Back to Journals » International Journal of Women's Health » Volume 18
Qualitative Analysis of Maternal Mortality Reporting Gaps and the Emerging Fourth Delay in Garut Regency, Indonesia
Authors Susiarno H, Adnani QES ![]() , Khaerani IN, Nurdiawan W
, Khaerani IN, Nurdiawan W ![]() , Nisa AS
, Nisa AS ![]() , Adepoju VA
, Adepoju VA
Received 9 July 2025
Accepted for publication 3 February 2026
Published 20 February 2026 Volume 2026:18 552705
DOI https://doi.org/10.2147/IJWH.S552705
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Matteo Frigerio
Hadi Susiarno,1 Qorinah Estiningtyas Sakilah Adnani,2,3 Ira Nufus Khaerani,4 Windi Nurdiawan,1 Aisyah Shofiatun Nisa,1 Victor Abiola Adepoju5
1Department of Obstetric and Gynecology, Faculty of Medicine, Universitas Padjadjaran, Dr. Hasan Sadikin General Hospital, Bandung, Indonesia; 2Department of Public Health, Faculty of Medicine, Universitas Padjadjaran, Bandung, Indonesia; 3Midwifery Working Group, Center for Health System Studies and Health Workforce Education Innovation, Faculty of Medicine, Universitas Padjadjaran, Bandung, Indonesia; 4Midwifery Profession Program, STIKes Karsa Husada, Garut, Indonesia; 5Jhpiego Nigeria, An Affiliate of Johns Hopkins University, Abuja, Nigeria
Correspondence: Hadi Susiarno, Email [email protected]
Background: Indonesia’s maternal mortality ratio (MMR) remains among the highest in Southeast Asia, with significant subnational disparities. Despite national reforms and insurance coverage have expanded, maternal deaths continue in districts with high facility birth rates, including Garut Regency, West Java. Investigating social, clinical, and systemic factors contributing to these deaths can inform improvements in maternal surveillance and care quality.
Methods: We conducted a qualitative study in Garut Regency through in-depth interviews with bereaved family members (n = 3), frontline midwives (n = 5), and the district maternal death registrar (n = 1). Thematic analysis followed Braun and Clarke’s six-phase reflexive method, supported by NVivo 14™. Triangulation, audit trails, member-checking, and reflexive journaling were employed to ensure rigour.
Results: Three interrelated themes emerged: (1) the support system surrounding women, (2) the actions and constraints of healthcare providers, and (3) the architecture of maternal death reporting. Despite high antenatal coverage and BPJS insurance, delays in care-seeking, transport, referral, and a newly identified “fourth delay”— administrative and digital barriers in the Maternal Death Notification (MDN) system. COVID-19 further strained services through ambulance delays, oxygen shortages, and MDN system interruptions. Indirect causes—such as asthma, tuberculosis, and cardiomyopathy—featured prominently, reflecting a shift in maternal mortality epidemiology. While community innovations (eg, mobile ultrasound, WhatsApp triage) were noted, structural and training gaps persist.
Conclusion: Maternal mortality in Garut reflects systemic gaps across health and reporting systems, including the newly identified fourth delay (digital barriers), rather than individual lapses. To achieve SDG targets, Indonesia must invest in digital resilience, integrated chronic disease services during ANC, equitable transport infrastructure, and respectful maternity care. A robust, real-time MPDSR system that includes maternal deaths outside of facilities is essential. Maternal survival depends on aligning national commitment with district-level readiness and action.
Keywords: maternal mortality, death surveillance, MDN system, qualitative study, maternal mortality, digital delay
Introduction
Maternal mortality remains an important global public health issue, with the vast majority of deaths occurring in low- and lower-middle-income countries (LMICs). In 2017, the global maternal mortality ratio (MMR) was estimated at 211 per 100,000 live births (80% uncertainty range of 199–243), representing a 38% reduction since 2000.1 Despite this progress, the burden remains unequally distributed, and countries like Indonesia—classified as a lower-middle-income country—continue to report relatively high numbers of maternal deaths.2,3
According to official surveillance data, Indonesia recorded 4627 maternal deaths in 2020, which increased sharply to 7389 in 2021, marking a 59% rise.4 West Java Province, although relatively well-resourced, reported 1204 maternal deaths in 2021, the second-highest figure among all provinces.4 Globally, maternal mortality is influenced by a combination of distal socio-economic factors—including poverty, women’s education, and gender norms—and health system determinants such as service availability, quality of care, and the effectiveness of referral effectiveness.5
The widely applied “Three Delays” model describes how delays in seeking, reaching, and receiving care contribute to maternal deaths. However, emerging evidence suggests that health information systems themselves may contribute as a “fourth delay”, whereby digital bottlenecks hinder timely reporting and response. In Indonesia, the Maternal Death Notification (MDN) platform was introduced in 2019 to strengthen Maternal Death Surveillance and Response (MDSR), yet concerns remain regarding underreporting and delayed data entry, particularly in remote districts.
Garut Regency, a partly remote, mountainous district located 66 kilometers southeast of Bandung, exemplifies these challenges. With a population of approximately 2.79 million and a mixed healthcare infrastructure, Garut reported 50 maternal deaths in 2024, contributing to West Java’s 749 maternal deaths that year.6 These figures suggest both high burden and potential underreporting relative to local estimates shared during Maternal Perinatal Death Notification (MPDN) meetings.
Previous qualitative studies in Indonesia have explored the clinical and systemic causes of maternal deaths, little is known about underreporting, the role of digital barriers, and the perspectives of families, frontline providers, and district registrars. Understanding these perspectives is essential for identifying gaps in surveillance and strengthening the implementation of MDN and MDSR, particularly as Indonesia works toward achieving the Sustainable Development Goal (SDG) target of reducing the MMR to no more than 70 per 100,000 live births by 2030.7
This study investigates the circumstances surrounding recent maternal deaths in Garut Regency and to critically examine the performance of the local MDN system. It documents the experiences of bereaved families, frontline midwives, and the district registrar, aiming to uncover sociocultural and health service factors preceding each death, identify reporting challenges—including the newly identified “fourth delay” in digital reporting—and provide actionable insights for improving MDSR processes and informing a forthcoming mixed-methods implementation study.
