Back to Journals » International Medical Case Reports Journal » Volume 18
Rapid Absorption of a Spontaneous Primary Intraventricular Hemorrhage
Received 17 February 2025
Accepted for publication 7 May 2025
Published 17 May 2025 Volume 2025:18 Pages 573—576
DOI https://doi.org/10.2147/IMCRJ.S521860
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xudong Zhu
Xiao-Yong Shi, Yue Lou
Brain Center, Zhejiang Hospital, Hangzhou, Zhejiang Province, People’s Republic of China
Correspondence: Yue Lou, Brain Center, Zhejiang Hospital, Hangzhou, Zhejiang Province, People’s Republic of China, Email [email protected]
Abstract: Spontaneous primary intraventricular hemorrhage (IVH) is a rare type of intracranial hemorrhage that can be concentrated in one or more ventricles. The clinical symptoms after bleeding are diverse, if there is significant bleeding or hydrocephalus, external ventricular drainage (EVD) treatment is often required. Absorption of the hematoma after ventricular hemorrhage usually takes several weeks, and there are very few articles in the literature on hematoma absorption. As far as we know early spontaneous disappearance of spontaneous primary IVH has not previously been reported in the literature. Herein, we describe a rare case of spontaneous primary IVH that rapidly disappeared without surgical intervention. The patient, a 73-year-old male, was admitted to the hospital for “unclear speech for 16 hours”. An initial head computed tomography (CT) scan showed significant accumulation of blood in both lateral ventricles, the third ventricle, midbrain aqueduct, and fourth ventricle, as well as acute hydrocephalus. The patient was conscious and did not undergo EVD treatment. After 24 hours, head CT re-examination showed that the accumulated blood had been significantly absorbed, and hydrocephalus had improved. Three days later, head CT re-examination showed that the accumulated blood in the ventricles had been absorbed, and the patient did not experience any discomfort. Following observation for a few more days, he was discharged from the hospital.
Keywords: intraventricular hemorrhage, intracranial hemorrhage, cerebrospinal fluid, external ventricular drainage, subarachnoid hemorrhage
Introduction
Spontaneous intraventricular hemorrhage (IVH) is classified into primary and secondary types, Approximately 70%1 of IVHs are secondary, usually as a common complication of intracerebral hemorrhage (ICH) or subarachnoid hemorrhage. Primary IVH is a rare type of hemorrhage without parenchymal involvement. Primary IVH accounts for approximately 3% of cerebral hemorrhages,2 and absorption can take several weeks. However, early spontaneous disappearance of primary IVH has not previously been reported in the literature.
Case Presentation
The patient, a 73-year-old male, was admitted to the hospital for “unclear speech for 16 hours”. He had a history of hypertension treated with antihypertensive drugs and his blood pressure was controlled within the normal range. Urgent CT angiography (CTA) of the head showed no abnormalities in cerebral blood vessels, with obvious accumulation of blood in both lateral ventricles, the third ventricle, midbrain aqueduct, and fourth ventricle (Figure 1). The ventricular system was dilated, indicating acute hydrocephalus. At this time, the patient was conscious and had indications for external ventricular drainage (EVD). However, due to the patient and his family’s fear of surgical treatment, they refused EVD. The patient’s condition was closely monitored. His mental status remained clear throughout. After 24 hours, head CT re-examination showed that hydrocephalus had improved, and the blood accumulation had been absorbed (Figure 2). The patient’s unclear speech had also improved. On the fourth day after admission, head CT re-examination showed that the blood accumulation in the brain ventricles had been absorbed (Figure 3), and the patient had no discomfort. Following several days of observation, the patient was discharged.
