Back to Journals » Drug Design, Development and Therapy » Volume 20
Quantum Computing and Quantum Technologies in Drug Discovery and Therapeutics: Evidence, Benchmarking, and Translational Integration
Authors Niazi SK ![]()
Received 21 December 2025
Accepted for publication 26 March 2026
Published 30 April 2026 Volume 2026:20 590730
DOI https://doi.org/10.2147/DDDT.S590730
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Anastasios Lymperopoulos
Sarfaraz K Niazi
Department of Pharmaceutical Sciences, University of Illinois, Chicago, IL, 60612, USA
Correspondence: Sarfaraz K Niazi, Email [email protected]
Abstract: Quantum technologies—quantum computing, quantum sensing, and quantum-enabled materials—are increasingly proposed as tools to accelerate drug discovery. Yet “quantum advantage” is frequently asserted without standardized benchmarks, clinically meaningful endpoints, or controlled comparisons against modern classical workflows. This review separates (i) quantum computing for molecular simulation and optimization, (ii) quantum sensing for structural/biophysical characterization and diagnostics, and (iii) quantum nanotechnologies for imaging and sensing, and then extends the framework to include device-led and physical therapies that increasingly co-evolve with drug development: photobiomodulation (red/NIR), focused ultrasound for blood-brain barrier opening and delivery enhancement, noninvasive neuromodulation devices (tDCS/TMS), and optogenetic therapies. We summarize demonstrated capabilities and constraints of NISQ-era computing, outline algorithmic classes for quantum chemistry and hybrid variational methods, evaluate quantum error-mitigation strategies and their limits, and contrast claimed performance with classical baselines in computational chemistry and machine learning. We conclude that near-term translational value is most substantial for quantum sensing and for device/physical platforms with established clinical evidence. In contrast, quantum computing remains principally hypothesis-generating until fault tolerance and reproducible advantage are established. Device-based modalities—including transcranial photobiomodulation for neuropsychiatric indications, focused ultrasound enabling CNS drug delivery, and home-supervised neuromodulation—are already reshaping therapeutic landscapes and clinical trial design. For drug discovery, the central requirement is not quantum novelty but validated decision impact, demonstrated under controlled benchmarks aligned with reproducibility expectations comparable to those evolving for AI/ML-driven methods in regulated contexts.
Keywords: quantum computing, quantum sensing, drug discovery, quantum chemistry, error mitigation, photobiomodulation, focused ultrasound, neuromodulation, optogenetics, regulatory science
Introduction: What “Quantum” Means in a Translational Pipeline
Introduction: What “Quantum” Means in a Translational Pipeline (Revised with Absorbed Citations)
Drug discovery is constrained by multi-scale complexity: electronic structure governs bonding and reactivity; molecular interactions emerge from ensembles and solvent; and organism-level outcomes reflect physiology, immune function, and patient heterogeneity. Classical methods such as DFT, post-HF approaches, molecular dynamics, and ML are powerful but face scaling limits and systematic errors for certain phenomena.1,2 Quantum technologies are compelling because molecular systems are quantum mechanical, and thus (in principle) quantum computers can represent and evolve states that are intractable for classical devices.3,4
However, translational claims must pass three independent gates. The first gate is physics validity, requiring that the computational or sensing method correctly encodes the relevant quantum mechanical model for the system under study—this encompasses appropriate treatment of electron correlation, spin-orbit coupling, relativistic effects where relevant, and proper boundary conditions for the simulation domain. The second gate is computational feasibility, demanding that the hardware-software stack can deliver reliable, reproducible results at the scale required for pharmaceutical decision-making; for quantum computing, this criterion encompasses qubit count, coherence times, gate fidelities, error correction or mitigation overhead, and the practical runtime required to achieve meaningful precision.5–8 The third gate is biological relevance, the requirement that the computed or measured quantity demonstrably changes experimental decisions and ultimately improves clinical outcomes—this final criterion is frequently underappreciated, as even exact electronic energies may not translate to better therapeutic candidates when binding affinity is predominantly governed by solvation effects, conformational entropy, and cellular context rather than gas-phase electronic structure.
Failures often arise when novelty is mistaken for relevance. For example, even perfect electronic energies may not translate to better clinical candidates when binding is governed by solvation, conformational entropy, and cellular context; likewise, quantum ML models must outperform well-tuned classical deep learning baselines under fair data splits and compute budgets.9–11 Error-mitigation strategies, while essential for extracting meaningful results from current hardware, introduce limitations regarding bias and reproducibility that must be rigorously characterized.12–14
This review, therefore, treats quantum computing, sensing, and quantum nanotechnologies as distinct readiness tracks. It then deliberately broadens the scope to non-molecular therapeutics and device-led modalities that are already clinically deployed and increasingly intersect with drug development programs: PBM/NIR,15–17 focused ultrasound for BBB opening and delivery enhancement,18–20 neuromodulation devices such as tDCS/TMS,21–24 and optogenetic therapies.25,26 Quantum sensing represents the most clinically.
Terminology: The following are the most used terminologies in the experimental work related to the subject:
DFT — Density Functional Theory is a computational quantum mechanical modeling method used to investigate the electronic structure of many-body systems, particularly atoms, molecules, and condensed phases. In pharmaceutical development, DFT serves as a foundational tool for calculating molecular properties, including electron density distributions, binding energies, molecular orbital configurations, and reaction pathways. It enables researchers to predict how drug molecules interact with biological targets at the electronic level, estimate the thermodynamic stability of polymorphic drug forms, and evaluate the energetic favorability of ligand–receptor binding poses. DFT approximates the many-electron Schrödinger equation using functionals of the electron density rather than many-body wavefunctions, making it computationally more tractable than full configuration interaction methods while retaining quantum-mechanical rigor sufficient for most pharmacologically relevant molecular systems. Its limitations include challenges in accurately capturing long-range dispersion interactions, strongly correlated electron systems, and the conformational flexibility inherent in large biomolecular complexes, which has motivated the exploration of quantum computing approaches that might eventually surpass DFT accuracy for these specific problem classes.
NISQ — Noisy Intermediate-Scale Quantum refers to the current generation of quantum computing hardware, a term coined by John Preskill in 2018, characterizing devices that contain approximately 50 to several hundred qubits but lack full quantum error correction capabilities. In the pharmaceutical context, NISQ devices represent both the promise and the principal limitation of quantum computing for drug discovery: while they can in principle execute quantum algorithms for molecular simulation, their susceptibility to decoherence, gate errors, crosstalk between qubits, and limited qubit connectivity means that the results they produce for pharmacologically relevant molecular systems frequently fail to surpass the accuracy achievable by well-established classical computational chemistry methods such as DFT or coupled cluster calculations. The NISQ era therefore represents a transitional phase in which proof-of-concept demonstrations on small molecular systems are feasible, but the reliable simulation of drug–target interactions involving hundreds of atoms with quantum chemical accuracy remains beyond practical reach, necessitating continued development of error mitigation strategies, hardware improvements in qubit coherence times, and hybrid quantum–classical algorithmic frameworks before quantum computing can deliver validated translational impact in pharmaceutical pipelines.
VQE — Variational Quantum Eigensolver is a hybrid quantum–classical algorithm specifically designed to operate within the constraints of NISQ-era quantum hardware for the purpose of estimating the ground-state energy of molecular systems. In pharmaceutical applications, VQE is considered one of the most promising near-term quantum algorithms for drug discovery because it combines quantum state preparation and measurement on quantum hardware with classical optimization routines that iteratively minimize a cost function corresponding to the expectation value of the molecular Hamiltonian. The algorithm prepares a parameterized quantum circuit (ansatz) representing a trial molecular wavefunction, measures the energy expectation value on the quantum processor, and then uses a classical optimizer to adjust the circuit parameters until convergence toward the ground-state energy is achieved. For drug discovery, VQE has been applied in proof-of-concept studies to calculate molecular energies of small pharmacophores, evaluate binding affinities, and explore potential energy surfaces relevant to reaction mechanisms in enzymatic catalysis. However, VQE faces significant practical challenges including the barren plateau problem in parameter optimization landscapes, sensitivity to quantum noise that introduces systematic errors in energy estimates, difficulty in constructing chemically accurate property for large molecular systems, and the exponential scaling of measurements required to achieve chemical accuracy for molecules of pharmaceutical relevance, all of which currently prevent VQE from delivering predictions that consistently outperform classical methods for real-world drug design applications.
NV — Nitrogen-Vacancy centers are atomic-scale point defects in diamond crystal lattices where a nitrogen atom substitutes for a carbon atom adjacent to a vacant lattice site. In the context of quantum sensing for pharmaceutical applications, NV centers possess remarkable quantum mechanical properties: their electron spin states can be optically initialized, coherently manipulated, and read out at room temperature, making them uniquely suited as nanoscale quantum sensors for detecting magnetic fields, electric fields, temperature variations, and strain with extraordinary sensitivity and spatial resolution. For pharmaceutical development and biomedical applications, NV center magnetometry enables the detection of single-molecule nuclear magnetic resonance signals, the mapping of intracellular magnetic fields generated by biological processes, and the identification of trace paramagnetic biomarkers at concentrations far below the detection limits of conventional analytical instruments. NV-based quantum sensing platforms are being explored for applications including real-time monitoring of drug–target binding events at the single-molecule level, high-resolution imaging of neural activity for neuropharmacological research, and quality control of pharmaceutical nanomaterials through precise characterization of their magnetic and electronic properties, positioning NV center technology as one of the quantum sensing modalities closest to practical clinical and industrial deployment.
