Back to Journals » Medical Devices: Evidence and Research » Volume 14
Rationale for Use of an FDA-Cleared Delivery System for Administration of Inhaled Nitric Oxide in Patients Undergoing Magnetic Resonance Imaging
Authors Salas M, Potenziano JL, Acker J
Received 29 May 2020
Accepted for publication 14 December 2020
Published 7 January 2021 Volume 2021:14 Pages 1—7
DOI https://doi.org/10.2147/MDER.S265099
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mauro Salas,1 Jim L Potenziano,2 Jaron Acker3
1Clinical Specialist, Children’s National Health System, Washington, DC, USA; 2Scientific Affairs, Mallinckrodt Pharmaceuticals, Bedminster, NJ, USA; 3Medical Device Marketing, Mallinckrodt Pharmaceuticals, Bedminster, NJ, USA
Correspondence: Mauro Salas
Children’s National Health System, 111 Michigan Ave NW, Washington, DC 20010, USA
Tel +1 202 602 4090
Email [email protected]
Abstract: Inhaled nitric oxide (iNO) is a pulmonary vasodilator approved for use to improve lung function in neonates > 34 weeks’ gestational age with hypoxic respiratory failure and pulmonary hypertension. Infants with severe respiratory disease frequently require magnetic resonance imaging (MRI) scans for evaluation of treatment and diagnosis of concurrent disease processes. Until 2015, incompatibility between the standard iNO delivery system components and the magnetic field within the MRI setting required iNO treatment to be interrupted for MRI, which could increase risk of deoxygenation and rebound pulmonary hypertension. In some cases, patients had to forego or delay MRI in order to maintain uninterrupted iNO delivery. The US Food and Drug Administration cleared the first iNO delivery system specifically modified for conditional use with MRI scanners (INOmax DSIR® Plus MRI) in 2015, based on the determination that the MRI-cleared system met the performance standards equivalent to the standard system. The system design and manufacturer risk management activities, as well as the regulatory requirements for clearance and continued use, provide necessary safeguards to ensure that high-risk neonates receive uninterrupted iNO in a safe manner. Anecdotal reports suggest that adoption of the MRI-cleared system may help optimize care for critically ill neonates who require concurrent administration of iNO and MRI scanning. Further research will be necessary to quantify the nature and magnitude of clinical improvements associated with adoption of the MRI iNO delivery system.
Keywords: critical care, drug delivery systems, magnetic resonance imaging, newborn, nitric oxide
The Role of Nitric Oxide in Neonatal Hypoxic Respiratory Failure
Nitric oxide (NO) is a naturally occurring, selective pulmonary vasodilator that plays a role in synaptic plasticity, cerebral blood flow, platelet aggregation, and other physiological functions.1 Due to its very short half-life (<1 second), the effects of inhaled NO (iNO) are limited to the pulmonary vasculature, where arterial dilation lowers arterial pressure and reduces right-to-left intra-cardiac shunting without the systemic hypotension associated with longer-acting pulmonary vasodilators.1–4 In the neonatal care setting, infants born at or near term with severe hypoxic respiratory failure are usually treated supportively with supplemental oxygen and positive pressure ventilation.3 In cases where infants have pulmonary hypertension and are not adequately responding to these supportive measures, treatment with iNO is often used. If these less-invasive therapies fail, the subsequent requirement for extracorporeal membrane oxygenation (ECMO) is associated with in-hospital mortality of up to 61%, and disability, cognitive or physical delays, or motor difficulties in as many as 26% of survivors.5–8
Treatment with iNO can reduce the need for ECMO,9–14 and in 1999 the US Food and Drug Administration (FDA) approved iNO (INOmax®; INO Therapeutics LLC, Hazelwood, MO, USA) to improve oxygenation and reduce the need for ECMO in neonates >34 weeks’ gestational age with hypoxic respiratory failure associated with pulmonary hypertension.15 The most predictable adverse effects of iNO (methemoglobinemia, bleeding disorders, and accumulation of potentially toxic levels of nitrogen dioxide [NO2]) are uncommon with the low doses used clinically.3,16 Toxic NO2 accumulation can also be minimized by mixing NO into ventilator circuits near the patient, flushing delivery systems before use, and constant monitoring of ventilator gas concentrations.3,16
