Back to Journals » Clinical Ophthalmology » Volume 20
Ray-Tracing-Guided Femtosecond LASIK: Refractive Outcomes, Visual Quality and Patient Satisfaction
Authors Yang L, Luo L ![]() , Zhang Y, Fan Y
, Zhang Y, Fan Y ![]() , Wang X, Hu Q, Cai Y
, Wang X, Hu Q, Cai Y ![]() , Tan S, Yu J, Liu Z
, Tan S, Yu J, Liu Z ![]() , Mi S
, Mi S
Received 14 October 2025
Accepted for publication 1 January 2026
Published 8 January 2026 Volume 2026:20 574112
DOI https://doi.org/10.2147/OPTH.S574112
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Scott Fraser
Linjuan Yang,1,* Lei Luo,1,* Yu Zhang,1 Yimeng Fan,1 Xindi Wang,1 Qianrong Hu,1 Yan Cai,1 Shimin Tan,2 Jingni Yu,3 Zhao Liu,1 Shengjian Mi1
1Department of Ophthalmology, the First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, Shaanxi, People’s Republic of China; 2Department of Ophthalmology, Xi’an No.9 Hospital, Xi’an, Shaanxi, People’s Republic of China; 3Department of Ophthalmology, Xi’an People’s Hospital, Xi’an, Shaanxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhao Liu, Department of Ophthalmology, the First Affiliated Hospital of Xi’an Jiaotong University, 277 West Yanta Road, Xi’an, Shaanxi, 710061, People’s Republic of China, Tel +86 029 85324452, Email [email protected]
Purpose: To assess the refractive outcomes, visual quality, and patient satisfaction after ray-tracing-guided femtosecond laser-assisted in situ keratomileusis (FS-LASIK) for the correction of moderate-to-high myopia and myopic astigmatism.
Methods: In this consecutive case series retrospective study, 51 patients (101 eyes) with moderate-to-high myopia and myopic astigmatism underwent ray-tracing-guided FS-LASIK. Visual acuity, manifest refraction, objective and subjective visual quality, patient satisfaction were assessed over 3 months. For objective visual quality, InnovEyes Sightmap was used to measure the higher-order aberrations (HOAs) over 5-mm optical zone, and Optical Quality Analysis System II was used to evaluate the modulation transfer function cut off (MTFcut off) frequency, Strehl ratio (SR), and ocular scattering index (OSI). Subjective visual quality was evaluated utilizing the National Eye Institute Refractive Error Quality of Life (NEI-RQL) questionnaire.
Results: Regarding visual and refractive outcomes, at 3 months, uncorrected distance visual acuity reached ≥ 20/20 in all eyes, ≥ 20/16 in 69% of eyes, and ≥ 20/12.5 in 18% of eyes. Best-corrected distance visual acuity was better in 61% of eyes. All eyes achieved manifest refractive spherical equivalent within ± 1.00 D and 86% of eyes achieved cylinder within ± 0.25 D. As for objective visual quality, total HOA increased significantly (P < 0.001), whereas spherical aberration showed no significant change (P = 0.225); no changes were found in MTFcut off, SR, and OSI (all P > 0.05). In terms of subjective visual quality, 100% of patients reported clear distance vision, and 96.10% had no near-reading difficulty. Investigation of patient satisfaction showed that 98.04% of patients were satisfied with the surgery, 98.04% would recommend it to others.
Conclusion: Ray-tracing-guided FS-LASIK may be an effective, safe and predictable procedure for moderate-to-high myopia and myopic astigmatism. It yielded favorable refractive outcomes, maintained objective visual quality, and achieved high patient satisfaction.
Keywords: ray tracing, FS-LASIK, refraction, visual quality, patient satisfaction
Introduction
Laser corneal refractive surgery, such as femtosecond laser-assisted in situ keratomileusis (FS-LASIK), aims to provide patients with optimal visual acuity and visual quality.1 Conventional FS-LASIK can often achieve excellent visual acuity. However, it induces an increase of higher-order aberrations (HOAs), which can lead to visual disturbances such as blurred vision, halos, and glare under low-light conditions and degrade overall visual quality.2 Although wavefront-guided FS-LASIK has been shown to induce fewer aberrations than standard procedure, it still leads to an increase in HOAs, particularly when correcting higher myopia.3 Numerous studies4,5 have identified that preoperative refractive error is strongly correlated with both corneal asphericity and surgically induced spherical aberration, since the intraocular multi-lens structure is not considered in conventional FS-LASIK.6
To enhance the customization of eye models, Mrochen et al7 proposed the ray tracing algorithm, considering all important optical elements of each eye. It incorporates the biometric, tomographic, and wavefront aberration data captured by multiple instruments. Recently, a diagnostic device named InnovEyes Sightmap (Alcon, Fort Worth, TX, USA) has integrated these ocular measurement instruments into a single device. A highly individualized eye model is generated using the collected data. Following several iterations of ray tracing algorithm, a unique and optimal corneal surface was derived. The difference between the current and the ideal corneal anterior surface topography is then calculated, forming an optimal ablation profile. Factors such as corneal epithelial remodeling and biomechanical changes caused by surgery are also taken into account to refine the ablation profile.7 Unlike traditional procedure based on manifest refraction, this profile is based on wavefront refraction evaluated by InnovEyes Sightmap (Alcon, Fort Worth, TX, USA), eliminating the need for nomogram adjustments.7 Previous studies8–13 have demonstrated the favorable visual and refractive outcomes of ray-tracing-guided FS-LASIK in correcting myopia with or without astigmatism, while the evaluation of postoperative visual quality has predominantly focused on HOAs and visual symptoms.14,15 Broader assessments of optical quality and patient-reported satisfaction remain limited, despite their clinical relevance.11,16 To address this gap, the present study was designed to incorporate objective visual quality and patient-reported outcomes, which are essential for fully understanding the real-world effectiveness and patient experience following refractive surgery.