PBM — Photobiomodulation is a therapeutic modality based on the quantum mechanical interaction between photons and biological chromophores, particularly cytochrome c oxidase in the mitochondrial electron transport chain. PBM involves the application of low-level laser or light-emitting diode irradiation, typically in the red (630–660 nm) and near-infrared (810–850 nm) wavelength ranges, to stimulate cellular metabolic processes through photon absorption events that are fundamentally governed by quantum mechanical selection rules, electronic transition probabilities, and vibronic coupling mechanisms. At the molecular level, photon absorption by cytochrome c oxidase dissociates inhibitory nitric oxide from the enzyme’s binuclear center, restores electron flow through the respiratory chain, enhances adenosine triphosphate production, modulates reactive oxygen species signaling, and activates downstream transcription factors including nuclear factor kappa-B and activator protein-1. In pharmaceutical and clinical contexts, PBM is already being deployed as an adjunctive or standalone therapy for wound healing, neurological disorders including traumatic brain injury and neurodegenerative diseases, musculoskeletal pain conditions, dermatological pathologies, and postoperative recovery, with a growing body of randomized controlled trial evidence supporting its efficacy and an expanding regulatory footprint that is reshaping clinical endpoint definitions for these therapeutic categories.
FUS — Focused Ultrasound in the context of this review specifically refers to focused ultrasound-mediated blood–brain barrier (BBB) opening, a technique that exploits the mechanical and thermal effects of acoustically driven microbubble oscillations to transiently and reversibly disrupt the tight junction integrity of the cerebrovascular endothelium. While the macroscopic physics of ultrasound propagation is classical, the molecular mechanisms underlying FUS BBB opening involve quantum-scale interactions including the mechanic transduction signaling cascades triggered by cavitation-induced membrane deformation, the conformational dynamics of tight junction proteins such as claudins, occludins, and zonula occludens under mechanical stress, and the activation energy barriers governing paracellular transport pathway opening, all of which are ultimately governed by quantum mechanical potential energy surfaces and intermolecular force fields. For pharmaceutical development, FUS BBB opening represents a transformative enabling technology because it addresses one of the most persistent challenges in central nervous system drug delivery: the inability of approximately 98% of small-molecule therapeutics and virtually all large-molecule biologics to cross the intact blood–brain barrier at pharmacologically effective concentrations. Clinical trials are now evaluating FUS BBB opening in combination with chemotherapeutic agents for glioblastoma, monoclonal antibodies for Alzheimer’s disease amyloid clearance, and gene therapy vectors for neurogenetic disorders, establishing new regulatory paradigms for device-drug combination products and redefining clinical endpoints for CNS therapeutic efficacy.
tDCS/TMS — Transcranial Direct Current Stimulation/Transcranial Magnetic Stimulation are non-invasive neuromodulation techniques that alter neuronal excitability and synaptic plasticity by applying weak electrical currents (tDCS) or time-varying magnetic fields (TMS) to specific cortical regions through the intact skull. The fundamental physics underlying both modalities is rooted in quantum mechanical principles: tDCS operates by shifting neuronal resting membrane potentials through externally applied electric fields that alter the quantum mechanical ion channel gating probability distributions governing sodium, potassium, and calcium conductance, while TMS employs electromagnetic induction to generate eddy currents in cortical tissue that depolarize or hyperpolarize neurons according to the spatial and temporal characteristics of the induced electric field, with the underlying ion channel dynamics, neurotransmitter release probabilities, and synaptic vesicle fusion events all governed by quantum tunneling, barrier crossing, and stochastic quantum thermodynamic processes. In pharmaceutical contexts, tDCS and TMS are reshaping therapeutic paradigms for major depressive disorder, treatment-resistant depression, chronic pain syndromes, post-stroke rehabilitation, and substance use disorders, with TMS having already received FDA clearance for several indications and tDCS advancing through pivotal clinical trials, together establishing regulatory precedents for how non-pharmacological, physics-based neuromodulation interventions are evaluated for safety and efficacy alongside conventional drug therapies.
Quantum Foundations and the “Biological Relevance” Constraint
Molecular modeling rests on the Schrödinger equation for interacting electrons and nuclei. Exact solutions are exponentially complex, motivating approximations such as DFT and coupled-cluster approaches.2,27 Quantum computing’s promise is the potential to represent many-body states more naturally than classical bitstrings.3
Yet biological environments are warm, wet, and noisy. Quantum coherence typically decays rapidly in such conditions, limiting functionally relevant quantum effects in vivo to specific mechanistic niches (eg, tunneling in enzymes) rather than long-lived coherent computation.28,29 Thus, even if quantum computing becomes practical for molecular simulation, the dominant translational challenge remains mapping computed molecular quantities into experimentally validated decision-making.
Quantum Computing Architectures and Realistic Capabilities
Gate-Based Quantum Computing and the NISQ Constraint
Today’s gate-based processors operate in the NISQ regime, characterized by limited qubit counts, high noise floors, short coherence times, and error accumulation that scales with circuit depth.5 Hybrid variational algorithms partially mitigate these limitations by offloading work to classical optimizers, thereby reducing the quantum circuit depth required.7,8,30 Although such methods have produced proof-of-concept electronic-structure calculations, the results typically exhibit wide error bars and are highly sensitive to the choice of ansatz and to device noise. For drug discovery, this means that NISQ variational workflows cannot yet deliver the consistent, chemically accurate energetics needed to rank drug candidates or predict binding affinities with confidence.
Quantum Annealing and the Optimization Framing
Quantum annealers solve problems cast as Ising or QUBO models and are therefore a natural fit for combinatorial optimization.31,32 However, many drug-discovery tasks—such as molecular docking, conformer generation, and chemical-library design—are inherently continuous and high-dimensional. Discretizing these problems to match the annealer’s binary framework introduces substantial mapping overhead that can dominate runtime and erode solution fidelity. Moreover, rigorous benchmarks remain scarce; without fair head-to-head comparisons against state-of-the-art classical heuristics, claims of quantum advantage in these applications remain premature.
The Fault-Tolerance Gap
Achieving chemical accuracy for drug-relevant molecules almost certainly requires fault-tolerant quantum hardware with many logical qubits.6,33,34 Recent resource-estimation studies reinforce this view, showing that simulating even moderately sized enzymatically active sites or protein–ligand complexes demands error-corrected architectures far beyond current capability.35 This gap between present-day devices and the hardware needed for industrially meaningful molecular simulation represents the central bottleneck for quantum-enabled drug discovery and underscores why near-term claims of practical impact should be evaluated with caution36(Table 1).
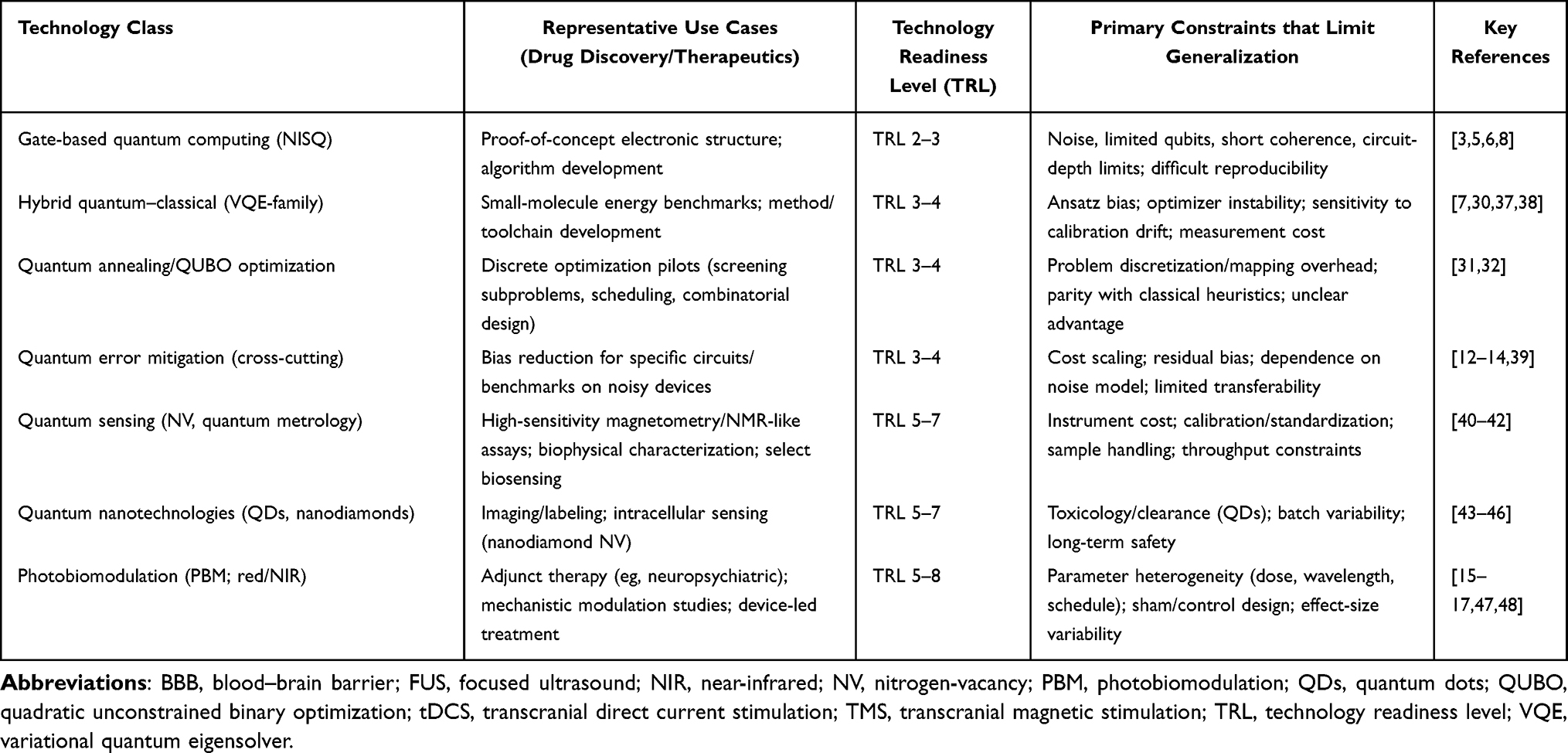 |
Table 1 Readiness of Quantum and Device/Physical Technologies Relevant to Drug Discovery and Therapeutics |
Quantum Computing for Chemistry: What Is Realistically “Actionable” in Drug Discovery?