The Need for Uninterrupted NO Delivery in the MRI Suite
Infants with severe respiratory disease frequently require magnetic resonance imaging (MRI) scans to evaluate treatment and diagnose concurrent disease processes. Until 2015, incompatibility between ferromagnetic components in the standard iNO delivery system and the magnetic field in the MRI suite often led to a dilemma in which clinicians had to choose to: 1) forgo or delay imaging; 2) interrupt continuous iNO delivery to perform imaging;17–20 or 3) modify the standard system for use in the MRI setting.21
Forgoing or delaying imaging could impede accurate diagnosis and treatment, and compromise clinical decision-making. Interruption of iNO delivery could lead to a potentially dangerous reduction in oxygenation and/or rebound pulmonary hypertension.17–20,22 Improvised modification of the standard iNO delivery system for use in an MRI setting could cause MRI or iNO system shutdown or malfunction and risk physical injury associated with magnetic attraction of system components. A few reports of investigator-improvised modifications have been published. Devendra et al21 evaluated administration of iNO using an investigator-modified system in a single adult male patient undergoing preoperative cardiac MRI. To allow the delivery system to remain outside the MRI suite, the investigators extended the delivery tubing using 5 pieces of standard 7-foot AirLife O2 tubing, connected by AirLife O2 tubing connectors (Cardinal Health, Dublin, OH, USA) and passed the extended tubing through a shielded electrical channel toward the patient. After a baseline MRI scan, the patient received 40 ppm iNO through a non-rebreather mask connected to the modified system. Measurement of mean NO and O2 delivery, and NO2 levels, indicated similar results when using the modified and standard (unmodified) systems at iNO doses of ≤20 ppm. However, at iNO doses ≥40 ppm, there was a statistically significant increase in NO2 levels delivered with the modified system compared with the standard system (0.5 vs 0.33 ppm [P=0.04] and 1.5 vs 0.73 ppm [P=0.02] with iNO doses of 40 and 80 ppm, respectively), possibly due to increased exposure time between NO and O2 in the extended tubing. Results from this single-patient study prompted the same investigators to conduct a larger study in which cardiac MRI was performed at 1.5 Tesla (Magnetom Avanto; Siemens Medical Systems, Erlangen, Germany) while delivering continuous iNO using their modified device in 16 patients with pulmonary valve insufficiency and repaired tetralogy of Fallot or pulmonary stenosis.23 In this study, all right and left ventricular volumetric measurements remained unchanged when using the modified device, and no significant changes in aortic flow parameters were observed. NO2 levels were not evaluated. Although the investigators concluded that this study demonstrated proof of concept for safe use of a modified iNO delivery system within the MRI suite, the safety risks and legal liabilities associated with adverse outcomes from use of an improvised system in larger, more heterogeneous patient populations were not addressed.
In all of the situations described previously the quality of care in critically ill neonates was at risk of being compromised due to limitations of the available technology. Clearly, there are numerous potentially serious hazards that can arise when untested improvisations are made to iNO delivery systems. An overview of potential hazards that have been identified to date in MRI settings is provided in the Table 1. During the past decade there has been increased focus on regulatory standards for validation and/or proof of appropriate use of medical devices, including International Organization for Standardization (ISO) standards 13485 and 14971, and the Medical Device Single Audit Program (MDSAP). Given these standards, modification or use of devices without regulatory clearance, not only runs the risk of serious patient harm, but may also have legal and/or regulatory consequences.
