Back to Journals » Clinical Ophthalmology » Volume 15
Real-World Effectiveness, Treatment Pattern, and Safety of Ranibizumab in Korean Patients with Neovascular Age-Related Macular Degeneration: Subgroup Analyses from the LUMINOUS Study
Authors Sagong M ![]() , Woo SJ
, Woo SJ ![]() , Lee Y
, Lee Y
Received 9 February 2021
Accepted for publication 14 April 2021
Published 11 May 2021 Volume 2021:15 Pages 1995—2011
DOI https://doi.org/10.2147/OPTH.S303884
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Min Sagong,1 Se Joon Woo,2 Youkyung Lee3 On behalf of the LUMINOUS™ study investigators from South Korea
1Department of Ophthalmology, Yeungnam University College of Medicine, Daegu, Korea; 2Department of Ophthalmology, Seoul National University Bundang Hospital, Seongnam, Korea; 3Novartis Korea Ltd., Seoul, Korea
Correspondence: Se Joon Woo
Department of Ophthalmology, Seoul National University Bundang Hospital, 173– 82 Gumi-ro, Bundang-gu, Seongnam-si, Gyeonggi-do, 13620, South Korea
Tel +82-31-787-7377
Fax +82-31-787-4057
Email [email protected]
Purpose: To evaluate the real-world effectiveness, treatment patterns, and safety of ranibizumab in Korean patients with neovascular age-related macular degeneration (nAMD).
Methods: LUMINOUS™ is a 5-year, global, prospective, observational, open-label study. Adults aged ≥ 18 years who were either treatment-naïve or prior-treated were enrolled and treated with ranibizumab 0.5 mg as per the local label. Outcome measures included mean (± standard deviation [SD]) changes from baseline in visual acuity (VA) and central retinal thickness (CRT), and rate of ocular and non-ocular adverse events (AEs).
Results: Overall, 367 Korean patients with nAMD (152 treatment-naïve and 215 prior-treated) were enrolled. The mean (SD) VA changes from baseline at 1-year were +10.1 (± 21.77; P=0.0005) and +1.4 (± 15.17; P=0.2142) Early Treatment Diabetic Retinopathy Study letters, with mean numbers of injections of 5.2 and 3.4 in the treatment-naïve and prior-treated groups, respectively. VA gains were greater in patients with lower baseline VA, who received a loading dose, and with polypoidal choroidal vasculopathy (PCV). Multivariate logistic regression analyses demonstrated younger age, worse baseline VA, and those who received loading dose being associated with higher odds of any gain in VA at 1 year (P< 0.05). Mean (SD) CRT changes from baseline were – 126.7 (± 174.90) μm (P< 0.0001) and +10.8 (± 89.62) μm (P=0.5833) in the treatment-naïve and prior-treated groups, respectively, with greater reductions observed in patients with PCV. Ocular and non-ocular AEs were reported in 8.4% (n=31) and 10.1% (n=37) of patients, respectively.
Conclusion: The LUMINOUS study confirms real-world effectiveness and safety of ranibizumab in Korean patients with nAMD; factors including age, baseline VA, and loading-dose were associated with VA gain at one-year post-treatment.
Keywords: neovascular age-related macular degeneration, polypoidal choroidal vasculopathy, ranibizumab, real-world
Introduction
Age-related macular degeneration (AMD) is the most common cause of irreversible vision loss.1 The Korea National Health and Nutrition Examination Survey, conducted from 2008 to 2011, showed that the estimated prevalence of AMD in the Korean population aged ≥40 years is 6.62% (6.02% in early AMD and 0.60% in late AMD).2 A nationwide population-based study conducted from 2008 to 2012 further showed that the prevalence of neovascular AMD (nAMD) in the Korean population aged ≥40 years was 0.36%;3 an effective treatment option is required to manage the associated disease burden. The introduction of anti-vascular endothelial growth factors (anti-VEGFs) has transformed the management of nAMD, making anti-VEGFs the current standard of care for nAMD treatment.4
Ranibizumab (Lucentis®; Novartis Pharma AG, Basel, Switzerland, and Genentech Inc., South San Francisco, CA, USA), a humanized monoclonal antibody Fab fragment specifically designed for ocular use, inhibits angiogenesis by binding with high affinity to all isoforms of VEGF-A.5 Ranibizumab was approved in Korea in 2007 for the treatment of patients with nAMD and is currently approved for the treatment of visual impairment due to nAMD, diabetic macular edema (DME), macular edema secondary to retinal vein occlusion (RVO), choroidal neovascularization (CNV) secondary to pathologic myopia (PM), and CNV other than secondary to PM and nAMD.6
Several studies have demonstrated the effectiveness and safety of ranibizumab in Korean patients with nAMD.7–9 A post hoc analysis of a ranibizumab post-marketing surveillance study in Korea demonstrated significant improvements in visual and anatomical outcomes after three-monthly ranibizumab injections.10 Theses prior studies included only small number of patients (N<40),7–9 or with a short follow-up period.10 Despite these evidences, the long-term effectiveness and safety of intravitreal ranibizumab 0.5 mg in Korean patients with nAMD needs to be explored further.
LUMINOUS™ (NCT01318941) is the largest prospective observational study in the field of medical retina, designed to evaluate the long-term effectiveness, safety, and treatment patterns with ranibizumab in routine clinical practice across 5 approved indications (nAMD, DME, branch retinal vein occlusion [BRVO], central retinal vein occlusion [CRVO], myopic choroidal neovascularization [mCNV]) in Asia, Australia, Europe, and North and South America.11
The Korea-specific 1- to 2-year effectiveness, treatment pattern, and overall safety outcomes in a subgroup of patients with nAMD enrolled in this study are reported.
Materials and Methods
Ethics Statement
The LUMINOUS study was conducted in accordance with the Guidelines for Good Pharmacoepidemiology Practices issued by the International Society for Pharmacoepidemiology, with any applicable national guidelines and ethical principles laid down in the Declaration of Helsinki. The study protocol was reviewed and approved by an Independent Ethics Committee or Institutional Review Board for each center. Patients provided written informed consent. The study is registered with clinicaltrials.gov as NCT01318941 (www.clinicaltrials.gov).
Study Design, Study Population and Treatment Protocol
LUMINOUS is a 5-year, prospective, observational, multicenter, open-label, single-arm, global study of ranibizumab 0.5 mg in patients with nAMD, DME, BRVO, CRVO, or mCNV. The study was conducted at 488 clinical sites across 42 countries.11
Overall for the LUMINOUS study, consenting adult patients within the age limit as defined by local regulations (≥18 years) with any of the approved indications included in the local ranibizumab label were enrolled; these included patients who were treatment-naïve (ie, patients who had not been pre-treated with any intravitreal medication in the primary treated eye), or prior-treated with ranibizumab or another ocular therapy. Patients were excluded if they were participating in other investigational studies or if they had received systemic anti-VEGF therapy in 90 days or ocular anti-VEGF therapy other than ranibizumab 30 days prior to enrolment. Patients were treated with intravitreal ranibizumab 0.5 mg according to the local product label at outpatient ophthalmology clinics.
Ranibizumab was re-administered according to the investigators’ discretion. It was recommended to capture data at every visit or at least every 3 months. As patients were recruited over time and the calendar time point of study completion was pre-set, follow-up time varied according to the entry date. The minimum potential follow-up for each patient was identified as 1 year in the protocol. Patients who did not attend a follow-up visit at least once per year, or who were switched to another anti-VEGF therapy, were discontinued from the study, and not included in the effectiveness analysis in subsequent study time points. The first eye treated was considered the primary treated eye. If both eyes were first treated on the same date, or if both eyes were pre-treated, the eye with the earliest diagnosis date was considered the primary treated eye.
The current subgroup analyses from the LUMINOUS study included Korean patients with nAMD who were treatment-naïve or prior-treated (ranibizumab or any other anti-VEGF agent) in their primary treated eye.
Study Objective and Assessments
The primary objective of the study, for all approved indications of ranibizumab in local product label, was to describe (i) the safety assessed by type, frequency, severity, and relationship of all non-ocular and ocular adverse events (AEs), and (ii) the effectiveness assessed by the mean change in VA over time and mean change in central retinal thickness (CRT) over time.
Demographic and baseline characteristics were collected at baseline, including ocular and non-ocular medical history, primary indication for initiation of ranibizumab treatment, and prior ocular treatments. Baseline lesion characteristics (lesion type, pigment epithelial detachment [PED], polypoidal choroidal vasculopathy [PCV], retinal angiomatous proliferation) for patients with nAMD were optional and collected if available, and were determined based on investigators’ judgement. PCV was typically diagnosed based on the presence of active macular polypoidal lesions with indocyanine green angiography.
