Back to Journals » International Journal of Nanomedicine » Volume 21
Recent Advances in Nanoscale Sprayable Hydrogels for Cancer Management: Nanoparticle-Loaded Formulations for Therapy and Prevention
Authors Lee JM, Kang SJ, Yoon MS, Jo MJ, Yoo MK, Park SY, Bong S ![]() , Kim J, Park S, Lee Y, Shin Y, Lee HJ, Kim JS, Park CW, Shin DH
, Kim J, Park S, Lee Y, Shin Y, Lee HJ, Kim JS, Park CW, Shin DH
Received 19 September 2025
Accepted for publication 6 January 2026
Published 14 January 2026 Volume 2026:21 558788
DOI https://doi.org/10.2147/IJN.S558788
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yan Shen
Jae Min Lee,1,* Su Jeong Kang,1,* Moon Sup Yoon,1 Min Jeong Jo,2 Myeong Kyun Yoo,1 So Yeon Park,1 Sunghyun Bong,1 Jonghyuk Kim,1 Seonmin Park,1 Yeseung Lee,1 Yuseon Shin,1 Hye Jin Lee,1 Jin-Seok Kim,3 Chun-Woong Park,1 Dae Hwan Shin1,4
1College of Pharmacy, Chungbuk National University, Cheongju, Chungcheongbuk-do, 28160, Republic of Korea; 2Department of Pharmaceutical Chemistry, University of Kansas, Lawrence, KS, 66047, USA; 3Drug Information Research Institute (DIRI), College of Pharmacy, Sookmyung Women’s University, Seoul, 04310, Republic of Korea; 4Chungbuk National University Hospital, Chungbuk National University, Cheongju, Chungcheongbuk-do, 28644, Republic of Korea
*These authors contributed equally to this work
Correspondence: Chun-Woong Park; Dae Hwan Shin, College of Pharmacy, Chungbuk National University, Osongsaengmyeong 1-ro, Osong-eup, Heungdeok-gu, Cheongju, Chungcheongbuk-do, 28160, Republic of Korea, Tel +82 43 261 3330 ; +82 43 261 2820, Fax +82 43 268 2732, Email [email protected]; [email protected]
Abstract: Sprayable hydrogels represent an emerging class of nanoscale, localized drug delivery systems in oncology, offering rapid in situ gelation, strong tissue adhesion, and minimally invasive administration. Recent advances have integrated nanotechnology into sprayable hydrogel formulations to enhance therapeutic efficacy at tumor sites through various strategies, including nanoemulsions, nanocomposites, nanoparticle-loaded matrices, nanovaccines, and nanosprays. Across preclinical models, these platforms have demonstrated quantitative improvements, including up to 70– 95% reductions in residual tumor burden, 2– 5-fold increases in intratumoral drug retention, and survival extensions ranging from 30% to over 60% compared with free-drug controls. These platforms have demonstrated the ability to eliminate residual tumor cells, activate antitumor immunity, and prevent recurrence at surgical margins or mucosal interfaces. Therapeutic modalities include the controlled release of chemotherapeutics, immune checkpoint inhibitors, and metabolic or oxidative regulators, all delivered within nanostructured hydrogel matrices. Several systems also reported over 80% suppression of local recurrence at surgical margins and significant potentiation of immune activation markers such as CD8⁺ T-cell infiltration and dendritic cell maturation. Nanoscale sprayable hydrogels have shown promise across diverse clinical applications, including peritoneal carcinomatosis, superficial skin tumors, and premalignant mucosal lesions. The hydrogels themselves comprise a wide range of nanostructured materials, such as thermosensitive polymers, self-gelling powders, supramolecular assemblies, and nanoparticle-laden scaffolds, that enable precise spatial and temporal control of drug delivery. In this review, we categorize these systems based on cancer type, underlying mechanisms of action, and therapeutic goals (treatment vs prevention). By integrating nanotechnology, immunotherapy, and tissue-responsive design, nanoscale sprayable hydrogels represent a modular and adaptable platform for personalized cancer care, with compatibility across surgical, endoscopic, and topical administration routes. However, despite these advances, the clinical translation of sprayable hydrogels remains limited by challenges such as sterilization constraints, device–material compatibility issues, storage and handling stability, and regulatory hurdles, all of which must be systematically addressed to enable widespread clinical adoption.
Keywords: sprayable hydrogel, localized drug delivery, postoperative cancer therapy, cancer immunotherapy, precancerous lesion prevention
Introduction
Localized drug delivery systems have long been recognized as an important strategy to achieve therapeutically effective concentrations of therapeutic agents at tumor sites while minimizing systemic toxicity.1 Systemic administration of chemotherapeutics or immunotherapeutics is often hindered by biological barriers such as abnormal vasculature, high interstitial pressure, and heterogeneous tissue permeability, resulting in suboptimal intratumoral accumulation.2 At the same time, high systemic doses can lead to dose-limiting toxicity, immunosuppression, and a significant reduction in the patient’s quality of life. By restricting therapeutic exposure to the diseased site, it is possible to maintain higher drug concentrations where they are most needed, extend the duration of therapeutic presence, and substantially reduce the burden on healthy tissues. This principle has been applied through various forms, including biodegradable implants, injectable hydrogels, microparticle depots, and implantable polymeric matrices. However, many of these approaches present practical limitations in surgical or clinical settings. Solid implants may fail to conform to the irregular geometry of resection cavities, injectable systems can be difficult to distribute evenly over large or complex surfaces, and invasive placement can extend surgical time and exacerbate tissue trauma.3 Hydrogels, as three-dimensional crosslinked polymer networks with tunable mechanics, high water content, and excellent biocompatibility, have been widely used in localized drug delivery because they conform to irregular tissues and can sustain therapeutic release.4
Sprayable hydrogels have emerged as a next-generation approach that directly addresses these limitations by combining the favorable drug release properties of hydrogels with the procedural simplicity of spray application.5 Typically formulated as low-viscosity liquids or colloidal dispersions, sprayable hydrogels can be delivered via manual spray devices, CO2-driven nebulizers, or catheter-based systems. Upon deposition onto the target site—such as a postsurgical cavity, organ surface, or mucosal layer—the formulation undergoes rapid sol–gel transition.6 This transformation can be triggered by physiological cues such as temperature, ionic strength, pH, or enzymatic activity, or by in situ chemical crosslinking reactions. The resulting hydrogel adheres intimately to the underlying tissue, forming a stable, continuous coating that remains intact under physiological conditions. Beyond acting as a physical barrier against tumor cell dissemination or bacterial invasion, the hydrogel functions as a local drug reservoir, releasing therapeutic payloads over periods ranging from days to weeks.7 Spray application offers precise dosing, site-specific targeting, and coverage of anatomically challenging areas, making it particularly advantageous in oncologic surgery where microscopic residual disease is a primary cause of recurrence.
The therapeutic capabilities of sprayable hydrogels are greatly enhanced through the integration of nanoscale components. In such systems, nanoparticles are either encapsulated within the hydrogel matrix or incorporated as part of the structural network itself. Polymeric nanoparticles, liposomes, micelles, dendrimers, metallic nanostructures, nanoemulsions, and protein-based nanocarriers have been incorporated into hydrogels to improve functional performance. These nanoscale entities enable the encapsulation of both hydrophilic and hydrophobic drugs, protect labile biomolecules such as nucleic acids and proteins from degradation, and facilitate transport across cellular and tissue barriers.8 Moreover, nanoparticles can be engineered to respond to tumor-specific microenvironmental cues—such as acidic pH, elevated glutathione, reactive oxygen species (ROS), or overexpressed enzymes—enabling precise spatial and temporal control over drug release.9–12 Nanoscale systems embedded within sprayable hydrogels can be designed for sequential or synergistic action, for instance by releasing immunomodulatory agents rapidly to prime the local immune environment, followed by sustained release of cytotoxic agents to eradicate residual tumor cells.
The combination of nanotechnology with sprayable hydrogel platforms offers advantages that extend beyond drug protection and controlled release. Nanoparticles can modulate the tumor microenvironment (TME) in ways unattainable with free drugs alone. For example, nanoparticle delivery of immune checkpoint inhibitors directly to the surgical site can elicit potent antitumor immune responses while minimizing systemic immune-related adverse events.13 Nanovaccines can enhance antigen uptake by dendritic cells and induce robust systemic antitumor immunity. Metallic nanoparticles can be activated by external stimuli—such as light, ultrasound, or magnetic fields—to generate localized hyperthermia or ROS, thereby augmenting cytotoxicity. Additionally, nanoscale components can serve as imaging agents, enabling theranostic applications that combine therapy with real-time monitoring of disease progression and treatment response.14
From a materials design perspective, the incorporation of nanoscale building blocks into sprayable hydrogels provides a modular framework.15 By varying the type of nanoparticles, surface functionalization, and therapeutic payload, the hydrogel system can be tailored to the specific molecular, anatomical, and microenvironmental characteristics of different tumor types. This aligns with the concept of precision medicine, in which treatment is adapted not only to the tumor’s molecular profile but also to its structural and biological context. The capacity to integrate multiple therapeutic mechanisms—chemotherapy, immunotherapy, photodynamic therapy, oxidative modulation—within a single continuous coating further broadens the clinical utility of this platform.16
Our review differs from prior hydrogel-based localized cancer therapy reviews by specifically focusing on nanoscale sprayable hydrogel systems that have emerged after 2020. Unlike earlier summaries that broadly discuss injectable or implantable hydrogels, this work uniquely highlights formulations that integrate nanomedicines with spray-deployable platforms, emphasizing their rapid in situ gelation, conformal tissue coverage, and enhanced translational potential for postoperative therapy and cancer prevention.17–19 This perspective provides a distinct and timely synthesis of next-generation hydrogel technologies that enable precise local deposition and synergistic nanoscale interactions not addressed in previous reviews.
This review provides a comprehensive synthesis of recent advances in nanoscale sprayable hydrogel-based systems for cancer therapy. Case studies are analyzed according to therapeutic mechanism, material composition, delivery strategy, and target disease context, highlighting the breadth of their applications across diverse tumor types and clinical scenarios. Through these examples, the review aims to illustrate how nanoscale sprayable hydrogels can contribute to the elimination of residual tumor cells, suppression of recurrence, modulation of the TME, and even preventive interventions in oncology (Figure 1).
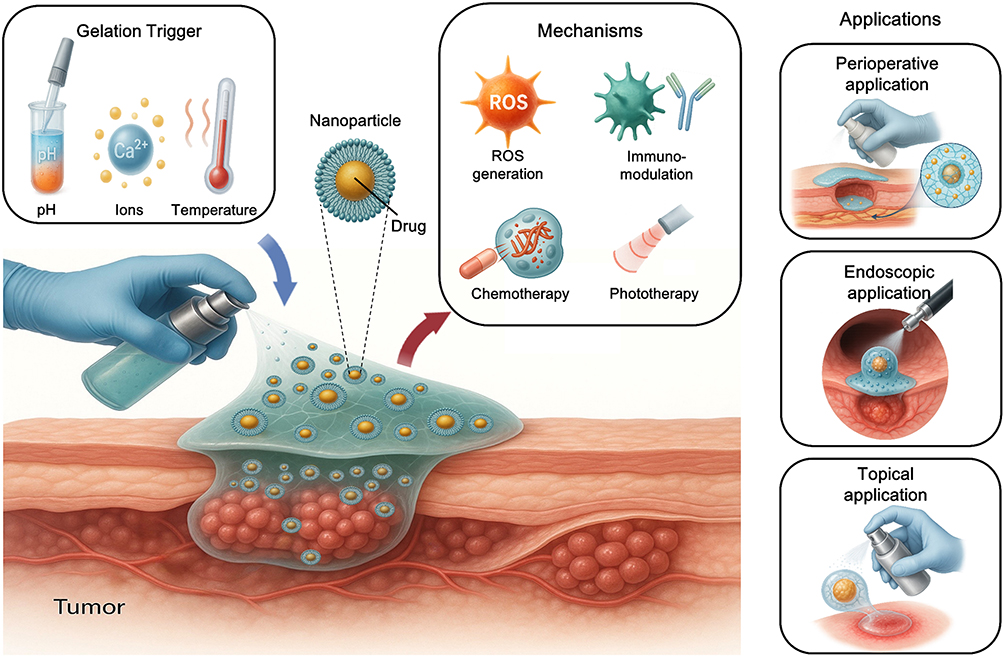 |
Figure 1 Schematic illustration of sprayable nanoparticle–hydrogel systems for localized cancer therapy. |
Design Principles of Sprayable Hydrogel Systems
Key Material Requirements
The design of sprayable hydrogel systems for oncologic applications requires careful consideration of several fundamental material properties to ensure functional performance and clinical translation. Biocompatibility is a primary prerequisite, as the hydrogel must not elicit significant inflammatory or toxic responses when applied to resection cavities, mucosal surfaces, or serosal tissues. This applies to both the bulk matrix and any incorporated therapeutic or diagnostic agents. Materials such as hyaluronic acid, gelatin, chitosan, alginate, and synthetic polymers including poly(ethylene glycol) (PEG) and poly(N-isopropylacrylamide) (PNIPAm) have been widely explored due to their favorable safety profiles, tunable degradation, and history of regulatory acceptance. The degradation products should be non-toxic and readily cleared through physiological pathways to avoid long-term accumulation in the body.
Adhesion to the target tissue is another essential property, especially in post-surgical contexts where surfaces are irregular, moist, and covered with biological fluids. Strong adhesion ensures that the hydrogel remains localized, forming a physical barrier to tumor cell dissemination and preventing premature loss of therapeutic agents.20 Strategies to enhance adhesion include catechol group modification inspired by mussel adhesive proteins, aldehyde–amine coupling to form Schiff base linkages, and the use of bioadhesive polymers.21 Adhesion must be balanced with reversibility where necessary, to prevent excessive tissue trauma upon degradation or removal.
Gelation kinetics are equally critical. The precursor solution must remain in a low-viscosity, sprayable state during application, but transition into a stable gel once deposited, even under challenging surgical conditions. Slow gelation risks precursor loss or dilution, whereas overly rapid gelation may cause clogging and uneven coverage. Optimal kinetics are achieved by tuning polymer concentration, crosslinker reactivity, and environmental triggers such as temperature or pH.22 Sprayability itself depends on rheology, device design, and formulation stability. The precursor should exhibit shear-thinning behavior for smooth extrusion, followed by rapid viscosity recovery after deposition. Formulations must remain stable during storage to prevent premature crosslinking or phase separation, with ready-to-use or easily reconstitutable options preferred in clinical settings. Additional considerations include optical transparency for intraoperative visibility, oxygen and nutrient permeability to support wound healing, and the ability to incorporate and protect nanoscale therapeutic carriers. These factors collectively determine whether a sprayable hydrogel can meet both therapeutic and procedural demands in oncology.
Beyond these macroscopic properties, experimental considerations such as polymer–drug compatibility, cytocompatibility testing, and nanoparticle stability during gelation also play pivotal roles.23 These evaluations help identify hidden risks-such as drug precipitation, nanoparticle aggregation, or unexpected cellular responses-that must be addressed early to ensure reliable therapeutic performance.
While these material parameters are often discussed independently, their practical implementation is inherently interconnected and must be optimized as a coupled design space. For example, enhancing tissue adhesion through catechol modification often accelerates oxidative crosslinking, which can shorten gelation time and consequently affect sprayability by increasing the risk of nozzle clogging.24 Similarly, increasing polymer concentration can improve mechanical robustness and drug retention, but may compromise biocompatibility or reduce shear-thinning behavior needed for smooth aerosolization.25,26 Fast gelation promotes retention on moist or vertical surgical surfaces, yet overly rapid network formation may impair uniform coating or lead to heterogeneous drug distribution. Conversely, slower gelation enhances coatability but increases the likelihood of precursor runoff in highly exudative environments. These interdependencies highlight that material design requires navigating intrinsic trade-offs between adhesion, gelation kinetics, mechanical integrity, and sprayability.
Modes of in Situ Gelation
Sprayable hydrogels are typically applied in a liquid or semi-liquid precursor state and undergo in situ gelation upon contact with the target surface. This transformation can be driven by various physical or chemical mechanisms, each with advantages and limitations. Ionic crosslinking is well-established, particularly for naturally derived polymers such as alginate and gellan gum. Multivalent cations diffuse into the polymer network, forming ionic bridges that induce rapid gelation under mild conditions. While this approach offers speed and biocompatibility, the resulting gels can be sensitive to ionic strength and may lack long-term mechanical stability.
Thermoresponsive gelation relies on polymers that undergo sol–gel transition upon temperature change, often triggered by the shift from ambient to body temperature.27 Poloxamers and PNIPAm derivatives exemplify this category, enabling minimally invasive delivery as a cold liquid that gels upon warming. This method avoids additional crosslinking agents and conforms well to complex tissue geometries, although thermal fluctuations can influence stability.28
Enzymatic crosslinking uses enzymes such as horseradish peroxidase or transglutaminase to catalyze covalent bond formation between polymer chains.29 These reactions occur under physiologically compatible conditions and allow precise control over gelation rates, but enzyme stability, immunogenicity, and co-substrate requirements can complicate formulation.
Self-gelling systems form gels spontaneously through intrinsic interactions like hydrophobic association, hydrogen bonding, or host–guest recognition. These eliminate the need for secondary triggers and simplify application, but ensuring reproducibility in varied environments is challenging.30 In many advanced designs, multiple gelation modes are combined to balance rapid setting, mechanical strength, and sustained stability.
Spray Technologies and Administration Routes
The translation of sprayable hydrogels into clinical oncology depends on effective delivery technologies and administration routes that enable uniform deposition. Manual spray devices, such as dual-syringe applicators or hand-held atomizers, are widely used in open surgery, offering direct control of spray rate and coverage. Components can be kept separate until application to prevent premature gelation, with mixing occurring at the nozzle or on the tissue surface.31
CO2-driven aerosolization produces fine mists capable of uniformly coating large or irregular surfaces, making it well-suited for minimally invasive or laparoscopic surgeries. This method can be combined with temperature or pH control to trigger gelation immediately after deposition, though viscosity optimization is essential to avoid clogging and ensure adherence before gelation completes.32
Endoscopic application extends the reach of sprayable hydrogels to internal mucosal surfaces such as the gastrointestinal or respiratory tracts. Delivery through catheters or specialized spray heads allows targeted therapy under visual guidance, particularly useful for early-stage cancers, precancerous lesions, or post-resection wound protection.33 These formulations require rapid gelation, strong adhesion to moist mucosa, and minimal interference with visualization.
Emerging strategies include robotic-assisted spraying for precision placement in complex anatomical regions and aerosolizable nanogel systems for ultrafine deposition across disseminated surfaces such as those in peritoneal or pleural carcinomatosis. Ultimately, device mechanics, formulation properties, and gelation mechanisms must be co-optimized to achieve effective, safe, and reproducible clinical outcomes.
Recent sprayable hydrogel systems exemplify how device mechanics, formulation properties, and gelation mechanisms are co-optimized to achieve clinically relevant performance. For instance, the CO2-driven UPy-PEG system developed by Braet et al leverages a minimally invasive aerosolization device to uniformly distribute the precursor across complex peritoneal surfaces, while the pH-responsive supramolecular formulation ensures instantaneous gelation upon CO2 exposure and prolonged intraperitoneal retention.34 Similarly, the ICP-loaded HA-based hydrogel reported by Wang et al integrates a shear-thinning, spray-compatible matrix with pH- and NIR-responsive gelation and release mechanisms, enabling sequential chemo-immunotherapeutic activation precisely at the resection margin.35 In the intracavitary GBM setting, the pectin–Ca2+ system by McCrorie et al3 exemplifies co-optimization through a hand-held dual-spray applicator that prevents premature mixing, a bioadhesive polymer network that conforms to irregular brain cavities, and ion-triggered gelation matched to cerebrospinal fluid composition. Together, these examples demonstrate that clinical performance arises not from isolated formulation choices but from deliberate integration of delivery device design, rheological tuning, and environment-specific gelation chemistry.
Classification Strategies for Sprayable Hydrogel Formulations
Sprayable hydrogel systems for oncology can be systematically categorized based on multiple criteria, each reflecting distinct therapeutic goals, compositional features, and modes of action. Such classification enables a structured understanding of the diversity in formulation strategies and facilitates rational selection or design for specific clinical scenarios. Four primary classification axes—therapeutic mechanism, material type, clinical application context, and responsiveness—are commonly employed in the literature, and each offers unique insights into the potential and limitations of the systems (Figure 2).
