Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Real-World Experience with Upadacitinib in Patients with Atopic Dermatitis and Hidradenitis Suppurativa: A Dual-Center Case Series
Authors Martora F ![]() , Megna M
, Megna M ![]() , Molinelli E, Gambini D, Simonetti O, Cimmino M, Napolitano M
, Molinelli E, Gambini D, Simonetti O, Cimmino M, Napolitano M ![]()
Received 8 December 2025
Accepted for publication 3 February 2026
Published 7 February 2026 Volume 2026:19 583223
DOI https://doi.org/10.2147/CCID.S583223
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Monica K. Li
Fabrizio Martora,1,* Matteo Megna,1,* Elisa Molinelli,2 Daisy Gambini,2 Oriana Simonetti,2 Marianna Cimmino,1 Maddalena Napolitano1
1Dermatology Unit, Department of Clinical Medicine and Surgery, University of Naples Federico II, Naples, Italy; 2Dermatology Unit, Department of Clinical and Molecular Sciences, Polytechnic Marche University, Ancona, Italy
*These authors contributed equally to this work
Correspondence: Fabrizio Martora, Section of Dermatology - Department of Clinical Medicine and Surgery, University of Naples Federico II, Via Pansini 5, Naples, 80131, Italy, Tel +39-081-7462457, Fax +39-081-7462442, Email [email protected]
Abstract: Hidradenitis suppurativa (HS) is a chronic, relapsing inflammatory skin disease with significant impact on quality of life and limited effective therapeutic options. Although biologic agents targeting TNF-α and IL-17A are approved for moderate-to-severe HS, many patients exhibit inadequate or unsustained responses. Janus kinase (JAK) inhibitors have recently emerged as potential alternatives. Upadacitinib, a selective JAK1 inhibitor approved for several immune-mediated disorders including atopic dermatitis (AD), may represent a novel therapeutic strategy. We conducted a real-world case series evaluating the efficacy and safety of upadacitinib in 10 patients with severe, refractory AD and/or HS treated at two dermatology centers. Patients received either 30 mg or 15 mg daily without concomitant systemic therapies and were assessed at baseline, 4 months, and 12 months using validated clinical scores. AD outcomes included EASI, Peak Pruritus NRS, and DLQI, while HS outcomes included IHS4, HiSCR, pain VAS, and DLQI. Marked clinical improvement was observed in AD, with progressive reductions in disease severity, pruritus, and quality-of-life impairment over 12 months. In contrast, HS patients demonstrated more modest improvements, with limited achievement of HiSCR despite reductions in IHS4 and pain scores. Treatment was well tolerated, with no reported adverse events. These findings suggest that upadacitinib is highly effective for AD, while its benefit in HS appears less pronounced, highlighting the need for larger controlled studies to better define its therapeutic role in HS.
Keywords: rifampicin, clindamycin, adalimumab, JAK1 inhibitors, treatment
Hidradenitis suppurativa (HS) is a chronic, inflammatory, and recurrent skin disorder that primarily affects the hair follicles. It is widely recognized as a debilitating condition with a complex and multifactorial pathogenesis involving genetic, immunological, and environmental factors. Clinically, HS is characterized by the development of painful, deep-seated nodules, abscesses, and sinus tracts that most commonly appear in intertriginous regions of the body such as the axillae, inframammary folds, groin, buttocks, and perineum. The disease often follows a relapsing course, significantly impairing quality of life for affected individuals.1,2
Managing patients with moderate-to-severe HS continues to represent a considerable clinical challenge, as treatment frequently requires a combination of systemic therapies alongside meticulous local wound care. To date, only two biologic agents—adalimumab, an anti–TNF-α monoclonal antibody, and secukinumab, an IL-17A inhibitor—have received approval from both the FDA and EMA specifically for the treatment of HS. Despite these advances, many patients experience inadequate response or eventual loss of efficacy, highlighting the unmet need for additional therapeutic options.3,4
Recently, Janus kinase (JAK) inhibitors have emerged as a promising new class of therapies for HS. Early clinical evidence, particularly from Phase II trials and real-world cohort studies, suggests that oral JAK1 inhibitors may provide meaningful clinical benefit. Several of these agents are now being further investigated in Phase III studies to better define their efficacy and safety profile.4
Upadacitinib, a selective JAK1 inhibitor, has already been approved for the treatment of multiple immune-mediated inflammatory diseases, including rheumatoid arthritis and atopic dermatitis (AD) in both adults and adolescents aged 12 years and older.4 Building on this background, we present a real-world case series evaluating the efficacy and safety of upadacitinib in patients with moderate-to-severe atopic dermatitis as well as in those with moderate-to-severe HS who had previously failed conventional biologic therapies such as TNF-α or IL-17 inhibitors.