This study aims to assess the refractive outcomes, visual quality and patient satisfaction after ray-tracing-guided FS-LASIK for moderate-to-high myopia and myopic astigmatism. We evaluated visual acuity, refraction, ocular HOAs, subjective and objective visual quality, as well as patient satisfaction at 3 months. This study is the first to incorporate both objective visual quality analyzed by Optical Quality Analysis System (OQAS) (OQAS II, Visiometrics S.L, Spain) and subjective visual quality assessed utilizing the National Eye Institute Refractive Error Quality of Life (NEI-RQL) questionnaire. We believed that integrating objective and subjective visual quality, as well as patient satisfaction will offer more clinical evidence to assess its potential advantages.
Patients and Methods
Study Design and Participants
This consecutive case series retrospective study included 51 patients (101 eyes) who received ray-tracing-guided FS-LASIK from October 2023 to October 2024 in the Ophthalmology Refractive Surgery Center of the First Affiliated Hospital of Xi’ an Jiaotong University. The study was approved by the ethics committee of the First Affiliated Hospital of Xi’an Jiaotong University (2020-W28) and adhered to the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants prior to the treatment.
Inclusion criteria included: (1) patients aged 18 to 39 years; (2) eyes with a stable refractive error with a change ≤ 0.50 D in the past year; (3) preoperative best-corrected distance visual acuity (CDVA) ≥ 1.0; (4) myopia ≥ −11.00 D and astigmatism ≥ −4.50 D; (5) soft contact lenses discontinued for >1 week, rigid gas-permeable contact lenses discontinued for >4 weeks, and orthokeratology lenses discontinued for >3 month; (6) the wavefront spherical equivalent at 4 mm and the manifest spherical equivalent were aligned within 0.50 D, and the cylinders were aligned within 0.75 D.
Exclusion criteria included: (1) pregnancy or breastfeeding; (2) severe diabetes, systemic connective tissue diseases, or autoimmune disorders; (3) abnormal ophthalmic conditions such as active eye disease, clinically significant dry eye, ectasia, keratoconus or suspected keratoconus, glaucoma or suspected glaucoma, cataract, severe retinal disease; (4) history of intraocular or corneal surgery; (5) follow-up time less than 3 months; (6) estimated postoperative thickness of residual stromal bed less than 280 µm.
Preoperative Examinations
Preoperative evaluations routinely included UDVA, CDVA, manifest cycloplegic and non-cycloplegic refraction, intraocular pressure measurements, slit-lamp microscopy and dilated fundus examinations.
Measurements including biometry, wavefront refraction, whole-eye aberrometry, and tomography were captured using the InnovEyes Sightmap (Alcon, Fort Worth, TX, USA), which were performed in a dark room with pupil diameter ≥6 mm (without pharmacological dilation). Near work was avoided for ≥10 minutes pre-examination. During capturing, patients were required to fixate on the inner target with full corneal exposure; examination time was minimized to reduce near-induced accommodative response. Four reproducible images were selected through a two-step process: automated quality-threshold flagging by the device, followed by manual exclusion to improve consistency.
Visual quality was quantitatively analyzed using the parameters from Optical Quality Analysis System II (OQAS II, Visiometrics S.L., Spain), including the modulation transfer function cut off (MTFcut off) frequency, Strehl ratio (SR), and objective ocular scattering index (OSI).
Examinations of manifest refraction, InnovEyes Sightmap (Alcon, Fort Worth, TX, USA) and OQAS (OQAS II, Visiometrics S.L, Spain) were performed by designated examiners (LY, YZ, ST), respectively.
Surgical Design
The target postoperative refraction for both eyes was 0 D. The treatment was performed as InnovEyes software suggested refraction without any nomogram adjustments. The wavefront spherical equivalent at 4 mm measured by InnovEyes Sightmap (Alcon, Fort Worth, TX, USA) and manifest spherical equivalent were required to be aligned within 0.50 D, with the cylinder differences within 0.75 D.
Surgical Procedure
The surgery was performed by a single surgeon (SM) under topical anesthesia. Each corneal flap was created using the WaveLight® FS200 femtosecond laser (Alcon Management S. A., Fort Worth, United States), with a major axis diameter ranging from 8.5 to 9.0 mm and a thickness of 100–110 μm. The orientation of the flap’s hinge was perpendicular to the astigmatism axis. The side-cut angle was 105°. Following blunt dissection and flap lift, the corneal stromal bed was ablated with the WaveLight® EX500 excimer laser (Alcon Management S. A., Fort Worth, United States) using an optical zone of 6.0–6.5 mm. Prior to laser treatment, iris registration was performed, and the laser treatment proceeded without interruption.
Postoperative Care and Examinations
Postoperatively, 0.1% tobramycin eye drops (Novartis, Peiris, Belgium) were administered four times a day for 7 days. 0.1% fluorometholone eye drops (Santen Pharmaceutical Co., Shiga, Japan) were applied four times a day, reduced once every 10 days. Polyvinyl alcohol eye drops (Hubei Yuanda Tian Tianming Pharmaceutical, Wuhan, China) were used four times a day as needed for 1 to 3 months.
Examinations included UDVA, CDVA, manifest refraction were performed at 1-week, 1-month, and 3-month postoperative follow-ups. At 3 months postoperatively, InnovEyes Sightmap (Alcon, Fort Worth, TX, USA) was used to evaluate HOAs at a 5-mm optical zone, the OQAS (OQAS II, Visiometrics S.L, Spain) was used to assess the objective visual quality, and the NEI-RQL questionnaire was employed to assess subjective visual quality.
Statistical Analysis
The sample size was calculated using PASS 2025 Software (NCSS, LLC, Kaysville, Utah, USA). Previous study17 reported that OSI increased by approximately 0.47 after traditional FS-LASIK for moderate-to-high myopia. We hypothesized that ray-tracing-guided FS-LASIK would achieve better results, with OSI increasing less than 0.20. The expected increase was 0.05 (representing no significant OSI change after surgery),18 with an estimated standard deviation of 0.4. A sample size of 63 eyes was needed to achieve a power of 0.9 and one-side type I error of 0.05.