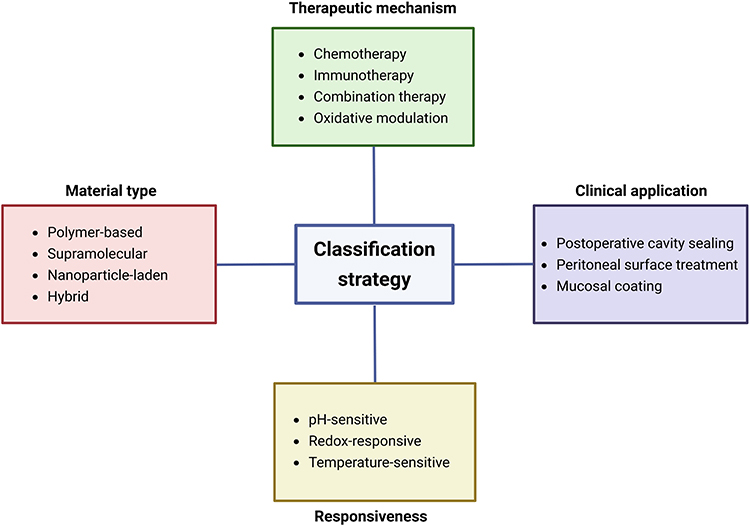 |
Figure 2 Classification strategies for sprayable hydrogel formulations. |
By Therapeutic Mechanism
Sprayable hydrogels can be grouped into those designed for chemotherapy, immunotherapy, combination therapy, and oxidative modulation. Chemotherapy-oriented systems primarily focus on the localized delivery of cytotoxic agents to eradicate residual tumor cells after surgical resection, minimizing systemic exposure and off-target toxicity.36 These hydrogels often incorporate hydrophobic or hydrophilic small-molecule drugs in a sustained-release matrix, allowing for extended exposure of the surgical cavity to therapeutic concentrations. Immunotherapy-based systems, on the other hand, are engineered to modulate the tumor immune microenvironment through the delivery of immune checkpoint inhibitors, cytokines, or tumor-associated antigens.37 Such hydrogels frequently aim to stimulate dendritic cell activation, cytotoxic T lymphocyte expansion, and memory T cell formation, thereby inducing durable antitumor immunity. Combination therapy formulations integrate chemotherapeutic and immunotherapeutic components, leveraging the immediate cytotoxic effects of chemotherapy alongside the longer-term immune priming provided by immunomodulators.38 Oxidative modulation represents a more specialized category, wherein the hydrogel either generates ROS to induce tumor cell apoptosis or scavenges ROS to mitigate oxidative stress in tissues, thus aiding tissue repair while exerting antitumor effects. The therapeutic mechanism-based classification is particularly useful for mapping hydrogel formulations to specific oncological needs, such as immediate tumor clearance versus long-term immune surveillance.
By Material Type
Sprayable hydrogels are differentiated into polymer-based, supramolecular, nanoparticle-laden, and hybrid systems. Polymer-based systems typically utilize natural or synthetic macromolecules such as chitosan, alginate, hyaluronic acid, PEG, or poloxamers, which can form stable gels upon exposure to physiological conditions.39–43 These polymers provide tunable mechanical properties, biodegradability, and biocompatibility, making them suitable for diverse anatomical sites. Supramolecular hydrogels rely on non-covalent interactions—such as hydrogen bonding, host–guest inclusion complexes, or π–π stacking—for network formation, often enabling reversible gelation and responsiveness to environmental cues. Nanoparticle-laden systems incorporate nanostructures such as liposomes, polymeric micelles, mesoporous silica nanoparticles, or metal-based nanocarriers into the hydrogel matrix.44 This design allows for co-delivery of multiple agents with distinct release profiles and offers additional functionalities, such as photothermal or photodynamic effects. Hybrid systems combine elements of the above categories, for instance embedding nanoparticles within a supramolecular polymer matrix, thus integrating the advantages of multiple material classes. Classifying by material type is critical for understanding not only the performance characteristics of the hydrogel but also its compatibility with specific therapeutic payloads and administration methods.
By Clinical Application Context
Sprayable hydrogels can be tailored for postoperative cavity sealing, peritoneal surface treatment, or mucosal coating. Postoperative cavity sealing refers to the use of hydrogels to fill or line the surgical bed after tumor excision, aiming to prevent local recurrence by eradicating microscopic residual disease and providing a physical barrier against tumor cell infiltration.45 In peritoneal surface treatment, the hydrogel is designed to uniformly coat the peritoneal cavity, often using spray or aerosolized delivery methods such as CO2-driven nebulization. This approach is particularly relevant for peritoneal metastases, where diffuse microscopic lesions are inaccessible to conventional surgical removal. Mucosal coating hydrogels are applied to epithelial surfaces such as those in the oral cavity or gastrointestinal tract, creating a protective layer that can deliver therapeutic agents for cancer prevention or early-stage treatment of localized lesions.46,47 Classification by application context is directly linked to the choice of delivery device, spray characteristics, and gelation kinetics, as these parameters must be optimized for the anatomical site.
By Responsiveness
Sprayable hydrogels are categorized as pH-sensitive, redox-responsive, or temperature-sensitive systems, depending on their ability to undergo structural or functional changes in response to specific stimuli in the TME. pH-sensitive hydrogels exploit the acidic conditions of tumor tissue to trigger drug release or gel degradation, ensuring site-specific therapeutic activation.48 Redox-responsive systems utilize the elevated glutathione concentrations or ROS levels in tumor cells to initiate cleavage of disulfide bonds or other redox-sensitive linkers, enabling controlled payload release. Temperature-sensitive hydrogels typically remain in a liquid state at ambient temperature but undergo rapid gelation at body temperature, a property that facilitates minimally invasive administration while ensuring retention at the target site.49 Responsiveness-based classification is especially valuable for designing intelligent systems capable of on-demand therapeutic release, thereby maximizing efficacy and minimizing off-target effects.
In practice, most sprayable hydrogel formulations cannot be strictly confined to a single classification category; instead, they often embody multiple attributes from different axes.50 For example, a nanoparticle-laden hydrogel for postoperative cavity sealing may also be thermoresponsive and designed for combination chemo-immunotherapy. This multidimensional nature underscores the versatility of sprayable hydrogels and highlights the importance of an integrated classification approach that considers therapeutic mechanism, material composition, application context, and responsiveness collectively. Such a framework not only aids in systematic literature analysis but also provides a rational basis for the future design and clinical translation of advanced sprayable hydrogel systems in oncology.51
Cross-Category or Hybrid Sprayable Hydrogel Systems
Although the above framework organizes sprayable hydrogels along therapeutic mechanism, material type, clinical application, and responsiveness, a growing number of state-of-the-art systems inherently span multiple categories. Such hybrid systems demonstrate the design flexibility and modularity of nanoscale sprayable hydrogels, and cannot be strictly confined to a single classification axis.
Representative examples of such cross-category designs further highlight the multidimensional nature of sprayable hydrogel systems. For instance, Wang et al developed the CT–CS–ZIF@CIP sprayable hydrogel employs a photocurable carboxymethyl chitosan–glycol glycidyl acrylate matrix that encapsulates ciprofloxacin-loaded ZIF-8 metal–organic framework nanoparticles together with Cu2Se photothermal agents.52 This multi-component architecture enables synergistic photothermal and chemotherapeutic activity through the integration of NIR-responsive Cu2Se nanoparticles and pH-degradable ZIF-8 carriers, while the photocurable CS-based network supports conformal spray deposition and rapid in situ crosslinking. Through the deliberate combination of polymeric scaffolds, MOF nanocarriers, and inorganic photothermal agents, the formulation simultaneously spans therapeutic mechanism, material composition, responsiveness, and application context. Likewise, the pH-responsive mupirocin-loaded hybrid nanoparticle system formulated within a hydrogel and film-forming spray merges polymeric networks with hybrid nanocarriers to achieve environment-triggered antibacterial activity and conformal coating of irregular wound surfaces.53 By combining multi-component material design, stimuli-responsive drug release, and spray-enabled in situ deposition, these systems exemplify sprayable hydrogels that cannot be adequately classified within a single axis and instead occupy multidimensional positions across the proposed framework.
These hybrid formulations demonstrate that contemporary sprayable hydrogels frequently span multiple design axes at once integrating therapeutic mechanisms, material architectures, and stimuli-responsive features, and in some cases extending into distinct clinical application contexts. Their multidimensional characteristics clearly illustrate why strict single-axis classification is insufficient and highlight the versatility and integrative design logic that define many state-of-the-art sprayable hydrogel systems.
Applications in Cancer Therapy
Cancer types differ markedly in their TMEs, anatomical constraints, and postoperative physiological conditions, and these variations fundamentally dictate the design logic of sprayable hydrogel systems. Differences in acidity, redox balance, enzymatic activity, vascularity, tissue stiffness, cavity geometry, and wound exudate profiles directly influence the selection of hydrogel triggering mechanisms, material compositions, adhesion strategies, and drug-release behaviors. Consequently, effective translation requires a tumor-specific design rationale in which the hydrogel’s gelation mode, mechanical properties, and degradation profile are matched to the unique challenges of each surgical site. In the following subsections, each tumor type is analyzed through this lens—linking its distinct TME characteristics and surgical constraints to the hydrogel formulations employed, thereby tightly integrating design principles with clinical application (Table 1).
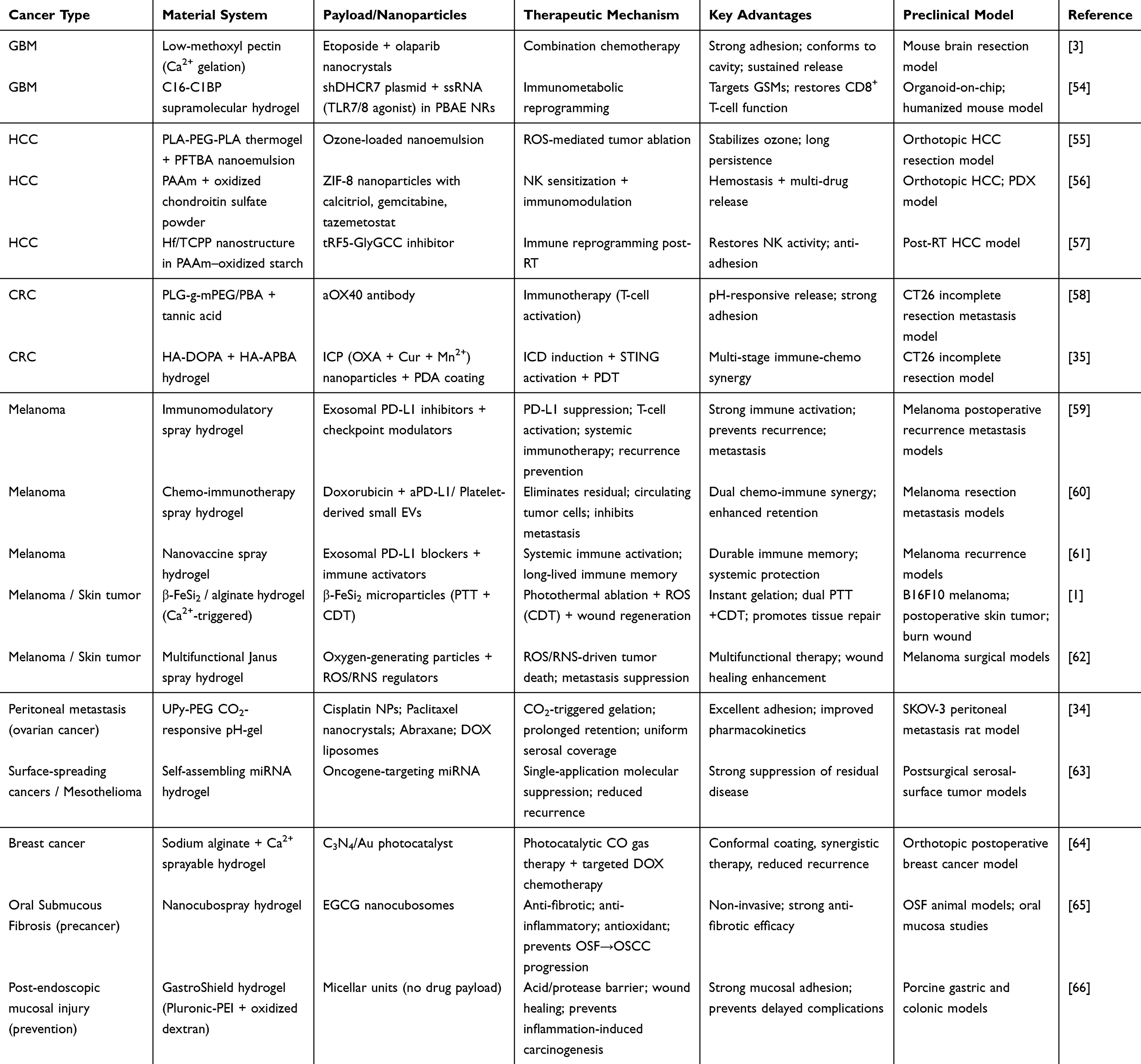 |
Table 1 Overview of Nanoparticle-Loaded Sprayable Hydrogel Systems by Cancer Type: Materials, Payloads, Mechanisms of Action, and Preclinical Models |
Brain Tumors
Glioblastoma multiforme (GBM) is the most aggressive primary brain tumor in adults, characterized by highly infiltrative growth, intrinsic therapeutic resistance, and a dismal prognosis. Despite maximal surgical resection followed by radiotherapy and temozolomide-based chemotherapy, the median overall survival remains approximately 14.6 months, and local recurrence is nearly inevitable.67 Complete resection is rarely achievable due to microscopic invasion into surrounding brain tissue, and residual tumor cells along the surgical cavity margin frequently seed early relapse. Moreover, the blood–brain barrier (BBB) significantly limits systemic drug penetration into the postoperative cavity, while systemic therapy carries a risk of toxicity. These challenges have driven interest in sprayable hydrogel-based local drug delivery systems that can conformally coat the irregular resection cavity, provide sustained local release of therapeutic agents, and potentially prevent tumor recurrence without systemic side effects.68
McCrorie et al developed a bioadhesive sprayable hydrogel designed for the local delivery of etoposide and olaparib to suppress postoperative GBM recurrence. Etoposide inhibits topoisomerase II to induce DNA double-strand breaks, while olaparib inhibits poly(ADP-ribose) polymerase (PARP) to block DNA repair, creating a synergistic cytotoxic effect against residual tumor cells. The team prepared high drug-loading nanocrystals of each drug, surface-coated with poly(lactic acid) (PLA)-PEG to enhance stability and reduce aggregation, yielding an average particle size of approximately 70 nm. The nanocrystals demonstrated stability in phosphate buffered saline (PBS), Dulbecco’s Modified Eagle Medium (DMEM), and artificial cerebrospinal fluid (aCSF) for at least 24 hours and released over 80% of their payload within 24 hours, achieving near-complete release by 48 hours. Olaparib exhibited slightly delayed release due to partial retention within the hydrogel matrix. The hydrogel matrix was formulated with low-methoxyl pectin, selected for its bioadhesive properties and calcium-induced gelation. Pectin transitions to a gel in the presence of 1.5–2 mM Ca2⁺, which mimics physiological brain conditions. This formulation remains liquid at room temperature for easy spraying and rapidly gels upon contact with the resection cavity, conforming to the irregular brain surface. Ex vivo testing on porcine brain tissue demonstrated uniform coating of the cavity wall, and Cy5-labeled nanocrystals diffused up to ~1.5 cm from the spray site. In vivo testing in mouse brains revealed no weight loss, behavioral abnormalities, or local inflammation on hematoxylin and eosin (H&E) staining, confirming high biocompatibility. This study demonstrates that a sprayable hydrogel can locally deliver combination chemotherapy to the postoperative GBM cavity, achieving conformal coverage and sustained release to target residual tumor cells while minimizing systemic toxicity.3
Dong et al reported a complementary nanoregulator-encased sprayable hydrogel designed to reprogram the tumor immune microenvironment after GBM surgery. The study focused on glioma-supportive macrophages (GSMs), a population of tumor-associated macrophages (TAMs) that promote tumor growth and immune evasion. GSMs exhibit high expression of 7-dehydrocholesterol reductase (DHCR7) and enhanced cholesterol synthesis and efflux, supplying exogenous cholesterol to tumor cells and contributing to CD8⁺ T-cell exhaustion. This immune-suppressive environment facilitates local recurrence and resistance to immunotherapy. To counteract this, the authors designed a nanoregulator (NR) carrying short hairpin RNA targeting DHCR7 (shDHCR7) plasmid to inhibit cholesterol metabolism and Toll-like receptor 7/8 (TLR7/8) agonistic single-stranded RNA (ssRNA) to stimulate immune activation. The NR was constructed using a Poly-β-amino-esters (PBAE)-based, biodegradable polymeric carrier optimized for uptake by GSMs, ensuring selective uptake and glutathione-sensitive release of the payload. The NR was encapsulated in a C16-C1BP supramolecular hydrogel, which rapidly forms a fibrous gel upon contact with moisture. When sprayed into the surgical cavity, the hydrogel adheres to irregular resection margins, providing sustained local release for over two weeks.69 In vitro and organoid-on-chip models demonstrated that shDHCR7 NRs reduced cholesterol efflux from GSMs, decreased programmed cell death protein 1 (PD-1) and lymphocyte-activation gene 3 (LAG3) expression on CD8⁺ T cells, and restored IFN-γ production, alleviating T-cell exhaustion. The combination of shDHCR7 and ssRNA NRs polarized GSMs toward a pro-inflammatory, tumor-suppressive phenotype and increased tumor cell apoptosis in organoid models. In vivo, intracavitary spraying of the NR hydrogel after tumor resection resulted in enhanced CD8⁺ T-cell activation, reduced regulatory T-cell (Treg) and GSM populations, significant suppression of local recurrence, and prolonged survival in murine models. In humanized mouse models implanted with patient-derived organoids, the treatment similarly induced tumor cell apoptosis and extended survival without causing weight loss or neurological toxicity. This study demonstrates that locally delivered immunometabolic reprogramming via a sprayable hydrogel can effectively suppress postoperative GBM recurrence by targeting macrophage-driven immune suppression.54
Together, these two studies illustrate complementary approaches for sprayable hydrogel applications in postoperative GBM therapy.70 McCrorie et al provide a strategy based on direct cytotoxicity through localized delivery of dual chemotherapeutics, leveraging bioadhesive hydrogel properties for conformal cavity coverage and sustained release. Dong et al present an immunometabolic reprogramming strategy, targeting the cholesterol-driven immune suppression mediated by GSMs to restore anti-tumor immunity. Within the classification framework introduced earlier, the McCrorie et al system represents a polymer-based, chemotherapy-oriented formulation designed for postoperative cavity sealing, with calcium-triggered in situ gelation serving as a key responsiveness feature. In contrast, the Dong et al platform exemplifies a supramolecular–nanoparticle hybrid system that operates through immunotherapy and metabolic reprogramming, tailored for intracavitary immune modulation and incorporating moisture-induced self-assembly and GSH-responsive payload release. Both systems share critical attributes: rapid in situ gelation, strong tissue adhesion, localized payload retention, and the ability to overcome the limitations of systemic delivery across the BBB. These studies underscore the potential of sprayable hydrogels as versatile postoperative platforms capable of integrating cytotoxic and immunomodulatory functions for precision GBM management.71,72 Future directions include the development of multifunctional formulations, long-term safety evaluation, and optimization of clinically compatible spraying devices to enable translation into neurosurgical practice.73
Hepatocellular Carcinoma (HCC)
Hepatocellular carcinoma (HCC) is one of the most challenging malignancies to manage postoperatively, with recurrence observed in over half of patients within two years after hepatectomy. Local recurrence is mainly driven by microscopic residual tumor cells and the immunosuppressive TME. Systemic chemotherapy and immunotherapy remain limited by poor drug penetration into the liver, systemic toxicity, and suboptimal modulation of the local TME.74 Sprayable hydrogels, which can be applied directly to the surgical bed immediately after resection, have emerged as promising local adjuvant therapies to prevent postoperative recurrence. Recent studies highlight three complementary strategies—chemical cytotoxicity, immune sensitization, and immune microenvironment reprogramming—that illustrate the versatility of sprayable hydrogel platforms in HCC management.75
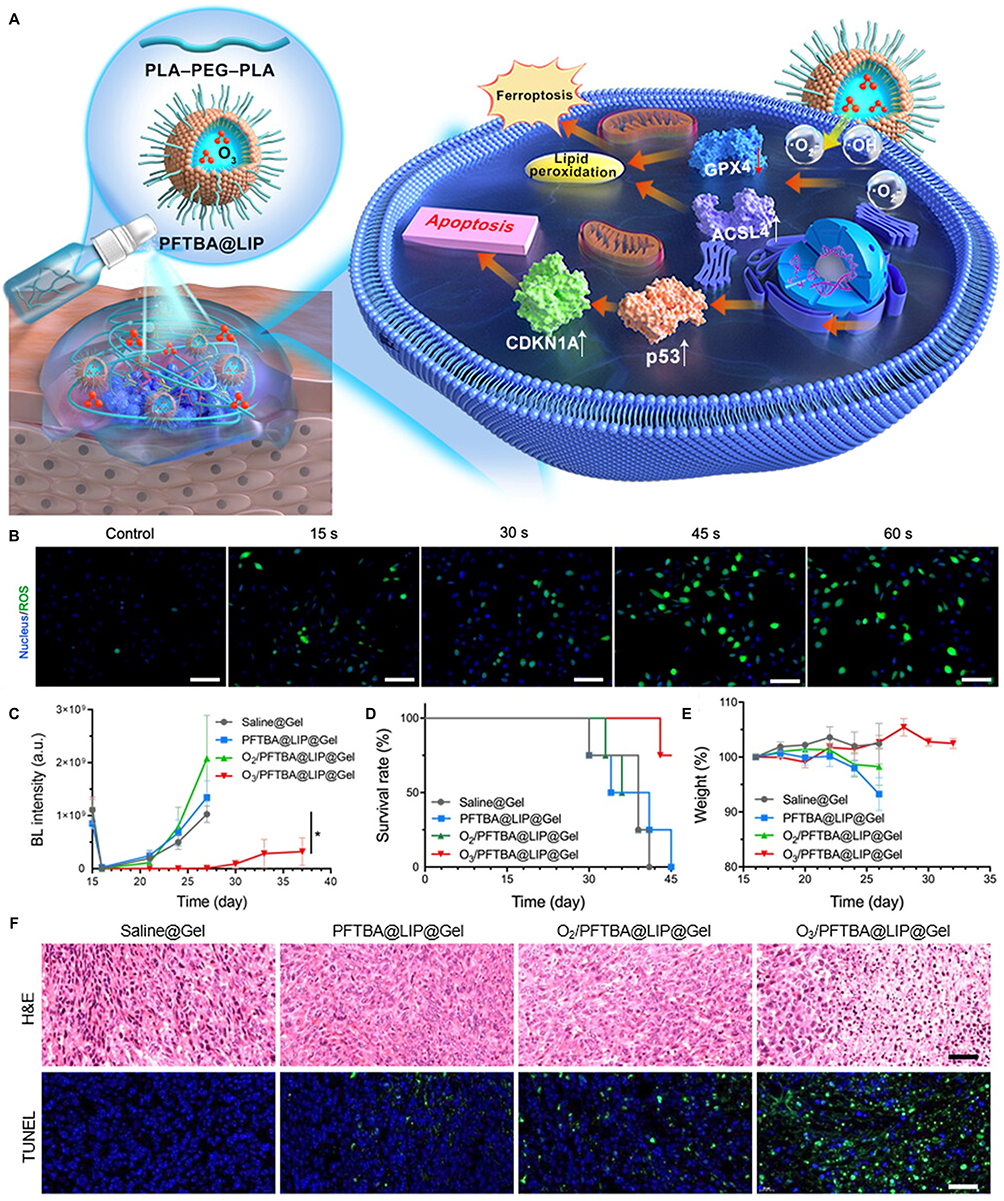 |
Figure 3 Therapeutic efficacy of thermoresponsive ozone-enriched spray gel against postsurgical hepatocellular carcinoma. (A) Schematic illustration of thermoresponsive ozone-enriched spray gel for postsurgical HCC treatment via ferroptosis and apoptosis (white arrows indicate increase; red arrows indicate decrease). (B) ROS staining of HuH-7 cells treated with O3/PFTBA@LIP of different O3 charging times (scale bar: 100 μm). (C) Bioluminescence intensity of tumor sites in HuH-7-Luc mice. (D) Survival rates of mice within 30 days. (E) Body weight changes of treated mice. (F) H&E staining of tumor tissue at day 30 (scale bar: 80 μm), and TUNEL staining of tumor tissue at day 25 (scale bar: 40 μm). Data are means ± SD *P < 0.05. Reprinted with permission from Zhang et al. Copyright 2023 American Chemical Society.55 |
