Back to Journals » Patient Preference and Adherence » Volume 20
Qualitative Assessment of Experiences and Challenges Faced by Mothers of Children Using an Insulin Pump in the United Arab Emirates
Authors Abdul Fattah L, Eldeeb NM, Farajallah A, Shankar PR ![]() , Palaian S
, Palaian S ![]()
Received 16 October 2025
Accepted for publication 18 February 2026
Published 9 April 2026 Volume 2026:20 574827
DOI https://doi.org/10.2147/PPA.S574827
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Lean Abdul Fattah,1 Nour Mostafa Eldeeb,1 Alaa Farajallah,2 Pathiyil Ravi Shankar,3 Subish Palaian2
1College of Pharmacy and Health Sciences, Ajman University, Ajman, United Arab Emirates; 2Department of Clinical Sciences, College of Pharmacy and Health Sciences, Ajman University, Ajman, United Arab Emirates; 3IMU Centre for Education, IMU University, Kuala Lumpur, Malaysia
Correspondence: Subish Palaian, Email [email protected]
Background: Various benefits and challenges influence insulin pump use by diabetic patients, especially children. Mothers, as the primary caregivers, can provide valuable feedback on their children’s health-related issues. This study aimed to explore the experiences and challenges faced by mothers of children using an insulin pump.
Methods: This qualitative exploratory research involved in-depth interviews of eight mothers in the United Arab Emirates selected purposively during March 2025, whose children had type 1 diabetes and used an insulin pump up to the age of 12 years old. A validated interview guide was used.
Results: The use of an insulin pump positively impacted the mothers’ and children’s quality of life. The main identified themes were mothers’ knowledge and perception of insulin pump use, the impact of insulin pump use clinically, psychologically, and socially, the challenges faced, and recommendations. All participants preferred the use of an insulin pump due to its positive properties. Yet, mothers mentioned some concerns, including sudden device malfunction, wrong placement of the cannula, financial burden and the lack of awareness of the needs of insulin pump users.
Conclusion: Insulin pump therapy has significant advantages and disadvantages, but in the opinion of the mothers interviewed, the advantages outweigh the drawbacks.
Keywords: challenges, children, insulin pump, mothers, perspective, type 1 diabetes, United Arab Emirates
Background
Type 1 diabetes mellitus (T1DM) is estimated to affect 652, 000 children worldwide,1 among which 109,000 are in the Middle East and North Africa.2 These alarming numbers call for immediate action to manage this disease among children. Patients with T1DM suffer from destruction of the β-cells in the pancreas, leading to a complete deficiency of insulin.3 Managing the disease is crucial, especially in children, to support healthy growth and reduce the risk of complications. This is done by lifelong insulin administration; the two approaches are multiple daily injections (MDI) and continuous subcutaneous insulin infusion (CSII). The insulin pump therapy employs CSII and is a well-known approach in pediatric diabetes management. Compared to the MDI therapy, it offers multiple benefits including reduced injection frequency, better glycemic control, improved quality of life for children and caregivers, flexibility in their meals and overall daily routine.4–10 There is a reduction in HbA1c level in children with CSII treatment compared with the MDI group.11 Despite all benefits, certain challenges could affect the use of an insulin pump. The high cost that often causes a financial burden for the caregiver, social challenges such as the use of technology in school and other settings, complexity of the process, the continuous need of education, adverse effects like the occurrence of dermatological problems and displacement of the needle in addition to device malfunction may reduce uptake of the device.7,12–18
Mothers are the primary caregivers for their children. They play a key role in managing their children using insulin pump. Their responsibilities include, but are not limited to, managing daily insulin administration, monitoring blood glucose levels, ensuring proper pump maintenance, educating their children about pump usage, and providing essential emotional and psychological support.19–21 Their continuous engagement, vigilance, and encouragement significantly influence the child’s confidence, independence, and long-term health outcomes. It is thus important to understand and support mothers’ roles in this process to achieve a lifelong healthier journey for their children.
A systematic review identified six studies conducted in the United States, the United Kingdom, and Sweden, all of which explored parents’ and/or children’s perspectives on the use of insulin pumps.22 Overall, parents expressed positive attitudes toward transitioning from MDI to insulin pump therapy, although some challenges related to pump use were also reported.23–25
This qualitative research aims to get a more comprehensive understanding of the mothers’ perspectives on the use of insulin pump among their T1DM children, covering every aspect of life that the child and the mother go through including psychological, clinical, difficulties, social challenges, and their recommendations. In Gulf Cooperation Council (GCC) countries, this topic is not widely researched, as reviewing the literature revealed only one study conducted in Kuwait to explore adult patients’ experience regarding insulin pump.26 In the United Arab Emirates (UAE), there is an absence of publications in this area. This scarcity shows the need to conduct research to explore the mothers’ perspectives on insulin pump use among their children. The authors conducted a qualitative research study to understand the mothers’ perspectives, experiences, and challenges faced while managing their children. This study aims to provide a deep insight and rich information from mothers, which could lead to more effective support for children and their families.
Methods
Study Design
This was a qualitative study involving mothers with diabetic children (≤12 years old) who were using the insulin pump to explore their perspectives on the pump use. The Consolidated Criteria for Reporting Qualitative Research (COREQ) was followed in this manuscript (Appendix 1).
Study Setting
Mothers of type 1 diabetic children using insulin pump participated in this study from different Emirates across the United Arab Emirates (UAE). The distribution was Sharjah (3), Abu Dhabi (3), Ras Al Khaima (1) and Umm Al Quwain (1) to establish diversity and obtain a broader spectrum of experiences. For the convenience and satisfaction of the participants, a hybrid approach was followed in this study, allowing both face-to-face interviews and online interviews.
Study Timeline
This study started toward the end of February 2025 and continued until mid-April 2025. Obtaining informed consent, developing the interview guide, conducting the interviews, producing the transcript, analysis and literature review were all completed during this period of time.
Sampling
A purposive sampling technique was followed to select the participants. The participants were approached through personal contacts in addition to the mothers’ support groups. Participating mothers referred other mothers whose child met the inclusion criteria. All contacts were made through WhatsApp and phone calls.
Inclusion and Exclusion Criteria
This study included mothers of children up to the age of 12 years who are using an insulin pump for at least 6 months, living in the United Arab Emirates (UAE), and who were willing to participate. Mothers were excluded if their children were above the age of 12, had type 1 diabetes but were not using an insulin pump, and were living outside of the UAE. Mothers were also excluded if they did not give consent to audio record the interview.
Developing the Interview Guide
All authors participated in developing the interview guide. Open-ended questions were used in developing the interview guide to obtain rich and relevant answers. Content validity was checked by sending the interview guide to three experts, and their feedback was considered in finalizing the guide. After that, a pilot interview was conducted, and eight questions were modified as shown in Table 1. Appendix 2 shows the finalized interview guide.
