Back to Archived Journals » Open Access Surgery » Volume 13
Pyloromyotomy in Hypertrophic Pyloric Stenosis: A Comparative Study Between Supraumbilical Curved Skin Incision and Standard (Right Upper Quadrant) Skin Incision: Study in a Resource Limited Setting
Authors Peyvasteh M, Askarpour S ![]() , Khoshkhabar M
, Khoshkhabar M ![]() , Javaherizadeh H
, Javaherizadeh H ![]()
Received 19 May 2020
Accepted for publication 21 September 2020
Published 19 October 2020 Volume 2020:13 Pages 79—83
DOI https://doi.org/10.2147/OAS.S262825
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Luigi Bonavina
Mehran Peyvasteh,1 Shahnam Askarpour,1 Mahmood Khoshkhabar,1 Hazhir Javaherizadeh2
1Department of Pediatric Surgery, Faculty of Medicine, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran; 2Alimentary Tract Research Center, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
Correspondence: Shahnam Askarpour
Department of Pediatric Surgery, Imam Khomeini Hospital, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
, Email [email protected]
Background: The main therapeutic option for hypertrophic pyloric stenosis (HPS) is pyloromyotomy surgical technique which can be performed via different methods, including right upper quadrant (RUQ) transverse incision and supraumbilical curved skin incision; thus, the aim of this study was to evaluate and compare clinical efficacy of supraumbilical curved skin incision and standard (RUQ) skin incision.
Materials and Methods: In this retrospective case-control study, 35 patients with HPS were initially evaluated. After evaluating hospital records, 31 patients with completed hospital records were included: 9 from case group and 22 from control group. Demographic information, surgery parameters and postoperative complications were extracted from the hospital records or calling parents.
Results: Results showed that the surgery parameters such as surgery duration (P=0.211), postoperative fasting duration (P=0.831), and hospitalization duration (P=0.521) in both groups were similar. Moreover, surgery complications such as duodenal or gastric perforation and surgical site infection did not differ between the groups (P> 0.05). While we found that Vancouver Scar Scale was significantly lower in supraumbilical curved skin incision as compared to control group (1.8 ± 0.5 vs 5.1 ± 0.7, P< 0.001, respectively).
Conclusion: The results of this study showed the beneficial effects of supraumbilical curved skin incision technique on surgery scar outcomes and gives best cosmetic results with minimal complications, which could be replaced to RUQ operative technique and significantly lead to better control of surgery scar.
Keywords: hypertrophic pyloric stenosis, supraumbilical curved skin incision, right upper quadrant transverse incision
Introduction
Hypertrophic pyloric stenosis (HPS) is a disorder causing hypertrophy and hyperplasia of pylorus wall, and incomplete mechanical obstruction. HPS is the one of the etiology of vomiting in infants (usually 10 to 30 min after feeding).1 The incidence of HPS is approximately 2 to 5 cases per 1000 live births, which is four times higher in male gender as compared to girls.2–4 The other main clinical symptoms except vomiting included visible peristaltic waves and olive-shaped lumps and finally causes severe malnutrition and death. Therefore, for a better prognosis results, early treatment is required.5
The main therapeutic option for HPS is pyloromyotomy surgical technique, was first described by Ramstedt in 1912, in which the hypertrophied pyloric muscle is divided and permits gastric to be empty.6 For seven decades, surgeons performed pyloromyotomy via different methods including midline or right upper quadrant (RUQ) transverse incision.7,8 In 1986, Tan and Bianchi showed that the supraumbilical curved skin can be used successfully in pyloromyotomy surgery for first time.9 Surgery through a supraumbilical curved skin incision9 subsequently became the choice method, as it tends to have better cosmetic outcomes.10 As to best of our knowledge, there is a limited about the efficacy of supraumbilical curved skin incision on pyloromyotomy surgical technique results, therefore, this study was designed to evaluate and compare clinical efficacy of supraumbilical curved skin incision and standard (RUQ) skin incision.
Materials and Methods
Study Design and Target Group
This retrospective case-control study was conducted in pediatric surgery department from November 2016 to May 2017. Study flowchart was seen in Figure 1. The surgical outcomes of patients underwent supra-umbilical curved skin incision (Figure 2) (cases group) were compared to patients underwent standard (RUQ) skin incision (control group) (Figure 3). Inclusion criteria consisted of patient referred to department of pediatric surgery department with a diagnosis of HPS (based on clinical examination, ultrasonography findings (muscle wall thickness ≥3 mm and pyloric channel length ≥14 mm in infants younger than 30 days). All surgical procedures was done by one experienced pediatric surgeon.
