Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
PVA Microsphere Injection Rhinoplasty with Surgical-Like Injection Technique for Asia Female Patients: A 30-Case Clinical Study
Received 26 February 2026
Accepted for publication 24 June 2026
Published 8 July 2026 Volume 2026:19 602177
DOI https://doi.org/10.2147/CCID.S602177
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Rungsima Wanitphakdeedecha
Fang Yang,1 Hong Xiao2
1Yestar Shenzhen Medical Beauty Hospital, 3024#, Middle Shennan Road, Shenzhen, People’s Republic of China; 2Department of Plastic Surgery, The Second Affiliated Hospital of Kunming Medical University, Kunming, 650000, People’s Republic of China
Correspondence: Fang Yang, Email [email protected]
Background: Asia females often have inherent nasal skeletal limitations, driving high demand for nasal augmentation. Surgical rhinoplasty involves prolonged recovery and high revision rates, while conventional hyaluronic acid (HA) injection is prone to nasal widening.
Objective: To evaluate the safety and efficacy of polyvinyl alcohol (PVA) microsphere injection combined with a surgical-like injection technique for nasal augmentation in Asia females, focusing on quantitative aesthetic indices and long-term stability.
Methods: Thirty Asia female patients undergoing PVA microsphere injection rhinoplasty were enrolled. The technique included two key steps: membranous nasal septum injection for nasal tip projection and nasal dorsum augmentation for height enhancement. Patients were followed up for 18– 24 months. Primary outcomes included nasal tip/dorsum aesthetic indices (nostril/nasal base ratio, nasolabial angle, nasofrontal angle, nasal root height difference) and morphology maintenance (no widening, regression rate). Secondary outcomes were patient satisfaction (10-point VAS, ROE questionnaire) and adverse events.
Results: All patients showed significant improvements in quantitative indices: nostril/nasal base ratio (0.42± 0.05 to 0.58± 0.04), nasolabial angle (85.3± 6.2° to 95.6± 5.8°), nasofrontal angle (135.2± 8.1° to 120.5± 7.3°), and nasal root height difference (2.1± 0.4 mm to 3.5± 0.7 mm) (all P< 0.001). No nasal widening occurred; 24-month regression rate was 8.3± 3.2%. Mean VAS score was 8.9± 0.7, and ROE score increased from 58.3± 6.5 to 89.6± 4.2 (P.001). Only three cases of transient erythema were reported, with no severe adverse events.
Conclusion: PVA microsphere injection combined with a surgical-like injection technique is a safe and effective option for Asia female nasal augmentation, significantly improving aesthetic indices, maintaining long-term stability (no widening, low regression), and achieving high patient satisfaction with minimal adverse events.
Keywords: injection rhinoplasty, PVA microspheres, Asia female patients, nasal aesthetic indices, morphology maintenance, patient satisfaction
Introduction
Nasal augmentation is one of the most popular aesthetic procedures among Asia female populations, primarily due to inherent skeletal characteristics such as a low and flat nasal dorsum, underprojected nasal tip, and weak nasal support structure.1,2 For decades, surgical rhinoplasty (for example, silicone implant and autologous cartilage graft) has been considered the gold standard for nasal augmentation; however, it is associated with several drawbacks, including prolonged recovery (2–4 weeks of edema and bruising), high revision rates (10–15%) due to implant displacement or capsular contracture, and potential intraoperative complications (eg, nasal septum injury and infection).3,4
In recent years, injectable fillers have gained widespread acceptance for minimally invasive nasal augmentation among Asia females, owing to their advantages of short recovery time, minimal invasiveness, and adjustable outcomes.5 Hyaluronic acid (HA) is the most commonly used injectable filler for nasal augmentation; however, its application in Asia female patients is limited by a high incidence of nasal widening (reported in 20–30% of cases)6 and unsatisfactory long-term stability. This phenomenon is attributed to the intrinsic properties of HA (high water absorption and moderate cohesiveness) and the weak nasal soft tissue support in Asia females—HA tends to diffuse laterally under the influence of facial dynamics and gravity, leading to a “broadened nose” appearance that compromises the aesthetic effect.7,8
Polyvinyl alcohol (PVA) microspheres, a new type of injectable filler composed of cross-linked PVA microspheres suspended in a hyaluronic acid matrix, have emerged as a promising alternative. PVA microspheres exhibit high cohesiveness, low water absorption, and excellent tissue adherence, which theoretically prevent lateral diffusion and nasal widening.9 Additionally, we developed a surgical-style injection technique that mimics the anatomical support principle of surgical rhinoplasty: first, augmenting the membranous nasal septum to establish a stable tip support, then elevating the nasal dorsum. This technique aims to address the root cause of nasal widening (lack of tip support) and enhance the long-term stability of the augmented nasal morphology, which is particularly valued by Asia female patients pursuing natural and durable aesthetic outcomes.