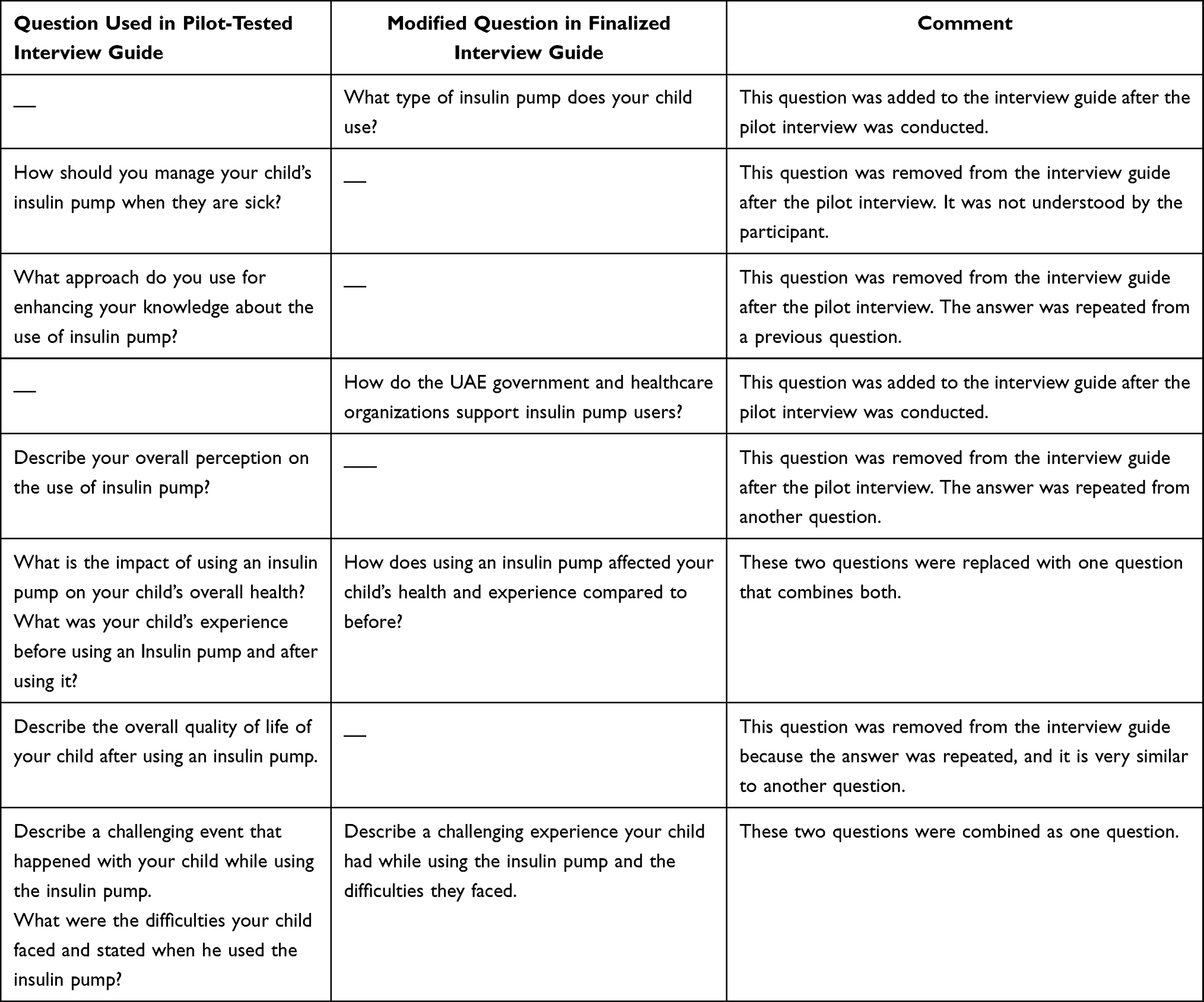 |
Table 1 Customization of the Interview Guide |
Interview Process
Face to face / online interviews were done to obtain comprehensive insights from mothers whose children met the study inclusion criteria. The interview started with collecting the children’s demographic and medical details, including the last HbA1c level, height, weight, co-morbidities, and the type of insulin pump used.
Pre-interview stage: Before conducting the interview, the participants were contacted by the first author through WhatsApp or a phone call to schedule the interview and ascertain the preferred interview mode (face-to-face or online). At this stage, the first author explained all details, including the audio recording and provided the consent form for those who were willing to participate.
Interview stage: Interviews were conducted in a quiet, private setting to ensure confidentiality and encourage open conversation. The first author began by greeting the participants and briefly introducing herself, building a rapport with them. Additionally, the participants were reminded about their voluntary participation and their right to withdraw at any stage of the interview. Then, the demographic and medical details were collected, and the interview was conducted. The pilot interview was conducted face-to-face, while all others were done virtually using online platforms. At the end of the interview, participants were given the opportunity to share any further thoughts or experiences that had not been discussed. The researcher thanked the participants for their valuable time and for sharing their experiences. The interview lasted between 18 to 50 minutes and all interviews were conducted in Arabic language.
Data Saturation
Data transcription and analysis were done concurrently. The data was coded and compared with the previous codes of other participants. Regular discussions among the researchers were conducted to review the coding framework and evaluate whether further interviews were needed. After the sixth interview, researchers noticed that multiple codes were being repeated and proposed that saturation had been reached, as no new themes or codes emerged. To confirm this, two more interviews were conducted, and their codes compared with the previous ones. At this stage, researchers reached a consensus to stop the interviews as no new codes could be found, and saturation may have been achieved.
Ethical Approval and Informed Consent
The study was conducted in accordance with the Declaration of Helsinki and the ethical approval was obtained from the Ethical Review Board of Ajman university, on February 18th, 2025 (Ref Number: P-F-H-18-Feb). Agreement of participants were confirmed before collecting the responses and that was considered as written consent. All methods applied were performed in accordance with the relevant guidelines and regulations.
Data Analysis
Data was analyzed using a thematic analysis approach and followed the six phases mentioned by Braun and Clarke.27 All interviews were audiotaped and transcribed verbatim and reviewed multiple times by three researchers (LAF, NM, AF) to ensure accuracy. The researchers were assisted by“TurboScrib” software to transcribe the interviews. They listened to each recording and verified the transcript accordingly. To ensure the accuracy and equivalence of the translation, a back-translation process was conducted and verified by an external person. The English-translated transcripts were independently translated back into Arabic and compared with the original Arabic transcripts to verify consistency and preserve meaning.
The verified transcripts were then sent to the mothers for review and to get their confirmation. Manual coding was performed by three researchers and transferred to an Excel spreadsheet. Further, the software ATLAS.ti was also used and compared with the manual coding to confirm that no codes were missing. All researchers were involved in deciding the themes, subthemes, and coding that emerged and reaching a consensus. Figure 1 demonstrates steps of data analysis.
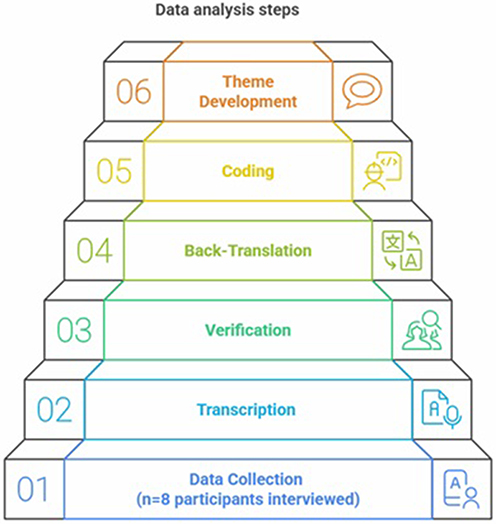 |
Figure 1 Steps followed during data analysis. |
The main identified themes were: mothers’ knowledge and perception on insulin pump use; the impact on the clinical, psychological, and social life of insulin pump use; challenges faced and mothers’ recommendations.
Results
Demographic Characteristics of Participants
Eight mothers participated in this study, with half of them holding a bachelor’s degree. One mother had two children of different genders and ages who used an insulin pump. The mean age of the children was 8.8±3.05 years, while the mean age at diagnosis was 4.1±2.1 years. Table 2 shows the details related to the demographic characteristics of the children.