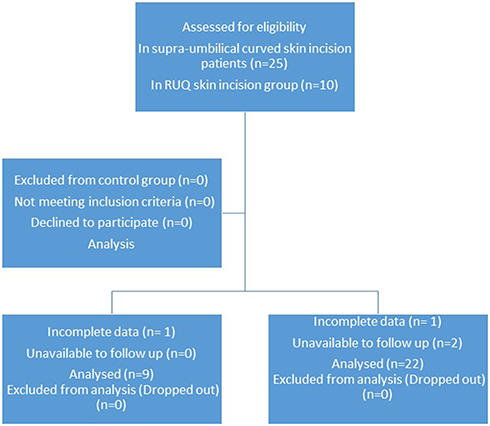 |
Figure 1 Study flow chart. |
 |
Figure 2 Supra-umbilical curved incision. |
 |
Figure 3 Classic incision. |
Follow up was done for all infant 6 months and 1 year after surgery. Duration of surgery was considered from incision to wound suturing.
Barium upper gastrointestinal study was done in cases that ultrasonography was not diagnostic. Parental patient informed consent to participate in the study was obtained. Exclusion criteria consisted of parental dissatisfaction with participation in the study, cases with defective hospital records, cases lost to follow-up. We also excluded patients with uncompleted data.
Participants
The study flowchart is shown in Figure 1. Thirty five patient’s hospital records with a diagnosis of HPS, who had been diagnosed by pediatric surgeon and based on clinical and para-clinical finding and inclusion and exclusion criteria were included.
Then, hospital records were divided into two pyloromyotomy surgery groups (supraumbilical curved skin incision and RUQ incision) based on the surgical description.
After evaluating hospital records, twenty nine patients with completed hospital records (after calling parents in cases with incomplete data) were included; 9 from case group and 22 from control group. The study received ethics approval from the Ethics Committee of Ahvaz Jundishapur University of Medical Sciences (IR.AJUMS.REC.1396.885).
Demographic information, duration of surgery, duodenal or gastric perforation occurrence during surgery, duration of hospitalization and postoperative fasting were extracted from the hospital records. Information on the surgical site infection was obtained by calling parents in addition to extracting from hospital records (because of the possibility of an infection after discharging from the hospital).
We used Vancouver Scar Scale11 for assessing the outcome of a surgical site by evaluating scar length (score 0-3), pigmentation (score 0-2), vascularity (score 0-3) and pliability (score 0-5) through photographs in the month 6 and 12 after surgery (these images were taken by the pediatric surgeons with the consent of the families).11,12
In summary, for performing open pyloromyotomy with supraumbilical curved skin incision, the skin, subcutaneous tissues, and fascia are undermined with diathermy dissection. Then the fascia is opened. The incision in the serosa of the pylorus is performed for exteriorization of the stomach with the pylorus. Then the muscle is split down to the submucosa. The stomach is replaced intra-abdominally. And finally linea alba is closed with absorbable interrupted sutures.
With Permission of Data Analysis
Data were analyzed and reported only for patients with completed information. Statistical analysis of data was performed using SPSS version 22 software (SPSS Inc., Chicago, IL, USA). Chi-square test was used to compare qualitative variables between groups. Kolmogorov–Smirnov test was used in order to evaluate the normal distribution of all quantitative studied parameters. Student’s t-test was used for variables with normal distribution, on the other hand Mann–Whitney and Wilcoxon tests were used for variables without normal distribution. The two tailed p-value less than 0.05 were considered significant.
Results
Demographic features in terms of age (P=0.233) and sex (P=0.121) in both groups were similar (Table 1). Six patients were dropped out and finally, 31 patients completed the study. Results showed that the surgery parameters such as surgery duration (P=0.211), postoperative fasting duration (P=0.831), and hospitalization duration (P=0.521) in both groups were similar. Moreover, surgery complications such as duodenal or gastric perforation and Surgical site infection (P>0.05) did not differ between the groups. While we found that Vancouver Scar Scale was significantly lower in supraumbilical curved skin incision as compared to control group (1.8 ± 0.5 vs 5.1 ± 0.7, P<0.001 respectively). Nausea and vomiting was seen in 3 children in both group.
 |
Table 1 Studied Variables During Different Periods of Time in Both Control and Supra-Umbilical Curved Skin Incision Groups |
Discussion
According to our results, supraumbilical curved skin incision had better effects on Vancouver Scar Scale as compared to traditional surgery incision method. However, the rate of surgery complications and other surgery parameters did not differ with traditional surgery incision method.
