Back to Journals » OncoTargets and Therapy » Volume 10
Real-world experience of everolimus as second-line treatment in metastatic renal cell cancer after failure of pazopanib
Authors Koutsoukos K, Bamias A ![]() , Tzannis K, Espinosa Montaño M, Bozionelou V, Christodoulou C
, Tzannis K, Espinosa Montaño M, Bozionelou V, Christodoulou C ![]() , Stefanou D, Kalofonos H, Duran I, Papazisis K
, Stefanou D, Kalofonos H, Duran I, Papazisis K
Received 6 May 2017
Accepted for publication 23 August 2017
Published 6 October 2017 Volume 2017:10 Pages 4885—4893
DOI https://doi.org/10.2147/OTT.S141260
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Geoffrey Pietersz
Konstantinos Koutsoukos,1,2 Aristotelis Bamias,1,2 Kimon Tzannis,1 Marta Espinosa Montaño,3 Vasiliki Bozionelou,4 Christos Christodoulou,5 Dimitra Stefanou,6 Haralabos Kalofonos,7 Ignacio Duran,3 Konstantinos Papazisis1,8
1Hellenic Genito-Urinary Cancer Group, 2Oncology Unit, Department of Clinical Therapeutics, Alexandra Hospital, National and Kapodistrian University of Athens, Athens, Greece; 3Medical Oncology Department, Hospital Universitario Virgen del Rocío, Sevilla, Spain; 4Department of Medical Oncology, University Hospital of Heraklion, Heraklion, 52nd Oncology Clinic, Metropolitan Hospital, Piraeus, 61st Department of Medical Oncology, Saint Savvas Anticancer Hospital, Athens, 7Division of Oncology, Department of Medicine, University Hospital, University of Patras Medical School, Patras, 8Euromedica General Clinic, Thessaloniki, Greece
Aim: We aimed to provide real-life data on the outcomes of metastatic renal cell carcinoma (mRCC) patients treated with everolimus as second-line treatment after failure of first-line pazopanib.
Patients and methods: Data from the medical charts of mRCC patients from 8 centers in Greece and Spain were reviewed. All patients had received or were continuing to receive second-line everolimus treatment after failure of first-line treatment with pazopanib. No other previous therapies were allowed. The primary end point was the determination of progression-free survival (PFS).
Results: In total, 31 patients were enrolled. Of these, 26% had performance status (PS) >0, 88% were of intermediate/poor Memorial Sloan-Kettering Cancer Center (MSKCC) risk group, and only 61% had undergone prior nephrectomy. Median PFS was 3.48 months (95% CI: 2.37–5.06 months). Median overall survival (OS) from everolimus initiation was 8.9 months (95% CI: 6.47–13.14 months). Median OS from pazopanib initiation was 14.78 months (95% CI: 10.54–19.08 months). Furthermore, 32% of patients temporarily discontinued everolimus due to adverse events (AEs), and 22% of patients discontinued everolimus permanently due to toxicity. Most common toxicities were anemia (29%), stomatitis (26%), pneumonitis (19%), and fatigue (10%). Moreover, 14 AEs (27%) were graded as 3 or 4 and were reported by 13 patients (42%).
Conclusion: This study provides data exclusively on the sequence pazopanib–everolimus in mRCC. Everolimus has a favorable safety profile and is active. The short PFS and OS could be attributed to the fact that the pazopanib–everolimus sequence was mainly offered to patients with adverse prognostic features, resulting in a modest increase in the combined OS of our population.
Keywords: pazopanib, everolimus, renal cell carcinoma
Introduction
The tyrosine-kinase inhibitors (TKIs) sunitinib and pazopanib, targeting vascular endothelial growth factor receptors (VEGFRs), and the combination of the anti-VEGF monoclonal antibody bevacizumab with interferon-α (IFN-α) are the approved first-line options for metastatic renal cell carcinoma (mRCC).1–3 For patients who fail first-line treatment with anti-VEGF/VEGFR therapy, 2 approved options exist: the VEGFR TKI axitinib and the mammalian target of rapamycin (mTOR) inhibitor everolimus.2
The optimal treatment following failure of first-line TKI has not been defined. There are no direct comparisons between the 2 current standards, while retrospective data have not suggested a superiority of one over the other.3–6 Furthermore, sufficient data regarding the activity of the approved second-line agents after exposure to first-line therapies exist only for sunitinib,7–12 but not for the other TKI standard, pazopanib. Pazopanib, an oral TKI targeting VEGFR, platelet-derived growth factor receptor (PDGFR), and c-kit receptor, has exhibited significant progression-free survival (PFS) benefit compared with placebo13 and has proven to be not inferior to sunitinib in first-line mRCC treatment,14 while a patient preference study showed that patients significantly preferred pazopanib over sunitinib.15 These results added important information in the decision-making process, and pazopanib has become a valid option in the first-line setting. Nevertheless, due to its later development, no patients pretreated with pazopanib were included in the 2 pivotal trials leading to the approval of everolimus and axitinib after first-line failure.12,16 For similar reasons, no such data could be extracted from the pivotal trial of pazopanib.13 Therefore, information regarding the activity of subsequent therapies after pazopanib is limited. Due to the approved indication of axitinib, ie, after first-line sunitinib, only the efficacy of everolimus after treatment with pazopanib can be realistically studied outside the context of a clinical trial.