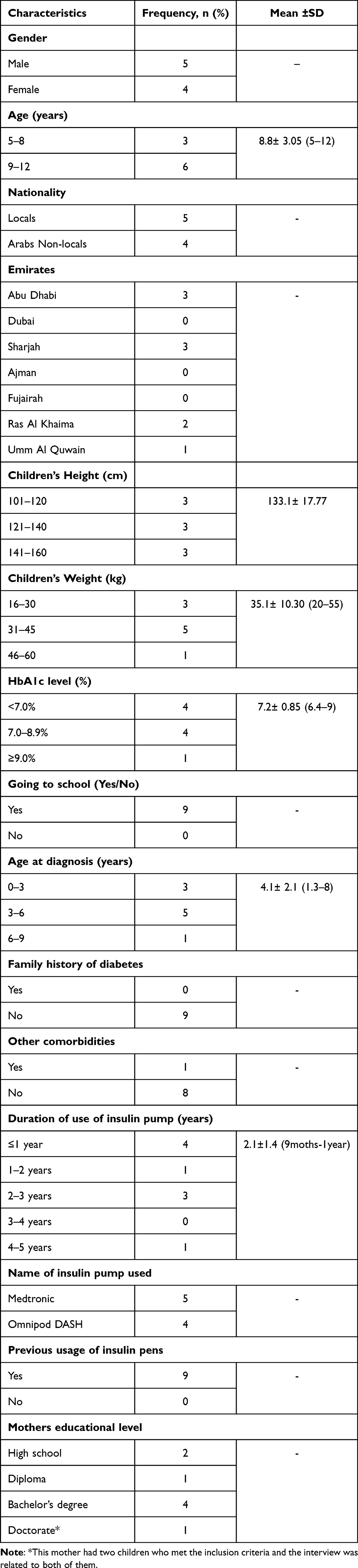 |
Table 2 Demographic Characteristics of Participants’ Children |
Themes
Eight mothers were interviewed. There were three main themes: mothers’ knowledge and perception on insulin pump use; the clinical, psychological, and social life impact of insulin pump use; challenges faced and mothers’ recommendations. Tables 3–5 show all themes, subthemes, and codes that emerged.
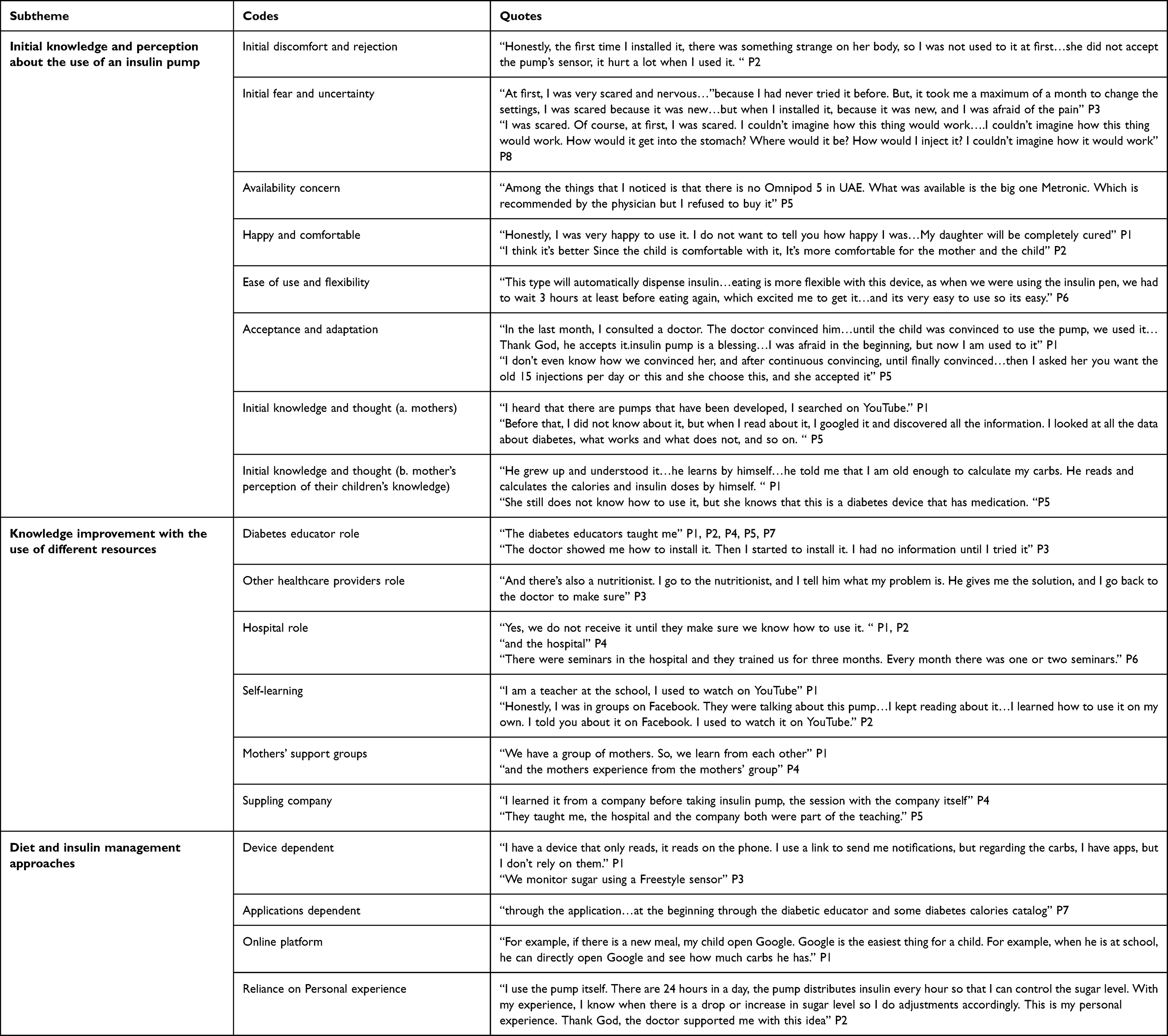 |
Table 3 Mothers’ Knowledge and Perception of Insulin Pump Use |
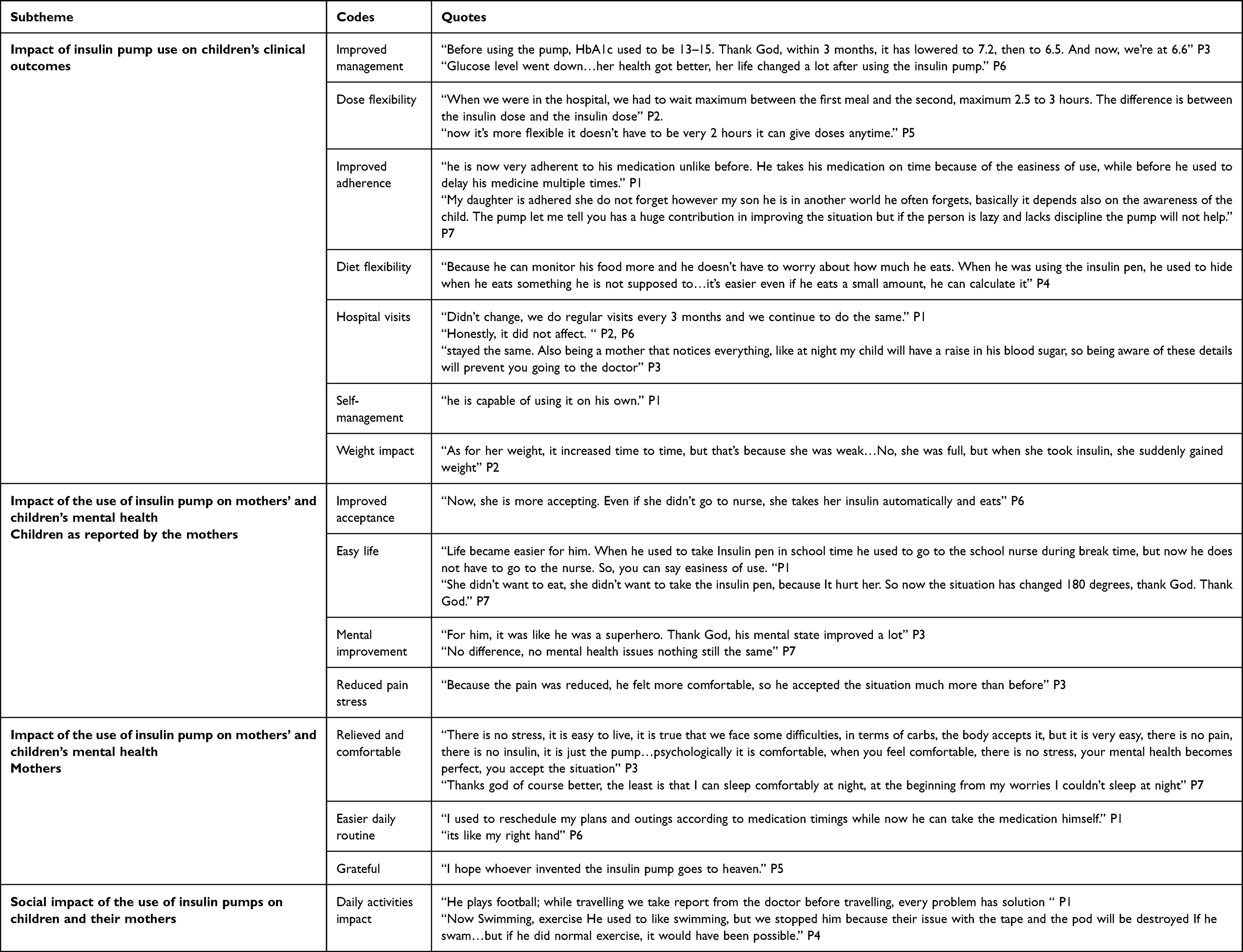 |
Table 4 The Clinical, Psychological, and Social Life Impact of Insulin Pump Use |
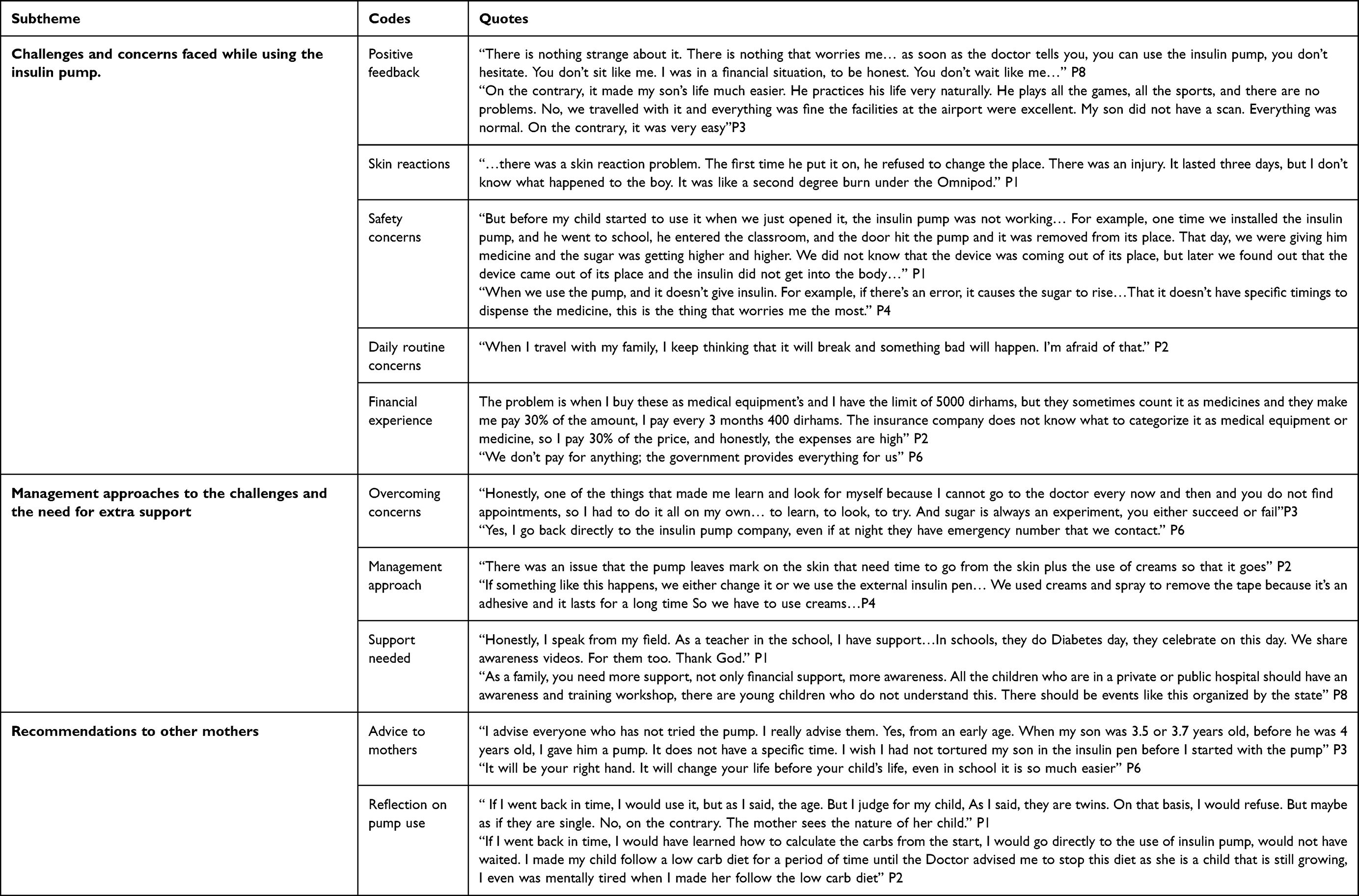 |
Table 5 Challenges Encountered by Mothers and Their Children in the Use of Insulin Pumps |
Theme 1: Mothers’ Knowledge and Perception of Insulin Pump Use
The overall knowledge of mothers on insulin pump use was adequate, with all participants having a positive perception. As the use of insulin pumps changed their children’s lives positively, mothers perceived this technology as a “blessing”. Table 3 shows more details on mothers’ knowledge and perception of insulin pump use.
Initial Knowledge and Perception About the Use of an Insulin Pump
The participants’ initial feelings were mixed between fear and unfamiliarity from the use of new technology, and excitement for the positive change that this technology will bring to their child’s life and its quality. For example, a mother said:
For example, something like this. You take insulin alone. How do you inject insulin? It changes every three days. How does it change? How does it not bother you? I was worried about this; how do you sleep? How do you wake up? How do you take a shower? I didn’t imagine it like this. P8.
