Back to Journals » Clinical Ophthalmology » Volume 19
Qualitative Factors Impacting Patients and Clinicians Regarding Intravitreal Injections for Retinal Disorders: A Scoping Review
Authors Ly A ![]() , Harnick E, Jowsey T, Bannatyne AJ
, Harnick E, Jowsey T, Bannatyne AJ
Received 3 August 2025
Accepted for publication 12 November 2025
Published 28 November 2025 Volume 2025:19 Pages 4349—4365
DOI https://doi.org/10.2147/OPTH.S558098
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Andrew Ly, Evan Harnick, Tanisha Jowsey, Amy Jean Bannatyne
Faculty of Health Sciences & Medicine, Bond University, Gold Coast, QLD, Australia
Correspondence: Andrew Ly, Bond University 14 University Drive, Robina, Gold Coast, QLD, Australia, Tel +61 422 369 218, Email [email protected]
Background: Intravitreal injections are among the most frequently performed eye procedures worldwide. They are vital in managing vision-related retinal conditions such as neovascular age-related macular degeneration, diabetic macular edema and retinal vein occlusion. This review scopes qualitative research concerning people’s beliefs, perspectives, experiences and behaviors towards intravitreal injections.
Methods: Academic databases (PubMed, Embase, CINAHL and Web of Science) were searched for studies focused on qualitative research of intravitreal injections in adult patients, published between January 2000 and May 2024. We extracted data regarding publication and participants’ characteristics, main study objectives, and methodological approaches.
Results: Of the 795 identified citations, 28 met the inclusion criteria. Most studies reported on patients’ emotional experiences of undergoing intravitreal injections, with the fear of vision loss compounded with ongoing injections prompting significant anxiety and uncertainty for patients. Other studies also reported on the physical component as the invasiveness of the procedure caused pain and discomfort, which varied with the clinician’s delivery of the injection. One study reported on clinician experiences of performing intravitreal injections, stating that the treatment decisions are dependent on patient-related factors such as their adherence to regular injections. Overall, qualitative research in ophthalmology is increasing, with most studies employing semi-structured interviews with thematic analysis.
Conclusion: Qualitative research offers valuable insights into both patient and clinician experiences of intravitreal injections, which can shape person-centered and sustainable models of intravitreal treatment. Understanding qualitative factors such as personal experiences and barriers to treatment can refine the delivery of intravitreal injections and ultimately improve patient adherence.
Keywords: qualitative research, intravitreal injections, anti-VEGF, ophthalmology, scoping review
Introduction
Qualitative research (QR) offers valuable insights into people’s experiences, beliefs, perspectives, and practices.1 QR helps us identify how and why people behave in certain ways, and how they make sense of their experiences.2 A conceptual framework study by Oben3 underscores the critical role of understanding patient experiences and behaviors in facilitating consistent and sustainable quality improvements in medical care. The past fifty years have seen increasing use of QR approaches to better understand and enhance patient and provider healthcare experiences.4,5 In ophthalmology, QR can explore the beliefs and preferences of both patients and healthcare professionals, translating these into opportunities for improved healthcare delivery.6
Despite its value, QR remains under-represented in ophthalmology journals.7 In 2017, Jones and Jefferis7 highlighted this gap and called for more qualitative studies to support ophthalmologists in delivering ophthalmic services. Similarly, Okada et al8 urged the use of qualitative approaches to better understand issues such as poor patient adherence and persistence with intravitreal injections.
This scoping review examined whether these calls to action by previous researchers (eg, Jones & Jefferis,7 Okada et al8) have been attended to. We focused specifically on QR related to intravitreal injections, one of the most frequently performed eye procedures worldwide.9 These injections involve administering medication into the eye’s vitreous humour using a fine needle.9 The main type of intravitreal injections is anti-VEGF agents, which include aflibercept (Eylea), ranibizumab (Lucentis) and bevacizumab (Avastin).9 These are mainly used to treat retinal conditions such as neovascular age-related macular degeneration, diabetic macular edema, and retinal vein occlusion.9 Anti-VEGF agents are usually needed for long-term, and often for life.9 Initially, the frequency of injections is high to gain adequate control and preserve vision, but it often decreases as the patient’s condition stabilises.9
To guide our approach, we replicated the process used by Gisselbaek et al10 in their systematic scoping review of published QR on perioperative anesthesiology. Replication was designed to enable cross-disciplinary comparisons in how QR is conducted and reported, and to build a cumulative evidence base to inform improvements in the standard of QR reporting. At the same time, we aimed to identify discipline-specific gaps and reporting challenges unique to ophthalmology. Ultimately, QR can empower clinicians to gain a better understanding of the patient experiences undergoing intravitreal injections, and apply this knowledge to improve patients’ care, adherence and experience with the regularity of intravitreal therapy.
Specifically, this review scopes QR regarding patients’ and ophthalmologists’ beliefs, perspectives, experiences, and behaviors towards intravitreal injections.
Methods
Study Design
A preliminary search of MEDLINE, the Cochrane Database of Systematic Reviews and JBI Evidence Synthesis on 5th July 2024, identified no existing or ongoing systematic or scoping reviews on the topic. Based on this preliminary search, a scoping review was deemed the most appropriate approach. This method is particularly well suited to providing a comprehensive overview of literature in emerging or under-researched areas.11
As such, a scoping review was conducted using the Joanna Briggs Institute Population, Concept, and Context (PCC) methodology12 and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist.13 The scoping review protocol was registered with Open Science Framework (OSF) on the 9th September 2024. The data were managed and stored using Covidence,14 an electronic review platform. The main results of this review, including “study characteristics of included studies” and “categorization of the main topic of research and objective of included studies”, are summarized in table format.
Eligibility Criteria
Table 1 shows the eligibility criteria as per the PCC framework.12
 |
Table 1 Population, Concept and Context Eligibility Criteria |
Additional eligibility criteria not captured in the PCC framework were that included studies needed to be (a) full-text, peer-reviewed studies, (b) published or translated into English, and (c) published from January 2000 to May 2024. The year range was restricted as our preliminary research highlighted an increase in relevant studies from the year 2000 to the conception month of this study.
We excluded records that were not journal articles (eg, conference abstracts, theses, book chapters), not a report of empirical research (eg, protocols, editorials), not focused on intravitreal injections (eg, simulation studies, education studies conducted outside of the clinical setting), and not reported or translated in English. We also excluded studies that involved animal subjects or pediatric patients.