Electronic Structure: Where QC Could Matter Most
Drug discovery applications where quantum computing could provide a meaningful impact include three principal domains. First, accurate calculation of reaction energetics is essential for computational synthetic route planning, where transition-state barriers and intermediate stabilities determine which synthetic pathways are feasible; quantum computers could provide more reliable barrier heights for reactions involving radical intermediates, organometallic catalysts, or multistep mechanisms, where density functional approximations exhibit systematic errors. Second, redox chemistry and photophysics directly relevant to drug toxicity assessment require accurate treatment of open-shell electronic configurations and excited-state manifolds—predictions of reactive metabolite formation, phototoxicity potential, and redox cycling behavior depend on electronic structure accuracy that often exceeds DFT capabilities for these challenging systems. Third, strongly correlated systems, particularly metalloenzyme active sites containing transition metals with near-degenerate electronic configurations, present fundamental challenges for single-reference quantum chemistry methods; quantum computers’ native ability to represent multi-configurational wavefunctions could address these systems without the exponential classical cost of full configuration interaction approaches.
However, the gap between toy systems and drug-like molecules remains large.3,6,33 Classical DFT and semi-empirical approaches already support many medicinal chemistry decisions at low cost.1,2 Therefore, a stringent benchmark for quantum advantage must compare against best-in-class classical methods on realistic tasks.
VQE and Hybrid Algorithms: Promise and Pitfalls
VQE demonstrates how hybrid workflows can approximate ground-state energies with short circuits.30,37,38,49 Yet results can be sensitive to the ansatz choice and the behavior of the classical optimizer; noisy hardware can bias gradients and lead to false convergence. These issues motivate error mitigation and robust benchmarking.12,13
Error Mitigation: Essential, but Not a Substitute for Fault Tolerance
Error mitigation strategies—randomized compilation, reference-state approaches, learned corrections—can improve NISQ outputs in narrow regimes.13,14,39,50 But mitigation often increases measurement cost and can introduce bias that is difficult to quantify without ground truth. For regulated contexts, bias and reproducibility matter as much as point accuracy (Figure 1 and Table 2).
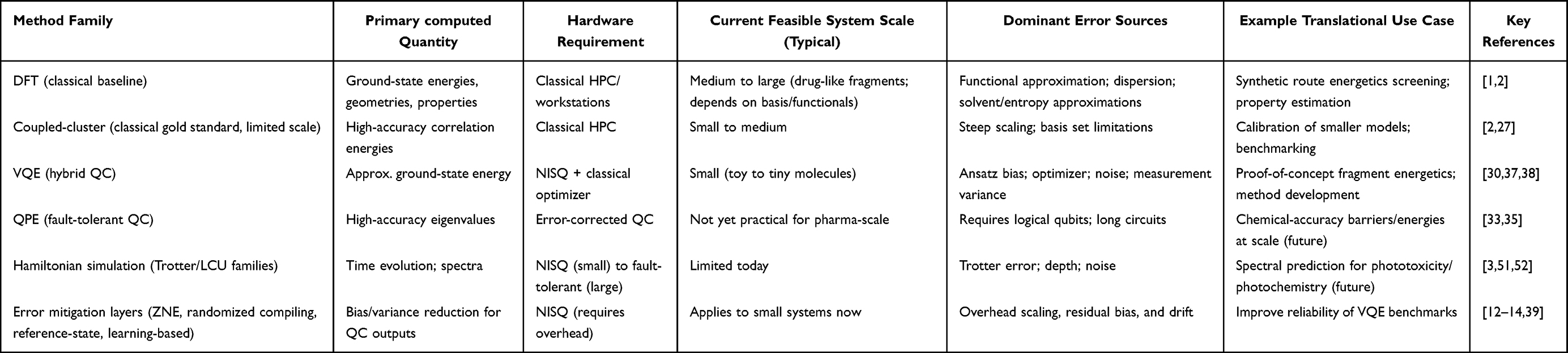 |
Table 2 Quantum Chemistry and Simulation Methods: Target Quantities, Feasibility, and Translational Relevance |
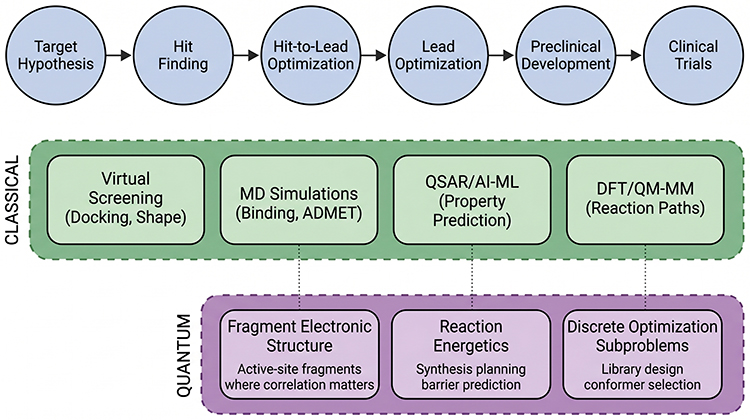 |
Figure 1 Integration map of quantum computing into modern drug discovery. Classical computational chemistry (DFT/MD) and AI/ML models remain primary decision engines. Quantum computing insertion points are restricted to specific subproblems where electronic structure or discrete optimization dominates and where validated benchmarks exist. (Created in BioRender. Niazi, S. (2026) https://BioRender.com/dokynk4). |
The Figure 1 emphasizes that near-term quantum methods are adjunct modules feeding into iterative experimental validation rather than stand-alone design engines.2,3,5,6
Quantum Optimization and Annealing: Docking and Design Claims Under Strict Controls
Optimization appears broadly applicable—docking, conformer selection, multi-objective lead optimization—yet stringent evaluation frequently shows that the mapping to discrete formulations dominates complexity.31,32 Docking is often not purely combinatorial: scoring functions are approximate, and success depends on protein flexibility and solvent factors poorly captured by simplistic discrete encodings (Table 3).
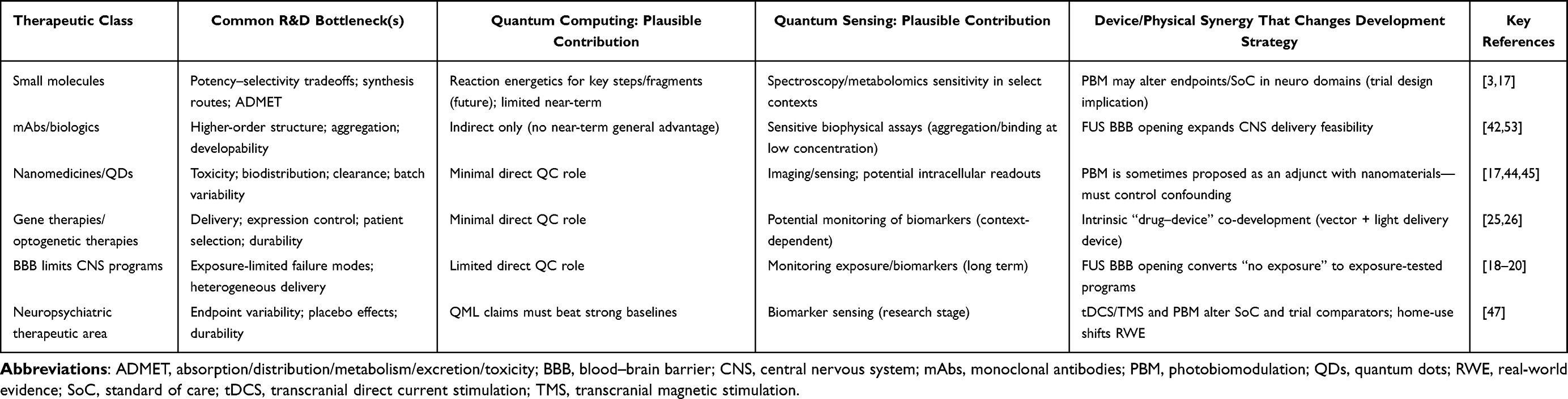 |
Table 3 Therapeutic Modality Mapping: Where Quantum Technologies and Device/Physical Platforms Intersect Drug Development |
A robust quantum advantage claim, therefore, requires:
- a defined task and success metric (eg, enrichment, pose RMSD, prospective hit rate),
- matched compute budgets,
- strong baselines (state-of-the-art classical methods),
- and either prospective experimental validation or blinded benchmarks.