The activity of everolimus in second-line treatment of mRCC following failure of anti-VEGF/VEGFR first-line treatment was shown in the RECORD-1 study,16 which reported a significant prolongation of PFS compared to placebo (4.9 vs 1.9 months; hazard ratio [HR], 0.33; p<0.001) in patients who previously received sunitinib, sorafenib, or both (previous cytokines and/or bevacizumab were also permitted). Because the antitumor mechanisms of the mTOR inhibitors largely differ from those of the anti-VEGFR agents used in the first-line treatment, with little overlap in their safety profiles, everolimus represents a rational option for post-TKI failure in mRCC. However, the results of the RECORD-1 study may not be fully applicable in the current mRCC treatment paradigm, since the RECORD-1 study did not include patients treated with first-line pazopanib. In addition, only 21% of patients received everolimus after only 1 previous anti-VEGF therapy. This is particularly relevant, since a subgroup analysis of RECORD-1 showed numerically longer median PFS in patients who previously received only 1 VEGFR-TKI than in patients who previously received more lines of therapy (5.4 and 4.0 months, respectively).8 Finally, outcomes of unselected patients outside the context of clinical trials may considerably differ from those of patients in controlled clinical trials.17
For all the aforementioned reasons, we conducted the RESCUE retrospective study, which provides real-life data on the outcomes of mRCC patients treated with everolimus as pure second-line treatment after failure of first-line pazopanib treatment.
Patients and methods
Study design
This study was conducted at 8 study sites in Greece and Spain (Supplementary material). It was a retrospective, medical chart review study of patients with mRCC who fulfilled all eligibility criteria mentioned herein. To ensure uniformity of data collection, all necessary information was collected with the use of an electronic case record form (eCRF).
Inclusion and exclusion criteria
Only patients between 18 and 85 years of age, with histologically and/or cytologically documented mRCC, who had received or were continuing (at the time of study enrollment) to receive second-line everolimus treatment after failure of first-line treatment with pazopanib were selected. No other treatment sequence was allowed. Cytokine treatment prior to pazopanib was also not allowed. Patients should have had measurable disease and should have undergone at least 1 evaluation (per local investigator assessment) after commencement of everolimus treatment. Patients must have initiated everolimus within 6 weeks from the date of disease progression on, or after, pazopanib. A minimum of 6 months should have elapsed from the time of everolimus initiation to the inclusion in the study.
Exclusion criteria included participation in any interventional trial during treatment with everolimus, prior therapy with cytokines (eg, IFN or interleukin) or TKIs other than pazopanib, major surgery or radiation within 4 weeks prior to everolimus initiation (palliative radiotherapy for bone lesions within 2 weeks of everolimus treatment initiation was allowed), or chronic systemic treatment with corticosteroids (dose ≥10 mg/d methylprednisolone or equivalent) or other immunosuppressants.
Everolimus was administered according to the approved product labels in the respective countries. Duration of treatment, assessment schedules, and follow-up were decided by the treating physician. Everolimus starting dose was 10 mg once daily. Dose interruptions, dose reduction to 5 mg once daily, or both could be used to manage adverse events (AEs) following the recommendations contained in the summary of product characteristics.
The study was approved by the ethical committees of the participating institutions (Supplementary material). Alive patients gave their written informed consent for collecting and analyzing their medical data pertinent to the objectives of this study. For deceased patients, a consent waiver by the ethical committees of the participating sites was granted.
Study end points and analysis
The primary end point was the determination of PFS, defined as the time elapsed between everolimus treatment initiation and the date of documentation of the first objective disease progression event as per local assessment, or the date of death, whichever occurred first. The secondary end points of the study were as follows: overall survival (OS), defined as the time from everolimus treatment initiation until death from any cause; and assessment of the safety profile of everolimus, including the incidence of the AEs recorded in the patients’ medical records during treatment with everolimus regardless of causal relationship with study medication (AEs were collected and coded to a preferred term using the Medical Dictionary for Regulatory Activities [MedDRA]); the impact of prior pazopanib duration of treatment on the PFS of second-line everolimus treatment; the determination of combined PFS, defined as the time from pazopanib treatment initiation until the time of documented tumor progression or death from any cause during everolimus treatment; the determination of clinical benefit rate (CBR), defined as the proportion of patients whose best response was complete response (CR), partial response (PR), or stable disease (SD) during second-line treatment with everolimus as per local assessment.
Continuous variables were summarized with the use of descriptive statistical measures (mean value, standard deviation, median and range [minimum, maximum]), and categorical variables were displayed as frequency tables. Response to treatment was assessed according to local standards. Chi-squared test was used to correlate the duration of pazopanib therapy and occurrence of grade 3/4 AEs. The Kaplan–Meier method was used to estimate the median PFS, as well as the analysis of OS and combined PFS. Log-rank tests were used to test the equality of survivor functions across groups. The percentage of patients who experienced disease progression and died due to any cause was calculated along with the respective 95% CI. All data were collected from May 2014 to December 2014 (database lock). According to the methodological features of an observational noninterventional study, all analyses were descriptive, and the results presented should be interpreted as such. All statistical analyses were performed using the STATA/SE 14.1 software (copyright 1985–2015; StataCorp LLC, College Station, TX, USA).