Zhang et al developed a thermoresponsive ozone-enriched spray gel designed to induce local cytotoxicity through ROS generation (Figure 3). The system consists of a perfluorotributylamine (PFTBA)-based nanoemulsion capable of dissolving ozone to enhance its stability, incorporated into a PLA-PEG-PLA thermosensitive hydrogel. The formulation remains in a liquid state at room temperature, allowing facile spraying onto the resection surface, and rapidly gels at body temperature to conform to the surgical cavity. PFTBA improves the solubility of both oxygen and ozone, allowing the otherwise short-lived gas to remain active for local therapy and stable during storage for up to 30 days. In vitro studies using Huh-7 hepatoma cells demonstrated robust ROS generation, mitochondrial damage, and inhibition of cell migration upon exposure to the ozone-loaded hydrogel.76 RNA sequencing and protein analysis revealed simultaneous activation of ferroptosis and apoptosis pathways, characterized by decreased glutathione peroxidase 4 (GPX4) expression, increased acyl-CoA synthetase long-chain family member 4 (ACSL4), and enhanced lipid peroxidation and p53 pathway activation was also observed. In an orthotopic tumor resection mouse model, local spraying of the hydrogel effectively suppressed tumor recurrence and significantly prolonged survival. Histological analysis with H&E and terminal deoxynucleotidyl transferase dUTP nick-end labeling (TUNEL) staining confirmed extensive tumor cell death, and no systemic toxicity was detected by blood tests or organ histology. This study demonstrates that sprayable hydrogels can stabilize and deliver otherwise unstable gaseous therapeutics, achieving potent local tumor ablation and postoperative recurrence prevention.55,77,78
Cheng et al introduced a self-gelling sprayable powder hydrogel designed to sensitize adoptive natural killer (NK) cell therapy and simultaneously provide local hemostasis. The formulation, referred to as CGT@POZ, is composed of a poly(acrylamide) (PAAm)-based structural hydrogel matrix combined with oxidized chondroitin sulfate (OCS) for wet tissue adhesion. ZIF-8 nanoparticles encapsulate three bioactive agents: calcitriol, which inhibits the Runx2–SerpinB9 axis in liver cancer stem cells (LCSCs) to restore NK susceptibility; gemcitabine, which selectively depletes myeloid-derived suppressor cells (MDSCs); and tazemetostat, which suppresses enhancer of zeste homolog 2 (EZH2) to increase C-X-C motif chemokine ligand 10 (CXCL10) expression and enhance NK cell homing. Upon spraying onto the resection surface, the powder absorbs physiological fluids, rapidly gels, and adheres strongly to the tissue, providing immediate hemostasis and sustained local release of the three drugs over several weeks.79 In vitro, the hydrogel increased NK cell cytotoxicity against epithelial cell adhesion molecule (EpCAM)high LCSCs, decreased MDSC recruitment, and induced a marked elevation in CXCL10. In orthotopic HCC and patient-derived xenograft (PDX) models, CGT@POZ alone suppressed recurrence and prolonged survival, while combination with chimeric antigen receptor-natural killer cell (CAR-NK) cell therapy achieved the greatest therapeutic benefit. Treated tumors exhibited enhanced NK infiltration and activation, evidenced by increased granzyme B and TNF-γ expression. Blood chemistry and organ histology showed no systemic toxicity, and the powder format was compatible with both open and laparoscopic surgeries. This work highlights the potential of sprayable self-gelling powders to serve as multifunctional local adjuvants that combine immunomodulation, targeted drug delivery, and surgical hemostasis.56,80
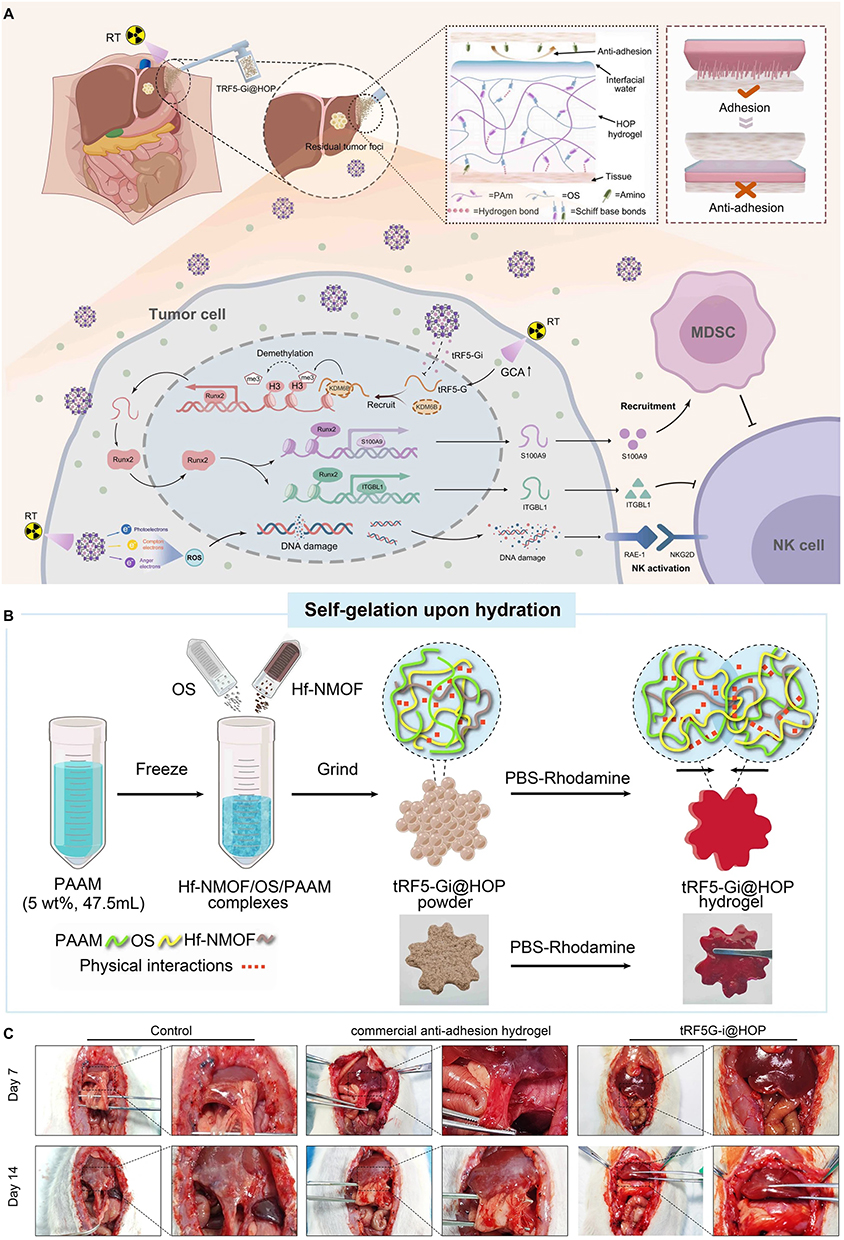 |
Figure 4 Radiotherapy combined with tRF5-Gi@HOP powder for postoperative HCC treatment. (A) Schematic illustration of tRF5-Gi@HOP powder enhancing NK cell-mediated antitumor immunity and preventing postoperative recurrence. (B) The diagram summarizing the process of fabrication of tRF5-Gi@HOP powder and its hydrogel. (C) Anti-adhesion performance of tRF5-Gi@HOP powder in a rat hepatectomy-induced adhesion models in different groups. Reprinted with permission from Gong et al. Copyright 2023 American Chemical Society.57 |
Gong et al developed a self-gelation powder hydrogel encapsulating a tRF5-GlyGCC inhibitor as a strategy to restore NK-mediated immunity in combination with radiotherapy (Figure 4). The study first elucidated a mechanistic pathway in which postoperative radiotherapy elevates glycocholic acid (GCA) levels, inducing tRF5-GlyGCC expression. This small RNA interacts with the Runx2-KDM6B axis, promoting ITGBL1 and S100A9 expression, which in turn suppresses NK cell cytotoxicity and recruits MDSCs to the tumor bed. To counteract this pathway, the team designed a hydrogel powder (tRF5-Gi@HOP) composed of hafnium ion (Hf4 +)/tetrakis (4-carboxyphenyl) porphyrin (TCPP) (Hf/TCPP)-based nanostructures carrying the tRF5-GlyGCC inhibitor, embedded in a PAAm and oxidized starch matrix that self-gels upon contact with tissue fluids. When sprayed onto the hepatic resection margin, the powder rapidly formed an adherent gel with self-healing properties, enabling prolonged local release of the inhibitor. In vivo, combination therapy with radiotherapy significantly increased NK infiltration and activation (granzyme B and IFN-γ expression), reduced MDSC prevalence, and suppressed tumor recurrence, resulting in improved survival.81 An additional benefit was the reduction of postoperative peritoneal adhesions, which is advantageous for surgical recovery. Blood biochemistry and histological assessments confirmed the absence of systemic toxicity. This study demonstrates that sprayable self-gelling powders can be engineered for precise immunometabolic intervention, synergizing with radiotherapy to prevent HCC recurrence by restoring local NK immunity.57
Collectively, these three studies illustrate the multifaceted capabilities of sprayable hydrogel systems for postoperative HCC therapy. Zhang et al focused on localized ROS-mediated tumor ablation using an ozone-enriched thermosensitive gel.82 Cheng et al developed a multifunctional self-gelling powder that provides immunomodulation, drug delivery, and hemostasis while sensitizing NK cell therapy. Gong et al introduced an immunoregulatory powder that reprograms the postoperative TME to restore NK activity in combination with radiotherapy.83 Within the classification framework outlined earlier, these platforms span multiple axes in distinct but complementary ways. The ozone-enriched thermogel by Zhang et al represents a thermoresponsive, polymer-based system designed for postoperative cavity sealing, leveraging temperature-triggered sol–gel transition for localized ROS release and ferroptosis induction. The CGT@POZ powder hydrogel developed by Cheng et al exemplifies a hybrid material architecture combining polymer matrices with nanoparticle-laden immunomodulators, functioning within the therapeutic category of immune sensitization and incorporating fluid-induced self-gelation as a key responsiveness feature. In contrast, the tRF5-Gi@HOP system by Gong et al operates as an immunometabolic reprogramming platform, integrating a nanoparticle-enabled inhibitor with a self-gelling polymer network that responds to tissue fluid absorption and radiotherapy-associated biochemical cues to sustain localized release. Despite their distinct mechanisms—direct cytotoxicity, immune sensitization, and immunometabolic reprogramming—all three platforms demonstrated effective suppression of tumor recurrence and significant survival benefits in preclinical models. These findings suggest that sprayable hydrogels can evolve into multifunctional local adjuvants for HCC, bridging surgical oncology with targeted drug delivery and immune modulation. Future translation will require optimization of long-term safety, degradation kinetics, and compatibility with diverse surgical environments, but the current preclinical evidence strongly supports their potential to address the unmet clinical challenge of postoperative HCC recurrence.
Colorectal Cancer
Colorectal cancer (CRC) is a common malignancy with a high risk of local recurrence and distant metastasis even after surgical resection.84 Postoperative recurrence is driven by residual microscopic tumor cells at the resection margin and by the immunosuppressive TME created after surgery.85 Additional challenges include the highly inflamed and exudative postoperative intestinal environment, which can dilute locally applied therapeutics and accelerate their clearance, as well as the complex geometry of the colorectal resection bed that complicates uniform drug deposition. Systemic chemotherapy and immunotherapy have limited efficacy in this setting because drug delivery to the surgical bed is poor and systemic administration is often accompanied by toxicity. Sprayable hydrogels that can be applied intraoperatively to conformally coat the resection surface have emerged as an innovative platform to provide local therapy, modulate the immune response, and potentially induce long-term tumor-specific immunity.86 Two representative studies illustrate distinct but complementary strategies: a dual-functional immunotherapeutic gel designed to alleviate postoperative immune suppression and trigger systemic antitumor immunity, and a hyaluronic acid-based multidrug composite hydrogel that integrates multi-stage immuno-chemotherapy for durable tumor eradication.
Si et al developed an in situ-sprayed dual-functional immunotherapeutic hydrogel (iSGels@aOX40) to prevent local recurrence and peritoneal metastasis following CRC surgery. The design of this system addresses the major challenge of the postoperative TME, which becomes immunosuppressive due to surgical trauma and residual tumor burden, facilitating rapid regrowth and systemic dissemination.87 The hydrogel consists of tannic acid (TA), a natural polyphenol that alleviates inflammation by destabilizing COX-2 mRNA, and a poly(l-glutamic acid) (PLG)-g-mPEG/phenylboronic acid (PBA) backbone that enables rapid gelation through reversible boronate ester bonds. The system incorporates anti-OX40 monoclonal antibody (aOX40) to directly stimulate T-cell activation and inhibit Treg activity, thereby inducing systemic antitumor immunity. When sprayed onto the resection site, the liquid precursor rapidly forms a strong adhesive hydrogel with tissue adhesion up to 6 kPa, conforming to the irregular surgical cavity. The material properties of iSGels@aOX40 were optimized to achieve sustained release and biodegradation under physiologic and tumor-associated conditions. In mildly acidic environments resembling the postoperative tumor bed (pH 6.8), the hydrogel degraded more rapidly, with only 15.6% residual mass after 19 days compared to 30.4% at pH 7.4. The release profile of aOX40 antibody was similarly pH-dependent, reaching 81.1% cumulative release at pH 6.8 over 20 days, while maintaining 45.5% release at pH 7.4. Importantly, the biological activity of the released antibody was preserved due to reversible interactions with TA, which stabilized the protein and allowed its functional recovery in situ. In vitro assessments demonstrated high cytocompatibility of the hydrogel components, with PLG-g-mPEG/PBA scaffolds and iSGels maintaining over 80% cell viability at concentrations up to 1000 μg/mL in CT26 colon cancer cells. Tannic acid exhibited moderate cytotoxicity only at high concentrations, confirming that the gel matrix itself is largely non-toxic. In vivo studies highlighted the robust therapeutic efficacy of this local immunotherapy system. In a subcutaneous incomplete resection model of CT26 tumors, free aOX40 antibody achieved partial tumor suppression, extending median survival to 46 days, while the iSGels@aOX40 group achieved complete local recurrence prevention and 100% survival at 90 days. Histologic analysis revealed enhanced CD4⁺ and CD8⁺ T-cell infiltration, maturation of dendritic cells, and a shift from immunosuppressive to immunostimulatory TME characterized by increased IFN-γ and TNF-α and decreased IL-10. In a peritoneal metastasis model, the treatment achieved 85% tumor suppression rate, reduced M2 macrophage and MDSC populations, and conferred long-term tumor-specific immune memory, as evidenced by resistance to tumor rechallenge in cured mice.88,89 No significant systemic toxicity, weight loss, or organ damage was observed. This study demonstrates that local delivery of an immunostimulatory hydrogel can effectively transform the postoperative immune environment, achieve durable local tumor control, and induce systemic antitumor immunity without systemic side effects.58
Wang et al reported a complementary approach using a sprayable hyaluronic acid-based multidrug composite hydrogel designed to provide ultra-efficient, long-lasting, multi-stage immuno-chemo synergistic therapy for postoperative CRC.90 This system is built upon the concept of eliminating residual tumor cells while simultaneously inducing robust and durable antitumor immunity to prevent recurrence and peritoneal dissemination. The core of the formulation is an infinite coordination polymer (ICP) nanoparticle composed of oxaliplatin (OXA), curcumin (Cur), and Mn2⁺ ions, which together orchestrate a multi-modal antitumor mechanism. OXA induces immunogenic cell death (ICD) through nuclear DNA damage, Cur generates mitochondrial ROS leading to mitochondrial DNA damage and activation of the cGAS- stimulator of interferon genes (STING) pathway, and Mn2⁺ amplifies STING-mediated immune signaling.91 These ICP nanoparticles were subsequently coated with polydopamine (PDA) to provide photothermal capability under 808 nm laser irradiation, prolong drug release, and enhance tissue adhesion. Finally, the nanoparticles were incorporated into a sprayable hyaluronic acid hydrogel composed of HA-DOPA and HA-APBA, which provides strong wet tissue adhesion and pH-responsive, stepwise drug release. The physicochemical characterization of this composite hydrogel revealed that ICP nanoparticles were approximately 18 nm in diameter and increased to 143 nm after PDA coating. Drug release was highly pH-dependent: under physiological conditions (pH 7.4), cumulative release of OXA and Cur after 48 hours was 15% and 12%, respectively, whereas in the mildly acidic tumor environment (pH 5.5) release increased to 79% and 71%, enabling selective activation in the surgical bed. The hydrogel exhibited strong tissue adhesion (3.99 ± 1.32 kPa in porcine skin models) and effective photothermal performance, reaching 56°C within 5 minutes under 808 nm laser irradiation. This combination of adhesion, controlled release, and photothermal responsiveness allows the hydrogel to achieve multi-stage therapeutic effects, including direct tumor cell killing, immunogenic modulation, and enhanced immune memory formation.92 In vitro studies with CT26 CRC cells demonstrated that the combination of ICP@PDA nanoparticles and laser irradiation reduced cell viability to below 10%, and 3D tumor spheroid models showed over 50% growth inhibition.93 ICD markers such as calreticulin (CRT) exposure, HMGB1 release, and ATP secretion were significantly elevated, and activation of the cGAS-STING pathway was confirmed.94 In vivo, the hydrogel adhered to the surgical bed and provided sustained local drug release for over 20 days without causing weight loss, hematologic abnormalities, or organ toxicity.95 In an incomplete resection mouse model, treatment achieved 80-day recurrence-free survival with 100% survival, and a tumor rechallenge experiment confirmed the establishment of long-term immune memory.96 Additionally, peritoneal dissemination was effectively suppressed, highlighting the systemic protective benefit of this local therapy.35,97
Together, these two studies demonstrate how sprayable hydrogel systems can be engineered for postoperative CRC management using distinct but complementary strategies. Si et al provide a platform focused on local immune activation and systemic antitumor immunity through the delivery of an immunostimulatory hydrogel incorporating anti-OX40 antibody and tannic acid. Wang et al present a multistage immuno-chemo approach that combines chemotherapy, ROS-mediated immunogenic modulation, STING pathway activation, and photothermal therapy to achieve ultra-efficient local tumor eradication and long-term protection.98,99 Within the classification framework outlined earlier, the iSGels@aOX40 platform developed by Si et al represents an immunotherapy-oriented system composed of a polymeric boronate-crosslinked hydrogel matrix, designed for postoperative cavity sealing and characterized by pH-responsive degradation and antibody release in the mildly acidic tumor bed. In contrast, the HA-based ICP@PDA composite hydrogel created by Wang et al exemplifies a hybrid material architecture integrating polymer matrices, coordination polymer nanoparticles, and photothermal components to deliver combination immuno-chemotherapy. This system aligns with the clinical application context of postoperative CRC management and incorporates dual responsiveness—pH-triggered drug release and NIR-driven photothermal activation—to enable multi-stage therapeutic engagement. Both platforms exploit the intrinsic advantages of sprayable hydrogels, including rapid in situ gelation, conformal coating of irregular surgical sites, sustained localized release, and minimal systemic exposure.100 These studies underscore the transformative potential of sprayable hydrogel systems as multifunctional postoperative adjuvants for CRC, capable of addressing the dual challenge of immediate local tumor control and durable immunologic protection against recurrence and metastasis.101
Melanoma and Skin Tumors
Melanoma is the most serious type of skin cancer, and surgery is an effective method to treat melanoma.102 However, local recurrence and distant metastasis frequently occur due to the presence of microscopic residual tumor cells and circulating tumor cells (CTCs). Surgical trauma and the associated inflammatory response create an immunosuppressive TME that promotes tumor regrowth.103 Furthermore, the dynamic wound environment of skin—including high protease activity, fluctuating oxygenation, and mechanical stretching—poses additional challenges for maintaining therapeutic concentration and gel stability. Systemic chemotherapy and immune checkpoint inhibitors can provide partial benefit but are limited by systemic toxicity and suboptimal local drug delivery to the surgical bed. To overcome these clinical challenges, sprayable hydrogel-based local therapy has emerged as a promising strategy. These systems conformally coat the irregular resection surface, enable sustained local release of therapeutic agents, minimize systemic exposure, and can stimulate long-term antitumor immune responses.104,105