Methods
Paradigm and Design
This study employed a qualitative interpretive–constructivist approach, grounded in the view that knowledge is co-constructed through interaction between participants and researchers. This approach was chosen to understand participants’ lived experiences and the meanings they attach to events, while recognizing the role of researcher interpretation in shaping knowledge. The research team comprised a multidisciplinary group, including an obstetrician, a midwife researcher, and a health systems scientist7. The study protocol, data analysis, and reporting were guided by the Consolidated Criteria for Reporting Qualitative Research (COREQ) framework.
Study Setting
Garut Regency, located in West Java Province, consists of 42 subdistricts served by 42 public primary health centres (Puskesmas) and two Type C referral hospitals. Internet connectivity is inconsistent, with patchy 3G/4G coverage, particularly in remote highland areas. Basic Emergency Obstetric and Neonatal Care (BEmONC, locally known as PONED) services are provided in 12 Puskesmas, while ambulance transfers from remote villages often take more than 60 minutes (see Figure 1). Garut has a population of approximately 2.6 million, with maternal health infrastructure including midwives in each village and two hospitals capable of comprehensive emergency obstetric care.
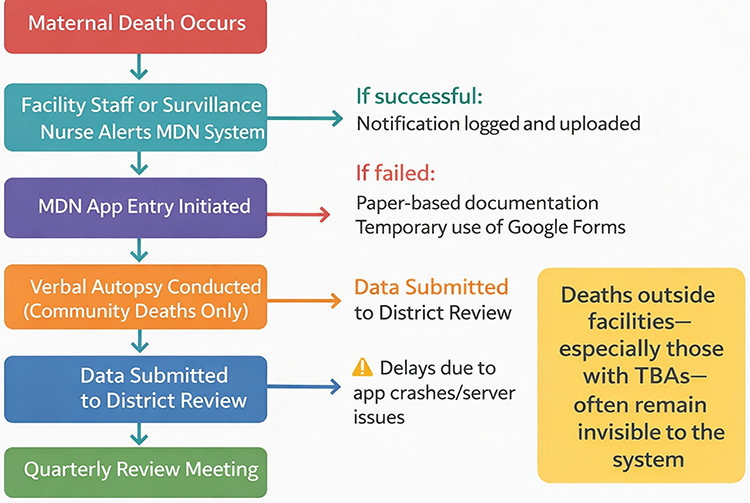 |
Figure 1 Process flow of the MDN system, highlighting systemic bottlenecks and infrastructure limitations that delay accurate maternal death reporting and learning. |
Sampling Strategy
We applied a maximum variation purposive sampling approach to capture diverse perspectives across key stakeholder groups. Participants included:
- Bereaved family members—specifically, the main caregiver (husband or mother-in-law) involved in each of three maternal death cases occurring between January 2022 and January 2023. The limited number of family cases was determined by ethical considerations and the goal of achieving information power sufficient for thematic saturation.
- Frontline providers—four village midwives and two coordinating midwives from the involved Puskesmas; and
- The district registrar—the MPDSR focal person responsible for monitoring and ensuring data quality within the Maternal Death Notification (MDN) system. Sampling was continued until information power was deemed sufficient. After nine interviews, no new codes emerged during analysis, indicating thematic saturation.
Recruitment and Consent
Eligible bereaved families were introduced by Puskesmas midwife coordinators, while the midwives and register were approached directly by the research team. We acknowledge that involving coordinators as first points of contact could introduce potential gatekeeper bias, as their organisational role may influence which families felt able or comfortable to participate. To minimise this risk, coordinators were explicitly instructed only to provide information about the study and to avoid recommending or discouraging specific families. Interested families contacted the research team independently. This mitigation strategy was discussed during peer-debriefing and documented in the reflexive journal. All families approached agreed to participate, and no individuals declined or withdrew after providing informed consent. All participants were provided with a written information sheet and gave informed written consent, which covered audio recording, anonymised use of quotations, and the right to withdraw participation at any point before transcript validation.
Data Collection Procedures
Data collection took place between May and June 2023. In-depth interviews were conducted in Bahasa Indonesia by INK, a female midwife with a master of Midwifery degree, who had no clinical relationship with participants. Interviews were held at the participant’s home or workplace, depending on their preference. All interviews were conducted privately; no non-participants (eg, other family members or colleagues) were present during the sessions. Participants were informed that the interviewer was a public health researcher seeking to understand barriers in maternal mortality reporting and to document family perspectives. A semi-structured interview guide explored key domains, including (a) events leading up to the maternal death, (b) decision-making and support processes, (c) experiences with referral and death reporting, and (d) suggestions for improving the MDN/MPDSR system. Each session lasted approximately 60 to 90 minutes, was audio-recorded with permission, and supplemented with detailed field notes. Transcripts were produced verbatim within 48 hours. Interview transcripts were originally produced in Bahasa Indonesia and subsequently translated into English by a bilingual qualitative researcher. A back-translation procedure was conducted for 20% of the dataset by an independent translator to ensure accuracy of meaning; any discrepancies were reviewed collaboratively and resolved through team discussion. Final translated quotations were checked against original transcripts to maintain contextual fidelity. Reflexive notes were kept throughout the process to document how the interviewer’s positionality and perceptions may have shaped interactions and interpretation.
Ethical Considerations
The study was approved by the Padjadjaran University Health Research Ethics Committee (No. 733/UN6.KEP/EC/2022) and was conducted in accordance with the principles of the Declaration of Helsinki. Phone counselling was offered to bereaved families; however, none requested this service. All patient data were fully de-identified and stored on password-protected drives to ensure confidentiality.