Quantum Machine Learning: The Imperative for Rigorous Benchmarking
QML proposes leveraging quantum feature spaces/kernels or quantum neural networks for classification/regression tasks.54 Yet multiple studies emphasize that data encoding, noise, and limited circuit depth can erase theoretical gains.9,55 A stringent view treats QML as a hypothesis: it must outperform well-tuned classical deep learning baselines under matched conditions.10,11
Key pitfalls that undermine QML advantage claims fall into three categories. Dataset leakage and non-independent train/test splits represent pervasive problems in molecular machine learning, where structural similarity between training and test molecules can artificially inflate apparent model performance; temporal splits, scaffold-based splits, or external validation on entirely separate chemical series provide more honest performance estimates. The absence of robust classical baselines constitutes another critical failure mode, as QML comparisons against shallow classifiers or minimally tuned feed-forward networks systematically overestimate quantum advantage—appropriate comparators include well-optimized graph neural networks, message-passing architectures, and modern transformer models that represent current best practice in molecular property prediction. Finally, parameter and compute budget asymmetries distort comparisons when small QML models with limited expressivity are evaluated against classical models with orders of magnitude more parameters and training compute, creating misleading impressions of efficiency rather than fundamental algorithmic advantage56 (Table 4).
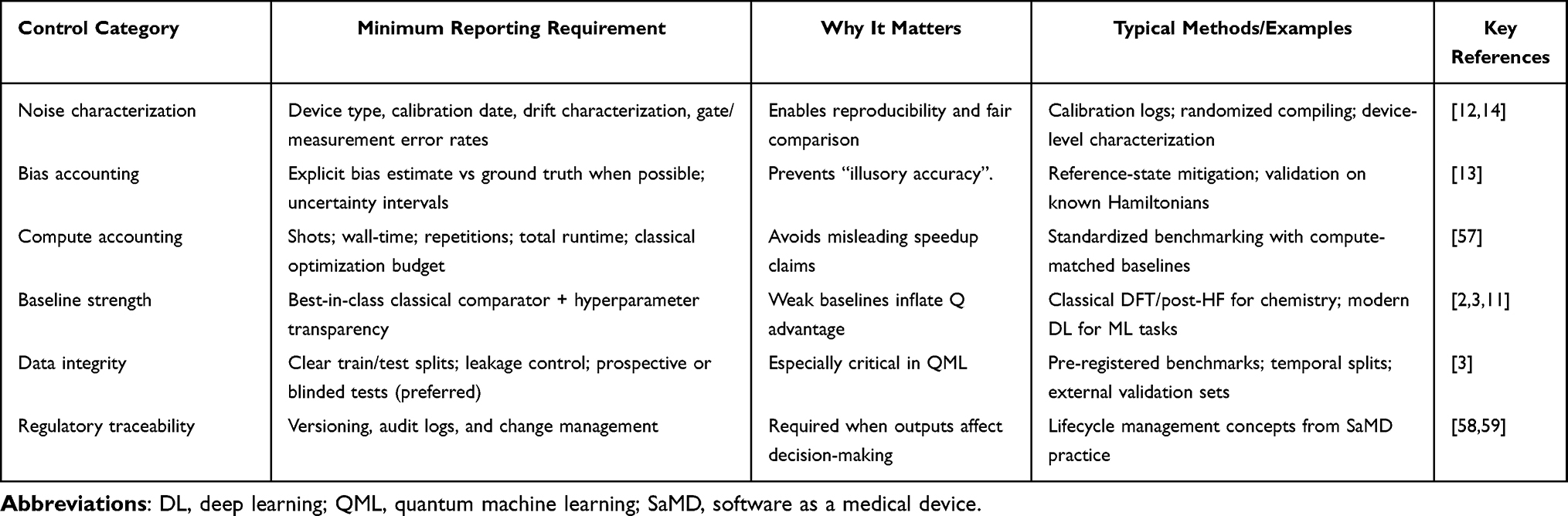 |
Table 4 Error-Mitigation and Benchmarking Controls Required for Credible Quantum Claims in Drug Discovery |
Benchmarking-centered analyses and critiques are therefore essential for any claim of advantage.60–62
Quantum Sensing: The Most Clinically Proximate Quantum Technology
Quantum sensing is arguably the most mature component of “quantum in biomedicine”. Reviews describe quantum sensors’ ability to measure magnetic/electric fields and resonance phenomena with high sensitivity.40,42,63,64 Nitrogen-vacancy (NV) centers in diamond enable nanoscale magnetometry and have motivated excitement about NMR-like sensing at small volumes and low concentrations.41,43,53,65
For drug development, the near-term utility of quantum sensing lies not in replacing established structural biology methods but in enabling capabilities that address specific sensitivity limitations in current workflows. Sensitive detection of binding and aggregation phenomena at concentrations below conventional assay thresholds opens the possibility of characterizing weak protein-ligand interactions, early-stage aggregation events in biologic formulations, and conformational dynamics that influence developability—measurements that may currently require impractical sample quantities or lengthy acquisition times. Improved assay sensitivity for scarce biological samples addresses practical constraints on patient-derived material availability, enabling pharmacokinetic measurements, biomarker detection, and target engagement assessment with reduced sample requirements, thereby expanding clinical pharmacology capabilities. Novel biosensing modalities based on quantum sensors’ unique measurement principles—including label-free detection via magnetic or electric-field perturbations—could eventually complement existing techniques by providing orthogonal readout mechanisms that convey distinct information about molecular interactions. However, scaling these laboratory demonstrations to pharmaceutical workflow integration, achieving robustness across diverse sample matrices and operators, and reducing instrument cost to levels compatible with routine deployment remain substantial practical barriers that temper near-term expectations. Scaling, robustness, and cost remain practical barriers66(Figure 2). NV-diamond and related quantum sensors offer sensitivity advantages for selected assays, with potential relevance from discovery biophysics to clinical monitoring, contingent on robustness, standardization, and cost.40–43,53
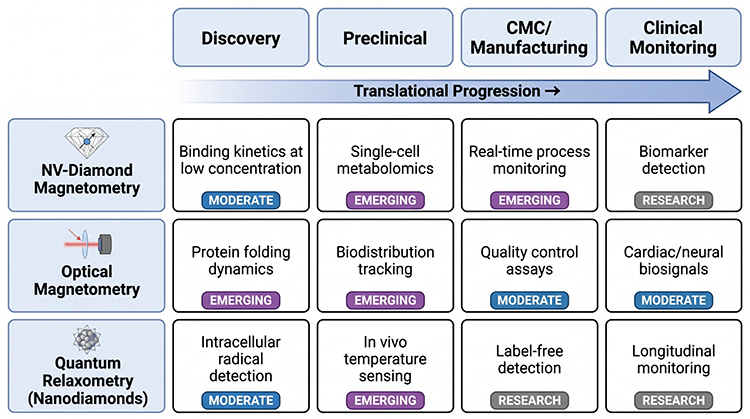 |
Figure 2 Quantum sensing across the translational continuum. Quantum sensing is positioned as a measurement enhancer rather than a computational replacement. (Created in BioRender. Niazi, S. (2026) https://BioRender.com/dokynk4). |
Quantum Nanotechnologies: Quantum Dots and Nanodiamonds as Practical Biomedical Tools
Quantum dots (QDs) and related nanomaterials have a long record in imaging and labeling; their quantum behavior is exploited for tunable optical properties rather than fragile coherence. The core translational issues are toxicity, biodistribution, and long-term clearance.44,45,67 Nanodiamonds with NV centers span both sensing and nano-bio use cases and are central in biomedical quantum sensing discussions.43,46,68,69
Physical Therapies and Devices as “Therapeutics”: PBM/NIR, FUS, tDCS/TMS, Optogenetics
Drug discovery increasingly intersects with devices and physical therapies through combination approaches, shared endpoints (eg, neuropsychiatric outcomes), and co-development strategies.
Photobiomodulation (PBM)/Near-Infrared Light
PBM employs red and near-infrared (NIR) light to modulate biological function through mechanisms linked to mitochondrial cytochrome c oxidase activity, as well as broader immunomodulatory and neurovascular pathways.15,17,70–75 Although clinical evidence remains heterogeneous owing to wide variation in treatment parameters—wavelength, irradiance, dose, and schedule—recent systematic reviews and randomized trials have substantially expanded neuropsychiatric interest, particularly in the treatment of depression.16,47,48,76–78
From a stringent translational perspective, PBM’s relevance to drug discovery operates along three axes. First, PBM functions as a stand-alone or adjunct therapeutic modality capable of altering clinical landscapes and redefining efficacy endpoints against which investigational drugs are measured.79,80 Second, PBM exposure in patient populations represents a potential confounder or effect modifier in clinical trials evaluating behavioral and neurological outcomes, necessitating prospective ascertainment and stratification. Third, PBM may serve as a synergistic platform for certain drug classes—particularly those targeting neuroinflammatory cascades—requiring carefully designed factorial or adaptive trial architectures to disentangle combinatorial effects.
