Back to Journals » Clinical Ophthalmology » Volume 19
Real-World Visual Outcomes and Rotational Stability of a Monofocal Toric Intraocular Lens
Authors LaHood B, Peterson RC
Received 7 April 2025
Accepted for publication 8 August 2025
Published 23 August 2025 Volume 2025:19 Pages 2945—2953
DOI https://doi.org/10.2147/OPTH.S532933
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Ben LaHood,1 Rachael C Peterson2
1Adelaide Eye and Laser Centre, Adelaide, South Australia, Australia; 2Alcon Research, Fort Worth, TX, USA
Correspondence: Ben LaHood, Adelaide Eye and Laser Centre, 215 Greenhill Road, Adelaide, South Australia, 5063, Australia, Tel +61 451545323, Email [email protected]
Purpose: To assess the real-world distance and intermediate visual outcomes, rotational stability, and adverse events (AEs) of patients implanted with a Clareon aspheric monofocal toric intraocular lens (IOL) preloaded in the AutonoMe delivery system (Alcon, USA; models CNA0T2 to CNA0T6) up to one-month postoperative.
Methods: Surgical charts from January 2021 to October 2023 were reviewed for adult patients (≥ 18 years) who previously received a CNA0T2 to CNA0T6 (T2 to T6) IOL during uneventful cataract surgery and were targeted for emmetropia/first minus. Overall, charts from 193 eyes of 121 patients were screened, with 161 eyes of 107 patients included in the study. Data were collected from preoperative, and postoperative records up to approximately one-month (4– 5 weeks), and included monocular corrected distance visual acuity (CDVA), uncorrected and distance-corrected intermediate visual acuity (UIVA and DCIVA), residual astigmatism, and absolute IOL rotation (measured from the axis position at the end of surgery up to one-month).
Results: For the full cohort (T2 to T6 IOLs, n=161 eyes), CDVA was − 0.01 ± 0.07 logMAR at one-month. Monocular UIVA was 0.22 ± 0.14 logMAR, DCIVA was 0.24 ± 0.12 logMAR, and absolute IOL rotation was 1.02 ± 1.21°. Residual astigmatism was very low (< 0.01D) and consistently low across T2 to T6 IOLs. A T3 to T6 sub-analysis (n=64 eyes) found CDVA of − 0.01 ± 0.07 logMAR, UIVA of 0.20 ± 0.14 logMAR, DCIVA of 0.23 ± 0.13 logMAR, and absolute rotation of 1.08 ± 1.26°. For all eyes, 1 serious ocular AE, cystoid macular edema, was identified. No serious non-ocular AEs, device deficiencies, or posterior capsular opacification were observed.
Conclusion: The Clareon aspheric monofocal toric IOL showed excellent improvement in distance visual acuity and treatment of astigmatism, with functional intermediate visual acuity and minimal rotation.
Keywords: Clareon toric, intermediate vision, residual astigmatism, rotational stability
Introduction
The Clareon monofocal toric intraocular lens (IOL) model CNA0TX has been recently released from Alcon Laboratories LLC (Fort Worth, Texas, USA). It has an optical design based on the AcrySof IQ aspheric monofocal toric IOL, with modifications made to the biomaterial and edge design aimed at improving visual clarity and reducing any potential photopic side effects.
The main outcomes of interest of a new toric IOL are their visual capabilities and rotational stability across the population. For distance visual acuities, the ability of toric IOLs to improve outcomes by correcting pre-existing astigmatism is well established.1–3 Recently, intermediate vision in monofocal IOLs has been a topic of interest. Previous studies by Micheletti et al4 and Blehm and Hall5 have shown good intermediate visual acuity at 66 cm with the Clareon monofocal non-toric IOLs; however, this outcome has not yet been investigated for the Clareon monofocal toric models.
Once a toric lens has been chosen and positioned, its performance is then dependent on postoperative rotational stability.6 In optical principals, for every 1° of rotation, the astigmatic refractive correction provided by the cylindrical power at a certain axis is degraded by 3.3%.2,6 Therefore, a rotation of 30° would hypothetically erase the astigmatic correction entirely while rotation greater than 30° would increase astigmatic refractive error.2 It is crucial that the rotational stability of a toric IOL be assessed to establish its capabilities.
This study aimed to retrospectively assess the real-world visual outcomes, rotational stability and adverse events (AEs) with the Clareon monofocal toric IOLs per standard of care.
Materials and Methods
Study Design
This was a retrospective, single surgeon, single-center, open-label, real-world study of adult eyes (≥ 18 years) that had undergone cataract surgery with implantation of a Clareon monofocal toric IOL. Although this was a retrospective study, care was taken where possible to perform this study in alignment with EN ISO 14155:2020 and the declaration of Helsinki and was prospectively granted ethical approval by the Belberry Human Research Ethics Committee before data extraction.
Study Population
Patient data were extracted from Adelaide Eye and Laser Centre, a private practice located in South Australia. The patient records were reviewed from January 1, 2021 to October 1, 2023.
Device Description
The Clareon monofocal toric IOLs are single-piece, aspheric, foldable lens with a C-loop haptic design for placement in the posterior chamber. They have a 6.0 mm fully refractive optic diameter and an overall haptic diameter of 13.0 mm.