Results
Patients
Data from 31 mRCC patients (Greece: 25, 81%; Spain: 6, 19%) were collected (Table 1). Patients started pazopanib between 1 February 2011 and 8 June 2013 and everolimus between 19 September 2011 and 16 January 2014. All but 1 patient discontinued pazopanib due to disease progression. Twenty-nine patients (94%) had clear cell histology, while 2 (6%) had mixed histology with a clear-cell component. Nineteen patients (61%) had undergone nephrectomy prior to initial treatment with pazopanib. Most patients were of intermediate (50%) or poor risk (33%) according to the Memorial Sloan-Kettering Cancer Center (MSKCC) prognostic survival risk score18 prior to commencement of pazopanib. The median number of disease sites was 2 (1–5). Six patients (19%) had only 1 disease site, 18 (42%) had 2, 8 (26%) had 3, 2 (6.5%) had 4, and 2 (6.5%) had 5 sites. All patients were eligible for efficacy and safety assessment. Median time from the diagnosis of metastatic disease to the initiation of pazopanib and everolimus was 1.1 and 7.8 months, respectively. Median duration of first-line pazopanib treatment was 5.6 months (range: 0.5–19 months).
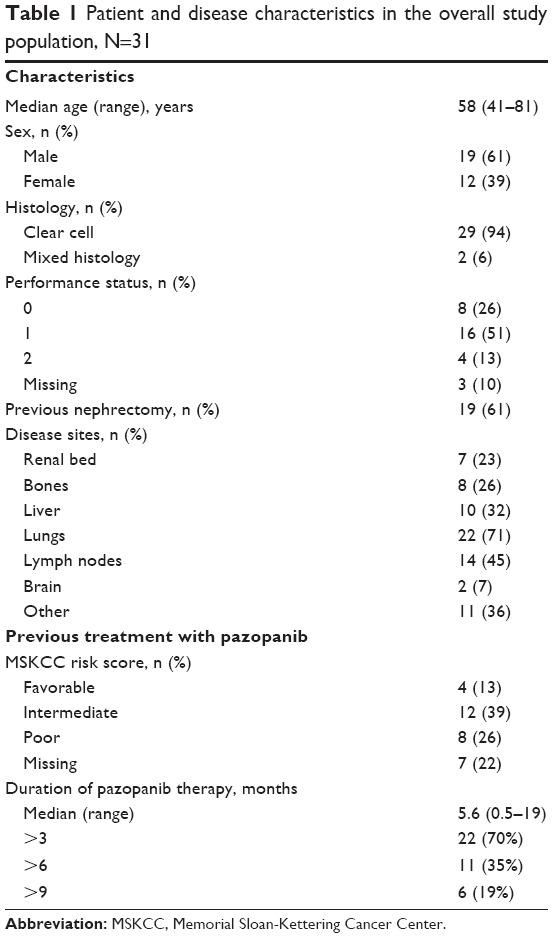 | Table 1 Patient and disease characteristics in the overall study population, N=31 |
Efficacy
All patients were assessable for response to everolimus. No CR was reported. Best tumor response was PR in 4 (13%) patients and SD in 8 (26%) patients, resulting in a CBR of 39%, while in 19 patients (61%) progressive disease (PD) was reported as the best response during everolimus treatment.
At the time of analysis, all patients had progressed during or after cessation of everolimus treatment and 5 patients (16%) were still alive. The median follow-up for everolimus therapy was 27 months (95% CI: 14.9 months – not reached). Median PFS from everolimus treatment initiation was 3.5 months (95% CI: 2.4–5.1 months) (Figure 1) and median OS was 8.9 months (95% CI: 6.5–13.1 months) (Figure 1). Combined median PFS was 9.2 months (95% CI: 8–10.8 months). The median OS from the time of pazopanib initiation was 14.8 months (95% CI: 10.5–19.1 months).
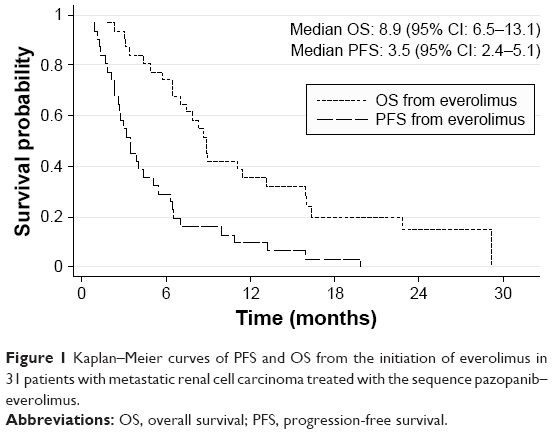 | Figure 1 Kaplan–Meier curves of PFS and OS from the initiation of everolimus in 31 patients with metastatic renal cell carcinoma treated with the sequence pazopanib–everolimus. |
There was no impact of first-line pazopanib treatment duration on everolimus PFS (p=0.170) when duration was used a continuous variable. When stratified according to time on first-line pazopanib duration (<3 months vs ≥3 months, <6 months vs ≥6 months, and <9 months vs ≥9 months), longer duration of previous pazopanib treatment tended to result in longer median PFS with second-line everolimus; however, no statistically significant differences were observed (Table 2). The respective analysis for OS after everolimus initiation yielded significant results. When time on pazopanib was studied as a continuous variable, there was a significant correlation with OS after everolimus initiation (p=0.005): for each additional month of pazopanib treatment, there was a 17% reduction in the risk of death. Similarly, when time on pazopanib was studied as a categorical variable, a significant correlation with post-everolimus OS was found for all time points studied, with a more pronounced difference observed when pazopanib was used for at least 9 months (Table 2, Figure 2).