According to the mothers, the children showed initial resistance because it is a device that should stay in their bodies all the time. However, with time, this was accepted by the children, and they expressed no desire to return to the use of an insulin pen. A mother said:
She didn’t want to use it at first, she was annoyed, then I asked her you want the old 15 injections per day or this and she chose this, and she accepted it. P5.
Results showed that children’s initial knowledge of the concept of the pump was very basic and simple, and it improved with time. The knowledge came mainly from their mothers, who simplified it as something beneficial to their bodies. As they grew up, their level of understanding improved, and they became more self-dependent.
Many mothers described their initial thought of the pump as an artificial pancreas “outsider pancreas” with limited knowledge reported. A mother stated:
Honestly, I thought it was an outsider pancreas. I thought it was an artificial pancreas. P2
Knowledge Improvement Using Different Resources
Over time, the knowledge becomes adequate with positive perception as it was supplemented and expanded by various sources, including a diabetes educator, self-learning from online resources, and mothers’ support groups. Mothers searched about the insulin pump and its benefits over the insulin pens and decided to switch, aiming to reduce the suffering experienced by their child while injecting insulin using a pen multiple times a day. This decision was further encouraged by the physicians and supported by the diabetes educator in the hospital.
6 out the 8 Mothers appreciated the role of the healthcare providers, mainly the physicians and diabetes educators, who supported them. As they mentioned:
The diabetes educators taught me P1, P2, P4, P5, P7 and The doctor showed me how to install it. Then I started to install it. I had no information until I tried it P3.