Inclusion and Exclusion Criteria
Eyes of adult patients aged 18 years or older that had previously undergone uncomplicated cataract surgery for senile cataract, with implantation of a Clareon monofocal toric IOL, targeted for emmetropia or first-minus, during the study period were included. Eyes were excluded if they had undergone previous ocular surgery or if they had other pre-existing ocular comorbidities such as macular degeneration, diabetic maculopathy, corneal scarring, irregular corneal astigmatism or any other ocular conditions other than cataracts that may have affected postoperative visual acuity, and if they had degenerative conditions, such as dementia, that could affect the ability to assess refractive outcomes.
Sample Size
This study aimed to collect a sample size of at least 100 eyes that met the inclusion and exclusion criteria and had a complete dataset of preoperative, operative, and up to approximately one month (4–5 weeks) of postoperative records.
Data Extraction
Pseudo-identified data from all eyes that met the inclusion and exclusion criteria were extracted from the records into a digital database by the principal investigator. Data verification was then conducted by a second ophthalmic professional (optometrist) to confirm the accuracy of the data transfer.
Surgical Procedures
Preoperative
For all patient data evaluated in this study, the following presurgical and surgical techniques were applied. Preoperative IOL calculation was performed using the Barrett Universal II toric formula based on biometry from the IOLMaster 700 device (Carl Zeiss, Germany). Standard anterior keratometry was used as opposed to total keratometry because additional benefit has not been consistently shown in astigmatic outcomes from incorporating posterior corneal astigmatism measurements in eyes that have not received laser vision correction.7 The refractive target in all included eyes was emmetropia or first minus and minimal estimated refractive astigmatism (regardless of flipped axis).
Intraoperative
For all eyes, cataract surgeries were performed per indication using the Centurion (Alcon, USA) phacoemulsification machine. All patients received intravenous sedation and regional anaesthesia. Implanted devices were Clareon monofocal toric IOLs, models CNA0T2 to CNA0T6 (T2 to T6; Alcon, USA) available at the time. These IOLs were preloaded in the AutonoMe Delivery Device (Alcon, USA) and inserted via a 2.2 mm clear corneal two-step incision using a wound-assisted technique. The main incision was placed on the horizontal axis at either 0° or 180° for left or right eyes, respectively. Toric alignment during surgery was achieved using the Callisto Eye digital overlay system (Carl Zeiss, Germany). Intracameral antibiotics were injected at the conclusion of the operation.
Postoperative
Data extracted from the records were for preoperative, operative, one-day, one-week, and one-month (4–5 weeks) postoperative visits, including any unscheduled visits that occurred. Visual acuity parameters were assessed in general room lighting conditions.
Objectives and Outcome Measures
The study objectives were to determine the distance and intermediate visual acuity, rotational stability, and other visual and AE outcomes in a real-world cohort of Clareon monofocal toric IOL implantations, up to one-month postoperative.
The primary outcome was corrected distance visual acuity (CDVA) at one-month postoperative. Secondary outcomes included monocular uncorrected distance visual acuity (UDVA) at 6 m, monocular uncorrected intermediate visual acuity (UIVA) and distance-corrected intermediate visual acuity (DCIVA) at 66 cm, refractive predictability (manifest refractive spherical equivalent [MRSE]), residual astigmatism between toric steps/models, IOL rotational stability measured as the change in absolute IOL position from immediately at the end of surgery (EOS) to one-day, one-week, and one-month postoperative (image analysis methods are described below), and surgically induced astigmatism (SIA) calculated as a vector (described below).
All AEs (ocular and non-ocular, serious and non-serious) were captured as part of the surgeon’s standard of care. The surgeon’s standard of care was to treat all eyes with postoperative topical steroid and non-steroidal anti-inflammatory drops postoperatively to reduce the risk of cystoid macular edema (CME).
Image Analysis for Rotational Stability
Absolute rotation was measured objectively as follows: a still image was taken immediately at the EOS to capture the toric IOL axis placement location via the Lumera 700 operating microscope (Carl Zeiss, Germany) while the patient was supine. Postoperatively, slit lamp photography using the SL-800 slit lamp imaging system (Carl Zeiss, Germany) was performed at one week and one-month to assess the IOL rotational position. Images were entered into Adobe Photoshop and then overlayed precisely using physical anchors (such as non-movable limbal vessels) to avoid the effects of cyclotorsion. The difference between the position of the operative and postoperative toric IOL markings was measured in degrees. The direction of rotation was not captured.
Surgically Induced Astigmatism
SIA was assessed using a double angle vector diagram where preoperative and postoperative astigmatism were plotted to provide individual eye changes in magnitude and direction of corneal astigmatism. A summated vector mean (or centroid) value was then calculated to provide an overall measure of SIA, again, with a magnitude and direction. The flattening effect of the incision was also analyzed. This was calculated by finding the mean vector component of each SIA vector aligned with the axis of the incision and averaging their magnitude. This indicates how much of a flattening effect occurs at the actual axis where an incision is made.