Search Strategy
We designed our search strategy with the assistance of a Faculty Librarian. The three main pre-specified concepts for our search were “adult patients” or “ophthalmic clinicians” as the population, “intravitreal injections” as the type of intervention, and “qualitative research” as a type of study design. Refer to Table 1 for PCC eligibility criteria. We conducted a preliminary initial search of relevant literature on PubMed to understand the topic better and identify possible key terms to search in titles and abstracts. Key index terms contained in titles and abstracts of relevant studies were identified and adapted appropriately in the development of our complete search strategy. We also screened the thesaurus of PubMed (MeSH), Embase (EmTree), CINAHL, and Web of Science to find additional important keywords.
Subsequently, a systematic search of the following electronic databases was undertaken from January 2000 to May 2024: PubMed, Embase, CINAHL, and Web of Science. The final search strategy for the four databases, including search strings, is reflected in Electronic Supplementary Material (ESM), eAppendix 1. To ensure all QR on this topic are captured, we also performed a hand/citation search of the included studies to identify any additional studies missed in the initial search. All identified citations were imported into Covidence, where duplicates were removed.
Study Selection
Two reviewers (AL & EH) independently screened the titles and abstracts of all studies identified via the search strategy, followed by the full-text reviews of relevant studies, using the eligibility criteria. Disagreements were resolved by consensus or with a third reviewer (TJ or AB).
Data Extraction and Analyses
Two independent reviewers (AL & EH) conducted a trial, extracting data from a small number of studies. Once consensus was achieved, data were extracted by one author (AL) from the included studies into tabular form. Broadly, information extracted included: publication characteristics; study aims and objectives; participant characteristics; study design (QR or mixed); QR theoretical framework; data collection methods; data analysis methods; and research quality criteria (see ESM, eAppendix 2 for details on the subcategories). As this study aimed to replicate the approach of Gisselbaek et al,10 all of the subcategories for extraction were pre-determined. The exception to this was extraction related to “main topic of research” and “general objective”. For research quality criteria, we identified whether or not studies had reported reflexivity, provided evidence to support their analytical claims,15 and stated ethical approval details. Reflexivity is defined as