 |
Figure 1 Initial CT (2023-8-6 9:48) scan showed significant accumulation of blood in both lateral ventricles, the third ventricle, midbrain aqueduct, and fourth ventricle, as well as acute hydrocephalus. |
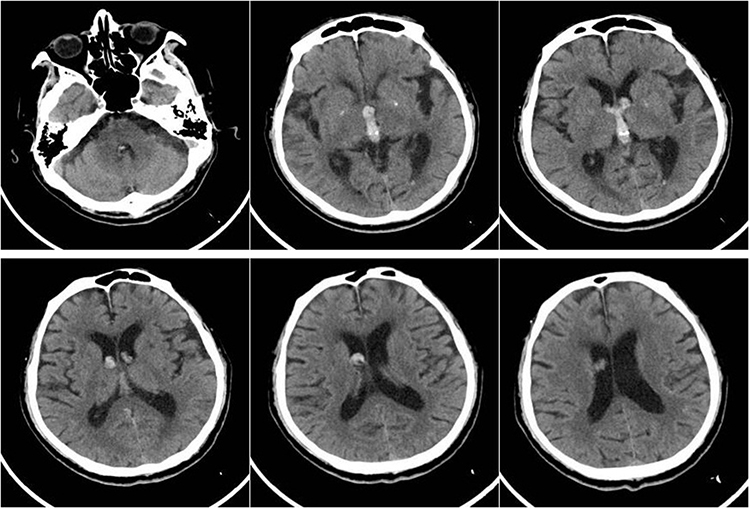 |
Figure 2 After 24 hours, head CT (2023-8-7 9:24) re-examination showed that the accumulation of blood had been significantly absorbed, and hydrocephalus had improved. |
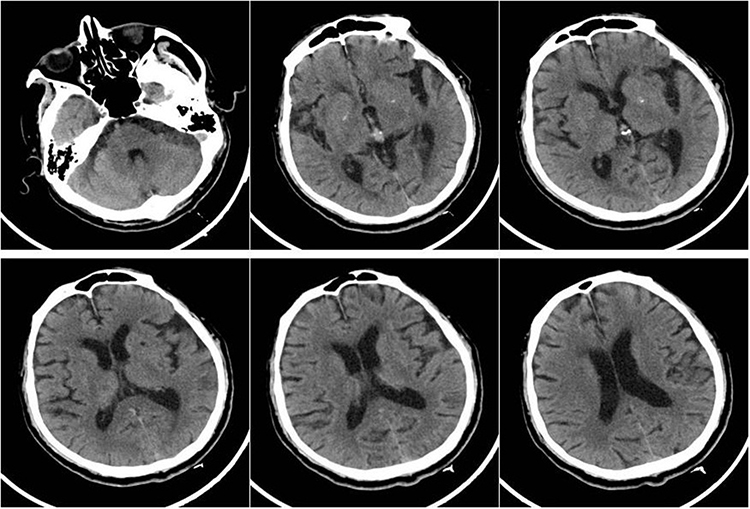 |
Figure 3 Four days after admission, head CT (2023-8-10 11:16) re-examination showed that the accumulation of blood in the ventricles had been absorbed. |
Discussion
Primary IVH can be due to different causes including trauma, vascular anomalies, tumors, coagulation disorders, and others. Recently, hypertension has been considered a direct cause of primary IVH.3,4 The presence of hydrocephalus has been reported in almost two-thirds of primary IVH cases, and 50% of these cases will require treatment with EVD.5 The complete absorption of ICH is related to the size of the hematoma, and larger intracerebral hematomas generally take 6 weeks or even longer to be fully absorbed. The absorption time of a hematoma after ventricular hemorrhage is relatively short, and can be completely absorbed within about 2–3 weeks. There are very few articles on the absorption of hematomas after ventricular hemorrhage; however, Naff et al6 conducted a very detailed study on this issue, and analyzed the CT scans of 17 adult patients with IVH. These authors indicated that the percentage rate of clot resolution was 10.8% per day, and was independent of initial clot volume, age, sex, type of underlying hemorrhage, and the use of EVD. By using this estimate, the clot half-life would be 5.4 days. Both large and small blood clots tended to have the same half-life. However, all 17 patients had secondary IVH and ten patients were treated with EVD. The absorption rate of primary ventricular hemorrhage may be different to that of secondary ventricular hemorrhage; however, this estimate can serve as a reference.