Implication for Pharmaceutical R&D
The maturation of PBM as a clinical intervention compels drug developers to account for it as a co-intervention variable in CNS trial design, reassess comparator arms and endpoint sensitivity in indications where PBM demonstrates efficacy, and explore intentional drug–device combination strategies that may unlock therapeutic enhancements inaccessible to either modality alone.
Focused Ultrasound (FUS) and Blood–Brain Barrier Opening
Focused ultrasound in combination with systemically administered microbubbles can transiently and reversibly open the blood–brain barrier (BBB), thereby enhancing delivery of large-molecule therapeutics to the central nervous system.81–85 The landmark New England Journal of Medicine trial combining FUS-mediated BBB opening with aducanumab represents a direct clinical demonstration of this delivery-enhancement paradigm.18,86,87 Comprehensive reviews have catalogued the growing body of clinical studies and delineated the safety-monitoring requirements essential for regulatory acceptance of this approach.19,88–92 From a translational standpoint, FUS fundamentally expands the feasible target space for CNS therapeutics by enabling brain penetration of biologics, antibodies, and gene therapies that were previously excluded on pharmacokinetic grounds. Critically, FUS also provides a rational basis for re-evaluating prior clinical failures: compounds that demonstrated target engagement deficits attributable to inadequate CNS exposure rather than target invalidity may warrant reassessment under FUS-assisted delivery conditions.
Implication for Pharmaceutical R&D
FUS-mediated BBB opening has the potential to reshape CNS drug development portfolios by converting previously undruggable intracranial targets into tractable opportunities, justifying the systematic re-examination of shelved CNS candidates for exposure-limited failure, and establishing a new regulatory and clinical paradigm in which drug–device co-development becomes integral to CNS therapeutic strategy.
Neuromodulation Devices: TDCS and TMS
Noninvasive neuromodulation has matured into an established therapeutic space with evolving protocols and evidence bases.22–24,93,94 Home-based or remotely supervised paradigms further expand real-world deployment.21 From a development standpoint, device therapeutics can compete with, complement, or alter the standard of care against which drugs are benchmarked, and they motivate hybrid trial designs in which devices and drugs interact.
Optogenetic Therapies
Optogenetics has made the most convincing clinical translation in retinal diseases, including landmark demonstrations of partial recovery of visual function26,95 and recent clinical reports on optogenetic therapy candidates.25 These programs are inherently combination-like (vector + device/light delivery), and thus directly relevant to regulatory frameworks for complex therapeutic systems (Table 5).
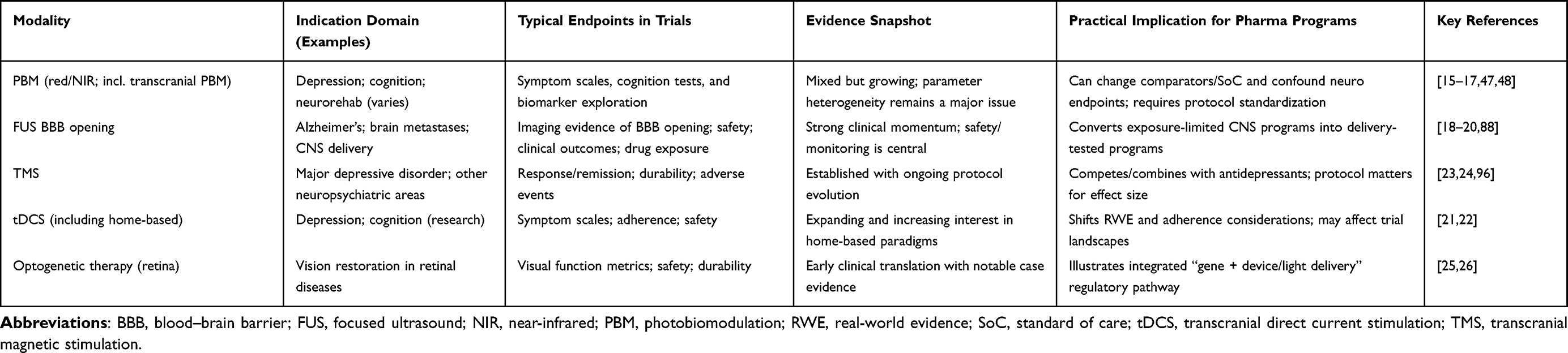 |
Table 5 Device and Physical Therapeutics: Evidence, Endpoints, and Implications for Pharma Development |
Validation, Reproducibility, and Regulatory Expectations
For any quantum-enabled workflow to influence regulated decisions, it must be reproducible, auditable, and benchmarked. This is conceptually aligned with how regulators view AI/ML tools in medical devices and software-as-a-medical-device contexts: lifecycle management, performance monitoring, and transparency.58,59
For device therapeutics (PBM, FUS, tDCS/TMS), the evidentiary requirements are inherently clinical and safety-oriented, with substantial emphasis on real-world performance and protocol standardization. Public regulatory records (eg, FDA device documentation) can serve as anchors for stringent review narratives where appropriate97,98 (Table 6 and Figure 3).
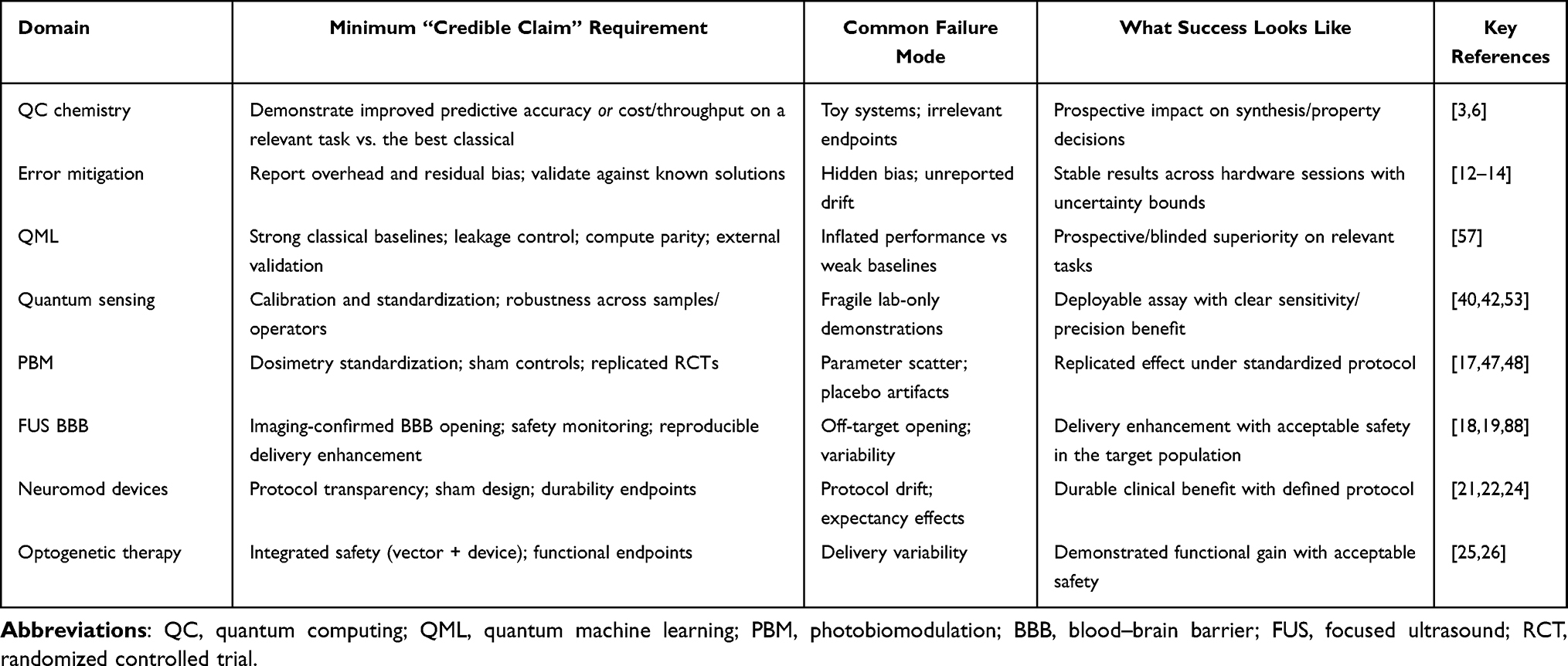 |
Table 6 Practical Translational Benchmark Checklist for Quantum-Enabled and Device-Enabled Claims |
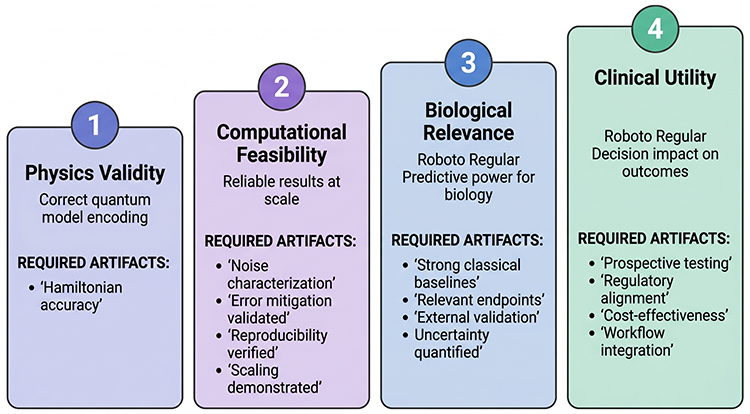 |
Figure 3 Evidence ladders for quantum-enabled translational claims. |
Figure 3 formalizes that progress in quantum method sophistication does not guarantee biological relevance or clinical utility; each step requires distinct validation artifacts and controls.5,9,11,58,59
Where the Field is Likely to Deliver Value in the Next 0–5 years
A stringent reading of the current evidence suggests three distinct trajectories over the next five years. Quantum sensing will continue producing practical gains in contexts where measurement sensitivity represents the limiting factor, with the most likely near-term pharmaceutical impact occurring in biophysical characterization workflows where quantum-enhanced detection enables measurements currently inaccessible or impractical with conventional instrumentation; applications in binding assay sensitivity, aggregation monitoring, and potentially diagnostic biosensing represent the most credible near-term translation pathways.40,42,53,99 Device-based and physical therapeutic modalities will increasingly reshape treatment landscapes and consequently affect pharmaceutical development strategy through multiple mechanisms: photobiomodulation trials in neuropsychiatric domains continue expanding with particular momentum in depression and cognitive endpoints,47,48,100 focused ultrasound blood-brain barrier opening strategies are creating new delivery paradigms for CNS therapeutics previously limited by exposure constraints,18 and home-use neuromodulation with remote supervision is shifting real-world evidence generation and comparator landscapes in ways that pharmaceutical developers must incorporate into trial design.21 Quantum computing, in contrast to both quantum sensing and device therapeutics, will remain largely pre-competitive and hypothesis-generating for pharmaceutical applications, with translational impact constrained until reproducible computational advantage is demonstrated against best-available classical methods on molecular systems and tasks directly relevant to drug discovery decisions—a milestone that current hardware and algorithmic capabilities have not yet achieved for industrially meaningful problems (Figure 4). Quantum sensing and device therapeutics show present-day clinical adjacency, whereas the fault-tolerance gap and benchmarking requirements constrain quantum computing’s impact on medicinal chemistry.5,6,18,21,40
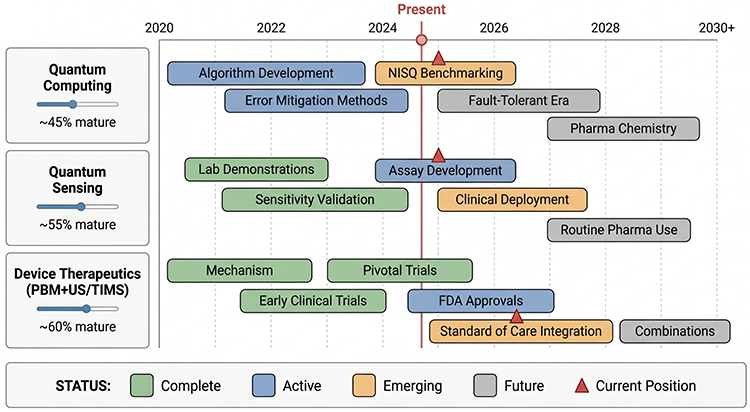 |
Figure 4 Roadmap of maturity by modality. (Created in BioRender. Niazi, S. (2026) https://BioRender.com/dokynk4). |
Conclusions