Participant Characteristics
A total of nine participants were interviewed, representing three key stakeholder groups: bereaved family members, frontline healthcare providers, and the district MPDSR registrar. The family group included two husbands (aged 32 and 28 years) and one mother-in-law (aged 54 years), each of whom had lost a close relative due to maternal death between January 2022 and January 2023. The reported places of death varied: one occurred at a Type A hospital, one during transit to care, and one at a Type B hospital.
Five midwives participated as frontline providers: three were village midwives with 6–17 years of experience, and two were coordinating midwives from local Puskesmas, each with over a decade of service. These providers were directly involved in the maternal death cases under investigation and offered insights into service delivery, referral pathways, and the notification process. One district-level informant, the MPDSR focal person, was also interviewed. This participant, a 45-year-old woman with 20 years of experience in the health system, was responsible for managing MDN data quality and overseeing maternal death surveillance in Garut Regency.
This diverse participant group enabled exploration of maternal deaths from multiple perspectives: the lived experiences of grieving families, the operational realities faced by midwives in both community and facility settings, and the systemic challenges observed by a registrar responsible for death reporting and data accuracy. Table 1 summarises participant demographic and professional characteristics.
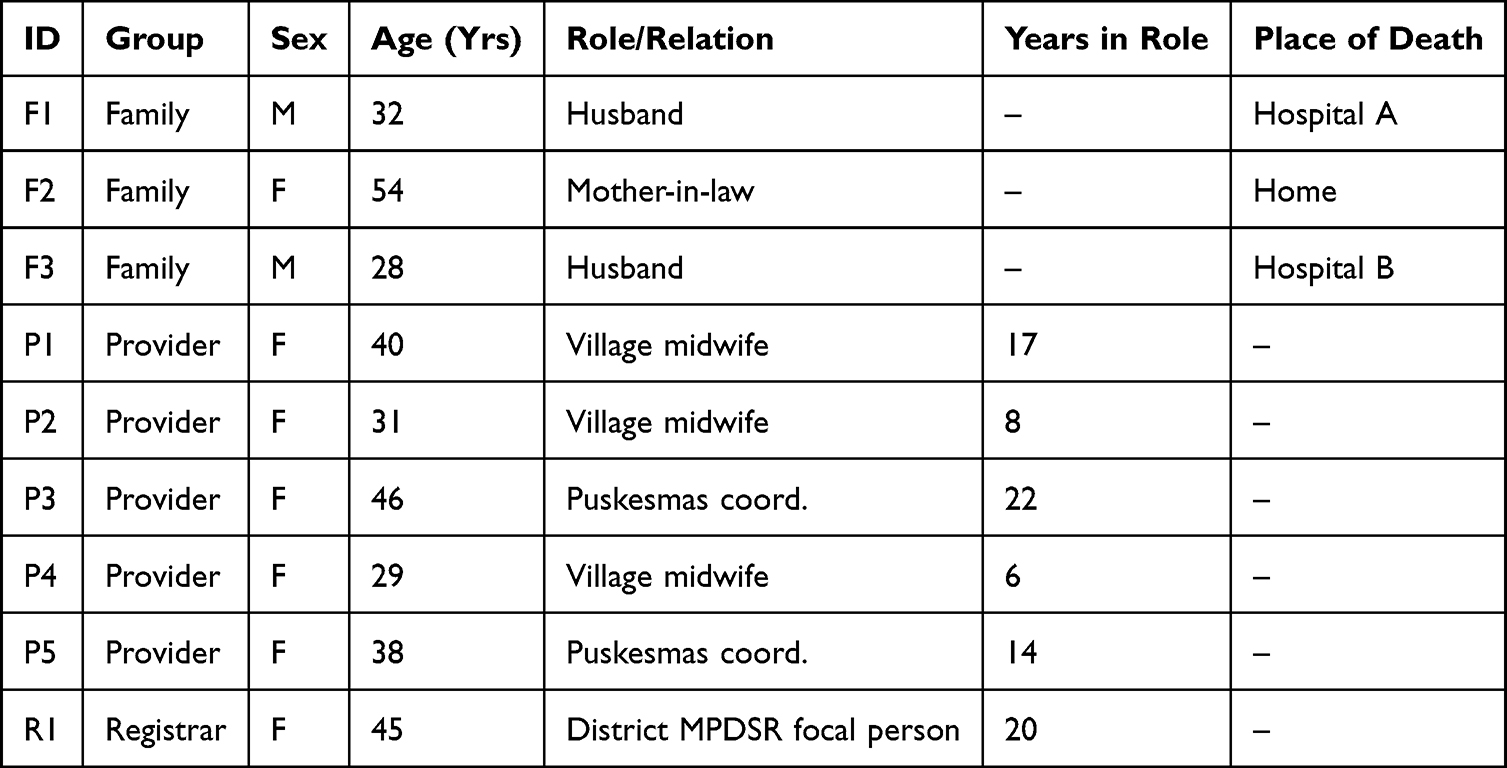 |
Table 1 Summarises Demographic and Professional Details |
Data Analysis
Data coding and thematic development were supported by NVivo 14™ software. We employed Braun and Clarke’s six-phase reflexive thematic analysis approach, which provided a structured yet flexible framework for exploring patterns across the dataset (see Table 2). The primary coding was conducted by INS, who undertook the first cycle of open, inductive coding, identifying both semantic and latent meanings. Consistent with the interpretive–constructivist paradigm underpinning Reflexive TA, no inter-coder reliability statistics were calculated, as the analytical process emphasised depth of interpretation rather than coder interchangeability. Instead, a second qualitative researcher reviewed the evolving code structure and offered critical feedback through reflexive dialogue to enhance analytic rigor. An audit trail of coding decisions was maintained in Microsoft Teams.
