Back to Journals » Clinical and Experimental Gastroenterology » Volume 13
Quantification of Intestinal Lactobacillus Species in Children with Functional Constipation by Quantitative Real-Time PCR
Authors Jomehzadeh N ![]() , Javaherizadeh H, Amin M
, Javaherizadeh H, Amin M ![]() , Rashno M, Teimoori A
, Rashno M, Teimoori A
Received 23 February 2020
Accepted for publication 17 April 2020
Published 5 May 2020 Volume 2020:13 Pages 141—150
DOI https://doi.org/10.2147/CEG.S250755
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Wing-Kin Syn
Nabi Jomehzadeh,1– 3 Hazhir Javaherizadeh,4 Mansour Amin,2,3 Mohammad Rashno,1 Ali Teimoori5
1Cellular and Molecular Research Center, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran; 2Infectious and Tropical Diseases Research Center, Health Research Institute, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran; 3Department of Microbiology, Faculty of Medicine, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran; 4Alimentary Tract Research Center, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Khouzestan, Iran; 5Department of Virology, Faculty of Medicine, Hamedan University of Medical Sciences, Hamedan, Iran
Correspondence: Mansour Amin
Infectious and Tropical Diseases Research Center, Health Research Institute, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
Tel +98 9163061096
Fax +98 61-3333 2036
Email [email protected]
Background: Functional constipation is a common and annoying gastrointestinal disorder among children worldwide in which the intestinal microbiota composition plays a fundamental role. This study aimed to compare the quantity of main intestinal Lactobacillus species in constipated children and healthy controls.
Materials and Methods: Fecal samples were collected from 40 children fulfilling Rome IV criteria for functional constipation and 40 healthy volunteers. Quantitative real-time polymerase chain reaction (qPCR) method with species-specific primers was used to investigate seven main Lactobacillus species in fecal samples.
Results: Lactobacillus strains of the patient group were different from the healthy controls, main differences being noticeable decrease in the population quantity of Lactobacillus reuteri (mean 102.61 CFU/gram feces) and lower abundance of Lactobacillus fermentum (p< 0.0001).
Conclusion: Lactobacillus species might be quantitatively altered in childhood functional constipation. Our findings on the different species of Lactobacillus population showed significantly decreased quantity in the patient group compared with the healthy subjects.
Keywords: constipation, Lactobacillus, microbiota, quantitative real-time PCR
Introduction
Chronic constipation is one of the most common pediatric healthcare problems worldwide, with an estimated prevalence ranging between 0.7% and 29.6% in both developed and developing countries. It is estimated that constipation in children causes 3 −5% of visits to pediatric physicians and up to 25% of referrals to children gastroenterologists worldwide.1 Although constipation may have several etiologies, in more than 90% to 95% of children, no underlying pathological cause can be identified and is described as functional constipation. Functional constipation is typically characterized by the painful passage of hard and/or large stools, abdominal pain, and fecal incontinence, which causes a significant impact on the child and family, as well as considerable effects on health-related quality of life.2 Functional constipation diagnosis is based on the Rome criteria for gastrointestinal functional disorders, currently, the Rome IV criteria.3 The large intestine is a natural reservoir for many different microorganisms. It is possible that alteration in gut flora an etiologic factor in the pathogenesis of functional bowel disorders in pediatrics. However, very few studies are available on the causal relationship between functional constipation and microbiome composition in children suffering from constipation.4 It is believed that colonic microflora, especially lactobacilli, can play a beneficial role in the prevention of constipation through several mechanisms such as producing lactic acid, acetic acid, and other acids, stimulating intestinal peristalsis, as well as increasing fecal bolus moisture.5 Based on this hypothesis, to evaluate which of the major Lactobacillus species might be useful in preventing functional constipation, determine phylogenetic diversity and the quantity of this flora in the intestine is pivotal.6 The present study was aimed to evaluate the quantities of the main seven Lactobacillus species in the stool samples of constipated children compared with healthy controls using quantitative real-time PCR (qPCR).
Materials and Methods
Ethical Consideration
This study protocol was conducted in accordance with the Declaration of Helsinki and approved by the Ethical Committee of Ahvaz Jundishapur University of Medical Sciences, Iran (No. IR.AJUMS.REC.1397.433). Written informed consent was obtained by the parents of the participants.
Subjects and Sample Collection
The case–control study comprised 40 children with functional constipation and 40 normal healthy children without any gastroenterological problems as a control group. The criteria for enrolling the study were aged 4 to 18 years and suffering from functional constipation, according to the criteria of ROME IV (for at least 2 months), which were examined and approved by a pediatrician. Exclusion criteria were history of long-term use of antispasmodic drugs, receiving of any oral laxative 4 weeks ago, consumption of antibiotics or probiotics within 15 days prior to enrollment, a diagnosis of metabolic and gastrointestinal diseases (such as hypothyroidism, inflammatory bowel disease and celiac disease), neurological conditions (such as Hirschsprung’s disease and spinal cord abnormalities), mental retardation, anorectal pathology and previous intestinal surgery. In addition, similar exclusion criteria were fulfilled by controls as the study group. The project was explained by clinical researchers to all recruited subjects and informed consent was obtained from the children’s parents or legal guardians.
All study subjects and controls were selected by a pediatric gastroenterologist and asked to provide information on demographic characteristics, medical history, current defection pattern, existence or absence of avoidance, stool incontinence, family history of constipation, frequency of abdominal pain per week, severity of constipation, duration of symptoms of constipation, no response to constipation treatment, and use of probiotics and other medication. Fecal samples were freshly collected from all the participants in a sterile plastic container at the hospital or at home and immediately refrigerated at 4 °C until transported to the laboratory, where the containers were stored frozen at −80 °C until DNA extraction.
Reference Strains
Seven Lactobacillus reference strains (L. casei ATCC 39392, L. paracasei ATCC 25598, L. rhamnosus ATCC 7469, L. plantarum ATCC 8014, L. reuteri ATCC 23272, L. fermentum ATCC 9338, L. acidophilus ATCC 4356) used to validate the assays in the study were ordered from the Iranian Research Organization for Science and Technology (IROST, Iran). All strains were grown in MRS broth under microaerophilic conditions at 37°C for 24 h.