In summary, this review has examined the emerging landscape of quantum science applications across pharmaceutical development, spanning quantum computing, quantum sensing, quantum nanotechnology, and device-based physical therapies grounded in quantum mechanical principles. The central thesis that emerges from this analysis is that these diverse quantum technologies should not be conflated into a single narrative of readiness but rather evaluated as separate maturity tracks, each requiring distinct regulatory frameworks, validation methodologies, and translational timelines. Quantum computing, while scientifically compelling in its potential to simulate molecular interactions, protein–ligand binding, and electronic structure calculations beyond the reach of classical hardware, remains translationally early; current noisy intermediate-scale quantum (NISQ) devices lack the error correction, qubit coherence, and gate fidelity required to deliver reproducible, pharmacologically actionable predictions that surpass classical computational chemistry benchmarks. In contrast, quantum sensing technologies, including nitrogen-vacancy center magnetometry, quantum dot–based diagnostic platforms, and entangled-photon imaging modalities, are considerably closer to clinical deployment, with demonstrated proof-of-concept applications in high-sensitivity biomarker detection, subcellular resolution imaging, and real-time pharmacokinetic monitoring that address tangible unmet needs in precision medicine. Similarly, specific quantum nanotechnologies, particularly quantum dot theragnostic conjugates and quantum-confined nanostructures engineered for targeted drug delivery, have progressed through preclinical validation and are approaching first-in-human clinical trials. Meanwhile, device-based and physical therapies rooted in quantum mechanical energy transfer, including photobiomodulation (PBM), focused ultrasound blood–brain barrier opening (FUS BBB), transcranial direct current stimulation and transcranial magnetic stimulation (tDCS/TMS), and optogenetics, are already actively reshaping therapeutic categories, redefining clinical endpoints, and generating regulatory precedents that will likely inform how future quantum-enabled interventions are evaluated. For drug discovery specifically, the central requirement that this review underscores is not quantum novelty per se but rather validated decision impact: any quantum-derived computational method, sensing platform, or nanoscale intervention must demonstrate, under controlled and reproducible benchmarks, that it materially improves target identification accuracy, lead optimization efficiency, toxicity prediction, or clinical outcome prediction relative to existing best-in-class approaches, and this demonstration must align with the reproducibility, transparency, and documentation expectations that are now evolving for AI/ML-driven methods in regulated contexts, as articulated in recent FDA guidance on artificial intelligence in drug development.58,59
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jones RO. Density functional theory: its origins, rise, and future. Rev Mod Phys. 2015;87:897–18. doi:10.1103/RevModPhys.87.897
2. Jensen F. Introduction to Computational Chemistry.
3. Cao Y, Romero J, Olson JP, et al. Quantum chemistry in the age of quantum computing. Chem Rev. 2019;119(19):10856–10915. doi:10.1021/acs.chemrev.8b00803
4. Feynman RP. Simulating physics with computers. Int J Theor Phys. 1982;21:467–488. doi:10.1007/BF02650179
5. Preskill J. Quantum computing in the NISQ era and beyond. Quantum. 2018;2:79. doi:10.22331/q-2018-08-06-79
6. McArdle S, Endo S, Aspuru-Guzik A, Benjamin SC, Yuan X. Quantum computational chemistry. Rev Mod Phys. 2020;92(1):015003. doi:10.1103/RevModPhys.92.015003
7. Cerezo M, Arrasmith A, Babbush R, et al. Variational quantum algorithms. Nat Rev Phys. 2021;3(9):625–644. doi:10.1038/s42254-021-00348-9
8. Bharti K, Cervera-Lierta A, Kyaw TH, et al. Noisy intermediate-scale quantum algorithms. Rev Mod Phys. 2022;94(1):015004. doi:10.1103/RevModPhys.94.015004
9. Huang HY, Broughton M, Mohseni M, Babbush R. Power of data in quantum machine learning. Nat Commun. 2021;12:2631. doi:10.1038/s41467-021-22539-9
10. LeCun Y, Bengio Y, Hinton G. Deep learning. Nature. 2015;521:436–444. doi:10.1038/nature14539
11. Esteva A, Robicquet A, Ramsundar B, et al. A guide to deep learning in healthcare. Nat Med. 2019;25:24–29. doi:10.1038/s41591-018-0316-0
12. Dalton K, Long CK, Yordanov YS, et al. Quantifying the effect of gate errors on variational quantum eigensolvers for quantum chemistry. Npj Quantum Inf. 2024;10:18. doi:10.1038/s41534-024-00808-x
13. Lolur P, Ralli A, Maskara N, Stilck Franca D, Wocjan P. Reference-state error mitigation: a strategy for high accuracy quantum computation of chemistry. J Chem Theory Comput. 2023;19(3):783–795. doi:10.1021/acs.jctc.2c01114
14. Kurita T, Matsumori M, Yamamoto T, Haruna T, Sato S, Emerson J. Synergetic quantum error mitigation by randomized compiling and zero-noise extrapolation for the variational quantum eigensolver. Quantum. 2023;7:1097. doi:10.22331/q-2023-08-29-1097
15. Nairuz T, Lee JH, Lee J-H. Photobiomodulation therapy on brain: pioneering an innovative treatment (mechanisms and applications). Cells. 2024;13(11):966. doi:10.3390/cells13110966
16. Wang L, Mao L, Huang Z, Switzer JA, Hess DC, Zhang Q. Photobiomodulation: shining a light on depression. Theranostics. 2025;15(2):362–383. doi:10.7150/thno.104502
17. Dompe C, Moncrieff L, Matys J, et al. Photobiomodulation--underlying mechanism and clinical applications. Int J Mol Sci. 2020;21(18):6526. doi:10.3390/ijms21186526
18. Rezai AR, Ranjan M, D’Haese PF, et al. Ultrasound blood-brain barrier opening and aducanumab in Alzheimer’s disease. N Engl J Med. 2024;390:55–62. doi:10.1056/NEJMoa2313041
19. Durham PG, Butnariu A, Alghorazi R, Pinton G, Krishna V, Dayton PA. Current clinical investigations of focused ultrasound BBB disruption. Neurotherapeutics. 2024;21(3):e00352. doi:10.1016/j.neurot.2024.e00352
20. Wu CC, Chen CY, Lee CH, et al. Blood-brain barrier opening with neuronavigation-guided focused ultrasound in pediatric patients with diffuse midline glioma. Sci Transl Med. 2025;17:eadq6645. doi:10.1126/scitranslmed.adq6645
21. Woodham RD, Selvaraj S, Lajmi N, et al. Home-based transcranial direct current stimulation treatment for major depressive disorder: a fully remote Phase 2 randomized sham-controlled trial. Nat Med. 2025;31:87–95. doi:10.1038/s41591-024-03305-y
22. Lefaucheur JP, Aleman A, Baeken C, et al. Evidence-based guidelines on the therapeutic use of transcranial direct current stimulation (tDCS). Clin Neurophysiol. 2020;131(1):56–92. doi:10.1016/j.clinph.2016.10.087
23. van Rooij SJH, Brunelin J, Haffen E, Lefaucheur JP, Bennabi D, Ayache SS. Accelerated TMS: state-of-the-art and future directions. Neuropsychopharmacology. 2024;2024:1.