Statistical Analysis
Descriptive statistics (mean ± standard deviation [SD]) are reported for visual acuities, prediction errors, and average postoperative rotation of the monofocal toric IOL for each time point. AE data were reported numerically and as a percentage of the cohort. Vector analyses were performed to examine SIA by the investigator using SPSS software and outcomes analysis was conducted according to the Standard Graphs for Reporting Refractive Outcomes Intraocular Lens-Based Refractive Surgery.
In some cases, data were collected from both eyes of patients who were implanted binocularly with Clareon toric IOLs. To eliminate any statistical bias, a separate ad hoc analysis was performed on the first eye of all patients. Additionally, a second ad hoc analysis was conducted on all eyes of the T3 to T6 IOL cylinder powers only, which are currently used in the USA.
Results
Patient records from 193 eyes of 121 patients were screened, and 161 eyes of 107 patients were included in this retrospective study. The mean ± SD patient age was 74 ± 7.57 years with 58% being female eyes (Table 1).
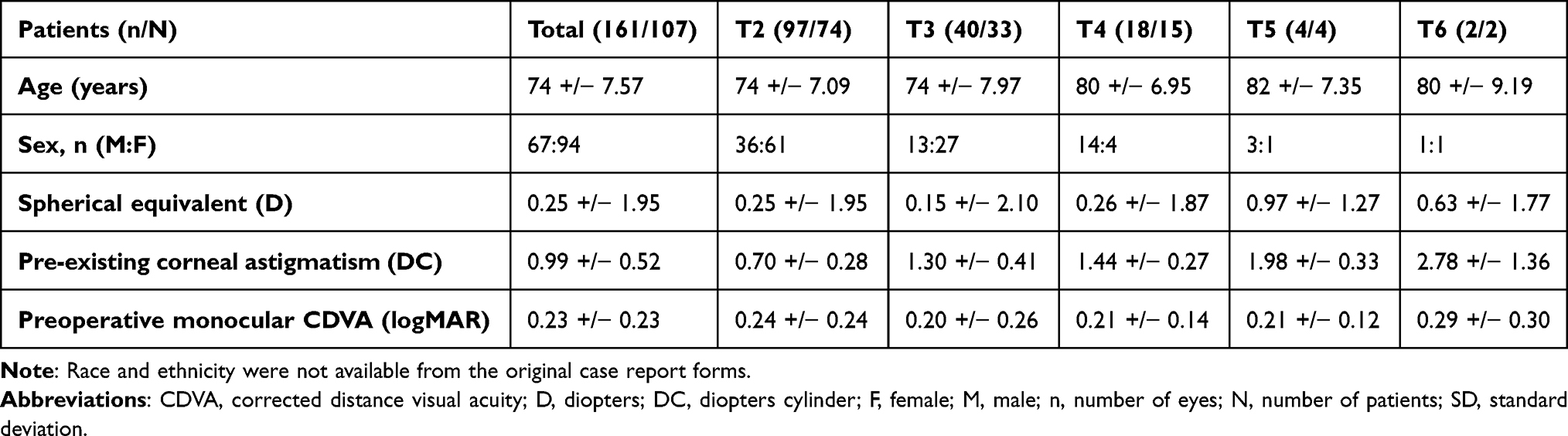 |
Table 1 Demographic and Preoperative Characteristics of the Patients (Mean +/− SD) |
Visual and Refractive Outcomes
Visual Acuity
Monocular CDVA was −0.01 ± 0.07 logMAR at one-month postoperation. Postoperatively, mean monocular DCIVA and UIVA were 0.24 ± 0.12 logMAR and 0.22 ± 0.14 logMAR, respectively (Table 2). Approximately 60.9% and 55.9% of eyes achieved UIVA and DCIVA of 0.24 logMAR or better, respectively (Figure 1). The mean MRSE was −0.07 ± 0.30 D with residual sphere of 0.04 ± 0.31 D.