Effectiveness was assessed using VA as the functional parameter for all patients and CRT as the anatomical parameter on available data. VA, and preferably best-corrected visual acuity (BCVA), was evaluated from baseline at visits per the treating physician’s discretion, using Early Treatment Diabetic Retinopathy Study (ETDRS)-like or Snellen charts. Snellen fractions and decimals were converted to the ETDRS equivalent letter scores to facilitate statistical analysis. Optical coherence tomography, to assess CRT, and ocular examination, to assess pre-injection intraocular pressure, were optional but included if the data were available. The number of ranibizumab injections administered overall, visit frequency, and treatment patterns were recorded. All AEs, irrespective of suspected causal association that occurred during the study, were collected.
Statistical Analysis
All effectiveness and safety data were summarized descriptively. The enrolled set included all patients who signed the informed consent and had at least a baseline assessment. The safety set comprised patients in the enrolled set who were treated with at least one dose of ranibizumab during the study or prior to study initiation and had at least one safety assessment post-initial treatment. The primary treated eye set included all primary treated eyes in patients included in the safety set. Treatment-naïve eyes are defined as eyes that have not been pre-treated with any intravitreal medication; prior-treated eyes are defined as eyes previously treated with any intravitreal medication (including ranibizumab). For treatment-naïve eyes, the date of first on-study injection with ranibizumab was considered the baseline date. For prior-treated eyes that were previously treated with ranibizumab, the date of study entry was considered the baseline date. Patients were generally stratified based on pre-treatment status (treatment-naïve/prior-treated) for all safety and effectiveness analyses.
The loading dose was defined as receiving at least 3 ranibizumab injections within 120 days from the baseline date. The mean change in VA from baseline at 1 year was analyzed by loading dose status (yes/no), injection frequency (0–<3, 3–6, and >6), baseline VA category (<23, 23–<39, 39–<60, 60–<74, and ≥74 letters), and PCV status (PCV/non-PCV). Logistic regression analysis was performed to investigate the factors that were associated with VA change (any VA improvement and ≥5 letters improvement from baseline at 1 year). Predictors with a P value <0.05 in the univariate analysis were considered significant and were fitted into the multivariate logistic regression. Changes in CRT from baseline at 1 year was analyzed by PCV status (PCV/non-PCV). A two-sided Student’s t-test was performed to compare demographics, characteristics, and mean change in VA and CRT between patient subgroups, and VA and CRT at baseline and Year 1. Statistical significance was defined as a P value of <0.05. The number of injections and monitoring visits up to 1 year were summarized for patients with VA assessed at Year 1. Safety over the 1- and 5-year periods was assessed based on the number and proportion of patients with ocular and non-ocular AEs. Ocular AEs were assessed for the primary treated eye set and non-ocular AEs were assessed for the safety set. No missing data imputation was carried out. Descriptive analysis was presented using observed data, whereas modelling analysis were performed on complete case (patients without missing data of relevant parameters or endpoints).
Results
Patient Disposition, Baseline Ocular Characteristics, and Treatment Patterns
The LUMINOUS study enrolled 30,138 patients worldwide across all approved indications.11 In this subgroup analysis, 367 Korean patients were enrolled. The safety set comprised 152 treatment-naïve and 215 prior-treated patients who were treated with ≥1 dose of ranibizumab during the study or prior to study initiation and had ≥1 safety assessment post-initial treatment. Overall, 159 (43.3%) patients discontinued the study by Year 1, of which 80 were treatment-naïve and 79 were prior-treated. In total, 265 (72.2%) patients discontinued the study by the end of Year 2, of which 116 were treatment-naïve and 149 were prior-treated. The main reasons for study discontinuation were loss to follow-up and patient switching to another anti-VEGF (Figure 1).
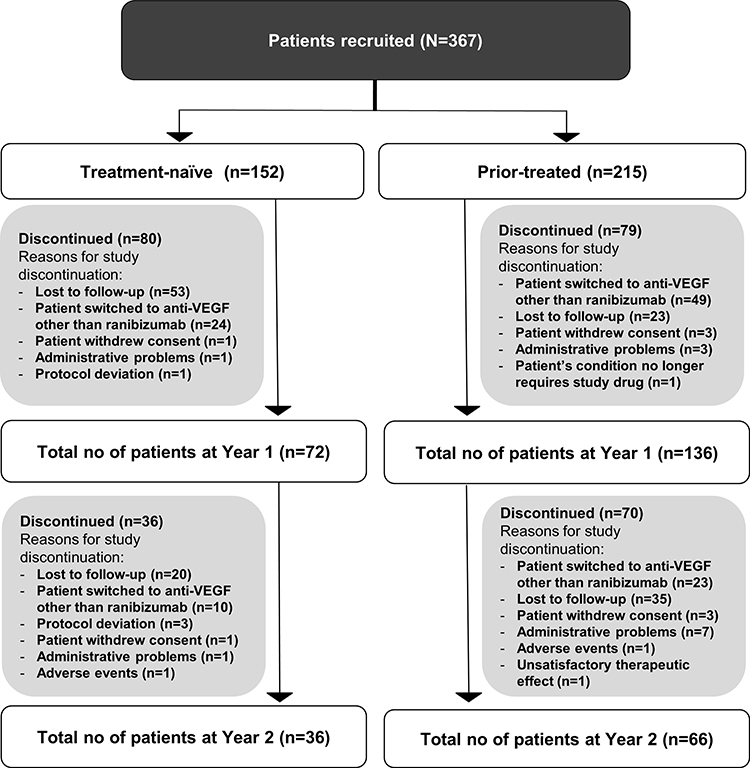 |
Figure 1 Disposition of Korean patients with nAMD. The safety set comprised patients in the enrolled set who were treated with at least one dose of ranibizumab during the study or prior to study initiation and had at least one safety assessment post-initial treatment. Patients with a baseline visit on or before March 2015 were included. Abbreviations: N, total number of patients; n, number of patients; nAMD, neovascular age-related macular degeneration; VEGF, vascular endothelial growth factor. |
At baseline, the mean (standard deviation [SD]) age was 72.2 (9.18) years in the treatment-naïve and 71.0 (8.20) years in the prior-treated patient groups. The majority of patients were male in both treatment-naïve (67.8%) and prior-treated (67.0%) patients. The patient demographics and baseline characteristics are summarized in Table 1. Generally, all baseline lesion characteristics were comparable. Compared with prior-treated patients, treatment-naive patients reported a lower mean (SD) VA (43.1 [26.30] vs 54.3 [21.29] letters, P<0.0001) and thicker CRT (400.3 [151.59] vs 288.8 [86.55] µm, P<0.0001) at baseline (Table 1). The median time from diagnosis to treatment was 4 days in treatment-naïve patients and 199 days in prior-treated patients (P<0.0001). A total of 192 (53.32%) patients received the loading dose and the proportion of patients who received the loading dose was relatively higher in treatment-naïve patients (82.90%) compared with prior-treated patients (30.70%) (P<0.0001). The median time of follow-up was 312 days in treatment-naïve patients and 442 days in prior-treated patients (P=0.0350) (Table 1). The baseline demographics and characteristics of patients with and without PCV is shown in Table S1.
