Back to Journals » International Medical Case Reports Journal » Volume 18
Pure Neuritic Leprosy In Children With Grade 2 Disability On Hands And Feet: A Rare Case And Literature Review
Authors Gunawan H ![]() , Ruchiatan K, Puspitosari D
, Ruchiatan K, Puspitosari D ![]() , Hindritiani R
, Hindritiani R ![]() , Usman HA
, Usman HA ![]() , Widjaja S
, Widjaja S
Received 25 September 2024
Accepted for publication 19 January 2025
Published 28 January 2025 Volume 2025:18 Pages 195—203
DOI https://doi.org/10.2147/IMCRJ.S497894
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Hendra Gunawan,1 Kartika Ruchiatan,1 Diah Puspitosari,1 Reti Hindritiani,1 Hermin Aminah Usman,2 Stephanie Widjaja1
1Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran, Dr. Hasan Sadikin Hospital, Bandung, Indonesia; 2Department of Anatomical Pathology, Faculty of Medicine, Universitas Padjadjaran, Dr. Hasan Sadikin Hospital, Bandung, Indonesia
Correspondence: Hendra Gunawan, Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran - Dr. Hasan Sadikin Hospital, Jl. Pasteur 38, Bandung, West Java, 40161, Indonesia, Tel +6281221111215, Email [email protected]
Abstract: Pure neuritic leprosy (PNL) is a rare clinical variant of leprosy, especially in children. This variant of leprosy only involves peripheral nerves without skin involvement or acid-fast bacilli (AFB) found on slit-skin smear examination. The challenging diagnosis and establishment of PNL due to the absence of skin lesions often lead to disability. A case of PNL with grade 2 disability of hands and feet in a 16-year-old boy was reported. The patient has been living in a leprosy-endemic area and has a history of contact with people who have symptoms of leprosy. On physical examination, there were finger contractures on both hands and feet, accompanied by bilateral ulnar, common peroneal, and posterior tibial nerve enlargement without any skin lesions. No AFB was found on the slit-skin smear examination. The diagnosis of PNL was established by the mononeuritis multiplex detected on the nerve conduction examination and the histopathological examine from the biopsy of the left ulnar nerve, which showed lymphocyte infiltration. The patient was treated with multidrug therapy for multibacillary leprosy and consulted with the Department of Physical Medicine and Rehabilitation and the Department of Orthopaedics and Traumatology for contracture management. Clinicians need to be aware of the signs and symptoms of PNL in order to avoid delays in diagnosis and treatment, as the diagnosis and establishment of PNL remain challenging.
Keywords: children, grade 2 disability, nerve biopsy, nerve conduction study, pure neuritic leprosy
Introduction
Leprosy is a chronic granulomatous infectious disease caused by Mycobacterium leprae (M. leprae)1 or M. lepromatosis,2 primarily targeting the Schwann cells of the nervous tissue.3,4 It is one of the most common causes of non-traumatic peripheral neuropathy worldwide.2 Invasion of Schwann cells by bacteria induces inflammation and fibrosis, resulting in nerve dysfunction and limb deformities.3
Pure neuritic leprosy (PNL) is a rare clinical variant of leprosy, characterized by peripheral nerve involvement without skin lesions or the detection of acid-fast bacilli (AFB) in slit-skin smear examination. Peripheral nerve dysfunction, with or without peripheral nerve thickening, constitutes the common manifestation of nerve involvement in PNL.4 PNL occurs in 4–8% of leprosy cases, and it also rarely develops in children.5 Indonesia currently ranks third globally for the highest number of leprosy cases, following India and Brazil.1 However, the incidence and prevalence of PNL in Indonesia are not well-established.
Delays in diagnosing PNL are more common compared to other clinical variants of leprosy due to the absence of skin lesions or AFB in slit-skin smear examinations.5,6 This delay in diagnosis often leads to disabilities in PNL patients.5,7 According to a study by Pitta et al8 in Brazil in 2021, it was found that a higher percentage of PNL cases (78.8%) presented with disabilities compared to other types of leprosy (40.3%) at the time of initial diagnosis. Disability refers to impairment or limitations in physical activities for an individual. As per the World Health Organisation (WHO), grade 2 disability in leprosy indicates visible physical abnormalities, especially in the eyes, hands, and feet.9 In most cases, grade 2 disabilities were already present at the time of PNL diagnosis.5,7 Therefore, comprehensive knowledge of the signs, symptoms, and various diagnostic examinations for confirming PNL by clinicians is crucial in preventing disabilities associated with PNL,5 especially in children.
