Back to Journals » International Medical Case Reports Journal » Volume 18
Rare Ocular Complication After Prone Position Surgery: Bilateral Subconjunctival Hemorrhage Following Endoscopic Lumbar Discectomy
Received 5 June 2025
Accepted for publication 21 October 2025
Published 25 October 2025 Volume 2025:18 Pages 1365—1370
DOI https://doi.org/10.2147/IMCRJ.S542197
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tanvi Dhere
Shin-Lin Chiu,1– 3 Chiu-Liang Chen4,5
1Department of Ophthalmology, Changhua Christian Hospital, Taiwan; 2Department of Optometry, Da-Yeh University, Changhua, Taiwan; 3Department of Post-Baccalaureate Medicine, College of Medicine, National Chung Hsing University, Taichung, Taiwan; 4Department of Orthopedics, Changhua Christian Hospital, Taiwan; 5Department of Nursing, Hungkuang University, Taichung, Taiwan
Correspondence: Chiu-Liang Chen, Department of Orthopedics, Changhua Christian Hospital, Taiwan, No. 135, Nanxiao St, Changhua, 50073, Taiwan, Email [email protected]; [email protected]
Abstract: Subconjunctival hemorrhage (SCH) is a rare complication in spinal surgery and is even more uncommon in endoscopic procedures, which are typically of short duration. We report the case of a 32-year-old male who developed bilateral SCH after an uneventful L4–L5 lumbar endoscopic discectomy performed under general anesthesia. The patient had a history of well-controlled hypertension and was not on anticoagulant therapy. The surgery lasted approximately 50 minutes, with appropriate head protection and smooth airway management. On the first postoperative day, bilateral SCH was observed without pain or visual disturbance. The hemorrhages resolved spontaneously within two weeks without complications. Although the exact mechanism remains unclear, contributing factors may include prone positioning, venous congestion, hemodynamic shifts, and hypertension-related vascular fragility. This case highlights the importance of recognizing subconjunctival hemorrhage as a rare but benign complication of prone spinal surgery, and suggests that patient reassurance and awareness are essential.
Plain Language Summary: This report describes a rare eye condition that occurred after an endoscopic spine surgery. A 32-year-old man underwent an endoscopic lumbar discectomy, a common procedure used to treat a herniated disc in the lower back. The surgery was short, lasted only 50 minutes, and went smoothly under general anesthesia. Postoperatively, the patient was found to have bleeding in both eyes, known as bilateral subconjunctival hemorrhage. Although this looked concerning, it caused no pain or vision problems and resolved on its own within two weeks. This type of bleeding after spine surgery is very rare, and there are no previous reports of it happening after endoscopic spine surgery. The exact cause is unknown, but it may be related to body positioning during surgery, increased pressure in the veins, or the patient’s history of high blood pressure. This case shows that even with short and low-risk procedures, rare but harmless complications can happen, and awareness of such events can help doctors reassure patients and avoid unnecessary alarm.
Keywords: intraocular pressure fluctuation, perioperative hemodynamics, postoperative eye finding, venous congestion, microvascular rupture
Introduction
Subconjunctival hemorrhage (SCH) is a rare but known complication following various surgical procedures, particularly those performed in the prone position, such as spinal surgeries.1,2 It is most often seen following prolonged surgeries that involve increased venous pressure, but its occurrence remains an underreported event in lumbar endoscopic discectomy. SCH may present as a self-limited condition,2 but it can cause significant concern for both patients and surgeons due to its visible nature and potential for misdiagnosis. The pathophysiology of SCH remains multifactorial,3 and most reported cases of SCH are unilateral. Hofer et al reported an ocular injury rate of approximately 0.19% in 20,128 spine surgeries,4 while Stevens et al found a 0.20% incidence of vision-loss-related complications in 3,450 major spine reconstructions.5 Perioperative visual loss has also been estimated to occur in 0.013–1% of cases in large reviews.6 However, subconjunctival hemorrhage remains an extremely rare event, especially in short-duration procedures such as endoscopic lumbar discectomy. The occurrence of bilateral SCH, as observed in our patient, is exceptionally rare and has not been documented in the context of endoscopic spine surgery. This report presents a case of bilateral SCH following L4-L5 lumbar endoscopic discectomy performed under general anesthesia, in which no major complications were noted during surgery. This report aims to explore the potential contributing factors and raise awareness of this rare postoperative finding in spine surgery.