Previous studies on injectable rhinoplasty have often relied on subjective aesthetic evaluations, lacking quantitative data on key nasal angles and proportions.10 To address this gap, the present study adopted a comprehensive evaluation system including quantitative aesthetic indices (nostril/nasal base ratio, nasolabial angle, nasofrontal angle, nasal root height difference), morphological maintenance indicators (absence of widening, regression rate), standardized patient satisfaction scales, and systematic adverse event monitoring. The study aimed to evaluate the safety and efficacy of PVA microsphere injection combined with this surgical-like injection technique in 30 Asia female patients, with long-term follow-up (18–24 months) to verify the stability of nasal morphology and absence of widening.
Materials and Methods
Patients
This retrospective study was performed in accordance with the principles in Declarations of Helsinki and was approved by the Institutional Review Board (IRB) of [The Second Affiliated Hospital of Kunming Medical University] (IRB No.: [kmmu20230115]), and written informed consent was obtained from each patient. This waiver was granted because the present study was a retrospective observational analysis using only fully de-identified clinical data retrieved from archived medical records. No additional clinical interventions, examinations, or direct contact with patients were conducted, and no identifiable personal information was included in data analysis or manuscript presentation. All patient-related data were securely stored, anonymized, and strictly managed to guarantee full confidentiality and protect patient privacy throughout the research process.
A total of 30 Asia female patients who underwent PVA microsphere injection rhinoplasty between January and December in 2023 were included. Inclusion criteria: 1) Oriental ethnicity; 2) Female gender; 3) Age ≥18 years; 4) Desire for nasal augmentation due to low nasal dorsum and/or underprojected nasal tip (preoperative nostril/nasal base ratio <0.50, nasolabial angle nasofrontal angle >125°); 5) No history of prior nasal surgery or injectable filler treatment; 6) Willingness to complete long-term follow-up and undergo standardized evaluations. Exclusion criteria: 1) Pregnancy or lactation; 2) History of autoimmune diseases, coagulation disorders, or infections; 3) Allergies to PVA or hyaluronic acid; 4) Nasal anatomical abnormalities (eg, severe septal deviation) requiring surgical correction.
The 30 female patients had an age range of 21–45 years (mean age: 32.6 ± 5.8 years). The follow-up duration was 18–24 months (mean: 18.3 ± 4.1 months).
Materials
The injectable filler used in this study was PVA microsphere filler (product name: Bonita, IMIEK, CHINA), composed of 20% cross-linked PVA microspheres (particle size: 40–120 μm) suspended in 80% non-cross-linked hyaluronic acid (molecular weight: 1.2 × 106 Da). The product has been approved by the National Medical Products Administration (NMPA) of China (Registration No.: 20163132497) and meets the ISO 10993 biocompatibility standards.
Surgical-Style Injection Technique
All procedures were performed by the same senior plastic surgeon with more than 10 years of experience in injectable aesthetics and nasal anatomy. The entire injection process adopted a “single-entry point” approach to minimize tissue trauma and ensure precise filler placement, following the steps below:
Preoperative Preparation and Anesthesia
Positioning and Disinfection
The patient was placed in a supine position with the head slightly elevated (15–20°) to facilitate nasal visualization and reduce venous congestion. The nasal region (including the nasal tip, dorsum, columella, and surrounding 2 cm area) was disinfected with 0.1% iodophor (three passes) and covered with a sterile surgical drape, exposing only the nasal operative field.
Entry Point Marking
The nasal tip midpoint (apex of the nasal tip) was marked with a sterile surgical marker as the single entry point, ensuring symmetry and accessibility to both the membranous nasal septum and nasal dorsum.
