Back to Journals » Clinical Ophthalmology » Volume 19
Real-World Visual and Anatomical Outcomes of Laser Therapy versus Intravitreal Anti-Vascular Endothelial Growth Factor Injection for Retinopathy of Prematurity: A 10-Year Retrospective Cohort Study at a Tertiary Center in Thailand
Authors Thanomteeranant S ![]() , Srisombut T
, Srisombut T ![]() , Sriwannavit S, Pongmee P
, Sriwannavit S, Pongmee P ![]() , Sujirakul T
, Sujirakul T ![]() , Thongborisuth T
, Thongborisuth T ![]() , Tipsuriyaporn B
, Tipsuriyaporn B ![]()
Received 15 September 2025
Accepted for publication 19 November 2025
Published 24 November 2025 Volume 2025:19 Pages 4301—4309
DOI https://doi.org/10.2147/OPTH.S562553
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yousef Fouad
Supanat Thanomteeranant,1 Thansit Srisombut,1 Sivapoj Sriwannavit,1 Pharuhad Pongmee,2 Tharikarn Sujirakul,1 Thitiporn Thongborisuth,1 Boontip Tipsuriyaporn1
1Department of Ophthalmology, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 2Department of Pediatrics, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Boontip Tipsuriyaporn, Department of Ophthalmology, Faculty of Medicine Ramathibodi Hospital, Mahidol University, 270 Rama VI Road, Ratchathewi, Bangkok, 10400, Thailand, Tel +6622011526, Email [email protected]
Purpose: To assess the visual and anatomical outcomes of retinopathy of prematurity (ROP) after treatment with laser therapy versus intravitreal anti-vascular endothelial growth factor (anti-VEGF) in real-world practice.
Methods: This retrospective cohort study included preterm infants with treatment-requiring ROP that underwent either laser indirect ophthalmoscopy (LIO) or intravitreal anti-VEGF therapy at Ramathibodi Hospital from January 2012 to October 2023.
Results: This study included 52 patients (104 eyes). The anti-VEGF (18 patients: 36 eyes) and LIO (34 patients: 68 eyes) groups had comparable baseline characteristics, including mean gestational age (25.80± 2.81 vs 25.89± 3.84 weeks; p=0.906), birth weight (693.0± 34.30 vs 784.5± 45.57 g; p=0.170), and mean follow-up duration (4.12± 0.59 vs 4.91± 0.57 years; p=0.361). Treatment occurred significantly earlier in the anti-VEGF group (postmenstrual age 33.94± 0.53 vs 36.30± 0.55 weeks; p=0.006). The anti-VEGF group required more follow-up visits from the initial exam until the complete regression of ROP (20.03± 10.00 vs 11.80± 6.03; p< 0.001). The mean final visual acuity (VA) was similar between the anti-VEGF and LIO groups (logMAR 0.490 vs 0.480; p=0.852), although Zone I eyes treated with anti-VEGF tended to have better VA. Among Zone I eyes, those treated with anti-VEGF had significantly less myopia (mean spherical equivalent: − 0.60 vs − 12.30 D; p=0.007). Only the anti-VEGF group underwent secondary treatment, mainly for persistent avascular retina (44.4% vs 0%; p< 0.001), and had treatment failure (16.7% vs 0%; p=0.002).
Conclusion: Both anti-VEGF and laser therapy demonstrated nonsignificant difference in functional and anatomical outcomes in treatment-requiring ROP. Notably, Zone I eyes treated with anti-VEGF exhibited significantly less myopia versus those treated with LIO. However, the anti-VEGF group required significantly more hospital visits and secondary treatments.
Keywords: retinopathy of prematurity, laser indirect ophthalmoscope, anti-VEGF treatment
Introduction
The World Health Organization recognizes retinopathy of prematurity (ROP) as a significant cause of preventable childhood blindness and visual impairment worldwide.1–3 Annually, approximately 32,300 infants globally develop permanent visual impairment due to ROP, with nearly 20,000 developing complete blindness or severe visual loss.4 In Thailand, 40.7% of preterm infants were affected by ROP from 2006 to 2010.5 ROP is a retinal vasoproliferative disorder that occurs due to the incomplete development of retinal vessels in premature infants. This vascular immaturity results in peripheral retinal ischemia, triggering the release of vascular endothelial growth factor (VEGF) and causing pathologic neovascularization.6 These abnormal vessels extend into the vitreous at the junction between vascular and avascular retina, progressing in a staged pattern. If left untreated, ROP can result in complications such as vitreous hemorrhage, tractional retinal detachment, and even blindness due to total retinal detachment and retrolental fibrovascular proliferation.7–10 The major risk factors that contribute to the development of ROP include young gestational age (GA), low birth weight, low Apgar scores, and prolonged exposure to supplemental oxygen.11–14 The current treatment guidelines are based on the Early Treatment for Retinopathy of Prematurity (ETROP) study, which established intervention thresholds for high-risk disease: Zone I and any-stage ROP with plus disease; Zone I and stage 3 ROP without plus disease; and Zone II and stage 2–3 ROP with plus disease.8 Its traditional treatments include cryotherapy and laser photocoagulation.8,11 More recently, intravitreal anti-VEGF agents (eg, bevacizumab and ranibizumab) have emerged as another option that offers potential advantages in preserving the visual field and reducing myopia,15,16 although there are concerns about its systemic absorption and long-term safety.7,17 However, few long-term comparative analyses exist from Southeast Asia.