the act of examining one’s own assumptions, beliefs and judgement systems, and thinking carefully and critically about how this influences the research process.16
Following Peters et al,12 we grouped included studies into inductively generated categories, with topics of interest developed from evaluating the data. Extraction and charting issues were resolved through discussion among all authors for consensus. Once data extraction was completed, we summarized qualitative results and undertook descriptive statistics of included studies.
Results
The results of the search and screening process are depicted in Figure 1. The search yielded 795 results. Once duplicates were removed, 450 studies were title and abstract screened, with 370 studies excluded due to irrelevance to the topic of interest. Eighty full-text studies were assessed for eligibility, with 28 studies included in the review. The reasons for exclusion for the 52 excluded studies are shown in Figure 1. The final list of studies is provided in the ESM, eAppendix 3. The key characteristics and findings of the 28 included studies are shown in Tables 2 and 3.
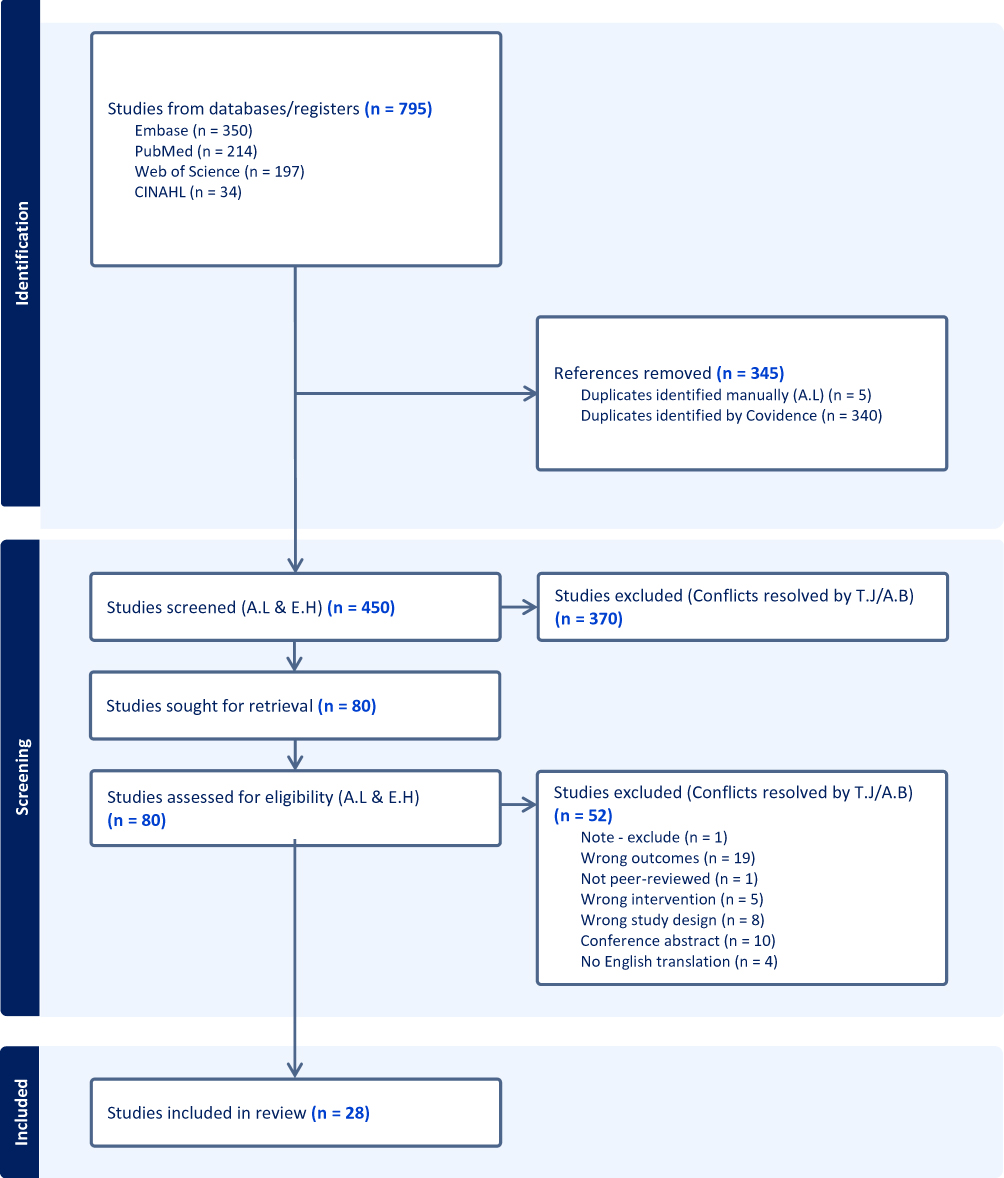 |
Figure 1 PRISMA Flowchart of included studies. |
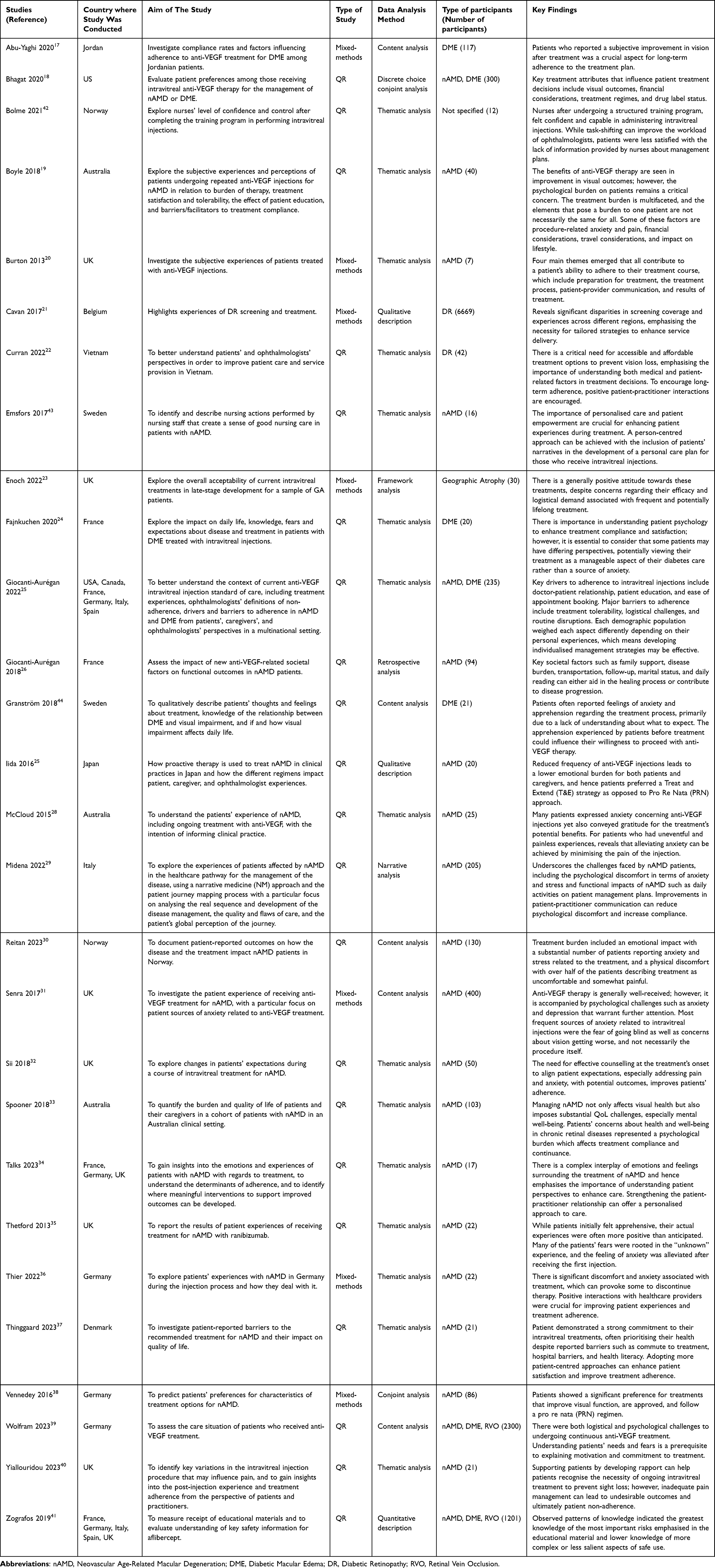 |
Table 2 Study Characteristics of Included Studies |
Study Characteristics
Most included studies (89%, n = 25)17–41 were published in medical journals, with the remaining 11% (n = 3)42–44 published in nursing journals. Over the past two decades, there has been a consistent trend in the publication of qualitative studies related to intravitreal injections in ophthalmology (see Figure 2).
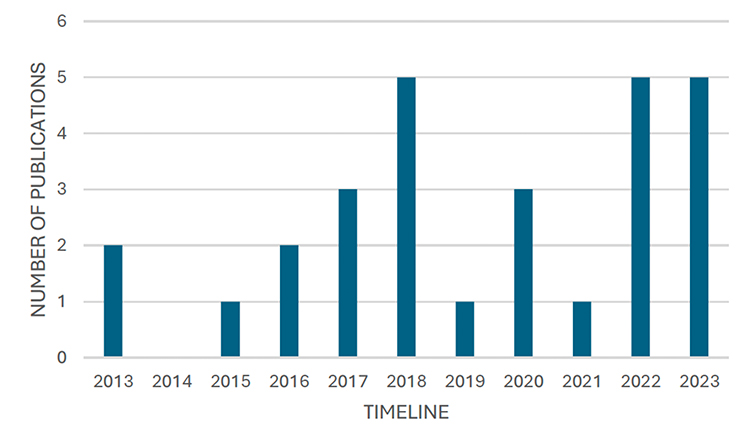 |
Figure 2 Number of qualitative publications per year within the scope of the review. The X-axis is the year, and the Y-axis indicates the number of publications. |
Most of the studies (64%, n = 18) were conducted in European countries, with the United Kingdom contributing the largest number (n = 6).20,23,31,32,35,40 Other European countries represented were Germany (n = 3),36,38,39 France (n = 2),24,26 Sweden (n = 2),43,44 Norway (n = 2),30,42 Denmark (n = 1),37 Belgium (n = 1),21 and Italy (n = 1).29 Studies from Oceania accounted for three publications,19,28,33 all from Australia. In Asia, there were three studies conducted in Vietnam (n = 1),22 Japan (n = 1),27 and Jordan (n = 1).17 Only one study18 was conducted in North America, specifically the United States.