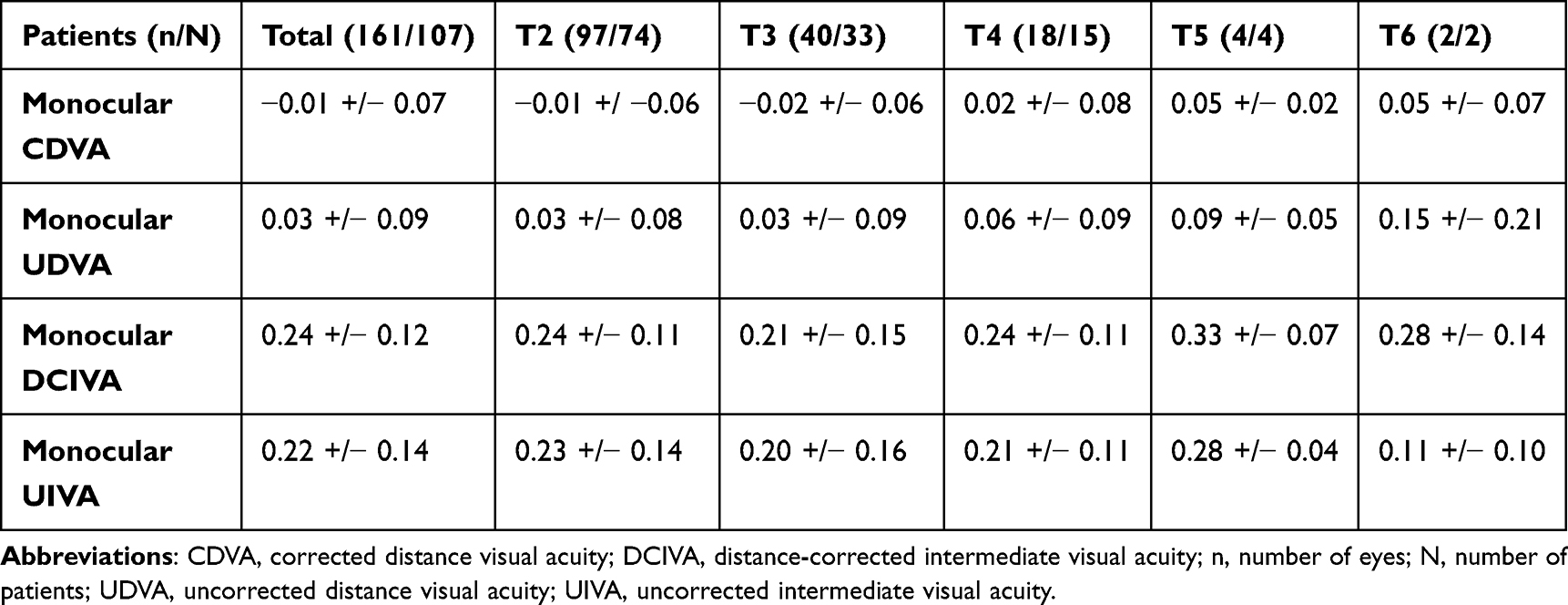 |
Table 2 Performance Endpoints in Visual Acuities (LogMAR) at One-Month Postoperatively |
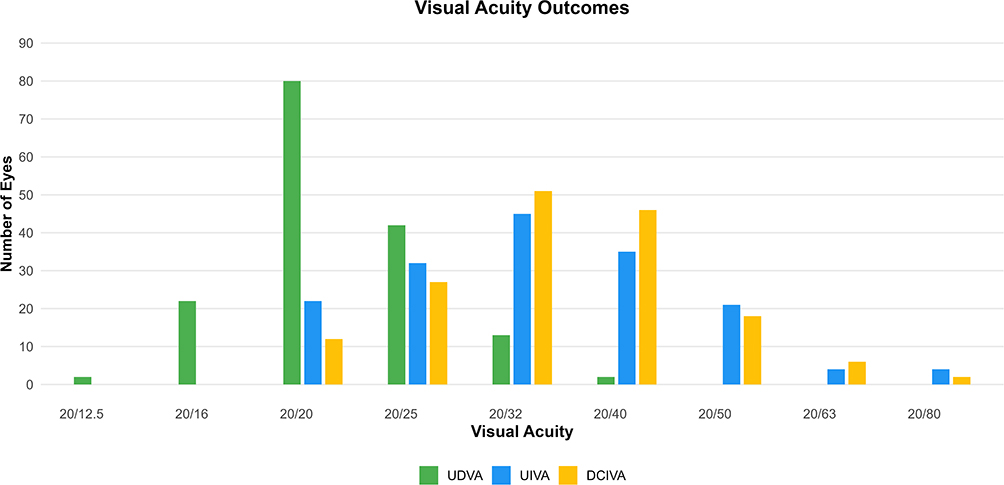 |
Figure 1 Visual Acuity Measurements. Abbreviations: DCIVA, distance-corrected intermediate visual acuity; UDVA, uncorrected distance visual acuity; UIVA, uncorrected intermediate visual acuity. |
Astigmatism
The Clareon monofocal toric IOL corrected, on average, 0.99 ± 0.52 D of pre-existing corneal astigmatism, resulting in absolute mean residual refractive cylinder of 0.22 ± 0.29 D at one-month following surgery across the T2 to T6 IOLs (Figure 2). Of the 161 eyes, 113 eyes (70.1%) had residual refractive astigmatism ≤ 0.25 D, 144 eyes (89.4%) had ≤ 0.50 D, 155 eyes (96.3%) had ≤ 0.75 D, and 160 eyes (99.4%) had ≤ 1.0 D of residual refractive astigmatism. SIA was calculated using preoperative versus postoperative optical biometry plotted on a double angle vector diagram and had a summated vector mean (centroid) magnitude of 0.07 D with an axis of 113°. The flattening effect at the location of the incision axis was 0.05 D. Mean magnitude of SIA not considering direction was 0.32 D.