Skin Puncture and Anesthesia
A 23G sharp needle was used to puncture the marked entry point perpendicularly (depth: 2–3 mm) to create a minimal skin opening (diameter <1 mm). The sharp needle was immediately withdrawn, and a 23G blunt-tip microcannula was inserted through the same opening. Under direct visualization and gentle palpation, the cannula was advanced to the target areas (membranous nasal septum and nasal dorsum deep layer) in a stepwise manner. A total of 0.2–0.3 mL of 2% lidocaine hydrochloride was injected in a retrograde manner: 0.1–0.15 mL for the membranous nasal septum region (distributed along the midline) and 0.1–0.15 mL for the nasal dorsum deep layer (along the nasal bone surface). The cannula was retained in situ for 2–3 minutes after anesthesia to allow sufficient local anesthetic effect and reduce injection-related pain.
Membranous Nasal Septum Augmentation (Tip Support and Projection)
Cannula Placement
Using the same 23G blunt cannula (without changing the entry point), the tip was advanced vertically along the midline of the membranous nasal septum to its base (depth: 1.8–2.2 cm), confirmed by tactile feedback (resistance from the septal cartilage, no vascular pulsation).
Surgical-Style Scaffold Construction
PVA microspheres were injected in a “tower-shaped” layered manner, mimicking the cartilage scaffold placement in surgical rhinoplasty:
Base Layer
A total of 0.2–0.3 mL of PVA microsphere was injected retrogradely at the inferior third of the membranous septum to establish a stable foundation, ensuring uniform distribution to avoid unilateral deviation.
Middle Layer
A total of 0.2–0.3 mL of filler was injected at the middle third of the septum to elevate the nasal columella, gradually increasing the projection height.
Apical Layer
A total of 0.1–0.4 mL of filler was injected at the superior third (near the nasal tip apex) to create distinct nasal tip defining points, with gentle pressure during injection to ensure tissue integration.
Total Dose and Shaping
The total injection volume for the membranous nasal septum was 0.5–1.0 mL (mean: 0.7 ± 0.2 mL). Immediately after injection, the surgeon used sterile gloves to perform bimanual shaping: the thumb and index finger gently stabilized the nasal tip, and the middle finger supported the columella to mold the tower-shaped filler into a smooth, symmetric structure, ensuring the columellar–lobular ratio approached 0.67 (ideal 2:1 ratio) and the nasolabial angle reached 90–100°.
Nasal Dorsum Augmentation (Root Height Enhancement)
Cannula Redirection
Without removing the 23G blunt cannula from the entry point, the tip was redirected horizontally and advanced parallel to the nasal bone surface, along the midline of the nasal dorsum, to the nasal root region (depth: 1.0–1.5 cm, above the periosteum, confirmed by tactile feedback of the bone surface).
Tunnel-Based Uniform Placement
A “tunnel-shaped” injection technique was adopted to ensure even filler distribution and natural contour:
Tunnel Creation
The blunt cannula was gently advanced and retracted 2–3 times along the nasal dorsum midline to create a subcutaneous tunnel (width: 3–4 mm) above the periosteum, avoiding lateral deviation to prevent nasal widening.
Retrograde Layered Injection
PVA microspheres were injected in a retrograde manner during cannula withdrawal, with a slow injection speed (0.1 mL/second) to ensure the filler fully fills the tunnel without voids. The injection was performed in a single layer to avoid excessive stacking and maintain a smooth dorsum curve.
Total Dose and Shaping
The total injection volume for the nasal dorsum was 0.5–1.0 mL (mean: 0.8 ± 0.2 mL). After injection, the cannula was withdrawn, and the nasal dorsum was shaped with gentle pressure using the palm of the hand: from the nasal root to the nasal tip, the filler was smoothed to form a natural S-shaped curve, ensuring the nasofrontal angle reached 115–125° and the nasal root height difference was 4.5–5.5 mm.
Post-Injection Hemostasis and Dressing
After cannula withdrawal, a sterile cotton ball was pressed on the entry point for 1–2 minutes to achieve hemostasis (no suturing required due to the minimal opening).
A thin layer of sterile antibiotic ointment (eg, mupirocin ointment) was applied to the entry point to prevent infection, and a nasal external splint (soft silicone material) was placed on the nasal dorsum for 24 hours to maintain the shaped contour and reduce edema.