Main Topic of Research and General Objective
Out of 14 pre-determined main topics of research (as per Gisselbaek et al10), the included studies investigated seven main topics of research: barriers to best care (32%; n = 9), patient experiences of care (29%; n = 8), and patients’ experiences undergoing intravitreal injections (25%; n = 7). Less commonly explored topics included: patient-healthcare professional interactions (7%; n = 2), implementation of changes to clinical practice (7%; n = 2), transfer of information (4%; n = 1), and ophthalmologists’ experiences of performing intravitreal injections (4%; n = 1). Two studies addressed more than one of the main topics. Specific research objectives varied within each main topic. Table 3 summarizes the study topics and corresponding research objectives of included studies. ESM eAppendix 3 provides detailed information for each included publication.
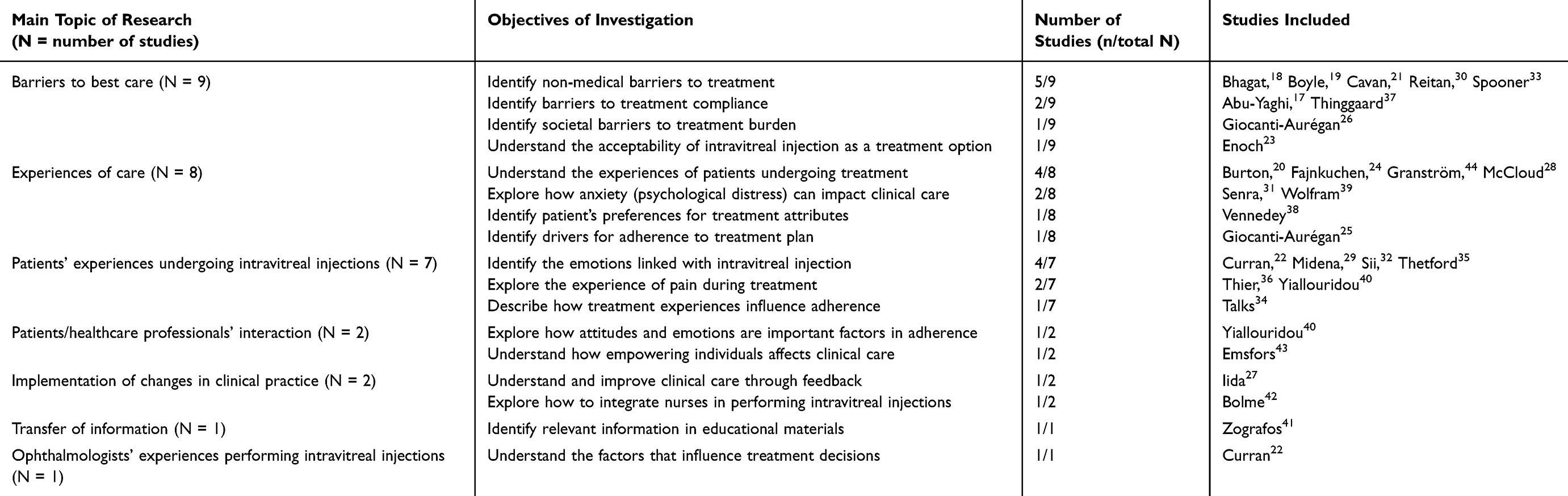 |
Table 3 Categorisation of the Main Topic of Research and Objective of Included Studies |
Research Team Characteristics
Most studies (68%, n = 19) were conducted by multi-professional teams,20–23,25,27,28,30–32,34–40,42,44 while the remaining nine studies (32%, n = 9) were led by uni-professional teams comprising either nurses only, ophthalmologists only or other professionals only.17–19,24,26,29,33,41,43
Participants Characteristics
Nearly all included studies (96%, n = 27) focused exclusively on patient experiences,17–21,23–44 with only one study22 examining the experiences of ophthalmologists alone.
Study Design and Theoretical Framework
Most included studies (75%, n = 21) employed a single-method QR approach, while seven (25%) reported using a mixed-methods design. The study design for included studies is shown in Table 2. Notably, 64% (n = 19) of the qualitative studies did not specify a theoretical framework or epistemology.17–19,21,22,24,26,27,29–33,35,38–41,44 Among those that did (n = 9), they reported grounded theory (11%, n = 3),25,34,36 phenomenology (7%, n = 2),20,28 critical incident technique (4%, n = 1),43 epistemological framework (4%, n = 1),37 inductive descriptive design (4%, n = 1),42 and framework method of analysis (4%, n = 1).23
Data Collection Method
As shown in Table 4, the most commonly reported method was individual interviews, either semi-structured (57%, n = 16) or in-depth (11%, n = 3). Surveys and questionnaires with an open text component were the second most frequently used data collection method (32%, n = 9).
 |
Table 4 Data Collection Methods |
Data Analysis Method
Half of the included studies (54%, n = 15) reported that they undertook thematic analysis. Other reported modes of analysis included content analysis (18%, n = 5), qualitative description (11%, n = 3), conjoint analysis (7%, n = 2), framework analysis (4%, n = 1), narrative analysis (4%, n = 1), and retrospective analysis (4%, n = 1). The data analysis methods for each study are shown in Table 2.
Summary of Qualitative Research Findings
The summary of qualitative findings are presented in Table 2.