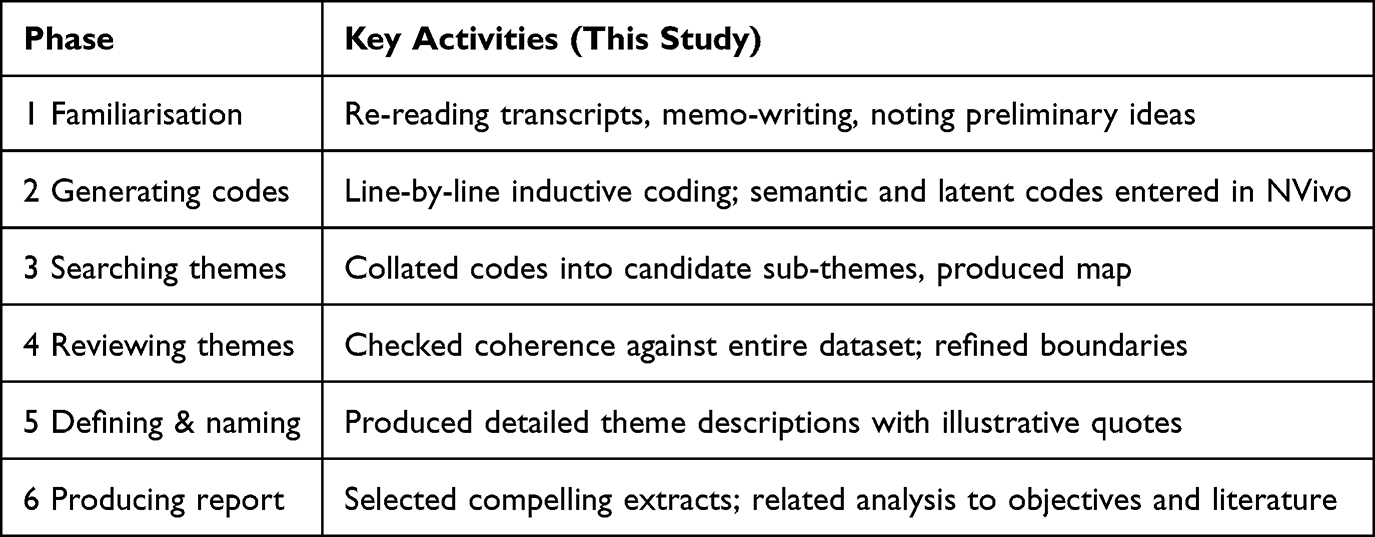 |
Table 2 Alignment of Analytic Activities with Braun & Clarke Phases |
The analytic process began with repeated reading of transcripts and memo writing to support immersion and early idea development. In the second phase, line-by-line coding was applied to capture both explicit content and underlying meaning. Codes were then grouped into candidate sub-themes, and visual mapping techniques were used to explore connections. Themes were iteratively reviewed for coherence and refined based on their consistency across the dataset. The final themes were clearly defined and named, with each supported by rich, illustrative quotes from participants (Supplementary Table 1). In the final phase, we selected compelling extracts that captured the essence of each theme and related our findings back to the study objectives and relevant literature.
Rigour and Reflexivity
Rigour in this study was established through a combination of methodological strategies rooted in established qualitative research principles. We enhanced credibility by conducting member-checking, whereby participants were provided with one-page summaries of their interviews for review. This process allowed them to confirm the accuracy of interpretations and, where needed, clarify or expand on their experiences. Additional credibility was gained through peer debriefing sessions with an independent qualitative expert not involved in data collection or initial analysis, which helped challenge assumptions and identify potential blind spots in interpretation.
A strong sense of transferability was supported by detailed contextual descriptions of the Garut health system, including infrastructure gaps, referral barriers, and local sociocultural dynamics. By presenting thick description alongside direct quotations from participants, we aimed to enable readers to judge the relevance of findings to other low- and middle-income country (LMIC) contexts.
Efforts to ensure dependability were reflected in systematic documentation of all analytic procedures. An external qualitative researcher reviewed the evolving codebook and assessed the rationale behind coding decisions. All raw data, coded transcripts, analytic memos, and team reflections were archived in secure, version-controlled Microsoft Teams folders to maintain a transparent and auditable trail.
Reflexivity was integrated throughout. The lead interviewer (INK) maintained a reflexive journal to capture her positionality, perceptions, and interactional dynamics. The research team engaged in regular discussions to acknowledge subjectivities and minimize interpretive bias. These reflexive discussions were documented and revisited during later stages of analysis to support transparency and integrity.
Result
Analysis generated three interrelated themes reflecting the multi-layered contributors to maternal mortality and under-reporting in Garut Regency: (1) the support system surrounding women, (2) the actions and constraints of healthcare providers, and (3) the architecture of maternal death recording and reporting. In contrast to existing literature that has broadly highlighted delays in care, our findings underscore a locally specific dimension: digital and systemic barriers in maternal death reporting, which emerged as a novel “fourth delay”. Each theme is presented alongside relevant analytic categories, integrating verbatim quotations that participants identified as representative of their experiences. Prior to detailing each theme, a comparative overview of family and provider perspectives on barriers to maternal survival and system functioning is provided in Table 3. In addition to these major themes, several minor but diverse themes also emerged, such as referral barriers, difficulties in information access, challenges in recording and reporting processes, and variations in health service quality. Although less frequent, these insights provided valuable nuance and are reflected in Table 3.