Postoperative Care and Follow-Up
Postoperative Care
Patients were instructed to avoid touching, pressing, or rubbing the nasal region for 3 days; avoid strenuous exercise and high-temperature environments (eg, saunas) for 1 week; and refrain from wearing glasses that exert pressure on the nasal dorsum for 1 week. Mild edema was managed with cold compresses (15–20 minutes, 3–4 times/day) for the first 48 hours.
Follow-Up Schedule
Patients were followed up at 1 week, 1 month, 3 months, 6 months, 12 months, and 24 months postoperatively. At each follow-up visit, standardized photography was repeated, and the following parameters were evaluated: quantitative aesthetic indices, nasal morphology maintenance, patient satisfaction, and adverse events.
Outcome Measures
Quantitative Aesthetic Indices (Measured via ImageJ Software)
Nasal Tip Aesthetic Changes
- Nostril/nasal base ratio: Ratio of the vertical height of the nostril (from the nasal tip to the nasal base) to the horizontal width of the nasal base (measured on frontal view).
- Nasolabial angle: Angle between the line from the nasal tip to the upper lip and the line from the upper lip to the nasal base (measured on lateral view).
Nasal Dorsum Aesthetic Changes
- Nasofrontal angle: Angle between the glabellar line (forehead midline) and the nasal dorsum line (measured on lateral view).
- Nasal root height difference: Vertical distance between the nasal root and the glabellar plane (measured on lateral view, with the glabellar plane as the reference).
Nasal Morphology Maintenance
- Absence of widening: Evaluated by the nasal width/nasal height ratio (measured on frontal view); a ratio increase >5% compared with postoperative 1 month was defined as “widening”.
- Regression rate: Calculated as [(postoperative 1-month index value - follow-up index value)/postoperative 1-month index value] × 100%, including regression rates of nostril/nasal base ratio, nasal root height difference, and nasal projection.
Patient Satisfaction Assessment
1. 10-point Visual Analog Scale (VAS): Patients rated their overall satisfaction with nasal appearance (1 = very dissatisfied, 10 = very satisfied).
2. Rhinoplasty Outcome Evaluation (ROE) Questionnaire: A validated 22-item scale evaluating nasal function and aesthetics, with scores ranging from 0 to 100 (higher scores indicate better outcomes).11
Adverse Events Monitoring
Systematic recording of adverse events including hyperplasia (abnormal tissue growth), erythema (persistent redness >7 days), nodules (palpable hard masses), and widening (nasal width/nasal height ratio increase >5%). Severity grading: Grade 1 (mild, no treatment needed), Grade 2 (moderate, symptomatic treatment needed), Grade 3 (severe, surgical intervention needed).
Statistical Analysis
Statistical analysis was performed using SPSS 22.0 software (IBM Corp., Armonk, NY, USA). The independent variable (IV) was defined as follow-up time points including baseline, 6 months, 12 months, and 24 months; the dependent variable (DV) was defined as quantitative nasal aesthetic indices. All quantitative data, including aesthetic indices, VAS scores, ROE questionnaire scores, and regression rate, were presented as mean ± standard deviation (SD). All enrolled patients completed full follow-up with no missing data. Paired t-tests were used to compare preoperative and postoperative quantitative indices. Repeated-measures analysis of variance (ANOVA) with Greenhouse–Geisser correction was performed to evaluate longitudinal changes across multiple time points to account for potential sphericity assumption violation. A two-tailed P-value < 0.05 was considered statistically significant.
Results
Quantitative Aesthetic Indices
All 30 female patients achieved significant improvements in nasal tip and nasal dorsum aesthetic indices, with stable maintenance during long-term follow-up (Table 1).
 |
Table 1 Changes in Quantitative Nasal Aesthetic Indices (Mean ± SD) |
Nasal Morphology Maintenance
- Absence of widening: The nasal width/nasal height ratio was 0.68±0.05 at postoperative 1 month, 0.69±0.04 at 12 months, and 0.70±0.04 at 24 months, with no significant increase (P>0.05) and no patient meeting the “widening” definition (ratio increase >5%).
- Regression rate: The overall regression rate of key indices was 5.2±2.1% at 12 months and 8.3±3.2% at 24 months, with the lowest regression rate observed in the nostril/nasal base ratio (4.1±1.8% at 24 months) (Table 2).