Case Report
A 32-year-old male patient presented with a three-month history of lower back pain accompanied by numbness and radicular pain in the right lower limb. Magnetic resonance imaging (MRI) revealed a paramedian-type herniated intervertebral disc at the L4–L5 level. (Figure 1: MRI) His medical history was significant for well-controlled hypertension, which had been diagnosed three years prior. He had been taking antihypertensive medication regularly, and his blood pressure was consistently maintained around 120/70 mmHg. The patient had no history of anticoagulant use or any known ocular or systemic conditions that could predispose him to subconjunctival hemorrhage.
 |
Figure 1 Preoperative lumbar spine MRI (T2-weighted images). Left: Sagittal image showing a herniated disc at the L4–L5 level compressing the thecal sac. Right: Axial image at the L4–L5 level. Green arrows indicate bilateral impingement of the traversing L5 nerve roots within the lateral recesses. |
The patient underwent L4-L5 lumbar endoscopic discectomy in the prone position and under general anesthesia. The procedure, lasting approximately 50 minutes, was executed with precision and care. A horseshoe-shaped viscoelastic gel headrest was used to support the patient’s head in the prone position without direct compression on the eyes. After positioning, the surgical and anesthesia teams verified proper alignment and facial symmetry to avoid unintended contact. This setup is consistent with current recommendations for ocular protection in prone spinal procedures. Throughout the operation, the patient’s blood pressure remained stable at approximately 120/70 mmHg, with no significant fluctuations noted. The intraoperative fluid input was 700 mL (lactated Ringer’s solution), and urine output was 21 mL, resulting in a positive fluid balance of 679 mL. The balanced intraoperative fluid status and the smooth performance of endotracheal intubation and extubation further ensured the patient’s safety.
On the first postoperative day, the patient was found to have SCH involving both eyes. He reported no pain or visual disturbances. An ophthalmological consultation was performed, which revealed normal intraocular pressure (IOP): 16 mmHg in the right eye and 15 mmHg in the left eye. Visual acuity was preserved, and there were no signs of corneal or retinal abnormalities. The patient’s blood pressure remained within normal limits postoperatively. Over the following two weeks, the SCH gradually resolved without intervention, and the patient experienced no long-term ocular complications (Figure 2: Day-1 clinical photo; Figure 3: Two-week follow-up).
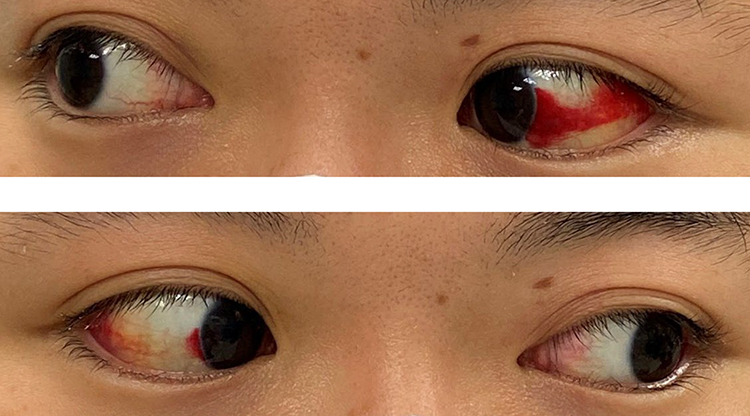 |
Figure 2 Photograph taken on postoperative day one, showing bilateral subconjunctival hemorrhage without associated periorbital swelling or ecchymosis. |
 |
Figure 3 Clinical photograph taken two weeks after surgery showing gradual resolution of bilateral subconjunctival hemorrhage. |
Discussion
SCH can be caused by a variety of factors, including trauma, contact-lens-induced injury, hypertension, and the use of aspirin.3,7,8 Transient increases in venous pressure due to coughing, vomiting, or surgical stress may also contribute.9 While ophthalmic complications after spinal surgery have been reported in the literature,1,10 most literature has focused on serious sequelae such as ischemic optic neuropathy, intraocular hemorrhage, or visual loss,5,11,12 and the incidence of minor events like SCH remains poorly defined. Although visual complications after spine surgery have been documented, there is currently no published data specifically reporting the incidence of SCH following spine surgery. Studies such as Hofer et al4 and Stevens et al5 have reported the overall incidence of ocular injuries as 0.19%–0.20%, but SCH was not mentioned. Therefore, the true frequency of SCH remains unknown, emphasizing the novelty and educational value of this case.