This retrospective cohort study evaluated the anatomical and visual outcomes of ROP in infants treated with laser therapy or intravitreal anti-VEGF at a tertiary care center in Thailand. The anti-VEGF therapy was preferred for cases of aggressive ROP involving zone I or posterior zone II, or in the patients who were unstable for laser photocoagulation. The laser treatment was selected for eye with active disease located in zone II or more anterior region, or frequent follow-up was not feasible. By analyzing real-world data spanning a decade, we aim to contribute valuable evidence for guiding clinical decision-making in managing ROP, particularly in middle-income settings wherein both modalities are utilized.
Patients and Methods
This retrospective cohort analysis recruited preterm infants diagnosed with treatment-requiring ROP at Ramathibodi hospital from January 2012 to October 2023. The study protocol was approved by the human research ethics committee of the Faculty of Medicine, Ramathibodi Hospital, Mahidol University, and adhered to the Declaration of Helsinki (COA. No. MURA2023/847).
The inclusion criteria were as follows: (1) preterm infants with treatment-requiring ROP based on the ETROP criteria; (2) received primary treatment with laser indirect ophthalmoscopy (LIO) or intravitreal anti-VEGF injections; and (3) with follow-up data at Ramathibodi Hospital until at least 1 year of age. According to the ETROP criteria, cases of ROP that require treatment include the following: Zone I and any-stage ROP with plus disease; Zone I and stage 3 ROP without plus disease; and Zone II and stage 2–3 ROP with ≥2 quadrants of plus disease. Cases of aggressive posterior ROP (APROP), a rapidly progressing and severe form of ROP that primarily occurs in the posterior retina (Zone I or posterior Zone II), were also included.
The exclusion criteria were as follows: (1) those with ROP disease characteristics other than the aforementioned; (2) ocular structural abnormalities with a clinically significant impact on study assessments; (3) medical conditions or clinically significant comorbidities that could impact study procedures or efficacy assessments; (4) a history of hypersensitivity to any of the investigational treatments; and (5) incomplete medical data or loss to follow-up after treatment.
The choice of ROP treatment was individualized based on disease zone and stage, the presence of APROP, and socioeconomic factors affecting follow-up adherence. Cases of Zone I ROP, APROP, or posterior Zone II involvement were preferentially treated with intravitreal anti-VEGF agents due to their favorable anatomical outcomes and peripheral retina preservation. Conversely, laser photocoagulation was preferred for cases with more anterior disease. Additionally, laser therapy was also preferred if frequent follow-up could not be ensured due to limited parental resources or transportation barriers; this could reduce the risk of unmonitored disease recurrence and the need for urgent retreatment.
The primary outcomes included (1) visual outcomes (ie, visual acuity [VA]) assessed via preferential looking tests, and (2) anatomical outcomes assessed via ophthalmoscopy or fundus camera imaging (Retcam or Phoenix Icon) at a minimum age of 1 year. According to the World Health Organization, a VA of 20/70 or better is considered normal or indicative of mild visual impairment that rarely interferes with daily activities. This was the standard used to evaluate visual outcomes. Favorable outcomes were defined as a regression of plus disease or neovascularization and an attached retina at the posterior pole. Meanwhile, unfavorable outcomes were defined as the presence of a detached retina at the posterior pole or abnormal structures (eg, retinal fold, disc dragging, and macular dragging) after treatment.18 The recurrence of ROP was defined as reactivation following a period of regression, showing a new demarcation line, ridge, extraretinal fibrovascular proliferation (EFP) or leakage on fluorescein angiography, along with or without a recurrence of plus disease. The reactivation at the site of the second arrest of intrinsic retinal vasculature following initial anterior progression was considered an anterior recurrence; recurrence at least three-disc diameters posterior to the current area of vascular arrest was considered a posterior recurrence. While persistence was defined as insufficient regression following therapy19 and failure was defined as no sign of regression or show disease progression after the treatment.
The secondary outcomes included (1) demographic data, (2) the incidence of recurrent disease requiring retreatment prior to 54 weeks of postmenstrual age (PMA), (3) the total number of clinic visits, (4) changes in visual acuity from baseline at one year of age to the last follow-up, (5) refractive outcomes at the final follow-up, and (6) orthoptic status. The number of clinic visits was counted from the initial retinal examination until complete ROP regression, defined as the resolution of all active disease signs (ie, disappearance of plus disease, ridge involution, and absence of neovascular/fibrovascular activity).9
Statistical Analysis
Statistical analysis was done using mixed-effect linear regression model adjusted for zone of ROP. Repeated measures and inter-eye correlations were accounted for in the model as random and fixed intercepts, respectively. Categorical data were compared between treatment groups using chi-square and Fisher-exact test as appropriate. Continuous data were presented as mean (±SD) or median (IQR) as appropriate. Categorical data were presented as frequency and percentage. All statistical procedure were performed using Stata (version 18.0), with p<0.05 considered statistically significant.
Results
A total of 52 preterm infants (104 eyes) with treatment-requiring ROP were included. Among them, 18 patients (36 eyes) were treated with intravitreal anti-VEGF injection, whereas 34 patients (68 eyes) underwent LIO. In the anti-VEGF group, 5 eyes were treated with ranibizumab, and the remaining 31 eyes received bevacizumab. There were 7 eyes diagnosed with AP-ROP. The demographic and baseline clinical characteristics are summarized in Table 1.