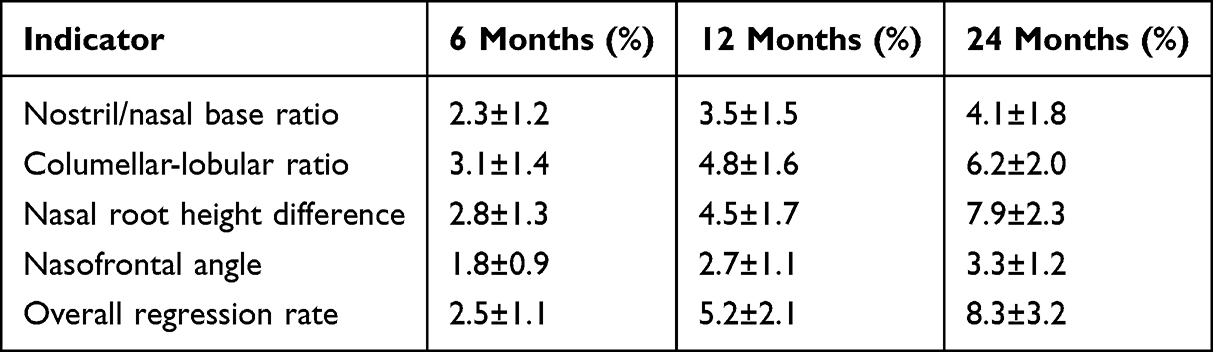 |
Table 2 Regression Rate of Key Nasal Aesthetic Indices During 24-Month Follow-Up (Mean ± SD) |
Patient Satisfaction
(1) VAS Score: The mean patient satisfaction VAS score was 9.2±0.6 at postoperative 1 month, 8.9±0.7 at 12 months, and 8.7±0.8 at 24 months, with no significant decline (P>0.05). A typical case is shown in Figure 1.
 |
Figure 1 Images were captured from five perspectives: frontal view, 45-degree lateral view and standard lateral view. The patient received nasal injection with 1.0mL Bonita (PVA microspheres), including 0.5mL for the nasal dorsum and 0.5mL for the nasal columella. The images present nasal appearances at pre-operation, immediate post-operation and 12 months post-operation. |
(2) ROE Questionnaire Score: The mean ROE score increased from 58.3±6.5 preoperatively to 91.2±4.0 at postoperative 1 month, 89.6±4.2 at 12 months, and 87.8±4.5 at 24 months, with a statistically significant difference between preoperative and postoperative scores (P<0.001) (Table 3).
 |
Table 3 Changes in Patient Satisfaction Scores Preoperatively and Postoperatively (Mean ± SD) |
Adverse Events
No severe adverse events (Grade 2 or 3) were reported during the follow-up period. Mild adverse events included:
(1) Transient erythema: Observed in three patients (10%) at postoperative 1–3 days, resolved spontaneously within 3–5 days without additional treatment.
(2) No hyperplasia, nodules, or widening were detected in any patient (Table 4).
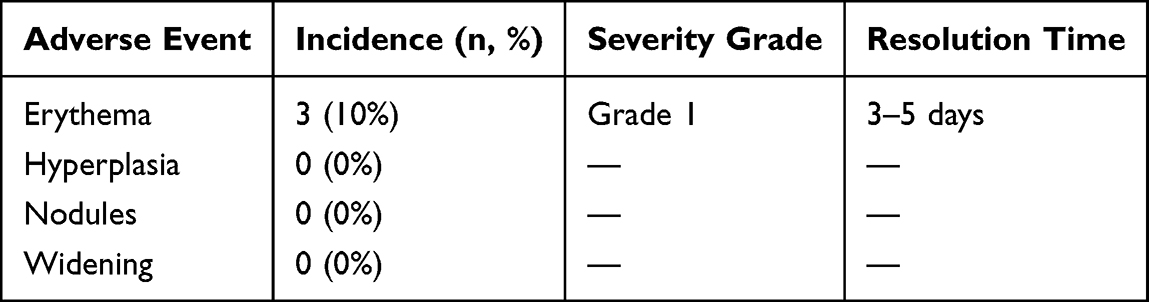 |
Table 4 Incidence of Adverse Events (n=30) |
Discussion
Asia female patients have unique nasal anatomical characteristics, including a thin nasal soft tissue envelope, weak nasal septal support, and flat maxillary bone,12 which differ slightly from male nasal structures and require individually tailored aesthetic strategies. These anatomical features present notable challenges to both surgical and injectable nasal augmentation. Surgical rhinoplasty demands precise anatomical dissection to reduce the risk of implant displacement, whereas conventional HA injection is susceptible to lateral spread due to inadequate soft tissue support,13 a concern particularly relevant to female patients pursuing delicate nasal contour refinement. The present study attempted to address these unmet clinical challenges by combining PVA microspheres with a surgical-style injection technique, alongside a quantitative evaluation system to preliminarily assess efficacy and safety in a cohort of 30 Asian female patients.