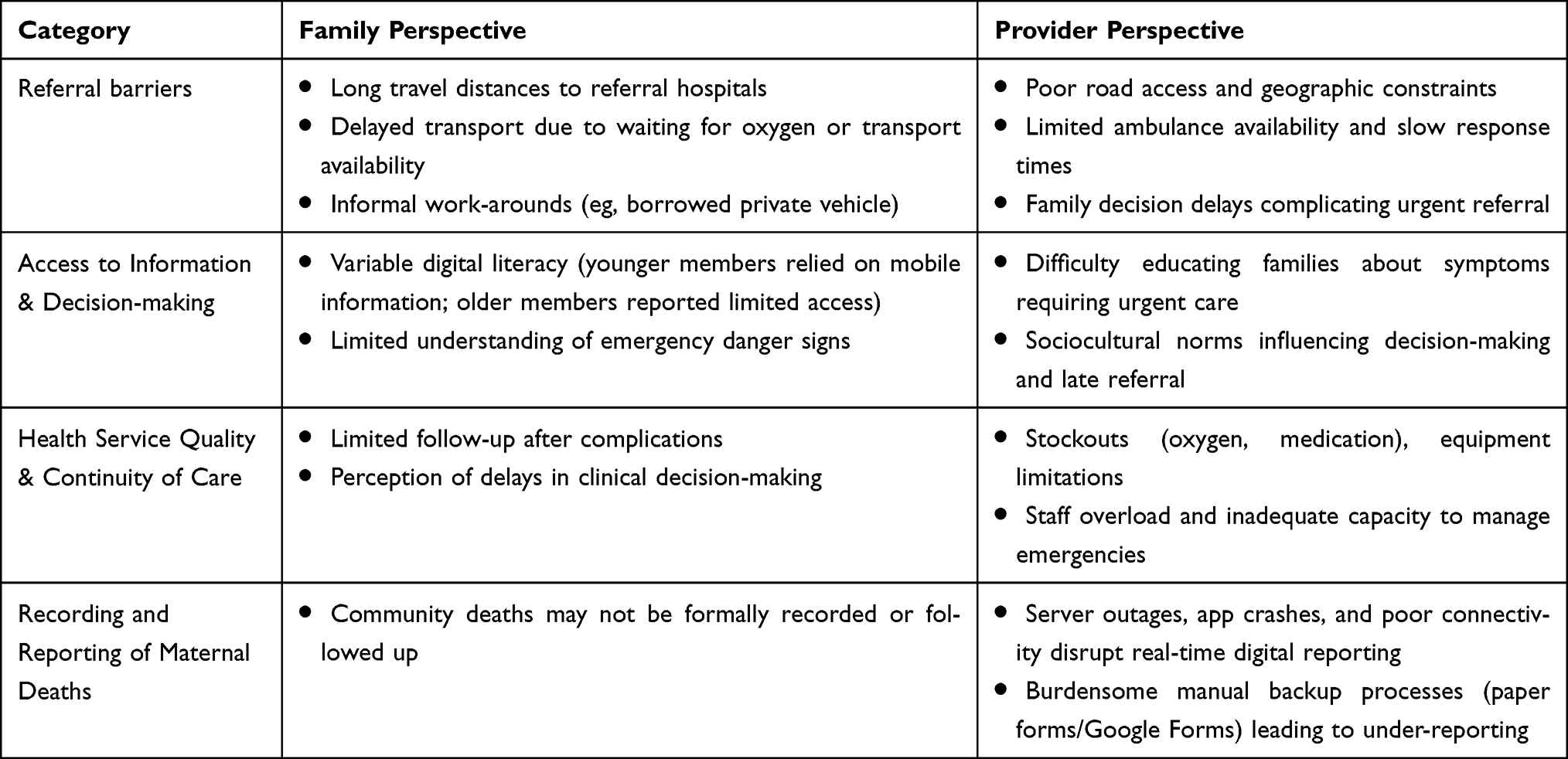 |
Table 3 Comparison of Family and Provider Perspectives on Barriers to Maternal Survival and System Function |
The Support System Surrounding Women
Families demonstrated strong emotional, logistical and financial support systems, which challenge common assumptions that poor family mobilisation drives maternal mortality. However, systemic obstacles ultimately undermined maternal survival. For example, although families rapidly coordinated transport and blood donors, delays stemmed from facility-level constraints such as oxygen shortages and slow referral activation. These infrastructure-related barriers extended response times beyond the family’s control, illustrating the interdependence between individual action and systemic readiness.
Healthcare-Service Accessibility
All three families reported routine care across multiple entry points—Posyandu, village midwives, Puskesmas, private doctors, and PONED facilities: “(She) periodically went to the Posyandu” (R1). A sibling confirmed, “Yes, she frequently went to the Posyandu, to the doctor, to the midwife” (R3).
Family Support Mechanisms
Practical help was conspicuous. Supplies for the expected baby had been bought “two months beforehand” (R8); blood donors were mobilised instantly, “all relatives willingly assisted” (R8). Transport, although improvised—“We used a borrowed car” (R1)—was never withheld. Each woman was also insured through the national BPJS scheme: “For childbirth we used BPJS” (R8).
Family Acceptance of Death
Families described religiosity and frustration with systemic delays: “…the critical situation involved family and parents together” (R1). Emotional responses spanned calm religiosity—“There is nothing to be done, this is fate” (R8)—to muted anger over perceived system delay—“Why not from earlier?” (R1).
Access to Health Information
Digital literacy also shaped families’ ability to interpret clinical symptoms and seek timely care. A younger husband “often searched on the phone” (R3), whereas older respondents reported limited access “Rarely” (R8), reflecting generational divides in recognising danger signs.
Maternal Complaints
Families recalled prodromal signs: facial erythema and pruritus (“red and itchy” [R1]); sudden dyspnoea (“shortness of breath” [R3]); severe hypertension (BP 180 mm Hg, R8); and dizziness.
Encountered Barriers
Three recurrent obstacles lengthened response times: waiting for oxygen because a clinic had none (“only waiting for the oxygen” [R1]); postponing the first doctor visit until 8 months gestation (“she insisted on waiting” [R3]); and a background of renal disease in mother and siblings.
Referral Procedures
One woman bypassed the health centre entirely: “She didn’t go to the Puskesmas first” (R1), yet was transported in a Puskesmas ambulance, underscoring informal work-arounds.
Chronology of the Fatal Episode
Delayed referral from a midwife’s surgery resulted in cardio-respiratory collapse in the ambulance: “When the midwife opened the door she was already unconscious” (R1). Another woman with proteinuria, dyspnoea and vomiting deferred hospital care until the night she decompensated (R3). A third arrived at Puskesmas with active haemorrhage; the fetus was found dead in hospital, the mother underwent two laparotomies and died 5 h later (R8).