Chen et al developed an in situ-sprayed immunotherapeutic hydrogel designed to prevent postoperative tumor recurrence and activate systemic immunity.13 The system integrates two key components. First, anti-CD47 (aCD47) antibody-loaded CaCO3 nanoparticles, which gradually dissolve under acidic TME conditions and release the antibody. CD47-SIRPα signaling functions as a “don’t eat me” signal for tumor cells, and blockade with aCD47 restores macrophage phagocytosis and antigen presentation.93 The dissolution of CaCO3 also consumes protons, locally buffering the acidic TME and promoting the polarization of TAMs from the M2 phenotype toward the M1 phenotype. Second, a fibrin-based hydrogel serves as a biocompatible and Food and Drug Administration (FDA)-approved scaffold. Fibrinogen and thrombin solutions are sprayed simultaneously using a dual-cartridge device, rapidly gelling on the surgical bed to form a local drug depot and wound-sealing layer.106 The formulation demonstrated favorable physicochemical and immunological properties. The aCD47@CaCO3 nanoparticles were approximately 100 nm in diameter, at pH 6.5, the CaCO3 core dissolved gradually, resulting in sustained antibody release over several weeks while consuming local H⁺ ions to modulate the TME. In vivo imaging confirmed prolonged retention and release for up to three weeks. Immunological analyses revealed a pronounced reprogramming of the TME: M2-type TAMs (CD206⁺) decreased, M1-type TAMs (CD80+) increased, and pro-inflammatory cytokines such as IL-12 and IFN-γ were upregulated while IL-10 was suppressed.107 Dendritic cell maturation and CD8+ T-cell infiltration were enhanced, while Foxp3+ Tregs were reduced, indicating a shift toward an immunostimulatory environment. Therapeutic efficacy was validated in a B16F10 melanoma model with incomplete tumor resection. Local application of the sprayable hydrogel significantly reduced recurrence rates, and 50% of treated mice survived to 60 days without recurrence. Notably, local therapy alone also inhibited contralateral tumor growth, suggesting that local immune activation expanded to a systemic antitumor response.108 Combination with systemic anti-PD-1 further enhanced both local and distant tumor suppression. Body weight and hematologic parameters remained stable, confirming minimal systemic toxicity. This study demonstrated that a locally applied immunotherapeutic sprayable hydrogel can effectively prevent recurrence, reprogram the TME, and initiate systemic immune responses.59
Zhao et al reported a sprayable chemo-immunotherapy hydrogel designed to simultaneously target residual tumor cells and circulating tumor cells to prevent postoperative recurrence and metastasis. This system combined three essential components. First, platelet-derived small extracellular vesicles (Pex) loaded with doxorubicin (PexD) functioned as a targeted chemotherapeutic platform.109 These vesicles retained key platelet proteins such as P-selectin, CD41, and CD61, enabling selective binding to CD44 on CTCs and residual tumor cells.110 Doxorubicin (DOX) induced ICD, enhancing antigen release and immune activation.111 Second, anti-programmed death-ligand 1 (aPD-L1) antibody was included to locally block PD-1/PD-L1 signaling, reactivating T-cell responses at the surgical bed. Third, a fibrin-based hydrogel was used to generate an in situ depot.112 Thrombin solution containing PexD and fibrinogen solution containing aPD-L1 were co-sprayed, forming a soft, porous hydrogel that adhered to the resection surface and enabled sustained release. The physicochemical evaluation showed that PexD had a diameter of ~157 nm with increased positive surface charge due to DOX loading. The hydrogel exhibited stable rheological properties, with a soft-gel profile (G′ > G″) and a porous 3D network suitable for drug release.113 At pH 6.5, 43.4% of DOX was released within 24 hours, providing TME-responsive delivery. In vitro studies confirmed superior cellular uptake of PexD compared with free DOX and enhanced cytotoxicity, with an IC50 of 0.115 μg/mL versus 0.341 μg/mL for free drug.97 PexD treatment induced hallmark ICD responses, including calreticulin exposure, HMGB1 release, and ATP secretion, and promoted dendritic cell maturation with increased CD80+/CD86+ expression.114 In vivo, this sprayable system achieved three major therapeutic outcomes. First, intravenously administered PexD captured CTCs in circulation and suppressed lung micrometastases.115 Second, in a postsurgical B16F10 incomplete resection model, local spray therapy markedly reduced tumor recurrence, with 50% of mice surviving to day 50.116 The local immune environment was remodeled with increased CD8⁺ T cells and M1-type macrophages and decreased Tregs and M2-type macrophages. Third, local therapy alone suppressed contralateral tumor growth and reduced major organ metastases, with systemic expansion of CD8+ T-cell responses.117 Body weight and organ histology showed no significant toxicity, supporting the safety of this localized approach.118 Overall, this study demonstrated that a sprayable chemo-immunotherapy gel can simultaneously eradicate residual tumor cells, capture CTCs, modulate the local and systemic immune landscape, and induce long-term protective immunity (Figure 5A).60
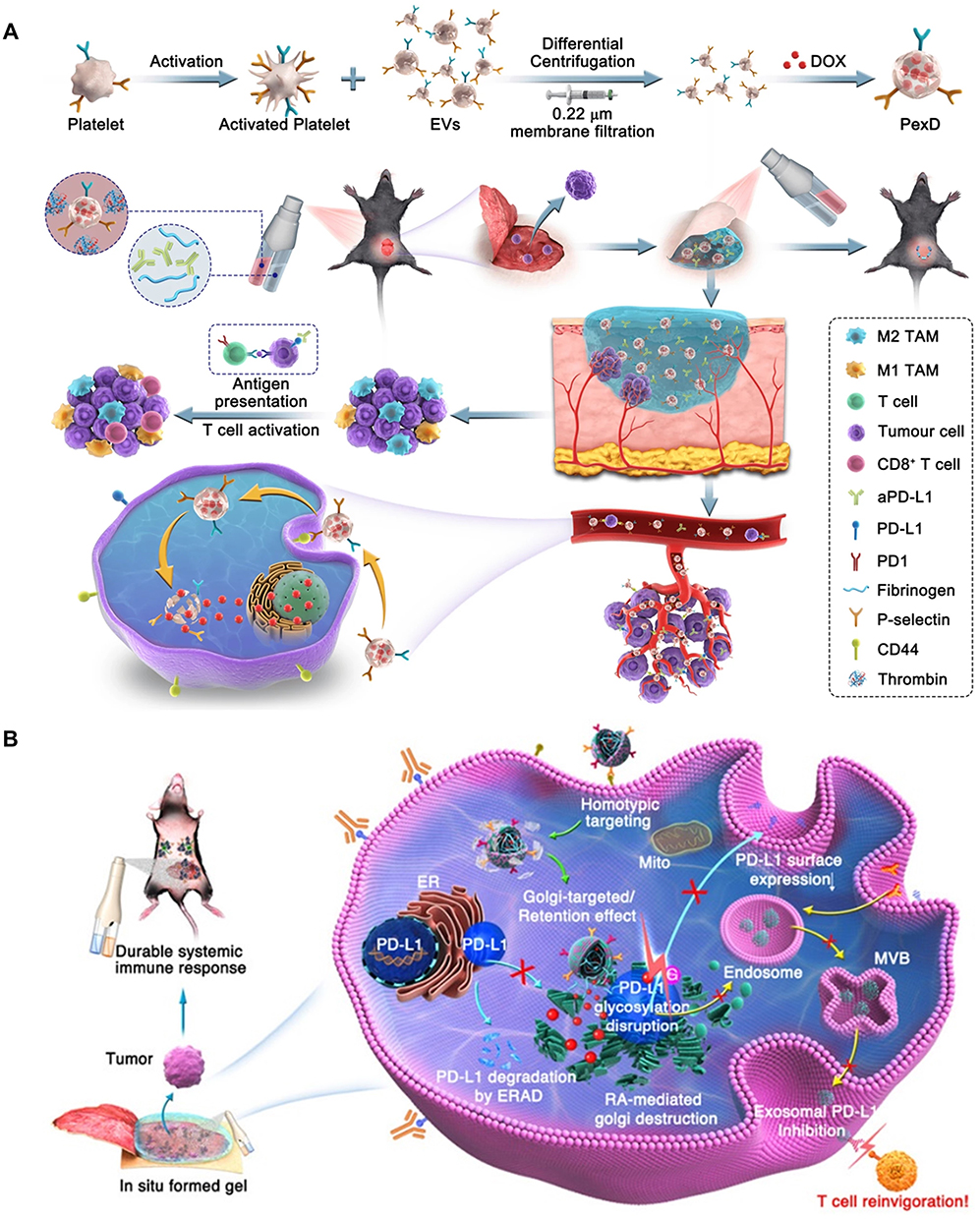 |
Figure 5 Localized sprayable hydrogel strategies in postsurgical melanoma therapy. (A) Sprayable chemo-immunotherapy gel (PexD) releasing aPD-L1 and platelet-derived EVs to prevent tumor recurrence by boosting antigen presentation and T cell activation. (B) Schematic illustration of aPD-L1&GENPs@Gel sprayed onto postsurgical tumor beds, showing GENPs-mediated disruption of PD-L1 glycosylation, ERAD-dependent degradation, and inhibition of exosomal PD-L1–mediated immunosuppression (green arrows: GENPs trafficking to the Golgi and RA release; blue arrows: ERAD-mediated degradation of PD-L1; yellow arrows: inhibition of exosomal PD-L1 secretion and its interaction with T cells). Reprinted with permission from Ye et al and Zhao et al. Copyright 2023 American Chemical Society.60,61 |
Ye et al developed an in situ-sprayed nanovaccine hydrogel designed to prevent postoperative melanoma recurrence and metastasis by simultaneously targeting cell surface and exosomal PD-L1, which are major mediators of immune evasion.119 The platform combined GENPs (Golgi–exosome hybrid membrane-coated poly(lactic-co-glycolic acid) (PLGA) nanoparticles loaded with all-trans retinoic acid) and aPD-L1 antibody, encapsulated within a poly(vinyl alcohol) acetoacetate (PVAA)/chitosan-based sprayable hydrogel that rapidly gels upon application to the surgical cavity. The GENPs were engineered with a PLGA core carrying retinoic acid, which disrupts Golgi function, and a hybrid membrane derived from PD-L1-knockout exosomes and Golgi membranes. This hybrid coating allowed for homotypic targeting to melanoma cells, efficient intracellular delivery, and specific localization to the Golgi apparatus.116 The strategy was designed to disorganize the Golgi structure, suppress exosomal PD-L1 secretion by approximately 40%, and promote the degradation of cellular PD-L1 via ER-associated degradation, collectively overcoming systemic immunosuppression mediated by PD-L1-positive exosomes.120 In vitro studies confirmed the functional performance of GENPs: they showed strong uptake by B16F10 melanoma cells, induced significant Golgi disassembly, and reduced exosome production. Functional immunological assays demonstrated enhanced activation of dendritic cells and increased priming of T cells after exposure to tumor antigens from treated cells.121 The hydrogel served as a local depot, maintaining the retention and controlled release of GENPs and aPD-L1 at the surgical site, reducing the need for systemic dosing and minimizing off-target toxicity.122 In vivo, this nanovaccine hydrogel demonstrated robust local and systemic effects in multiple murine melanoma models. In an incomplete resection model, application of the hydrogel led to marked suppression of local tumor recurrence and extended median survival, with 50% of treated mice surviving up to day 52 without recurrence.123 Histological analysis of the tumor bed revealed dense infiltration of CD8+ cytotoxic T lymphocytes and a significant reduction in Foxp3+ Tregs, indicative of a favorable immunological shift. Importantly, the therapy generated systemic antitumor immunity despite being delivered locally. Contralateral tumors and lung metastasis models showed suppressed growth, reduced metastatic burden, and evidence of effector memory T cell expansion in the spleen, confirming the induction of long-lasting systemic immune responses.111 No significant body weight loss or organ toxicity was observed, underscoring the safety of localized immunotherapy. Overall, this study highlights a rational approach that combines exosomal PD-L1 suppression, checkpoint blockade, and local retention to achieve durable local and systemic antitumor effects, positioning sprayable nanovaccine hydrogels as a potent strategy for postoperative melanoma immunotherapy (Figure 5B).61
Ma et al reported a sprayable β-FeSi2 (FS)/alginate composite hydrogel that integrates tumor ablation and wound healing to address the dual challenges of residual tumor eradication and skin regeneration after surgery for melanoma or other skin tumors.124 The system leveraged FS microparticles embedded in a sodium alginate (SA) hydrogel, which could be instantly cross-linked with calcium ions upon spraying to form a conformal gel coating on irregular wound surfaces. β-FeSi2 served as a multifunctional therapeutic component through its dual role in photothermal therapy (PTT) and chemodynamic therapy (CDT).1 Under 808 nm near-infrared irradiation, FS particles converted light into heat, rapidly increasing the local temperature to ~60°C within 10 minutes, sufficient to ablate residual tumor cells.125 Simultaneously, in the acidic and hydrogen peroxide-rich TME, Fe ions released from FS catalyzed Fenton-like reactions to generate highly reactive hydroxyl radicals (•OH), amplifying oxidative stress to induce tumor cell death.116 The hydrogel also gradually released Fe and Si ions that promoted angiogenesis, enhanced endothelial cell migration, and accelerated tissue regeneration. Extensive in vitro studies confirmed the synergy of PTT and CDT in eliminating melanoma cells.126 Treatment of B16F10 cells with SA-FS hydrogels under NIR irradiation reduced cell viability to approximately 5%, and live/dead staining combined with ROS fluorescent probes revealed extensive apoptosis and ROS accumulation. In 3D tissue-mimicking assays, the hydrogel uniformly coated the tumor surface and maintained its photothermal and catalytic performance after repeated laser exposures.126 In vivo experiments in a postsurgical skin tumor model demonstrated potent therapeutic and regenerative effects. The group treated with SA-FS hydrogel plus NIR irradiation exhibited rapid and complete tumor ablation, with histological analysis confirming full necrosis of residual tumor tissue. Remarkably, the treated wounds exhibited accelerated healing, with near-complete closure within 12 days, re-epithelialization, and new dermis formation.127 Further angiogenesis assays revealed enhanced expression of VEGF, CD31, and HIF-1α-driven signaling in regenerating tissue, correlating with robust neovascularization.128 In a burn wound model, the hydrogel further demonstrated its wound healing potential, achieving full closure within 14 days and promoting the formation of vascularized skin tissue.129 Collectively, this sprayable FS/alginate hydrogel offered a portable, minimally invasive strategy that not only eradicated residual skin tumors through PTT/CDT synergy but also actively facilitated wound regeneration, making it highly promising for postoperative melanoma management and emergency applications in dermatologic oncology.1
Chen et al advanced the concept of multifunctional in situ-sprayed hydrogels by developing an oxygen-actuated Janus therapeutic system that simultaneously targets postoperative melanoma recurrence, metastasis suppression, and wound healing.130 The hydrogel, designated HIL@Z/P/H, incorporated three coordinated therapeutic elements. First, HIL@Z nanoparticles were formulated by loading indocyanine green (ICG) and L-arginine into ZIF-8 particles and coating them with hyaluronic acid for CD44-mediated tumor targeting. Upon 808 nm irradiation, ICG generated ROS, which reacted with L-arginine to produce nitric oxide (NO), leading to the formation of peroxynitrite (ONOO−) and inducing potent oxidative and nitrosative stress to kill residual tumor cells.62 Second, the hydrogel encapsulated photosynthetic cyanobacteria (PCC 7942), which generated oxygen under 635 nm red light, alleviating local hypoxia, enhancing ROS/reactive nitrogen species (RNS) efficacy, and downregulating HIF-1α-mediated pro-metastatic signaling.131 Third, the alginate-calcium matrix ensured rapid in situ gelation, tissue adhesion, and localized retention of therapeutic agents.132 In vitro evaluations confirmed the multifaceted functionality of the hydrogel. ROS, NO, and ONOO− production was robust, accompanied by significant glutathione depletion in B16F10 melanoma cells, resulting in enhanced late apoptosis and necrosis.133 Cellular oxygenation assays using Ru(dpp)3Cl2 showed marked relief of hypoxia in the presence of P/H and red light irradiation. Gene expression analysis revealed suppression of HIF-1α and its downstream targets, including MMP-9 and EPO, along with restoration of E-cadherin, consistent with inhibition of metastasis-associated pathways.134 In vivo, the therapeutic hydrogel demonstrated a remarkable “Janus” effect in murine models.135 Local application of HIL@Z/P/H with dual-wavelength irradiation achieved near-complete suppression of local recurrence, significant reduction of lung metastases, and extended survival, with 80% of mice surviving to day 42. Immunohistochemical analysis of the tumor bed revealed increased infiltration of CD8+ T cells and F4/80+ macrophages, indicating a shift toward an immunostimulatory microenvironment.136 Simultaneously, the hydrogel promoted rapid wound healing, with complete closure and regeneration of hair-bearing skin within 14 days, accompanied by enhanced collagen deposition and expression of angiogenic markers such as CD31 and α-SMA.137 Safety assessments showed minimal systemic toxicity, stable body weight, and no significant histopathological abnormalities in major organs.138 This comprehensive platform thus demonstrated the capacity to integrate tumor ablation, metastasis inhibition, immune modulation, and tissue regeneration within a single sprayable hydrogel system, representing a highly versatile and translational strategy for postoperative melanoma therapy.62
Together, these five studies illustrate the wide-ranging potential of sprayable hydrogel platforms for melanoma and skin tumor management, each addressing the dual imperatives of local tumor control and tissue recovery through distinct mechanisms. Chen et al presented a strategy focused on reprogramming the local immune microenvironment and stimulating systemic immunity, while Zhao et al implemented a combined chemo-immunotherapy approach to eliminate residual and circulating tumor cells and suppress distant metastasis.139 Ye et al achieved systemic immune activation and durable antitumor memory by suppressing exosomal PD-L1 and leveraging checkpoint blockade.61 Ma et al demonstrated that combining photothermal and chemodynamic effects within a portable sprayable hydrogel could eradicate residual tumors while actively promoting wound repair.140 Chen et al delivered a next-generation multifunctional Janus hydrogel that integrated oxygen generation, ROS/RNS-mediated cytotoxicity, metastasis suppression, and regenerative effects.62 Within the classification framework outlined earlier, these formulations collectively occupy multiple design dimensions rather than a single category. The aCD47@CaCO3–fibrin system developed by Chen et al is an immunotherapy-oriented, polymer–inorganic hybrid hydrogel applied to postoperative skin defects, in which pH-responsive CaCO3 dissolution governs sustained antibody release and local buffering of the acidic TME. Zhao’s PexD/aPD-L1–fibrin platform exemplifies a chemo-immunotherapy system that combines nanoparticle-laden vesicles with a protein-based spray gel for postoperative wound coverage, while exploiting TME-responsive DOX release to coordinate local and systemic CTC targeting. The nanovaccine hydrogel reported by Ye et al represents an immunotherapy-focused, nanoparticle-loaded polymeric matrix designed for intracavitary application, using prolonged local retention and controlled release to modulate both cellular and exosomal PD-L1. In contrast, the FS/alginate composite gel by Ma et al integrates a polysaccharide matrix with inorganic microparticles to provide a surface-coating postoperative dressing that is strongly responsive to NIR irradiation and tumor-associated H2O2 and acidity, thereby enabling synergistic photothermal and chemodynamic tumor ablation alongside pro-angiogenic wound repair. Finally, the HIL@Z/P/H Janus hydrogel described by Chen et al constitutes a highly hybrid, multi-stimuli-responsive system in which an alginate–calcium network supports ZIF-8 nanoparticle-mediated chemo-phototherapy and cyanobacteria-derived oxygen generation under dual-wavelength light, situating it at the intersection of combination therapy, complex material design, and responsiveness-based classification. Despite their mechanistic diversity, all platforms exploit the intrinsic advantages of sprayable hydrogels—rapid in situ gelation, conformal coating of complex surgical sites, sustained local release, and minimized systemic exposure—to meet the complex demands of postoperative melanoma therapy. Collectively, these studies support the advancement of sprayable hydrogels as next-generation adjuvant treatments that bridge local tumor eradication, systemic immune engagement, and accelerated wound healing, offering a transformative approach to the management of melanoma and other skin malignancies.141
Surface-Spreading and Serosal Cancers
Surface-spreading and serosal cancers—such as peritoneal metastasis from ovarian, gastric, or colorectal cancer, and pleural dissemination in mesothelioma—pose unique therapeutic challenges. These malignancies propagate across extensive, curved, and fluid-bathed serosal surfaces where complete surgical removal is rarely feasible. The postoperative environment is characterized by constant peritoneal or pleural fluid turnover, limited vascularity, and poor penetration of systemic drugs, all of which restrict effective local retention of therapeutics. Conventional intraperitoneal or intrapleural chemotherapy suffers from rapid clearance, gravity-dependent pooling, and heterogeneous surface coverage. These constraints underscore the need for sprayable or aerosolizable hydrogels that can uniformly coat complex anatomic surfaces, rapidly gel under serosal fluid conditions, and provide prolonged local drug release despite continuous fluid exposure. Such design requirements have motivated the development of supramolecular, peptide-based, and nanoparticle-integrated sprayable hydrogels optimized for serosal delivery.