DNA Extraction from Fecal Samples
Bacterial DNA from frozen fecal samples was extracted using a QIAamp DNA stool mini kit (Qiagen, Hilden, Germany) according to the manufacturer’s instructions with some modifications. Prior to the kit protocol, the equivalent volume to 1 g of fecal material homogenized in ice water and centrifuged at 1000 × g for 1 min to remove large particles and debris. About 300 mg of supernatants was transferred to a new tube and 200 μL of TE buffer (Tris-HCl [10mM]: EDTA 10 mM], lysozyme [20mg/mL]; pH 8.0) was added. The tubes were then vortexed for 1 min and incubated at 37° C for1 h. The protocol was then continued as the manufacturer (Qiagen, Hilden, Germany) described. In addition, because the target microorganisms were Gram-positive, to improve the bacterial cell rupture, the lysis temperature was increased to 95°C. Finally, total genomic DNA was stored at −20 °C until use. NanoDrop One spectrophotometer (Thermo Scientific, Wilmington, DE, USA) was used to quantify DNA extracted by different methods, and the quality of the extracted DNA was estimated at 260 and 280 nm from the absorbance ratio.
Oligonucleotide Primers
The specifications of oligonucleotide primers for the detection of lactobacilli are listed in Table 1.7–11 A new specific primer pair was designed for amplification and detection of L. casei using an alignment of 16S-23S intergenic spacer region and obtained with the primer3 online software tool (http://bioinfo.ut.ee/primer3-0.4.0/). The sequences were retrieved from the GenBank database (http://www.ncbi.nlm.nih.gov) and aligned using multiple sequence alignment with Molecular Evolutionary Genetics Analysis (MEGA) software V 6. The oligonucleotide primers were synthesized by Sinaclon Company (Sinaclon, Tehran, Iran). The specificity of L. casei primer pair was initially evaluated in silico using the BLAST (Basic Local Alignment Search Tool) database search program (http://www.ncbi.nlm.nih.gov/BLAST). The specificity was subsequently confirmed by conventional and quantitative PCR assays using DNA extracted from pure cultures of 21 lactobacilli and non-lactobacilli strains obtained from the Iranian Research Organization for Science and Technology (IROST, Iran) as a control (Table 2). The specificity of Primers for the other Lactobacillus species assays has been previously tested. However, once again their specificity was checked in silico by performing BLAST searches of the Gene Bank database.