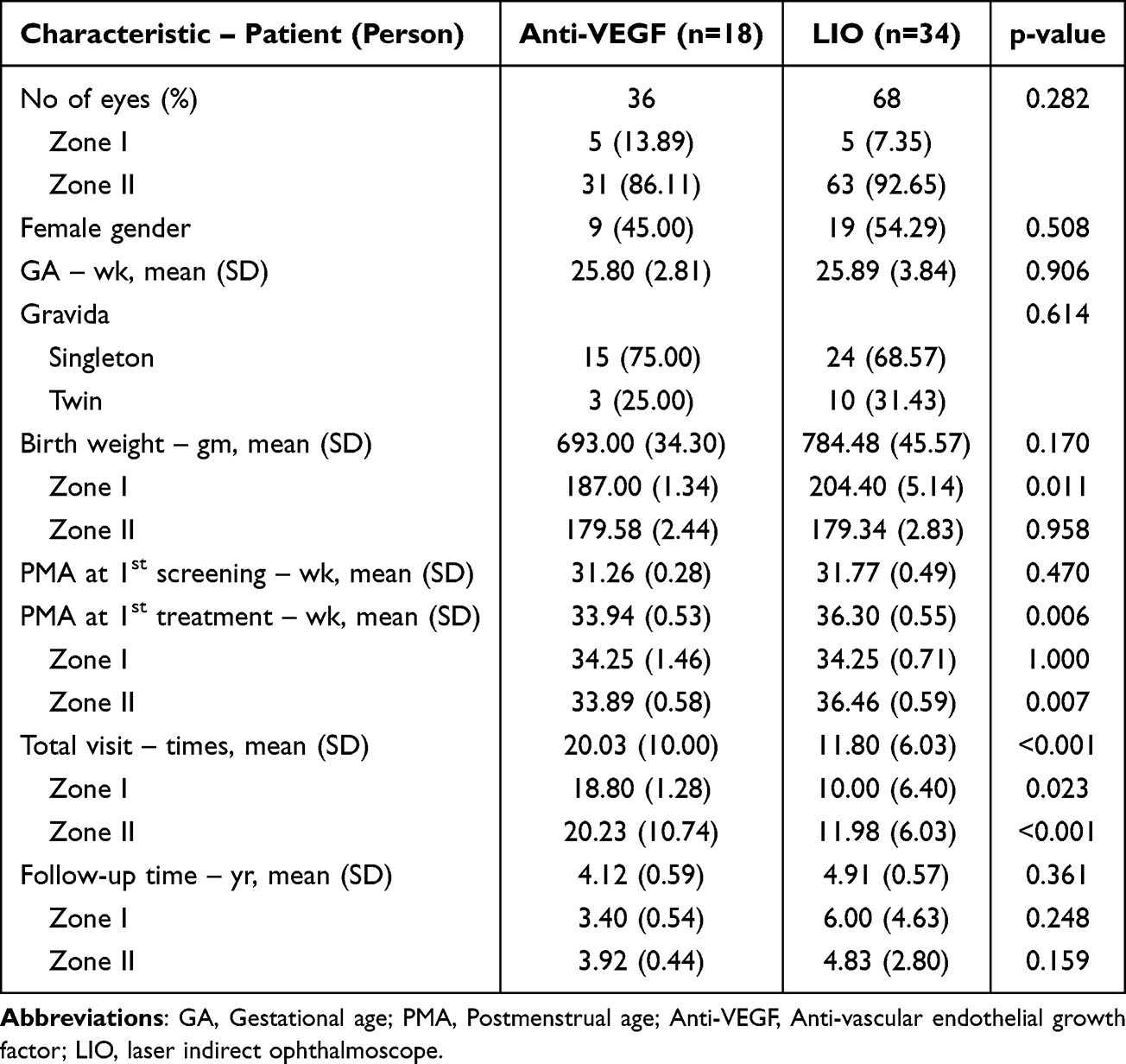 |
Table 1 Demographic Data and Characteristics of Preterm Infants with ROP Requiring Treatment |
The anti-VEGF and LIO groups were comparable in terms of mean GA at birth (p=0.906) and birth weight (693.00±34.30 vs 784.50±45.57 g; p=0.170). The sex distribution (p=0.508) and twin gestation rates (p=0.614) were also similar. In both anti-VEGF and LIO groups, most cases were classified as Zone II disease (86.11% vs 92.65%). Zone I disease was more frequently treated with anti-VEGF (13.89% vs 7.35%). The mean PMA at first screening was comparable between the anti-VEGF and LIO groups (p=0.470). However, treatment was administered significantly earlier in the anti-VEGF group (33.94±0.53 vs 36.30±0.55 weeks; p=0.006). Among eyes with Zone II disease, those treated with anti-VEGF also received earlier intervention versus those treated with LIO (33.89 vs 36.46 weeks; p=0.007). The mean number of follow-up visits was significantly higher in the anti-VEGF group (20.03±10.00 vs 11.80±6.03 visits; p<0.001), and this trend remained consistent across both subgroups of Zone I (18.80 vs 10.00 visits; p=0.023) and Zone II (20.23 vs 11.98 visits; p<0.001) disease. The average follow-up duration was not significantly different (p=0.361).