Nutritional Intake Patterns
Rather than indicating mere lifestyle variation, reports of diverse diets— “I enjoy meat; I often eat it” (R3) — challenge simplistic narratives of maternal mortality as a result of malnutrition, instead directing analytic attention toward acute complications and systemic referral failures. Ultimately, strong family support alone was insufficient to navigate fragmented care pathways, revealing what participants perceived as preventable delays beyond their control.
Healthcare Provider Perspective
Providers identified both competencies and systemic constraints affecting maternal survival. They consistently emphasized the gap between established referral protocols and on-the-ground realities such as transport delays, limited ambulance access, and sociocultural factors influencing decision-making.
Knowledge
Midwives defined maternal death as “death during pregnancy, childbirth or the postpartum period” (R2, R7) and recognised cessation of breathing as the final common pathway (R6).
Skill/Competency Constraints
Lifestyle counselling sometimes clashed with local habits (“we advise reducing savoury foods” [R7]). Providers struggled with undocumented migrants, damaged roads, scarce ambulances and family decision delays. One midwife lamented, “The community is difficult to manage, so referral becomes challenging” (R6).
Midwifery Care
Emergencies and lack of follow-up were cited together: “It happens because there is an emergency or no follow-up” (R7). Hypertensive disorders of pregnancy, short inter-pregnancy intervals (<2 y), eclampsia, haemorrhage, infection, PPCM, malnutrition, tuberculosis and extreme maternal ages were all named as proximate causes (R5–R7).
Quality-Improvement Efforts
Reported actions ranged from ANC outreach, ULIN mobile ultrasonography and WhatsApp triage groups to Jampersal financial protection and MELANI high-risk screening. Yet the same providers recounted catastrophic failures: “No contractions, continuous bleeding… the patient died during transport” (R6) and “asthma with CED and anaemia… she bled and had difficulty breathing, then died” (R5).
The Architecture of Death Recording and Reporting
A key novel contribution lies in identifying “digital reporting delays” as a distinct barrier. Maternal deaths in Garut are recorded through the national Maternal Death Notification (MDN) system. Facility-based deaths trigger an automated alert in the MPDN platform, followed by a verbal autopsy and medical record upload by the surveillance nurse. For community deaths, the nurse must first visit the family and reconstruct the antenatal care chronology: “First we visit the family… then trace the ANC chronology” (R9). Upload is completed via the national MPDN mobile app. However, server overload and limited internet connectivity in remote areas frequently necessitate temporary reversion to paper forms or Google Forms.
While quarterly and annual review meetings are held to reflect on aggregated maternal death review (MDR) data, persistent under-reporting was evident, particularly for community deaths outside health facilities. The district officer noted that, “Deaths outside facilities, especially with traditional birth attendants, are likely unreported” (R9). Figure 1 illustrates the reporting workflow and highlights multiple points of delay, including app crashes, server issues, and connectivity limitations. This complements the Four Delays model (Figure 2) by expanding it to include administrative and digital obstacles, thus offering a novel conceptual refinement for maternal mortality surveillance.
 |
Figure 2 Adapted Four Delays Model showing Systemic and Structural Contributors to Maternal Mortality in Garut Regency, Indonesia. |
Although participants recognised the importance of timely maternal death reporting, they also described repeated disruptions caused by server downtime, unstable internet access and temporary reversion to manual reporting methods. These reporting bottlenecks created uncertainty and slowed coordinated response efforts, particularly for deaths occurring outside health facilities. Participants perceived these administrative and digital constraints as extending the timeline for case verification and review, which in turn limited opportunities to prevent recurrent deaths. While not originally conceptualised within the classic Three Delays model, these findings suggest an emerging dimension related to system accountability and real-time information flow, indicating the potential value of considering a “fourth delay” associated with digital and bureaucratic barriers.
Discussion
This exploratory qualitative study provides context-specific insights into the ongoing maternal health challenges in Garut Regency, where maternal mortality persists despite national reforms. While Indonesia has made substantial progress, the national maternal mortality ratio (MMR) continues to lag behind regional benchmarks, and the SDG target of reducing MMR to 70 per 100,000 live births by 2030 remains challenging to achieve.7 Our findings contribute local perspectives from families, health providers, and district registrars, particularly regarding the operation of the Maternal Death Notification (MDN) system. We emphasise that findings are drawn from a small purposive sample in one district and should therefore be interpreted as exploratory evidence that may generate hypotheses for wider investigation rather than as definitive proof of national trends.
Although maternal deaths are predominantly concentrated in under-resourced eastern provinces, Garut’s persistently high mortality rate, despite its location in the better-resourced Java-Bali corridor, highlights entrenched subnational disparities.8,9 West Java is among the highest contributors to national maternal mortality, and Garut exemplifies how geographic and systemic inequities can persist even within high-coverage regions.6
Key Findings and Family Perspectives
Families reported difficulties recognizing complications, reaching health facilities in time, and navigating referral pathways, often relying on informal social support networks. These narratives illustrate how social support can buffer—but not fully overcome—structural barriers. Midwives and district stakeholders described operational challenges, including heavy workloads, inconsistent supervision, supply chain disruptions, and limited training opportunities. Importantly, failures in the MDN system—including server crashes, data backlogs, and connectivity problems—emerged as a novel “digital/systemic delay”. This finding directly correlates with the study’s objective of examining underreporting and surveillance gaps.
Comparison with Literature and Mechanisms
The COVID-19 pandemic exacerbated these challenges. Between 2020 and 2022, respondents described how service disruptions—ranging from delayed ambulance dispatch and oxygen stockouts to server crashes in the Maternal Death Notification (MDN) system—magnified existing vulnerabilities.10,11 Our analysis, integrating perspectives from families, midwives, and district-level stakeholders, aligns with the established Three Delays framework.12 Participants described barriers in care-seeking, logistical access, and facility-level response.