In our study 10 patients with atopic dermatitis (AD) severe and refractory HS both were treated with upadacitinib at our department and at the department of Dermatology, Polytechnic Marche University, Ancona, Italy.
Dosing regimens varied based on patient’s comorbidities and disease severity: 8 patients received 30 mg daily and two received 15 mg daily. No concomitant systemic therapies were permitted. All patients received standard wound care and routine laboratory monitoring throughout treatment. The inclusion and exclusion criteria are the same as those used for all clinical studies conducted on HS and AD.
Patients were assessed at baseline, 4 months, and 12 months using the International Hidradenitis Suppurativa Severity Score System (IHS4), achievement of IHS4-55, Visual Analog Scale (VAS) for pain, and Dermatology Life Quality Index (DLQI) for HS while were assessed EASI (Eczema Area and Severity System), Peak Pruritus Numerical Rating Scale (PP-NRS) and DLQI for AD.
The cohort comprised 5 females and 5 males, with a mean age of 28.3 years (SD ±13.78) and mean BMI of 27.11 kg/m2 (SD ±3.11). Comorbidities and previous treatments are reported in Table 1.
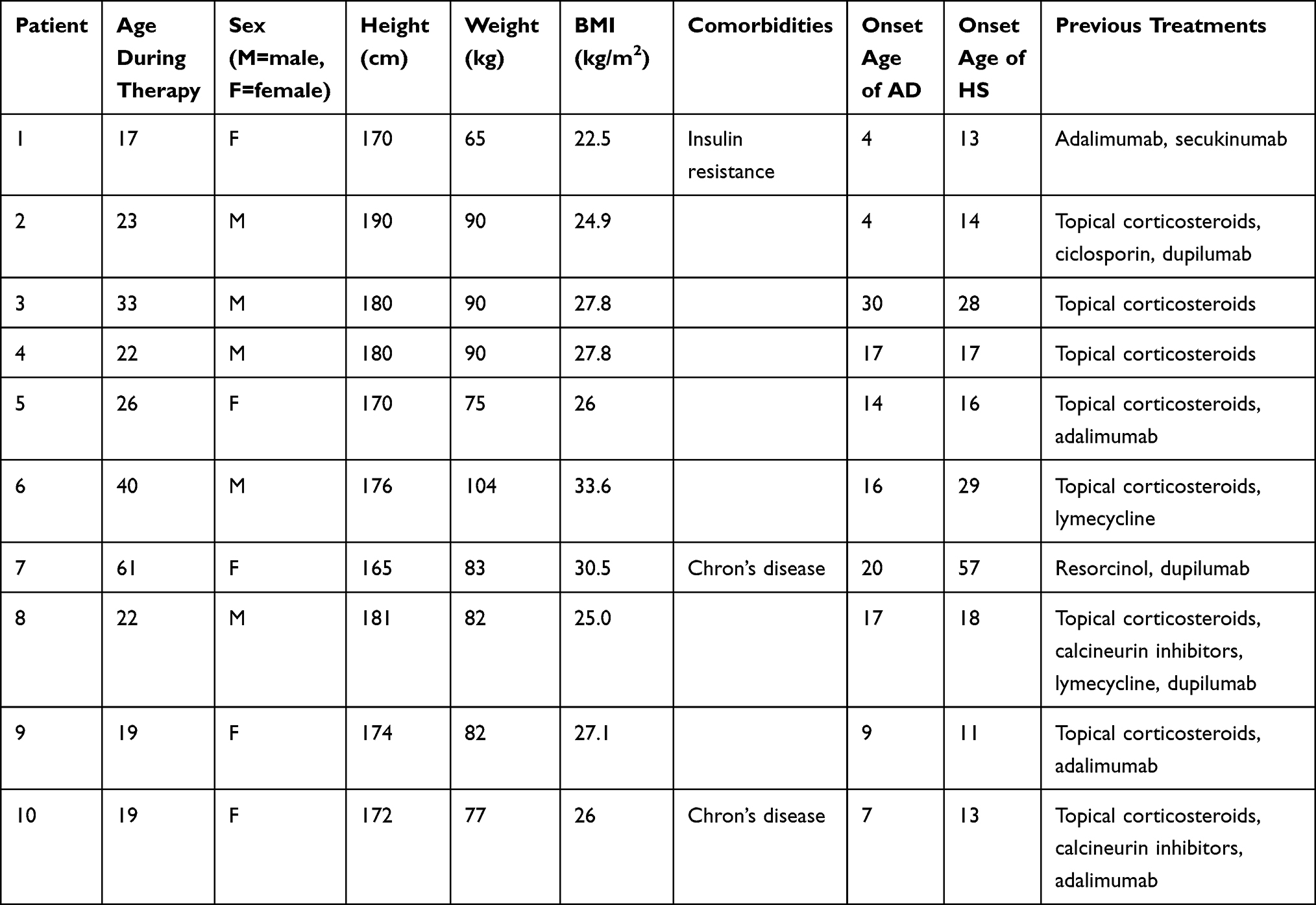 |
Table 1 All the Patients Had AD and HS |
Regarding AD at baseline, the mean EASI was 19.1, PP-NRS was 8.2 and DLQI was 17.7. At 4 months, these values improved to EASI =9.8, PP-NRS= 5 and DLQI = 9.3. At 12 months, further improvements were observed: EASI=4.7, PP-NRS= 0.2 and DLQI= 4.3 (Figure 1).
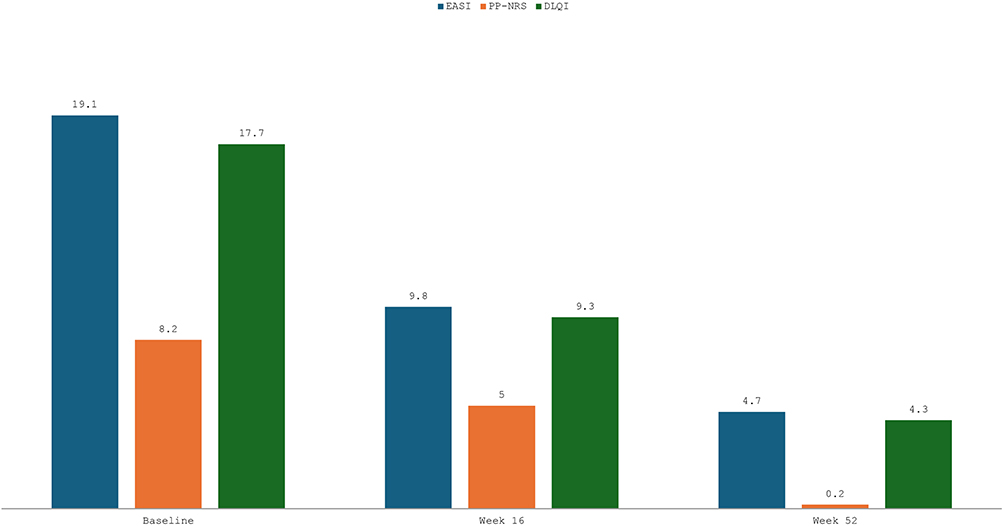 |
Figure 1 Data regarding Atopic Dermatitis score. |
At baseline, the mean IHS4 score was 14; mean VAS pain score (HS), 6.2; and mean DLQI score (HS), 17.7. At 4 months, these values improved to IHS4 = 11, VAS = 5.6 and DLQI = 13.1. Only two patients reached the HiSCR score at week 16 and then three patients at week 48. At 12 months, further improvements were observed: IHS4 = 10.2, VAS = 5 and DLQI = 12 (Figure 2).
