions requires further verification through multi-center, large-sample cohort studies. Additionally, the management pathway established in this study was developed based on the experience of our center and recommendations from existing guidelines, and its effectiveness has not yet been verified by prospective randomized controlled trials.
Conclusion
The analysis of 3 treatment cases preliminarily identifies transfusion refractoriness as a core early-warning indicator for the management of pregnancy complicated with TDT. Centered on this early-warning concept, a standardized clinical management pathway was proposed, whose core protocol requires the immediate concurrent implementation of irregular antibody screening and DAT upon the identification of transfusion refractoriness. This pathway is designed to enable rapid triage and precise intervention for alloimmunization and AIHA. The contrasting outcomes of failure and success in these cases underscore the urgency of leveraging this early-warning-driven pathway to reduce diagnostic delays and optimize maternal-fetal outcomes. Given the limited sample size of the current study, the universality and effectiveness of this management strategy necessitate further verification through large-scale, prospective clinical trials.
Abbreviations
ALB, albumin; AIHA, autoimmune hemolytic anemia; BP, blood pressure; BSH, British Society for Hematology; CBC, complete blood count; CHD, congenital heart disease DAT, direct antiglobulin test; FGR, fetal growth restriction; GDM, gestational diabetes mellitus; HbH, hemoglobin H; HCT, hematocrit; hsCRP, high-sensitivity C-reactive protein; ICU, intensive care unit; IVF-ET, in vitro fertilization-embryo transfer; MDT, multidisciplinary team; NC, absolute neutrophil count; NEUT%, neutrophil percentage; NT-proBNP, N-terminal pro-B-type natriuretic peptide; NTDT, non-transfusion-dependent thalassemia; OCT, oxytocin challenge test; PCT, procalcitonin; PE, preeclampsia; RBC, red blood cell; TAIHC, transfusion-associated immune hemolytic crisis; TDT, transfusion-dependent thalassemia; TIF, Thalassemia International Federation; UA, uric acid; U, units; wAIHA, warm AIHA; WBC, white blood cell count.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics Approval and Informed Consent
This case series has been approved by the Ethical Review Committee of Wuming Hospital of Guangxi Medical University [Approval No. WM-2025(160)], including approval of the study protocol and permission to publish the case details.
Consent for Publication
For the three cases presented in this manuscript, written consent for the publication of any potentially identifiable images or data has been properly obtained as follows: for the deceased patient, written consent was acquired from the patient prior to death; for the remaining two living patients, written consent was obtained directly from the patients themselves.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas. They also took part in drafting, revising, or critically reviewing the article All authors have given a full approval of this manuscript to be published, and have agreed on the journal to which the article should be submitted. They also agree to be accountable for all aspects of the work.
Funding
This work was supported by the Self-financed Project of the Health Commission of Guangxi Zhuang Autonomous Region entitled “Correlation Analysis between Thromboelastography Parameters and Postpartum Hemorrhage in Pregnant Women with Preeclampsia“ (No. Z20210050) and the Self-financed Project of the Health Commission of Guangxi Zhuang Autonomous Region entitled “Correlation Study between Group B Streptococcus (GBS) Infection at Various Stages of Pregnancy, Vaginal Microecological Imbalance and Adverse Pregnancy Outcomes (No. Z-A20230788).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lee JS, Rhee TM, Jeon K, et al. Epidemiologic trends of thalassemia, 2006-2018: a nationwide population-based study. J Clin Med. 2022;11(9):2289. doi:10.3390/jcm11092289
2. Su Y, Xie J, He J, et al. Screening and treatment of thalassemia. Clin Chim Acta. 2025;570. 120211. doi:10.1016/j.cca.2025.120211
3. Wang R, Xu S, Hao X, et al. Anemia during pregnancy and adverse pregnancy outcomes: a systematic review and meta-analysis of cohort studies. Front Glob Womens Health. 2025;6:1502585. doi:10.3389/fgwh.2025.1502585
4. Shah FT, Nicolle S, Garg M, et al. Guideline for the management of conception and pregnancy in thalassaemia syndromes: a British society for haematology guideline. Br J Haematol. 2024;204(6):2194–12. doi:10.1111/bjh.19362
5. Bezirgiannidou Z, Christoforidou A, Kontekaki E, et al. Hyperhemolytic syndrome complicating a delayed hemolytic transfusion reaction due to anti-p1 alloimmunization, in a pregnant woman with hbo-arab/β-thalassemia. Mediterr J Hematol Infect Dis. 2016;8(1):e2016053. doi:10.4084/MJHID.2016.053
6. Cannas G, Dubreuil L, Fichez A, et al. Delayed severe hemolytic transfusion reaction during pregnancy in a woman with β-thalassemia intermediate: successful outcome after eculizumab administration. Am J Case Rep. 2021;22:e931107. doi:10.12659/AJCR.931107
7. Shaiegan M, Moghaddam M, Maghsudlu M, et al. Red blood cell immunization and contributing factors in 685 thalassemia patients. Int J Hematol Oncol Stem Cell Res. 2022;16(1):9–14. doi:10.18502/ijhoscr.v16i1.8435
8. Baudo F, Perotti C, Branscomb J, White MS, Gibson RW, Eckman JR. Red blood cell alloimmunization in transfusion-dependent thalassemia: a systematic review. Transfus Med Rev. 2019;33(1):12–19. doi:10.1016/j.tmrv.2018.12.001
9. Patel PB, Patel N, Hedges MA, et al. Hematologic complications of pregnancy. Eur J Haematol. 2025;114(4):596–614. doi:10.1111/ejh.14372
10. Zhou Y, Ding YL, Zhang LJ, et al. Direct antiglobulin test-negative autoimmune hemolytic anemia in a patient with β-thalassemia minor during pregnancy: a case report. World J Clin Cases. 2022;10(4):1388–1393. doi:10.12998/wjcc.v10.i4.1388
11. Ren H, Wang Y. Hemolytic crisis. Chin Pediatr Emerg Med. 2020;27(8):577–581. doi:10.3760/cma.j.issn.1673-4912.2020.08.004
12. Hill QA, Stamps R, Massey E, et al. The diagnosis and management of primary autoimmune haemolytic anaemia. Br J Haematol. 2017;176(3):395–411. doi:10.1111/bjh.14478
13. Barcellini W, Fattizzo B. How I treat warm autoimmune hemolytic anemia. Blood. 2023;141(4):438–439. doi:10.1182/blood.2022019024
14. Society of Perinatal Medicine, Chinese Medical Association; Obstetrics Group. Obstetrics and Gynecology Branch, Chinese Medical Association. Experts consensus on thalassaemia during pregnancy. Chin J Perinat Med. 2020;23(9):577–584. doi:10.3760/cma.j.cn113903-20200401-00293.