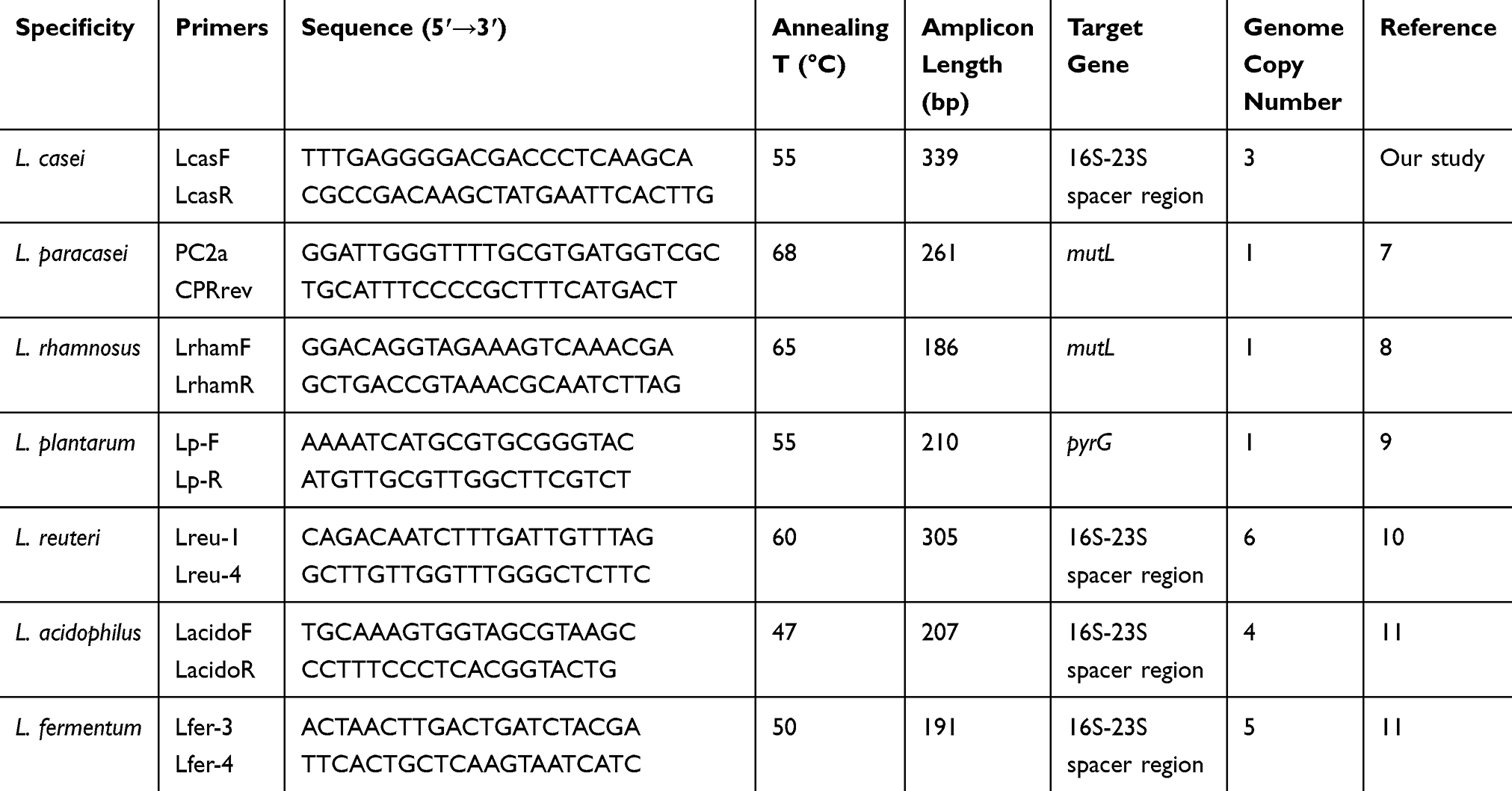 |
Table 1 List of Primers Used in This Study |
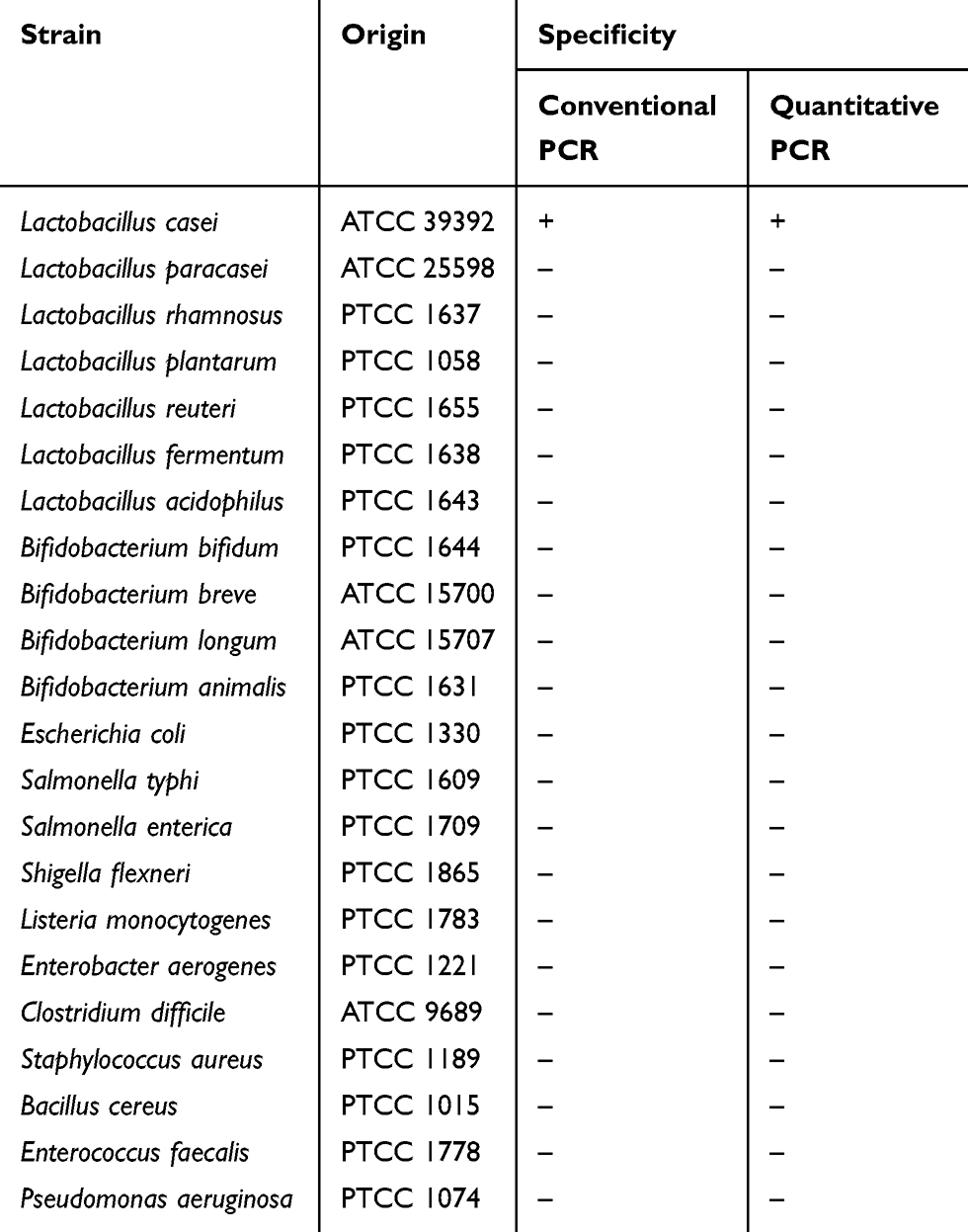 |
Table 2 Specificity of the L. Casei Primer Pair Used in This Study |
Standard Curves for qPCR
In order to verify the sensitivity of the test and compare the real-time PCR outputs with the bacterial colony-forming units (CFU) acquired with the plating, standard curves were constructed by plotting the threshold cycles (Ct) values against the log input extracted DNA from respective reference strains. Briefly, bacterial suspension was grown in 5 mL of MRS broth to an OD 600 nm of 0.6 (Nanodrop One, Thermo Scientific, Wilmington, DE, USA) and serially diluted to a final concentration range of 101–107 CFU mL−1. A 100 µL of each dilution was plated on MRS agar and incubated under the microaerophilic condition for 48h at 37°C. Colonies were then enumerated and used for colony-forming unit extrapolation (CFU per milliliter). All experiments were performed at least in triplicate and the average titer (CFU mL-1) of three replicates was determined. For spiking, fresh fecal samples were from three healthy volunteers initially examined for the absence of the investigated Lactobacillus species by both bacteriological and conventional PCR methods. An amount of 500 μL of each bacterial dilution was spiked into 200 μL of fecal homogenates to make final concentrations (101–107 CFU/g) of feces. Community DNA from spiked feces was extracted using a QIAamp DNA stool mini kit (Qiagen, Hilden, Germany) as described above. By comparing the Ct values acquired to the standard curve, the number of cells of lactobacilli in the fecal samples was determined. For each dilution, average Ct values (from triplicates) and standard deviations (SD) were calculated. As previously described,12 the total number of bacteria (CFU) was interpolated from the average standard curves. When qPCR was conducted in unknown fecal samples, these standard curves were used to determine the quantity of the lactobacilli population.