This case report aimed to present a rare occurrence of PNL, which is a rare case, in a child complicated by grade 2 disabilities on hands and feet at the time of the initial diagnosis.
Case Illustration
A 16-year-old high school student was referred to the Tropical Dermatology Clinic at the tertiary referral hospital in West Java, Indonesia, with a finger and toe deformity suspected to be due to leprosy.
In the last 12 years, until three months prior to consulting, the patient experienced multiple paresis followed by contracture that occurred in a random order on some of his fingers and toes. Seven years before the consultation, the third toe of the left foot underwent amputation due to a chronic, non-healing ulcer. However, the family did not seek medical attention for the multiple contractures that had occurred. The patient was taken for treatment by a surgeon at the local hospital, then referred to the Department of Plastic Surgery and Reconstruction at our hospital, and later consulted at our clinic due to suspected leprosy.
The patient was born and raised in an endemic leprosy area, living at home with his unaffected parents and an older brother. However, when the patient was two years old, their family was frequently visited by a neighbor who had clawed hands as a result of perhaps having leprosy. A physical examination indicated normal vital signs, with the exception of being underweight. A dermatological examination revealed no leprosy-related skin lesions (Figure 1). The patient had contractures in both hand’s third, fourth, and fifth fingers (Figure 2), as well as hypothenar and thenar muscle atrophy. Amputation of the third left toe, contracture of the first right toe, contractures in the toes of the left foot’s toes, trophic ulcer, and hypertrophic scar were among the lower extremity injuries (Figures 3 and 4). Enlargement was observed in both the ulnar nerves, common peroneal nerves, and posterior tibial nerves, with string-like consistency. AFB was not detected in the skin smears from both the earlobes and the back of the left hand.
 |
Figure 1 No leprosy-related skin lesions were seen. |
 |
Figure 2 Finger deformities. |
 |
Figure 3 Toe deformity of the right foot with trophic ulcer and hypertrophic scar. |
 |
Figure 4 Toe deformities of the left foot. |
Serological testings for anti-phenolic glycolipid-1 (PGL-1) immunoglobulin (Ig)M and IgG antibodies were nonreactive. However, since the case happens in an endemic leprosy area, further investigation was carried out. The patient was consulted with the Neurology Department, and nerve conduction studies (NCS) were performed that showed mononeuritis multiplex. An attempt to rule out other conditions that may result in peripheral neuropathy has been made. Histopathological nerve examination with hematoxylin eosin staining revealed axon and Schwann cell within normal limit (Figure 5A and B), fibroblast cells in between within normal limit (Figure 5C and D), and lymphocytic infiltration in the fibrocollagen stroma (Figure 5E). No AFB was detected in the histopathological examination of the left ulnar nerve biopsy as shown in 20x magnification (Figure 6A and B) in 200x magnification. The patient was diagnosed with PNL with grade 2 disability. Therefore, the patient received multidrug therapy (MDT) for multibacillary leprosy. The patient also consulted with the Department of Physical Medicine and Rehabilitation and the Department of Surgery for the management of disabilities. The patient had recurrent severe reversal reactions throughout a follow-up period of 14 months, which resolved after systemic corticosteroid therapy. At the end of the follow-up, the slit-skin smear examination revealed no AFB and no further development of the signs and symptoms of leprosy.