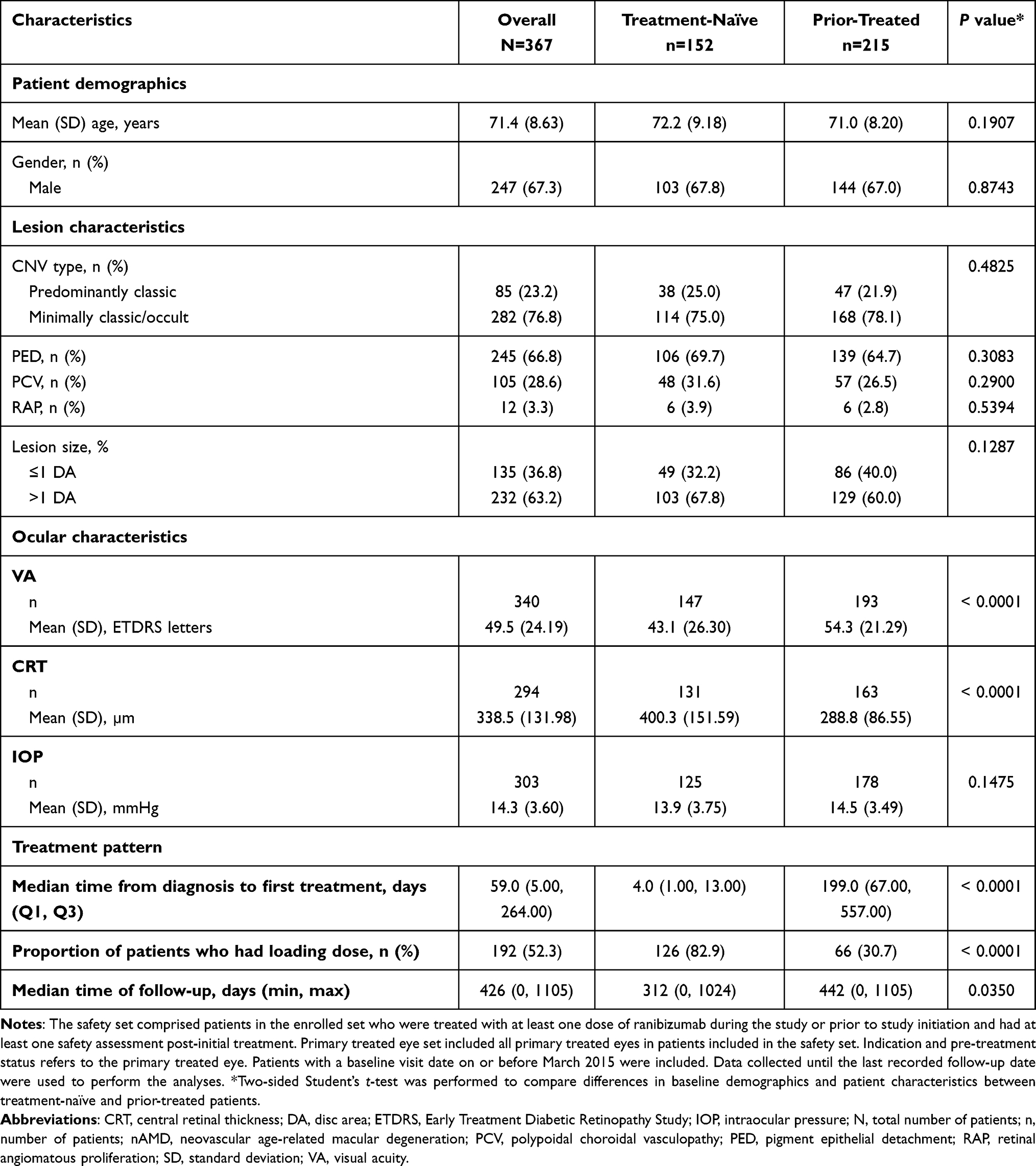 |
Table 1. Baseline Demographic, Patient Characteristics and Treatment Pattern at Year 1: Safety Set and Primary Treated Eye Set |
Effectiveness Outcomes
Visual Acuity
The mean (SD) VA at baseline, month 12 and month 24 were: 43.1 (26.30), 61.6 (23.31) and 63.4 (23.20) letters in treatment-naïve patients, and 54.3 (21.29), 57.4 (20.35) and 53.1 (25.11) letters in prior-treated patients. Figure 2 shows the changes in mean VA for the primary treated eyes from baseline to 2 years. VA improvements were observed as early as 3 months post-baseline and treatment-naïve patients showed a higher VA gain compared with prior-treated patients (Figure 2, mean [SD] +9.0 [17.21] vs +3.1 [11.71] letters), a trend that was maintained from 3 to 21 months. At Month 24, there was a decline in the number of patients continuing in the study with evaluable VA in both groups (treatment-naïve, n=20; prior-treated, n=30). At Month 24, the mean (SD) change in VA were +3.2 (26.18) letters and +6.7 (21.88) letters in treatment-naïve and prior-treated patients, respectively.
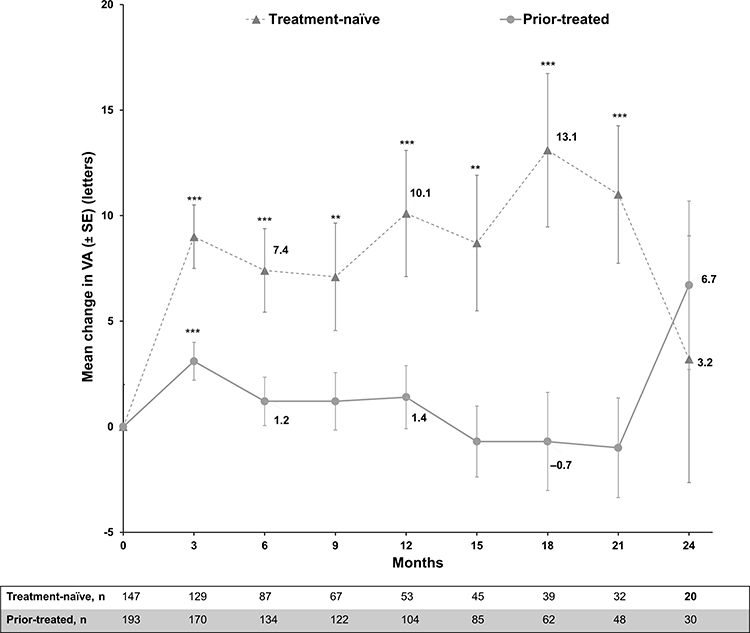 |
Figure 2 Mean change from baseline in visual acuity (ETDRS letter score): primary treated eye set. Primary treated eye set included all primary treated eyes in patients included in the safety set. Mean ± SE was presented. The study entry date was defined as baseline date if the primary-treated eye has been pre-treated with ranibizumab. If the eyes were not pre-treated with ranibizumab, the date of the first on-study ranibizumab injection was considered as the baseline date. Statistical analyses were performed using two-sample Student’s t-tests to compare VA between baseline and specific time point, **P<0.01, ***P<0.001. Abbreviations: ETDRS, Early Treatment Diabetic Retinopathy Study; n, number of patients, SE, standard error; VA, visual acuity. |
At Month 12, the mean VA significantly increased from baseline by +10.1 (21.77) letters (P=0.0005) in treatment-naïve patients, while the VA letter change was +1.4 (15.17) letters (P=0.2142) in prior-treated patients. The mean (SD) VA at Month 12 was comparable in both treatment-naïve (61.6 [23.31] letters) and prior-treated patients (57.4 [20.35] letters) (Figure 3A). When stratified by baseline VA of <23, 23–<39, 39–<60, 60–<74, and ≥74 letters, mean VA changes after 1 year of ranibizumab treatment were +20.8, +21.8, +11.7, +4.2, and –1.9 letters in treatment-naïve patients, and +21.0, +5.1, +2.0, +0.4, and –5.0 letters in prior-treated patients, respectively (Figure 3B). When stratified by patients who did or did not receive the loading dose, mean VA changes after 1 year of ranibizumab treatment were +10.2 and +4.0 letters in treatment-naïve patients and +6.0, and −0.7 letters in prior-treated patients (Figure 4A). When presented by injection frequencies over 1 year, the mean change in VA letter score was +4.0, +10.8, and +8.0 in treatment-naïve patients who received 0–<3, 3–6, and >6 injections, respectively. The mean change in VA letter score was lower in prior-treated patients, with changes of +2.8, +0.4, and +1.7 in patients who received 0–<3, 3–6, and >6 injections, respectively (Figure 4B).