Braet et al reported the development of a CO2-driven sprayable hydrogel platform for the treatment of peritoneal metastasis in patients with advanced ovarian cancer, where complete surgical resection is often not feasible.34,142 The system is based on pH-sensitive supramolecular ureido-pyrimidinone (UPy)-PEG hydrogel precursors, which undergo in situ gelation upon CO2 exposure due to a pH drop in the pneumoperitoneum. This approach was designed to address the fundamental limitation of conventional intraperitoneal chemotherapy, which suffers from rapid clearance of free drug solutions, limited retention on peritoneal surfaces, and insufficient tumor specificity. The hydrogel is nebulized using a Medspray multi-directional nozzle in combination with electrostatic pressurized intraperitoneal aerosol chemotherapy (ePIPAC), which allows uniform deposition on the peritoneal cavity, including the diaphragmatic dome and recesses, overcoming gravity-driven pooling observed with conventional Capnopen delivery. The UPy-PEG system forms a thin, conformal gel layer that adheres to complex serosal surfaces and enables prolonged local drug retention and sustained release. Indeed, quantitative analyses demonstrated that CO2-driven nebulization resulted in markedly greater intraperitoneal retention of UPy-PEG compared with either direct injection or N2-driven aerosolization. Two hours after IP administration, significantly higher hydrogel deposition was observed with CO2 nebuliation, and this advantage persisted at both 2 and 7 days post-treatment, underscoring the importance of CO2-mediated pH modulation for sustained peritoneal coverage. For therapeutic evaluation, the hydrogel was loaded with various nanomedicines, including cisplatin nanoparticles, paclitaxel nanocrystals (PNC), Abraxane, and doxorubicin liposomes, to assess compatibility and release profiles. In vitro, cisplatin nanoparticles showed rapid release within 2 days, while paclitaxel-based formulations exhibited prolonged release up to 16 days, supporting extended exposure for poorly soluble agents. PNC- or Abraxane-loaded hydrogels maintained cytotoxicity against SKOV-3 IP2 ovarian cancer cells for 10 days, whereas free formulations lost activity more rapidly. In vivo studies using a luciferase-expressing SKOV-3 peritoneal metastasis rat model demonstrated that PNC-loaded UPy-PEG hydrogel delivered via CO2 nebulization achieved the most pronounced therapeutic effect. Animals treated with the hydrogel exhibited complete tumor suppression for 28 days, no ascites formation, and 100% survival, while free-drug controls showed rapid disease progression. The hydrogel layer persisted up to 7 days in the peritoneum and degraded naturally without adverse effects. This study highlights a rationally engineered, sprayable pH-responsive hydrogel capable of converting minimally invasive aerosol delivery into a durable local therapy for peritoneal metastasis, with the potential to enhance the clinical utility of PIPAC by adding sustained local drug release and improved tumor control (Figure 6).34
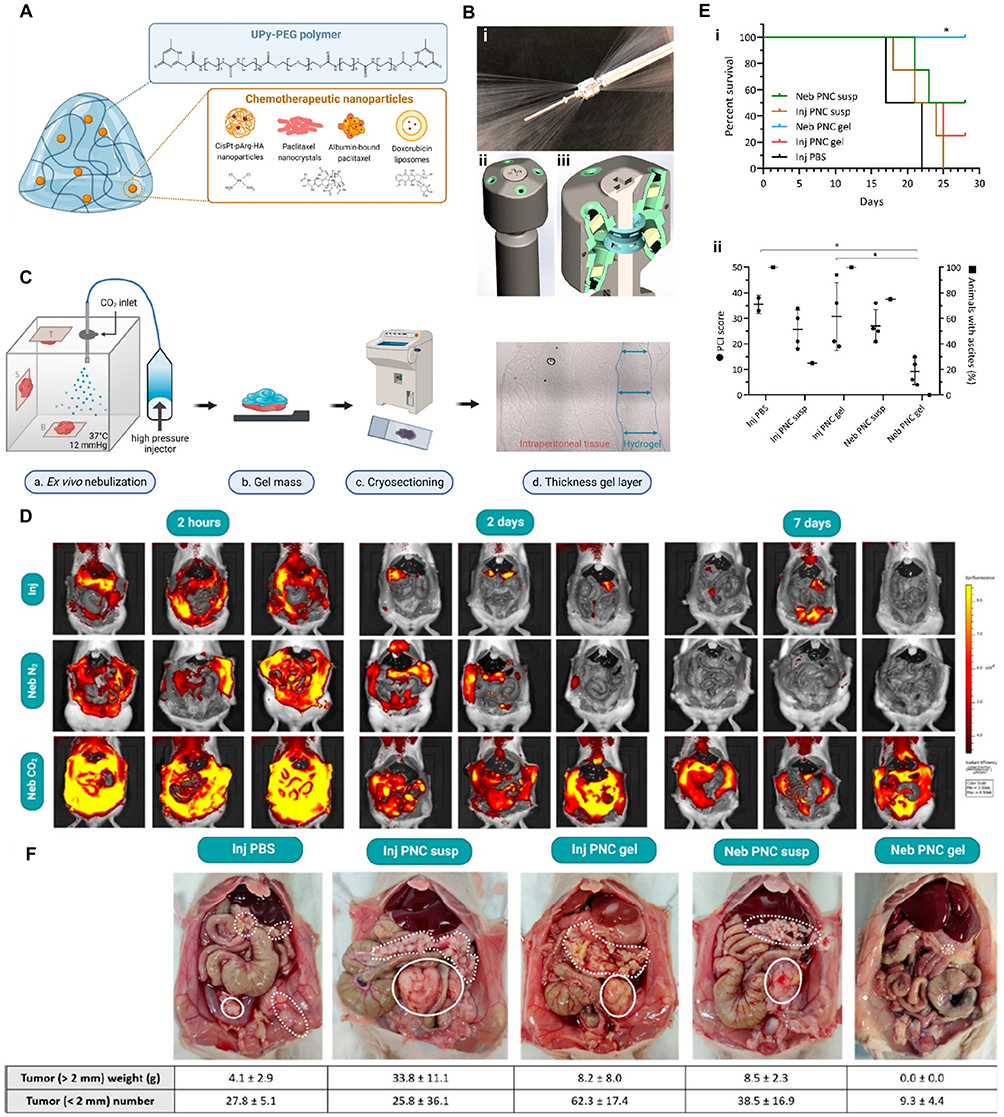 |
Figure 6 CO2-driven nebulization of a pH-sensitive supramolecular hydrogel for treatment of Peritoneal Metastasis. (A) UPy-PEG hydrogel loaded with multiple chemotherapeutic nanoparticles. (B) (i) Medspray nozzle showing multidirectional spray pattern, (ii) external, and (iii) cross-section with spray units. (C) Evaluation of spatial distribution of nebulized UPy-PEG hydrogel in an ex vivo peritoneal cavity model. (D) Time-course fluorescence imaging of Cy7-UPy-PEG hydrogel administered IP injection or nebulization using N2 or CO2. (E) (i) Survival outcomes with extended lifespan in nebulized PNC gel group and (ii) PCI score (●) and animals with ascites (■) at the study endpoint. (F) Macroscopic inspection of the peritoneal cavity: extensive tumors in the PBS, injected PNC, and nebulized PNC groups (tumor nodules indicated by dashed lines and large dorsal tumors by solid lines), whereas only limited nodules were observed after nebulized PNC gel. Data are means ± SD *P < 0.05. Reprinted with permission from Braet et al. Copyright 2023 American Chemical Society.34 |
Majumder et al introduced a surface-fill sprayable hydrogel system (SFH) as a single-application local therapy for cancers growing along complex anatomical surfaces, such as pleural mesothelioma, peritoneal mesothelioma, ovarian peritoneal metastasis, and metastatic CRC.143 The motivation for this approach stems from the clinical challenge that these surface-spreading malignancies are rarely fully resectable, and systemic chemotherapy fails to eradicate microscopic residual disease along serosal planes. SFH was designed as a shear-thinning, self-assembling peptide hydrogel that can be sprayed to conformally coat irregular surgical or anatomical surfaces and persist as a local therapeutic depot. The hydrogel encapsulated miRNA-based nanomedicines, specifically miR-215 and miR-206 complexes, which target oncogenic pathways by activating p53 signaling and inhibiting Ras/CDK4-driven proliferation, respectively. The miRNA complexes were formulated as cationic amphiphilic peptide nanoparticles (~50–200 nm), optimized for cellular uptake and endosomal escape.144 These particles were electrostatically entrapped within the hydrogel network, which allowed gradual and sustained release while protecting the cargo from premature degradation. In vitro studies demonstrated selective cytotoxicity toward H2052 mesothelioma cells, with minimal impact on normal mesothelial cells, supporting a tumor-targeted molecular mechanism.145 In vivo, SFH demonstrated efficacy across multiple preclinical models. In a subcutaneous xenograft model, a single peritumoral application of SFH carrying miRNA resulted in tumor growth suppression, decreased Ki67 proliferation index, and increased TUNEL-positive apoptotic cells. In a peritoneal metastasis model using H2373 cells, a single intraperitoneal administration led to marked reduction in tumor burden and prolonged survival.146 Similarly, in a pleural dissemination model, one-time hydrogel treatment delayed disease progression and extended survival, showing that local miRNA delivery can suppress oncogenic signaling across multiple serosal surfaces. A postsurgical residual disease model further highlighted the adjuvant potential of SFH: the hydrogel-treated side showed markedly reduced recurrence compared with the untreated side. The hydrogel formed a thin 200–250 μm film, adhered to wet tissue, and biodegraded via macrophage uptake, minimizing foreign-body response.147 This work underscores the concept that single-application, sprayable hydrogel therapy can attenuate the oncogenic signature and prevent recurrence on complex anatomical surfaces, providing a new paradigm for localized molecular therapy in mesothelioma and related surface-spreading malignancies.63
Collectively, these two studies demonstrate the emerging role of sprayable hydrogel systems in the local management of anatomically complex surface cancers, with a particular focus on peritoneal and pleural metastases.148 Braet et al focused on a pH-sensitive CO2-nebulized hydrogel to enhance the retention and efficacy of conventional chemotherapeutics in peritoneal metastasis, enabling durable local control through sustained drug release and uniform coverage in minimally invasive settings. In contrast, Majumder et al leveraged a self-assembling miRNA hydrogel to directly modulate oncogenic pathways and achieve molecular tumor suppression with a single application, bridging postoperative adjuvant therapy and local molecular intervention. Within the classification framework outlined earlier, the UPy-PEG hydrogel developed by Braet et al represents a supramolecular, chemotherapy-oriented formulation designed for intraperitoneal surface treatment, in which CO2-driven pH reduction triggers rapid gelation and facilitates uniform aerosol deposition as a key responsiveness feature. Meanwhile, the SFH system introduced by Majumder et al constitutes a peptide-based, nanoparticle-laden hydrogel for molecular gene therapy, optimized for conformal serosal coverage in both pleural and peritoneal settings. This platform exhibits responsiveness through fluid-induced self-assembly and sustained-release kinetics that maintain miRNA stability and bioactivity across extended periods. Despite the difference in therapeutic cargo—chemotherapeutic nanoparticles versus gene-regulatory miRNAs—both platforms exploit the core strengths of sprayable hydrogels: rapid in situ gelation, conformal coating of irregular serosal surfaces, sustained local delivery, and minimal systemic toxicity. Together, these strategies illustrate the transformative potential of sprayable hydrogels as next-generation local adjuvant therapies for surface-spreading malignancies that remain challenging for conventional systemic or surgical approaches.
Breast Cancers
Breast cancer remains one of the leading causes of cancer-related morbidity among women worldwide, and local recurrence after breast-conserving surgery continues to limit long-term disease control despite advances in endocrine therapy, targeted agents, and radiotherapy. The tumor bed frequently contains microscopic residual disease, and conventional postoperative therapies often show limited effectiveness in eliminating these cells. As a result, approaches that enhance the efficacy of adjuvant treatments and more effectively eradicate residual tumor populations to prevent recurrence and metastasis are needed.5
 |
Figure 7 Spray-enabled photocatalytic system for CO-mediated chemosensitization and in situ hydrogel formation. (A) Schematic representation of CO-mediated chemosensitization induced by spray-applied C3N4/Au nanophotocatalysts. (B) Visualization of the sequential steps involved in the in situ formation of the C3N4/Au/SA hydrogel via spray application. Reprinted with permission from Wang et al. Copyright 2025 American Chemical Society.64 |
Wang et al recently introduced a nanoscale sprayable hydrogel system specifically designed for postoperative breast cancer treatment (Figure 7). The platform forms a stable hydrogel network through rapid Ca2+-induced crosslinking that occurs when the sprayed sodium alginate precursor contacts the CaCl2 solution containing the gold-modified graphitic carbon nitride photocatalyst (C3N4/Au), thereby enabling uniform incorporation of the photocatalyst and enhancing the pro-apoptotic efficacy of subsequently administered doxorubicin. Upon spraying onto the surgical cavity, the low-viscosity precursor undergoes immediate gelation, forming a conformal, adherent coating that localizes therapeutic payloads within the resection bed. Under visible-light irradiation, C3N4/Au catalytically converts endogenous CO2 into carbon monoxide, enabling in situ CO-based gas therapy, while FA@DM provides folate-targeted chemotherapy to selectively eliminate residual tumor cells. This sprayable photocatalytic hydrogel demonstrates multiple therapeutic advantages relevant to postoperative breast cancer management. The localized generation of CO induces oxidative stress, mitochondrial dysfunction, and apoptosis in residual tumor cells, while the micellar doxorubicin enhances cytotoxicity with minimal systemic exposure. The system’s rapid gelation and strong tissue adhesion ensure sustained retention at the surgical site, preventing premature washout and enabling prolonged combinatorial treatment. In orthotopic postoperative breast cancer models, the spray gel significantly suppressed tumor regrowth, reduced metastatic dissemination, and achieved improved local disease control compared with either chemotherapy or phototherapy alone. The integration of light-activatable gas therapy with a spray-deployable hydrogel platform highlights a novel paradigm for breast cancer surgery, where minimally invasive intraoperative application can deliver multi-modal adjuvant therapy directly to the tumor bed without altering surgical workflow.64
Overall, this study demonstrates that sprayable nanoscale hydrogels can be rationally engineered to provide conformal coverage, rapid in situ gelation, and synergistic catalytic–chemotherapeutic activity tailored to the postoperative breast cavity. As one of the first demonstrations of a truly spray-deployable nanomedicine hydrogel for breast cancer, this work establishes a foundation for future designs that integrate patient-specific targeting, deeper-tissue activation strategies, and clinically compatible light delivery modalities.
Applications in Cancer Prevention
Cancer prevention has increasingly shifted from general lifestyle or systemic chemoprevention approaches toward localized intervention strategies that directly modulate high-risk tissue environments. Mucosal and serosal surfaces are particularly susceptible to malignant transformation, as they are exposed to chronic irritation, inflammation, or procedural injuries that can initiate the cascade toward cancer. Precancerous lesions and wounds left after surgical or endoscopic interventions represent high-risk sites where unprotected tissue may progress to dysplasia or carcinoma. Conventional systemic therapy often cannot adequately protect these localized environments or maintain sufficient drug levels for extended periods. In this context, sprayable hydrogels have emerged as an appealing strategy, combining rapid in situ gelation, conformal coverage of irregular surfaces, prolonged local retention, and minimal systemic exposure. By enabling early, site-specific intervention, sprayable hydrogels offer a unique avenue for preventing malignant progression.18 The following two representative studies demonstrate how this approach can be leveraged for oral premalignant lesions and gastrointestinal mucosal protection after endoscopic procedures.
Mehta et al developed a nanocubospray formulation containing epigallocatechin-3-gallate (EGCG) to prevent oral submucous fibrosis (OSF), a prototypical precancerous condition that can evolve into oral squamous cell carcinoma.149 OSF is characterized by progressive submucosal fibrosis, collagen accumulation, chronic inflammation, and eventual limitation of mouth opening, all of which predispose to malignant transformation. Traditional therapies such as corticosteroid injections, antioxidants, and physiotherapy offer only partial relief and are limited by low patient compliance, short local residence, and potential systemic side effects. EGCG, a natural polyphenolic compound with strong anti-fibrotic, anti-inflammatory, and antioxidant properties, is well-suited for OSF prevention but is poorly retained on the oral mucosa. To overcome this limitation, Mehta et al formulated NanoCuboSpray (NCS) using self-assembled cationic nanocubosomes (~140 nm, +46.9 mV) that encapsulate EGCG and are suspended in a gellan/xanthan gum-based sprayable film-forming hydrogel system.150 This design enables shear-thinning for easy spraying, followed by uniform film formation on the mucosa for sustained local drug delivery.151 The performance of this formulation was rigorously evaluated. In ex vivo porcine mucosa studies, the NCS achieved approximately five-fold higher penetration over 12 hours compared to free EGCG (296 µg vs 57.7 µg), and fluorescent labeling confirmed deep tissue infiltration and prolonged retention. The release profile followed zero-order super case-II transport, providing stable, extended local delivery without burst loss. In vivo efficacy was demonstrated in a rat model of areca nut–induced OSF. Animals treated with EGCG NCS exhibited marked functional recovery, including improved mouth opening, re-epithelialization with 6–10 cell layers, restoration of rete ridges, and reduced submucosal collagen deposition. Histological analysis revealed suppression of TGF-β1 and collagen I expression, while biochemical assays showed a favorable oxidative balance: thiobarbituric acid reactive substances (TBARS) and nitric oxide decreased, whereas catalase, superoxide dismutase (SOD), and 2,2-diphenyl-1-picrylhydrazyl (DPPH) activity increased. No local irritation, systemic toxicity, or organ damage was observed, and serum biochemistry remained within normal limits. Compared with conventional betamethasone injection therapy, the nanocubospray achieved comparable anti-fibrotic efficacy with superior safety and patient compliance due to its non-invasive and sustained-release profile. This work demonstrates that localized, sprayable hydrogel-based drug delivery can effectively suppress fibrotic and oxidative pathways, reducing the risk of malignant progression in oral premalignant conditions (Figure 8).65,152
 |
Figure 8 Applications in Cancer Prevention. (A) NanoCuboSpray for prevention of oral submucous fibrosis (*P < 0.0001 and # P < 0.0001). (B) Histopathological evaluation of buccal mucosa, liver, and kidney from different treatment groups, along with serum biochemical parameters; photomicrographs obtained at 100X magnification. Reprinted with permission from Mehta et al. Copyright 2025 American Chemical Society.65 |
Taboada et al focused on gastrointestinal mucosal protection after endoscopic procedures, developing a sprayable hydrogel sealant (GastroShield) to prevent delayed complications that could contribute to secondary malignancy risk.153 Endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD) are widely used to remove early gastric and colorectal neoplasia, but they leave exposed mucosal wounds susceptible to delayed bleeding, perforation, and leakage. Such events not only threaten immediate patient safety but can induce prolonged inflammation and impaired healing, which are unfavorable for long-term cancer prevention.154 Conventional closure methods, such as metallic clips and hemostatic powders, suffer from short retention (<48 hours) and frequent dislodgment under peristalsis or acidic gastric conditions.155 To address these limitations, the authors engineered GastroShield, a low-viscosity sprayable hydrogel composed of Pluronic- polyethyleneimine (PEI) micelles crosslinked with oxidized dextran, which gelates within two seconds upon tissue contact to form a thin (≤2 mm) conformal protective layer.156 The network is stabilized by imine bond formation (C=N) between aldehyde and amine groups, covalent interactions with tissue amines, and additional hydrogen bonding and electrostatic forces, ensuring firm adhesion even in dynamic gastrointestinal environments.157 The hydrogel exhibited robust protective performance in vitro and in vivo. In acidic and enzymatic conditions simulating the gastric environment, the hydrogel acted as a proton-buffering barrier, limiting pepsin penetration to ~250 µm and maintaining >98% protective efficacy for over one week. Scratch assays with L929 fibroblasts under acidic, pepsin-rich conditions showed significant enhancement of wound closure, with ~80% recovery at 48 hours compared to ~7% in unprotected controls. Biocompatibility evaluations, including cytotoxicity, rabbit subcutaneous implantation, and genotoxicity testing, revealed no evidence of inflammation, necrosis, or systemic toxicity. In porcine gastric and colonic models, GastroShield adhered within seconds, achieving an initial burst pressure of 64.7 mmHg and maintaining 56.3 mmHg after 24 hours. The hydrogel remained stably attached for at least three days, naturally detached by day 7, and was excreted without complications. Histological analysis showed accelerated wound healing, with early neovascularization observed on day 3 in the treatment group, compared to day 7 in controls. No perforations, leaks, or delayed adverse events occurred. This study establishes GastroShield as a safe, rapidly gelating, and durable sprayable hydrogel sealant that can shield mucosal wounds, prevent delayed complications, and promote healing in cancer-preventive endoscopic interventions.66
Together, these studies highlight the emerging role of sprayable hydrogels in cancer prevention by stabilizing high-risk mucosal environments and interrupting early carcinogenic processes. Mehta et al addressed oral submucous fibrosis by delivering EGCG locally in a sustained manner to suppress fibrosis and oxidative stress, thereby preventing progression to oral cancer. Taboada et al focused on gastrointestinal mucosal injury after endoscopic resection, creating a sprayable hydrogel that provided immediate coverage, acid and enzyme protection, and accelerated tissue recovery, reducing the risk of delayed complications that could predispose to malignancy. Although the anatomical targets differ, both strategies leverage the core strengths of sprayable hydrogels—instant in situ gelation, conformal surface coating, sustained local release, and minimal systemic exposure—to enable early, site-specific cancer prevention. These approaches represent a paradigm shift toward localized, minimally invasive chemoprevention that complements existing surgical and endoscopic oncology practices.