The role of the pharmacist was addressed by one mother as a primary, reliable, constant source of information in case she had a question. Another mother appraised the nurses’ role in providing one-to-one educational sessions.
Diet and Insulin Management Approaches
Mothers showed different approaches to measuring the blood sugar and managing their children’s diet. Some used sensors for monitoring blood sugar, while others did regular blood checks due to the high expense of the sensor and its noise. For the diet, few mothers used carb-counting applications, whereas others sought aid from the nutritionist, and the majority considered themselves experts and stated self-dependency and referred to Google or the leaflets on the package of the food supplements. One mother even showed that her 12-year-old child started to be self-dependent in counting the carbs, she stated:
For example, if there is a new meal, my child opens Google. Google is the easiest thing for a child. For example, when he is at school, he can directly open Google and see how many carbs he has. P1
Theme 2: The Clinical, Psychological, and Social Impact of Insulin Pump Use
In general, the impact of insulin pump use on mothers and their children was positive. Mothers mentioned that using the insulin pump affected their lives positively as “everything changed after using the pump”, reducing stress, allowing for flexibility in diet, and improving their children’s quality of life. Table 4 illustrates the impact of insulin pump use on different aspects of children’s and their mothers’ lives.
Advantages of Insulin Pump Use on Children’s Clinical Outcomes
All participants agreed that the use of an insulin pump provided an adequate management of the blood glucose levels and a visible improvement in the HbA1c level compared with the previous insulin pen treatment. A mother said:
Thank God, the sugar level improved, as you can see in HbA1c, the sugar level decreased a lot. P1
Mothers mostly mentioned that the use of an insulin pump improved their child’s adherence due to the ease of use, being easily portable, and fewer injections required than the insulin pen. In contrast, one mother believed there should be no effect whether it is an insulin pen or pump, as the adherence of the child to the medication falls within the mother’s responsibility. She said:
I made her adhere, it is my responsibility, so I give her all the medications on time.P5.
Additionally, the use of an insulin pump reduced frequent hospital visits, as stated by most mothers. Mothers’ responses to their children’s ability to manage and control their sugar levels varied depending on their children’s age. Younger children who are 5 years old cannot have full control by themselves, and they need their mothers’ assistance.
However, mothers mentioned that those children were fully aware of their condition, and when the sugar level is high or low. In contrast, older children were more self-dependent and could deal with their conditions independently.
One mother addressed the importance of having a sensor for younger children, as it will ring an alarm when the sugar level is irregular. She said:
If there was a sensor, for a younger child, this sensor is important for them. For me, I have an older son, so I don’t need it. But for young children, this sensor is important. Because it’s a warning signal P8
The mothers mentioned that their children’s food intake has improved with the use of the insulin pump, their appetite increased, and they wanted to try new food, having freedom in their food choices with no restrictions, less stress, and more organized eating habits.
Impact of the Use of Insulin Pump on Mothers’ and Children’s Mental Health
Mothers explained that initially their children were afraid and nervous when they started using the pump. Some stated that their children refused to go to school while wearing the pump. With time, they adapted, and the fear shifted to acceptance and happiness as they experienced less pain, more engagement with their friends at school, and an easier and more comfortable life than before. A mother said:
For him, it was like he was a superhero. Thank God, his mental state improved a lot. Because the pain was reduced, he felt more comfortable, so he accepted the situation much more than before. P3.
Two mothers illustrated the noticeable positive shift in their son’s mental health during school time after using the pump. They explained how their sons isolated themselves from their classmates and preferred to eat privately to avoid drawing attention or questions when they were using the insulin pen. one said:
Before, he was nervous, he was upset, he would go to the nurse and say, I’m not playing with the children. He used to say, I don’t want to eat, I don’t want to eat. He would go to the nurse and eat in front of her, this affected him a lot. Especially in the first two years, he didn’t enjoy school at all. He hated school. After using the insulin pump… he would go to school and enjoy his break with the children and the adults who were playing. He used to say now I don’t worry about them at all. P8
Mental health also improved among mothers after the introduction of an insulin pump in their children’s lives.
Social Impact of the Use of Insulin Pumps on Children and Their Mothers
According to the mothers, there was little to no negative impact on their children’s daily activities from using the insulin pump. Some restrictions and worries were reported from a few mothers during travelling, exercising, and swimming, whereas others described a normal, active lifestyle for their children.
However, other mothers stated “every problem has solution” showing their ability to overcome these restrictions. For example, during travelling, they prepare a medical report from the hospital to ensure safe travel “while travelling we take report from the doctor before travelling” P1.
Some mothers reported receiving support from the government and other institutions, which positively affected their social life. Local participants received full funding from the government. Additionally, non-local participants benefit from different sources of funding aimed at supporting children with diabetes. For example, one participant acknowledged the support from the charitable organizations that provided the pump for her child. All mothers were grateful for the role of the UAE government in supporting children with diabetes.
Theme 3: Challenges Faced and Mothers’ Recommendations
Challenges and Concerns Faced While Using the Insulin Pump
Generally, the mothers appreciated the use of new technology in making their children’s lives normal and easier. A mother said,
On the contrary, it made my son’s life much easier. He practices his life very naturally. He plays all the games, all the sports, and there are no problems.P3.
However, most mothers were concerned about the adverse events from the insulin pump, including sudden device malfunction and wrong placement of the cannula, leading to spikes in the blood sugar and an increase in ketone levels. They shared several stories about their children, where improper insulin pump placement led to complications and required immediate hospitalization, raising safety issues with the pump. A mother stated:
We put a pump on her. Then she slept, keeping in mind that the pump was new, we kept it for three days, so when she woke up her blood sugar was high, to eventually find out that the pump needle was not fully entered inside the body so the insulin was not reaching her body, her ketone was 5 then went to the hospital and stayed there for 2 days, it was due to inappropriate placement. P2
Skin irritation and infection were also mentioned as adverse reactions caused by the use of the pump, leaving marks on the skin. There was a near consensus about the suitable age to use an insulin pump. They said it is better to start at a young age so they adapt to it more easily, while only one mother insisted on using it when the child is 11–12 years old.
Regardless of their financial category, all participants reported additional expenses for device accessories and maintenance, which could be an added burden. Some expressed concerns about the high costs and financial strain associated with insulin pump use.
The financial impact is more, honestly…It’s expensive P8
Addressing the Challenges and the Need for Extra Support
The mothers addressed these challenges by following the physicians’ instructions, using Google, or their mothers’ WhatsApp support groups. For skin reactions, they used creams, protective tissue, and rotated the locations while inserting the canula of the insulin pump. If the device broke for any reason, the participants used to replace it.
Two participants believed that no additional support was necessary, as comprehensive assistance was already available, including support in schools, awareness programs, activities, and parental guidance. The others addressed the need for more support and assistance in different ways. One participant reported the need for a faster response from the company that provides the pump, as they usually have a delay in their answers. Another participant suggested that companies should offer a one-month trial period before purchase, allowing children to determine whether they are comfortable using the device. Some mentioned that their children require more medical support and faster access to care, prioritizing their mental health. The need for more training for mothers, staff at schools and supportive society was also addressed,
Yes, I need more learning, I applied for the new Insulin Pump even though I don’t know what’s the benefits of it, so I am waiting till I got the approval, and they train me on how to use it. P2.
When a child sees a diabetic baby with a pump, he feels normal. He does not feel alone. Now he is the only child with diabetes. He always asks me why only me? When we go out as a group of mothers with diabetes, I feel like it supports my son. Or we have more diabetic meetings and activities. I wish there was more awareness regarding diabetes. P3
Recommendations to Other Mothers
All participants provided positive feedback, highly praising and recommending the use of the insulin pump. The mothers advised others not to fear starting insulin pump therapy, emphasizing the importance of starting at the right age, learning to count carbohydrates, and ensuring the child’s acceptance of the device. They described the pump as life-changing, bringing peace of mind and a sense of relief for both the mother and the child.