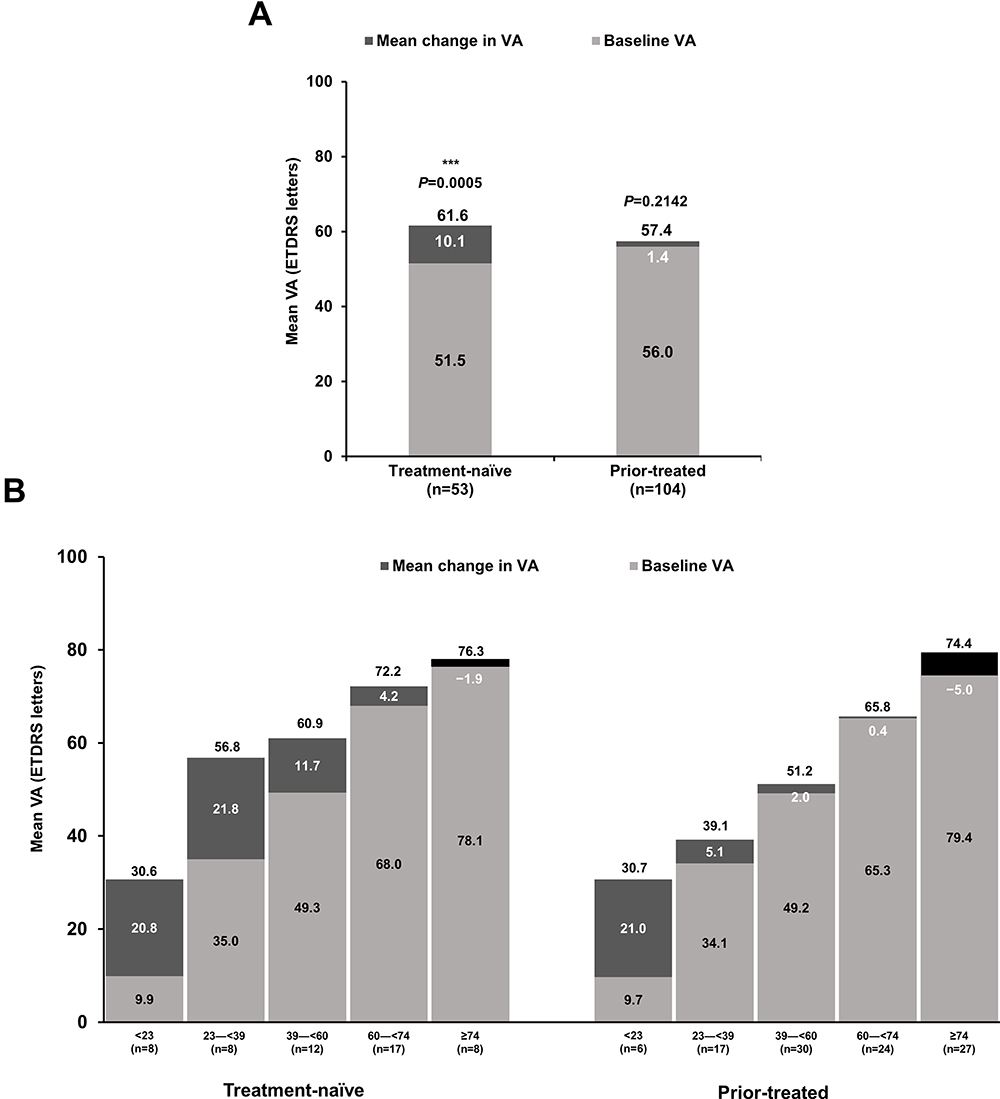 |
Figure 3 Mean change in VA from baseline to Month 12 in primary treated eye set by (A) pre-treatment status; (B) baseline VA. Observed data set for VA change in primary treated eye set. Primary treated eye set included all primary treated eyes in patients included in the safety set. Statistical analyses were performed using two-sample Student’s t-tests to compare VA between baseline and Year 1, ***P<0.001. Abbreviations: ETDRS, Early Treatment Diabetic Retinopathy Study; n, number of patients; VA, visual acuity. |
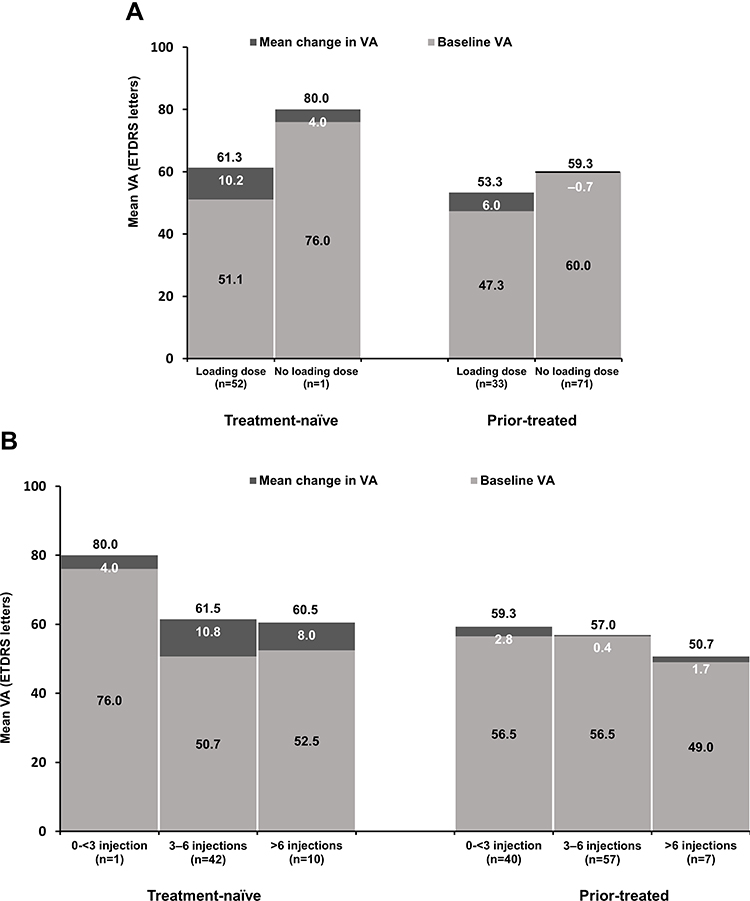 |
Figure 4 Mean change in VA from baseline to Month 12 in primary treated eye set by (A) loading dose status (B) injection number. Observed data set for VA change in primary treated eye set. Primary treated eye set included all primary treated eyes in patients included in the safety set. Loading dose was defined as receiving at least 3 ranibizumab injection within 120 days from baseline date. Abbreviations: ETDRS, Early Treatment Diabetic Retinopathy Study; n, number of patients; VA, visual acuity. |
When presented by PCV status in treatment-naïve patients, the mean change in VA was +16.7 letters in patients with PCV, and +6.7 letters in patients without PCV, the differences was not statistically significant (P=0.1169). Similarly, in prior-treated patients, the mean change in VA was +4.0 letters in patients with PCV and +0.5 letters in patients without PCV (P=0.1958). In the overall population, including both treatment-naïve and prior-treated patients, the difference in mean change was 6.5 letters (PCV vs non-PCV:+9.0 vs +2.5 letters, P=0.0388) (Figure 5).
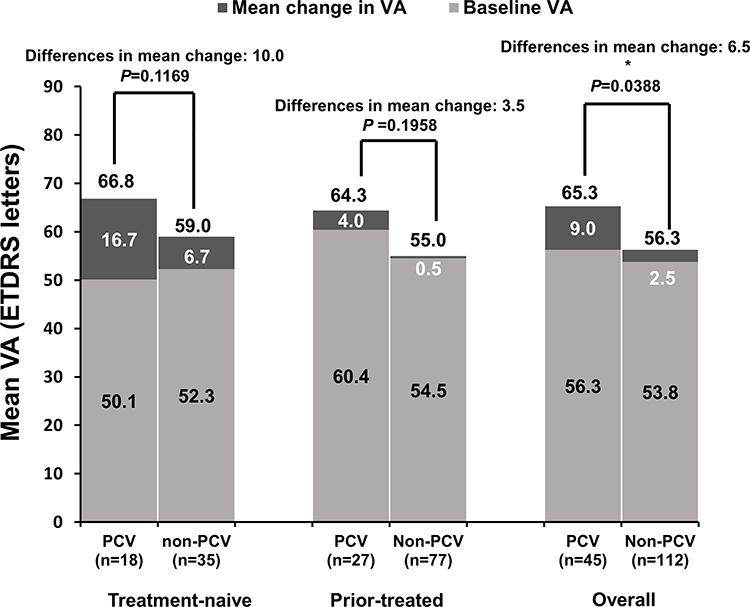 |
Figure 5 Mean change in VA from baseline to Month 12 by PCV status: primary treated eye set. Observed data set for VA change in primary treated eye set. Primary treated eye set included all primary treated eyes in patients included in the safety set. Statistical analyses were performed using two-sample Student’s t-tests to compare the mean change in VA between patients with/without PCV, *P < 0.05. Abbreviations: ETDRS, Early Treatment Diabetic Retinopathy Study; n, number of patients; PCV, polypoidal choroidal vasculopathy; VA, visual acuity. |
Association of Baseline Characteristics and Visual Outcomes
Univariate analysis showed that younger age (P=0.0087), lower baseline VA (P=0.0131), and patients who received a loading dose (P=0.0159) were associated with higher odds of any gain in VA by Month 12. Treatment-naïve (P=0.0038) patients with worse baseline VA (P=0.0051) who received a loading dose (P=0.0010) were associated with higher odds to gain ≥5 VA letters by Month 12. Multivariate analysis showed that younger age (P=0.0021), worse baseline VA (P=0.0190), and patients who received loading dose (P=0.0410) were associated with higher odds of having any gain in VA by Month 12. However, only worse baseline VA (P=0.0313) was associated with a better response to ranibizumab treatment for a gain of ≥5 VA letters (Table 2).