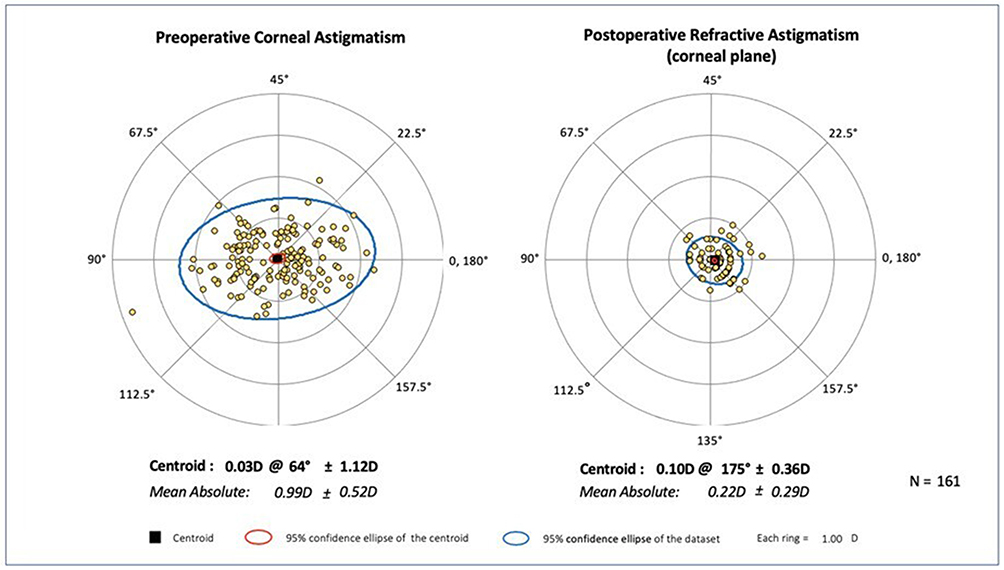 |
Figure 2 Preoperative and Postoperative Astigmatism at the Corneal Plane. Abbreviations: D, diopters; N, number of patients. |
Rotational Stability
Toric IOL rotation from EOS to one day postoperation was an average of 0.87 ± 1.16°. No additional rotation occurred after one week from EOS and total rotation at one-month postoperation was 1.02 ± 1.21 (Table 3). No IOL rotation magnitude was great enough to cause significant residual astigmatic refractive error requiring optical or surgical correction. One eye was found to have an IOL with 6° of rotation, which likely occurred due to pre-existing capsular fibrosis noted intraoperatively.
 |
Table 3 Absolute IOL Rotational Stability (Degrees) Over Time, After Baseline Implantation |
Ad Hoc Analyses
The first ad hoc analysis of first eyes only (n=107 eyes) was conducted to remove potential bias from analyzing two eyes of the same patient. The findings were consistent with the results of the full cohort analysis, with mean ± SD monocular CDVA of −0.01 ± 0.07 logMAR, UDVA of 0.03 ± 0.09 logMAR, UIVA of 0.21 ± 0.13 logMAR, and DCIVA of 0.22 ± 0.12 logMAR. Mean ± SD residual refractive cylinder was 0.22 ± 0.31 D and was consistently low across all models. An IOL rotation of 1.12 ± 1.29° was found on average, with ≤ 1° of rotation in 70% of lenses and ≤ 5° of rotation in 99% of lenses at one-month postoperation.
The second ad hoc analysis (n=64 eyes) was comprised of all eyes with toric IOL powers T3 to T6 to provide applicable data to regions without T2 availability. The analysis found mean ± SD monocular CDVA of −0.01 ± 0.07 logMAR, UDVA of 0.04 ± 0.10 logMAR, UIVA of 0.20 ± 0.14 logMAR, and DCIVA of 0.23 ± 0.13 logMAR. Residual refractive cylinder of 0.26 ± 0.31 D and an average IOL rotation of 1.08 ± 1.26° were observed, with ≤ 1° of rotation in 66% of eyes and ≤ 5° of rotation in 100% of eyes at the one-month timepoint.
Adverse Events
For all eyes, 11 postoperative ocular AEs were identified: 1 mild case of CME, 9 cases of dry eye requiring lubricants, and 1 case of posterior capsulotomy (Nd:YAG [Neodymium-doped Yttrium Aluminum Garnet] laser) due to capsule fibrosis noted intraoperatively. No non-ocular AEs or device deficiencies were identified, and no cases of postoperative posterior capsular opacification (PCO) were observed within one-month postoperation (Table 4). Three patients complained of negative dysphotopsia at their one-day postoperative appointment with descriptions of a dark crescent in their temporal vision; however, these were all completely resolved by their one-month assessments.