The reliability criteria of standard curves were verified by the amplification efficiency (E) and the correlation coefficient (R2). The amplification efficiency (E) was calculated by using the slope of the line derived from the standard curves and the equation E = 10 (−1/slope) −1, where b is the slope of the linear fit (eg, E = 1 or 100%). In an acceptable reaction, when the efficiency is 100%, the slope will generate −3.32. The correlation coefficient (R2) obtained for each standard curve is a measure of how well the data fit in a straight line and should be less than 0.99. The detection limit was defined as the lowest concentration presenting a positive threshold cycle (Ct) value in the standard curves at which linearity was retained. The coefficients of variation (CV%) within each triplex qPCR assay were determined for DNA extracts from three fecal samples spiked with different cell numbers of each seven reference strains. The procedure was performed five times to determine inter-assay reproducibility and three times in triplicate for Intra-assay repeatability.
Quantitative Real-Time PCR
Real-time quantitative PCR was performed using genus and species-specific primer sets (Table 1), to measure the quantity of the total Lactobacillus and the quantity of each of the seven Lactobacillus species detected by conventional PCR in each fecal sample. Amplifications were carried out in an ABI StepOne (Applied Biosystems, USA), according to the protocol previously described with a few modifications.13 Briefly, the reaction was performed in a final volume of 25 μL containing 10 μL SYBR Green PCR Master mix 2X (Ampliqon, Denmark), 5 μL nuclease-free water, 2 μL template DNA, and 1 μL (10 pmol μL−1) of each forward and reverse primer. Amplification consisted of 1 min pre-incubation at 95 °C (hot start), followed by 40 cycles with 1 min at 95 °C, 15 s at 60 °C and 30 s at 72 °C. Amplifications were measured in triplicate. Bacterial DNA of reference strains was composed in all qPCR plates as positive control while PCR mixture solution without community DNA was used as the negative control. To determine the specificity of the PCR reactions, post-amplification melting curve analyses were performed automatically by slowly increasing the temperature from 60°C - 98°C (ramp rate 0.11 °C/s), with continuous fluorescence collection. The qPCR amplified amplicon was finally confirmed by using 2.5% agarose gel electrophoresis. In addition, qPCR products were sequenced in 10% of all isolates. Results were analyzed using Sequence Detection Software version 2.1, supplied by Applied Biosystems.
Statistical Analysis
Shapiro–Wilk test was used to investigate the normal distribution of quantitative variables. In the case of a normal distribution, independent t-test, and in the absence of normal distribution, the non-parametric Mann–Whitney U-test or Kruskal–Wallis test was used. One-way ANOVA was performed to detect significant differences among the Lactobacillus species. Chi-square test and Fisher’s exact test were used to analyze the qualitative variables. The software used is SPSS version 24.0 (SPSS Inc., Chicago, IL, USA), Microsoft Office Excel version 2016 and GraphPad Prism version 8 (GraphPad Software, Inc). Statistical significance was considered P-value <0.05 in all tests. Diversity of species in both groups of volunteers was measured using the Shannon index.
Results
Demographic and Clinical Symptoms
In total 80 children (40 functional constipation and 40 healthy controls) participated in the study. Patients with functional constipation (diagnosed using Rome IV criteria, n = 40) and healthy controls (n = 40) were comparable in age (mean 8.1±3.1 years vs 8.1±3.2 years) and gender (23/40 [57.5] vs 19/40 [47.5] female). In this study, no statistically significant differences were found between the study population in the findings at presentation, gender (P = 0.950), and age (P = 0.925) distribution. The most commonly observed symptoms among the symptoms of presentation in the patients were (in descending order), painful defecation (92.5%), abdominal pain (90%), and fecal retention (87.5%). In the last three months before incorporation, four healthy children recorded abdominal pain; however, none of these children met the Rome IV criteria. Demographic and Clinical Symptoms of both study groups are displayed in Table 3.
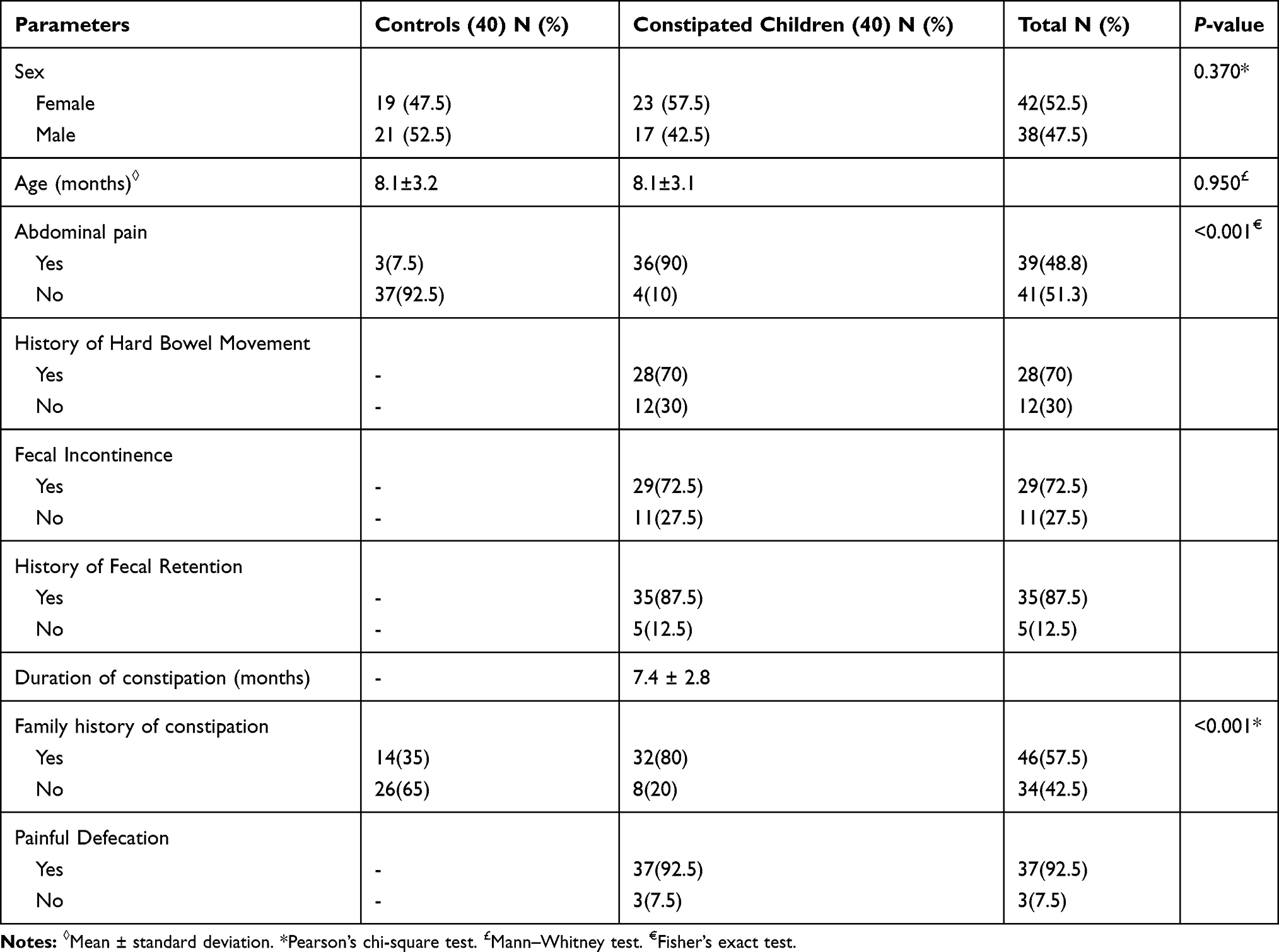 |
Table 3 Demographic and Clinical Characteristics of the Subjects |
The Specificity of the Primers