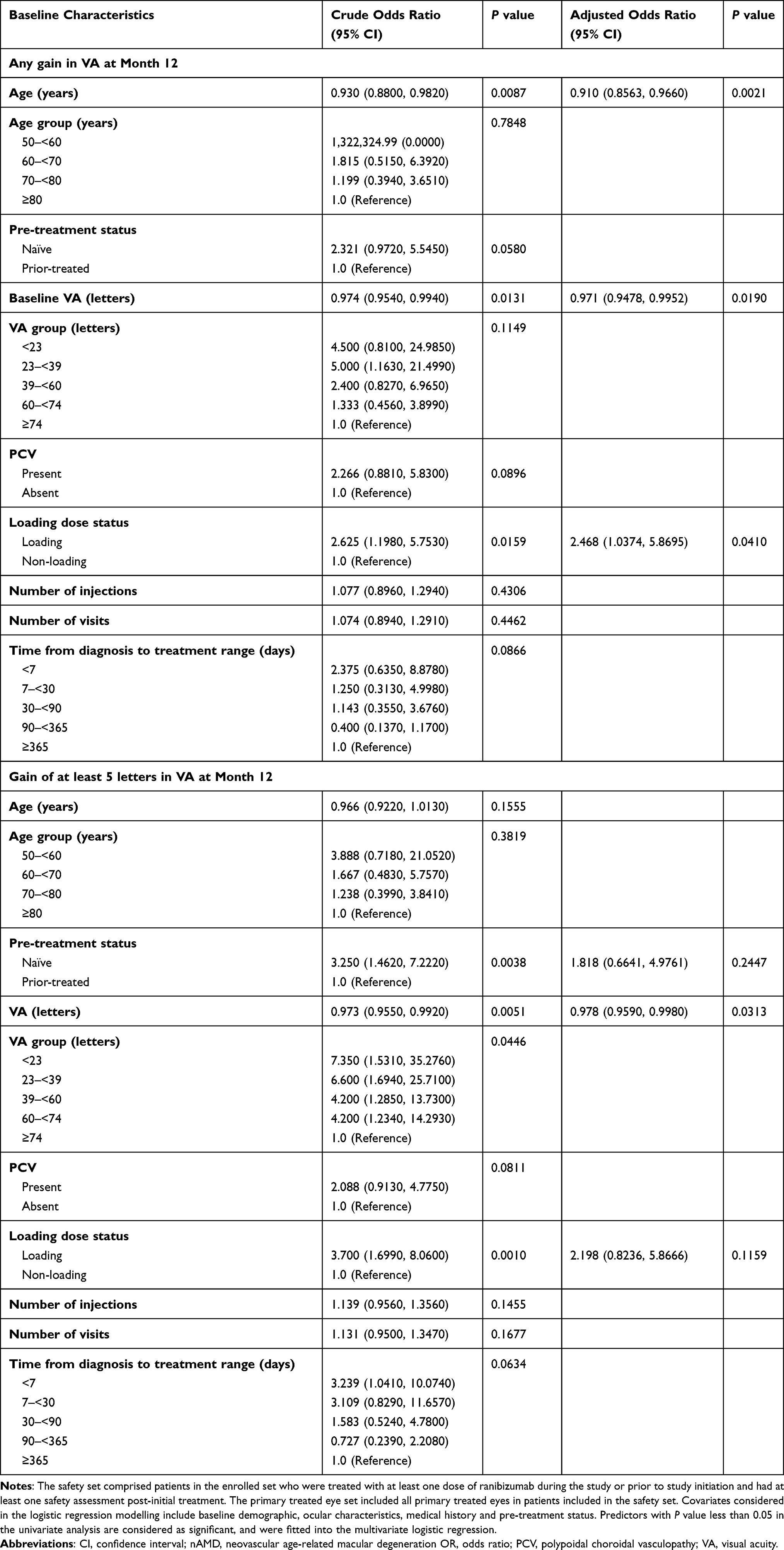 |
Table 2. Association of Visual Acuity Change with Baseline Characteristics and Treatment Pattern in Korean Patients with nAMD: Safety Set and Primary Treated Eye Set |
Treatment Exposure and Patient Visits for Patients with VA Assessed at Year 1
Overall, in patients with VA assessed at Year 1, the mean (SD) number of ranibizumab injections administered up to Year 1 was higher in treatment-naïve patients (5.2 [1.8]) compared with prior-treated patients (3.4 [2.1]). Similarly, the mean (SD) number of monitoring visits was also higher in treatment-naïve patients (9.2 [2.6]) compared with prior-treated patients (6.8 [2.8]). In the first year, the majority of treatment-naïve patients received ≥4 injections (77.3%), while only 44.2% of prior-treated patients received ≥4 injections (Figure 6).
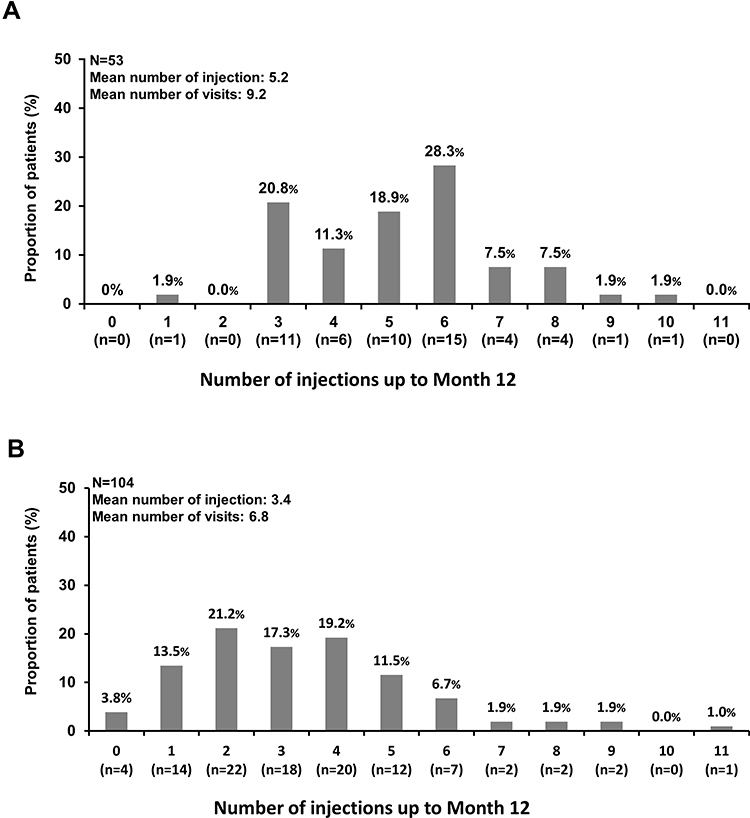 |
Figure 6 Frequency of visit and injections over 12 months in Korean patients with nAMD and VA assessed at Month 12 in primary-treated eye and safety sets (A) treatment-naïve patients; (B) prior-treated patients. The safety set comprised patients in the enrolled set who were treated with at least one dose of ranibizumab during the study or prior to study initiation and had at least one safety assessment post-initial treatment. Primary treated eye set included all primary treated eyes in patients included in the safety set. Abbreviations: n, number of evaluable patients with baseline and Month 12 data; nAMD, neovascular age-related macular degeneration; VA, visual acuity. |
Central Retinal Thickness
The mean (SD) CRT at baseline, month 12 and month 24 were: 400.3 (151.59), 272.4 (83.82) and 234.6 (55.21) µm in treatment-naïve patients, and 288.8 (86.55), 292.0 (95.65) and 248.6 (57.95) µm in prior-treated patients. Figure 7 shows the changes in mean CRT for the primary treated eyes from baseline to 2 years. Similar to VA improvement, reduction of CRT was observed as early as 3 months post-baseline and treatment-naïve patients showed a greater CRT reduction (mean [SD] –115.2 [147.41] vs –8.9 [67.14] µm). This trend of better CRT improvement in treatment-naïve patients relative to prior-treated patients was maintained from 3 months to 2 years. At Month 12, the overall mean (SD) CRT reductions were –126.7 (174.90) µm (P<0.0001) in treatment-naïve patients and +10.8 (89.62) µm (P=0.5833) in prior-treated patients. The mean (SD) CRT at Month 12 was comparable for treatment-naïve (272.4 [83.82] µm) and prior-treated patients (292.0 [95.65] µm; Figure S1). At Month 24, the mean (SD) CRT reductions were –97.6 (84.92) µm in treatment-naïve patients and –0.7 (48.75) µm in prior-treated patients (Figure 7).