Quantitative Aesthetic Improvements
This study represents one of the relatively few investigations to systematically evaluate injectable rhinoplasty using objective nasal morphological indices. Our quantitative measurements indicated that PVA microsphere injection was associated with favourable changes in key aesthetic parameters: the nostril/nasal base ratio (an indicator of nasal tip projection) increased from 0.42±0.05 to 0.58±0.04, the nasolabial angle (reflecting tip–lip harmony) increased from 85.3±6.2° to 95.6±5.8°, the nasofrontal angle (defining the dorsum–forehead transition) decreased from 135.2±8.1° to 120.5±7.3°, and nasal root height difference (representing dorsal height) increased from 2.1±0.6 mm to 4.8±0.7 mm. These morphological alterations align with the typical aesthetic preferences of Asian female patients for a natural, refined, and proportionate nasal contour.14 The relative stability of these indices over the 24-month follow-up suggests potential long-term durability of PVA microsphere treatment, though these findings should be interpreted with caution given the exploratory nature of this single-cohort study.
Advantages in Morphology Maintenance (No Widening, Low Regression Rate)
Nasal widening is a well-recognised common complication of HA injectable rhinoplasty in Oriental populations, with reported incidence ranging from 20% to 30%.6 In the present cohort, no clinically obvious nasal widening was observed, supported by a stable nasal width/height ratio with an increase below 5% throughout follow-up. This favourable outcome may be largely attributable to two material and technical factors: (1) PVA microspheres possess high cohesiveness and relatively low water absorption (2–3 times their original volume), in contrast to HA fillers (10–15 times),9 which may help minimise lateral filler diffusion; (2) the surgical-like injection technique emphasises membranous nasal septum augmentation to establish stable nasal tip support, potentially counteracting lateral muscular traction and reducing filler migration.15 Furthermore, the overall morphological regression rate of PVA microspheres was only 8.3±3.2% at 24 months, comparatively lower than the reported 15–25% regression rate of HA fillers at 2 years,16 implying a possible advantage in mid-to-long-term morphological stability.
High Patient Satisfaction and Safety
Patient-reported satisfaction is an important complementary outcome for aesthetic procedures. We adopted a 10-point VAS scale and the validated ROE questionnaire to comprehensively evaluate patient satisfaction. The mean VAS score remained consistently above 8.7 during the 24-month follow-up period, and ROE scores increased by 50.6% after treatment, indicating generally favourable patient acceptance and subjective aesthetic perception. In terms of safety profile, no tissue hyperplasia, nodule formation, and nasal widening were recorded, with only three cases of mild and transient erythema. This low rate of adverse events is broadly consistent with the good biocompatibility of ISO 10993-certified PVA microspheres.9 The low incidence of hyperplasia and nodules may be partly related to the uniform particle size (40–120 μm) and favourable tissue integration, which could lower the likelihood of foreign body reactions. Nevertheless, safety observations are limited by sample size and follow-up length, and longer-term monitoring remains necessary.
Clinical Significance, Limitations, and Potential Biases
Within the constraints of its study design, this exploratory investigation suggests that PVA microsphere injection combined with the surgical-like injection technique may serve as a promising minimally invasive option for nasal augmentation in Asian female patients. The approach appears to mitigate some drawbacks associated with conventional HA injection (particularly nasal widening) and invasive surgical rhinoplasty (prolonged downtime and higher revision risk), with measurable aesthetic improvement, acceptable mid-term stability, and satisfactory patient feedback.