Statistical analysis was conducted by SPSS 22.0 for Windows (IBM, Armonk, NY, USA). The normality of continuous variables was assessed using the Kolmogorov–Smirnov test. The paired t-test was used to compare normally distributed variables and Wilcoxon signed rank test was used to compare the non-normally distributed. A two-side P-value of less than 0.05 was considered statistically significant.
Results
Characteristics of the Patients
A total of 51 patients (101 eyes) were included in this study, with 20 males (39.2% of patients) and 31 females (60.8% of patients). The mean age was 27.1 ± 5.8 years (range: 18 to 39 years). For the enrolled eyes, the preoperative manifest equivalent refraction was −6.63 ± 1.51 D, with 39 (38.6%) moderate myopia eyes and 62 (61.4%) high myopia eyes. Preoperative parameters are presented in Table 1.
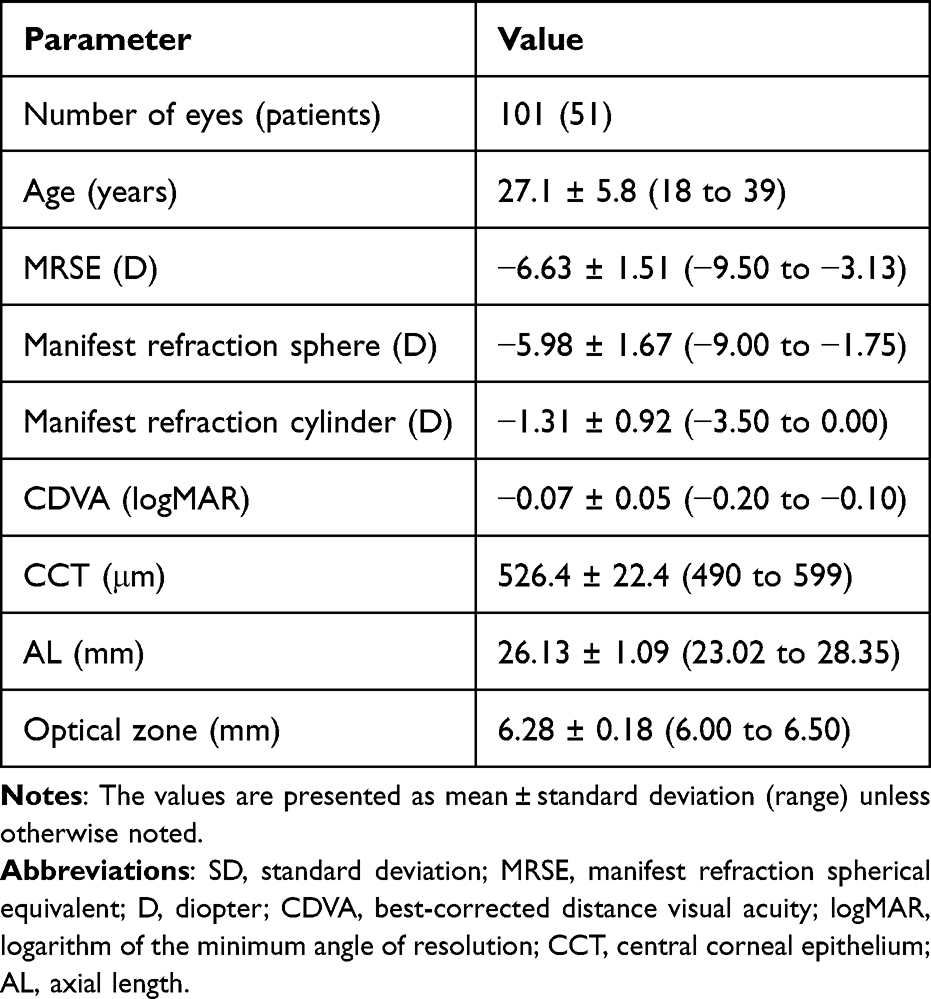 |
Table 1 Preoperative Parameters of the Patients |
Postoperative Visual and Refractive Outcomes
At the 3-month follow-up, all eyes achieved UDVA of 20/20 or better, with 70 eyes (69%) achieving UDVA of 20/16, and 18 eyes (18%) achieving UDVA of 20/12.5 (Figure 1A). When comparing postoperative UDVA to preoperative CDVA, 54 eyes (53%) had the same UDVA as their preoperative CDVA, 32 eyes (32%) showed improvement by 1–2 Snellen lines, and 15 eyes (15%) showed a decrease of 1 Snellen line (Figure 1B). For CDVA, none of eyes lost lines, 53 eyes (52%) improved by 1 Snellen line, and 9 eyes (9%) improved by 2 or more lines (Figure 1C). A very strong correlation was observed between attempted and achieved spherical equivalent refraction (R2 = 0.974) (Figure 1D). A total of 101 eyes (100%) achieved an MRSE within ± 1.00D (Figure 1E). At 1-week, 1-month, and 3-month follow-ups, the MRSE were 0.14 ± 0.21 D, 0.12 ± 0.21 D, and 0.14 ± 0.25 D, respectively. No eye changed more than 0.50 D over the 3 months (Figure 1F).
 |
Figure 1 Visual and refractive outcomes at 3 months after ray-tracing-guided FS-LASIK. Abbreviations: UDVA, uncorrected distance visual acuity; CDVA, best-corrected distance visual acuity; VA, visual acuity; SEQ, spherical equivalent refraction; D, diopter; TIA, target induced astigmatism; SIA, surgically induced astigmatism; Arith, arithmetic; Abs, absolute. Notes: (A) Cumulative postoperative UDVA compared with preoperative CDVA. (B) Line difference between postoperative UDVA and preoperative CDVA. (C) Change in lines between preoperative and postoperative CDVA. (D) Attempted versus achieved spherical equivalent refraction. Above the blue line: overcorrection; below the blue line: undercorrection. (E) Spherical equivalent refraction accuracy. (F) Spherical equivalent refraction stability. (G) Comparison of preoperative and postoperative refractive astigmatism. (H) Target-induced astigmatism versus surgically induced astigmatism. Above the blue line: overcorrection; below the blue line: undercorrection. (I) Refractive astigmatism angle of error. Positive value: counterclockwise; negative value: clockwise. |
Additionally, 87 eyes (86%) achieved postoperative refractive astigmatism within 0.25 D (Figure 1G). And we found that surgically induced astigmatism (SIA) vector was highly correlated with target induced astigmatism (TIA) vector (R2 = 0.947, Figure 1H). Eighty-seven eyes (86%) had a postoperative astigmatism axis difference within 5° compared to preoperative axis (Figure 1I).