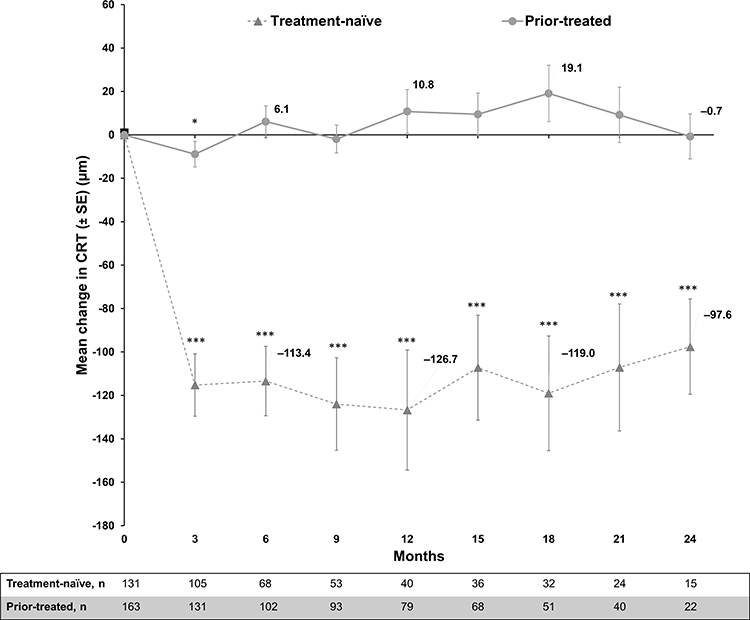 |
Figure 7 Mean change from baseline in CRT (µm): Primary treated eye set. Primary treated eye set included all primary treated eyes in patients included in the safety set. Mean ± SE was presented. The study entry date was defined as baseline date if the primary-treated eye has been pre-treated with ranibizumab. If the eyes were not pre-treated with ranibizumab, the date of the first on-study ranibizumab injection was considered as the baseline date. Statistical analyses were performed using two-sample Student’s t-tests to compare CRT between baseline and specific time point, *P<0.05, ***P<0.001. Abbreviations: CRT, central retinal thickness; n, number of patients; SE, standard error. |
When stratified by PCV and non-PCV, mean CRT changes after 1 year of ranibizumab treatment were –160.6 µm and –99.0 µm in treatment-naïve patients (mean differences in change: 61.6 µm P=0.3025) and –14.9 µm and +20.1 µm in prior-treated patients (mean difference in change: 35.0 µm, P=0.1266), respectively. In the overall group, including both treatment-naïve and prior-treated patients, the mean differences in change between PCV and non-PCV patients was 69.4 µm (P=0.0293; Figure S2).
Safety Outcomes
Over the 5-year period, the overall rate of ocular and non-ocular AEs in patients was 8.4% and 10.1%, respectively. Table S2 lists all ocular and non-ocular AEs by the end of the 5-year period. In treatment-naïve and prior-treated patients, ocular AEs were reported in 10.5% and 7.0% of patients, respectively. Conjunctival hemorrhage in 3 treatment-naïve patients (2.0%) and cataract in 1 treatment-naïve patient (0.7%) were suspected to be related to ocular injection and/or ranibizumab treatment (Table S3). Non-ocular AEs were reported in 11.8% and 8.8% of treatment-naïve and prior-treated patients, respectively (Table S2). No patients reported a non-ocular AE suspected to be related to ocular injection and/or ranibizumab. Table S4 showed the rate of ocular and non-ocular AEs by preferred term by the end of Year 1.
Discussion
To our knowledge, the LUMINOUS subgroup analysis represents the first long-term study in Korean patients with nAMD assessing the real-world effectiveness and safety of ranibizumab 0.5 mg. The study findings demonstrated that ranibizumab 0.5 mg resulted in improved VA and CRT outcomes at the end of Year 2 in treatment-naïve patients. Also, by Year 1, patients who were treatment-naïve, those with worse baseline VA, and those who received a loading dose achieved better VA gain. In patients with PCV, better VA and CRT improvements were observed at the end of Year 1. Multivariate logistic regression analyses confirmed that younger age, worse baseline VA and those receiving a loading dose were associated with higher odds of having any gain in VA by Year 1. Overall, ranibizumab 0.5 mg was well tolerated with no new safety findings in the real-world setting, consistent with the findings of global LUMINOUS nAMD populations.
In the current study, 43.3% and 72.2% of patients discontinued by Years 1 and 2, respectively, with loss to follow-up and patient switching to another anti-VEGF being the main reasons for study discontinuation. This highlights poor compliance of patients returning to the clinic for follow-up, likely due to high treatment burden12 or patient relocation and transfer to another healthcare facility. The high discontinuation rate was expected, and aligned with real-world trends in Korea, that have also been reported in other real-world studies.13,14 In the current study, 28.9% of patients switched to anti-VEGFs other than ranibizumab, and the majority were prior-treated. The 2019 Preferences and Trends Survey showed that 68.4% of Asia Pacific physicians would switch to another anti-VEGF when patients do not respond adequately to first-line anti-VEGF therapy.15 This switching is to potentially improve visual outcomes in patients who do not respond adequately to initial treatment, assuming potential differences in the molecular structure and biochemical properties of anti-VEGFs, and thus effect.16 In addition, when the LUMINOUS global study was conducted, the national health insurance system in Korea had set reimbursement limitations for ranibizumab injection. Thus, patients that required additional anti-VEGF treatment over and above the reimbursement limit might have switched to a more cost effective option, such as bevacizumab (off-label use).10
Comparing baseline characteristics of treatment-naïve patients in the Korean and global populations of the LUMINOUS study, it was observed that the former had a slightly lower baseline VA (43.1 vs 49.7 letters), higher baseline mean CRT values (400.3 vs 365.7 µm), a higher proportion of minimally classic/occult CNV lesion type (75.0 vs 55.4%), PED (69.7 vs 42.7%), and PCV (31.6 vs 9.2%).11 In the current study, PCV was diagnosed in 28.6% of Korean patients with nAMD regardless of pre-treatment status. This observation is aligned with the finding that PCV prevalence was observed to be higher in the Asian population; PCV is shown to occur in ~22–55% of Asian and 4–14% of Caucasian patients with nAMD.17
Both VA gain and CRT improvements were better in treatment-naïve patients compared with those prior-treated. This result is consistent with findings from Levy et al 18 and the Korean PMS study10 which demonstrated that prior-treated patients generally do not show as much response to anti-VEGFs as treatment-naïve patients. Prior-treated patients had relatively better baseline VA and CRT, which would have likely benefited from previous anti-VEGF treatment. Even though the VA gain and CRT reduction were better in treatment-naïve patients, both groups had comparable VA (61.6 vs 57.4 letters) and CRT (272.4 vs 292.0 µm) values at Year 1. The result was consistent with findings that ranibizumab 0.5 mg stabilizes vision in nAMD patients with relatively good baseline VA.19,20 The higher VA gain of treatment-naïve patients than that of prior-treated patients was not maintained at Year 2, which is likely due to large variations in VA between the low number of patients who remained in the study in both groups, and may not reflect the actual trend.
In Korean patients with VA assessed at Year 1, treatment-naïve patients received a higher number of injections (5.2) and recorded a higher number of monitoring visits (9.2) by Year 1 compared with prior-treated patients (3.4 injections, 6.8 visits). Compared with the global LUMINOUS treatment-naïve population, the Korean treatment-naïve patients reported comparable injection numbers (5.2 vs 5.0) and monitoring visits (9.2 vs 8.8),11 yet with a relatively better VA outcome (VA gain of 10.1 vs 3.1 letters). The VA gain observed in prior-treated patients was consistent with that of the global population, whereby patients treated with ranibizumab maintained their vision at Year 1.11,21 The better visual outcomes in treatment-naïve Korean patients compared with the treatment-naïve global population might also be attributed to a relatively younger age (72.2 vs 75.0 years), a worse baseline VA (43.1 vs 49.7 letters), and a shorter time from diagnosis to first treatment (4 vs 12 days).11,21 The VA gain reported in treatment-naïve patients in this subgroup analysis was comparable to those reported in the pivotal MARINA and ANCHOR studies (7.2 letters in MARINA22 and 11.3 letters in ANCHOR23), but relatively higher than randomized controlled trials conducted in Korea and other real-world studies. Kim et al demonstrated that treatment-naïve Korean patients with nAMD treated with a mean of 4.5 injections showed significant BCVA improvement (0.14 logMAR, P=0.017) and CRT reduction (139.3µm, P <0.001) from baseline to Year 1.7 In the REAL study conducted in Taiwanese patients with nAMD, the mean number of ranibizumab injections was 3.2 and the VA gain at 1 year was only 1.1 letters.24 The AURA study reported comparable injection numbers in Year 1 (5 injections) with a VA gain of 2.4 letters.25 Similarly, the LUMIERE study reported a lower VA gain (3.2 letters) with a comparable number of injections (5.1) in Year 1 versus the current study.19 The UNCOVER study reported 4.2 injections and 7 visits per year with a VA reduction of 0.7 letters in Year 1.26 However, most of the pivotal trials and real-world studies did not stratify the results based on prior-treatment status. CRT reduction in treatment-naïve patients in this study (160.6 µm) was also better than other real-world studies of ranibizumab (51.5 µm in Providência et al).27
The median time from diagnosis to treatment in treatment-naïve patients in this subgroup analysis was relatively short (4 days) compared with the global LUMINOUS population (12 days).11 Korean patients can easily visit retina clinics without referral from primary physicians, and the short distance from home to clinics or hospitals in Korea might enable early detection and timely treatment of nAMD patients. It has been established that delay from symptoms to anti-VEGF treatment is associated with reduced VA outcome.28 Timely initiation of anti-VEGF treatment might also explain the favorable visual outcome in the Korean nAMD population in the current study compared with the LUMINOUS global population, as well as other real-world studies.