The prone position during surgery is associated with increased IOP and venous congestion, which can predispose small conjunctival vessels to rupture.1,13,14 Akhaddar and Boucetta described a case where intraoperative positioning alone was sufficient to induce SCH.2 Cheng et al demonstrated that IOP increases significantly during prone general anesthesia, particularly with longer procedures.14 General anesthesia itself may impair normal IOP regulation, amplifying the effect of venous congestion.13
Ophthalmic complications following spinal surgery have been attributed primarily to direct external compression of the eye, as reported by some investigators.10 These cases typically present as unilateral vision loss. In addition, thromboembolic events involving the internal carotid artery have also been proposed as a possible mechanism, leading to vascular occlusion and subsequent ocular complications. These findings reinforce that prone spine surgery, especially under general anesthesia, may alter ocular hemodynamics, and that protecting the eyes from direct compression is critical.
Although IOP elevation has been implicated in various visual complications,13 there is no direct evidence linking IOP to SCH. Moreover, IOP is not routinely monitored intraoperatively in spine surgery, limiting real-time correlation. Further investigation is warranted to better understand the pathophysiology and perioperative risk factors associated with rare ophthalmic events like SCH. This case suggests that even brief prone positioning, when combined with underlying microvascular fragility from chronic hypertension, may be sufficient to precipitate bilateral subconjunctival vessel rupture in the absence of direct ocular trauma or anticoagulant use.
To mitigate such rare but potentially distressing ophthalmic complications, several preventive strategies should be considered. Ensuring standardized head positioning with equipment designed to suspend the eyes and eliminate facial pressure is essential. In this case, a horseshoe-shaped viscoelastic gel headrest was used to provide adequate support. The gel material redistributed pressure evenly across the forehead and chin, effectively suspending the orbital region and minimizing the risk of ocular compression, and contributing to the prevention of positioning-related complications.2,14,15
Additionally, preoperative identification of patients with vascular risk factors, such as hypertension or known ocular conditions, may help guide intraoperative precautions.11,15 For high-risk patients undergoing longer procedures in the prone position, intraoperative IOP monitoring may be considered, though current technical limitations in real-time measurement should be acknowledged. Together, these strategies may enhance the safety of spinal procedures and raise awareness of uncommon but clinically relevant ocular complications.
Transient increases in thoracic venous pressure from intubation and extubation may also contribute. Although airway management during intubation and extubation was uneventful, Valsalva-like maneuvers may still occur, affecting venous return and pressure.1 Laborda et al have shown that Valsalva maneuvers can significantly affect venous return and pressure dynamics in the thoracic cavity, reinforcing its potential link to vascular rupture.16
Chronic hypertension may further increase SCH susceptibility. Even with adequate blood pressure control, cumulative structural changes in the vessel walls may render conjunctival vessels more susceptible to rupture under transient stressors such as intraoperative positioning, fluctuations in venous pressure, and perioperative fluid shifts.11 Beevers et al emphasized that even well-managed hypertension can predispose patients to microvascular rupture under transient stressors, such as perioperative positioning and pressure shifts.17
SCH is typically unilateral. The present case of bilateral SCH is unusual, especially in the absence of risk factors such as trauma or anticoagulant use. Although rare bilateral cases have been reported in the context of trauma or coagulopathy, this may be the first documented instance following endoscopic spine surgery without identifiable triggers. While most SCH cases are benign and self-limiting, certain clinical features warrant further evaluation, including persistence beyond two weeks, recurrence, ocular discomfort, visual changes, or signs of systemic bleeding.8,10,12 Routine ophthalmologic consultation may not be necessary in asymptomatic cases, but awareness of these red flags is essential. Given its benign course, SCH may also be discussed preoperatively as a rare complication of prone spine surgery, particularly in patients with vascular risk factors such as hypertension.