15. Society of Perinatal Medicine. Chinese medical association; clinical blood transfusion management committee of chinese blood transfusion association. expert consensus on blood transfusion in obstetrics. Chin J Perinat Med. 2023;26(1):4–10. doi:10.3760/cma.j.cn113903-20220401-00315.
16. Fontaine MJ. Role of complement in patients with autoimmune hemolytic anemia and platelet transfusion refractoriness. Transfus Clin Biol. 2019;26(3):152–154. doi:10.1016/j.tracli.2019.06.232
17. Jäger U, Barcellini W, Broome CM, et al. Diagnosis and treatment of autoimmune hemolytic anemia in adults: recommendations from the first international consensus meeting. Blood Rev. 2020;41:100648. doi:10.1016/j.blre.2019.100648
18. Cappellini MD, Cohen A, Porter J, et al. Guidelines for the Management of Transfusion Dependent Thalassaemia (TDT).
19. Cappellini MD, Farmakis D, Porter J, et al. Guidelines: For the Management of Transfusion Dependent Thalassaemia (TDT).
20. Fattizzo B, Bortolotti M, Fantini NN, et al. Autoimmune hemolytic anemia during pregnancy and puerperium: an international multicenter experience. Blood. 2023;141(16):2016–2021. doi:10.1182/blood.2022018890
21. Xia R, Zhang Q, Chen QF. Expert consensus on pre-transfusion testing and clinical transfusion for patients with autoimmune hemolytic anemia. Chin J Blood Transfusion. 2017;30(7):663–665. doi:10.13303/j.cjbt.issn.1004-549x.2017.07.002
22. Manduzio P. Alloantibody identification: the importance of temperature, strength reaction and enzymes-a practical approach. Hematol Rep. 2024;16(4):815–824. doi:10.3390/hematolrep16040077
23. Abdallah GEM, Abbas WA, Elbeih EAS, et al. Systemic corticosteroids in the treatment of warm autoimmune hemolytic anemia: a clinical setting perspective. Blood Cells Mol Dis. 2021;92:102621. doi:10.1016/j.bcmd.2021.102621
24. Das SS, Mukherjee S, Chakrapani A, et al. Clinical perspectives, immunohematologic insights, and transfusion management in IgA-associated autoimmune hemolytic anemia. Immunohematology. 2022;38(3):82–89. doi:10.21307/immunohematology-2022-047
25. Farmakis D, Porter J, Taher A, et al. Thalassaemia international federation guidelines for the management of transfusion-dependent thalassemia. Hemasphere. 2022;6(8):e732. doi:10.1097/HS9.0000000000000732
26. Gupta KP, Gajjar MD, Patel TR, et al. Antibody screening and identification in donors and general patients at a tertiary care teaching hospital in Western India. Asian J Transfus Sci. 2019;13(1):34–38. doi:10.4103/ajts.AJTS_94_17
27. Li S, Li Y. The characteristics of aiha patients benefited from glucocorticoid treatment. Indian J Hematol Blood Transfus. 2020;36(2):429–431. doi:10.1007/s12288-019-01224-4
28. Binsfeld M, Devey A, Gothot A. Transfusion support and pre-transfusion testing in autoimmune haemolytic anaemia. Vox Sang. 2024;119(10):1029–1038. doi:10.1111/vox.13699
29. Royal College of Obstetricians and Gynaecologists. Management of Beta Thalassaemia in Pregnancy (Green-Top Guideline No. 66). London: RCOG; 2014.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cost-Benefit Analysis of Genetic Testing as a Prenatal Diagnostic Tool for Thalassemia: A Single-Center Study From Central Thailand
Malasai K, Jittikoon J, Udomsinprasert W, Talungchit P, Youngkong S, Sangroongruangsri S, Mahasirimongkol S, Chaikledkaew U
ClinicoEconomics and Outcomes Research 2025, 17:33-43
Published Date: 4 February 2025