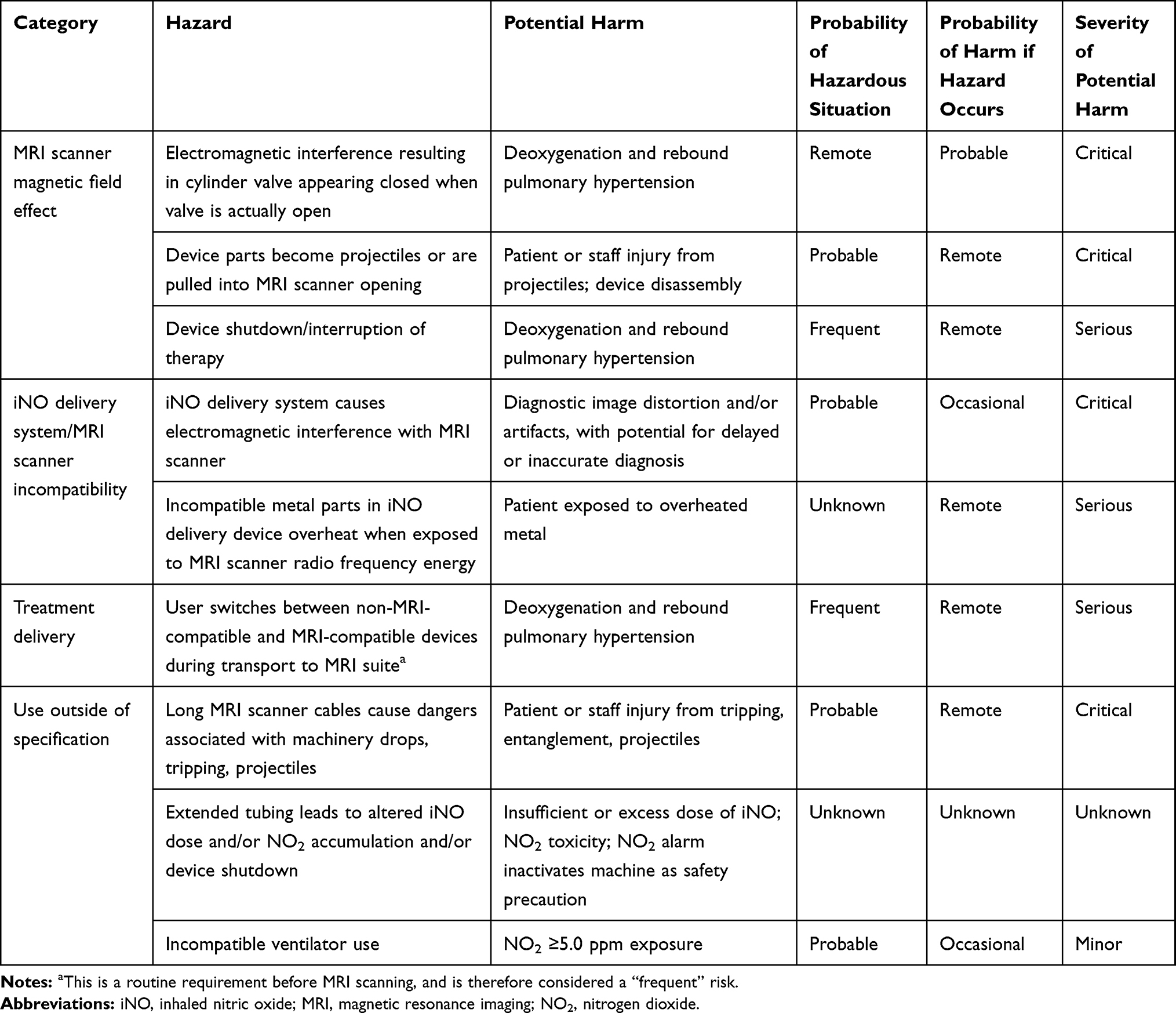 |
Table 1 Potential Hazards When Using Improvised Devices to Deliver Inhaled Nitric Oxide in the MRI Suite |
Development and Evaluation of an MRI-Compatible NO Delivery System
With the goal of improving patient access with ensured safety in MRI settings, the manufacturer (Mallinckrodt Pharmaceuticals, Bedminster, NJ) undertook development of an MRI-compatible iNO delivery system to meet the unmet need for such a system. The FDA-mandated process to obtain clearance for an MRI-compatible system required the manufacturer to demonstrate that it was at least as safe and effective as the legally marketed standard system (INOmax DSIR®; Mallinckrodt Pharmaceuticals), a standard known as substantial equivalence. In order to minimize potential harm to patients and achieve regulatory clearance, rigorous steps had to be taken by the manufacturer to address foreseen risks associated with the MRI-compatible system. As part of the clearance process, the system was tested inside both 1.5- and 3.0-Tesla MRI suites with the MRI scanner running, while concurrently testing 3 commonly used ventilators. Other parameters assessed under these 1.5- and 3.0-Tesla MRI conditions include: quantitative analysis of impact of the iNO system on signal-to-noise ratio of acquired MRI images and evaluation of image artifacts; displacement testing of all iNO system components; validation of overall proper functioning of the iNO system; and validation of overall proper functioning of both the iNO system and ventilator or other gas delivery systems when used concomitantly with the iNO system. This testing revealed a negligible effect on acquired image quality (signal-to-noise ratio, geometric distortion) for image sequences anticipated to be susceptible to imaging artifacts.24 The device manufacturer also implemented a comprehensive risk management plan with defined risk management activities for the system hardware, software, cart, regulator, and the iNO blender system, which mixes iNO with O2 before patient delivery. The plan defined criteria for risk acceptability, ensured that risk controls built in during system design addressed identified hazards, and ensured that the system was compliant with the ISO 14971 standard for application of risk management to medical devices.25 It also provided for postmarketing risk reviews and external audits to be conducted every 24 months.