In the study performed by Teehan et al reported supraumbilical transverse midline skin incision as new method for HPS surgery with retraction of the two rectus muscles apart. This surgery incision method gives good exposure, and improves the delivery of the pylorus, with producing a strong closure, and giving a good cosmetic result.13 In another study performed by Ghaffarpour et al showed that the operating time with the supraumbilical incision with U-umbilicoplasty is not longer than in standard surgery method, the access to the abdomen is more than adequate, and furthermore the incidence of postoperative complications such as infection was similar and the cosmetic results were excellent.14 Eltayeb et al showed that supra-umbilical pyloromyotomy with intracavitary technique is safe and can be done in large pyloric masses or HPS without wound extension. Moreover, they demonstrated that this method gives best cosmetic results with minimal complications.15 In the term of scar outcomes Cozzi et al reported that 100% of families reported an excellent or good scar and finally concluded that overall satisfaction with the cosmetic outcome is very high.16 All these results are similar to our results. We found that supra-umbilical curved skin incision gives best cosmetic results with minimal complications and is similar to traditional surgical method, while the scar outcome was better than RUQ approach, which indicates that supraumbilical curved skin incision approach is much better than RUQ approach.
While, in an article published by Carrera et al showed that 22.2% of major complications occurred in the supraumbilical approach versus 2.6% in the RUQ approach, and 44.4% of minor complications were encountered in the supraumbilical approach versus 2.6% in the RUQ approach, which may due to more difficult delivery of the pylorus through the supraumbilical incision.17 Ladd et al showed that the rate of infection in RUQ approach was 2.3% and in supraumbilical approach was a statistically significant increase (7%), however, the use of prophylactic antibiotics reduced this rate of infection back to 2.3%.18 All these results were in contrast to ours, which may due to different sample size, different demographic features, and different periods of follow up. Furthermore, Kim et al demonstrated that circumumbilical technique is associated with the greatest mean operative time and costs as compared to laparoscopic pyloromyotomy and RUQ operative technique.19 However, we found higher surgery duration in supraumbilical approach, but this difference was not statically significant, which may due to different sample size. Therefore, another prospective clinical trial with higher sample size is needed in order to control confounding variables and divided patients into two groups bases on random methods.
In another study performed by Leinwand et al demonstrated that circumumbilical approach to pyloromyotomy was cosmetically superior to RUQ approach but increased complication rates such as postoperative complications, and wound infection. But they found that technical complications were easily corrected by the use of prophylactic antibiotics and length of stay was not affected.20 While we found superiority supra-umbilical curved skin incision technique without any increase in postoperative complications and wound infection.
We know that scar of laparoscopic pyloromyotomy is superior to open procedures,21 but the main limitation of this study was low resource setting and unavailable laparoscopy in our setting.
Limitation
Single center study and low sample size.
Conclusions
The results of this study showed the beneficial effects of supraumbilical curved skin incision technique on surgery scar outcomes and gives best cosmetic results with minimal complications, which could be replaced to RUQ operative technique and significantly lead to better control of surgery scar in the short term and increase the quality of life for long time.
Acknowledgments
This study was financially supported by Technology and Research Development Department of Ahvaz Jundishapur University of Medical Sciences, Ahvaz, south-east Iran. Data was used in this paper was from thesis of general surgery resident (Dr. Khoshkhabar). We gratefully acknowledge the dedicated efforts of the investigators, the coordinators, the volunteer patients who participated in this study.
Disclosure
The authors have indicated that they have no conflicts of interests regarding the content of this article.
References
1. Peeters B, Benninga MA, Hennekam RC. Infantile hypertrophic pyloric stenosis—genetics and syndromes. Nat Rev Gastroenterol Hepatol. 2012;9:646.