All surgeries were successfully performed, with no surgery-related complications, such as diffuse lamellar keratitis, corneal haze, or intraoperative epithelial implantation.
Objective Visual Quality
As shown in Table 2, total HOA increased significantly from 0.21 ± 0.08 μm to 0.31 ± 0.11 μm across 5-mm optical zone postoperatively (P < 0.001). Spherical aberration decreased in the moderate myopia group (0.03 ± 0.06 μm vs 0.00 ± 0.09 μm, P = 0.02) while remained in the high myopia group (0.03 ± 0.07 μm vs 0.03 ± 0.09 μm, P = 0.908). The absolute value of spherical aberration showed no significant changes in both groups (+0.02 ± 0.06 μm, P = 0.117; +0.01 ± 0.07 μm, P = 0.117). Vertical coma showed a negative shift in both groups (0.08 ± 0.12 μm vs −0.09 ± 0.13 μm, P < 0.001; 0.03 ± 0.12 μm vs −0.16 ± 0.16 μm, P < 0.001), while horizontal coma remained unchanged (−0.01 ± 0.06 μm vs −0.02 ± 0.08 μm, P = 0.58; 0.00 ± 0.07 μm vs 0.00 ± 0.20 μm, P = 0.996). Both the absolute of vertical and horizontal coma unchanged in moderate myopia group (+0.01 ± 0.12 μm, P = 0.652; +0.01 ± 0.06 μm, P = 0.498) and increased in high myopia group (+0.09 ± 0.15 μm, P < 0.001; +0.10 ± 0.13 μm, P < 0.001).
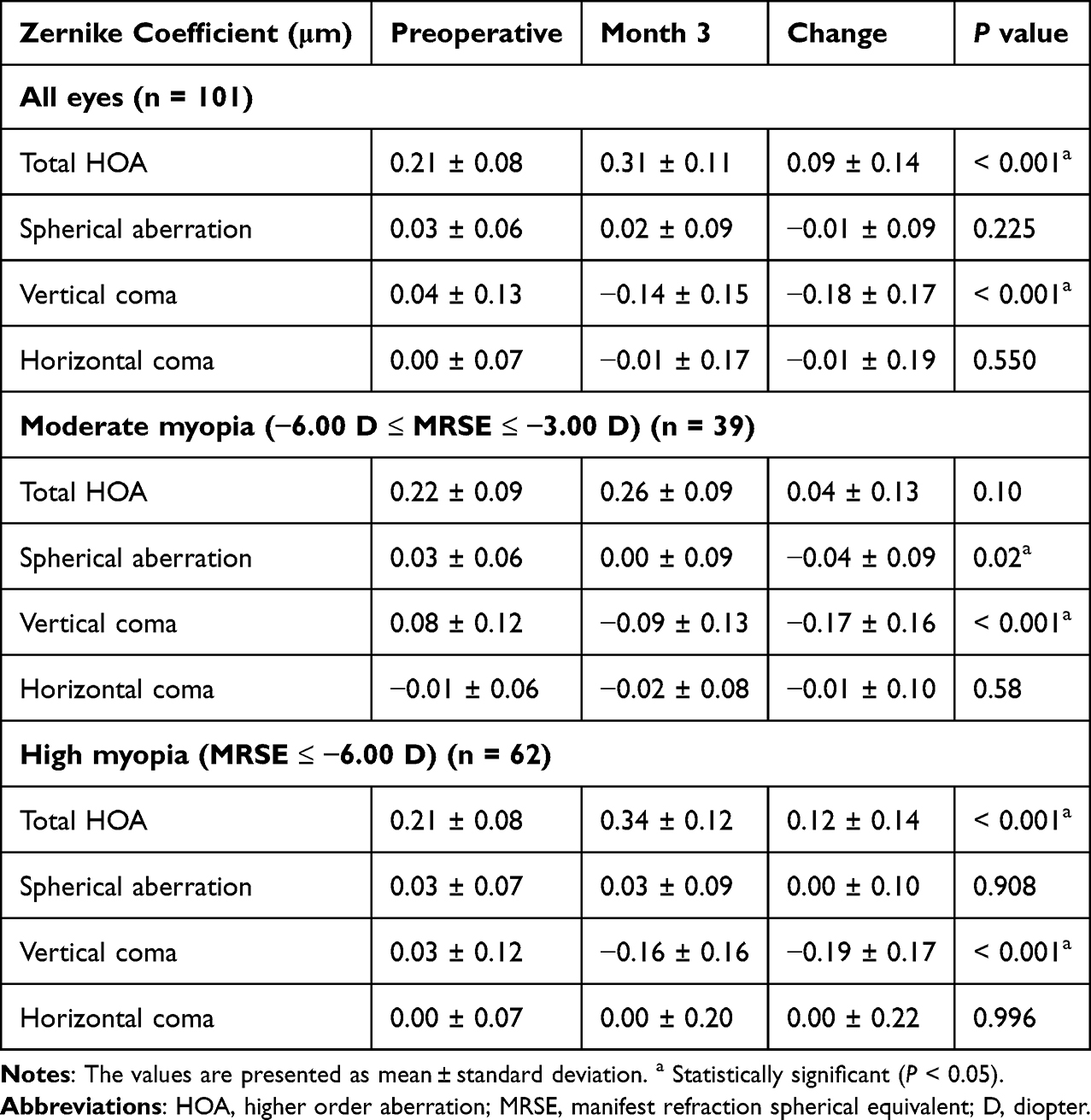 |
Table 2 Preoperative and 3-Month Postoperative Ocular Higher Order Aberrations (μm) at 5mm Optical Zone |
The OSI, MTFcut off and SR had no change at 3 months after surgery (all P > 0.05). And there were also no significant differences in simulated photopic vision, twilight vision, or night vision before and after surgery (P > 0.05), as shown in Table 3.