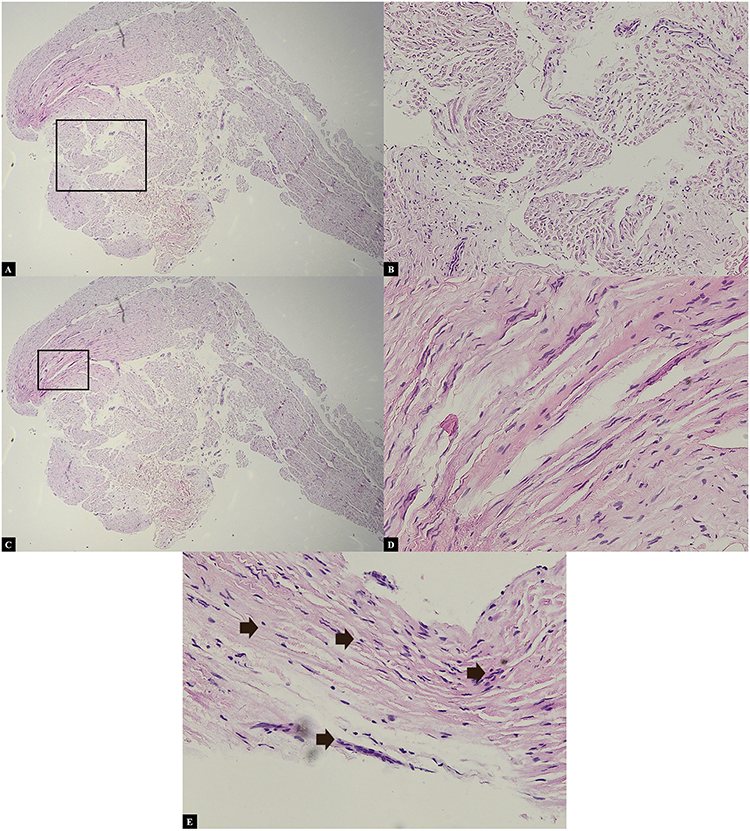 |
Figure 5 Histopathological nerve examination with hematoxylin eosin staining revealed axon and Schwann cell within normal limit (A) in 20x magnification and (B) in 100x magnification (for parts enclosed within the black box), fibroblast cells in between within normal limit (C) in 20x magnification and (D) in 200x magnification (for parts enclosed within the black box), and (E) lymphocytic infiltration in the fibrocollagen stroma (black arrow). |
 |
Figure 6 No AFB were found in histopathological nerve examination with Fite-Faraco staining as shown (A) in 20x magnification and (B) in 200x magnification (for parts enclosed within the black box). |
Discussion
PNL was first identified by Wade in 1952 and accepted as one of the leprosy subtypes by the International Congress in Madrid in 1953, later incorporated into the classification of the Indian Association of Leprologists (IAL) in 1955.3,10 However, PNL is not included in the widely used Ridley-Jopling classification.5 The prevalence of PNL in India varies from 4.3–5.6% in Northern India to 17.7% in Southern India.3 PNL occurs more frequently in males than females, with a ratio of 3.7:1, predominantly in the age group of 41–60 years.5 In a study by Bhalla et al3 in Northern India in 2022, it was found that PNL mostly occurred in the age group of 15–35 years (63%), with 3 (7%) cases occurring in those <14 years old. The patient in this case report is a 16-year-old boy.
Clinical characteristics of PNL include sensory nerve dysfunction with or without motor nerve impairment and enlargement of peripheral nerves. The condition must be accompanied by the absence of skin lesions and the absence of AFB in the slit-skin smear examination. Peripheral nerve enlargement is found only in 40–75% of PNL cases.11 Histopathological examinations may yield varying results.3 According to a study by Rodriguez et al12 in Colombia in 2013, diagnostic criteria for PNL include: (1) clinical signs and symptoms of nerve dysfunction with or without nerve enlargement; (2) neuritis or perineural inflammation in nerve biopsy; (3) finding of AFB in nerve biopsy; (4) polymerase chain reaction (PCR) examination with positive results for M. leprae deoxyribonucleic acid (DNA); (5) detection of positive IgM antibodies anti-PGL-1; and (6) abnormal findings in NCS12,13 after ruling out causes other than leprosy.12 Additionally, research conducted by Razdan et al13 revealed that the diagnosis of PNL can be improved using a non-invasive method, which is NCS. Individuals with peripheral nerve disturbances with or without nerve enlargement living in leprosy-endemic areas should be managed as PNL.1 The management should be carried on even without AFB findings in a slit-skin smear examination or nerve biopsy and negative results in an anti-PGL-1 antibody or PCR examination.12 The diagnosis of PNL in this case was confirmed based on clinical symptoms, including the finding of nerve enlargement in several peripheral nerves accompanied by motor function disturbances in the form of contractures in the fingers and toes, without skin abnormalities, and the absence of AFB in a slit skin smear examination. Histopathological examination of the ulnar nerve biopsy showed lymphocytic inflammatory cell infiltration, indicating perineural inflammation. Nerve conduction studies revealed sensory neuropathy in the right peroneal nerve and motor neuropathy in the right peroneal and left ulnar nerves. The finding suggested mononeuritis multiplex. The patient lives and grew up in Karawang District, one of the endemic leprosy areas in West Java, Indonesia.