24. Trapp NT, Arbuckle N, Baeken C. Consensus recommendations for rTMS in depression: an international survey. Clin Neurophysiol. 2024;170:206–233. doi:10.1016/j.clinph.2024.12.015
25. Lam BL, Zak V, Gonzalez VH, et al. Safety and efficacy of MCO-010 optogenetic therapy in patients with Stargardt disease in USA (STARLIGHT): an open-label multi-center phase 2 trial. EClinicalMedicine. 2025;87:103430. doi:10.1016/j.eclinm.2025.103430
26. Sahel JA, Boulanger-Scemama E, Pagot C, et al. Partial recovery of visual function in a blind patient after optogenetic therapy. Nat Med. 2021;27:1223–1229. doi:10.1038/s41591-021-01351-4
27. Szabo A, Ostlund NS. Modern Quantum Chemistry: Introduction to Advanced Electronic Structure Theory. Dover Publications; 1996.
28. Tegmark M. Importance of quantum decoherence in brain processes. Phys Rev E. 2000;61:4194–4206. doi:10.1103/PhysRevE.61.4194
29. Kohen A, Klinman JP. Hydrogen tunneling in biology. Chem Biol. 1999;6:R191–R198. doi:10.1016/S1074-5521(99)80058-3
30. McClean JR, Romero J, Babbush R, Aspuru-Guzik A. The theory of variational hybrid quantum-classical algorithms. New J Phys. 2016;18(2):023023. doi:10.1088/1367-2630/18/2/023023
31. Hauke P, Katzgraber HG, Lechner W, Nishimori H, Oliver WD. Perspectives of quantum annealing: methods and implementations. Rep Prog Phys. 2020;83(5):054401. doi:10.1088/1361-6633/ab85b9
32. Lucas A. Ising formulations of many NP problems. Front Phys. 2014;2:5. doi:10.3389/fphy.2014.00005
33. Reiher M, Wiebe N, Svore KM, Wecker D, Troyer M. Elucidating reaction mechanisms on quantum computers. Proc Natl Acad Sci USA. 2017;114(29):7555–7560. doi:10.1073/pnas.1619152114
34. Zhang Y, Lu Y, Zhang M, Yuan X, Wang S. Quantum algorithms for molecular systems: near-term and fault-tolerant outlook. WIREs Comput Mol Sci. 2025. doi:10.1002/wcms.1674
35. Kim IH, Liu YH, Pallister S, Pol W, Roberts S, Lee E. Fault-tolerant resource estimate for quantum chemical simulations: case study on Li-ion battery electrolyte molecules. Phys Rev Res. 2022;4(2):023019. doi:10.1103/PhysRevResearch.4.023019
36. Blunt NS, Camps J, Crawford O, et al. Perspective on the current state-of-the-art of quantum computing for drug discovery applications. J Chem Theory Comput. 2022;18(12):7001–7023. doi:10.1021/acs.jctc.2c00574
37. Peruzzo A, McClean J, Shadbolt P, et al. A variational eigenvalue solver on a photonic quantum processor. Nat Commun. 2014;5:4213. doi:10.1038/ncomms5213
38. Tilly J, Chen H, Cao S, et al. The variational quantum eigensolver: a review of methods and best practices. Phys Rep. 2022;986:1–128. doi:10.1016/j.physrep.2022.08.003
39. Jiang T, Huang C, Kairys P, Boothby K, Girard J, Sundaresan N. Error mitigation in variational quantum eigensolvers using tailored probabilistic error cancellation. Phys Rev Res. 2024;6(3):033069. doi:10.1103/PhysRevResearch.6.033069
40. Degen CL, Reinhard F, Cappellaro P. Quantum sensing. Rev Mod Phys. 2017;89(3):035002. doi:10.1103/RevModPhys.89.035002
41. Barry JF, Turner MJ, Schloss JM, et al. Sensitivity optimization for NV-diamond magnetometry. Rev Mod Phys. 2020;92(1):015004. doi:10.1103/RevModPhys.92.015004
42. Aslam N, Zhou H, Urbach EK, et al. Quantum sensors for biomedical applications. Nat Rev Phys. 2023;5:157–169. doi:10.1038/s42254-023-00558-3
43. Schirhagl R, Chang K, Loretz M, Degen CL. Nitrogen-vacancy centers in diamond: nanoscale sensors for physics and biology. Annu Rev Phys Chem. 2014;65:83–105. doi:10.1146/annurev-physchem-040513-103659
44. Derfus AM, Chan WCW, Bhatia SN. Probing the cytotoxicity of semiconductor quantum dots. Nano Lett. 2004;4(1):11–18. doi:10.1021/nl0347334
45. Medintz IL, Uyeda HT, Goldman ER, Mattoussi H. Quantum dot bioconjugates for imaging, labelling and sensing. Nat Mater. 2005;4:435–446. doi:10.1038/nmat1390
46. Chipaux M, Wrachtrup J. Nanodiamonds and NV centers for biology and nanoscale NMR. J Appl Phys. 2018;123(24):244502. doi:10.1063/1.5029751
47. Ji Q, Li Y, Zhang H, Zhang C, Li R, Zhang Y. Photobiomodulation improves depression symptoms: systematic review/meta-analysis. Front Psychiatry. 2024;15:1365992. doi:10.3389/fpsyt.2024.1365992
48. Guu TW, Cassano P, Li WJ, et al. Wearable, self-administered transcranial photobiomodulation for major depressive disorder and sleep: a randomized, double-blind, sham-controlled trial. J Affect Disord. 2025;372:635–642. doi:10.1016/j.jad.2024.12.065
49. Kumar S, Ghosh K, Lee SC, Yamijala SS. Quantum computing for chemical applications: variational algorithms and beyond. J Indian Inst Sci. 2025. doi:10.1007/s41745-025-00488-2
50. Zou H, Magnusson E, Brunander H, Dobrautz W, Rahm M. Multireference error mitigation for quantum computation of chemistry. Digit Discov. 2025;4:2521–2533. doi:10.1039/D5DD00202H
51. Babbush R, McClean JR, Wecker D, Aspuru-Guzik A, Wiebe N. Chemical basis of Trotter-Suzuki errors in quantum chemistry simulation. Phys Rev A. 2018;91:022311. doi:10.1103/PhysRevA.91.022311
52. Babbush R, Wiebe N, McClean J, McClain J, Neven H, Chan GKL. Low-depth quantum simulation of materials. Phys Rev X. 2018;8(1):011044. doi:10.1103/PhysRevX.8.011044
53. Du J, Kong X, Le Floch JM, Jia Y, Wrachtrup J. Single-molecule scale magnetic resonance spectroscopy using quantum diamond sensors. Rev Mod Phys. 2024;96:025001. doi:10.1103/RevModPhys.96.025001
54. Biamonte J, Wittek P, Pancotti N, Rebentrost P, Wiebe N, Lloyd S. Quantum machine learning. Nature. 2017;549:195–202. doi:10.1038/nature23474
55. Aaronson S. Read the fine print. Nat Phys. 2015;11:291–293. doi:10.1038/nphys3271
56. Gonzalez-Casares M, Arrasmith A, Nicoli MA, et al. Benchmarking QML models: pitfalls, controls, and baselines. Nat Mach Intell. 2024;2024:1.
57. Schnabel J, Roth M. Quantum kernel methods under scrutiny: a benchmarking study. Quantum Mach Intell. 2025;7:58. doi:10.1007/s42484-025-00273-5
58. US Food and Drug Administration. Artificial Intelligence/Machine Learning (AI/ML)-Based Software as a Medical Device (SaMD) Action Plan. FDA; 2021. Available from: https://www.fda.gov/media/145022/download.
59. US Food and Drug Administration. Discussion Paper and Request for Feedback on AI/ML-Based Software as a Medical Device (SaMD). FDA; 2023. Available from: https://www.fda.gov/media/167288/download.
60. Schuld M, Killoran N. Quantum machine learning in feature Hilbert spaces. Phys Rev Lett. 2019;122(4):040504. doi:10.1103/PhysRevLett.122.040504
61. Abbas A, Sutter D, Zoufal C, Lucchi A, Figalli A, Woerner S. The power of quantum neural networks. Nat Comput Sci. 2021;1:403–409. doi:10.1038/s43588-021-00084-1
62. Alvarez-Estevez D. Benchmarking quantum machine learning kernel training for classification tasks. arXiv. 2025. Available from https://arxiv.org/abs/2408.10274.