Notably, our study surfaced a fourth, emerging delay: digital breakdown. Failures in the MDN platform during peak periods delayed death audits and feedback loops, limiting timely learning and undermining surveillance efficacy. These local challenges mirror global patterns, where maternal outcomes during the pandemic were shaped not only by infection risk but also by systemic resilience; for instance, a retrospective study of cesarean sections found that unvaccinated pregnant patients infected with SARS-CoV-2 had higher ICU admissions and maternal complications, whereas vaccinated patients fared markedly better.13 Together, these findings emphasize that maternal survival depends on both the robustness of clinical care and the strength of system-level support—including timely service delivery, functional digital reporting, and preventive measures such as vaccination.
These findings resonate with broader international evidence on how health systems mediate maternal and perinatal outcomes under pressure. For instance, during the COVID-19 pandemic, studies among Syrian refugees in Turkey reported that, despite significantly lower antenatal care coverage, perinatal and neonatal outcomes were largely comparable to those of the host population—a reflection of the Turkish health system’s resilience and ability to buffer vulnerable groups.14 In contrast, the Garut context illustrates the opposite pattern: even with relatively high antenatal care coverage and near-universal health insurance, systemic breakdowns—particularly in transport, referral pathways, and digital reporting—undermined timely response and contributed to persistently high maternal mortality. Together, these contrasts highlight that maternal survival is not determined by coverage alone, but by the depth of system resilience, responsiveness, and equity in practice.
The causes of maternal mortality are evolving. While obstetric haemorrhage, hypertensive disorders, and sepsis remain predominant, chronic conditions such as asthma, tuberculosis, cardiomyopathy, and renal disease are increasingly implicated.15 Indirect causes now account for nearly 49% of maternal deaths in Indonesia, a marked rise from 10% in 1990.8 These epidemiological shifts necessitate an expanded focus in antenatal care (ANC), incorporating screening and management of non-communicable diseases (NCDs), in alignment with WHO and national guidelines.9,16
Policy Implications
Although health insurance coverage through BPJS is near-universal among study participants, financial access alone did not ensure service utilisation. Geographic factors—such as steep terrain, long travel distances, and poor road infrastructure—emerged as major determinants of delayed care, particularly in remote subdistricts. These findings support the need for subsidized maternal transport schemes and targeted investment in rural infrastructure.17
Midwives were identified as highly resourceful yet overstretched frontline actors. Community-level innovations, including WhatsApp triage groups, ULIN mobile ultrasound, MELANI high-risk screening, and Jampersal-funded integrated services, were frequently highlighted. However, service delivery was constrained by inconsistent supervision, supply chain disruptions, and variable training quality. These gaps point to the importance of structured mentorship models and peer learning platforms across districts.9
Our findings also align with broader maternal health frameworks. McCarthy and Maine’s conceptual model of proximate, intermediate, and distal determinants is evident, particularly where distal factors such as digital systems and geographic barriers directly influenced clinical outcomes.12 Similarly, Cameron et al’s framework—which locates maternal mortality within broader social and systemic realities—is supported by narratives reflecting both structural barriers and community-level agency.18
Garut’s MDN system is relatively well-structured, with established protocols for home visits, verbal autopsies, and routine audits. However, recurrent challenges—including server overload, weak connectivity, and data-entry backlogs—were widely reported. Stopgap solutions, such as paper-based forms and Google Forms, were commonly used but undermined real-time data flow, reducing system responsiveness.
Community narratives revealed both strengths and weaknesses in facility-based care. While participants valued the affordability of services and presence of qualified staff, concerns were raised about long wait times, limited privacy, drug stockouts, and perceived lack of respectful treatment. These perceptions can significantly influence health-seeking behaviour and must be considered in quality improvement and respectful maternity care initiatives.
From a policy perspective, Indonesia has made notable progress through the WHO Country Cooperation Strategy (2019–2024), Joint External Evaluation initiatives, and partnerships with USAID MCGL.9,19 However, without equitable subnational financing and better coordination between national and district authorities, national-level progress may obscure persistent local stagnation. These findings may offer useful considerations for policymakers and programme implementers working in comparable resource-constrained districts. Potential areas for exploration include strengthening maternal transport schemes, improving infrastructure reliability, supporting digital readiness for MDN reporting, and enhancing mentorship models for midwives. Further research across multiple settings would be valuable to test whether similar constraints emerge elsewhere.
Limitations and Future Research
This study provides rich qualitative insights but has some limitations. Conducted in a single district, findings may not be generalizable to areas with different infrastructure or sociocultural contexts. Social desirability bias may have influenced responses, particularly among providers with pre-existing relationships with participants. The study also did not include direct clinical observation, which could have offered additional insight into decision-making and emergency responses. Despite these limitations, methodological strengths—including purposive sampling, triangulation of respondent types, use of verbatim quotations, and linkage with official MPDN records—support the credibility and trustworthiness of the findings. Future research should evaluate the effectiveness of digital MDN improvements, community-based interventions, and expanded ANC programs incorporating chronic disease management. Quantifying the impact of family and community support on maternal survival would further strengthen the evidence base for policy interventions.
Conclusion
Maternal mortality in Garut Regency illustrates ongoing challenges in timely access to care and system responsiveness. This exploratory qualitative study identified barriers including transport difficulties, staff shortages, referral delays, and interruptions in reporting processes. Participant narratives also pointed to an emerging concern around administrative and digital failures within the MPDSR system, proposed here as a hypothesis-generating “digital delay” that requires further investigation rather than representing a definitive extension of existing delay frameworks. While respondents described system weaknesses, they also highlighted strengths such as high ANC coverage and BPJS enrolment, indicating potential leverage points for improvement. These findings offer contextual insights that may support efforts to strengthen emergency referral coordination and digital readiness within maternal death surveillance. Given the single-district setting and small sample size, transferability is limited. Future multi-site or mixed-methods research is needed to test whether similar patterns and the digital-delay concept appear in other regions and health system contexts.