50% of the mothers expressed regret over delaying the use of the insulin pump, wishing they had started sooner. Additionally, one participant wished she had learned carbohydrate counting earlier, as it would have made her experience much smoother. Another mother suggested that the decision to start the insulin pump should be based on the child’s individual needs, as mothers know their children best.
Discussion
This study assessed the mothers’ perspectives on various aspects of insulin pump usage among their children. A broader look at the results showed that mothers found the insulin pump device useful, while there were also multiple challenges. A more detailed discussion on specific themes analyzed in this research is provided below.
Theme 1: Initial Knowledge and Perception About the Use of an Insulin Pump
The initial perception among mothers fluctuated between fear and excitement regarding the use of new technology. Children also reported initial rejection of the use of the insulin pump. As another study mentioned, some parents heard positive things about diabetes technologies, yet some families had concerns about using the insulin pump, like child willingness and its cost.28 However, over time, mothers and their children changed their perceptions of the insulin pump and accepted it, and even called it an outsider pancreas with no willingness to go back to insulin pens. In another study, the parents expressed their willingness to use the insulin pump and consider it the future of diabetes management.29
Knowledge Improvement Using Different Resources
Respondents obtained knowledge from different sources, including physicians and even self-learning. All parents obtained the information from direct resources such as physicians, but a good number also used technology to get the information needed.28 The mothers praised the healthcare team, especially their physicians and diabetes educators. Almost all mothers received training session from the hospital or the device supplying company. Several factors including effective communication between the patient and the care provider, patient education about diabetes and emotional support, will enhance the patient’s adherence to the insulin pump.30
Diet and Insulin Management Approaches
Different methods were followed by the mothers to measure and monitor their children’s insulin and diet. Using an insulin pump, continuous glucose monitoring as well as following a nutritional strategy like advanced carbohydrate counting maximized the efficacy and enhanced the quality of life of T1DM.31,32 Our findings are supported by other studies which reported dietary management was taught by a nutritionist through educational classes, and by learning from other parents, but also “self-taught” was how most parents described themselves.33
Theme 2: The Impact of Insulin Pump Use on the Clinical, Psychological, and Social Life
The current study’s findings indicated that insulin pump therapy has a positive impact on children, including better glycemic control, improved adherence to insulin doses, improved HbA1c levels, and reduced frequency of hospital visits. These results are supported by other findings.11 A multicenter study showed improved clinical outcomes of early initiation of insulin pump therapy in children.34 Further, a German study concluded that the use of insulin pumps reduced long-term hospital stays among pediatric patients.35
Results of this study showed a flexibility in food choices with minimal restriction after using the pump, which lessened the stress on mothers and their children. Insulin pump therapy provides greater flexibility in meal timing and food choices for patients.36
Mental Health
Results of this study revealed initial fear and hesitation among children when they started using the pump due to concerns about wearing a device all the time and potential discomfort. Initially they were apprehensive to interact with their classmates but later they were more accepting of the device. A case-control study conducted in Egypt showed that children with CSII have better health-related quality of life and confidence in diabetes self-management scores than those on MDI,11 and a cross-sectional study conducted in Saudi Arabia revealed the same.37 However, a randomized control trial showed that CSII alone does not appear to significantly improve neuropsychological outcomes in children with T1DM.38
Social
Results of this research showed some restrictions while using the pump on certain children’s activities, especially during swimming, traveling, and exercising. However, many mothers denied these restrictions, describing a normal, active lifestyle among their children. Insulin pumps can generally be disconnected for no more than an hour during activities like swimming, showering, or participating in high-contact sports.39,40
Theme 3: Challenges and Concerns Faced While Using the Insulin Pump
Adverse Events
Mothers generally did not encounter serious obstacles; quite the opposite, it offered them and their children comfort and a good quality of life with few restrictions. However, some mothers expressed concerns about the adverse effects of the pump, such as technical malfunction and skin reactions, based on past incidents their children had experienced. Their primary concern was that the pump might stop functioning or become dislodged without them noticing. The technical faults were mainly due to the dislodged cannula or sport-related incidents where the pump stopped releasing insulin, and the children experienced severe hyperglycaemia and diabetic ketoacidosis that required immediate hospitalization. Similar findings are reported in the literature.39,41 A systematic review revealed that the increased use of insulin pump, dermatological concerns became more common. Mothers in the current study reported mild skin reactions as an adverse effect of pump use, which they managed by applying topical creams and regularly rotating the pump insertion sites. To avoid this, it is recommended to insert the pump to dry non-broken skin and to rotate the insertion site every three days.42
Moreover, to prevent the recurrence of such incidents, some mothers reported using protective tissues. Meser et al recommended various techniques to reduce the likelihood of hypersensitivity reactions, such as the use of a hydrocolloid patch that acts as a barrier between the adhesive and the skin.42 Another study showed the advantage of the use of the corticosteroid medication, fluticasone propionate spray to the cutaneous lesions. The researchers demonstrated that applying two sprays to the skin prior the insertion of the sensor was beneficial in avoiding the incidence of contact dermatitis.43
The challenges encountered by mothers were mainly addressed by following guidance from healthcare providers, searching for information online, or seeking advice from experienced mothers through a WhatsApp group chat. Most mothers advised the early usage of the pump at a younger age. According to the International Society for Pediatric and Adolescent Diabetes (ISPAD) guidelines 2022, insulin pump therapy is the recommended insulin delivery method for young children under 7 years old with T1DM, provided it is accessible and affordable.44
In this study, our findings identified two major groups based on financial aspects related to insulin pump access. The first group consisted of UAE nationals fully covered by the government. The second group included non-nationals who either had insurance coverage or relied on charitable organizations for pump provision. Additionally, some of those non-nationals are without any financial assistance and depend solely on self-payment. All mothers agreed that the device accessories were not covered by insurance and they had to purchase them.39
The literature acknowledged the dramatic rise in insulin prices during recent years.45,46 A qualitative study conducted in the United States to explore the views of parents with children with T1DM about the financial aspects and expenses revealed that supporting families requires an understanding of the financial challenges parents face and their impact on family well-being.46
Mothers’ Recommendations and Advice
All participants recommended the use of insulin pump therapy, as it ensures proper growth for their child, manages their metabolic conditions, and reduces the risk of long-term complications. They stated that they regret not initiating the pump therapy earlier, as it would have saved them a lot of time and struggle. Some participants stated that the school staff lacked knowledge and were not able to handle the children correctly, which resulted in multiple incidents leading to hospitalization. Other findings suggest there is insufficiency in the training of school nurses regarding diabetes knowledge.47–49 A study reveals that school nurses encountered obstacles in finding training on how to properly manage the pump use and the study suggested that there are currently no clear guidelines in paediatric diabetes management in schools where they spend most of their weekdays, and recommended enhancing the teamwork based system between school nurses and healthcare providers to ensure effective diabetes management.50
A qualitative study explored the preferences of youth and their parents regarding an ideal artificial pancreas system. Participants suggested a variety of innovative features aimed at improving both ease of use and safety, such as ketone monitoring integration, voice command functionality, and location tracking.51
Study Strengths and Limitations
This study has several notable strengths. Its qualitative design enabled an in-depth exploration of mothers’ perspectives on insulin pump use in their children, providing rich insights. Furthermore, the study included participants from diverse demographic backgrounds, enhancing the breadth and relevance of the findings. Importantly, this is the first study of its kind to be conducted in the UAE, contributing to a better understanding of diabetes management.