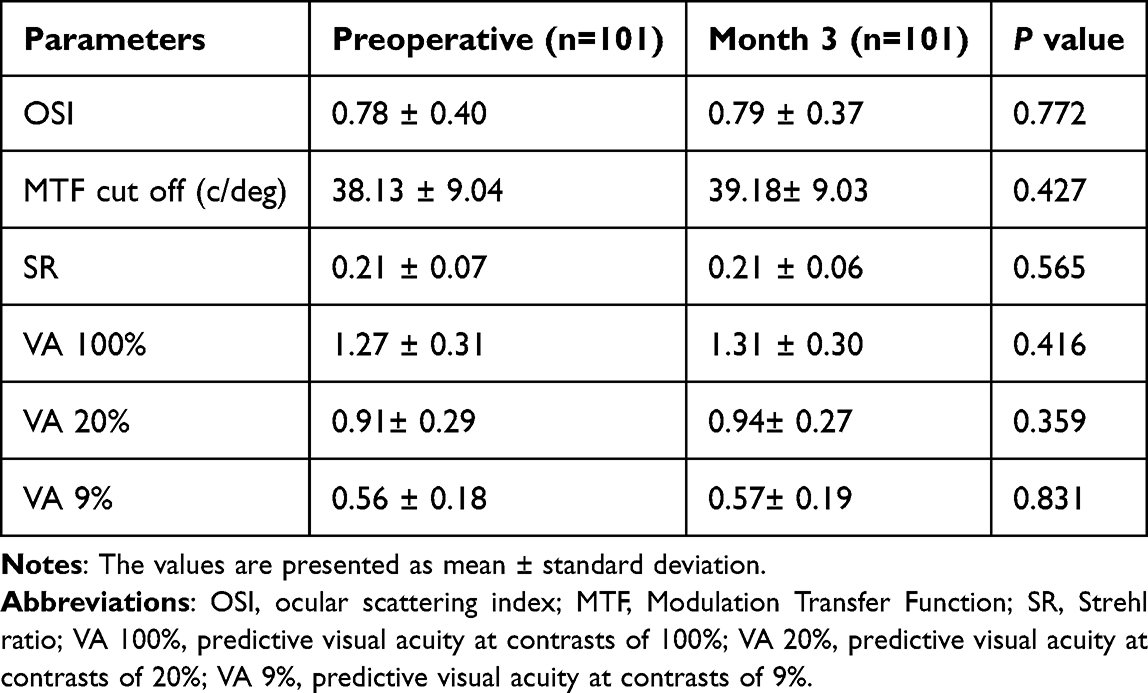 |
Table 3 Preoperative and Postoperative Objective Visual Quality Parameters |
Subjective Visual Quality
Ninety-eight percentages of patients expressed satisfaction with the surgical outcomes (Figure 2A), and 98.04% of patients would recommend the surgery to family and friends (Figure 2B). Details regarding patients’ distance and near visual acuity, night vision, comfort, presence of dry eyes, glare, halo, and other subjective visual quality concerns are provided in Supplementary Table 1. It demonstrated that 100% of patients achieved clear distance vision, 96.10% of patients had no reading difficulties, and 98% of patients no longer required spectacles for night driving.
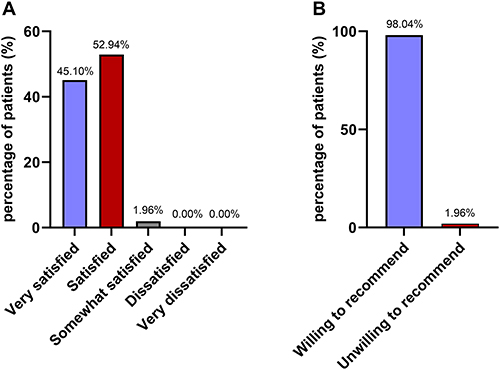 |
Figure 2 Patient satisfaction at 3 months after ray-tracing-guided FS-LASIK. Notes: (A) Patient satisfaction rate. (B) Patients’ willingness to recommend the surgery. |
Discussion
Ray tracing-guided FS-LASIK uses a single diagnostic device, InnovEyes Sightmap (Alcon, Fort Worth, TX, USA), to measure comprehensive ocular data, automatically creating a virtual eye model for ablation design. The optimization process is iterative, continuing until the desired result is achieved.7 By comprehensively considering the structural characteristics of the eye’s multiple refractive media, the aberrations of the entire ocular system can theoretically be eliminated, solving the significant increase in spherical aberration after refractive treatment in previous wavefront-guided surgeries.7 Additionally, the expected corneal biomechanical response to laser ablation is considered, including the effects of corneal wound healing.9,19
Several studies have demonstrated the safety and efficacy of ray-tracing-guided FS-LASIK for correcting myopia and astigmatism. Previous studies8,20–22 demonstrated that, after conventional FS-LASIK, UDVA of ≥20/20 was achieved in 83% to 97% of eyes, which seemed inferior or similar to our results (100%). In terms to the studies for ray-tracing-guided FS-LASIK, Kanellopoulos et al16 reported that 98.1% of eyes achieving UDVA ≥ 20/20 at 3 months postoperatively. Cummings et al23 found that 87% of eyes of 42 eyes achieved UDVA ≥ 20/20, 73% of eyes achieved UDVA ≥ 20/16, and 30% of eyes achieved UDVA ≥ 20/12.5 at 6 months. In our study, 100% of eyes had UDVA ≥ 20/20, 69% of eyes achieved UDVA ≥ 20/16, and 18% of eyes achieved UDVA ≥ 20/12.5, which aligns closely with prior results. He et al9 found that 100% of eyes had UDVA ≥ 20/20 at 3 months, with 89% of eyes achieving UDVA ≥ 20/16 and 51% of eyes achieving UDVA ≥ 20/12.5. Cao et al10 reported 84% of eyes achieved UDVA ≥ 20/16 at 3 months. These two studies were slightly better than ours, likely due to the lower preoperative MRSE in their studies (−3.39 ± 1.58 D, −5.06 ± 2.10 D).