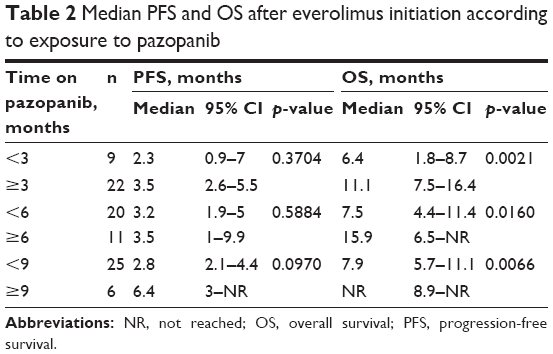 | Table 2 Median PFS and OS after everolimus initiation according to exposure to pazopanib |
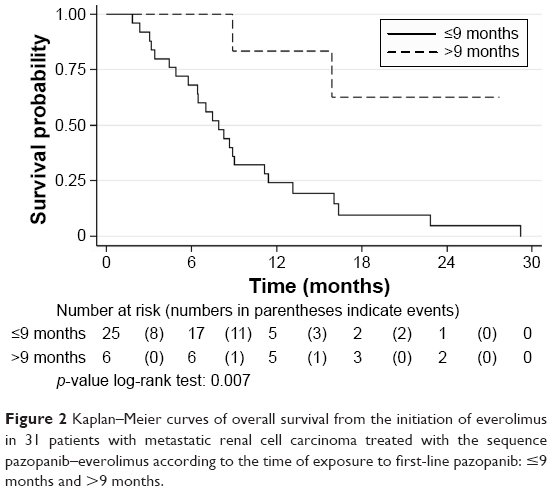 | Figure 2 Kaplan–Meier curves of overall survival from the initiation of everolimus in 31 patients with metastatic renal cell carcinoma treated with the sequence pazopanib–everolimus according to the time of exposure to first-line pazopanib: ≤9 months and >9 months. |
Safety
The median duration of everolimus therapy was 3.5 months (range: 1–20 months). The median everolimus daily dose was 10 mg (5–10 mg), while the mean daily dose was 9.3 mg. Nine patients (32%) temporarily discontinued everolimus treatment, 2 of them twice. There were 11 temporary discontinuations due to the following AEs: grade 2 edema (n=1), grade 3 proteinuria–acute renal failure (n=1), grade 4 anemia (n=1), grade 1 diarrhea and fever (n=2), hypercalcemia (n=1), grade 2 elevated gamma-glutamyl transferase (GGT) (n=1), grade 3 mucositis (n=2), grade 3 anemia (n=1), and grade 2 mucositis (n=1). At the time of analysis, all patients had permanently discontinued everolimus: 7 (23%) due to AEs, 23 (74%) due to disease progression, and 1 case (3%) due to unknown reasons. The toxicities that led to discontinuation were grade 3 stomatitis (n=1), grade 3 pneumonitis (n=2), grade 2 rash (n=1), grade 3 anemia (n=1), repeated episodes of grade 1 diarrhea and fever (n=1), and grade 2 gastric bleeding (n=1).
Twenty-four patients (77%) reported 51 AEs (Table 3). From among these, only 14 (27%) were graded as 3 or 4 and were reported by 13 patients (42%). No deaths due to AEs were reported. The most common AEs were anemia (29%), stomatitis (26%), and pneumonitis (23%). The most common grade 3/4 AEs were anemia and stomatitis (10% each), while grade 3 pneumonitis was reported in 2 cases (7%).
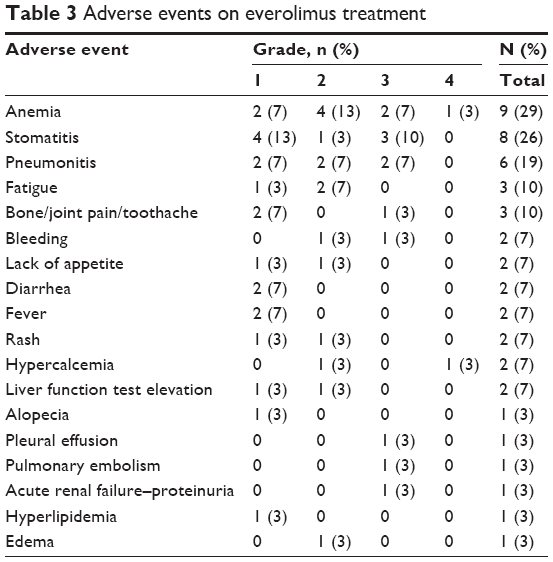 | Table 3 Adverse events on everolimus treatment |
Previous length of exposure to pazopanib was not associated with the occurrence of a grade 3/4 event: the median exposure to pazopanib was 5.1 months for the 18 patients with no such events vs 5.9 months for the 13 patients reporting grade 3 or 4 events.
Discussion
Data regarding the efficacy and safety of available agents following first-line pazopanib in mRCC are scarce. This is the only study providing data exclusively on the sequence pazopanib–everolimus in mRCC with no other first- or second-line therapies having been used. Limitations to this study are those inherent to the small number of patients, as well as the retrospective and noninterventional design, more importantly, the absence of standardized assessments at predefined intervals as there are in clinical trials. However, first- and second-line treatment was highly homogeneous (in contrast to most other similar studies, Table 4), and the median follow-up was among the longest reported for similar studies. Furthermore, observational noninterventional studies are important sources of information about the use of agents in the real-world clinical setting. Therefore, we believe that the information provided is reliable and of importance.