Table 2 presents the visual outcomes, specifically VA and refractive outcomes. After excluding those lost to follow-up, 31 eyes in the anti-VEGF group and 54 eyes in the LIO group remained. The mean final logMAR VA for all eyes was similar between the anti-VEGF and LIO groups (p=0.852). The Zone I subgroup treated with anti-VEGF had better average VA, although this did not reach statistical significance (p=0.208). Meanwhile, among Zone II eyes, the mean final VA was not significantly different between treatment modalities (p=0.936). The change in VA from baseline was only minimally different between both treatment modalities, as shown in Figure 1.
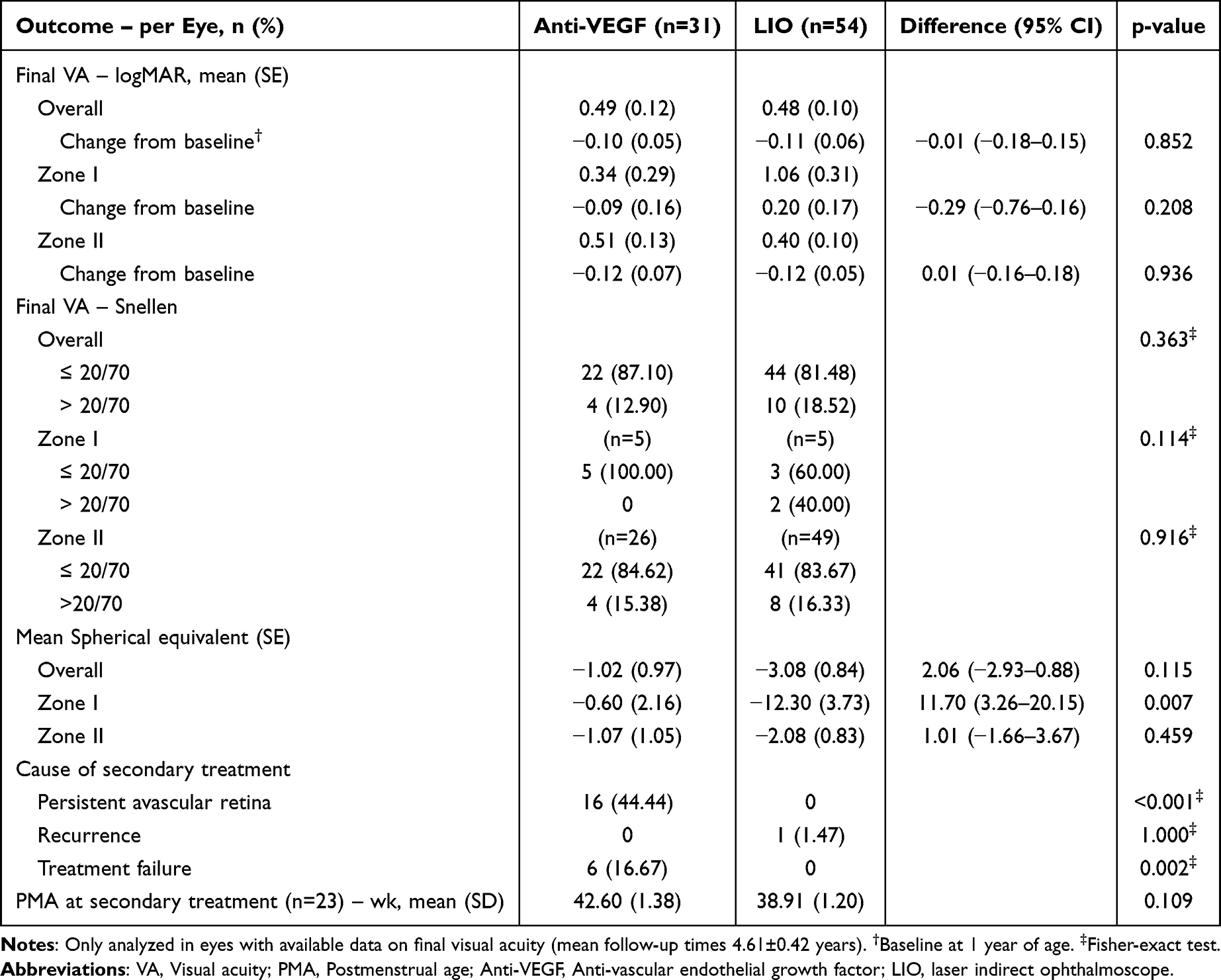 |
Table 2 Visual Acuity, Refractive and Treatment Outcomes Between Anti-VEGF and LIO Group |
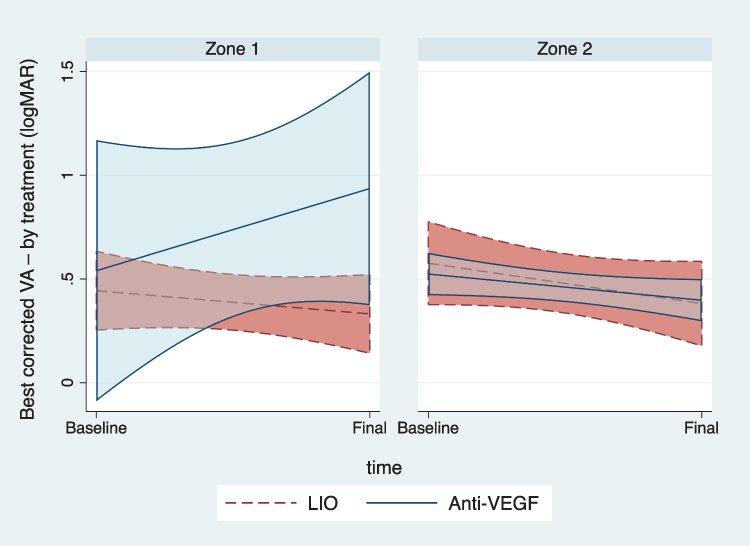 |
Figure 1 Best corrected visual acuity (logMAR) outcomes. Baseline refers to the first measurable visual acuity, obtained within the first year of age in ROP patients using the preferential looking test during an outpatient follow-up visit. Final refers to the visual acuity measured at the last follow-up visit. Abbreviations: LIO, Laser indirect ophthalmoscope; Anti-VEGF, Anti-vascular endothelial growth factor. |
When categorically analyzed using Snellen equivalents, a slightly larger proportion of eyes achieved a VA of at least 20/70 in the anti-VEGF group (p=0.363), and this trend was more pronounced in Zone I eyes, although not significant (p=0.114). Meanwhile, the outcomes of Zone II eyes were nearly identical between treatment modalities.