Eom KS7 described a rare case of traumatic IVH that rapidly disappeared within 3 days without surgical intervention. He believed that the thrombolytic enzyme system in the cerebrospinal fluid (CSF) or the circulation of CSF plays an important role in the rapid resolution of traumatic IVH. M Ali M et al8 reported an extremely rare case of isolated traumatic IVH with spontaneous and rapid disappearance within four days. These authors supported the hypothesis that CSF and its circulation are major players in the rapid resolution of isolated traumatic IVH.
Our patient had a history of hypertension, and CTA examination showed no obvious abnormalities in cerebral blood vessels. Further cerebral digital subtraction angiography was not performed due to the patient’s refusal. Bleeding in this patient also caused acute hydrocephalus but he refused surgical treatment. After admission, CT examination showed significant accumulation of blood in multiple ventricles and no significant abnormalities in coagulation function. Naff et al6 found that within the first 48 hours, 29.4% of the study population, demonstrated a greater than 5% increase in clot volume beyond their initial clot volume. After this initial 48-hour period, clot resolution seemed to proceed at a constant percentage rate. Unlike this, our patient’s CT scan 24 hours later showed a significant reduction in IVH, suggesting that this may have been related to the rapid circulation of CSF. Three days later, another CT scan showed that the hemorrhage had been absorbed.
Conclusion
We report that rapid absorption of spontaneous primary IVH may be related to the rapid circulation of CSF, and further research is warranted to clarify this rare phenomenon.
Ethics and Consent Statements
The patient provided informed consent for publication of the case. This case report has been certified by the ethics committee of Zhejiang Hospital.
Acknowledgments
There was no funding source for this manuscript.
Disclosure
The authors declare that they have no competing interests for this work.
References
1. Pan K, Pandit A, Bhattacharyya B, et al. Primary intraventricular haemorrhage: clinical and aetiological profile with predictors of outcome-a hospital based study. J Clin Diagn Re. 2018;12(6):OCO1–OCO4.
2. Robles LA, Volovici V. Hypertensive primary intraventricular hemorrhage: a systematic review. Neurosurg Rev. 2022;45(3):2013–2026. doi:10.1007/s10143-022-01758-8
3. Jiang Z, Peng Y, Zhang M, et al. Etiological factors of spontaneous primary intraventricular hemorrhage. Br J Neurosurg. 2020;34(4):423–426. doi:10.1080/02688697.2020.1751067
4. Pai A, Hegde A, Nair R, et al. Adult primary intraventricular hemorrhage: clinical characteristics and outcomes. J Neurosci Rural Pract. 2020;11(4):623–628. doi:10.1055/s-0040-1716770
5. Flint AC, Roebken A, Singh V. Primary intraventricular hemorrhage: yield of diagnostic angiography and clinical outcome. Neurocrit Care. 2008;8(3):330–336. doi:10.1007/s12028-008-9070-2
6. Naff NJ, Williams MA, Rigamonti D, et al. Blood clot resolution in human cerebrospinal fluid: evidence of first-order kinetics. Neurosurgery. 2001;49(3):614–619. doi:10.1097/00006123-200109000-00015
7. Eom KS. A Case of Rapid Spontaneous Disappearance of Traumatic Intraventricular Hemorrhage. Korean J Neurotrauma. 2020;16(2):273–277. doi:10.13004/kjnt.2020.16.e44
8. Ali M M, Elbasuny A H, Meshref M, et al. Fast resolution and good outcomes of isolated traumatic intraventricular haemorrhage: a case report. Folia Neuropathol. 2021;59(3):317–321. doi:10.5114/fn.2021.108294
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.