A comprehensive risk review conducted in October 2015 concluded that all identified hazards/associated risk level scores were as low as reasonably possible. Later that year, the FDA cleared the first iNO delivery system for conditional use with MRI scanners, allowing uninterrupted iNO delivery during transport to and from the MRI scanner, and during MRI scanning (INOmax DSIR® Plus MRI; Mallinckrodt Pharmaceuticals, Bedminster, NJ) (Figure 1).24
 |
Figure 1 Schematic diagram of the INOmax DSIR Plus Magnetic Resonance Imaging System. Reproduced with permission from INOmax DSIR® Plus MRI Operation Manual, Mallinckrodt Pharmaceuticals, Hampton, NJ, USA; 2015.24 Abbreviations: CPU, central processing unit; DSIR, inhaled nitric oxide delivery system; iNO, inhaled nitric oxide; MR, magnetic resonance; NO, nitric oxide; ppm, parts per million. |
Safety Features of the MRI-Validated iNO Delivery System
Key modifications to the standard iNO delivery system made to facilitate safe use in the MRI suite include installation of auto-brake engagement of cart casters; integrated gauss alarms on both sides of the cart that are triggered if the system breaches the safety zone around the magnetic resonance bore; integrated tether attachment; modified system software to improve user safety in MRI environments; and adaptations to the cart hardware. Other safety features of the MRI-cleared system include integrated monitoring of inspired O2, NO, and NO2 levels, longer injector module cables, tubes and sample lines than the standard system to ensure that the MRI-cleared system can be located at a safe distance from the scanner, and backup functions for critical components (battery that provides up to 6 hours of uninterrupted iNO delivery; integrated pneumatic iNO delivery backup that provides 250 mL/min of iNO, which equates to delivery of 10 L/min of oxygen and 20 ppm of iNO to the patient breathing circuit). Labeling for the MRI-cleared system allows for use in environments with MRI scanners of 1.5- or 3.0-Tesla strength, in areas with field strength <100 gauss, with compatible ventilators including MVP-10 (Bio-Med Devices, Guilford, CT), LTV 1200 MRI (CareFusion, Franklin Lakes, NJ), and SERVO-i (Maquet, Wayne, NJ), and with a nasal cannula with 7-foot supply tubing (infant, 1601; Salter Labs, Lake Forest, IL, USA).
The system’s “dual-channel” design has one channel that includes the delivery central processing unit (CPU), flow controller, and injector module to ensure accurate delivery of iNO and ventilator waveform tracking. The second channel (the monitoring system) includes a separate monitor CPU; NO, O2, and NO2 cells; and the user interface, including the display and a wide-ranging alarm system. This design permits iNO delivery independent of monitoring and allows the monitoring system to shut down iNO delivery if the monitored concentration exceeds 100 ppm for 12 consecutive seconds, or if serious problems with the monitoring system are detected.
Application of the INOmax DSIR Plus MRI System: Case Examples
Clinician experiences from Children’s National Health System in Washington, DC demonstrate successful applications of the INOmax DSIR Plus MRI system. Two MRI-cleared systems were obtained to guarantee continued operation in case of single device malfunction, and these were stationed near the cardiac catheterization lab and the MRI suite. The MRI-cleared systems were commonly used in the cardiac intensive care unit for patients who had congenital heart disease requiring MRI visualization of cardiac defects; many patients in the neonatal intensive care unit also required the new technology. Manufacturer-sponsored educational support and in-service programs provided training to ensure that hospital staff were confident in operating the system. Anecdotal staff reports suggest that the number of patients receiving iNO while undergoing MRI scans increased after MRI-cleared systems became available.
Review of medical records at Children’s National identified three illustrative cases in which use of the INOmax DSIR Plus MRI system allowed patients receiving extended iNO therapy to undergo timely diagnostic MRI scanning that facilitated appropriate management. In the first case, a 5-month-old female with a double inlet left ventricle and aortic coarctation experienced seizures following stage 2 cardiac repair. While the infant was intubated on pressure control ventilation and iNO therapy at 5 ppm, MRI scanning revealed a possible left-sided middle cerebral artery aneurysm. Repeat MRI excluded an aneurysm, confirming that the visualized area of reduced blood flow was due to a previous postoperative stroke. In this case, the MRI-cleared system allowed this ventilated patient to continue receiving her iNO therapy without interruption during MRI scanning.