Patient Experiences
Most of the studies included in this review explored patients’ emotional experiences with receiving intravitreal anti-VEGF injections for retinal conditions such as neovascular age-related macular degeneration, diabetic macular edema, and retinal vein occlusion. A key concern reported by many patients was the realization that they may need multiple injections and lifelong treatment.23 For some, treatment represented hope and an opportunity for improved or preserved vision.20 Burton et al20 highlighted that patients were often willing to endure the associated distress of an invasive procedure in order to maintain vision. Burton et al20 also accentuates that time spent with patients to alleviate their concerns is vital for their emotional well-being and may prevent patients from ceasing their treatment. Fajnkuchen et al24 noted that, as an invasive procedure, intravitreal injections frequently elicited stress and anxiety for patients. Fears of vision loss were intensified by the recurring nature of the injections, leading some patients to experience existential concerns about losing their vision and how to cope with everyday life.44 Importantly, these anxieties appeared to persist regardless of treatment stage, being reported by both newly diagnosed and longer-term patients.31 However, Thetford et al35 found that patients’ initial feelings of anxiety and apprehension about intravitreal injections often reduced following the first injection, as many of their fears were tied to the uncertainty of the procedure being an “unknown” experience. Particularly, there were aspects of procedure that caused pain and discomfort, in particular, the application of anaesthetic and use of surgical drapes along with the needle entry itself, which if addressed effectively, can help reduce anxiety levels.35
In addition to emotional responses, the physical aspects of intravitreal injections also contributed to heightened anxiety.32 Anticipation of pain was a common concern, particularly among patients undergoing their first injection.29 Thier et al36 reported variability in pain experiences based on factors such as the clinician administering the injection, the dosage and timing of anaesthetic, and procedural differences, including the location of injection and the time delay between applying the anaesthetic and the injection itself. While the pain sensation varied, all of the patients described feeling the sting of the injection, despite the anaesthetic given.36 Yiallouridou et al40 further noted that post-injection ocular pain, including soreness and irritation lasting up to 36 hours, was more prevalent than previously acknowledged, which can be addressed to improve the patient experience. However, not all patients reported pain or distress; for some, the injection was uneventful and associated with low levels of anxiety.28
Access to Healthcare Services
Several studies reported on barriers to accessing and maintaining intravitreal injection treatment. Curran et al22 examined structural challenges in Vietnam, where high treatment costs and transportation costs along with distance from clinics, frequently disrupted patient access. Access to healthcare services was similarly identified by Thinggaard et al,37 who found that while Denmark’s tax-funded system reduced the financial burden, transport and commuting (particularly for patients reliant on public transport) remained significant obstacles. Similarly, in Australia, Spooner et al33 noted that despite government subsidies for anti-VEGF injections through the Pharmaceutical Benefits Scheme,45 patients still incurred personal expenses for mobility aids, low-vision equipment, and home modifications. The ALBATROS study by Wolfram et al39 provided a comprehensive categorization of treatment barriers, identifying four main domains that influence patients’ treatment decisions: tolerability, clinical factors, logistical issues, and human factors.
Quality of Care
A minority of the studies reported on the quality of care associated with intravitreal injections. Yiallouridou et al40 demonstrated that patient-practitioner interactions play a crucial role in shaping patients’ understanding of treatment expectations and individual needs, enabling more tailored advice for managing pain before and immediately after injection. Curran et al22 also underpins the importance of positive patient–practitioner interactions built from previous appointments that encouraged patients to adhere to the recommended series of treatments. Similarly, Wolfram et al39 recognize that a key role in maintaining adherence was seen in the quality of the relationship between patient and clinician, especially through actively assessing and addressing patients regularly along the course of treatment. Comparably, for ophthalmic nurses, Emsfors et al43 described how nurses being respectful, engaged and present in consultations improved the quality of care as patients responded well to treatment due to increased participation in the decision-making process.
Additionally, the quality of care was impacted by changes in clinical practice. Given that intravitreal injections are among the most frequently performed eye procedures worldwide,9 the shortage of ophthalmologists has placed significant pressure on ophthalmology departments worldwide, including the National Health Service in England.46 Bolme et al42 revealed that following a training program, nurses felt confident and in control when administering intravitreal injections, suggesting that performing intravitreal injections can shift from ophthalmologists to nurses in the near future. In contrast, Iida and Ishii27 examined different treatment regimens for intravitreal therapy, each with associated advantages and disadvantages. The Treat and Extend (T&E) approach involved an increased number of injections and associated financial burden; however, it decreased emotional burden for patients by offering reassurance their condition was being actively managed.27 In comparison, the pro re nata (PRN) regimen involved fewer injections, but was associated with increased anxiety, as patients feared receiving “bad news” and the possibility of unexpected injections in response to disease exacerbations.27
Moreover, Zografos et al41 explored how information is transferred between ophthalmologists and patients regarding the safety and proper use of Aflibercept (Eylea), a common intravitreal medication. This study demonstrated that patients possessed relatively high levels of knowledge despite low reported receipt of educational materials, suggesting that patients were obtaining information from sources other than their ophthalmologists.41
Ophthalmologist Experiences
Only one study reported on ophthalmologists’ experiences with intravitreal injections.22 Curran et al22 explored the factors influencing ophthalmologists’ treatment decisions and their recommendations for improving care for patients at risk of requiring, or already receiving, intravitreal injections. Three common factors that shaped treatment plans included: medical considerations (ie, severity of disease, benefits, and risks), availability (ie, treatment and resources), and patient-related factors (ie, costs and adherence).22 Ophthalmologists postulated that balancing realistic treatment goals with these factors may improve the care for patients requiring intravitreal injections.22 Comprehending patient-related factors such as personal experiences, financial situation, and transportation logistics can address poor patient adherence in long courses of intravitreal therapy.22
Research Quality
Reflexivity
Reflexivity was addressed in varying degrees across the included studies. Potential research subjectivity and limitations were acknowledged in 23 studies (82%).17–20,22–25,27–38,40–42 However, only three studies explicitly described steps taken to actively mitigate researcher biases (11%).17,34,40 Selection bias was identified as a concern in four studies (14%).20,24,31,42 Positionality statements, which are considered good practice in qualitative research as they offer insights into researchers’ identities and perspectives,47 were included in only four studies (14%).22,36–38
Presentation of Evidence to Support Analysis Claims
Just over half of the included studies (54%, n = 15) transcribed and presented verbatim participant quotes to illustrate their analytical interpretations and support study conclusions.19–23,25,28,34–37,40,42–44
Ethical Review
Twenty-seven studies (96%) reported they had sought and obtained approval from a registered human ethics research board.17–19,21–44
Discussion
This systematic scoping review aimed to map and synthesize qualitative research exploring human lived experiences of intravitreal injections in ophthalmology. To our knowledge, this is the first review to focus specifically on qualitative inquiry in this context. The review included 28 studies, the majority of which employed interview-based data collection and were published in the past two decades, indicating growing interest in qualitative methodologies within ophthalmic research. While this upward trend is promising, our review also highlights variability in methodological rigor and reporting quality across studies.
Methodological Patterns and Gaps
Most studies utilised individual interviews, typically semi-structured, as their primary method of data collection, and thematic analysis as the most common approach to data interpretation. These methods, while accessible and widely used, often reflect pragmatic rather than theoretically grounded research. Only a small number of studies explicitly reported their epistemological stance or theoretical framework. This limited transparency makes it difficult to assess how researchers’ philosophical positions informed the design, conduct, and interpretation of their studies.