The results of the analysis for the specificity of the L. casei primer pair used in this study, as well as the results obtained by testing the various strains with the conventional and quantitative PCR procedure, are shown in Table 2. The results showed high specificity of the designed primer set for the detection of L. casei. The sizes of the amplicon generated by conventional PCR were 339 bp. All DNA samples from non-target strains tested with L. casei primer showed no amplification during conventional PCR and no increase in fluorescence during real-time PCR. The specificity of primers for the other Lactobacillus species was tested by submitting each oligonucleotide sequence to the Gene Bank database, and the results demonstrated that no mismatches with the rest of the analyzed microorganisms.
Standard Curves and Limit of Detection
Standard curves for the quantification of Lactobacillus species were constructed from 10-fold serial dilutions of genomic DNA extracted from each of seven reference strains. A highly linear correlation between the Ct values and the quantity of each species (CFU/mL) was obtained for different standard curves with coefficients of determination (R2 values) ranged from 0.995 to 1.000 (Figure 1). According to the run, the amplification efficiencies for seven intended species were from 97.9% to 102.9%. The detection limit was considered as the lowest concentration at which linearity of the standard curves was preserved. The coefficients of variation of inter-assay reproducibility and intra-assay repeatability, as well as detection limits of the different specific real-time PCR procedures (ranged from 2.84 to 3.86 CFU/gr feces), are shown in Table 4. Based on Ct values, the reproducibility of qPCR assays was found to be very high, indicating that qPCR assays were accurate and that the DNA extraction method was highly reproducible.
 |
Figure 1 Representative standard curves obtained by plotting the average Ct values against the estimated log10 CFU/PCR for L. casei (A), L paracasei (B), L rhamnosus (C), L fermentum (D), L acidophilus (E), L plantarum (F) and L. reuteri (G). |
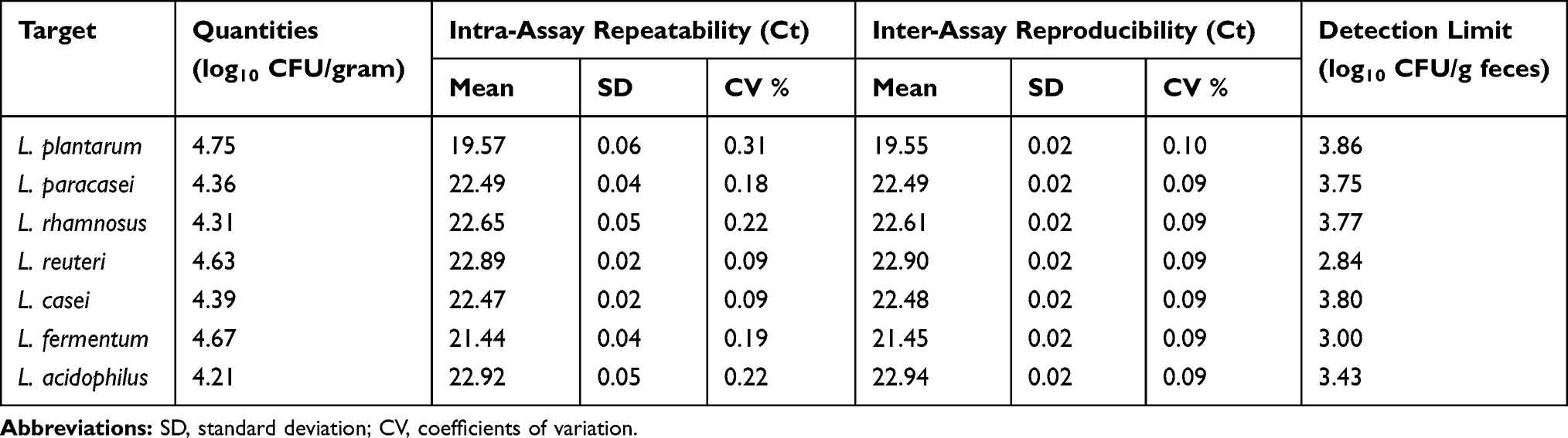 |
Table 4 Intra-Assay Repeatability, Inter-Assay Reproducibility and Detection Limits of qPCR |
Quantification of Lactobacilli in Feces
Differences in the Lactobacillus composition in healthy subjects’ stool samples compared with those found in the constipated patients’ fecal microbiota were assessed using species-specific qPCR. In the present study, seven different Lactobacillus species were detected in the feces of constipated and non-constipated children. Each of the twenty-five constipated patients positive for lactobacilli (out of forty) only had one detectable Lactobacillus species, whereas all forty healthy patients were positive for lactobacilli and five had two distinct Lactobacillus species present. According to the species-specific qPCR results, L. paracasei (30%) followed by L. plantarum (25%) had the highest prevalence among all species isolated from both patient and healthy groups (Table 5). The diversity index (Shannon H score) of fecal Lactobacillus species in constipated children was higher in compared with healthy controls (1.81 versus 1.72, p < 0.001). In all samples containing lactobacilli, the average quantity of seven Lactobacillus species was ranged between 6.95 and 6.01 (Log10 CFU/gram of feces) and 4.71–2.61 (Log10 CFU/gram of feces) for non-constipated and constipated children, respectively (Table 6). In addition, except for L. casei, there was a significant difference in the amount of six other species (Log10 CFU/gram of feces) between the constipated patients and healthy controls (p < 0.05) (Figure 2). As shown in Table 6, the amount of L. casei in the stool of healthy subjects was also significantly higher than constipated children (mean 6.55±0.01 log10 CFU/gram of feces versus mean 3.77±0.13 log10 CFU/gram of farces), but because of the low sample size, the difference was not statistically significant (p <0.2). Higher amounts of L. fermentum and L. reuteri (mean 106.95 and 106.91 CFU/gram feces, respectively) were detected in fecal samples of the healthy subjects than other species. In contrast, the population quantity of L. reuteri (mean 102.61 CFU/gram feces) was lower in constipated patients compared with other species. These results showed there was a significant difference in quantity (Log10 CFU/gram feces) between Lactobacillus species in constipated children and healthy controls (p < 0.0001) (Figure 2, Table 6).