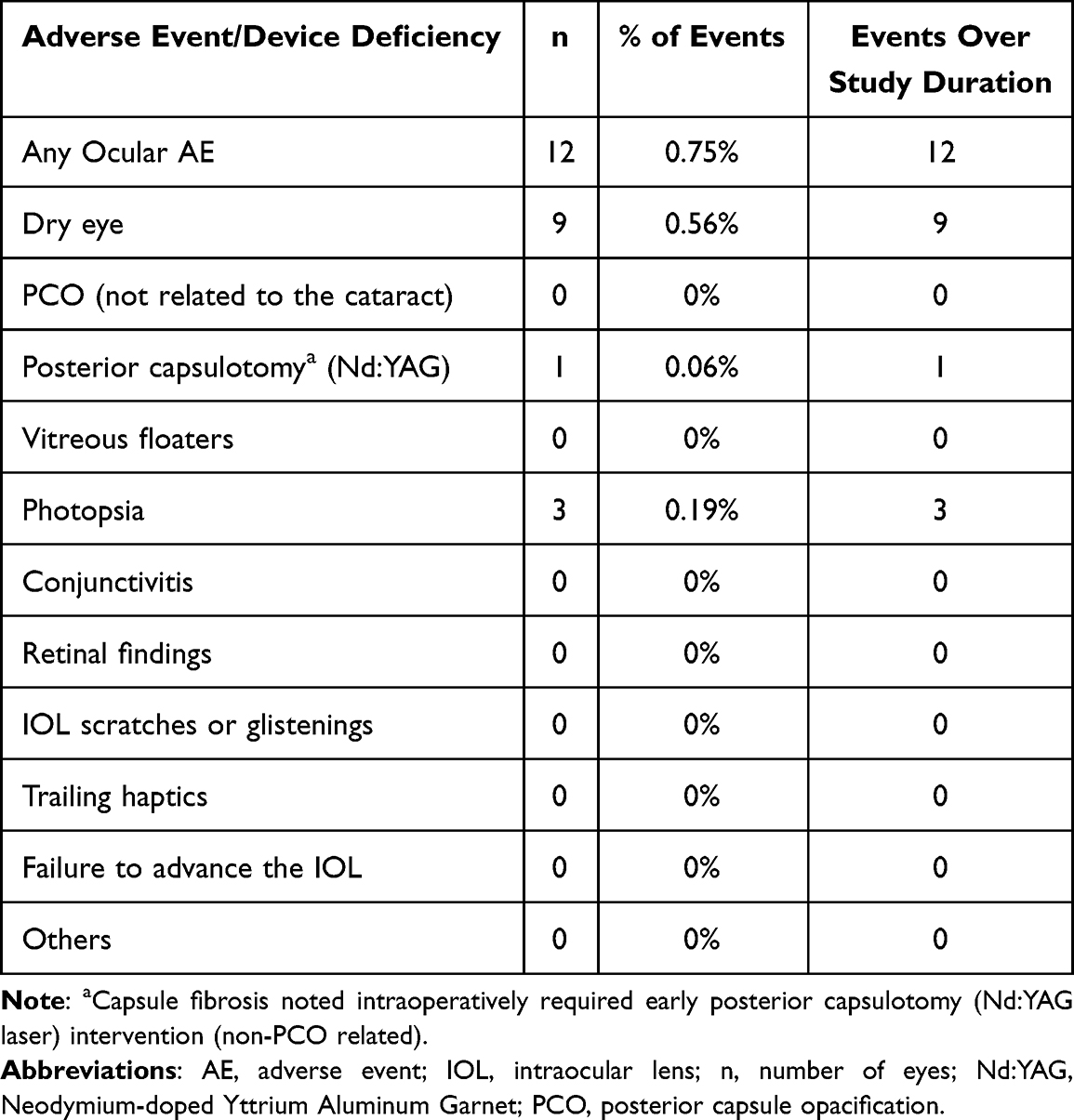 |
Table 4 Summary of All Ocular Adverse Events and Device Deficiencies |
Discussion
This study investigated the real-world visual and refractive outcomes, rotational stability and AEs of the Clareon AutonoMe monofocal toric IOLs postoperatively at one-month.
The results show that the IOL performed well with an excellent ability to treat refractive errors of both sphere and cylinder. There was an improvement in CDVA in all eyes from pre to postoperative timepoints. The IOL provided very good monocular UDVA and CDVA, with a mean of 0.03 and −0.01 logMAR, respectively, at one-month postoperative.
Intermediate vision (at 66 cm) for this monofocal toric IOL was very good given that all eyes targeted emmetropia or first minus. DCIVA was slightly worse than UIVA, likely due to the small amount of residual myopia in some patients. The ability to provide intermediate visual acuity may be due to the aspheric lens design, which only partially reduces corneal spherical aberration. This allows some of the natural depth of focus provided by the cornea to be retained, while still aiming to improve quality of vision compared to a spherical monofocal IOL.8,9
The mean monocular UIVA and DCIVA outcomes of 0.22 and 0.24 logMAR, respectively at 66 cm (for all eyes) in this study are consistent with the findings of Micheletti et al4 and Blehm and Hall5 published in 2023. Micheletti et al4 compared the Clareon monofocal non-toric IOL with the Eyhance monofocal Toric IOL (Johnson & Johnson, USA) in a binocular study design with 155 patients per group and found non-inferior intermediate vision results to those reported for Clareon monofocal toric IOLs in this current study: Clareon non-toric DCIVA of 0.24 ± 0.11 logMAR (n=155) at 3-months. Blehm and Hall5 also found binocular UIVA of 0.24 ± 0.14 logMAR and DCIVA of 0.23 ± 0.14 logMAR for the Clareon monofocal non-toric IOL at 3-months postoperative. These results indicate that Clareon monofocal IOLs provide good intermediate vision at 66 cm, enabling patients to perform tasks such as reading vehicle dashboards, working on laptops or tablets, and using smart phones without spectacle correction.