However, this study has some limitations. The sample did not include non-Arab participants, which may limit the diversity of perspectives captured. Additionally, mothers were recruited from only four of the seven emirates. Furthermore, the use of purposive sampling, while effective for reaching a specific population, may have introduced selection bias and limited the generalizability of the results. Another possible limitation of the study is the small sample size (n=8) of the study. Though we aimed to continue as much as sample, the study was stopped after authors confirmed that no new responses were being obtained by doing further interviews and the responses reached saturation. However, it is remotely possible that the respondents were relatively homogenous and this may have contributed to getting similar responses.
Recommendations
Based on the findings of this study, several recommendations can be proposed to improve insulin pump use and support for families managing childhood diabetes in the UAE. There is a clear need to strengthen educational and support systems for parents. Healthcare providers should offer comprehensive training and continuous education on insulin pump use, including troubleshooting common issues. Additionally, developing accessible, evidence-based resources in multiple languages could help reduce parents’ reliance on informal sources such as social media or peer advice.
The study also highlighted the value of peer support, particularly through platforms like WhatsApp, where experienced mothers shared practical advice. Formalizing such support networks through healthcare institutions or patient organizations could provide structured, reliable guidance and emotional support for newly diagnosed families.
Furthermore, concerns about device-related issues, such as technical malfunctions, skin irritation, and accidental dislodgement, should be addressed by both healthcare providers and device manufacturers. Innovations like improved adhesives, waterproofing, and early alert systems could enhance safety and usability, particularly during physical activities or when parents are not present. The authors would also like to recommend future studies on specific themes generated by this research and on the children’s perspective on the use of an insulin pump. A detailed quantitative study involving more mothers, preferably from a large pool across multiple countries, can help validate the qualitative findings and help associate them with demographics and other related parameters. This can further provide the opportunity to device interventions targeted at specific patient group.
Conclusions
Study findings clearly show the positive impact of technology on managing chronic diseases like diabetes. Mothers appreciated the technology, noticed better glycaemic control, and found their initially reluctant children were positive about insulin pump use. Though mothers found the benefits outweigh the drawbacks, they raised concerns about device failure, which in a type 1 diabetes child can be dangerous. Improved education to parents, involvement of the child as the end-user, and more failproof and patient-friendly insulin pumps can further add to the benefits of insulin pumps. More detailed analysis on glycaemic control, pharmacoeconomic evaluation, and quality of life studies can further enhance the widespread use of this novel technology, which can be a game-changer in diabetes management.
Acknowledgments
The authors are grateful to the participating mothers who spent their valuable time to provide their feedback. Their cooperation, openness, and the generous time they dedicated to discussing their journeys are deeply appreciated. Authors further wish to thank Dr. Ayat Ahmed Farajallah, Lecturer at College of Humanities and Sciences, Ajman University, who validated the two Arabic versions of each participant’s transcript. The authors would also like to acknowledge Dr. Wasiq Ali Khan, RPh, Managing Director of Makkah Group of Pharmacies, United Arab Emirates, for facilitating the interviewing process. The authors would also like to thank Ajman University for paying the article processing fee.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no funding for this study.
Disclosure
The authors declare that they have no conflict of interests.
References
1. Elflein J. Children type 1 diabetes worldwide key facts 2021. Statista; 2021. Available from: https://www.statista.com/statistics/241818/key-facts-on-children-and-type-1-diabetes-worldwide/.
2. Saleh S. MENA: children and adolescents with type 1 diabetes 2021 | statista. Available from: https://www.statista.com/statistics/1459482/mena-children-and-adolescents-type-1-diabetes/.
3. Speight J, Pouwer F. Diabetes mellitus, type 1. In: Cambridge Handbook of Psychology, Health and Medicine. 2019:477–20. doi:10.29309/tpmj/2017.24.12.614
4. Shulman R, Miller FA, Daneman D, Guttmann A. Valuing technology: a qualitative interview study with physicians about insulin pump therapy for children with type 1 diabetes. Health Policy. 2016;120(1):64–71. doi:10.1016/j.healthpol.2015.10.006
5. Ata A, Er E, Evin F, et al. Treatment and long-term follow-up of patients diagnosed with type 1 diabetes mellitus before age 5. J Pediatr Endocrinol Metab. 2021;34(2):201–207. doi:10.1515/jpem-2020-0205
6. Babiker A, Alammari N, Aljuraisi A, et al. The effectiveness of insulin pump therapy versus multiple daily injections in children with type 1 diabetes mellitus in a specialized center in Riyadh. Clin Med Insights Endocrinol Diabetes. 2022;15. doi:10.1177/11795514221128495
7. Berget C, Wyckoff L. The use of technology in managing diabetes in youth part 2—insulin pump technologies: information and tips for the school nurse. NASN Sch Nurses. 2020;35(4):188–195. doi:10.1177/1942602X20928914
8. Ooi HL, Wu LL. Insulin pump therapy in children and adolescents with type 1 diabetes: improvements in glycemic control and patients’ satisfaction - hospital UKM experience. Med J Malaysia. 2011;66(4):308–312.
9. Adolfsson P, Ziegler R, Hanas R. Continuous subcutaneous insulin infusion: special needs for children. Pediatr Diabetes. 2017;18(4):255–261. doi:10.1111/pedi.12491
10. Peters JE, Mount E, Huggins CE, Rodda C, Silvers MA. Insulin pump therapy in children and adolescents: changes in dietary habits, composition and quality of life. J Paediatr Child Health. 2013;49(4). doi:10.1111/jpc.12162
11. El Samahy MH, Salah NY, Abdeen MS, Falastin BRK. Psychosocial aspects of continuous subcutaneous insulin infusion in children with type 1 diabetes in Egypt; a limited resources country perspective. Diabetol Metab Syndr. 2022;14(1). doi:10.1186/s13098-022-00853-6
12. Prentice P, Elleri D. Fifteen-minute consultation: insulin pumps for type 1 diabetes in children and young people. Arch Dis Child Educ Pract Ed. 2018;103(3):131–136. doi:10.1136/archdischild-2016-310884
13. Aiello EM, Deshpande S, Özaslan B, et al. Review of automated insulin delivery systems for individuals with type 1 diabetes: tailored solutions for subpopulations. Curr Opin Biomed Eng. 2021;19. doi:10.1016/j.cobme.2021.100312
14. Campbell F, Macdonald AL, Gelder C, Reynolds C, Holland P, Feltbower RG. Embedding CSII therapy in the routine management of diabetes in children: a clinical audit of this service in Leeds. Pract Diabetes Int. 2009;26(1):24–28. doi:10.1002/pdi.1324
15. Lombardo F, Passanisi S, Caminiti L, et al. High prevalence of skin reactions among pediatric patients with type 1 diabetes using new technologies: the alarming role of colophonium. Diabetes Technol Ther. 2020;22(1):53–56. doi:10.1089/dia.2019.0236
16. Hughes CR, McDowell N, Cody D, Costigan C. Sustained benefits of continuous subcutaneous insulin infusion. Arch Dis Child. 2012;97(3):245–247. doi:10.1136/adc.2010.186080