Reflexivity was inconsistently reported. Although 82% of included studies acknowledged potential subjectivity and limitations, only a few articulated the steps taken to mitigate researcher bias, and just four studies included positionality statements. Verbatim quotes, an important marker of qualitative trustworthiness, were used in only half the studies. These gaps reflect similar concerns raised by Gisselbaek et al10 in their review of 107 qualitative studies in perioperative anesthesiology. While that review uncovered a rich array of patient and clinician experiences with the potential to shape clinical practice, many of the included studies were poorly reported, with essential methodological details often missing.10
Our review identified similar patterns. Nine studies reported qualitative results of the open-ended questions in their questionnaires. While we have included these, the data richness was variable. Nearly all studies documented ethical approval and discussed study limitations and sources of subjectivity. However, as with the broader dataset, only half included verbatim quotes to support their findings, limiting the reader’s ability to evaluate the credibility of interpretations.
Overall, these methodological limitations underscore the need for qualitative researchers in ophthalmology to adopt established reporting standards such as the Consolidated Criteria for Reporting Qualitative Research (COREQ) and the Standards for Reporting Qualitative Research (SRQR). Doing so would enhance methodological transparency, support critical appraisal, and strengthen the contribution of qualitative research to ophthalmic care.
Encouragingly, our review revealed a steady increase in qualitative research publications over the past two decades, with approximately 90% of included studies published in medical journals. This growth reflects a rising interest in exploring patient and clinician perspectives within ophthalmology. However, as in anaesthesiology,10 the reporting of qualitative studies remains inconsistent. Few studies clearly articulated the philosophical assumptions guiding their research, and most relied on relatively straightforward qualitative methods, such as semi-structured interviews and thematic analysis. These approaches, while practical and time-efficient, may limit the depth and theoretical contribution of findings when not rigorously executed or clearly contextualized.
Insights Into the Patient Experience
The included studies offered valuable insights into patients’ perceptions and experiences of receiving intravitreal injections. A dominant theme across the literature was the profound significance patients placed on maintaining their vision.20 Intravitreal injections were often viewed as essential, sometimes even life-defining, interventions to preserve sight.23 This is consistent with broader sensory anthropology literature,48 where vision is frequently positioned as the most privileged sense. Regardless of whether one accepts the hierarchy of the senses, for the patients in these studies, preserving sight was clearly central to their identity, independence, and quality of life.
Anxiety and fear associated with the injection procedure were also commonly reported. These emotional responses have clinical significance. Previous research has demonstrated that anxiety can negatively impact treatment adherence and health outcomes across a range of chronic conditions.49 Given that many ophthalmic conditions requiring intravitreal injections are chronic and progressive, these findings highlight the importance of integrating psychological support into routine care.
Some studies also identified non-ophthalmic factors such as barriers impacting access to intravitreal treatment, including economic and transportation costs influencing treatment adherence. These factors can impact treatment decisions, such as determining an appropriate frequency of injections to improve treatment adherence. For instance, Ashrafzadeh’s retrospective analysis50 during the COVID-19 pandemic revealed that demographic and socio-contextual factors affected treatment continuity. These findings underscore the need for equity-informed, patient-centered approaches that consider the broader social determinants of health.
Clinicians Perspectives
Although less frequently studied, one included paper explored the experiences of ophthalmologists performing intravitreal injections and how their perspective can translate in improved clinical outcomes.22 This study highlighted how clinician awareness of patient fears, barriers to adherence, and systemic pressures could shape more realistic and empathic care plans. A systematic review by Ehlken et al51 exploring non-adherence and non-persistence in intravitreal injections, similarly, emphasized the importance of clinician insight into potential barriers in improving clinical outcomes. Expanding research into the experiences and perspectives of ophthalmologists represents a valuable direction for future inquiry.
Implications for Practice
The insights generated by QR into intravitreal injections have practical implications. First, the recurrent theme of anxiety highlights a need for enhanced communication strategies and psychological support interventions. Second, the importance placed on preserving sight suggests that clinical interactions should centre not only on biomedical outcomes but also on personal goals and living priorities. Finally, improved understanding of clinician perspectives could inform interventions to support both patients and providers in managing the long-term demands of chronic eye conditions.
Strengths and Limitations
A key strength of this review is its novel focus on qualitative literature in ophthalmology, which has received relatively little attention in previous reviews. By including both interview-based and open-ended questionnaire studies, we captured a broad range of perspectives. However, limitations include the exclusion of pediatric studies and treatments beyond intravitreal injections. Additionally, data extraction was completed by a single reviewer and checked by others, rather than being independently conducted by multiple reviewers, which may have introduced bias.
Future Directions
Future reviews should explore qualitative studies focusing on other ophthalmic procedures and include pediatric populations, whose experiences may differ considerably from adults. There is also a need for deeper exploration of clinician perspectives, as well as co-produced research that engages patients as partners. Across all future studies, clear articulation of philosophical underpinnings, reflexivity, and methodological transparency should be prioritized to strengthen the credibility and utility of findings.
Conclusion
This review affirms the central importance of sight to patients and highlights the psychological complexities surrounding intravitreal injection treatments, which, if addressed appropriately, can foster stronger patient-centered ophthalmic management. Important qualitative factors, such as patient and clinician personal experiences and barriers to treatment can be focused upon to improve the manner in which intravitreal treatment is delivered to patients. These qualitative findings provide meaningful insights into how intravitreal injections impact patients in terms of emotional burden and discomfort, which clinicians and nurses are able to address these factors and coordinate compassionate, effective, and equitable ophthalmic care.
Data Sharing Statement
The authors confirm that the data supporting the findings of the study are available within the article and its supplementary materials.
Ethics Approval
This scoping review did not involve human participants or the collection of primary data and was therefore exempt from ethics approval, in accordance with Bond University Human Research Ethics Committee (BUHREC) and the National Statement on Ethical Conduct in Human Research (2023).