Critical Evaluation of Current Sprayable Hydrogel Systems
Technical and Material Limitations
Despite substantial progress, current nanoscale sprayable hydrogel platforms still face several translational barriers that require careful consideration. Mechanical instability remains a common limitation, as many hydrogels exhibit insufficient robustness under physiological motion, shear forces, or fluid exposure, leading to premature detachment from resection cavities or serosal surfaces.158 Achieving stable yet flexible mechanical strength without compromising sprayability continues to be a major material design challenge.
Biodegradation control presents another critical issue. Numerous formulations demonstrate either overly rapid degradation-resulting in insufficient therapeutic retention-or excessively slow degradation that increases the risk of local accumulation and impairs tissue remodeling.159 Precise tuning of hydrogel degradation kinetics to match postoperative healing timelines remains difficult, particularly because nanoparticles and crosslinkers can alter degradation behavior unpredictably.
Immunogenicity also requires more systematic evaluation. Although most polymers and nanomaterials are considered biocompatible, emerging data indicate that certain nanoparticle-hydrogel combinations may trigger local inflammation, macrophage activation, or off-target immune responses.38 Comprehensive long-term immunotoxicity studies, especially in large-animal models, are still lacking. Moreover, the chronic effects of nanoparticle accumulation in regional lymph nodes and other clearance organs remain incompletely characterized.
Translational and Regulatory Challenges
Clinical scalability and regulatory compliance represent some of the most significant bottlenecks in translating nanoscale sprayable hydrogels to clinical practice. Many reported platforms rely on complex chemistries, multi-step nanoparticle integration, or customized spray devices that are challenging to reproduce under good manufacturing practice (GMP) conditions. Maintaining batch-to-batch consistency during scale-up remains difficult, as sensitive polymer modifications, supramolecular interactions, and biological crosslinkers can introduce variability. Ensuring sterilization stability, long-term storage, and reproducible rheological behavior under GMP is particularly challenging for systems incorporating biological materials, enzymatic crosslinkers, or gaseous components.158 Furthermore, the lack of standardized characterization protocols for critical quality attributes—such as nanoparticle size distribution, drug encapsulation efficiency, and gelation reproducibility—complicates process validation and regulatory documentation.
Another central issue is the ambiguous device–drug combination classification in regulatory frameworks.160 Sprayable hydrogels operate at the interface of a medical device (spray system, nebulizer, catheter) and a therapeutic product (drug-loaded hydrogel matrix containing nanoparticles). Regulatory agencies may categorize these platforms differently depending on the primary mode of action, which influences approval pathways, safety testing requirements, and clinical trial design.161 For example, a chemotherapy-loaded sprayable hydrogel may be classified as a combination product requiring dual regulatory review in the United States, while European agencies might prioritize the device or drug component based on jurisdictional guidelines. Inconsistent classification across regions further complicates global translation, and the absence of established regulatory precedents for multifunctional nanomaterial-hydrogel systems introduces additional uncertainty regarding approval timelines and requirements.
Additionally, device–formulation co-validation is often overlooked in early-stage research. Spray characteristics—atomization behavior, droplet size distribution, deposition uniformity, and clogging risk—must be validated in conjunction with the hydrogel’s gelation kinetics and nanoparticle release profile.23 Minor changes in polymer concentration or nanoparticle loading can significantly alter both the sprayability and device compatibility, necessitating iterative engineering, extensive stability testing, and strong alignment with regulatory expectations. Device-specific parameters such as nozzle gauge, spray pressure, and application angle remain poorly standardized across reported studies, limiting cross-platform comparisons and hindering the identification of optimal design parameters.
These translational considerations collectively highlight that successful clinical adoption will require simplified chemistries, scalable fabrication routes, standardized spray devices, and early engagement with regulatory agencies to ensure a predictable and feasible approval pathway. Collaborative efforts involving material scientists, regulatory consultants, clinicians, and manufacturing specialists will be essential to navigate these multifaceted challenges and accelerate the transition of sprayable hydrogels from laboratory innovation to clinical reality.
Discussion
Sprayable hydrogel systems have emerged as a unique therapeutic platform within localized drug delivery, offering an unprecedented degree of versatility in both therapeutic function and material design. Unlike rigid implants or preformed depots, sprayable hydrogels can conform to complex anatomical geometries and generate an in situ formed matrix that precisely fits the surgical or pathological cavity.112 This adaptability is particularly critical in oncology, where tumor resection sites often present with irregular surfaces, residual microcavities, and variable tissue stiffness that challenge conventional local drug delivery methods. The modular nature of these systems allows for the integration of multiple therapeutic agents—including chemotherapeutics, immunomodulators, gene-silencing constructs, and biologics—within a single formulation, enabling simultaneous or sequential release to address the multifaceted biology of cancer progression and recurrence.
From a functional standpoint, sprayable hydrogels surpass many limitations inherent to traditional localized delivery systems. For instance, their ability to form a continuous, adherent film over residual tumor beds ensures a maximized contact surface area, thereby enhancing drug penetration into surrounding tissues while minimizing leakage into non-target regions. This is especially advantageous for preventing postoperative recurrence, as residual cancer cells are often distributed heterogeneously at the margins of resected tissue. Furthermore, their inherent tunability in mechanical strength, porosity, and degradation kinetics allows for the fine-tuning of drug release profiles, degradation rates, and tissue integration, facilitating a customizable therapeutic window based on disease type, location, and postoperative recovery dynamics.162
The integration of nanoscale components within hydrogel matrices has amplified their therapeutic potential.163 Nanoparticles embedded in the hydrogel can function as drug reservoirs with controlled release properties, as carriers for stimuli-responsive activation, or as active therapeutic agents themselves—such as photothermal nanoparticles or immune adjuvants.164 Moreover, the nanoscale crosslinking motifs introduced into the hydrogel network can impart environment-specific responsiveness, enabling on-demand drug release triggered by pH gradients, enzymatic activity, or redox changes characteristic of TMEs. This combination of macrostructural conformity and nanostructural precision offers a dual-level control over therapeutic delivery that traditional formulations cannot achieve.165
Despite these advantages, the translation of sprayable hydrogel technologies from laboratory to clinic faces significant hurdles. One major challenge is scalable manufacturing with consistent quality control.166 Hydrogels, particularly those containing bioactive agents or labile nanoparticles, are sensitive to variations in temperature, humidity, and processing conditions during production. This sensitivity complicates their mass production and long-term storage, necessitating the development of robust stabilization strategies such as lyophilization-compatible formulations, cold-chain logistics, or shelf-stable precursors that can be activated at the point of care.
Regulatory complexity also presents a barrier. As combination products that integrate drug and device characteristics, sprayable hydrogels often fall under hybrid regulatory pathways that require compliance with both pharmaceutical and medical device standards. This duality increases the time and cost of approval, especially for formulations containing novel nanomaterials that lack established safety profiles.167 Additionally, reproducibility of application in the surgical field must be addressed; differences in surgeon technique, anatomical variability, and intraoperative conditions can influence gel deposition, coverage, and performance. This underscores the importance of developing standardized delivery devices—whether manual, CO2-driven, or endoscopic—that ensure consistent spray patterns and gel formation across clinical settings.
Addressing these challenges will require multidisciplinary collaboration from the earliest stages of development.168 Materials scientists must work alongside pharmaceutical formulators to optimize physicochemical properties, while clinical teams provide feedback on surgical feasibility, intraoperative handling, and postoperative outcomes.169 Regulatory experts can guide the integration of compliance requirements into the design process, minimizing delays during approval phases. Preclinical studies should be designed not only to demonstrate efficacy in relevant tumor models but also to validate stability, ease of use, and scalability—factors that are often overlooked but critical for real-world adoption.
Ultimately, the promise of sprayable hydrogels lies in their ability to bridge the gap between precision nanomedicine and practical, surgeon-friendly interventions. Their capacity for rapid, adaptable deployment in the operating room, combined with tailored pharmacokinetics and biological activity, positions them as a next-generation modality for preventing recurrence and enhancing local control in cancer therapy. The challenge ahead is to systematically address the engineering, regulatory, and logistical barriers to ensure that this promising technology moves from conceptual innovation to standardized clinical practice.
Conclusion and Future Perspectives
Sprayable hydrogel systems represent a convergence of soft material engineering and nanoscale technology, offering a transformative approach to localized cancer treatment. By enabling in situ formation of conformal, drug-laden barriers over surgical beds or mucosal surfaces, these systems directly target the critical window after tumor resection when residual disease and early recurrence risks are at their peak.170 Beyond simple drug depots, sprayable hydrogels can modulate the TME-reducing immunosuppression, alleviating hypoxia, or stimulating immune activation-while simultaneously delivering cytotoxic or targeted therapies in a controlled manner.
One of the most compelling advances in recent years is the incorporation of nanoscale engineering principles into hydrogel formulations. This includes nanoparticle loading for sustained drug release, the integration of nanostructured crosslinkers for stimuli-responsive behavior, and the use of nanocarriers to improve drug solubility, stability, and tumor specificity.171 Such strategies not only enhance therapeutic efficacy but also open new avenues for combining hydrogels with cutting-edge treatments such as immune checkpoint blockade, mRNA delivery, or PTT.
Looking forward, three strategic directions are likely to define the next generation of sprayable hydrogel systems. First, smart, multi-stimuli-responsive hydrogels that dynamically adjust drug release in response to complex tumor cues—pH gradients, enzymatic patterns, redox status, or oxygen levels—will enable more precise and context-specific therapy.172 Achieving such responsiveness will require modular crosslinking chemistries and orthogonal trigger–response mechanisms that can be tuned to heterogeneous postoperative environments.
Second, patient-personalized hydrogel formulations will allow tailoring of drug combinations, release kinetics, and gel composition based on individual tumor profiles, leveraging advances in biomarker discovery and predictive modeling.173 Practical implementation will depend on rapid formulation screening platforms and the incorporation of patient-derived organoid or tissue models to validate individualized hydrogel performance prior to clinical application.
Third, integration with minimally invasive delivery modalities such as robotic-assisted surgery or image-guided endoscopy could expand the applicability of these systems beyond open surgical fields, reaching anatomically challenging or metastatic sites with precision.174 This will require co-design of hydrogel precursors and delivery devices including nozzle geometries, catheter-compatible viscosities, and aerosolization systems, to ensure accurate and reproducible deposition under minimally invasive conditions.
While these three directions outline the trajectory of next-generation sprayable hydrogel systems, several unresolved research gaps must still be addressed to realize their full clinical potential. Achieving scalable and GMP-compatible manufacturing is essential, as many current formulations depend on complex chemistries that are difficult to standardize. Miniaturization of spray devices is also needed to support catheter-based and robotic-assisted procedures, enabling hydrogel application in deep or confined anatomical spaces. In parallel, more robust frameworks for patient-personalized formulations must be established, integrating tumor biology, immune status, and postoperative tissue conditions into the design of hydrogel stiffness, degradation kinetics, and drug combinations. Finally, the long-term biocompatibility of these systems in human tissues remains insufficiently characterized, highlighting the need for extended in vivo studies that evaluate chronic immune responses, nanoparticle retention, and cumulative toxicity.
For successful clinical translation, the field must address not only biological performance but also practical implementation.175 This includes optimizing preloaded and ready-to-use formulations, validating compatibility with sterilization methods, and ensuring shelf stability without compromising functional integrity.176 Multi-center clinical trials with standardized protocols will be crucial to demonstrate reproducibility, safety, and superiority over existing local delivery methods.177 Regulatory approval will be expedited by aligning material selection, manufacturing processes, and safety testing with established international guidelines from the earliest stages of development.178
In the long term, sprayable hydrogels could evolve into multifunctional surgical adjuncts that combine therapeutic, protective, and regenerative functions.179 For example, a single hydrogel could provide hemostasis, deliver chemotherapy, release immunostimulants, prevent infection, and promote wound healing in a coordinated manner.180 The integration of such multifunctionality with precision nanomedicine principles may fundamentally shift the paradigm of perioperative cancer care toward interventions that are more targeted, less toxic, and more durable in their clinical impact.181
Ultimately, the vision is not merely to prove that sprayable hydrogels work in controlled experimental settings, but to refine, standardize, and scale them into accessible, surgeon-ready solutions that can be deployed across diverse healthcare environments. By combining scientific innovation with pragmatic design and clinical insight, sprayable hydrogel systems hold the potential to become a cornerstone of multimodal cancer therapy in the coming decades.
Abbreviations
ROS, reactive oxygen species; TME, tumor microenvironment; PEG, poly(ethylene) glycol; PNIPAm, poly(N-isopropylacrylamide); GBM, glioblastoma multiforme; BBB, blood-brain barrier; PARP, poly(ADP-ribose) polymerase; PLA, poly(lactic acid); PBS, phosphate buffered saline; DMEM, Dulbecco’s Modified Eagle Medium; aCSF, artificial cerebrospinal fluid; GSMs, gliomasupportive macrophages; H&E, hematoxylin and eosin; TAM, tumor-associated macrophage; DHCR7, 7-dehydrocholesterol reductase; NR, nanoregulator; shDHCR7, short hairpin RNA targeting DHCR7; TLR7/8, Toll-like receptor 7/8; ssRNA, single-stranded RNA; PBAE, Poly-β-amino-esters; PD-1, programmed cell death protein 1; LAG3, lymphocyte-activation gene 3; Treg, regulatory T cell; HCC, hepatocellular carcinoma; PFTBA, perfluorotributylamine; GPX4, glutathione peroxidase 4; ACSL4, acyl-CoA synthetase long-chain family member 4; TUNEL, terminal deoxynucleotidyl transferase dUTP nick-end labeling; NK cell, natural killer cell; PAAm, poly(acrylamide); OCS, oxidized chondroitin sulfate; LCSCs, liver cancer stem cells; MDSCs, myeloid-derived suppressor cells; EZH2, enhancer of zeste homolog 2; CXCL10, C-X-C motif chemokine ligand 10; EpCAM, epithelial cell adhesion molecule; PDX, patient-derived xenograft; CAR-NK cell, chimeric antigen receptor-natural killer cell; GCA, glycocholic acid; TCPP, tetrakis (4-carboxyphenyl) porphyrin; CRC, colorectal cancer; TA, tannic acid; PLG, poly(l-glutamic acid); PBA, phenylboronic acid; aOX40, anti-OX40; ICP, infinite coordination polymer; OXA, oxaliplatin; Cur, curcumin; ICD, immunogenic cell death; STING, stimulator of interferon genes; PDA, polydopamine; CRT, calreticulin; CTCs, circulating tumor cells; aCD47, anti-CD47; FDA, Food and Drug Administration; Pex, platelet-derived small extracellular vesicles; PexD, Pex loaded with doxorubicin; DOX, doxorubicin; aPD-L1, anti-programmed death-ligand 1; PLGA, poly(lactic-co-glycolic acid); PVAA, poly(vinyl alcohol) acetoacetate; FS, β-FeSi2; SA, sodium alginate; PTT, photothermal therapy; CDT, chemodynamic therapy; ICG, indocyanine green; NO, nitric oxide; ONOO−, peroxynitrite; RNS, reactive nitrogen species; UPy, ureido-pyrimidinone; ePIPAC, electrostatic pressurized intraperitoneal aerosol chemotherapy; PNC, paclitaxel nanocrystals; SFH, surface-fill hydrogel; EGCG, epigallocatechin-3-gallate; OSF, oral submucous fibrosis; NCS, NanoCuboSpray; TBARS, thiobarbituric acid reactive substances; SOD, superoxide dismutase; DPPH, 2,2-diphenyl-1-picrylhydrazyl; EMR, endoscopic mucosal resection; ESD, endoscopic submucosal dissection; PEI, polyethyleneimine.
Data Sharing Statement
All the data contained in the article is available.