Regarding refractive outcomes, the anti-VEGF group showed a tendency toward less myopia, with a mean spherical equivalent (SE) of −1.02 D versus −3.08 D in the LIO group (p=0.115). Among Zone I eyes, the anti-VEGF group had significantly less myopia (−0.60 vs −12.30 D; p=0.007). Among Zone II eyes, there was no significant difference in SE between the two modalities p=0.459).
The secondary treatment outcomes are detailed in Table 2. A significantly greater proportion of eyes in the anti-VEGF group required secondary treatment due to persistent avascular retina (44.4% vs 0%; p<0.001). Treatment failure was observed only in the anti-VEGF group and not in the LIO group (16.7% vs 0%; p=0.002). Recurrence occurred in one eye in the LIO group and none in the anti-VEGF group (p=1.000). Additional treatment was done with LIO in both groups. However, only one eye in the anti-VEGF group, which experienced treatment failure, progressed to stage 5A and subsequently underwent pars plana vitrectomy. The anti-VEGF group presented with an older mean PMA at secondary treatment, although this was not statistically significant.
The anatomical and orthoptic outcomes at the final follow-up are shown in Table 3. The unfavorable anatomical outcomes included disc dragging (n=2), macular dragging (n=1), and retinal detachment (n=2, 1 eye in each group), although these complications were rare and not significantly different between groups (p=0.807).
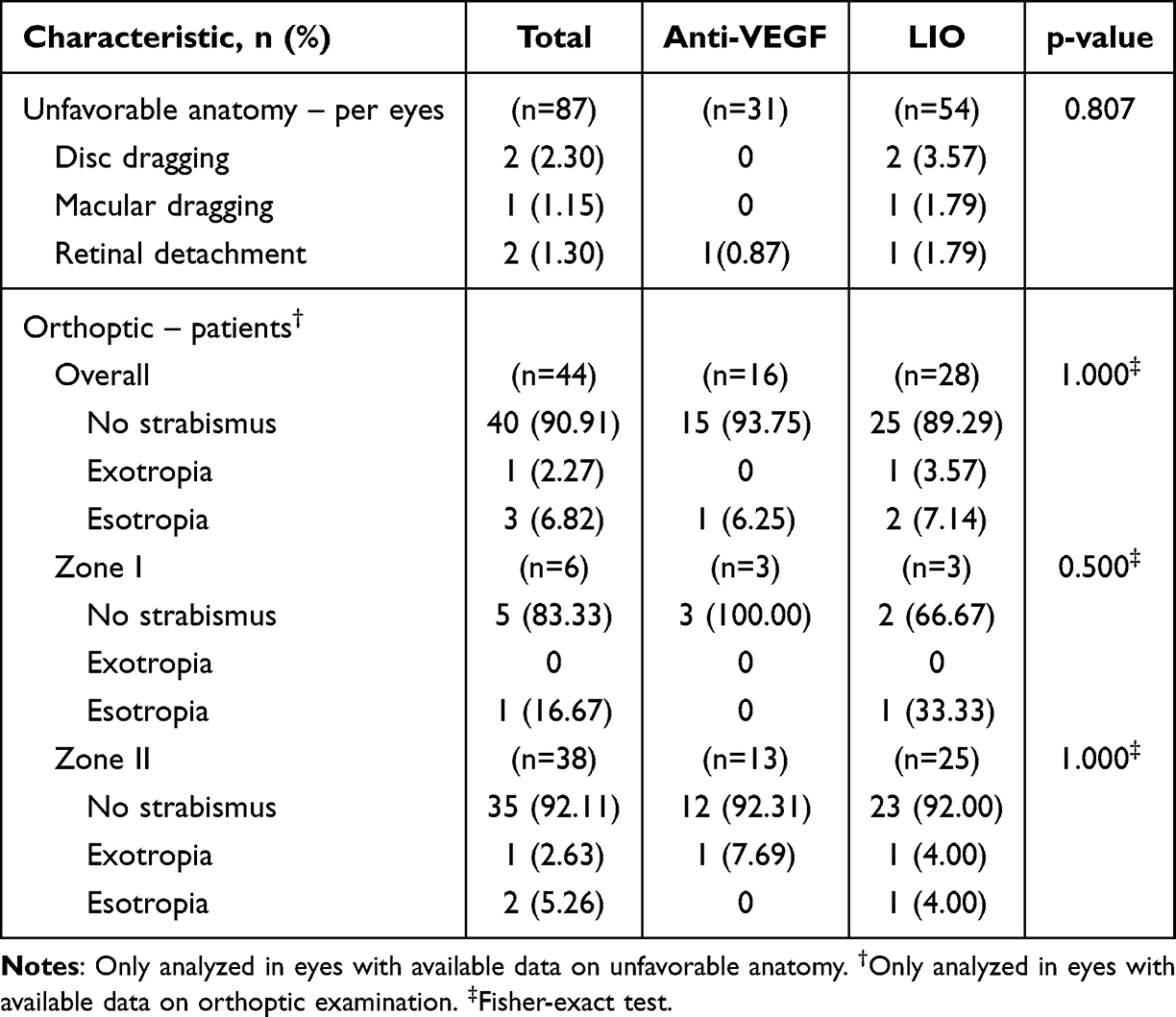 |
Table 3 Unfavorable Anatomical and Orthoptic Outcomes Between Groups at Last Follow-Up |
Orthoptic outcomes were available for 44 patients. Strabismus was observed in 4 patients, with no significant difference between groups (p=1.000). Esotropia was slightly more frequent than exotropia. Among patients with Zone I disease, strabismus developed in only 1 patient in the LIO group (33.3%) and none in the anti-VEGF group (p=0.500). Among those with Zone II disease, the prevalence of strabismus was similar between groups (p=1.000).