In our study, UDVA improved by 1 or 2 Snellen lines over preoperative CDVA in 32% of eyes. Meanwhile, CDVA improved by 1 or 2 lines in 61% of eyes, surpassing the results of Yuan et al8 (24%) for Q-value–adjusted LASIK and Stulting et al24 (46%) for topography-guided LASIK. Kanellopoulos et al16 reported 26% of eyes had UDVA improved by 1 Snellen line compared to preoperative CDVA after ray-tracing-guided FS-LASIK, with 36% of eyes improving CDVA by 1 or 2 lines. He et al9 reported that 39% of eyes had UDVA improved by 1 Snellen line and 48% of eyes had CDVA improved by 1or 2 lines. These results demonstrate the favorable safety and efficacy of ray-tracing-guided FS-LASIK compared to Q-value-adjusted and topography-guided FS-LASIK.
In our study, MRSE within ± 0.50 D was achieved in 96% of eyes, and high correlation between achieved and attempted MRSE (R2 = 0.9742) was observed, Kanellopoulos16 and He9 had similar results (95%, R2 = 0.9720; 96%. R2 = 0.9757). In several studies concerned with conventional FS-LASIK,8,20–22 MRSE within ± 0.50 D was achieved in 90% to 98% of eyes. These findings suggest that ray-tracing-guided FS-LASIK offers high predictability postoperative refractive outcomes, underscoring the advantages of iterative optimization. However, our study showed a slight overcorrection, with a postoperative 3-month MRSE of +0.14 ± 0.25 D. Similar findings were reported by Yuan et al8 and He et al.9 We speculate this may be due to the built-in InnovEyes nomogram, epithelial remodeling compensation, or imprecise fogging during wavefront aberration data collection. In the later stage, adjustments to the built-in nomogram may be required, and more effective fog vision functions should be implemented during preoperative examinations to relax the eye’s accommodation.8 Larger multicenter studies with longer follow-ups are needed to confirm our speculations.
Astigmatic correction is more challenging in refractive surgery. In our study, 86% of eyes had residual astigmatism < 0.25 D, with 86% of eyes showing less than 5° difference between postoperative astigmatic axis and preoperative subjective refraction axis. After conventional FS-LASIK, the rates of residual astigmatism within 0.25 D were reported to range from 58% to 85%,8,20–22 seemingly inferior to or similar to ours. The results of Yuan,8 He,9 and Cao10 for ray-tracing-guided FS-LASIK were consistent with ours, indicating that the iterative nature of ray-tracing optimization ensures relative high precision in astigmatic correction compared to traditional planning methods.
Visual quality after laser corneal refractive surgery is commonly correlated with HOAs. It is now understood that correcting lower order aberrations may simultaneously introduce higher-order aberrations, thus affecting visual quality.9 Previous studies have shown that for patients with a refractive error > −5.00 D, conventional laser corneal refractive surgery increases HOA and spherical aberration by 2–17 times.9,25–27 In our study, 73.3% of eyes had a refractive error > −5.00 D, and the results showed spherical aberration reduced in moderate myopia eyes but had no change in high myopia eyes. He et al9 found that despite 20% of eyes having spherical correction > −5.00 D, the ray-tracing-guided FS-LASIK still resulted in lower ocular total aberration. Yuan’s study,8 with 67.7% of eyes having a refractive error greater than −5.00D, reported similar findings of ray-tracing-guided FS-LASIK, showing significantly lower postoperative spherical aberration compared to Q-value-adjusted group. These results may be attributed to the ray tracing algorithm, which creates highly customized ablation profiles.28 Cao et al10 also found a slight increase in total HOA after surgery, while the spherical aberration decreased significantly. Our study showed slight increases in total HOA (+0.09 ± 0.14). Previous literature27 indicates that conventional FS-LASIK surgery significantly increases total HOA from 0.38 preoperatively to 0.6 postoperatively, with an average increase of 0.22. Thananjeyan28 and other studies11,12 demonstrated that ray-tracing-guided FS-LASIK results an increase of less than 0.1 µm in total HOA, consistent with our findings that show a minor increase in total HOA, which was still lower than conventional FS-LASIK. Aberration measurements can be influenced by various factors (pupil diameter, different equipment), and changes smaller than 0.1 µm are not clinically significant.2,29 He9 and Kanellopoulos11 also highlighted that a key advantage of ray-tracing-guided FS-LASIK is reducing surgical induced HOAs, thus preserving visual quality.
Objective visual quality analysis systems, such as the OQAS (OQAS II, Visiometrics S.L, Spain), can quantify the combined effects of scattering, aberration, and diffraction with high repeatability and reproducibility, thereby avoiding the overestimation of visual function that may arise from neglecting scattering and diffraction in previous wavefront aberration instruments.30 OSI reflects the degree of scatter which reduces retinal image quality. Prior study demonstrated that OSI increased after conventional LASIK, leading to a decline in optical quality.17 However, in this study, the OSI remained its value postoperatively, indicating that the retinal imaging quality after ray-tracing-guided FS-LASIK surgery was good, resulting in excellent visual quality for the patients. There were no differences in simulated photopic vision, twilight vision, or night vision compared to preoperative values, suggesting that the patients maintained good visual quality in various lighting conditions postoperatively.