Abbreviations
ANC, Antenatal Care; BEmONC, Basic Emergency Obstetric and Neonatal Care; BPJS, Badan Penyelenggara Jaminan Sosial (National Health Insurance Agency of Indonesia); CED, Chronic Energy Deficiency; COREQ, Consolidated Criteria for Reporting Qualitative Research; COVID-19, Coronavirus Disease 2019; LMICs, Low- and Middle-Income Countries; MDN, Maternal Death Notification; MDR, Maternal Death Review; MELANI, Monitoring and Early Detection of High-Risk Pregnancies (local acronym/program); MMR, Maternal Mortality Ratio; MPDSR, Maternal and Perinatal Death Surveillance and Response; MPDN, Maternal and Perinatal Death Notification (national online platform); NCDs, Non-Communicable Diseases; PONED, Pelayanan Obstetri Neonatal Emergensi Dasar (Basic Essential Obstetric and Neonatal Care); POSYANDU, Pos Pelayanan Terpadu (Integrated Service Post); Puskesmas, Pusat Kesehatan Masyarakat (Community Health Centre); SDG, Sustainable Development Goals; TBA, Traditional Birth Attendant; TPMB, Tempat Praktik Mandiri Bidan (the Independent Midwifery Practice); ULIN, Ultrasound Keliling (Mobile Ultrasound Program, Indonesia); USAID, United States Agency for International Development; WHO, World Health Organization.
Data Sharing Statement
The dataset used and /or analysed during the current study is available from the corresponding author on reasonable request.
Acknowledgment
The authors are grateful to Universitas Padjadjaran, West Java, Indonesia, for supporting the publication fees. We also thank all participants who took part in the study. We are grateful to the Garut District Health Office.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors are grateful to Universitas Padjadjaran, West Java, Indonesia, for supporting the publication fees.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. World Health Organization. World health statistics 2020: monitoring health for the SDGs, sustainable development goals. World Health Organization; 2020. Available from: https://www.who.int/data/gho/publications/world-health-statistics.
2. The World Bank. World bank country and lending groups. 2022. Available from: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups.
3. The World Bank. Lower middle income. 2022. Available from: https://data.worldbank.org/country/XN.
4. Pusat Data Dan Teknologi Informasi Kementerian Kesehatan RI. Profil Kesehatan Indonesia 2021. 2022. Available from: https://www.kemkes.go.id/downloads/resources/download/pusdatin/profil-kesehatan-indonesia/Profil-Kesehatan-2021.pdf.
5. Cameron L, Contreras Suarez D, Cornwell K. Understanding the determinants of maternal mortality: an observational study using the Indonesian population census. PLoS One. 2019;14(6):e0217386. doi:10.1371/journal.pone.0217386
6. Maternal perinatal death notification. 2025.
7. World Health Organization. Maternal mortality. 2021. Available from: https://www.who.int/europe/news-room/fact-sheets/item/maternal-mortality.
8. Syairaji M, Nurdiati DS, Wiratama BS, Prüst ZD, Bloemenkamp KW, Verschueren KJ. Trends and causes of maternal mortality in Indonesia: a systematic review. BMC Pregnancy Childbirth. 2024;24(1):515. doi:10.1186/s12884-024-06687-6
9. Suparji S, Nugroho HSW, Sunarto S, Prayogi AS. High maternal mortality rate in Indonesia: a challenge to be addressed immediately. PAMJ-One Health. 2024;14(13). doi:10.11604/pamj-oh.2024.14.13.44464
10. Ratna Dewi Puspita Sari S, Wardani DWSR, Bakri S, Tugiyono HB. Indonesian maternal mortality: a systematic review of three-level determinants 1992–2024. Kurdish Stud. 2024;12.
11. Sejati EN, Rosa EM, Pramesona BA. Trends and determinants of the maternal mortality ratio based on healthcare resources. Unnes J Public Health. 2023;12(1):1–13. doi:10.15294/ujph.v12i1.57020
12. Aeni N. Faktor risiko kematian ibu. Kesmas. 2013;7(10):453–459. doi:10.21109/kesmas.v7i10.4
13. Yeniocak AS, Tercan C, Dagdeviren E, Arabaci O, Arabaci EEG. Impact of SARS-CoV-2 infection and vaccination on cesarean section outcomes: a retrospective analysis. Ann Saudi Med. 2024;44(5):306–318. doi:10.5144/0256-4947.2024.306
14. Aktoz F, Tercan C, Vurgun E, Gelir BD, Polat I, Yucel B. Evaluation of perinatal and neonatal outcomes of syrian refugees compared to Turkish population: a snapshot during the COVID-19 pandemic. J Immigrant Minority Health. 2023;25(3):522–528. doi:10.1007/s10903-023-01470-9
15. Respati SH, Sulistyowati S, Nababan R. Analisis faktor determinan kematian ibu di kabupaten sukoharjo Jawa Tengah Indonesia. Jurnal Kesehatan Reproduksi. 2019;6(2):52–59. doi:10.22146/jkr.43463
16. Surat Edaran Kementerian Kesehatan Republik Indonesia Tentang Peningkatan Peran Rumah Sakit dalam Percepatan Penurunan Angka Kematian Ibu dan Angka Kematian Bayi. 2020.
17. Sukirman R, Wahyono TYM, Shivalli S. Determinants of healthcare facility utilization for childbirth in Kuantan Singingi regency, Riau province, Indonesia 2017. BMC Public Health. 2020;20(1):1–10. doi:10.1186/s12889-020-09035-3
18. Haryanto S. Sosiologi ekonomi. Yogyakarta: Ar-Ruzz Media; 2011.
19. World Health Organization. A woman dies every two minutes due to pregnancy or childbirth: UN agencies. World Health Organization; 2023:23.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.