 |
Figure 2 Quantity of seven Lactobacillus species in the feces of constipated children and healthy controls. Statistical significance of observed differences in the amount of Lactobacillus species between both constipated and healthy groups was measured by the Mann–Whitney U-test. Bars represent standard errors. P < 0.05 was marked with one asterisk (∗), and P < 0.2 with two asterisks (∗∗). One-way ANOVA testing shows the significant differences in quantity (log10 CFU/gram) between Lactobacillus species. |
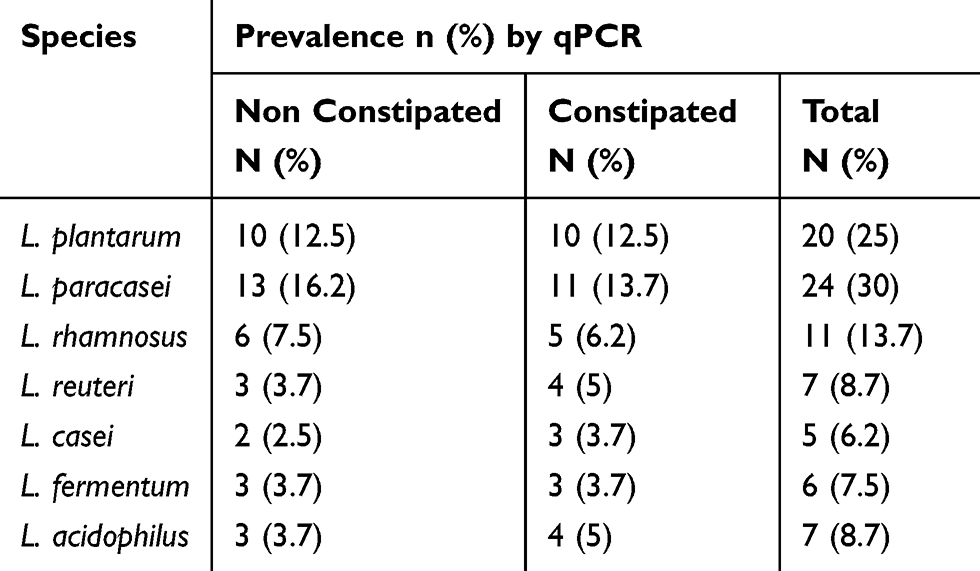 |
Table 5 Prevalence of Lactobacillus Species, Detected by Quantitative PCR |
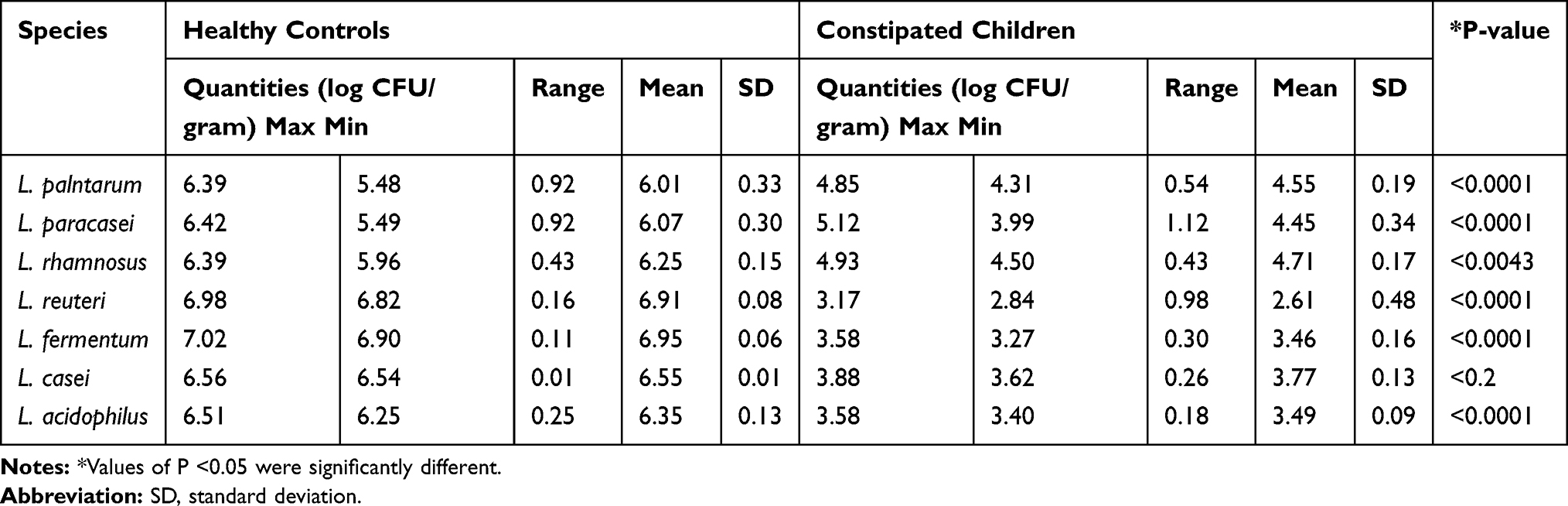 |
Table 6 The Quantity of Fecal Lactobacilli in Constipated Children and Healthy Controls |
Discussion
Growing evidence indicates that alterations in the gut microbiota composition are associated with the pathophysiology of several gastrointestinal disorders such as chronic constipation. Lactobacilli as an essential part of healthy gastrointestinal microecology attracts considerable interest among gastrointestinal researchers in recent years. Thus far, several randomized controlled trials have been conducted on the use of lactobacilli for the management of chronic constipation;6 however, the amount of intestinal lactobacilli in functional constipation are yet poorly investigated, especially in children. The overall aim of our study was to determine the quantitative difference between seven fecal Lactobacillus populations of constipated children and nonconstipated controls.