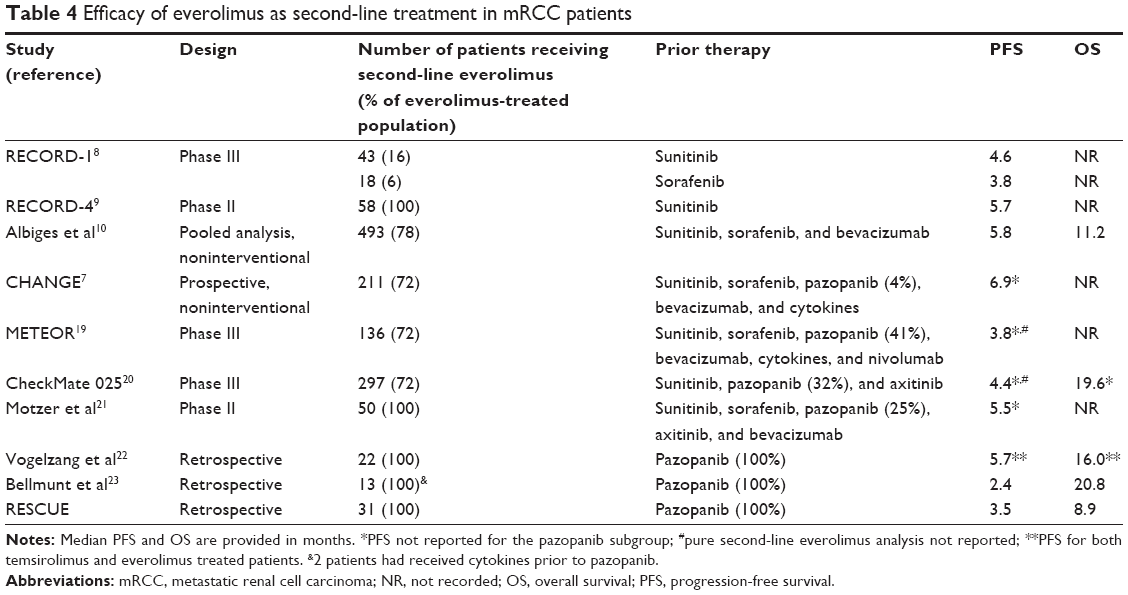 | Table 4 Efficacy of everolimus as second-line treatment in mRCC patients |
Earlier, patients treated with everolimus after exposure to pazopanib have been included as part of a broader population in 6 studies,22 but results on this exact sequence have been reported only in one of them (Table 4). In all cases, patients treated with pure second-line everolimus after first-line pazopanib formed minority subgroups in the total population. In the randomized Phase III study METEOR,19 which compared cabozantinib with everolimus as second- or third-line treatment, first-line pazopanib was used in 41% of included patients in the everolimus arm, while 28% had received 2 previous lines of therapy. The median PFS in the everolimus arm was 3.8 months, but no information about the pazopanib pretreated subgroup yet exists. Similarly, in 2 other randomized trials,20,21 pazopanib was the first-line agent in 32% and 25%, respectively, while second-line everolimus formed 72% and 100% of the everolimus arm. Median PFSs of 4.4 and 5.5 months for the whole populations were reported. In the recently published prospective, observational CHANGE study,7 median PFS for mRCC patients receiving everolimus as second-line treatment (again a subgroup of the total population) was 6.9 months. However, only 4% of the patients had received pazopanib as first-line treatment. Interestingly, patients pretreated with pazopanib had the numerically shortest treatment duration with everolimus (only 3 months vs at least 6 months with any other agent administered in first line). Finally, in 2 retrospective studies including 35 patients each, all patients received first-line pazopanib.22,23 A median PFS of 5.7 months for a mixed population of everolimus and temsirolimus was found in the first study, while Bellmunt et al23 reported a median PFS of 2.8 months in a subpopulation of 13 patients, 2 of whom had received IFN-α prior to pazopanib.
We report a PFS of 3.5 months. Although the 13% response rate we found is encouraging, our median PFS as well as that reported by Bellmunt et al23 seem modest compared to those reported so far for everolimus given after failure of other anti-VEGF/VEGFR treatment in the largest series (Table 4). In most cases, pure second-line everolimus populations represented subgroups (thus limiting the power of those analyses) of broader populations who had been exposed to a variety of first-line agents and/or had received everolimus not only in second but also in subsequent lines of therapy. In the RECORD-1 study,8 the subgroup of patients who received only 1 previous VEGFR-TKI (21%) had a median PFS of 4.6 and 3.8 months for first-line sunitinib and sorafenib, respectively. In the recently reported prospective Phase II RECORD-4 study,9 a median PFS of 5.7 months was recorded for patients receiving first-line sunitinib. Similar PFS for pure second-line use of everolimus was also found in a pooled analysis of 4 noninterventional European studies10 (Table 3). The reasons for the numerically longer PFS reported in those studies, apart from the limitations inherent to across-studies comparisons, are unclear. It is unlikely that this was related to the use of pazopanib in the first line. Pazopanib has been shown to be noninferior to sunitinib14 in a randomized study, wherein the use of subsequent therapies, including everolimus, was balanced between the 2 arms.24 Differences in the prognostic characteristics of our population might account for the seemingly “inferior” PFS observed in our study. Several of the previously mentioned studies are prospective Phase II or III national or international studies. Patients enrolled in such trials do not reflect real-world patients and everyday clinical practice, since most trials have strict eligibility criteria, assessment times, and follow-up schedules. This results in selection of patients with better prognosis, as shown by a significantly shorter second-line PFS for trial-ineligible patients in a retrospective analysis of 768 patients.17 Features of poor prognosis were observed at the initiation of both first- and second-line therapies in our series. Indeed, only 13% were favorable-risk patients at the initiation of pazopanib, reflected by a respective median OS of 14.8 months, which is numerically shorter than that reported in the pivotal trial of pazopanib,13 but which is in line with data from unselected cohorts.25 Furthermore, at the initiation of second-line treatment, only 26% of patients had performance status (PS) 0, most belonged to the intermediate or poor MSKCC risk groups (88%), only 61% had undergone nephrectomy, while 80% had at least 2 metastatic sites. These features are indicative of poor outcome26–28 and are in sharp contrast with the 91% good or intermediate risk and 89% nephrectomy rate in the noninterventional study by Albiges et al10 in a non-pazopanib-treated population.