2. Feng Z, Nie Y, Zhang Y, et al. The clinical features of infantile hypertrophic pyloric stenosis in Chinese Han population: analysis from 1998 to 2010. PLoS One. 2014;9:e88925. doi:10.1371/journal.pone.0088925
3. Malcom III GE, Raio CC, Del Rios M, et al. Feasibility of emergency physician diagnosis of hypertrophic pyloric stenosis using point-of-care ultrasound: a multi-center case series. J Emerg Med. 2009;37:283–286. doi:10.1016/j.jemermed.2007.11.053
4. AlMaramhy HH. Is there a relation between pyloric muscle thickness and clinical and laboratory data in infants with hypertrophic pyloric stenosis? Indian J Surg. 2015;77:827–830. doi:10.1007/s12262-013-1021-2
5. Gotley LM, Blanch A, Kimble R, et al. Pyloric stenosis: a retrospective study of an Australian population. Emerg Med Australas. 2009;21:407–413.
6. Ramstedt C. Zur operation der angeborenen pylorusstenose. Med Klin. 1912;8:1702.
7. Dufur H. La sténose hypertrophique du pylore chez le nourrisson et son traitement chir surgical. Rev Chir. 1908;37:208.
8. Tan K, Bianchi A. Circumumbilical incision for pyloromyotomy. Br J Surg. 1986;73:399. doi:10.1002/bjs.1800730529
9. Safford SD, Pietrobon R, Safford KM, et al. A study of 11,003 patients with hypertrophic pyloric stenosis and the association between surgeon and hospital volume and outcomes. J Pediatr Surg. 2005;40:967–973. doi:10.1016/j.jpedsurg.2005.03.011
10. Ballouhey Q, Clermidi P, Roux A, et al. Differential learning processes for laparoscopic and open supraumbilical pyloromyotomy. Pediatr Surg Int. 2016;32:1047–1052. doi:10.1007/s00383-016-3920-3
11. Sullivan T, Smith J, Kermode J, Mclver E, Courtemanche DJ. Rating the burn scar. J Burn Care Rehabil.1990;11(3):256–260. doi:10.1097/00004630-199005000-00014.
12. Oliveira GV, Chinkes D, Mitchell C, et al. Objective assessment of burn scar vascularity, erythema, pliability, thickness, and planimetry. Dermatol Surg. 2005;31:48–58. doi:10.1097/00042728-200501000-00010
13. Teehan EP, Garrow E. A new incision for pyloromyotomy. Int Surg. 1993;78:143–145.
14. Ghaffarpour N, Svensson PJ, Svenningsson A, et al. Supraumbilical incision with U-u umbilicoplasty for congenital duodenal atresia: the Stockholm experience. J Pediatr Surg. 2013;48:1981–1985. doi:10.1016/j.jpedsurg.2013.06.028
15. Eltayeb AA, Othman MH. Supraumbilical pyloromyotomy: a comparative study between intracavitary and extracavitary techniques. J Surg Educ. 2011;68:134–137. doi:10.1016/j.jsurg.2010.09.008
16. Cozzi DA, Ceccanti S, Mele E, et al. Circumumbilical pyloromyotomy in the era of minimally invasive surgery. J Pediatr Surg. 2008;43:1802–1806. doi:10.1016/j.jpedsurg.2008.02.066
17. Carrera N, Cerda JA, Canizo A, et al. [Hypertrophic pyloric stenosis: comparison between transversal and supraumbilical incision]. Cir Pediatr. 2010;23:77–81. Spanish.
18. Ladd AP, Nemeth SA, Kirincich AN, et al. Supraumbilical pyloromyotomy: a unique indication for antimicrobial prophylaxis. J Pediatr Surg. 2005;40(6):
19. Kim SS, Lau ST, Lee SL, et al. Pyloromyotomy: a comparison of laparoscopic, circumumbilical, and right upper quadrant operative techniques. J Am Coll Surg. 2005;201:66–70. doi:10.1016/j.jamcollsurg.2005.03.020
20. Leinwand MJ, Shaul DB, Anderson KD. The umbilical fold approach to pyloromyotomy: is it a safe alternative to the right upper-quadrant approach? J Am Coll Surg. 1999;189:362–367. doi:10.1016/S1072-7515(99)00136-2
21. St Peter SD, Acher CW, Shah SR, et al. Parental and volunteer perception of pyloromyotomy scars: comparing laparoscopic, open, and nonsurgical volunteers. J Laparoendosc Adv Surg Tech A. 2016;26:305–308. doi:10.1089/lap.2015.0566
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.