Author Contributions
Conceptualization, J.M.L., S.J.K., Y.S.S., H.J.L., C.-W.P., J.-S.K., and D.H.S.; methodology, J.M.L., S.J.K., M.S.Y., M.J.J., M.K.Y., S.Y.P., S.H.B., J.H.K., S.M.P., and Y.S.L.; literature search and analysis, J.M.L., S.J.K., M.S.Y., M.J.J., M.K.Y., S.Y.P., S.H.B., J.H.K., S.M.P., and Y.S.L.; writing—original draft preparation, J.M.L. and S.J.K.; writing—review and editing, J.M.L., S.J.K., M.S.Y., M.J.J., M.K.Y., S.Y.P., S.H.B., J.H.K., S.M.P., Y.S.L., Y.S.S., H.J.L., C.-W.P., J.-S.K., and D.H.S.; visualization, S.J.K., M.S.Y., S.Y.P., S.H.B., and S.M.P.; supervision, Y.S.S., H.J.L., J.-S.K., C.-W.P., and D.H.S.; project administration, D.H.S. All authors have read and agreed to the published version of the manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF), by the Regional Innovation System & Education (RISE) program through the Chungbuk Regional Innovation System & Education Center, funded by the Ministry of Education (MOE) and Chungcheongbuk-do, Republic of Korea (2025-RISE-11-014-03), and by an NRF grant funded by the Ministry of Science and ICT (MSIT) (No. RS-2025-02273102). This work was also supported by a funding for the academic research program of Chungbuk National University in 2024.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ma W, Ma H, Qiu P, et al. Sprayable β-FeSi2 composite hydrogel for portable skin tumor treatment and wound healing. Biomaterials. 2021;279:121225. doi:10.1016/j.biomaterials.2021.121225
2. Godau B, Samimi S, Seyfoori A, et al. A Drug-Eluting Injectable NanoGel for Localized Delivery of Anticancer Drugs to Solid Tumors. Pharmaceutics. 2023;15(9):2255. doi:10.3390/pharmaceutics15092255
3. McCrorie P, Mistry J, Taresco V, et al. Etoposide and olaparib polymer-coated nanoparticles within a bioadhesive sprayable hydrogel for post-surgical localised delivery to brain tumours. Eur J Pharm Biopharm. 2020;157:108–39. doi:10.1016/j.ejpb.2020.10.005
4. Savekar PL, Nadaf SJ, Killedar SG, et al. Citric acid cross-linked pomegranate peel extract-loaded pH-responsive β-cyclodextrin/carboxymethyl tapioca starch hydrogel film for diabetic wound healing. Int J Biol Macromol. 2024;274:133366. doi:10.1016/j.ijbiomac.2024.133366
5. Yang X, Gao L, Wei Y, et al. Photothermal hydrogel platform for prevention of post-surgical tumor recurrence and improving breast reconstruction. J Nanobiotechnol. 2021;19(1):307. doi:10.1186/s12951-021-01041-w
6. Bao P, Gu H-Y, Jiang Y-C, et al. In situ sprayed exosome-cross-linked gel as artificial lymph nodes for postoperative glioblastoma immunotherapy. ACS nano. 2024;18(20):13266–13276. doi:10.1021/acsnano.4c02425
7. Zhang W, Jing H, Niu Q, et al. Sprayable, thermosensitive hydrogels for promoting wound healing based on hollow, porous and pH-sensitive ZnO microspheres. J Mat Chem B. 2024;12(31):7519–7531. doi:10.1039/D4TB00961D
8. Zhang Q, Zhang Y, Chen H, et al. Injectable hydrogel with doxorubicin-loaded ZIF-8 nanoparticles for tumor postoperative treatments and wound repair. Sci Rep. 2024;14(1):9983. doi:10.1038/s41598-024-57664-0
9. Moreno VM, Baeza A, Vallet-Regí M. Evaluation of the penetration process of fluorescent collagenase nanocapsules in a 3D collagen gel. Acta Biomater. 2021;121:263–274. doi:10.1016/j.actbio.2020.12.022
10. Kasiński A, Zielińska-Pisklak M, Oledzka E, Sobczak M. Smart hydrogels–synthetic stimuli-responsive antitumor drug release systems. Int J Nanomed. 2020;4541–4572. doi:10.2147/IJN.S248987
11. Chu B, Qu Y, He X, et al. ROS‐responsive camptothecin prodrug nanoparticles for on‐demand drug release and combination of chemotherapy and photodynamic therapy. Adv Funct Mater. 2020;30(52):2005918. doi:10.1002/adfm.202005918
12. Mayol B, García-Díez E, Hoppe A, et al. A novel Janus nanomachine based on mesoporous silica nanoparticles anisotropically modified with PAMAM dendrimers for enzyme-controlled drug delivery. Nanoscale. 2025;17(13):8183–8191. doi:10.1039/D4NR03740E
13. Chen Q, Ci T, Gu Z. Sprayable gel for postsurgical immunotherapy. Immuno-Oncology Technol. 2019;2:11–13. doi:10.1016/j.iotech.2019.07.001
14. Jeong D, Jang SY, Roh S, et al. Sprayable hydrogel with optical mRNA nanosensors for Real-Time monitoring and healing of diabetic wounds. Chem Eng J. 2024;493:152711. doi:10.1016/j.cej.2024.152711
15. Yoon MS, Lee JM, Jo MJ, et al. Dual-Drug Delivery Systems Using Hydrogel–Nanoparticle Composites: recent Advances and Key Applications. Gels. 2025;11(7):520. doi:10.3390/gels11070520
16. Yu J, Liu Y, Zhang Y, et al. Smart nanogels for cancer treatment from the perspective of functional groups. Front Bioeng Biotechnol. 2024;11:1329311. doi:10.3389/fbioe.2023.1329311
17. Edo GI, Jikah AN, Elooghene EM, et al. Exploring Carrageenan: biological Activities and Applications in Drug Delivery and Tissue Engineering. Current Pharmacol Rep. 2025;11(1):34. doi:10.1007/s40495-025-00415-0
18. Qian Q, Song J, Chen C, Pu Q, Liu X, Wang H. Recent advances in hydrogels for preventing tumor recurrence. Biomater Sci. 2023;11(8):2678–2692. doi:10.1039/D3BM00003F
19. Wang Z, Zhai B, Sun J, et al. Recent advances of injectable in situ-forming hydrogels for preventing postoperative tumor recurrence. Drug Deliv. 2024;31(1):2400476. doi:10.1080/10717544.2024.2400476
20. Zhang W, Wang R, Sun Z, et al. Catechol-functionalized hydrogels: biomimetic design, adhesion mechanism, and biomedical applications. Chem Soc Rev. 2020;49(2):433–464. doi:10.1039/C9CS00285E
21. Wang Z, Xu J, Wu X, et al. A sprayable Janus hydrogel as an effective bioadhesive for gastrointestinal perforation repair. Adv Funct Mater. 2024;34(48):2408479. doi:10.1002/adfm.202408479
22. Rungrod A, Makarasen A, Patnin S, Techasakul S, Somsunan R. Design and Development of a Sprayable Hydrogel Based on Thermo/pH Dual-Responsive Polymer Incorporating Azadirachta indica (Neem) Extract for Wound Dressing Applications. Polymers. 2025;17(15):2157. doi:10.3390/polym17152157
23. Kianfar E, Kadhum WR, Mahmoud ZH. Hydrogel Nanoparticles in Drug Delivery: a Review. Intelligent Pharmacy. 2025. doi:10.1016/j.ipha.2025.11.002
24. Shin J, Lee JS, Lee C, et al. Tissue adhesive catechol‐modified hyaluronic acid hydrogel for effective, minimally invasive cell therapy. Adv Funct Mater. 2015;25(25):3814–3824. doi:10.1002/adfm.201500006
25. Farasati Far B, Omrani M, Naimi Jamal MR, Javanshir S. Multi-responsive chitosan-based hydrogels for controlled release of vincristine. Commun Chem. 2023;6(1):28. doi:10.1038/s42004-023-00829-1
26. Crowell AD, FitzSimons TM, Anslyn EV, Schultz KM, Rosales AM. Shear thickening behavior in injectable tetra-PEG hydrogels cross-linked via dynamic thia-michael addition bonds. Macromolecules. 2023;56(19):7795–7807. doi:10.1021/acs.macromol.3c00780
27. Zhang K, Xue K, Loh XJ. Thermo-responsive hydrogels: from recent progress to biomedical applications. Gels. 2021;7(3):77. doi:10.3390/gels7030077
28. Tanga S, Aucamp M, Ramburrun P. Injectable thermoresponsive hydrogels for cancer therapy: challenges and prospects. Gels. 2023;9(5):418. doi:10.3390/gels9050418
29. Naranjo-Alcazar R, Bendix S, Groth T, Gallego Ferrer G. Research progress in enzymatically cross-linked hydrogels as injectable systems for bioprinting and tissue engineering. Gels. 2023;9(3):230. doi:10.3390/gels9030230
30. Lai Y, Peng W, Jiang Y, et al. Sprayable self-gelling powder based multifunctional tissue adhesives for rapid hemostasis and robust tissue adhesion. Chem Eng J. 2025;513:162928. doi:10.1016/j.cej.2025.162928
31. Song W, Ko J, Choi YH, Hwang NS. Recent advancements in enzyme-mediated crosslinkable hydrogels: in vivo-mimicking strategies. APL Bioeng. 2021;5(2). doi:10.1063/5.0037793
32. Jeon YR, Jo YK. Multi-bioinspired sprayable nanotherapeutics for tumor-specific focal cancer therapy. Biotechnol Bioprocess Eng. 2023;28(5):781–789. doi:10.1007/s12257-023-0224-z
33. Jeong Y, Jo YK, Kim BJ, Yang B, Joo KI, Cha HJ. Sprayable adhesive nanotherapeutics: mussel-protein-based nanoparticles for highly efficient locoregional cancer therapy. ACS nano. 2018;12(9):8909–8919. doi:10.1021/acsnano.8b04533
34. Braet H, Fransen -P-P, Mariën R, et al. CO2-driven nebulization of pH-sensitive supramolecular polymers for intraperitoneal hydrogel formation and the treatment of peritoneal metastasis. ACS Appl Mater Interfaces. 2023;15(42):49022–49034. doi:10.1021/acsami.3c11274
35. Wang Y, Zhang X, Zhang Y, et al. Sprayed hyaluronic acid based multidrug composite hydrogel for postoperative colorectal cancer ultra-efficient long-lasting multi-stage immuno-chemo synergistic therapy. Mater Horizons. 2025;12(12):4317-4335. doi:10.1039/d5mh00108k
36. Zang C, Tian Y, Tang Y, et al. Hydrogel-based platforms for site-specific doxorubicin release in cancer therapy. J Transl Med. 2024;22(1):879. doi:10.1186/s12967-024-05490-3
37. Liu C, Liao Y, Liu L, et al. Application of injectable hydrogels in cancer immunotherapy. Front Bioeng Biotechnol. 2023;11:1121887. doi:10.3389/fbioe.2023.1121887
38. Erfani A, Diaz AE, Doyle PS. Hydrogel-enabled, local administration and combinatorial delivery of immunotherapies for cancer treatment. Mater Today. 2023;65:227–243. doi:10.1016/j.mattod.2023.03.006
39. Tan Y, Xu C, Liu Y, Bai Y, Li X, Wang X. Sprayable and self-healing chitosan-based hydrogels for promoting healing of infected wound via anti-bacteria, anti-inflammation and angiogenesis. Carbohydr Polym. 2024;337:122147. doi:10.1016/j.carbpol.2024.122147
40. Chen X, Wang X, Pan T, Mao L, Wang H. Highly flexible magnesium–calcium alginate dense hydrogel manufactured by soft spray for drug loading. ACS Appl Polymer Mater. 2024;6(9):5070–5079. doi:10.1021/acsapm.4c00052
41. Hsu N-S, Huang W, Chang H-M, et al. Development of a sprayable thermosensitive lysine-modified pluronic hyaluronic acid hydrogel for enhanced wound healing and adhesion prevention in laparoscopic applications. Int J Biol Macromol. 2025;321:146297. doi:10.1016/j.ijbiomac.2025.146297
42. Ishikawa S, Kamata H, U-i C, Sakai T. Tissue-adhesive hydrogel spray system for live cell immobilization on biological surfaces. ACS Appl Bio Mater. 2023;6(11):4613–4619. doi:10.1021/acsabm.3c00378
43. Smith R, Brogden N, Fiegel J. Sprayable ciprofloxacin-loaded poloxamer hydrogels for wound infection treatment. J Drug Delivery Sci Technol. 2023;89:105000. doi:10.1016/j.jddst.2023.105000
44. Liu C, Zeng H, Chen Z, et al. Sprayable methacrylic anhydride-modified gelatin hydrogel combined with bionic neutrophils nanoparticles for scar-free wound healing of diabetes mellitus. Int J Biol Macromol. 2022;202:418–430. doi:10.1016/j.ijbiomac.2022.01.083
45. Feng Y, Zhang Z, Tang W, Dai Y. Gel/hydrogel‐based in situ biomaterial platforms for cancer postoperative treatment and recovery. Paper presented at: exploration. 2023.
46. Zhao B, Wang C, Qiu X, et al. A Sprayable Temperature-Sensitive Hydrogel Promotes Oral Ulcer Healing through NGFR/ERK Signaling Pathway. ACS Appl Mater Interfaces. 2025;17(21):30478–30491. doi:10.1021/acsami.5c02326
47. Ortega A, da Silva AB, da Costa LM, et al. Thermosensitive and mucoadhesive hydrogel containing curcumin-loaded lipid-core nanocapsules coated with chitosan for the treatment of oral squamous cell carcinoma. Drug Delivery Transl Res. 2023;13(2):642–657. doi:10.1007/s13346-022-01227-1
48. Farouk HO, Nagib MM, Fouad AG, et al. Fabrication of an In Situ pH-Responsive Raloxifene-Loaded Invasome Hydrogel for Breast Cancer Management: in Vitro and In Vivo Evaluation. Pharmaceuticals. 2024;17(11):1518. doi:10.3390/ph17111518
49. Liu Y, Ma W, Zhou P, et al. In situ administration of temperature-sensitive hydrogel composite loading paclitaxel microspheres and cisplatin for the treatment of melanoma. Biomed. Pharmacother. 2023;160:114380. doi:10.1016/j.biopha.2023.114380
50. Zarrin-Nahand N, Mardani H, Roghani-Mamaqani H, Shahi S, Abdollahi M, Salami-Kalajahi M. Dual pH-and redox-responsive hydrogel particles as smart carriers for controlled release of doxorubicin. Colloids Surf A. 2025;725:137625. doi:10.1016/j.colsurfa.2025.137625
51. Solanki R, Bhatia D. Stimulus-responsive hydrogels for targeted cancer therapy. Gels. 2024;10(7):440. doi:10.3390/gels10070440
52. Wang X, Zhang X, Li S, et al. Chitosan and gelatin based sprayable hydrogels incorporating photothermal and long-acting antibiotic sterilization for infected wound management with shape adaptability. Carbohydr Polym. 2025;350:123046. doi:10.1016/j.carbpol.2024.123046
53. Khan SA, Ahmed N, Khan D, Bibi A, Ur Rehman A. pH-responsive mupirocin-loaded hybrid nanoparticles in hydrogel and film forming spray against resistant bacterial wound infections. J Drug Delivery Sci Technol. 2024;101:106187. doi:10.1016/j.jddst.2024.106187
54. Dong Y, Zhang J, Wang Y, et al. Intracavitary Spraying of Nanoregulator-Encased Hydrogel Modulates Cholesterol Metabolism of Glioma-Supportive Macrophage for Postoperative Glioblastoma Immunotherapy. Adv Mater. 2024;36(13):e2311109. doi:10.1002/adma.202311109
55. Zhang Y, Zhang C, Wu B, Li C, Lin J, Huang P. Thermoresponsive Ozone-Enriched Spray Gel for Postsurgical Treatment of Hepatocellular Carcinoma. ACS Nano. 2023;17(4):3518–3527. doi:10.1021/acsnano.2c09893
56. Cheng Y, Gong Y, Li X, et al. A spreadable self-gelling hemostatic powder sensitizes CAR-NK cell therapy to prevent hepatocellular carcinoma recurrence postresection. J Nanobiotechnology. 2025;23(1):353. doi:10.1186/s12951-025-03424-9
57. Gong Y, Zeng F, Zhang F, et al. Radiotherapy plus a self-gelation powder encapsulating tRF5-GlyGCC inhibitor potentiates natural kill cell immunity to prevent hepatocellular carcinoma recurrence. J Nanobiotechnology. 2025;23(1):100. doi:10.1186/s12951-025-03133-3
58. Si X, Ji G, Ma S, et al. In-Situ-Sprayed Dual-Functional Immunotherapeutic Gel for Colorectal Cancer Postsurgical Treatment. Adv Healthc Mater. 2021;10(20):e2100862. doi:10.1002/adhm.202100862
59. Chen Q, Wang C, Zhang X, et al. In situ sprayed bioresponsive immunotherapeutic gel for post-surgical cancer treatment. Nat Nanotechnol. 2019;14(1):89–97. doi:10.1038/s41565-018-0319-4
60. Zhao J, Ye H, Lu Q, et al. Inhibition of post-surgery tumour recurrence via a sprayable chemo-immunotherapy gel releasing PD-L1 antibody and platelet-derived small EVs. J Nanobiotechnology. 2022;20(1):62. doi:10.1186/s12951-022-01270-7
61. Ye H, Wang K, Zhao J, et al. In Situ Sprayed Nanovaccine Suppressing Exosomal PD-L1 by Golgi Apparatus Disorganization for Postsurgical Melanoma Immunotherapy. ACS Nano. 2023;17(11):10637–10650. doi:10.1021/acsnano.3c01733
62. Chen S, Luo Y, He Y, et al. In-situ-sprayed therapeutic hydrogel for oxygen-actuated Janus regulation of postsurgical tumor recurrence/metastasis and wound healing. Nat Commun. 2024;15(1):814. doi:10.1038/s41467-024-45072-x
63. Majumder P, Singh A, Wang Z, et al. Surface-fill hydrogel attenuates the oncogenic signature of complex anatomical surface cancer in a single application. Nat Nanotechnol. 2021;16(11):1251–1259. doi:10.1038/s41565-021-00961-w
64. Wang Z, Zhu J, Mi B, et al. Photocatalytic CO-releasing spray hydrogel for in situ postoperative cancer treatment. Bioact Mater. 2025;53:893–907. doi:10.1016/j.bioactmat.2025.07.024
65. Mehta CH, Velagacherla V, Manandhar S, et al. Nanocubospray of Epigallocatechin Gallate for Prevention of Oral Submucous Fibrosis. AAPS Pharm Sci Tech. 2025;26(6):184. doi:10.1208/s12249-025-03180-x
66. Muñoz Taboada G, Dahis D, Dosta P, Edelman E, Artzi N. Sprayable Hydrogel Sealant for Gastrointestinal Wound Shielding. Adv Mater. 2024;36(24):e2311798. doi:10.1002/adma.202311798
67. Gherardini L, Vetri Buratti V, Maturi M, et al. Loco-regional treatment with temozolomide-loaded thermogels prevents glioblastoma recurrences in orthotopic human xenograft models. Sci Rep. 2023;13(1):4630. doi:10.1038/s41598-023-31811-5
68. Malfanti A, Catania G, Degros Q, Wang M, Bausart M, Préat V. Design of bio-responsive hyaluronic acid–doxorubicin conjugates for the local treatment of glioblastoma. Pharmaceutics. 2022;14(1):124. doi:10.3390/pharmaceutics14010124
69. Chen S, Qiu Q, Wang D, et al. Dual-sensitive drug-loaded hydrogel system for local inhibition of post-surgical glioma recurrence. J Control Release. 2022;349:565–579. doi:10.1016/j.jconrel.2022.07.011
70. Ahmed YW, Wu T-Y, Tsai H-C, et al. Synergistic Local Delivery of Gemcitabine and Resiquimod (R848) via Janus Micelles Encapsulated in a Dual-Responsive Hydrogel for Subcutaneous Glioblastoma Treatment Models. J Drug Delivery Sci Technol. 2025;112:107255. doi:10.1016/j.jddst.2025.107255
71. Shadab A, Farokhi S, Fakouri A, et al. Hydrogel-based nanoparticles: revolutionizing brain tumor treatment and paving the way for future innovations. Eur J Med Res. 2025;30(1):71. doi:10.1186/s40001-025-02310-2
72. Anas Z, Hasan SFS, Moiz MA, et al. The role of hydrogels in the management of brain tumours: a narrative review. Ann Med Surg. 2024;86(4):2004–2010. doi:10.1097/MS9.0000000000001809
73. Yang J, Wang Z, Ma C, et al. Advances in hydrogels of drug delivery systems for the local treatment of brain tumors. Gels. 2024;10(6):404. doi:10.3390/gels10060404
74. Hu Y, Chen L, Liu M, et al. Multifunctional immunotherapeutic gel prevented postoperative recurrence of hepatocellular carcinoma. Chem Eng J. 2023;457:141124. doi:10.1016/j.cej.2022.141124
75. Ke J, Liu Y, Liu F, et al. In-situ-formed immunotherapeutic and hemostatic dual drug-loaded nanohydrogel for preventing postoperative recurrence of hepatocellular carcinoma. J Control Release. 2024;372:141–154. doi:10.1016/j.jconrel.2024.06.030
76. Wang N, Yu -K-K, Li K, Yu X-Q. A biocompatible polyethylene glycol/alginate composite hydrogel with significant reactive oxygen species consumption for promoting wound healing. J Mat Chem B. 2023;11(29):6934–6942. doi:10.1039/D3TB00771E
77. Li S, Luo M, Li J, Huang Q, Lei B. Sprayable Nanocomposites Hydrogel for Wound Healing and Skin Regeneration. Adv Healthcare Mater. 2024;13(32):2402549. doi:10.1002/adhm.202402549
78. Lu H, Li Y, Chen J, et al. In-situ-formed TCM-inspired dual-function nanocomposite hydrogel for intraoperative hemostasis and postoperative recurrence prevention in hepatocellular carcinoma. Mater Today Bio. 2025;34:102192. doi:10.1016/j.mtbio.2025.102192
79. Li X, Zhang Y, Fan Y, et al. Preparation and evaluation of novel mixed micelles as nanocarriers for intravenous delivery of propofol. Nanoscale Res Lett. 2011;6(1):275. doi:10.1186/1556-276X-6-275
80. Liao J, Wu Z, Qiu Y, et al. Injectable thermosensitive microsphere-hydrogel composite system: combined therapy of hepatocellular carcinoma by remodeling tumor immune microenvironment. Sci China Mater. 2024;67(10):3379–3391. doi:10.1007/s40843-024-3001-3
81. Du C, Wang Y, Shi K, et al. Efficient suppression of liver metastasis cancers by paclitaxel loaded nanoparticles in PDLLA-PEG-PDLLA thermosensitive hydrogel composites. J Biomed Nanotechnol. 2017;13(11):1545–1556. doi:10.1166/jbn.2017.2454
82. Cheng H, Shi Z, Yue K, et al. Sprayable hydrogel dressing accelerates wound healing with combined reactive oxygen species-scavenging and antibacterial abilities. Acta Biomater. 2021;124:219–232. doi:10.1016/j.actbio.2021.02.002
83. Gong Y, Cheng Y, Zeng F, et al. A self-gelling hemostatic powder boosting radiotherapy-elicited NK cell immunity to combat postoperative hepatocellular carcinoma relapse. Biomaterials. 2025;317:123068. doi:10.1016/j.biomaterials.2024.123068
84. Kumbhar PS, Kolekar KA, Khandale NB, et al. Expanding arsenal against colorectal cancer using guar gum-based nanocarriers: a review. Int J Biol Macromol. 2025;320:145765. doi:10.1016/j.ijbiomac.2025.145765
85. Guo Y, Wang M, Zhang Y, Zhao Z, Li J. Advanced hydrogel material for colorectal cancer treatment. Drug Delivery. 2025;32(1):2446552. doi:10.1080/10717544.2024.2446552
86. Wang Z, Li S, Qi D, et al. Tissue‐Adhesive, Antibacterial, and Antioxidant Hydrogel Sealant for Sealing Colorectal Anastomotic Leakage and Preventing Postoperative Adhesion. Adv Healthcare Mater. 2025;14(13):2501171. doi:10.1002/adhm.202501171
87. Cheng X, Zhang H, Hamad A, Huang H, Tsung A. Surgery-mediated tumor-promoting effects on the immune microenvironment. Paper presented at: seminars in cancer biology. 2022.