The reason for the inclusion of predominantly bad prognosis patients in our study is unclear. It could be suggested that pazopanib and everolimus were intuitively offered to patients of relatively poor prognosis due to their favorable toxicity profiles compared to other drugs.14,15 This hypothesis is supported by the lower-than-expected nephrectomy rate in our population, since nephrectomy is usually offered to patients of good PS.3 Therefore, it seems plausible that oncologists might offer this agent to patients of poor PS and, therefore, poor prognosis. A large multinational study of real-life pazopanib use,29 which has completed accrual, will shed light on the utilization of pazopanib in everyday practice. Another reason for the unfavorable outcome of our patients was the timing of everolimus treatment in this study, which did not allow for the inclusion of long-term responders to pazopanib. Indeed, 18 patients (58%) started everolimus prior to 2013, while pazopanib was approved in Greece and Spain in 2011. The possibility that long-term responders to pazopanib were offered a TKI rather than everolimus cannot also be excluded, while the inclusion of patients with favorable characteristics in clinical trials conducted at the same period could also represent another reason for a negative selection in the RESCUE study. It should be stressed that even in this population of unfavorable prognosis, median PFS on everolimus was numerically 2-fold higher than that reported in the RECORD-1 study for placebo, underlying the efficacy of everolimus after first-line pazopanib.
The correlation between response to a first-line VEGF-targeted agent and second-line therapy remains controversial. There is some evidence that longer exposure to first-line VEGF-targeted agents may be associated with increased efficacy of second-line everolimus therapy,7,30,31 although opposite results have also been published.10 Likewise, similar studies for second-line TKIs have been inconclusive.32 In our analysis, there was a significant prolongation of OS after everolimus with longer previous exposure to pazopanib. Similar findings were reported in a subanalysis of the AXIS trial33 for axitinib and sorafenib following sunitinib. These findings taken together suggest that longer first-line treatment duration may correspond to a less-aggressive tumor behavior rather than higher efficacy of everolimus after long exposure to pazopanib.
The safety profile of everolimus when used after pazopanib in mRCC patients was similar to that observed after other anti-VEGF therapies, as reported in clinical trials16,32 and noninterventional studies.7,10 Importantly, previous exposure to pazopanib does not seem to affect the tolerability of subsequent everolimus administration. Dose interruptions were similar to those reported in RECORD-1 (32% vs 38%). The rate of discontinuation due to AEs was higher (23%) than in the expanded access study (17%)23 or RECORD-1 (13%)16 but identical to those of the noninterventional studies by Albiges et al (25%)10 and Bergmann et al (21%).7 This discrepancy could be a result of the different methods of reporting AEs in clinical practice and clinical trials, but it could also reflect the poorer PS and higher incidence of comorbidities of patients in real-life practice.
It is important that our findings are viewed within the context of the rapid developments in the mRCC treatment paradigm. Recently, 2 Phase III randomized trials showed superiority of nivolumab, an immune checkpoint inhibitor, and cabozantinib, a multi-TKI of MET, AXL, and VEGF, over everolimus after VEGFR-targeted treatment failure.19,20 These results have granted these agents a dominant position in the treatment of relapsed mRCC patients.34 Nevertheless, only nivolumab is yet freely available in Europe, while availability of both agents may be a problem in some countries worldwide. Therefore, our results will still be applicable for the immediate future. More importantly, the recent improvements in the prognosis of mRCC patients have been achieved through the utilization of multiple effective agents. The emergence of new drugs should be viewed as a valuable addition to the existing agents rather than as a competing process of replacement, since they can all contribute toward an improved therapeutic effect for mRCC patients.
Conclusion
We showed that everolimus used as second-line treatment after pazopanib in mRCC patients is effective and safe in a real-life, multi-institutional setting. This sequence could be considered a standard option for these patients in cases of unavailability or contraindication of other more effective agents.
Acknowledgments
This study was sponsored by the Hellenic Genito-Urinary Cancer Group and supported by Novartis Pharmaceuticals. Study design, data collection, access to the data, and analysis, as well as writing of the manuscript, were solely the responsibility of the sponsor and the authors.