The goal of refractive surgery is not only to improve vision but also to enhance visual function, quality, and patient satisfaction.31 NEI-RQL questionnaire and satisfaction surveys indicated that 98.04% of patients were satisfied with ray-tracing-guided FS-LASIK myopia correction, 98.04% of patients would recommend the surgery to others, 100% of patients had clear distance vision, 96.10% of patients had no reading difficulties, and 98% of patients no longer required spectacles for night driving. Kanellopoulos et al16 found that 94.7% of patients were satisfied with the surgery’s visual quality at 2 years post-surgery, and 94.7% of patients were satisfied with their distance vision, 84.2% with near vision, and 94.7% with night vision. The difference between Kanellopoulos’ results and ours is that their patient satisfaction rate for near vision was slightly lower, which is likely related to the older participants of Kanellopoulos’ study (21 to 49 years vs 18 to 65 years). In another international multicenter study for ray-tracing-guided LASIK,11 Kanellopoulos et al investigated patient satisfaction and found that 96.3% of patients were completely or very satisfied with the surgery, which was similar to our results. These high satisfaction rates are multifactorial, reflecting not only the achievement of satisfactory subjective visual quality, but also the favorable visual outcomes and objective visual quality. Overall, ray-tracing-guided FS-LASIK achieved favorable post-operative distance, near, and night vision, leading to high patient satisfaction.
This study has several limitations. Firstly, the follow-up period is relatively short and the sample size is relatively small. Secondly, the study is a case series retrospective study and lacks data of preoperative subjective satisfaction. A prospective head-to-head study with an expanded sample and extended timeframe will be further performed to achieve more comprehensive and conclusive results.
Conclusion
Our study confirms that ray-tracing-guided FS-LASIK for moderate-to-high myopia and myopic astigmatism is effective, safe and predictable within 3 months postoperatively. All eyes achieved UDVA ≥ 20/20, 87% of eyes achieved UDVA ≥ 20/16. A mild MRSE overcorrection (+0.14 ± 0.25 D) suggests that adjustments to the built-in nomogram of InnovEyes Sightmap (Alcon, Fort Worth, TX, USA) or the implementation of a more effective fogging function to relax the eye’s accommodation might be necessary. Postoperative total HOA exhibited a statistically significant but clinically nonsignificant increase, while spherical aberration remained unchanged. Meanwhile, it maintained objective visual quality, and achieved high patient satisfaction.
Abbreviations
FS-LASIK, femtosecond laser-assisted in situ keratomileusis; UDVA, uncorrected distance visual acuity; CDVA, best-corrected distance visual acuity; MRSE, manifest refraction spherical equivalent; HOA, higher-order aberration; OQAS, Optical Quality Analysis System; MTFcut off, modulation transfer function cut off; SR, Strehl ratio; OSI, ocular scattering index; NEI-RQL, National Eye Institute Refractive Error Quality of Life; VA, visual acuity.
Data Sharing Statement
The data sets used and/or analyzed during the current study available from the corresponding author on reasonable request.
Acknowledgments
Linjuan Yang and Lei Luo are co-first authors for this study. We sincerely thank the patients who participated in the study for their contribution.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Supported by the Key Research and Development Program of Shaanxi, China (Grant No. 2023-YBSF-568), the Natural Science Basic Research Program of Shaanxi (Grant No. 2024JC-YBQN-0962, 2023-JC-YB-685), the Integration Innovation Program of Xi’an Jiaotong University Health Science Center (Grant No. YXJLRH2022037).
Disclosure
The authors have no conflicts of interest concerning this study.
References
1. Wen D, McAlinden C, Flitcroft I, et al. Postoperative efficacy, predictability, safety, and visual quality of laser corneal refractive surgery: a network meta-analysis. Am J Ophthalmol. 2017;178:65–11. doi:10.1016/j.ajo.2017.03.013
2. Feng Z, Wang Q, Du C, Yang F, Li X. High-order aberration changes after femtosecond LASIK surgery in patients with high myopia. Ann Palliat Med. 2021;10(7):7689–7696. doi:10.21037/apm-21-1677
3. Zhang Y, Du Y, He M, Zhang Y, Du Z. Comparison of visual quality after wavefront-guided LASIK in patients with different levels of preoperative total ocular higher-order aberrations: a retrospective study. PeerJ. 2024;12:e17940.
4. Bottos KM, Leite MT, Aventura-Isidro M, et al. Corneal asphericity and spherical aberration after refractive surgery. J Cataract Refract Surg. 2011;37(6):1109–1115. doi:10.1016/j.jcrs.2010.12.058
5. George MR, Shah RA, Hood C, Krueger RR. Transitioning to optimized correction with the WaveLight ALLEGRETTO WAVE: case distribution, visual outcomes, and wavefront aberrations. J Refract Surg. 2010;26(10):S806–13. doi:10.3928/1081597X-20100921-07
6. Mastropasqua L, Nubile M, Ciancaglini M, Toto L, Ballone E. Prospective randomized comparison of wavefront-guided and conventional photorefractive keratectomy for myopia with the meditec MEL 70 laser. J Refract Surg. 2004;20(5):422–431. doi:10.3928/1081-597X-20040901-03
7. Mrochen M, Bueeler M, Donitzky C, Seiler T. Optical ray tracing for the calculation of optimized corneal ablation profiles in refractive treatment planning. J Refract Surg. 2008;24(4):S446–451. doi:10.3928/1081597X-20080401-23