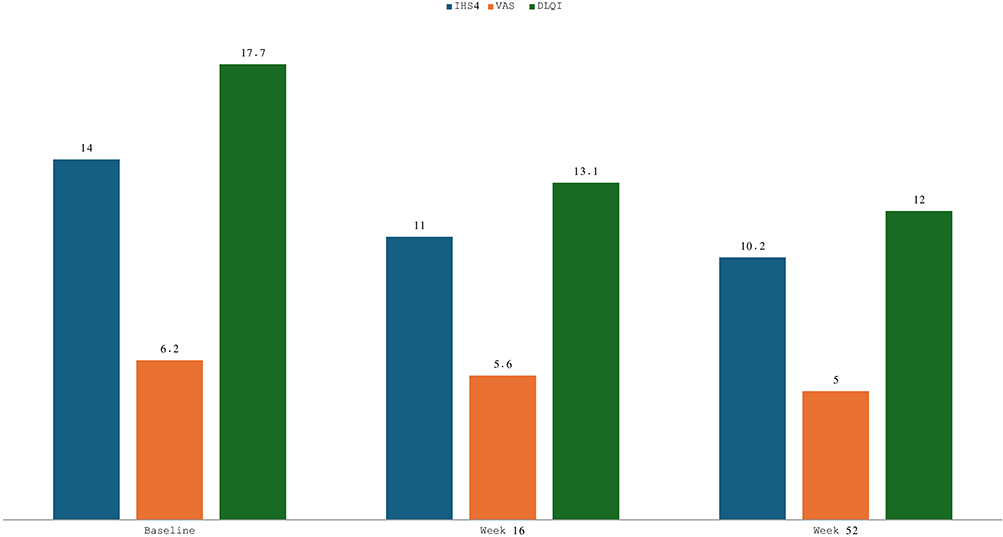 |
Figure 2 Data regarding Hidradenitis Suppurativa score. |
No adverse events were reported across the follow-up period. Treatment was well tolerated across all dosing regimens.
Our real-world experience highlights the differential response to upadacitinib in patients with AD and HS. In the Phase 2 trial published regarding HS, upadacitinib 30 mg once daily improved lesions and pain in moderate-to-severe hidradenitis suppurativa, achieving HiSCR50 in 38% vs 25% (historical placebo) and pain NRS30 in 36% vs 22.5%, with a favorable safety profile supporting Phase 3 evaluation. Our findings are overall consistent with those from the phase 2 randomized trial.5
While patients with AD achieved marked clinical improvements across all outcomes, consistent with findings from published clinical trials and real-world studies, the response in HS, although present, was less pronounced and did not reach the same level of efficacy. These findings are noteworthy, as they suggest that while JAK1 inhibition may represent a valid therapeutic option for AD, its role in HS remains to be fully defined. Importantly, this observation emphasizes the need to refine patient selection or identify subgroups that might derive the greatest benefit from this approach.3–5 We acknowledge the limitations of our small case series of 10 patients, yet we believe that our results add valuable real-world insights to the existing literature. Larger, controlled studies are urgently required to confirm whether upadacitinib could become an effective therapeutic option for HS in routine practice.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author.
Ethic Statement
This study was performed in accordance with the Declaration of Helsinki. Ethical approval was not required for this retrospective analysis of anonymized clinical data, as per local IRB guidelines of University of Naples Federico II. All patients had previously given informed consent for the use of their anonymized data for research purposes.
Funding
There is no funding to report.
Disclosure
All the authors declare that have no conflict of interest.
References
1. Marasca C, Megna M, Balato A, Balato N, Napolitano M, Fabbrocini G. Secukinumab and hidradenitis suppurativa: friends or foes? JAAD Case Rep. 2019;5(2):184–4. PMID: 30740502; PMCID: PMC6357542. doi:10.1016/j.jdcr.2018.12.002
2. Napolitano M, Calzavara-Pinton PG, Zanca A, et al. Comparison of clinical and ultrasound scores in patients with hidradenitis suppurativa: results from an Italian ultrasound working group. J Eur Acad Dermatol Venereol. 2019;33(2):e84–e87. PMID: 30176092. doi:10.1111/jdv.15235
3. Martora F, Marasca C, Cacciapuoti S, et al. Secukinumab in hidradenitis suppurativa patients who failed adalimumab: a 52-week real-life study. Clin Cosmet Invest Dermatol. 2024;17:159–166. PMID: 38283798; PMCID: PMC10821645. doi:10.2147/CCID.S449367
4. Martora F, Marasca C, Battista T, Fabbrocini G, Ruggiero A. Management of patients with hidradenitis suppurativa during COVID-19 vaccination: an experience from southern Italy. Comment on: ‘Evaluating the safety and efficacy of COVID-19 vaccination in patients with hidradenitis suppurativa’. Clin Exp Dermatol. 2022;47(11):2026–2028. PMID: 35727206; PMCID: PMC9349663. doi:10.1111/ced.15306
5. Ackerman LS, Schlosser BJ, Zhan T, et al. Improvements in moderate-to-severe hidradenitis suppurativa with upadacitinib: results from a phase 2, randomized, placebo-controlled study. J Am Acad Dermatol. 2025;92(6):1252–1260. doi:10.1016/j.jaad.2024.12.046
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.