The following persons also contributed to data acquisition and analysis: Loukas Kontovinis (clinical investigator; Hellenic Genito-Urinary Cancer Group [HGUCG]; Euromedica General Clinic, Thessaloniki, Greece), Angelos Koutras (clinical investigator; Division of Oncology, Department of Medicine, University Hospital, University of Patras Medical School, Patras, Greece), J Varkarakis (participating investigator; HGUCG; 2nd Urology Department, National and Kapodistrian University of Athens, Athens, Greece), J Adamakis (participating investigator; 1st Urology Department, National and Kapodistrian University of Athens, Athens, Greece), J Anastasiou (participating investigator; 1st Urology Department, National and Kapodistrian University of Athens, Athens, Greece), Nikolaos K Kentepozidis (clinical and participating investigator; HGUCG; Department of Oncology, Department of Medical Oncology, 251 Airforce General Hospital, Athens, Greece, ), Alexandros Ardavanis (clinical and participating investigator; Saint Savvas Anticancer Hospital, Athens, Greece), Constantine A Constantinides (participating investigator; HGUCG; 1st Urology Department, National and Kapodistrian University of Athens, Athens, Greece), and Meletios A Dimopoulos (clinical and participating investigator; HGUCG; Oncology Unit, Department of Clinical Therapeutics, Alexandra Hospital, National and Kapodistrian University of Athens, Athens, Greece).
Disclosure
The authors report no conflicts of interest in this work.
References
NCCN. Clinical Practice Guidelines in Oncology: Kidney Cancer; 2015; Version 1. Available from: http://www.nccn.org/professionals/physician_gls/pdf/kidney.pdf. Accessed August 28, 2017. | ||
Ljungberg B, Bensalah K, Canfield S, et al. EAU guidelines on renal cell carcinoma: 2014 update. Eur Urol. 2015;67(5):913–924. | ||
Escudier B, Porta C, Schmidinger M, et al. Renal cell carcinoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2014;25(suppl 3):iii49–iii56. | ||
Alimohamed N, Lee JL, Srinivas S, et al. A population-based overview of sequences of targeted therapy in metastatic renal cell carcinoma. Clin Genitourin Cancer. 2014;12(4):e127–e131. | ||
Ko JJ, Choueiri TK, Rini BI, et al. First-, second-, third-line therapy for mRCC: benchmarks for trial design from the IMDC. Br J Cancer. 2014;110(8):1917–1922. | ||
Heng DY, Signorovitch J, Swallow E, et al. Comparative effectiveness of second-line targeted therapies for metastatic renal cell carcinoma: a systematic review and meta-analysis of real-world observational studies. PLoS One. 2014;9(12):e114264. | ||
Bergmann L, Kube U, Doehn C, et al. Everolimus in metastatic renal cell carcinoma after failure of initial anti-VEGF therapy: final results of a noninterventional study. BMC Cancer. 2015;15:303. | ||
Calvo E, Escudier B, Motzer RJ, et al. Everolimus in metastatic renal cell carcinoma: subgroup analysis of patients with 1 or 2 previous vascular endothelial growth factor receptor-tyrosine kinase inhibitor therapies enrolled in the phase III RECORD-1 study. Eur J Cancer. 2012;48(3):333–339. | ||
Motzer RJ, Alyasova A, Ye D, et al. Phase II trial of second-line everolimus in patients with metastatic renal cell carcinoma (RECORD-4). Ann Oncol. 2016;27(3):441–448. | ||
Albiges L, Kube U, Eymard JC, et al. Everolimus for patients with metastatic renal cell carcinoma refractory to anti-VEGF therapy: results of a pooled analysis of non-interventional studies. Eur J Cancer. 2015;51(16):2368–2374. | ||
Kontovinis L, Laschos K, Karadimou A, et al. Sequential treatment with sorafenib and sunitinib in metastatic renal cell carcinoma: clinical outcomes from a retrospective clinical study. Med Oncol. 2012;29(2):750–754. | ||
Rini BI, Escudier B, Tomczak P, et al. Comparative effectiveness of axitinib versus sorafenib in advanced renal cell carcinoma (AXIS): a randomised phase 3 trial. Lancet. 2011;378(9807):1931–1939. | ||
Sternberg CN, Davis ID, Mardiak J, et al. Pazopanib in locally advanced or metastatic renal cell carcinoma: results of a randomized phase III trial. J Clin Oncol. 2010;28(6):1061–1068. | ||
Motzer RJ, Hutson TE, Cella D, et al. Pazopanib versus sunitinib in metastatic renal-cell carcinoma. N Engl J Med. 2013;369(8):722–731. | ||
Escudier B, Porta C, Bono P, et al. Randomized, controlled, double-blind, cross-over trial assessing treatment preference for pazopanib versus sunitinib in patients with metastatic renal cell carcinoma: PISCES Study. J Clin Oncol. 2014;32(14):1412–1418. | ||
Motzer RJ, Escudier B, Oudard S, et al; Ravaud A; RECORD-1 Study Group. Efficacy of everolimus in advanced renal cell carcinoma: a double-blind, randomised, placebo-controlled phase III trial. Lancet. 2008;372(9637):449–456. | ||
Heng DY, Choueiri TK, Rini BI, et al. Outcomes of patients with metastatic renal cell carcinoma that do not meet eligibility criteria for clinical trials. Ann Oncol. 2014;25(1):149–154. | ||
Motzer RJ, Bacik J, Schwartz LH, et al. Prognostic factors for survival in previously treated patients with metastatic renal cell carcinoma. J Clin Oncol. 2004;22(3):454–463. | ||