63. Taylor MA, Bowen WP. Quantum metrology and its application in biology. Phys Rep. 2016;615:1–59. doi:10.1016/j.physrep.2015.12.002
64. Budker D, Romalis M. Optical magnetometry. Nat Phys. 2007;3:227–234. doi:10.1038/nphys566
65. Li Y, Han L, Yi T, Li C, Wei J. A review of the study of diamond NV color centers: fabrication, application and challenge. Funct Diamond. 2025;5(1):2567286. doi:10.1080/26941112.2025.2567286
66. Katsumi R, Wrachtrup J. Recent progress in hybrid diamond photonics for quantum technologies. Adv Photonics Res. 2025. doi:10.1002/adpr.202400255
67. Zrazhevskiy P, Gao X. Quantum dot imaging platform for single-cell molecular profiling. Nat Commun. 2013;4:1619. doi:10.1038/ncomms2635
68. Zhang J, Wrachtrup J. Capturing elusive intracellular bio-signals using NV centers in nanodiamonds. Biosens Bioelectron. 2025;2025:1.
69. Asadi S, Jamali M, Habibi M, Mazlomzadeh S. Nanodiamonds and NV centers in biology: intracellular sensing and imaging. ACS Nano. 2021;15(4):6654–6667. doi:10.1021/acsnano.0c10496
70. Wade ZS, Barrett DW, Gonzalez-Lima F, Nguyen A, Venkat S, Gonzalez-Lima F. PBM duration-of-action on cytochrome c oxidase in brain (histochemical mapping). Front Neurosci. 2023;17:1243527. doi:10.3389/fnins.2023.1243527
71. Yan B, Zhou J, Yan F, et al. Unlocking the potential of photobiomodulation therapy for brain neurovascular coupling: the biological effects and medical applications. J Cereb Blood Flow Metab. 2025;45(5):800–830. doi:10.1177/0271678X241311695
72. Huang Y, Gonzalez-Lima F, Yang C, Xu M, Yuan Z. Recent advances in near-infrared photobiomodulation for neuro/brain applications. J Innov Opt Health Sci. 2025;18(1):2530001. doi:10.1142/S1793545825300012
73. Hamblin MR. Mechanisms and applications of the anti-inflammatory effects of photobiomodulation. AIMS Biophys. 2017;4(3):337–361. doi:10.3934/biophy.2017.3.337
74. Eells JT, Wong-Riley MT, VerHoeve J, et al. Mitochondrial signal transduction in accelerated wound and retinal healing by near-infrared light therapy. Proc SPIE. 2004;5686:294–304. doi:10.1117/12.596831
75. Maghfour J, Ozog DM, Mineroff J, Jagdeo J, Kohli I, Lim HW. Photobiomodulation CME part I: overview and mechanism of action. J Am Acad Dermatol. 2024;91(5):793–802. doi:10.1016/j.jaad.2023.10.073
76. Trofimov AO, Kalinichenko LS, Prazdnova EV, Krupitskii EM, Knyazev NA. Near-infrared light-induced transcranial PBM enhances neural/visual pathways: randomized controlled trial. J Biomed Opt. 2025;30(1):018001. doi:10.1117/1.JBO.30.1.018001
77. Helali H, Samani N, Tabeie F, et al. The effectiveness of transcranial photobiomodulation therapy (tPBM) on reducing anxiety, depression, and opioid craving in patients undergoing methadone maintenance treatment: a double-blind, randomized, controlled trial. BMC Psychiatry. 2025;25:94. doi:10.1186/s12888-025-06555-3
78. Hu S, Li X, Guo B, Xu W, Liu TCY, Hamblin MR. Photobiomodulation as a therapeutic strategy for major depressive disorder: mechanisms and prospects. Photobiomodulation Photomed Laser Surg. 2025;43(1):3–14. doi:10.1089/photob.2024.0040
79. Barrett DW, Gonzalez-Lima F. Transcranial infrared laser stimulation produces beneficial cognitive and emotional effects in humans. Neuroscience. 2013;230:13–23. doi:10.1016/j.neuroscience.2012.11.016
80. Rojas JC, Gonzalez-Lima F, Elson D. Low-level light therapy of the eye and brain. Ann Biomed Eng. 2013;41(1):1–14. doi:10.1007/s10439-012-0634-8
81. Hynynen K, McDannold N, Vykhodtseva N, Jolesz FA. Noninvasive MR-guided focal blood-brain barrier opening in rabbits. Radiology. 2001;220:640–646. doi:10.1148/radiology.220.3.r01se19640
82. Choi JJ, Pernot M, Small SA, Konofagou EE. Transcranial localized blood-brain barrier opening with focused ultrasound in mice. Ultrasound Med Biol. 2007;33:95–104. doi:10.1016/j.ultrasmedbio.2006.07.018
83. Burgess A, Ayala-Grosso CA, Ganguly M, Jordao JF, Aubert I, Hynynen K. Focused ultrasound-mediated blood-brain barrier disruption increases amyloid-beta plaque clearance in an Alzheimer’s disease mouse model. Radiology. 2014;273:736–745. doi:10.1148/radiol.14141114
84. Kinoshita M, McDannold N, Jolesz FA, Hynynen K. Noninvasive localized blood-brain barrier disruption using focused ultrasound. Biochem Biophys Res Commun. 2006;340(3):1085–1090. doi:10.1016/j.bbrc.2005.12.128
85. Meairs S. Facilitation of drug transport across the blood-brain barrier with ultrasound and microbubbles. Pharmaceuticals. 2015;8(3):489–508. doi:10.3390/ph8030489
86. Ye BS, Lee S, Jeon S, et al. Repetitive and extensive FUS-mediated BBB opening in Alzheimer’s disease. J Neurosurg. 2025;142:1263–1270. doi:10.3171/2024.8.JNS24989
87. Jeong J, Gonzalez-Lima F. Aducanumab delivery facilitated by FUS-induced BBB disruption (preclinical). Sci Rep. 2025;2025:1.
88. McMahon D, Poon C, Hynynen K. Evaluating the safety profile of focused ultrasound and microbubbles to increase blood-brain barrier permeability. Expert Opin Drug Deliv. 2019;16:129–142. doi:10.1080/17425247.2019.1567493
89. Meng Y, Pople CB, Suppiah S, et al. MR-guided focused ultrasound enhances delivery of trastuzumab to HER2+ brain metastases. Sci Transl Med. 2021;13(613):eabg6604. doi:10.1126/scitranslmed.abg6604
90. Woodworth GF, Gonzalez-Lima F, Ozair A. Microbubble-enhanced transcranial focused ultrasound enabling BBB opening for localized drug delivery. Lancet Oncol. 2025;26:1651–1664. doi:10.1016/S1470-2045(25)00492-9
91. Grasso G, Torregrossa F, Noto M, et al. MR-guided focused ultrasound-induced blood-brain barrier opening for brain metastasis: a review. Neurosurg Focus. 2023;55(2):E11. doi:10.3171/2023.5.FOCUS23227
92. Li H, Gonzalez-Lima F. Microbubble delivery platforms and safety profiling for FUS-mediated BBB opening. Sci Rep. 2025;2025:1.
93. Brunoni AR, Amadera J, Berbel B, Volz MS, Rizzerio BG, Fregni F. Transcranial direct current stimulation for acute major depressive episodes: meta-analysis of individual patient data. JAMA Psychiatry. 2017;74(6):633–639. doi:10.1001/jamapsychiatry.2017.0596
94. Carpenter LL, Janicak PG, Aaronson ST, et al. Transcranial magnetic stimulation (TMS) for major depression: a multisite, naturalistic, observational study of acute treatment outcomes in clinical practice. Depress Anxiety. 2012;29(7):587–596. doi:10.1002/da.21969
95. Busskamp V, Duebel J, Balya D, et al. Genetic reactivation of cone photoreceptors restores visual responses in retinitis pigmentosa. Science. 2010;329(5990):413–417. doi:10.1126/science.1190897
96. O’Reardon JP, Solvason HB, Janicak PG, et al. Efficacy and safety of transcranial magnetic stimulation in the acute treatment of major depression: a multisite randomized controlled trial. Biol Psychiatry. 2007;62(11):1208–1216. doi:10.1016/j.biopsych.2007.01.018
97. US Food and Drug Administration. Premarket Approval (PMA) Database Entry for Flow FL-100 (P230024). FDA; 2025. Available from: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfPMA/pma.cfm?id=P230024.
98. US Food and Drug Administration. Summary of Safety and Effectiveness Data (SSED) for Flow FL-100. PMA P230024. FDA; 2025. Available from: https://www.accessdata.fda.gov/cdrh_docs/pdf23/P230024B.pdf.
99. Fairbairn R, Sharma O, Forsythe I, Williams O, Green E, Mkwashi A. Emerging applications of quantum sensing technology in healthcare. NIHR Innovation Observatory Report; 2025. Available from: https://io.nihr.ac.uk/wp-content/uploads/2025/03/NIHR-IO-Quantum-Sensing-Technology-Report_Jan-2025.pdf.
100. Blivet G, Touchon J, Meftah S. Brain photobiomodulation as a potential treatment in Alzheimer’s and Parkinson’s diseases. Brain Stimul. 2025;18(1):e9–e10. doi:10.1016/j.brs.2024.12.004
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.