88. Ji G, Zhang Y, Si X, et al. Biopolymer immune implants’ sequential activation of innate and adaptive immunity for colorectal cancer postoperative immunotherapy. Adv Mater. 2021;33(3):2004559. doi:10.1002/adma.202004559
89. Tan Z, Tian L, Luo Y, et al. Preventing postsurgical colorectal cancer relapse: a hemostatic hydrogel loaded with METTL3 inhibitor for CAR-NK cell therapy. Bioact Mater. 2025;44:236–255. doi:10.1016/j.bioactmat.2024.10.015
90. Olguin JE, Mendoza-Rodriguez MG, Sanchez-Barrera CA, Terrazas LI. Is the combination of immunotherapy with conventional chemotherapy the key to increase the efficacy of colorectal cancer treatment? World Journal of Gastrointestinal Oncology. 2023;15(2):251. doi:10.4251/wjgo.v15.i2.251
91. Xiao Y, Guo G, Wang H, et al. Curcumin/L‐OHP co‐loaded HAP for cGAS‐STING pathway activation to enhance the natural immune response in colorectal cancer. Bioeng Transl Med. 2024;9(1):e10610. doi:10.1002/btm2.10610
92. Hu B, Gao J, Lu Y, Wang Y. Applications of degradable hydrogels in novel approaches to disease treatment and new modes of drug delivery. Pharmaceutics. 2023;15(10):2370. doi:10.3390/pharmaceutics15102370
93. Ma H, He C, Chen X. Injectable hydrogels as local depots at tumor sites for antitumor immunotherapy and immune‐based combination therapy. Macromol Biosci. 2021;21(6):2100039. doi:10.1002/mabi.202100039
94. Liu L, Pan Y, Zhao C, Huang P, Chen X, Rao L. Boosting Checkpoint Immunotherapy with Biomaterials. ACS Nano. 2023;17(4):3225–3258. doi:10.1021/acsnano.2c11691
95. Liu Y, Si L, Jiang Y, et al. Design of pH-Responsive nanomaterials based on the tumor microenvironment. Int J Nanomed. 2025;Volume 20:705–721. doi:10.2147/IJN.S504629
96. Si X, Ji G, Ma S, et al. Biodegradable implants combined with immunogenic chemotherapy and immune checkpoint therapy for peritoneal metastatic carcinoma postoperative treatment. ACS Biomater Sci Eng. 2020;6(9):5281–5289. doi:10.1021/acsbiomaterials.0c00840
97. Zhu X, Li S. Nanomaterials in tumor immunotherapy: new strategies and challenges. Mol Cancer. 2023;22(1):94. doi:10.1186/s12943-023-01797-9
98. Chen J, Gu H, Fu S, et al. Multifunctional injectable hydrogels for three-in-one cancer therapy: preoperative remission via mild photothermal-enhanced supramolecular chemotherapy and prevention of postoperative recurrence and adhesion. Chem Eng J. 2021;425:130377. doi:10.1016/j.cej.2021.130377
99. Zhang Z, He C, Chen X. Designing Hydrogels for Immunomodulation in Cancer Therapy and Regenerative Medicine. Adv Mater. 2024;36(4):e2308894. doi:10.1002/adma.202308894
100. Zeting Y, Shuli M, Yue L, et al. Tissue adhesive indocyanine green‐locking granular gel‐mediated photothermal therapy combined with checkpoint inhibitor for preventing postsurgical recurrence and metastasis of colorectal cancer. Bioeng Transl Med. 2023;8(6):e10576. doi:10.1002/btm2.10576
101. Li J, Yu H, Kang Y, et al. STING membrane prevents post‐surgery tissue adhesion and tumor recurrence of colorectal cancer. Adv Mater. 2024;36(21):2309655. doi:10.1002/adma.202309655
102. Khot C, Kolekar K, Dabhole S, et al. Optimized albendazole-loaded nanostructured lipid carrier gel: a redefined approach for localized skin cancer treatment. RSC Pharmaceutics. 2024;1(5):1042–1054. doi:10.1039/D4PM00207E
103. Wu M, Niu X, Zhang R, Xu ZP. Two-dimensional nanomaterials for tumor microenvironment modulation and anticancer therapy. Adv Drug Delivery Rev. 2022;187:114360. doi:10.1016/j.addr.2022.114360
104. Fanfoni L, Marsich E, Turco G, Breschi L, Cadenaro M. Development of di-methacrylate quaternary ammonium monomers with antibacterial activity. Acta Biomater. 2021;129:138–147. doi:10.1016/j.actbio.2021.05.012
105. Liang Q, Chen J, Hou S, et al. Activatable Mn2+-Armed nanoagonist augments antitumor immunity in colorectal cancer: a NIR-II Photonic neoadjuvant paradigm. Biomaterials. 2023;300:122206. doi:10.1016/j.biomaterials.2023.122206
106. Han R, Yu L, Zhao C, et al. Inhibition of SerpinB9 to enhance granzyme B-based tumor therapy by using a modified biomimetic nanoplatform with a cascade strategy. Biomaterials. 2022;288:121723. doi:10.1016/j.biomaterials.2022.121723
107. Zhao D-W, Gao Z, Si M, et al. Immune checkpoint-regulatable hydrogel-immobilized nanotherapeutics for post-surgical treatment of osteosarcoma. Chem Eng J. 2024;498:155072. doi:10.1016/j.cej.2024.155072
108. Hong JK, Schutzman R, Olsen K, Chandrashekar A, Schwendeman SP. Mapping in vivo microclimate pH distribution in exenatide-encapsulated PLGA microspheres. J Control Release. 2022;352:438–449. doi:10.1016/j.jconrel.2022.08.043
109. Kim JH, Dareowolabi BO, Thiruvengadam R, Moon E-Y. Application of nanotechnology and phytochemicals in anticancer therapy. Pharmaceutics. 2024;16(9):1169. doi:10.3390/pharmaceutics16091169
110. Tang J, Li D, Wang R, Li S, Xing Y, Yu F. Engineered extracellular vesicles: an emerging nanomedicine therapeutic platform. Chem Commun. 2025;61(21):4123–4146. doi:10.1039/D4CC06501H
111. Ma C, Cheng Z, Tan H, et al. Nanomaterials: leading immunogenic cell death-based cancer therapies. Front Immunol. 2024;15:1447817. doi:10.3389/fimmu.2024.1447817
112. Liao Y, Xie L, Ye J, et al. Sprayable hydrogel for biomedical applications. Biomater Sci. 2022;10(11):2759–2771. doi:10.1039/D2BM00338D
113. Pramanik S, Alhomrani M, Alamri AS, et al. Unveiling the versatility of gelatin methacryloyl hydrogels: a comprehensive journey into biomedical applications. Biomed Mater. 2024;19(4):042008. doi:10.1088/1748-605X/ad4df7
114. Lu Y, Ye H, Zhao J, et al. Small EV-based delivery of CpG ODNs for melanoma postsurgical immunotherapy. J Control Release. 2023;363:484–495. doi:10.1016/j.jconrel.2023.07.065
115. Yang F, Kong Z, Ji Q, et al. Platelet-inspired nanotherapeutics for biomedical applications. ACS Mater Lett. 2023;5(2):429–449. doi:10.1021/acsmaterialslett.2c00832
116. Zhang K, Li H, Ma Z, Zhong W, Yu Y, Zhao Y. Engineered Platelets for Cancer Therapy. Aggregate. 2025;6(2):e704. doi:10.1002/agt2.704
117. Chen Z, Kankala RK, Yang Z, et al. Antibody-based drug delivery systems for cancer therapy: mechanisms, challenges, and prospects. Theranostics. 2022;12(8):3719. doi:10.7150/thno.72594
118. Yourdkhani A, Esfandyari-Manesh M, Ranjbaran P, Amani M, Dinarvand R. Recent progress in topical and transdermal approaches for melanoma treatment. Drug Delivery Transl Res. 2025;15(5):1457–1495. doi:10.1007/s13346-024-01738-z
119. Chen Z, Rong Y, Ding J, Cheng X, Chen X, He C. Injectable polypeptide hydrogel depots containing dual immune checkpoint inhibitors and doxorubicin for improved tumor immunotherapy and post-surgical tumor treatment. Pharmaceutics. 2023;15(2):428. doi:10.3390/pharmaceutics15020428
120. Liu H, Mei Y, Zhao Q, et al. Black phosphorus, an emerging versatile nanoplatform for cancer immunotherapy. Pharmaceutics. 2021;13(9):1344. doi:10.3390/pharmaceutics13091344
121. Mamidi N, Salehi AOM. Advances in Three-Dimensional Hydrogel Networks for Cancer Immunotherapy. J Mat Chem B. 2025;13(34):10440–10459. doi:10.1039/D5TB01133G
122. Zhou -J-J, Feng Y-C, Zhao M-L, Guo Q, Zhao X-B. Nanotechnology-driven strategies in postoperative cancer treatment: innovations in drug delivery systems. Front Pharmacol. 2025;16:1586948. doi:10.3389/fphar.2025.1586948
123. Yu Z. Reversal of postoperative breast cancer metastasis by the use of embedded hydrogel. Am J Transl Res. 2024;16(11):6991. doi:10.62347/VZAW2270
124. Wang H, Jin Y, Tan Y, et al. Photo-responsive hydrogel facilitates nutrition deprivation by an ambidextrous approach for preventing cancer recurrence and metastasis. Biomaterials. 2021;275:120992. doi:10.1016/j.biomaterials.2021.120992
125. Zheng Y, Wang W, Gao Y, et al. Nanosonosensitizers-engineered injectable thermogel for augmented chemo-sonodynamic therapy of melanoma and infected wound healing. Mater Today Bio. 2023;20:100621. doi:10.1016/j.mtbio.2023.100621
126. Zhu H, Peng X, Liu Y, et al. Self‐Adaptive Dynamic Hydrogel Disrupts Ironclad Defense to Augment Photothermal‐Catalytic Therapy Against Melanoma Recurrence and Promote Post‐Surgical Wound Healing. Adv Funct Mater. 2025;35(34):2420553. doi:10.1002/adfm.202420553
127. Wang L, Lu X, Wang Y, et al. Research Progress on the Application of Novel Wound Healing Dressings in Different Stages of Wound Healing. Pharmaceutics. 2025;17(8):976. doi:10.3390/pharmaceutics17080976
128. Huang M, Huang Y, Liu H, et al. Hydrogels for the treatment of oral and maxillofacial diseases: current research, challenges, and future directions. Biomater Sci. 2022;10(22):6413–6446.
129. Zhao C, Wan J, Zhang L, et al. Two-dimensional borocarbonitride nanosheet-engineered hydrogel as an all-in-one platform for melanoma therapy and skin regeneration. Chem. Mater. 2022;34(14):6568–6581.
130. Yue J, Miao P, Li L, Yan R, Dong W-F, Mei Q. Injectable carbon dots-based hydrogel for combined photothermal therapy and photodynamic therapy of cancer. ACS Appl Mater Interfaces. 2022;14(44):49582–49591. doi:10.1021/acsami.2c15428
131. Zhang X, Zhang Y, Zhang C, et al. An injectable hydrogel co-loading with cyanobacteria and upconversion nanoparticles for enhanced photodynamic tumor therapy. Colloids Surf B. 2021;201:111640. doi:10.1016/j.colsurfb.2021.111640
132. Araujo TAT, Almeida MC, Avanzi I, et al. Collagen membranes for skin wound repair: a systematic review. J Biomater Appl. 2021;36(1):95–112. doi:10.1177/0885328220980278
133. Jia X, Wang Y, Qiao Y, Jiang X, Li J. Nanomaterial-based regulation of redox metabolism for enhancing cancer therapy. Chem Soc Rev. 2024;53(23):11590–11656. doi:10.1039/d4cs00404c
134. He S, Gou X, Zhang S, et al. Nanodelivery systems as a novel strategy to overcome treatment failure of cancer. Small Methods. 2024;8(1):2301127. doi:10.1002/smtd.202301127
135. Liu G, Zhou Y, Xu Z, Bao Z, Zheng L, Wu J. Janus hydrogel with dual antibacterial and angiogenesis functions for enhanced diabetic wound healing. Chin Chem Lett. 2023;34(4):107705. doi:10.1016/j.cclet.2022.07.048
136. Wang M, Zhang X, Liu B, et al. Immunotherapeutic hydrogel with photothermal induced immunogenic cell death and STING activation for post‐surgical treatment. Adv Funct Mater. 2023;33(29):2300199. doi:10.1002/adfm.202300199
137. Xie Y, Li G, Wu J, et al. Injectable self-healing alginate/PEG hydrogels cross-linked via thiol-Michael addition bonds for hemostasis and wound healing. Carbohydr Polym. 2025;348:122864. doi:10.1016/j.carbpol.2024.122864
138. Wu D, Shi X, Zhao F, et al. An injectable and tumor-specific responsive hydrogel with tissue-adhesive and nanomedicine-releasing abilities for precise locoregional chemotherapy. Acta Biomater. 2019;96:123–136. doi:10.1016/j.actbio.2019.06.033
139. Chen X, Ding W, Jiang Y, et al. Emerging strategies for local delivery of immune checkpoint inhibitors to potentiate cancer immunotherapy: current status and future prospects. ACS Appl Mater Interfaces. 2024;16(44):59682–59696. doi:10.1021/acsami.4c12603
140. Chen L, Chen G, Hu K, et al. Combined photothermal and photodynamic therapy enhances ferroptosis to prevent cancer recurrence after surgery using nanoparticle-hydrogel composite. Chem Eng J. 2023;468:143685. doi:10.1016/j.cej.2023.143685
141. Peng Y, Liang S, Meng QF, et al. Engineered bio‐based hydrogels for cancer immunotherapy. Adv Mater. 2024;36(21):2313188.
142. Wang F, Chen J, Liu J, Zeng H. Cancer theranostic platforms based on injectable polymer hydrogels. Biomater Sci. 2021;9(10):3543–3575.
143. Y-n D, Wei Q, L-j Z, et al. Hydrogel-based co-delivery of CIK cells and oncolytic adenovirus armed with IL12 and IL15 for cancer immunotherapy. Biomed. Pharmacother. 2022;151:113110.
144. Wang Y, Li Z, Ouyang J, Karniadakis GE. Controlled release of entrapped nanoparticles from thermoresponsive hydrogels with tunable network characteristics. Soft Matter. 2020;16(20):4756–4766. doi:10.1039/D0SM00207K
145. Song W, Lee C, Jeong H, Kim S, Hwang NS. Sprayable anti-adhesive hydrogel for peritoneal macrophage scavenging in post-surgical applications. Nat Commun. 2024;15(1):8364. doi:10.1038/s41467-024-52753-0
146. Wintjens AG, Liu H, Fransen -P-PK, et al. Treating colorectal peritoneal metastases with an injectable cytostatic loaded supramolecular hydrogel in a rodent animal model. Clin Exp Metastasis. 2023;40(3):243–253. doi:10.1007/s10585-023-10210-0
147. Erdi M, Rozyyev S, Balabhadrapatruni M, et al. Sprayable tissue adhesive with biodegradation tuned for prevention of postoperative abdominal adhesions. Bioeng Transl Med. 2023;8(1):e10335. doi:10.1002/btm2.10335
148. Zhong Z, Gan L, Feng Z, et al. Hydrogel local drug delivery systems for postsurgical management of tumors: status Quo and perspectives. Mater Today Bio. 2024;29:101308. doi:10.1016/j.mtbio.2024.101308
149. Yu B, Zhan A, Liu Q, et al. A designed supramolecular cross-linking hydrogel for the direct, convenient, and efficient administration of hydrophobic drugs. Int J Pharm. 2020;578:119075. doi:10.1016/j.ijpharm.2020.119075
150. Yano H, Sasaki F, Maeda H, et al. Effect of sprayable, highly adhesive hydrophobized gelatin microparticles on esophageal stenosis after endoscopic submucosal dissection: an experimental study in a swine model. Esophagus. 2025;22(1):95–104. doi:10.1007/s10388-024-01090-8
151. Atoosh IJ, Ghareeb MM, Atoosh I. Optimizing Mucoadhesive Film-Forming Spray for Efficient Oral Delivery of Fluconazole in Candidiasis Treatment. Cureus. 2024;16(9). doi:10.7759/cureus.70359
152. Shi Y, T-x X, Leach DG, et al. Local anti–PD-1 delivery prevents progression of premalignant lesions in a 4NQO-oral carcinogenesis mouse model. Cancer Prev Res. 2021;14(8):767–778. doi:10.1158/1940-6207.CAPR-20-0607
153. Wang W, Vikesland PJ. SERS-active printable hydrogel for 3D cell culture and imaging. Anal Chem. 2023;95(49):18055–18064. doi:10.1021/acs.analchem.3c02641
154. Hu X, Grinstaff MW. Advances in hydrogel adhesives for gastrointestinal wound closure and repair. Gels. 2023;9(4):282. doi:10.3390/gels9040282
155. Dhar J, Ramai D, Samanta J, Facciorusso A. Hemostatic powders and gels in gastrointestinal endoscopy: current perspective and future recommendations. Expert Review Gastroenterol Hepatol. 2023;17(11):1061–1065. doi:10.1080/17474124.2023.2274913
156. Cho R, Kamata H, Tsuji Y, et al. Optimizing a self-solidifying hydrogel as an endoscopically deliverable hydrogel coating system: a proof-of-concept study on porcine endoscopic submucosal dissection-induced ulcers. Polym J. 2024;56(9):855–863. doi:10.1038/s41428-024-00921-w
157. He J, Zhang Z, Yang Y, et al. Injectable self-healing adhesive pH-responsive hydrogels accelerate gastric hemostasis and wound healing. Nano-Micro Lett. 2021;13(1):80. doi:10.1007/s40820-020-00585-0
158. Baweja R, Ravi R, Baweja R, et al. A comprehensive review of hydrogels as potential drug carriers for anticancer therapies: properties, development and future prospects. Next Mater. 2025;8:100913. doi:10.1016/j.nxmate.2025.100913
159. Lee Y, Kim M, Kim N, Byun S, Seo S, Han JY. Injectable Hydrogel Systems for Targeted Drug Delivery: from Site-Specific Application to Design Strategy. Appl Sci. 2025;15(21):11599. doi:10.3390/app152111599
160. Foulkes R, Man E, Thind J, Yeung S, Joy A, Hoskins C. The regulation of nanomaterials and nanomedicines for clinical application: current and future perspectives. Biomater Sci. 2020;8(17):4653–4664. doi:10.1039/D0BM00558D
161. Rodríguez-Gómez FD, Monferrer D, Penon O, Rivera-Gil P. Regulatory pathways and guidelines for nanotechnology-enabled health products: a comparative review of EU and US frameworks. Front Med. 2025;12:1544393. doi:10.3389/fmed.2025.1544393
162. Xiao T, Dai H, Wu Y, et al. Tailoring Physicochemical Properties of Photothermal Hydrogels Toward Intrinsically Regenerative Therapies. Adv Funct Mater. 2025;35(5):2414419. doi:10.1002/adfm.202414419
163. Liu M, Zeng X, Ma C, et al. Injectable hydrogels for cartilage and bone tissue engineering. Bone Res. 2017;5(1):1–20.
164. Yue L, Yu G, Rao L, Wang R, Chen X. Supramolecular Aggregates and Hitchhikers. Acc Mater Res. 2024;5(10):1237–1250. doi:10.1021/accountsmr.4c00172
165. Lim J, Lin Q, Xue K, Loh X. Recent advances in supramolecular hydrogels for biomedical applications. Mater Today Adv. 2019;3:100021. doi:10.1016/j.mtadv.2019.100021
166. Li H, Gu T, Xu J, et al. Hydrogel-based biomaterials for brain regeneration after stroke: gap to clinical translation. Biomaterials Translational. 2025;6(2):165. doi:10.12336/bmt.24.00020
167. Tinkle S, McNeil SE, Mühlebach S, et al. Nanomedicines: addressing the scientific and regulatory gap. Ann NY Acad Sci. 2014;1313(1):35–56. doi:10.1111/nyas.12403
168. Yang L, Zhang X. Advanced Functional Materials for Disease Diagnosis, Drug Delivery and Tissue Repair. Vol. 13. Frontiers Media SA; 2025:1602628.
169. Liu Y, Xu J, Guo Y. Natural polysaccharide-based nano-drug delivery systems: innovative strategies and research advances in cancer therapy–A review. Int J Biol Macromol. 2025;321:146081. doi:10.1016/j.ijbiomac.2025.146081
170. Fu Y, Zhu X, Ren L, Wan J, Wang H. Syringeable near-infrared light-activated in situ immunogenic hydrogel boosts the cancer-immunity cycle to enhance anticancer immunity. ACS nano. 2024;18(23):14877–14892. doi:10.1021/acsnano.3c08425
171. Qin J, Sun M, Hu W, Cheng J, Fan Z, Du J. Stimuli-responsive hydrogels for cancer immunotherapy. Polym Chem. 2023;14(7):793–802. doi:10.1039/D2PY01308H
172. Hao J, Li Y, Huang L, et al. Smart Nanoarchitectures for Precision RNA Delivery: harnessing Endogenous and Exogenous Stimuli in Cancer Treatment. Theranostics. 2025;15(15):7747. doi:10.7150/thno.112492
173. Katopodi T, Petanidis S, Floros G, Porpodis K, Kosmidis C. Hybrid Nanogel Drug Delivery Systems: transforming the Tumor Microenvironment through Tumor Tissue Editing. Cells. 2024;13(11):908. doi:10.3390/cells13110908
174. Cheng Y, Zhang H, Wei H, Yu C-Y. Injectable hydrogels as emerging drug-delivery platforms for tumor therapy. Biomater Sci. 2024;12(5):1151–1170. doi:10.1039/D3BM01840G
175. Mohapatra S, Mirza MA, Hilles AR, et al. Biomedical application, patent repository, clinical trial and regulatory updates on hydrogel: an extensive review. Gels. 2021;7(4):207. doi:10.3390/gels7040207
176. Park S-J, Hwang T, Jo S, et al. Unveiling the Diverse Principles for Developing Sprayable Hydrogels for Biomedical Applications. Biomacromolecules. 2025;26(2):753–772. doi:10.1021/acs.biomac.4c01312
177. Xu C, Ivanovski S. Clinical translation of personalized bioengineered implant scaffolds. Nature Reviews Bioeng. 2025;3(5):390–407. doi:10.1038/s44222-024-00269-z
178. Singhal R, Sarangi MK, Rath G. Injectable hydrogels: a paradigm tailored with design, characterization, and multifaceted approaches. Macromol Biosci. 2024;24(7):2400049. doi:10.1002/mabi.202400049
179. Cheng Y, Zhang H, Wei H, Yu C-Y Injectable hydrogels as emerging drug-delivery platforms for tumor therapy. Biomaterials Science. 2024;12(5):1151–1170. doi:10.1039/d3bm01840g
180. Zhang H, Zhang M, Zhang X, et al. Enhanced postoperative cancer therapy by iron-based hydrogels. Biomater Res. 2022;26(1):19. doi:10.1186/s40824-022-00268-4
181. Zhu H, Zheng J, Oh XY, et al. Nanoarchitecture-integrated hydrogel systems toward therapeutic applications. ACS nano. 2023;17(9):7953–7978. doi:10.1021/acsnano.2c12448
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.