Discussion
This study provides a comprehensive comparison of clinical outcomes between intravitreal anti-VEGF therapy and laser photocoagulation in the treatment of ROP. Over a mean follow-up of 4.6 years, no significant difference was found in terms of final visual acuity, anatomical outcomes, or orthoptic results between treatment modalities. However, key differences were noted in the timing of treatment initiation, frequency of hospital visits, and rates of persistent avascular retina and treatment failure.
Compared to previous studies, our cohort had similar demographics in terms of GA and birth weight.17,20,21 Notably, treatment with anti-VEGF was initiated significantly earlier than laser, which aligns with the typical clinical practice of targeting early neovascular activity, particularly in posterior disease.22
The functional outcomes after anti-VEGF therapy and LIO were not significantly difference in Snellen visual acuity at the last follow-up. Likewise, the RAINBOW trial, a landmark Phase III study, demonstrated the non-inferiority of ranibizumab compared to laser therapy in terms of efficacy, with a favorable safety profile.15 Similarly, the BEAT-ROP study highlighted the comparable efficacy of bevacizumab and laser therapy, particularly for Zone I disease, where laser outcomes are historically poorer.7 In Thailand, ranibizumab was administered to patients covered under the government employee health insurance scheme or those with financial support, while bevecizumab was used for other health insurance scheme. In our study, most eyes receiving anti-VEGF therapy were treated with bevacizumab due to its more available and lower cost. To date, no head-to-head trials have compared bevacizumab and ranibizumab for the treatment of ROP. However, several studies suggest that bevacizumab demonstrates comparable efficacy and reproducibility to laser photocogulation, leading to its common use in clinical practice.7,20
In our cohort, particularly in Zone I disease, anti-VEGF treatment resulted in a significantly lower myopic shift compared to laser therapy. In line with this, the literature has consistently reported lower rates of high myopia after anti-VEGF treatment.6,23,24 In contrast, among eyes with Zone II disease, the anti-VEGF and LIO groups had a comparable final spherical, which is consistent with previous findings.6 Despite its effectivity in inducing regression of neovascularization, laser therapy often leads to extensive ablation of the peripheral retina, thereby contributing to ocular growth restriction and myopic progression. This is especially true for Zone I disease, whereas such effects are not significantly observed in Zone II disease.10
Persistent avascular retina was significantly more common in the anti-VEGF, which is in line with previous reports.25,26 Delayed peripheral vascularization is a known concern that necessitates extended surveillance and, if present, secondary laser treatment.27 Laser therapy typically induces regression of neovascular signs within 4–6 weeks. Conversely, anti-VEGF therapy often leads to earlier regression within 1–2 weeks, but it requires prolonged monitoring due to delayed peripheral vascularization, potentially extending beyond 60 weeks PMA.15,20 This is supported by our data as well, seeing that the anti-VEGF group required significantly more hospital visits than the laser group. Long-term follow-up is crucial because late reactivation of ROP can occur even months after initial regression.28,29
One notable limitation of anti-VEGF therapy is treatment failure, as seen in 16.67% of eyes in our cohort. All six eyes with treatment failure have severe disease at baseline, including four with zone I and two with AP-ROP, including 1 eye that progressed to stage 5A and eventually required pars plana vitrectomy. Although relatively rare, this outcome underscores the importance of timely identification and intervention. Conversely, only one recurrence was seen in the laser group. This supports the findings of the ETROP study, which established laser photocoagulation as the gold standard for Type 1 ROP prior to the advent of anti-VEGF agents.8
Despite these challenges, the incidence of strabismus was comparable between the two treatment groups. Strabismus remains a common sequela among ROP survivors, although this is typically influenced by disrupted binocular development and neurodevelopmental comorbidities rather than by the treatment modality itself. Similarly, Geloneck et al and Hwang et al also reported no difference in strabismus rates between eyes treated with laser therapy and anti-VEGF.24,30 This observation is further supported by the recent study, which also noted that the neurodevelopmental and orthoptic parameters were comparable between anti-VEGF and laser-treated infants when adjusted for confounders.31
The anti-VEGF group notably had a prolonged follow-up and increased visit burden. From a practical perspective, these raise concerns about healthcare accessibility and parental compliance, especially in resource-limited settings.30,32 Therefore, despite the clinical advantages of anti-VEGF agents, especially for posterior and aggressive ROP, laser therapy remains a robust alternative, particularly for Zone II disease.