Acknowledgments
The authors would like to thank Sarah Bateup, Faculty Librarian, Bond University, for her invaluable assistance in designing our search strategy.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Bond University MD Program. No external funding was received for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pathak V, Jena B, Kalra S. Qualitative research. Perspect Clin Res. 2013;4(3):192. doi:10.4103/2229-3485.115389
2. Cleland JA. The qualitative orientation in medical education research. Korean J Med Educ. 2017;29(2):61–71. doi:10.3946/kjme.2017.53
3. Oben P. Understanding the patient experience: a conceptual framework. J Patient Exp. 2020;7(6):906–910. doi:10.1177/2374373520951672
4. Thelwall M, Nevill T. Is research with qualitative data more prevalent and impactful now? Interviews, case studies, focus groups and ethnographies. Libr Inf Sci Res. 2021;43(2):101094. doi:10.1016/j.lisr.2021.101094
5. Alasuutari P. The rise and relevance of qualitative research. Int J Soc Res Methodol. 2010;13(2):139–155. doi:10.1080/13645570902966056
6. Murthy GV, Gupta SK. Qualitative research in ophthalmic sciences. Indian J Ophthalmol. 1999;47(4):257–264.
7. Jones RK, Jefferies JM. Is qualitative research under-represented in ophthalmology journals? Eye. 2017;31:1117–1119. doi:10.1038/eye.2017.49
8. Okada M, Mitchell P, Finger RP, et al. Nonadherence or nonpersistence to intravitreal injection therapy for neovascular age-related macular degeneration: a mixed-methods systematic review. Ophthalmology. 2021;128(2):234–247. doi:10.1016/j.ophtha.2020.07.060
9. Lam LA, Mehta S, Lad EM, Emerson GG, Jumper JM, Awh CC. Intravitreal injection therapy: current techniques and supplemental services. J Vitreoretin Dis. 2021;5(5):438–447. doi:10.1177/24741264211028441
10. Gisselbaek M, Hudelson P, Savoldelli GL. A systematic scoping review of published qualitative research pertaining to the field of perioperative anesthesiology. Can J Anaesth. 2021;68(12):1811–1821. doi:10.1007/s12630-021-02106-y
11. Munn Z, Pollock D, Khalil H, et al. What are scoping reviews? Providing a formal definition of scoping reviews as a type of evidence synthesis. JBI Evid Synth. 2022;20(4):950–952. doi:10.11124/JBIES-21-00483
12. Peters MDJ, Godfrey CM, Khalil H, McInerney P, Parker D, Soares CB. Guidance for conducting systematic scoping reviews. Int J Evid Based Healthc. 2015;13(3):141–146. doi:10.1097/XEB0000000000000050
13. Tricco AC, Lillie E, Zarin W, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and Explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
14. Veritas Health Innovation. (2025). Covidence Systematic Review Software. Available from: www.covidence.org.
15. Thorne S. On the use and abuse of verbatim quotations in qualitative research reports. Nurse Author Ed. 2020;30(6). doi:10.1111/nae2.2
16. Jamieson MK, Govaart GH, Pownall M. Reflexivity in quantitative research: a rationale and beginner’s guide. Soc Personal Psychol Compass. 2023;17(4):e12735. doi:10.1111/spc3.12735
17. Abu-Yaghi NE, Abed AM, Khlaifat DF, et al. Factors affecting compliance to anti-vascular endothelial growth factor treatment of diabetic macular edema in a cohort of jordanian patients. Clin Ophthalmol. 2020;14:921–929. doi:10.2147/OPTH.S248661
18. Bhagat D, Kirby B, Bhatt H, Jager R, George M, Sheth V. Patient preferences associated with anti-vascular endothelial growth factor therapies for neovascular age-related macular degeneration and diabetic macular edema. Clin Ophthalmol. 2020;14:2975–2982. doi:10.2147/OPTH.S273564
19. Boyle J, Vukicevic M, Koklanis K, Itsiopoulos C, Rees G. Experiences of patients undergoing repeated intravitreal anti-vascular endothelial growth factor injections for neovascular age-related macular degeneration. Psychol Health Med. 2018;23(2):127–140. doi:10.1080/13548506.2016.1274040
20. Burton AE, Shaw R, Gibson J. Experiences of patients with age-related macular degeneration receiving anti-vascular endothelial growth factor therapy: a qualitative study. Br J Vis Impair. 2013;31(3):178–188. doi:10.1177/0264619613490517
21. Cavan D, Makaroff L, da Rocha Fernandes J, et al. The diabetic retinopathy barometer study: global perspectives on access to and experiences of diabetic retinopathy screening and treatment. Diabet Res Clin Pract. 2017;129:16–24. doi:10.1016/j.diabres.2017.03.023
22. Curran K, Lohfeld L, Congdon N, et al. Ophthalmologists’ and patients’ perspectives on treatments for diabetic retinopathy and maculopathy in Vietnam: a descriptive study. BMJ Open. 2022;12(7):e055061. doi:10.1136/bmjopen-2021-055061
23. Enoch J, Ghulakhszian A, Sekhon M, Crabb DP, Taylor DJ, Dinah C. Exploring patient acceptability of emerging intravitreal therapies for geographic atrophy: a mixed-methods study. Eye. 2023;37(17):3634–3642. doi:10.1038/s41433-023-02571-3
24. Fajnkuchen F, Delyfer M, Conrath J, et al. Expectations and fears of patients with diabetes and macular edema treated by intravitreal injections. Acta Diabetol. 2020;57(9):1081–1091. doi:10.1007/s00592-020-01513-9
25. Giocanti-Aurégan A, García-Layana A, Peto T, et al. Drivers of and barriers to adherence to neovascular age-related macular degeneration and diabetic macular edema treatment management plans: a multi-national qualitative study. Patient Prefer Adherence. 2022;16:587–604. doi:10.2147/PPA.S347713
26. Giocanti-Aurégan A, Chbat E, Darugar A, et al. Influence of new societal factors on neovascular age-related macular degeneration outcomes. BMC Ophthalmol. 2018;18(1):22. doi:10.1186/s12886-018-0690-9
27. Iida T, Ishii K. Physician, patient and caregiver experience of different wet age-related macular degeneration anti-VEGF treatment regimes in Japan: a qualitative assessment. Clin Ophthalmol. 2016;10:2505–2513. doi:10.2147/OPTH.S120803
28. McCloud C, Lake S. Understanding the patient’s lived experience of neovascular age-related macular degeneration: a qualitative study. Eye. 2015;29(12):1561–1569. doi:10.1038/eye.2015.167