Following the development of culture-independent methods, it has been found that the numbers of autochthonous Lactobacillus were approximately 1% of the total bacterial inhabitants in the human colon. Furthermore, specific species Lactobacillus that persists in the intestines of some individuals, in others undetectable or representing transient alterations in composition.14 Among over 50 Lactobacillus species that were detected in the stools of healthy individuals, L. acidophilus, L. salivarius, L. casei, L. plantarum, L. fermentum, L. reuteri, L. rhamnosus, L paracasei and L. brevis are the most commonly isolated species. In this study, we focused on the intended seven Lactobacillus species because they were previously described as members of the fecal microbiota of healthy humans.15–18 Furthermore, several clinical trials have shown that they were effective in treating a variety of gastrointestinal disorders, such as functional constipation.6
Recently, many investigators have used the SYBR green qPCR technique to detect different bacterial species in stool samples.13,19 In this study, we used species-specific qPCR primers to investigate some predominant Lactobacillus species colonizing the gut of both healthy and patient volunteers. As previously reported,20 we detected lactobacilli in 65 (81%) of the fecal samples by the culture and conventional PCR methods, and in all samples by quantitative PCR, which indicates the higher diagnostic ability of the qPCR technique than the other two methods in complex samples. So far, only three studies have described the gut microbiome composition in children with functional constipation. In a culture-based methods study, Zoppi et al showed that lactobacilli were significantly decreased in the fecal samples of constipated children as compared with healthy controls.21 In another study, Moraes et al used real-time quantitative PCR to demonstrate that constipated patients had a significantly lower level of lactobacilli than non-constipated children.22 Similar to these findings, based on the quantitative real-time PCR analysis, we observed a significant decreased in the population of lactobacilli in constipated patients’ stool samples compared to healthy controls (p < 0.0001). Contrarily, Zhu et al using 16S rRNA gene pyrosequencing technique demonstrated that the lactobacilli have not decreased in the microbiomes of the constipated obese children.23 Differences between our findings and those from the Zhu et al study may be due to obese subjects’ specific phenotype, as obesity is associated with particular intestinal microbiota composition.
Interestingly, based on the quantitative real-time PCR method, it was found that Lactobacillus acidophilus was present in amounts very close to its detection limit in constipated children’s feces (103.43 CFU/g of feces). So, it can be deduced that the mere presence of different species of Lactobacillus in the colon is not sufficient to impact and prevent certain diseases such as functional constipation and their amount plays a decisive role. Our data showed a significantly lower amount of all species in constipated patients compared to healthy controls. Nevertheless, in the case of L. casei, because of the low sample size, the P-value could not accurately be measured and therefore the results were not statistically significant (P < 0.2).
Although the major intestinal Lactobacillus species were detected in our study, the bacterial coverage was still incomplete, and we did not examine other probiotic bacteria especially bifidobacteria. Furthermore, this work did not assess the metabolic activities of intended Lactobacillus strains. These are the main limitations of our study, and hence further studies on healthy and patient subjects should be able to elucidate the clinical significance of colonizing with these genera, as well as the influence of Lactobacillus species metabolic activities in context to functional constipation.
Another limitation is that we used SYBR green-based qPCR for the quantitative determination of seven Lactobacillus species rather than more sophisticated techniques such as shotgun metagenome sequencing analysis. However, qPCR is also very sensitive, specific, and cost-effective method that has been successfully used to quantify probiotic microorganisms in complex bacterial ecosystems such as stool samples.13,24–26
Conclusion
Our study shows that quantitative real-time PCR assay is a simple, rapid, sensitive, and specific method for strain-specific identification of Lactobacillus species from stool samples without prior DNA purification. This study is valuable not only because it showed the quantitative difference in the lactobacilli flora of patients with functional constipation vs healthy subjects, but also because it is one of the few studies that has been performed on the intestinal Lactobacillus flora in children with this age range. Moreover, this is the first study that has been conducted on the number of various Lactobacillus species in children with functional constipation.
Abbreviations
MRS, Man Rogosa Sharp; Polymerase chain reaction (PCR); qPCR, QuantitativeReal-Time polymerase chain reaction.
Acknowledgments
We thank the laboratory and nursing personnel of children ward in teaching hospitals in Ahvaz, who assisted to collect the clinical specimens. This study was a part of PhD thesis of Nabi Jomehzadeh, which was approved in Cellular and Molecular Research Center, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This study was funded by a grant (CMRC9709) from Research Affairs, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran.
Disclosure
The authors declared no conflict of interest.