In the second case, an 11-month-old male with DiGeorge syndrome, tetralogy of Fallot, and pulmonary atresia had undergone banding of the left subclavian artery, and right ventricle to right and left pulmonary vessel conduit surgery. Following the most recent surgery, during which the patient was intubated and receiving iNO at 5 ppm, neurological examination revealed almost no movement in his right upper extremities. MRI scanning demonstrated findings consistent with a recent left centrum semiovale, perirolandic infarction, and a small subdural hematoma. Identification of the stroke informed the medical plan for this patient.
In the third case, an 11-year-old male with heterotaxy, an atrioventricular canal defect, and pulmonary atresia had undergone multiple previous surgical procedures, including a bilateral bidirectional Glenn procedure with a fenestrated fontan. Cardiac hemodynamics had been favorable since then. On presenting with acute respiratory distress, the patient was found to have plastic bronchitis requiring frequent therapeutic bronchoscopies to remove airway casts. After pulmonary consultation determined probable pulmonary lymphatic perfusion syndrome, MR lymphangiography was undertaken to assess the patient, who was mechanically ventilated and on iNO at 20 ppm. MRI demonstrated contrast in the upper thorax, suggesting reflux of lymph fluid above the level of the thoracic ducts. The patient was transferred to a specialist facility for lymphatic intervention. In this case, the MRI-conditional system allowed uninterrupted delivery of iNO during confirmation of etiology, which facilitated rapid specialist care.
Conclusion
Use of modified iNO delivery systems that have not received regulatory clearance for use in the MRI suite can result in treatment interruption and poses other safety risks to patients, including critically ill neonates, as well as healthcare providers. An iNO delivery system designed and cleared for safe use in the MRI suite offers clinicians and hospital administrators the opportunity to optimize care by providing continuous iNO to some of the most vulnerable patients, while still meeting their MRI needs.
Abbreviations
CPU, central processing unit; ECMO, extracorporeal membrane oxygenation; FDA, US Food and Drug Administration; FiO2, fraction of inspired oxygen; ICU, intensive care unit; iNO, inhaled nitric oxide; ISO, International Organization for Standardization; IV, intravenous; MDSAP, Medical Device Single Audit Program; MR, magnetic resonance; MRI, magnetic resonance imaging; NO, nitric oxide; NO2, nitrogen dioxide.
Funding
Medical writing and editorial support, which was conducted in accordance with Good Publication Practice (GPP3) and the International Committee of Medical Journal Editors (ICMJE) guidelines, was provided by Michael D. Morren, RPh, MBA, of Peloton Advantage, LLC, an OPEN Health company, funded by Mallinckrodt Pharmaceuticals.
Disclosure
Jaron Acker is an employee of Mallinckrodt Pharmaceuticals and may hold stock or stock options in that company. Jim L. Potenziano is a former employee of Mallinckrodt Pharmaceuticals and holds stock in that company. The authors report no other conflicts of interest in this work.
References
1. Luiking YC, Engelen MP, Deutz NE. Regulation of nitric oxide production in health and disease. Curr Opin Clin Nutr Metab Care. 2010;13(1):97–104. doi:10.1097/MCO.0b013e328332f99d
2. Muzevich KM, Chohan H, Grinnan DC. Management of pulmonary vasodilator therapy in patients with pulmonary arterial hypertension during critical illness. Crit Care. 2014;18(5):523. doi:10.1186/s13054-014-0523-z
3. Sokol GM, Konduri GG, Van Meurs KP. Inhaled nitric oxide therapy for pulmonary disorders of the term and preterm infant. Semin Perinatol. 2016;40(6):356–369. doi:10.1053/j.semperi.2016.05.007
4. Bin-Nun A, Schreiber MD. Role of iNO in the modulation of pulmonary vascular resistance. J Perinatol. 2008;28(Suppl 3):S84–S92. doi:10.1038/jp.2008.161
5. Van Litsenburg R, De Mos N, Edgell D, Gruenwald C, Bohn DJ, Parshuram CS. Resource use and health outcomes of paediatric extracorporeal membrane oxygenation. Arch Dis Child Fetal Neonatal Ed. 2005;90(2):F176–F177. doi:10.1136/adc.2003.047779