One of the key attributes of a toric IOL is its ability to treat astigmatism consistently and accurately, reducing preoperative corneal cylinder to minimize postoperative refractive astigmatism.10 In this cohort, postoperative absolute magnitude of refractive astigmatism was very low and was consistently low across the different toric IOL cylinder power steps, based on the results of the first-eye only analysis. This indicates that the IOL performs well in this area. SIA was low magnitude for the studied combination of a 2.2 mm temporal clear corneal incision, wound-assisted implantation of the Clareon monofocal toric IOL using the AutonoMe injector system. At such a low centroid vector magnitude, direction becomes irrelevant, but it is interesting to note that direction of individual SIA vectors was quite randomly distributed, making predictions of individual eye SIA extremely difficult. Such a low magnitude SIA is beneficial in providing accurate refractive astigmatic outcomes in terms of predictability across the cohort. These results for refractive astigmatism and SIA are similar to recent findings reported by Connell et al.11
Regarding study design, the one-month follow-up based on the surgeon’s standard of care provides data from the point where both the eye and toric IOL are considered postoperatively stable.12 In terms of toric IOL stability, according to current literature, the majority of IOL rotation and fixation in the bag usually occurs in the first few hours postoperatively with little movement observed after, which is consistent with these study outcomes.13,14
From immediately after surgery while the patient was supine, the IOL demonstrated excellent rotational stability with minimal rotation, averaging 1.02° of absolute rotation up to one week postoperatively and no movement seen in the subsequent visit. This amount of rotation would have little impact on the refractive error and is not considered clinically relevant. There was only one case reported of an IOL that rotated 6°, which occurred in an eye with capsular fibrosis noted intraoperatively.
Walters et al6 investigated the postoperative rotational stability of the Clareon monofocal non-toric IOLs with toric markings per ISO protocol for new IOL designs. Their findings showed a mean absolute IOL rotation of 1.56° on day one and 1.96° at 6 months with 93.5% of eyes with an absolute IOL rotation of ≤ 5°. Compared to those outcomes, our study exhibited even better results with the actual toric models (Table 3). Connell et al11 have reported outcomes from baseline (EOS) to a final assessment from 3-weeks to 6-months postoperative that were higher than identified in our investigation. Their study was also a retrospective real-world analysis, but the duration of follow-up was longer and this may have impacted the results.11 In a 2018 study comparing two toric IOLs, Lee and Chang13 found that the mean rotation of AcrySof IQ toric IOLs (the parent to Clareon toric IOLs) was 2.72° (95% confidence interval [CI]: 2.35–3.08°; n=626), and the mean rotation of the Tecnis Toric IOL (Johnson & Johnson, USA) was 3.79° (95% CI: 3.36–4.22°; n=647). In context with other IOL platforms, the Connell et al11 study reported comparable results between the Clareon and Tecnis Toric II platform with Eyhance Toric IOLs (p>0.05) over a longer period, while a study from 2022 also investigating IOL rotation also at one month found that the Tecnis Toric II IOL (Johnson and Johnson, USA) deviated from its intended position by 4.7 ± 4.2°, while the Hoya XY-1 IOL (HOYA Surgical Optics) rotated by 5.43 ± 4.67°.15
The role of fibronectin-binding between the IOL and the posterior capsule is important in maintaining IOL stability and may result in less IOL rotation within one month.15 In 2022, Jaitli et al16 observed that fibronectin adsorption significantly increased adhesion forces between acrylic foldable IOLs and the posterior capsule at physiological temperature; this increased adhesion may impact the stability and positioning of the IOL within the eye. One of the 2 reasons as to why the Clareon toric IOL shows such good rotational stability may be due to the material having a fibronectin-binding surface that gives it excellent capsular adhesion. Another reason for the high stability may be related to unfolding speed, with slightly more rapid unfolding possibly allowing the IOL to be completely expanded within the capsular bag at the conclusion of the operation, following removal of viscoelastic. This should allow for more stable contact of the posterior IOL surface and haptics with the capsule to hold it in place accurately. Understanding how fibronectin interacts with IOLs and the impact of surface modifications is crucial for optimizing IOL design and minimizing complications such as PCO in clinical practice.16
The rate of AEs in this study was very low, with only 1 eye of 1 subject having a serious event of postoperative CME. All eyes were prophylactically treated with topical steroid (dexamethasone four times daily for one month) and non-steroidal drops (ketorolac twice daily for two weeks) in an attempt to prevent CME, although occurrence is still possible and unrelated to the specific IOL. Postoperative rates of dry eye were relatively low considering the average age of the study population, which coincides with a higher rate of pre-existing dry eye. One eye required postoperative Nd:YAG capsulotomy within the one-month follow-up period for capsular fibrosis which was noted intraoperatively, relating to a very dense posterior subcapsular cataract and not to postoperative development of PCO. Otherwise, no postoperative PCO was observed within the follow-up period.
One limitation of the study design was its retrospective nature and evaluation of real-world cases of eyes that underwent cataract surgery by a single surgeon. Additionally, only one-month postoperative data were assessed, which, although within standard of care, provides only short to medium-term information on IOL safety and performance. Finally, IOL rotation and other aspects may be more variable in eyes with higher toric powers, few of which were available for evaluation in this dataset (following the expected population distribution).