29. Midena E, Varano M, Pilotto E, et al. Real-life patient journey in neovascular age-related macular degeneration: a narrative medicine analysis in the Italian setting. Eye. 2022;36(1):182–192. doi:10.1038/s41433-021-01470-9
30. Reitan G, Kjellevold Haugen IB, Andersen K, Bragadottir R, Bindesbøll C. Through the eyes of patients: understanding treatment burden of intravitreal Anti-VEGF injections for nAMD Patients in Norway. Clin Ophthalmol. 2023;17:1465–1474. doi:10.2147/OPTH.S409103
31. Senra H, Balaskas K, Mahmoodi N, Aslam T. Experience of Anti-VEGF treatment and clinical levels of depression and anxiety in patients with wet age-related macular degeneration. Am J Ophthalmol. 2017;177:213–224. doi:10.1016/j.ajo.2017.03.005
32. Sii S, Aspinall P, Borooah S, Dhillon B. Exploring factors predicting changes in patients’ expectations and psychosocial issues during the course of treatment with intravitreal injections for wet age-related macular degeneration. Eye. 2018;32(4):673–678. doi:10.1038/eye.2017.271
33. Spooner KL, Mhlanga CT, Hong TH, Broadhead GK, Chang AA. The burden of neovascular age-related macular degeneration: a patient’s perspective. Clin Ophthalmol. 2018;12:2483–2491. doi:10.2147/OPTH.S185052
34. Talks SJ, Daien V, Mitchell P, et al. The patient voice in neovascular age-related macular degeneration: findings from a qualitative study. Ophthalmol Ther. 2022;12(1):561–575. doi:10.1007/s40123-022-00631-7
35. Thetford C, Hodge SM, Harding S, Taylor S, Knox PC. Living with age-related macular degeneration treatment: patient experiences of being treated with ranibizumab (Lucentis)® intravitreal injections. Br J Vis Impair. 2013;31(2):89–101. doi:10.1177/0264619613481778
36. Thier A, Breuning M, Wolfram C, Zeitz Holmberg C, Holmberg C. Emotional and physical experiences of people with neovascular age-related macular degeneration during the injection process in Germany: a qualitative study. BMJ Open. 2022;12(6):e058266. doi:10.1136/bmjopen-2021-058266
37. Thinggaard BS, Pedersen M, Sorensen TL, Grauslund J, Stokholm L. Patient perspectives and barriers in the treatment of neovascular age-related macular degeneration in Denmark: a qualitative study. BMJ Open. 2023;13(11):e077175. doi:10.1136/bmjopen-2023-077175
38. Vennedey V, Danner M, Evers SM, et al. Using qualitative research to facilitate the interpretation of quantitative results from a discrete choice experiment: insights from a survey in elderly ophthalmologic patients. Patient Prefer Adherence. 2016;10:993–1002. doi:10.2147/PPA.S101584
39. Wolfram C, Pfeiffer N, Hudde T, et al. The psychological, social and behavioral Impact of intravitreal anti-VEGF therapy: an analysis from the ALBATROS data. J Clin Med. 2023;12(23):7435. doi:10.3390/jcm12237435
40. Yiallouridou C, Acton JH, Banerjee S, Waterman H, Wood A. Pain related to intravitreal injections for age-related macular degeneration: a qualitative study of the perspectives of patients and practitioners. BMJ Open. 2023;13(8):e069625. doi:10.1136/bmjopen-2022-069625
41. Zografos LJ, Andrews E, Wolin DL, et al. Physician and patient knowledge of safety and safe use information for aflibercept in Europe: evaluation of Risk-Minimization Measures. Pharmaceut Med. 2019;33(3):219–233. doi:10.1007/s40290-019-00279-y
42. Bolme S, Austeng D, Gjeilo KH. Task shifting of intravitreal injections from physicians to nurses: a qualitative study. BMC Health Serv Res. 2021;21(1):1185. doi:10.1186/s12913-021-07203-8
43. Emsfors Å, Christensson L, Elgán C. Nursing actions that create a sense of good nursing care in patients with wet age-related macular degeneration. J Clin Nurs. 2017;26(17–18):2680–2688. doi:10.1111/jocn.13749
44. Granström T, Forsman H, Brorsson AL, Granstam E, Leksell J. Patients’ experiences before starting anti-VEGF treatment for sight-threatening diabetic macular oedema: a qualitative interview study. Nord J Nurs Res. 2017;38(1):11–17. doi:10.1177/2057158517709409
45. Mitchell P. Eyes on the future: A clear outlook on Age-related Macular Degeneration. Macular Degeneration Foundation Australia; 2011. Available from: https://www.mdfoundation.com.au/content/eyes-future-%E2%80%93-clear-outlook-age-related-macular-degeneration.
46. Michelotti MM, Abugreen S, Kelly SP, et al. Transformational change: nurses substituting for ophthalmologists for intravitreal injections – a quality-improvement report. Clin Ophthalmol. 2014;8:755–761. doi:10.2147/OPTH.S59982
47. Sibbald KR, Phelan SK, Beagan BL, Pride TM. Positioning positionality and reflecting on reflexivity: moving from performance to practice. Qual Health Res. 2025;10497323241309230. doi:10.1177/10497323241309230
48. Classen C. Foundations for an anthropology of the senses. Int Soc Sci J. 2010;49(153):401–412. doi:10.1111/j.1468-2451.1997.tb00032.x
49. Clarke DM, Currie KC. Depression, anxiety and their relationship with chronic diseases: a review of the epidemiology, risk and treatment evidence. Med J Aust. 2009;190(S7):S54–60. doi:10.5694/j.1326-5377.2009.tb02471.x
50. Ashrafzadeh S, Gundlach BS, Tsui I. The impact of non-ophthalmic factors on intravitreal injections during the COVID-19 lockdown. Clin Ophthalmol. 2021;15:3661–3668. doi:10.2147/OPTH.S314840
51. Ehlken C, Ziemssen F, Eter N, et al. Systematic review: non-adherence and non-persistence in intravitreal treatment. Graefes Arch Clin Exp Ophthalmol. 2020;258(10):2077–2090. doi:10.1007/s00417-020-04798-2
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
Patient Perspectives and Concerns Regarding Cataract Surgery and Cataract Surgery Sedation: A Qualitative Study
Molina L, Lyang N, Schwartz R, Parikh N, Ramanathan S, Huang AJ, Chen CL
Clinical Ophthalmology 2025, 19:2011-2020
Published Date: 27 June 2025
Patient Experiences of Intravitreal Anti-Vascular Endothelial Growth Factor Injections for Age-Related Macular Degeneration: A Meta-Synthesis of Qualitative Studies
Liu D, Bi H, Sun Y, Gao Z, Lu P
Patient Preference and Adherence 2026, 20:610930
Published Date: 19 June 2026