6. Hanekamp MN, Mazer P, van der Cammen-van MH, et al. Follow-up of newborns treated with extracorporeal membrane oxygenation: a nationwide evaluation at 5 years of age. Crit Care. 2006;10(5):R127. doi:10.1186/cc5039
7. UK Collaborative ECMO Trial Group. UK collaborative randomised trial of neonatal extracorporeal membrane oxygenation. Lancet. 1996;348(9020):75–82. doi:10.1016/S0140-6736(96)04100-1
8. Hirakawa E, Ibara S, Tokuhisa T, et al. Extracorporeal membrane oxygenation in 61 neonates: single-center experience. Pediatr Int. 2017;59(4):438–442. doi:10.1111/ped.13178
9. Field D, Elbourne D, Hardy P, et al. Neonatal ventilation with inhaled nitric oxide vs. ventilatory support without inhaled nitric oxide for infants with severe respiratory failure born at or near term: the INNOVO multicentre randomised controlled trial. Neonatology. 2007;91(2):73–82. doi:10.1159/000097123
10. Christou H, Van Marter LJ, Wessel DL, et al. Inhaled nitric oxide reduces the need for extracorporeal membrane oxygenation in infants with persistent pulmonary hypertension of the newborn. Crit Care Med. 2000;28(11):3722–3727. doi:10.1097/00003246-200011000-00031
11. Clark RH, Kueser TJ, Walker MW, et al. Low-dose nitric oxide therapy for persistent pulmonary hypertension of the newborn. Clinical Inhaled Nitric Oxide Research Group. N Engl J Med. 2000;342(7):469–474. doi:10.1056/NEJM200002173420704
12. The Neonatal Inhaled Nitric Oxide Study Group. Inhaled nitric oxide in full-term and nearly full-term infants with hypoxic respiratory failure. The Neonatal Inhaled Nitric Oxide Study Group [published correction appears in N Engl J Med. 1997;337:434]. N Engl J Med. 1997;336(9):597–604.
13. Roberts JD
14. Davidson D, Barefield ES, Kattwinkel J, et al. Inhaled nitric oxide for the early treatment of persistent pulmonary hypertension of the term newborn: a randomized, double-masked, placebo-controlled, dose-response, multicenter study. The I-NO/PPHN Study Group. Pediatrics. 1998;101(3 Pt 1):325–334. doi:10.1542/peds.101.3.325
15. INOmax [package insert]. Bedminster, NJ: INO Therapeutics; 2019.
16. DiBlasi RM, Myers TR, Hess DR. Evidence-based clinical practice guideline: inhaled nitric oxide for neonates with acute hypoxic respiratory failure. Respir Care. 2010;55(12):1717–1745.
17. Miller OI, Tang SF, Keech A, Celermajer DS. Rebound pulmonary hypertension on withdrawal from inhaled nitric oxide. Lancet. 1995;346(8966):51–52. doi:10.1016/S0140-6736(95)92681-X
18. Atz AM, Adatia I, Wessel DL. Rebound pulmonary hypertension after inhalation of nitric oxide. Ann Thorac Surg. 1996;62(6):1759–1764. doi:10.1016/S0003-4975(96)00542-5
19. Cueto E, Lopez-Herce J, Sanchez A, Carrillo A. Life-threatening effects of discontinuing inhaled nitric oxide in children. Acta Paediatr. 1997;86(12):1337–1339. doi:10.1111/j.1651-2227.1997.tb14909.x
20. Lavoie A, Hall JB, Olson DM, Wylam ME. Life-threatening effects of discontinuing inhaled nitric oxide in severe respiratory failure. Am J Respir Crit Care Med. 1996;153(6 Pt 1):1985–1987. doi:10.1164/ajrccm.153.6.8665066
21. Devendra GP, Hart SA, Kim YY, Setser RM, Flamm SD, Krasuski RA. Modified INOvent for delivery of inhaled nitric oxide during cardiac MRI. Magn Reson Imaging. 2011;29(8):1145–1149. doi:10.1016/j.mri.2011.05.008
22. Davidson D, Barefield ES, Kattwinkel J, et al. Safety of withdrawing inhaled nitric oxide therapy in persistent pulmonary hypertension of the newborn. Pediatrics. 1999;104(2 Pt 1):231–236. doi:10.1542/peds.104.2.231
23. Hart SA, Devendra GP, Kim YY, et al. PINOT NOIR: pulmonic insufficiency improvement with nitric oxide inhalational response. J Cardiovasc Magn Reson. 2013;15:75. doi:10.1186/1532-429X-15-75
24. INOmax DSIR Plus MRI operation manual. Hampton, NJ: Mallinckrodt Pharmaceuticals; 2015.
25. Medical Devices - Quality Management Systems - Requirements for Regulatory Purposes (ISO 13485:2016). London, United Kingdom: British Standards Institution; 2017.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.