Serological testing by detecting IgM antibodies against PGL-1 can aid in diagnosing PNL.4 The sensitivity and specificity of this test in PNL are 21% and 91%, respectively, with higher sensitivity in MB-type PNL compared to PB-type PNL.5 IgM anti-PGL-1 testing can also be used to assess therapy response in PNL.6 IgM anti-PGL-1 testing can also be used to assess therapy response in PNL4 The IgM anti-PGL-1 test in this case report showed a negative result. This could be due to the low sensitivity (21%) of the IgM anti-PGL-1 test in PNL.
The nerve biopsy is the gold standard examination for confirming PNL diagnosis, and tissue should ideally be taken from the sensory nerves innervating the affected area.1 The definitive diagnosis of PNL is made based on the presence of AFB in a nerve biopsy.14 However, this examination has low sensitivity and carries a high risk of nerve injury.4 In a study by Hui et al14 in India in 2015, AFB was found in only 24 (52.17%) out of 46 PNL patient nerve biopsies. In a study by Jardim et al15 in Brazil in 2004, AFB was found in only 4 (21%) out of 19 PNL patient nerve biopsies. This might be due to the small number of bacteria.14 Furthermore, there is a high possibility of failure to obtain infected nerve tissue because the infection does not occur uniformly along the nerve fibers.12
Changes in histopathology such as reduced myelinated nerve fibers, perineural thickening, endoneurial fibrosis, and endoneurial infiltrate can aid in confirming the diagnosis of PNL if AFB is not found.4,14 A study of nerve biopsy specimens from 19 PNL patients in Brazil showed that in the nerve biopsy specimens with AFB-negative inflammatory infiltrate, the predominant cell was the lymphocyte, accompanied by epithelioid granulomas. Meanwhile, the nerve biopsy specimens with AFB-positive lepromatous infiltrates revealed easily identifiable macrophages.15 The finding of an intraneural epithelioid granuloma is especially significant in confirming the diagnosis of PNL.12 However, such granulomas were found in only 14% of cases in a study by Jardim et al.16
The PCR examination of nerve tissue can help to confirm the diagnosis if AFB is not found in the histopathological examination of nerve biopsies.15,17,18 In this patient, AFB was not found in histopathological examination with Hematoxylin-Eosin staining and Fite Faraco in the left ulnar nerve, and PCR examination was not conducted due to insufficient tissue specimens from the nerve tissue biopsy. However, lymphocytic infiltration was seen in the nerve biopsy specimen, supporting the diagnosis of leprosy.
Clinical manifestations due to nerve involvement in leprosy occur after nerve fiber damage reaches 30%. Therefore, diagnostic tests to detect nerve damage are important to perform, even if no clinical manifestations are found.12 NCS is the most sensitive modality to detect subclinical neuropathy.12 It is more sensitive to detect nerve function disturbances than a physical examination. Many abnormal NCS findings are obtained in nerves that are not enlarged.19 Hence, it is recommended for all PNL cases4,14 to aid in diagnosis.4,14 The nerve function pattern observed in PNL can be axonal neuropathy, demyelination, or a combination of both.14 Demyelination patterns are more common in the initial stages of leprosy-related nerve damage, and axonal patterns indicate chronic nerve damage in leprosy.18 Nerve involvement in leprosy may manifest as mononeuritis, mononeuritis multiplex, or polyneuritis. The latter is an accumulation of mononeuritis multiplex involving many nerve roots.11 Jardim et al15 in Brazil conducted an investigation using NCS involving 19 PNL patients, revealing axonal patterns (94.7%) and demyelination (0.5%). Mononeuritis multiplex was the most frequent presentation (78.9%), followed by mononeuritis simplex (10.5%), and polyneuritis (10.5%). Similar results were obtained in the study involving 52 PNL patients by Pitta et al18 in Brazil. According to the 10-year observation by Kolleri et al5 in India, the most commonly affected nerves were the ulnar nerve, common peroneal nerve, radial nerve, and sural nerve. In the study by Rodriguez et al12 in Colombia, the most commonly affected nerves were the ulnar nerve, radial nerve, common peroneal nerve, median nerve, great auricular nerve, and posterior tibial nerve. These nerves are superficially located in areas with temperatures between 33°C and 36°C, and are susceptible to trauma, potentially serving as entry points for M. leprae.12 The NCS results in this patient showed mononeuritis multiplex, which consisted of sensory neuropathy in the right peroneal nerve as well as motor neuropathy in the right peroneal and left ulnar nerves.