8. Yuan Y, Zhang R, Wang Z, Wang Y, Zhang Y, Chen Y. Ray-tracing-guided or Q-value-adjusted FS-LASIK for correction of myopia and myopic astigmatism: a comparative contralateral eye study. J Refract Surg. 2024;40(11):e804–e813. doi:10.3928/1081597X-20240917-01
9. He G, Bala C. Ray-tracing-guided myopic LASIK: real-world clinical outcomes. J Cataract Refract Surg. 2023;49(11):1140–1146. doi:10.1097/j.jcrs.0000000000001286
10. Cao X, Zhang J, Shao J, Zhang Y, Zheng L. Optimization of ray-tracing-guided LASIK outcomes: a prospective comparative study of ZZ InnovEyes strategy versus automated strategy. Clin Ophthalmol. 2024;18:1879–1888. doi:10.2147/OPTH.S468069
11. Kanellopoulos AJ, Maus M, Bala C, et al. International multicenter, myopic and myopic astigmatism femto LASIK, customized by automated ray-tracing ablation profile calculation: a postmarket study. Clin Ophthalmol. 2024;18:525–536. doi:10.2147/OPTH.S435581
12. Kanellopoulos AJ, Maus M, Bala C, et al. Initial outcomes with customized myopic LASIK, guided by automated ray tracing optimization: a novel technique. Clin Ophthalmol. 2020;14:3955–3963. doi:10.2147/OPTH.S280560
13. Luo L, Fan Y, Wang X, et al. Ray tracing-guided LASIK for high myopia and astigmatism: initial clinical outcomes. Photodiagnosis Photodyn Ther. 2025;55:104715. doi:10.1016/j.pdpdt.2025.104715
14. Sitto MM, Moshirfar M, Crook TB, Hoopes PC. Comparison of U.S. FDA premarket approval studies between ray tracing-guided LASIK with InnovEyes Sightmap Versus topography-guided LASIK using custom ablation treatment (T-CAT). Ophthalmol Ther. 2025;14(12):2983–3005. doi:10.1007/s40123-025-01245-5
15. Huang Y, Li J, Zhang F, et al. Changes of refraction and visual quality after ray-tracing guided FS-LASIK in Chinese high myopia versus low-to-moderate myopia. Photodiagnosis Photodyn Ther. 2025;56:105216. doi:10.1016/j.pdpdt.2025.105216
16. Kanellopoulos AJ. Ray-tracing customization in myopic and myopic astigmatism LASIK treatments for low and high order aberrations treatment: 2-year visual function and psychometric value outcomes of a consecutive case series. Clin Ophthalmol. 2024;18:565–574. doi:10.2147/OPTH.S444174
17. Zou H, Wei X, Li L, et al. Comparison of objective visual quality between SMILE and FS-LASIK in moderate-to-high myopia. Front Med Lausanne. 2024;11:1408516. doi:10.3389/fmed.2024.1408516
18. Miao H, He L, Shen Y, Li M, Yu Y, Zhou X. Optical quality and intraocular scattering after femtosecond laser small incision lenticule extraction. J Refract Surg. 2014;30(5):296–302. doi:10.3928/1081597X-20140415-02
19. Schumacher S, Seiler T, Cummings A, Maus M, Mrochen M. Optical ray tracing-guided laser in situ keratomileusis for moderate to high myopic astigmatism. J Cataract Refract Surg. 2012;38(1):28–34. doi:10.1016/j.jcrs.2011.06.032
20. Zhao X, Zhang L, Ma J, et al. Comparison of wavefront-guided femtosecond LASIK and optimized SMILE for correction of moderate-to-high astigmatism. J Refract Surg. 2021;37(3):166–173. doi:10.3928/1081597X-20201230-01
21. Zhang Y, Chen Y. A randomized comparative study of topography-guided versus wavefront-optimized FS-LASIK for correcting myopia and myopic astigmatism. J Refract Surg. 2019;35(9):575–582. doi:10.3928/1081597X-20190819-01
22. Khoramnia R, Naujokaitis T, Blöck L, et al. Prospective intraindividual comparison of automated customized ray-tracing-guided versus wavefront-optimized LASIK. Ophthalmology. 2025;132(10):1169–1179. doi:10.1016/j.ophtha.2025.05.025
23. Cummings AB, Kelly GE. Optical ray tracing-guided myopic laser in situ keratomileusis: 1-year clinical outcomes. Clin Ophthalmol. 2013;7:1181–1191. doi:10.2147/OPTH.S44720
24. Stulting RD, Lobanoff M, Mann PM 2nd, Wexler S, Stonecipher K, Potvin R. Clinical and refractive outcomes after topography-guided refractive surgery planned using Phorcides surgery planning software. J Cataract Refract Surg. 2022;48(9):1010–1015. doi:10.1097/j.jcrs.0000000000000910
25. Lim DH, Chung ES, Kim MJ, Chung TY. Visual quality assessment after presbyopic laser in-situ keratomileusis. Int J Ophthalmol. 2018;11(3):462–469. doi:10.18240/ijo.2018.03.17
26. Kim J, Choi SH, Lim DH, Yang CM, Yoon GJ, Chung TY. Topography-guided versus wavefront-optimized laser in situ keratomileusis for myopia: surgical outcomes. J Cataract Refract Surg. 2019;45(7):959–965. doi:10.1016/j.jcrs.2019.01.031
27. Taskov G, Taskov T. Higher Order Aberrations (HOA) Changes after Femto-LASIK in Topography and Wavefrontguided Treatments. Folia Med. 2020;62(2):331–337. doi:10.3897/folmed.62.e39507
28. Thananjeyan AL, Bala C. Higher-order aberrations following ray trace LASIK and the impact of eye movement on coma. Clin Ophthalmol. 2024;18:3389–3398. doi:10.2147/OPTH.S497131
29. Xu Z, Hua Y, Qiu W, Li G, Wu Q. Precision and agreement of higher order aberrations measured with ray tracing and Hartmann-Shack aberrometers. BMC Ophthalmol. 2018;18(1):18. doi:10.1186/s12886-018-0683-8
30. Cabot F, Saad A, McAlinden C, Haddad NM, Grise-Dulac A, Gatinel D. Objective assessment of crystalline lens opacity level by measuring ocular light scattering with a double-pass system. Am J Ophthalmol. 2013;155(4):629–635,635.e1–2. doi:10.1016/j.ajo.2012.11.005
31. Han T, Xu Y, Han X, Shang J, Zeng L, Zhou X. Quality of life impact of refractive correction (QIRC) results three years after SMILE and FS-LASIK. Health Qual Life Outcomes. 2020;18(1):107. doi:10.1186/s12955-020-01362-8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.