Several inherent limitations and potential biases in this study should be acknowledged when interpreting the findings. First, the study is a retrospective single-centre investigation with a relatively small sample size (30 female participants), which may introduce selection bias and limit generalisability. Future prospective, multicentre studies with larger cohorts are required to corroborate our results. Second, follow-up was restricted to 24 months; longer surveillance of 3–5 years is essential to fully evaluate the sustained performance and safety of PVA microspheres in this patient group. Third, the absence of a parallel control group (eg, HA injection) prevents direct head-to-head comparison, and further controlled comparative trials are warranted to clarify the relative efficacy and safety between PVA microspheres and HA fillers. Fourth, enrolment was limited exclusively to female patients, so the observed outcomes cannot be readily extrapolated to male populations. Lastly, as an exploratory uncontrolled case series, our results should not be regarded as definitive clinical conclusions, and overinterpretation of the observed favourable outcomes should be avoided.
Conclusion
In conclusion, PVA microsphere injection combined with a surgical-like injection technique (membranous nasal septum tip projection + deep-layer nasal dorsum augmentation) is a safe and effective approach for nasal augmentation in Asia female patients. This method significantly improves key quantitative nasal aesthetic indices, maintains long-term morphological stability (no widening, low regression rate), achieves high patient satisfaction, and has a low incidence of adverse events. It provides a valuable minimally invasive alternative to traditional surgical rhinoplasty and conventional HA injection for this patient population.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lee JW, Kim HT, Park JY. Rhinoplasty in Asians: anatomical considerations and surgical approaches. Aesthet Surg J. 2018;38(1):92–9.
2. Chen Y, Zhang Y, Li J. Current trends in minimally invasive nasal augmentation: a systematic review. J Cosmet Dermatol. 2020;19(6):1352–1360.
3. Rohrich RJ, Ghavami A, Constantian MB. Rhinoplasty: avoiding and managing complications. Plast Reconstr Surg. 2016;137(3):893e–906e.
4. Kim HS, Park SS, Lee SH, Blanc O, Emodi O, Rachmiel A. Revision rhinoplasty for implant displacement: a retrospective study of 52 cases. J Craniofac Surg. 2019;30(7):2065–2068. doi:10.1097/SCS.0000000000005960
5. Alam M, Dover JS, Arndt KA, MacFarlane DF. Injectable fillers in aesthetic medicine: an overview. J Am Acad Dermatol. 2015;73(1):1–14. doi:10.1016/j.jaad.2014.10.047
6. Park JY, Kim JW, Lee DH. Nasal widening after hyaluronic acid injection rhinoplasty: risk factors and prevention strategies. Dermatol Surg. 2017;43(10):1273–1278.
7. Weiss RA, Weiss MA. Hyaluronic acid fillers: complications and their management. Facial Plast Surg Clin North Am. 2018;26(2):209–218.
8. Cho KH, Kim YH, Park HJ. Analysis of nasal widening after hyaluronic acid injection rhinoplasty in Asian patients. Aesthet Plast Surg. 2019;43(3):789–795.
9. Wang Y, Li X, Zhang L. Biocompatibility and long-term efficacy of polyvinyl alcohol microsphere filler in soft tissue augmentation. J Biomed Mater Res B Appl Biomater. 2021;109(5):1689–1696. doi:10.1002/jbm.b.34825
10. Gunter JP, Rohrich RJ, WP A Jr. Aesthetic rhinoplasty: analyzing, planning, and executing the ideal nose. Plast Reconstr Surg. 2018;141(2):317e–330e.
11. Guyuron B, Davis J, Lee R. Development and validation of the rhinoplasty outcome evaluation questionnaire. Plast Reconstr Surg. 2007;120(3):680–686.
12. Hu S, Chen L, Liu Y, Yin N, Wang Y. Anatomical characteristics of the nasal soft tissue envelope in oriental patients: a cadaveric study. J Craniofac Surg. 2020;31(3):821–824. doi:10.1097/SCS.0000000000006235
13. Lee DH, Park JY, Kim JW. Minimally invasive nasal augmentation in Asians: challenges and solutions. Dermatol Surg. 2021;47(2):213–220.
14. Hu S, Chen L, Liu Y. Aesthetic standards for nasal augmentation in Asia female patients: a survey-based study. J Cosmet Laser Ther. 2021;23(5):1245–1250.
15. Toriumi DM, Hecht D. Nasal tip dynamics: the role of the membranous septum. Plast Reconstr Surg. 2017;140(4):631–638.
16. Narins RS, Brandt FS, Frankel AS. Long-term efficacy of hyaluronic acid fillers in nasal augmentation: a 2-year follow-up study. Clin Plast Surg. 2018;45(4):567–573.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.