References
1. Koppen IJ, Lammers LA, Benninga MA, Tabbers MM. Management of functional constipation in children: therapy in practice. Pediatr Drugs. 2015;17(5):349–360. doi:10.1007/s40272-015-0142-4
2. Tabbers MM, DiLorenzo C, Berger MY, et al. Evaluation and treatment of functional constipation in infants and children: evidence-based recommendations from ESPGHAN and NASPGHAN. J Pediatr Gastroenterol Nutr. 2014;58(2):258–274. doi:10.1097/MPG.0000000000000266
3. Wojtyniak K, Szajewska H. Systematic review: probiotics for functional constipation in children. Eur J Pediatr. 2017;176(9):1155–1162. doi:10.1007/s00431-017-2972-2
4. Kim SE, Choi SC, Park KS, et al. Change of fecal flora and effectiveness of the short-term VSL# 3 probiotic treatment in patients with functional constipation. J Neurogastroenterol Motil. 2015;21(1):111. doi:10.5056/jnm14048
5. Dimidi E, Christodoulides S, Scott SM, Whelan K. Mechanisms of action of probiotics and the gastrointestinal microbiota on gut motility and constipation. Adv Nutr. 2017;8(3):484–494. doi:10.3945/an.116.014407
6. Ohkusa T, Koido S, Nishikawa Y, Sato N. Gut microbiota and chronic constipation: a review and update. Front Med. 2019;6. doi:10.3389/fmed.2019.00019
7. Bottari B, Felis GE, Salvetti E, et al. Effective identification of Lactobacillus casei group species: genome-based selection of the gene mutL as the target of a novel multiplex PCR assay. Microbiol. 2017;163(7):950–960. doi:10.1099/mic.0.000497
8. Huang C-H, Huang L. Rapid species-and subspecies-specific level classification and identification of Lactobacillus casei group members using MALDI Biotyper combined with ClinProTools. J Dairy Sci. 2018;101(2):979–991. doi:10.3168/jds.2017-13642
9. Yu J, Wang HM, Zha MS, et al. Molecular identification and quantification of lactic acid bacteria in traditional fermented dairy foods of Russia. J Dairy Sci. 2015;98(8):5143–5154. doi:10.3168/jds.2015-9460
10. Song Y-L, Kato N, Liu C-X, Matsumiya Y, Kato H, Watanabe K. Rapid identification of 11 human intestinal Lactobacillus species by multiplex PCR assays using group-and species-specific primers derived from the 16S–23S rRNA intergenic spacer region and its flanking 23S rRNA. FEMS Microbiol Lett. 2000;187(2):167–173. doi:10.1111/j.1574-6968.2000.tb09155.x
11. Garg KB, Ganguli I, Das R, Talwar G. Spectrum of Lactobacillus species present in healthy vagina of Indian women. Indian J Med Res. 2009;129(6):652.
12. Lyons SR, Griffen AL, Leys EJ. Quantitative real-time PCR for Porphyromonas gingivalis and total bacteria. J Clin Microbiol. 2000;38(6):2362–2365. doi:10.1128/JCM.38.6.2362-2365.2000
13. Junick J, Blaut M. Quantification of human fecal bifidobacterium species by use of quantitative real-time PCR analysis targeting the groEL gene. Appl Environ Microbiol. 2012;78(8):2613–2622. doi:10.1128/AEM.07749-11
14. Heeney DD, Gareau MG, Marco ML. Intestinal Lactobacillus in health and disease, a driver or just along for the ride? Curr Opin Biotechnol. 2018;49:140–147. doi:10.1016/j.copbio.2017.08.004
15. Rossi M, Martínez‐Martínez D, Amaretti A, Ulrici A, Raimondi S, Moya A. Mining metagenomic whole genome sequences revealed subdominant but constant Lactobacillus population in the human gut microbiota. Environ Microbiol Rep. 2016;8(3):399–406. doi:10.1111/1758-2229.12405
16. Mitsuoka T. The human gastrointestinal tract. In: The Lactic Acid Bacteria. Vol. 1. Boston, MA: Springer; 1992:69–114.
17. Mikelsaar M, Annuk H, Shchepetova J, Mändar R, Sepp E, Björkstén B. Intestinal lactobacilli of Estonian and Swedish children. Microb Ecol Health Dis. 2002;14(2):75–80.
18. Ahrné S, Lönnermark E, Wold AE, et al. Lactobacilli in the intestinal microbiota of Swedish infants. Microbes Infect. 2005;7(11–12):1256–1262. doi:10.1016/j.micinf.2005.04.011
19. Yang YG, Song MK, Park SJ, Kim SW. Direct detection of Shigella flexneri and Salmonella typhimurium in human feces by real-time PCR. J Microbiol Biotechnol. 2007;17(10):1616–1621.
20. Štšepetova J, Sepp E, Kolk H, Loivukene K, Songisepp E, Mikelsaar M. Diversity and metabolic impact of intestinal Lactobacillus species in healthy adults and the elderly. Br J Nutr. 2011;105(8):1235–1244. doi:10.1017/S0007114510004770
21. Zoppi G, Cinquetti M, Luciano A, Benini A, Muner A, Minelli EB. The intestinal ecosystem in chronic functional constipation. Acta Paediatr. 1998;87(8):836–841. doi:10.1111/j.1651-2227.1998.tb01547.x
22. Moraes J, Motta M, Beltrão M, Salviano TL, Silva G. Fecal microbiota and diet of children with chronic constipation. Int J Pediatr. 2016;2016:1–8. doi:10.1155/2016/6787269
23. Zhu L, Liu W, Alkhouri R, et al. Structural changes in the gut microbiome of constipated patients. Physiol Genomics. 2014;46(18):679–686. doi:10.1152/physiolgenomics.00082.2014
24. Wu ZW, Lu HF, Wu J, et al. Assessment of the fecal lactobacilli population in patients with hepatitis B virus-related decompensated cirrhosis and hepatitis B cirrhosis treated with liver transplant. Microb Ecol. 2012;63(4):929–937. doi:10.1007/s00248-011-9945-1
25. Ahlroos T, Tynkkynen S. Quantitative strain‐specific detection of Lactobacillus rhamnosus GG in human faecal samples by real‐time PCR. J Appl Microbiol. 2009;106(2):506–514. doi:10.1111/j.1365-2672.2008.04018.x
26. Costa GN, Marcelino-Guimarães FC, Vilas-Bôas GT, Matsuo T, Miglioranza LH. Potential fate of ingested Lactobacillus plantarum and its occurrence in human feces. Appl Environ Microbiol. 2014;80(3):1013–1019. doi:10.1128/AEM.02588-13
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.