Conclusion
Clareon monofocal toric IOLs provided excellent distance and functional intermediate visual acuities, minimal rotation following implantation, and low residual refractive astigmatism while exhibiting a low incidence of AEs.
Acknowledgments
The manuscript writing and editorial services were provided by Anshul Tank, PharmD and Ramandeep Singh, PhD (both employed by Alcon). The authors would also like to thank Val Injev, MBA, PE for his valuable inputs in the preparation of this manuscript.
Funding
This study was funded by Alcon Research LLC, Fort Worth, TX.
Disclosure
Ben LaHood is a consultant for Alcon, Zeiss, and Rayner. Rachael C Peterson is an employee of Alcon Research LLC.
References
1. Kessel L, Andresen J, Tendal B, Erngaard D, Flesner P, Hjortdal J. Toric intraocular lenses in the correction of astigmatism during cataract surgery: a systematic review and meta-analysis. Ophthalmology. 2016;123:275–286. doi:10.1016/j.ophtha.2015.10.002
2. Xue K, Jolly JK, Mall SP, et al. Real-world refractive outcomes of toric intraocular lens implantation in a United Kingdom National Health Service setting. BMC Ophthalmol. 2018;18:30. doi:10.1186/s12886-018-0692-7
3. Oshika T, Nakano S, Fujita Y, et al. Long-term outcomes of cataract surgery with toric intraocular lens implantation by the type of preoperative astigmatism. Sci Rep. 2022;12:8457. doi:10.1038/s41598-022-12426-8
4. Micheletti JM, Duncan NB, Hall B. Head-to-head comparison of intermediate vision of two monofocal intraocular lenses. Clin Ophthalmol. 2023;17:3983–3990. doi:10.2147/OPTH.S444696
5. Blehm C, Hall B. Evaluation of visual outcomes and 3-month refractive stability of a new hydrophobic acrylic intraocular lens. Clin Ophthalmol. 2023;17:1859–1864. doi:10.2147/OPTH.S415400
6. Walters TR, Lehmann R, Moyes A, French JW, Sreenivasan V, Modi SS. Rotational stability of the Clareon monofocal aspheric hydrophobic acrylic intraocular lens 6 months after implantation. Clin Ophthalmol. 2022;16:401–409. doi:10.2147/OPTH.S348551
7. Zhao H, Chen X, Liu B, Liu X, Liu Y. Accuracy of refractive outcomes using standard or total keratometry for intraocular lens power formulas in conventional cataract surgery. BMC Ophthalmol. 2023;23(1):346. doi:10.1186/s12886-023-03094-x
8. Pérez-Vives C, Ferrer-Blasco T, García-Lázaro S, Albarrán-Diego C, Montés-Micó R. Optical quality comparison between spherical and aspheric toric intraocular lenses. Eur J Ophthalmol. 2014;24(5):699–706. doi:10.5301/ejo.5000440
9. Alarcon A, Cánovas C, Koopman B, Weeber H, Auffarth GU, Piers PA. Enhancing the intermediate vision of monofocal intraocular lenses using a higher order aspheric optic. J Cataract Refract Surg. 2020;36(8):520–527. doi:10.3928/1081597X-20200612-01
10. Ma JJ, Tseng SS. Simple method for accurate alignment in toric phakic and aphakic intraocular lens implantation. J Cataract Refract Surg. 2008;34(10):1631–1636. doi:10.1016/j.jcrs.2008.04.041
11. Connell B, LaHood B. Comparing rotational stability of Clareon and Eyhance Toric IOLs in a real-world setting. Clin Ophthalmol. 2025;19:141–149. doi:10.2147/OPTH.S503337
12. Khan AM, Waldner DM, Luong M, Sanders E, Crichton ACS, Ford BA. Stabilization of refractive error and associated factors following small incision phacoemulsification cataract surgery. BMC Ophthalmol. 2022;22:13. doi:10.1186/s12886-021-02221-w
13. Lee BS, Chang DF. Comparison of the rotational stability of two toric intraocular lenses in 1273 consecutive eyes. Ophthalmology. 2018;125(9):1325–1331. doi:10.1016/j.ophtha.2018.02.012
14. Inoue Y, Takehara H, Oshika T. Axis misalignment of toric intraocular lens: placement error and postoperative rotation. Ophthalmology. 2017;124(9):1424–1425. doi:10.1016/j.ophtha.2017.05.025
15. Osawa R, Sano M, Yuguchi T, Kaiya T, Oshika T. Effects of modified haptics on surgical outcomes and rotational stability of toric intraocular lens implantation. J Cataract Refract Surg. 2022;38(10):648–653. doi:10.3928/1081597X-20220715-02
16. Jaitli A, Roy J, Chatila A, Liao J, Tang L. Role of fibronectin and IOL surface modification in IOL: lens capsule interactions. Exp Eye Res. 2022;221:109135. doi:10.1016/j.exer.2022.109135
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparing Rotational Stability of Clareon and Eyhance Toric IOLs in a Real-World Setting
Connell B, LaHood B
Clinical Ophthalmology 2025, 19:141-149
Published Date: 13 January 2025