This study has several limitations. First, the retrospective study design carries an inherent risk of selection bias in treatment assignment and reliance on available clinical records, which may have led to incomplete data capture. Second, the sample size was relatively small, especially for Zone I cases, thereby limiting the statistical power for subgroup analysis. Third, in the assessment of VA, using the preferential looking test is less precise compared to formal visual testing. Lastly, the follow-up duration and visit frequency varied between treatment groups, which could influence the detection of recurrence or complications.
Conclusions
Nevertheless, this study offers meaningful insights in terms of long-term comparative outcomes between anti-VEGF and laser therapy in ROP, with a minimum follow-up of one year. Both anti-VEGF and laser appeared to demonstrate nonsignificant difference in functional and anatomical outcomes. In cases of zone I, posterior zone II involvement were preferentially treated with anti-VEGF due to their favorable anatomical outcomes and preservation of the peripheral retina, particularly when regular follow-up could be ensured. These findings meaningfully contribute to our growing understanding of treatment impact in different ROP zones and can be used to support more tailored management strategies in clinical practice. Prospective, multicenter trials are needed to compare each anti-VEGF and quantify the risk and timing of ROP reactivation. Extended follow-up results are needed to assess not only ophthalmological outcomes but also for potential neurodevelopmental effect of anti-VEGF exposure in premature infants.
Disclosure
None of the authors has a financial or proprietary interest in any material or method mentioned. The authors report no conflicts of interest in this work.
References
1. Nair A, El Ballushi R, Anklesaria BZ, Kamali M, Talat M, Watts T. A review on the incidence and related risk factors of retinopathy of prematurity across various countries. Cureus. 2022;14(11):e32007. doi:10.7759/cureus.32007
2. Pizzarello L, Abiose A, Ffytche T, et al. VISION 2020: the right to sight: a global initiative to eliminate avoidable blindness. Arch Ophthalmol. 2004;122(4):615–620. doi:10.1001/archopht.122.4.615
3. Gilbert C. Retinopathy of prematurity: a global perspective of the epidemics, population of babies at risk and implications for control. Early Hum Dev. 2008;84(2):77–82. doi:10.1016/j.earlhumdev.2007.11.009
4. Bowe T, Nyamai L, Ademola-Popoola D, et al. The current state of retinopathy of prematurity in India, Kenya, Mexico, Nigeria, Philippines, Romania, Thailand, and Venezuela. Digit J Ophthalmol. 2019;25(4):49–58. doi:10.5693/djo.01.2019.08.002
5. Alajbegovic-Halimic J, Zvizdic D, Alimanovic-Halilovic E, Dodik I, Duvnjak S. Risk factors for retinopathy of prematurity in premature born children. Med Arch. 2015;69(6):409–413. doi:10.5455/medarh.2015.69.409-413
6. Chen J, Stahl A, Hellstrom A, Smith LE. Current update on retinopathy of prematurity: screening and treatment. Curr Opin Pediatr. 2011;23(2):173–178. doi:10.1097/MOP.0b013e3283423f35
7. Mintz-Hittner HA, Kennedy KA, Chuang AZ. Efficacy of intravitreal bevacizumab for stage 3+ retinopathy of prematurity. N Engl J Med. 2011;364(7):603–615. doi:10.1056/NEJMoa1007374
8. Early Treatment for Retinopathy of Prematurity Cooperative Group. Revised indications for the treatment of retinopathy of prematurity: results of the early treatment for retinopathy of prematurity randomized trial. Arch Ophthalmol. 2003;121(12):1684–1694. doi:10.1001/archopht.121.12.1684
9. Chiang MF, Quinn GE, Fielder AR, et al. International classification of retinopathy of prematurity, third edition. Ophthalmology. 2021;128(10):e51–e68. doi:10.1016/j.ophtha.2021.05.031
10. Mills MD. Evaluating the cryotherapy for retinopathy of prematurity study (CRYO-ROP). Arch Ophthalmol. 2007;125(9):1276–1281. doi:10.1001/archopht.125.9.1276
11. Cryotherapy for Retinopathy of Prematurity Cooperative Group. Multicenter trial of cryotherapy for retinopathy of prematurity: preliminary results. Archiv Ophthalmol. 1988;106(4):471–479. doi:10.1001/archopht.1988.01060130517027
12. Freitas AM, Mörschbächer R, Thorell MR, Rhoden EL. Incidence and risk factors for retinopathy of prematurity: a retrospective cohort study. Int J Retina Vitreous. 2018;4(1):20. doi:10.1186/s40942-018-0125-z
13. Kim SJ, Port AD, Swan R, Campbell JP, Chan RVP, Chiang MF. Retinopathy of prematurity: a review of risk factors and their clinical significance. Surv Ophthalmol. 2018;63(5):618–637. doi:10.1016/j.survophthal.2018.04.002