17. Abdullah N, Pesterfield C, Elleri D, Dunger DB. Management of insulin pump therapy in children with type 1 diabetes. Arch Dis Child Educ Pract Ed. 2014;99(5):214–220. doi:10.1136/archdischild-2013-304501
18. Shulman R, Miller FA, Stukel TA, Daneman D, Guttmann A. Pediatric insulin pump therapy: reflecting on the first 10 years of a universal funding program in Ontario. Healthc Q. 2017;19(4):6–9. doi:10.12927/hcq.2017.25019
19. Papadakis JL, Anderson LM, Garza K, et al. Psychosocial aspects of diabetes technology use: the child and family perspective. Endocrinol Metab Clin North Am. 2020;49(1):127–141. doi:10.1016/j.ecl.2019.10.004
20. Sherr JL, Tauschmann M, Battelino T, et al. ISPAD clinical practice consensus guidelines 2018: diabetes technologies. Pediatr Diabetes. 2018;19:302–325. doi:10.1111/pedi.12731
21. Perlberg M, Katz I, Loewenthal N, et al. The role of autonomy-supportive parenting in the competence, adherence and glycemic control of adolescents with type 1 diabetes. Diabet Res Clin Pract. 2021:173. doi:10.1016/j.diabres.2021.108679
22. Alsaleh FM, Smith FJ, Taylor KM. Experiences of children/young people and their parents, using insulin pump therapy for the management of type 1 diabetes: qualitative review. J Clin Pharm Ther. 2012;37(2):140–147. doi:10.1111/j.1365-2710.2011.01283.x
23. Sullivan-Bolyai S, Knafl K, Tamborlane W, Grey M. Parents’ reflections on managing their children’s diabetes with insulin pumps. J Nurs Scholarsh. 2004;36(4):316–323. doi:10.1111/j.1547-5069.2004.04058.x
24. Alsaleh FM, Smith FJ, Thompson R, Al-Saleh MA, Taylor KMG. Insulin pump therapy: impact on the lives of children/young people with diabetes mellitus and their parents. Int J Clin Pharm. 2014;36(5):1023–1030. doi:10.1007/s11096-014-9990-1
25. Rankin D, Harden J, Noyes K, Waugh N, Barnard K, Lawton J. Parents’ experiences of managing their child’s diabetes using an insulin pump: a qualitative study. Diabet Med. 2015;32(5):627–634. doi:10.1111/dme.12683
26. Alsairafi ZK, Smith FJ, Taylor KMG, Alsaleh F, Alattar AT. A qualitative study exploring patients’ experiences regarding insulin pump use. Saudi Pharm J. 2018;26(4):487–495. doi:10.1016/j.jsps.2018.02.010
27. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
28. Commissariat PV, Whitehouse AL, Hilliard ME, et al. Sources and valence of information impacting parents’ decisions to use diabetes technologies in young children <8 years old with type 1 diabetes. Diabetes Technol Ther. 2020;22(9):697–700. doi:10.1089/dia.2019.0497
29. Fu VR, Irwine K, Browne-Cooper K, et al. Outcomes and experiences of families with children with type 1 diabetes on insulin pumps through subsidised pump access programs in Western Australia. Front Endocrinol. 2023:14. doi:10.3389/fendo.2023.1173559
30. Trandafir LM, Moisa SM, Vlaiculescu MV, et al. Insulin pump therapy efficacy and key factors influencing adherence in pediatric population—a narrative review. Med. 2022;58(11). doi:10.3390/medicina58111671
31. Anandhakrishnan A, Hussain S. Automating insulin delivery through pump and continuous glucose monitoring connectivity: maximizing opportunities to improve outcomes. Diabetes Obes Metab. 2024;26(S7):27–46. doi:10.1111/dom.15920
32. Donzeau A, Bonnemaison E, Vautier V, et al. Effects of advanced carbohydrate counting on glucose control and quality of life in children with type 1 diabetes. Pediatr Diabetes. 2020;21(7):1240–1248. doi:10.1111/pedi.13076
33. Patton SR, Clements MA, George K, Goggin K. “I don’t want them to feel different”: a mixed methods study of parents’ beliefs and dietary management strategies for their young children with type 1 diabetes mellitus. J Acad Nutr Diet. 2016;116(2):272–282. doi:10.1016/j.jand.2015.06.377
34. Kamrath C, Tittel SR, Kapellen TM, et al. Early versus delayed insulin pump therapy in children with newly diagnosed type 1 diabetes: results from the multicentre, prospective diabetes follow-up DPV registry. Lancet Child Adolesc Heal. 2021;5(1):17–25. doi:10.1016/S2352-4642(20)30339-4
35. Auzanneau M, Karges B, Neu A, et al. Use of insulin pump therapy is associated with reduced hospital-days in the long-term: a real-world study of 48,756 pediatric patients with type 1 diabetes. Eur J Pediatr. 2021;180(2):597–606. doi:10.1007/s00431-020-03883-2
36. Ghazanfar H, Rizvi S, Khurram A, Orooj F, Qaiser I. Impact of insulin pump on quality of life of diabetic patients. Indian J Endocrinol Metab. 2016;20(4):506–511. doi:10.4103/2230-8210.183472
37. Al Shaikh A, Al Zahrani AM, Qari YH, et al. Quality of life in children with diabetes treated with insulin pump compared with multiple daily injections in tertiary care center. Clin Med Insights Endocrinol Diabetes. 2020:13. doi:10.1177/1179551420959077
38. O’Connell MA, Northam EA, Brown A, et al. Does insulin pump therapy offer benefits for behaviour, mood, cognition and HbA1c in children and adolescents with type 1 diabetes? A randomised controlled trial with observational follow-up. Arch Dis Child. 2024;109(10):806–811. doi:10.1136/archdischild-2023-326007
39. Al-Beltagi M, Saeed NK, Bediwy AS, Elbeltagi R. Insulin pumps in children - a systematic review. World J Clin Pediatr. 2022;11(6):463–484. doi:10.5409/wjcp.v11.i6.463
40. MacNeill G, Fredericks C. Vacation Ease: travelling with an Insulin Pump. Can J Diabetes. 2015;39(3):178–182. doi:10.1016/j.jcjd.2015.02.004
41. Hou M, Amed S, Goldman RD. Insulin pump complications among children with diabetes. Can Fam Physician. 2022;68(12):893–895. doi:10.46747/cfp.6812893
42. Messer LH, Berget C, Beatson C, Polsky S, Forlenza GP. Preserving skin integrity with chronic device use in diabetes. Diabetes Technol Ther. 2018;20:S254–S264. doi:10.1089/dia.2018.0080
43. Paret M, Barash G, Rachmiel M. “Out of the box” solution for skin problems due to glucose-monitoring technology in youth with type 1 diabetes: real-life experience with fluticasone spray. Acta Diabetol. 2020;57(4):419–424. doi:10.1007/s00592-019-01446-y
44. Sundberg F, deBeaufort C, Krogvold L, et al. ISPAD clinical practice consensus guidelines 2022: managing diabetes in preschoolers. Pediatr Diabetes. 2022;23(8):1496–1511. doi:10.1111/pedi.13427
45. Brown-Georgi J, Chhabra H, Vigersky RA. The rising cost of insulin for pump users: how policy drives prices. J Diabetes Sci Technol. 2020;15(5):1177–1180. doi:10.1177/1932296820947100
46. Rohilla L, Gujjar N, Kaur G, Walia P, Dayal D. Financial burden for families of children with type 1 diabetes: a cross-sectional survey from North India. Diabetol Int. 2022;13(4):665–671. doi:10.1007/s13340-022-00589-8
47. Joshi A, Komlodi A, Arora M. School nurses’ perceived barriers to diabetes knowledge, communication and management in children with type 1 diabetes. School Nurse News. 2008;25(3):24–29.
48. Holmström MR, Häggström M, Söderberg S. Being facilitators in a challenging context-school personnel’s experiences of caring for youth with diabetes type 1. J Pediatr Nurs. 2018;43:e114–e119. doi:10.1016/j.pedn.2018.08.007
49. Boden S, Lloyd CE, Gosden C, Macdougall C, Brown N, Matyka K. The concerns of school staff in caring for children with diabetes in primary school. Pediatr Diabetes. 2012;13(6). doi:10.1111/j.1399-5448.2011.00780.x
50. March CA, Nanni M, Kazmerski TM, Siminerio LM, Miller E, Libman IM. Modern diabetes devices in the school setting: perspectives from school nurses. Pediatr Diabetes. 2020;21(5):832–840. doi:10.1111/pedi.13015
51. Commissariat PV, Volkening LK, Butler DA, Dassau E, Weinzimer SA, Laffel LM. Innovative features and functionalities of an artificial pancreas system: what do youth and parents want? Diabet Med. 2021;38(10). doi:10.1111/dme.14492
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.