Stratified by different baseline characteristics and treatment categories, it was demonstrated that in both treatment-naïve and prior-treated patients those with worse baseline vision (<23 letters and 23–<39 letters), those who received the loading dose, and those with PCV achieved higher VA gain by Year 1. Although VA improvement at Year 1 was notably higher in treatment-naïve compared with prior-treated patients, univariate logistic regression analyses did not support the association of pre-treatment status to any gain of VA, but showed that treatment-naïve patients have higher odds of achieving a VA gain of ≥5 letters by Year 1. However, multivariate logistic regression analysis showed that only patients with younger age, worse baseline VA, and those who received a loading dose were associated with higher odds of any gain in VA by Year 1, while only patients with worse baseline VA was associated with VA gain of ≥5 letters in Year 1.
Younger age as a prediction factor for better response to ranibizumab treatment is in-line with the Korean PMS study10 and several post hoc analyses of pivotal trials and studies assessing predictors of response to ranibizumab.29–34 Findings from the current study also strengthen the observation regarding baseline VA being an important factor in predicting visual outcome, consistent with the Korean PMS study,10 the study by Pedrosa et al 35 the LUMIERE study,19 and the global LUMINOUS study.11,21 These findings could be explained by the “ceiling effect” whereby patients with higher baseline VA have limited potential to gain more letters, while those with lower baseline VA have little possibility for further loss of vision. However, patients with higher baseline VA had relatively higher mean VA by the end of Year 1; ie, the VA at Year 1 were highest in patients with baseline VA of ≥74 letters in both treatment-naïve and prior-treated patients. The result indicated that even though eyes with poor VA responded well to treatment, they did not catch up with eyes with better baseline VA.
Additionally, Korean patients who received the loading dose showed better VA improvement compared with those who did not, which is consistent with the BeMOc study,20 the real-world LUMIERE study,19 and the global LUMINOUS study.11 It should also be noted that in both treatment-naïve and prior-treated groups, patients who received a loading dose had worse baseline VA compared with patients who did not. However, multivariate analyses adjusted for age and baseline VA confirmed that receiving a loading dose is associated with any gain in VA in Year 1. Findings from LUMINOUS highlighted the importance of receiving a loading dose for VA improvements. This was not aligned with findings from the ARTIS study which showed that ranibizumab treatment regimens with 1 and 3 initial injections followed by a pro re nata regimen are equally effective in improving VA.36
VA gain and CRT reduction in the Korean treatment-naïve patients with PCV (16.7 letters and 160.6 µm) was better than the global treatment-naïve population with PCV (5.0 letters and 91.3 µm).37 The better visual outcome in treatment-naïve Korean patients with PCV compared with the treatment-naïve global population with PCV might be due to a relatively younger age (68.4 vs 72.8 years) and a worse baseline VA (49.0 vs 53.8 letters).37 However, due to the small sample size and large variance in the current subgroup analyses, no statistically significant difference was noted in differences in changes in VA and CRT between treatment-naïve PCV and non-PCV patients (P>0.05). Nonetheless, when VA and CRT were compared between patients with and without PCV in the overall group including both treatment-naïve and prior-treated patients, the differences in mean change was statistically significant for both VA (P=0.0388) and CRT (P=0.0293) at Year 1. In this subgroup analyses, PCV patients were relatively younger compared with patients without PCV (treatment-naïve: 68.4 vs 73.9 years, P=0.0514; prior-treated: 68.7 vs 71.8 years; P=0.8609); this is in line with previous studies that showed PCV tends to present in younger Asian patients compared with typical CNV.38–40 In fact, univariate and multivariate logistic regression analysis did not support an association of having PCV with any VA gain or gain of ≥5 letters at Year 1. The age difference between the PCV and non-PCV patients in this subgroup analyses might have driven the differences in the outcome at Year 1.
In both treatment-naïve and prior-treated Korean patients with nAMD in this subgroup analyses, the frequency of ocular and non-ocular AEs over 1 and 5 years was low and were consistent with the well-established safety profile of ranibizumab with no new safety findings identified.10,22,23 Ocular AEs related to ranibizumab treatment and/or ocular injection were rare. There was no significant difference in the rate of ocular or systemic AEs between the treatment-naïve and prior-treated patients.
The current study had various limitations. The high discontinuation rate only allowed the treatment effectiveness to be meaningfully analyzed up to 2 years. Being a real-world study, there was no comparator arm. There could be treatment bias due to patient’s access to treatment, physicians’ treatment decisions based on clinical judgement, local healthcare systems, and reimbursement policies, which limit interpretation of data to some extent. Besides, there were no strict criteria for disease diagnosis at the time of patient enrolment; hence, results may vary between study sites. Most of the limitations described are common to any real-world evidence study which collect real-world clinical practice data. The low number of patients with PCV also limits confirmation on the effect of ranibizumab in treatment-naïve Korean patients with nAMD and PCV, and needs to be validated in a prospective study with a larger sample size and longer follow-up period.
Conclusion
To conclude, real-world evidence from the LUMINOUS subgroup analysis in Korean patients with nAMD confirmed the long-term effectiveness and safety of ranibizumab 0.5 mg for the treatment of nAMD, including PCV. In addition, Korean patients achieved better effectiveness outcomes compared with the global population, with a comparable number of injections and patient clinic visits in Year 1. The safety findings were consistent with the well-established safety profile of ranibizumab. The current study findings may help ophthalmologists to understand treatment outcomes in real-world clinical practice in Korean nAMD patients and assist in optimizing the treatment and clinical management of the disease.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The LUMINOUS study was conducted in accordance with the Guidelines for Good Pharmacoepidemiology Practices issued by the International Society for Pharmacoepidemiology, with any applicable national guidelines and ethical principles laid down in the Declaration of Helsinki. The study protocol was reviewed and approved by an Independent Ethics Committee or Institutional Review Board for each center. Patients provided written informed consent.
Acknowledgments
The authors thank all the investigators (global11 and South Korea (Table S5) and patients in the LUMINOUS™ study for their valuable contribution towards this study. The authors thank Khi Khi Choo, PhD (Novartis Corporation Malaysia) and Najeeb Ashraf, MD, MBA (Novartis Healthcare Pvt. Ltd. India) for providing medical writing support/editorial support, which was funded by Novartis, in accordance with Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3).
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
Novartis Pharma AG, Basel, Switzerland sponsored the LUMINOUS study and was involved in the study design, conducting the study, and data collection, management, analysis, and interpretation. Novartis Korea funded the subgroup analyses, medical writing and editorial assistance for this article.
Disclosure
Youkyung Lee is a full time employee of Novartis Korea Ltd. Se Joon Woo is a paid consultant of Samsung Bioepis Inc., Songdo, South Korea and Novelty Nobility Inc., Seoul, South Korea; reports grants from Curacle, Novartis, Bayer, Allergan, Abbie, Alcon, SCAI Therapeutics, Alteogen, and Philophos, and is a co-founder of RetiMark Inc., in Seoul, South Korea. Dr Min Sagong reports grants from Novartis, Allergan, and Bayer, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. World Health Organization. Blindness and vision impairment; 2019. Available from: https://www.who.int/news-room/fact-sheets/detail/blindness-and-visual-impairment.
2. Park SJ, Lee JH, Woo SJ, et al. Age-related macular degeneration: prevalence and risk factors from Korean national health and nutrition examination survey, 2008 through 2011. Ophthalmology. 2014;121(9):1756–1765. doi:10.1016/j.ophtha.2014.03.022
3. Park SJ, Kwon K, Choi N-K, Park KH, Woo SJ. Prevalence and incidence of exudative age-related macular degeneration in South Korea: a nationwide population-based study. Ophthalmology. 2015;122(10):2063–2070.e1. doi:10.1016/j.ophtha.2015.06.018
4. Flaxel CJ, Adelman RA, Bailey ST, et al. Age-related macular degeneration preferred practice pattern®. Ophthalmology. 2019;127(1):P1–P65. doi:10.1016/j.ophtha.2019.09.024
5. Cornel S, Adriana ID, Mihaela TC, et al. Anti-vascular endothelial growth factor indications in ocular disease. Rom J Ophthalmol. 2015;59(4):235–242.