14. Gaber R, Sorour OA, Sharaf AF, Saad HA. Incidence and risk factors for retinopathy of prematurity (ROP) in biggest neonatal intensive care unit in Itay Elbaroud City, Behera Province, Egypt. Clin Ophthalmol. 2021;15:3467–3471. doi:10.2147/OPTH.S324614
15. Stahl A, Lepore D, Fielder A, et al. Ranibizumab versus laser therapy for the treatment of very low birthweight infants with retinopathy of prematurity (RAINBOW): an open-label randomised controlled trial. Lancet. 2019;394(10208):1551–1559. doi:10.1016/S0140-6736(19)31344-3
16. Pertl L, Steinwender G, Mayer C, et al. A systematic review and meta-analysis on the safety of vascular endothelial growth factor (VEGF) inhibitors for the treatment of retinopathy of prematurity. PLoS One. 2015;10(6):e0129383. doi:10.1371/journal.pone.0129383
17. Murakami T, Okamoto F, Kinoshita T, et al. Comparison of long-term treatment outcomes of laser and anti-VEGF therapy in retinopathy of prematurity: a multicentre study from J-CREST group. Eye. 2023;37(17):3589–3595. doi:10.1038/s41433-023-02559-z
18. Sen P, Abraham S, Jain S, Gopal L, Bhende P. Treatment outcomes of zone 1 retinopathy of prematurity: a study from a tertiary eye care center in South India. Taiwan J Ophthalmol. 2019;9(4):255–261. doi:10.4103/tjo.tjo_62_18
19. Hu J, Blair MP, Shapiro MJ, Lichtenstein SJ, Galasso JM, Kapur R. Reactivation of retinopathy of prematurity after bevacizumab injection. Arch Ophthalmol. 2012;130(8):1000–1006. doi:10.1001/archophthalmol.2012.592
20. Mintz-Hittner HA, Kuffel RR. Intravitreal injection of bevacizumab (avastin) for treatment of stage 3 retinopathy of prematurity in zone I or posterior zone II. Retina. 2008;28(6):831–838. doi:10.1097/IAE.0b013e318177f934
21. Fierson WM, Chiang MF, Good W. Screening examination of premature infants for retinopathy of prematurity. Pediatrics. 2018;142(6). doi:10.1542/peds.2018-3061
22. Linghu D, Cheng Y, Zhu X, et al. Comparison of intravitreal anti-VEGF agents with laser photocoagulation for retinopathy of prematurity of 1627 eyes in China. Front Med Lausanne. 2022;9:911095. doi:10.3389/fmed.2022.911095
23. Li Z, Zhang Y, Liao Y, Zeng R, Zeng P, Lan Y. Comparison of efficacy between anti-vascular endothelial growth factor (VEGF) and laser treatment in Type-1 and threshold retinopathy of prematurity (ROP). BMC Ophthalmol. 2018;18(1):19. doi:10.1186/s12886-018-0685-6
24. Geloneck MM, Chuang AZ, Clark WL, et al. Refractive outcomes following bevacizumab monotherapy compared with conventional laser treatment: a randomized clinical trial. JAMA Ophthalmol. 2014;132(11):1327–1333. doi:10.1001/jamaophthalmol.2014.2772
25. Tan TF, Tay SA, Agarwal-Sinha S, Tan GSW, Wu WC, Tsai ASH. Persistent avascular retina in retinopathy of prematurity. Graefes Arch Clin Exp Ophthalmol. 2025;263(8):2177–2190. doi:10.1007/s00417-025-06820-x
26. Murakami T, Nudleman E. Persistent avascular retina in eyes with retinopathy of prematurity: a comprehensive review. Taiwan J Ophthalmol. 2025. doi:10.4103/tjo.TJO-D-24-00157
27. Chen J, Hao Q, Zhang J, Du Y, Chen H, Cheng X. The efficacy and ocular safety following aflibercept, conbercept, ranibizumab, bevacizumab, and laser for retinopathy of prematurity: a systematic review and meta-analysis. Ital J Pediatr. 2023;49(1):136. doi:10.1186/s13052-023-01543-3
28. Yasin A, Sinha S, Smith R, Jain SF, Hejkal T, Rychwalski P. Reactivation of retinopathy of prematurity six years after intravitreal injection of bevacizumab. J Aapos. 2023;27(4):236–239. doi:10.1016/j.jaapos.2023.05.008
29. Morin J, Luu TM, Superstein R, et al. Neurodevelopmental outcomes following bevacizumab injections for retinopathy of prematurity. Pediatrics. 2016;137(4). doi:10.1542/peds.2015-3218
30. Hwang CK, Hubbard GB, Hutchinson AK, Lambert SR. Outcomes after intravitreal bevacizumab versus laser photocoagulation for retinopathy of prematurity: a 5-year retrospective analysis. Ophthalmology. 2015;122(5):1008–1015. doi:10.1016/j.ophtha.2014.12.017
31. Barbeau LDY, Agarwal S. Does the newer anti-vegf therapy impact neurodevelopmental outcomes more than conventional laser therapy in infants treated for retinopathy of prematurity? J AAPOS. 2019;23(4):e18–e9. doi:10.1016/j.jaapos.2019.08.061
32. Senjam SS, Chandra P. Retinopathy of prematurity: addressing the emerging burden in developing countries. J Family Med Prim Care. 2020;9(6):2600–2605. doi:10.4103/jfmpc.jfmpc_110_20
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.