Choueiri TK, Escudier B, Powles T, et al; METEOR Investigators. Cabozantinib versus everolimus in advanced renal-cell carcinoma. N Engl J Med. 2015;373(19):1814–1823. | ||
Motzer RJ, Escudier B, McDermott DF, et al; CheckMate 025 Investigators. Nivolumab versus everolimus in advanced renal-cell carcinoma. N Engl J Med. 2015;373(19):1803–1813. | ||
Motzer RJ, Hutson TE, Glen H, et al. Lenvatinib, everolimus, and the combination in patients with metastatic renal cell carcinoma: a randomised, phase 2, open-label, multicentre trial. Lancet Oncol. 2015;16(15):1473–1482. | ||
Vogelzang NJ, Hackshaw MD, Hutson TE, et al. First-line and sequential use of pazopanib followed by mammalian target of rapamycin inhibitor therapy among patients with advanced renal cell carcinoma in a US community oncology setting. Clin Genitourin Cancer. 2015;13(3):210–217. | ||
Bellmunt J, Pons F, Foreshew A, et al. Sequential targeted therapy after pazopanib therapy in patients with metastatic renal cell cancer: efficacy and toxicity. Clin Genitourin Cancer. 2014;12(4):262–269. | ||
Motzer RJ, Hutson TE, McCann L, Deen K, Choueiri TK. Overall survival in renal-cell carcinoma with pazopanib versus sunitinib. N Engl J Med. 2014;370(18):1769–1770. | ||
Soerensen AV, Donskov F, Hermann GG, et al. Improved overall survival after implementation of targeted therapy for patients with metastatic renal cell carcinoma: results from the Danish Renal Cancer Group (DARENCA) study-2. Eur J Cancer. 2014;50(3):553–562. | ||
Heng DY, Xie W, Regan MM, et al. Prognostic factors for overall survival in patients with metastatic renal cell carcinoma treated with vascular endothelial growth factor-targeted agents: results from a large, multicenter study. J Clin Oncol. 2009;27(34):5794–5799. | ||
Bamias A, Tzannis K, Papatsoris A, et al. Prognostic significance of cytoreductive nephrectomy in patients with synchronous metastases from renal cell carcinoma treated with first-line sunitinib: a European multiinstitutional study. Clin Genitourin Cancer. 2014;12(5):373–383. | ||
Bamias A, Tzannis K, Beuselinck B, et al. Development and validation of a prognostic model in patients with metastatic renal cell carcinoma treated with sunitinib: a European collaboration. Br J Cancer. 2013;109(2):332–341. | ||
Bamias A, Bono P, Procopio G. PRINCIPAL: a prospective observational study of real-world treatment patterns and treatment outcomes in patients with advanced or metastatic renal cell carcinoma (mRCC) receiving pazopanib. J Clin Oncol. 2014;32(5s):(sul;abstrTS4600^). | ||
Chen CC, Hess GP, Liu Z, et al. Second-line treatment outcomes after first-line sunitinib therapy in metastatic renal cell carcinoma. Clin Genitourin Cancer. 2012;10(4):256–261. | ||
Buchler T, Bortlicek Z, Poprach A, et al. Efficacy of everolimus in second- and third-line therapy for metastatic renal cell carcinoma: a registry-based analysis. Urol Oncol. 2014;32(5):569–575. | ||
Grunwald V, Karakiewicz PI, Bavbek SE, et al; REACT Study Group. An international expanded-access programme of everolimus: addressing safety and efficacy in patients with metastatic renal cell carcinoma who progress after initial vascular endothelial growth factor receptor-tyrosine kinase inhibitor therapy. Eur J Cancer. 2012;48(3):324–332. | ||
Escudier B, Michaelson MD, Motzer RJ, et al. Axitinib versus sorafenib in advanced renal cell carcinoma: subanalyses by prior therapy from a randomised phase III trial. Br J Cancer. 2014;110(12):2821–2828. | ||
Powles T, Staehler M, Ljungberg B, et al. Updated EAU guidelines for clear cell renal cancer patients who fail VEGF targeted therapy. Eur Urol. 2016;69(1):4–6. |
Supplementary material
The centers that participated in the RESCUE study and the relevant ethical committees are as follows:
- Hospital Virgen del Rocío, Sevilla, Spain; Ethics and Scientific Committee, Hospital Virgen del Rocío, Sevilla, Spain.
- Department of Clinical Therapeutics, Alexandra Hospital, National and Kapodistrian University of Athens, Athens, Greece; Scientific Committee, Alexandra Hospital, Athens, Greece.
- University Hospital of Heraklion, Heraklion, Greece; Scientific Committee, University Hospital of Heraklion, Heraklion, Greece.
- 251 Airforce General Hospital, Department of Medical Oncology, Athens, Greece; Scientific Committee, 251 Airforce General Hospital, Athens, Greece.
- Department of Oncology, Euromedica Geniki Kliniki, Thessaloniki, Greece; Ethics and Scientific Committee, Euromedica General Clinic, Thessaloniki, Greece.
- 2nd Oncology Clinic, Metropolitan Hospital, Piraeus, Greece; Scientific Committee, Metropolitan Hospital, Piraeus, Greece.
- Saint Savvas Anticancer Hospital, Athens, Greece; Scientific Committee, Saint Savvas Anticancer Hospital, Athens, Greece.
- Division of Oncology, Department of Medicine, University Hospital, University of Patras Medical School, Patras, Greece; Scientific Committee, University Hospital, Patras, Greece.
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.