6. Novartis. Lucentis (ranibizumab) PFS Korean NPI; Published online 2019.
7. Kim JH, Lee DW, Chang YS, Kim JW, Kim CG. Twelve-month outcomes of treatment using ranibizumab or aflibercept for neovascular age-related macular degeneration: a comparative study. Graefes Arch Clin Exp Ophthalmol. 2016;254(11):2101–2109. doi:10.1007/s00417-016-3353-7
8. Kang HM, Koh HJ. Long-term visual outcome and prognostic factors after intravitreal ranibizumab injections for polypoidal choroidal vasculopathy. Am J Ophthalmol. 2013;156(4):652–660. doi:10.1016/j.ajo.2013.05.038
9. Shin JY, Yu HG. Optical coherence tomography-based ranibizumab monotherapy for retinal angiomatous proliferation in Korean patients. Retina. 2014;34(12):2359–2366. doi:10.1097/IAE.0000000000000225
10. Woo SJ, Cho GE, Cho JH. Short-term efficacy and safety of ranibizumab for neovascular age-related macular degeneration in the real world: a post-marketing surveillance study. Korean J Ophthalmol. 2019;33(2):150–166. doi:10.3341/kjo.2018.0081
11. Holz FG, Figueroa MS, Bandello F, et al. Ranibizumab treatment in treatment-naive neovascular age-related macular degeneration: results From LUMINOUS, a Global Real-World Study. Retina. 2019. doi:10.1097/IAE.0000000000002670
12. Parikh R, Pirakitikulr N, Chhablani J, Sakurada Y, Singh RP, Modi YS. A multinational comparison of anti–vascular endothelial growth factor use: the United States, the United Kingdom, and Asia-Pacific. Opthalmol Retina. 2019;3(1):16–26. doi:10.1016/j.oret.2018.08.002
13. Lotery A, Griner R, Ferreira A, Milnes F, Dugel P. Real-world visual acuity outcomes between ranibizumab and aflibercept in treatment of neovascular AMD in a large US data set. Eye (Lond). 2017;31(12):1697–1706. doi:10.1038/eye.2017.143
14. Khanani AM, Skelly A, Bezlyak V, Griner R, Torres LR, Sagkriotis A. SIERRA-AMD: a retrospective, real-world evidence study of patients with neovascular age-related macular degeneration in the USA. Opthalmol Retina. 2019;4(2):122–133. doi:10.1016/j.oret.2019.09.009
15. American Society of Retina Specialist. 2019 global trends in retina survey; 2019. Available from: https://www.asrs.org/content/documents/2019-global-trends-survey-for-website.pdf.
16. Mantel I, Gillies MC, Souied EH. Switching between ranibizumab and aflibercept for the treatment of neovascular age-related macular degeneration. Surv Ophthalmol. 2018;63(5):638–645. doi:10.1016/j.survophthal.2018.02.004
17. Hatz K, Prünte C. Polypoidal choroidal vasculopathy in caucasian patients with presumed neovascular age-related macular degeneration and poor ranibizumab response. Br J Ophthalmol. 2014;98(2):188–194. doi:10.1136/bjophthalmol-2013-303444
18. Levy J, Shneck M, Rosen S, et al. Intravitreal bevacizumab (avastin) for subfoveal neovascular age-related macular degeneration. Int Ophthalmol. 2009;29(5):349–357. doi:10.1007/s10792-008-9243-1
19. Cohen SY, Mimoun G, Oubraham H, et al. Changes in visual acuity in patients with wet age-related macular degeneration treated with intravitreal ranibizumab in daily clinical practice: the LUMIERE study. Retina. 2013;33(3):474–481. doi:10.1097/IAE.0b013e31827b6324
20. Menon G, Chandran M, Sivaprasad S, Chavan R, Narendran N, Yang Y. Is it necessary to use three mandatory loading doses when commencing therapy for neovascular age-related macular degeneration using bevacizumab? (BeMOc Trial). Eye (Lond). 2013;27(8):959–963. doi:10.1038/eye.2013.93
21. Holz FG, Mitchell P, Macfadden W, Parikh S Treatment patterns in prior ranibizumab-treated patients with neovascular age-related macular degeneration: real-world outcomes from the LUMINOUSTM study. 18th EURETINA Congress; Published online 2018.
22. Rosenfeld PJ, Brown DM, Heier JS, et al. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1419–1431. doi:10.1056/NEJMoa054481
23. Brown DM, Kaiser PK, Michels M, et al. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1432–1444. doi:10.1056/NEJMoa062655
24. Chen S-N, Cheng C-K, Yeung L, et al. One-year real-world outcomes of ranibizumab 0.5 mg treatment in Taiwanese patients with polypoidal choroidal vasculopathy: a subgroup analysis of the REAL study. Int J Ophthalmol. 2018;11(11):1802–1808. doi:10.18240/ijo.2018.11.11
25. Holz FG, Tadayoni R, Beatty S, et al. Multi-country real-life experience of anti-vascular endothelial growth factor therapy for wet age-related macular degeneration. Br J Ophthalmol. 2015;99(2):220–226. doi:10.1136/bjophthalmol-2014-305327
26. Eldem B, Lai TYY, Ngah NF, et al. An analysis of ranibizumab treatment and visual outcomes in real-world settings: the UNCOVER study. Graefes Arch Clin Exp Ophthalmol. 2018;256(5):963–973. doi:10.1007/s00417-017-3890-8
27. Providência J, Rodrigues TM, Oliveira M, et al. Real-world results of aflibercept versus ranibizumab for the treatment of exudative AMD using a fixed regimen. Biomed Res Int. 2018;2018:1–7. doi:10.1155/2018/9276580
28. Lim JH, Wickremasinghe SS, Xie J, et al. Delay to treatment and visual outcomes in patients treated with anti-vascular endothelial growth factor for age-related macular degeneration. Am J Ophthalmol. 2012;153(4):678–686.e2. doi:10.1016/j.ajo.2011.09.013
29. Lanzetta P, Cruess AF, Cohen SY, et al. Predictors of visual outcomes in patients with neovascular age-related macular degeneration treated with anti-vascular endothelial growth factor therapy: post hoc analysis of the VIEW studies. Acta Ophthalmol. 2018;96(8):e911–e918. doi:10.1111/aos.13751
30. Regillo CD, Busbee BG, Ho AC, Ding B, Haskova Z. Baseline predictors of 12-month treatment response to ranibizumab in patients with wet age-related macular degeneration. Am J Ophthalmol. 2015;160(5):1014–1023.e2. doi:10.1016/j.ajo.2015.07.034
31. Ying G, Huang J, Maguire MG, et al. Baseline predictors for one-year visual outcomes with ranibizumab or bevacizumab for neovascular age-related macular degeneration. Ophthalmology. 2013;120(1):122–129. doi:10.1016/j.ophtha.2012.07.042
32. Zhang X, Lai TYY. Baseline predictors of visual acuity outcome in patients with wet age-related macular degeneration. Biomed Res Int. 2018. doi:10.1155/2018/9640131
33. Kaiser PK, Brown DM, Zhang K, et al. Ranibizumab for predominantly classic neovascular age-related macular degeneration: subgroup analysis of first-year ANCHOR results. Am J Ophthalmol. 2007;144(6):850–857. doi:10.1016/j.ajo.2007.08.012
34. Boyer DS, Antoszyk AN, Awh CC, et al. Subgroup analysis of the MARINA study of ranibizumab in neovascular age-related macular degeneration. Ophthalmology. 2007;114(2):246–252. doi:10.1016/j.ophtha.2006.10.045
35. Pedrosa AC, Reis-Silva A, Pinheiro-Costa J, et al. Treatment of neovascular age-related macular degeneration with anti-VEGF agents: retrospective analysis of 5-year outcomes. Clin Ophthalmol. 2016;10:541–546. doi:10.2147/OPTH.S90913
36. Wang F, Yuan Y, Wang L, et al. One-year outcomes of 1 dose versus 3 loading doses followed by pro re nata regimen using ranibizumab for neovascular age-related macular degeneration: the ARTIS Trial. J Ophthalmol. 2019;2019:1–6. doi:10.1155/2019/7530458
37. Koh A, Lai TYY, Wei WB, et al. Real-world effectiveness and safety of ranibizumab treatment in patients with and without polypoidal choroidal vasculopathy: twelve-Month Results From the LUMINOUS Study. Retina. 2019. doi:10.1097/IAE.0000000000002624
38. Woo SJ, Ahn J, Morrison MA, et al. Analysis of genetic and environmental risk factors and their interactions in Korean patients with age-related macular degeneration. PLoS One. 2015;10(7):e0132771. doi:10.1371/journal.pone.0132771
39. Laude A, Cackett PD, Vithana EN, et al. Polypoidal choroidal vasculopathy and neovascular age-related macular degeneration: same or different disease? Prog Retin Eye Res. 2010;29(1):19–29. doi:10.1016/j.preteyeres.2009.10.001
40. Sakurada Y, Yoneyama S, Imasawa M, Iijima H. Systemic risk factors associated with polypoidal choroidal vasculopathy and neovascular age-related macular degeneration. Retina. 2013;33(4):841–845. doi:10.1097/IAE.0b013e31826ffe9d
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.