Conclusion
This rare case of bilateral SCH following prone spine surgery under general anesthesia underscores the importance of heightened awareness of ophthalmic complications, even in short and minimally invasive procedures. Proper head positioning, careful intraoperative monitoring, and consideration of patient-specific risk factors such as hypertension may help minimize such events. Postoperative ocular evaluation should be considered in selected cases to ensure timely detection and reassurance.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval and Informed Consent
The study protocol was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of Changhua Christian Hospital, Taiwan (IRB approval number: 250401; approval date: April 28,2025). According to institutional policy, publication of the case report was included in the approved protocol and did not require additional separate approval for publication. The patient provided written informed consent for the publication of this case report, including clinical information and accompanying images. The patient reviewed the final version of the manuscript and understands that identifiable details will be published with efforts made to ensure anonymity. A copy of the signed consent form is available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There was no funding for this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. DePasse JM, Palumbo MA, Haque M, Eberson CP, Daniels AH. Complications associated with prone positioning in elective spinal surgery. World J Orthop. 2015;6(3):351–359. doi:10.5312/wjo.v6.i3.351
2. Akhaddar A, Boucetta M. Subconjunctival hemorrhage as a complication of intraoperative positioning for lumbar spinal surgery. Spine J. 2012;12(3):274. doi:10.1016/j.spinee.2012.02.007
3. Mimura T, Usui T, Yamagami S, et al. Recent causes of subconjunctival hemorrhage. Ophthalmologica. 2010;224(3):133–137. doi:10.1159/000236038
4. Hofer RE, Evans KD, Warner MA. Ocular injury during spine surgery. Can J Anaesth. 2019;66(7):772–780. doi:10.1007/s12630-019-01323-w.
5. Stevens WR, Glazer PA, Kelley SD, Lietman TM, Bradford DS. Ophthalmic complications after spinal surgery. Spine. 1997;22(12):1319–1324. doi:10.1097/00007632-199706150-00008
6. Epstein NE. Perioperative visual loss following prone spinal surgery: a review. Surg Neurol Int. 2016;7(Suppl 13):S347–60. doi:10.4103/2152-7806.182550
7. Hu DN, Mou CH, Chao SC, et al. Incidence of non-traumatic subconjunctival hemorrhage in a nationwide study in Taiwan from 2000 to 2011. PLoS One. 2015;10(7):e0132762. doi:10.1371/journal.pone.0132762
8. Tarlan B, Kiratli H. Subconjunctival hemorrhage: risk factors and potential indicators. Clin Ophthalmol. 2013;7:1163–1170. doi:10.2147/OPTH.S35062
9. Tampoya C, Sawamura MH, Tong J, Ilsen PF. Ocular manifestations of valsalva maneuver. Clin Refractive Optometry. 2017;4:132–138.
10. Delattre O, Thoreux P, Liverneaux P, et al. Spinal surgery and ophthalmic complications: a French survey with review of 17 cases. J Spinal Disord Tech. 2007;20(4):302–307. doi:10.1097/01.bsd.0000211290.21766.04
11. Tabandeh H. Intraocular hemorrhages associated with endoscopic spinal surgery. Am J Ophthalmol. 2000;129(5):688–690. doi:10.1016/s0002-9394(99)00470-5
12. Khalatbari MR, Khalatbari I, Moharamzad Y. Intracranial hemorrhage following lumbar spine surgery. Eur Spine J. 2012;21(10):2091–2096. doi:10.1007/s00586-012-2187-1
13. VANW SA. Systematic review and meta-analysis of prone position on intraocular pressure in adults undergoing surgery. Int J Spine Surg. 2020;14(2):195–208. doi:10.14444/7029
14. Cheng MA, Todorov A, Tempelhoff R, McHugh T, Crowder CM, Lauryssen C. The effect of prone positioning on intraocular pressure in anesthetized patients. Anesthesiology. 2001;95(6):1351–1355. doi:10.1097/00000542-200112000-00012
15. Lee LA, Roth S, Posner KL, et al. The American society of anesthesiologists postoperative visual loss registry: analysis of 93 spine surgery cases with postoperative visual loss. Anesthesiology. 2006;105(4):652–9;quiz867–8. doi:10.1097/00000542-200610000-00007
16. Laborda A, Sierre S, Malve M, et al. Influence of breathing movements and Valsalva maneuver on vena caval dynamics. World J Radiol. 2014;6(10):833–839. doi:10.4329/wjr.v6.i10.833
17. Beevers G, Lip GY, O’Brien E. ABC of hypertension: the pathophysiology of hypertension. BMJ. 2001;322(7291):912–916. doi:10.1136/bmj.322.7291.912
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.