Pure neuritic leprosy can be classified as paucibacillary or multibacillary for treatment purposes.3,19 The National Leprosy Eradication Programme (NLEP) categorises therapy for PNL based on the number of involved nerves.3 In paucibacillary type PNL, involvement occurs in only one nerve, while multibacillary type PNL involves more than one nerve.19 The patient in this case report was classified as having multibacillary type PNL according to NLEP criteria due to the involvement of more than one nerve, hence receiving multidrug therapy for multibacillary leprosy.
Signs and symptoms of neuritis or acute neuropathy are indications for systemic corticosteroid therapy at a dose equivalent to prednisone 1 mg/kgBW/day.19 Prednisone is the primary therapy for neuritis as it can reduce edema, produce immunosuppressive effects, and reduce scar tissue formation after inflammation, thus inhibiting the progression of peripheral neuropathy and even aiding in the recovery of ongoing early damage.20 The patient in this case report experienced two episodes of type I leprosy reaction, one at the beginning of MDT therapy and the other after six months of treatment, due to physical and psychological fatigue. The manifestations of leprosy reaction in this patient were pressure pain on the nerves during the first episode and sensory nerve function impairment without other symptoms during the second episode. The leprosy reaction in this patient was treated with gradually reduced prednisone at a dose of 40 mg/day, along with education on managing physical and psychological fatigue.
Leprosy reaction is an acute inflammatory episode occurring in the chronic clinical course of leprosy.2 This reaction is found in 30–50% of leprosy cases,8 in the form of type 1 and type 2 leprosy reactions.2 Leprosy reaction can occur before, during, or after MDT due to acute changes in the host’s immune response to M. leprae.8 Neuritis is the main cause of nerve damage in leprosy and can occur during leprosy reactions, as well as being an isolated event.8 Neuritis can be accompanied by pain along the inflamed nerve fibers,8 but it can also manifest solely as nerve function impairment, without other known symptoms, known as silent neuritis.8,11,20 According to Pitta et al8 in Brazil in 2022, studying 52 PNL patients and 67 patients with other types of leprosy, leprosy reactions occurred more frequently in other clinical variants of leprosy (59.7%) compared to PNL (23.1%). However, silent neuritis is more commonly found in PNL cases compared to other types of leprosy because the presence of M. leprae within Schwann cells in the peripheral nerves can trigger nerve damage, even without the accompanying host inflammatory response.8,11
Disability is a major factor leading to social stigma5,9 and can cause a significant social impact and economic burden.21 WHO classifies the levels of disability in leprosy as: (1) Grade 0, meaning no nerve function impairment due to leprosy; (2) Grade 1, indicating no visible deformities due to leprosy on hands, feet, or eyes, with vision >6/60; and (3) Grade 2, showing visible deformities on hands, feet, or eyes, with vision <6/60.9 Nerve damage in leprosy is caused by either M. leprae invasion or leprosy reactions.1 It is the main factor underlying the development of disabilities.2,8 Motor nerve imbalance due to nerve damage can lead to deformities like claw hands and claw toes.22 Neglected or poorly managed sensory and motor nerve function impairments in leprosy can progress to secondary complications like contractures and ulcers.22,23 Physical disability and nerve damage-related deformities are the most severe complications of leprosy.21,22 Grade 2 disability is more common in PNL than in other clinical variants of leprosy due to delays in diagnosis and therapy initiation.7 According to a study by Narang et al7 in India in 2016, grade 2 disability was found in 66.7% of PNL cases at diagnosis. Additionally, the study by Kolleri et al5 in India in 2019 found a higher prevalence of grade 2 disability, reaching 80% of PNL cases at diagnosis.
From the study conducted by Goncalves et al24 in Brazil in 2009, it was found that with pharmacological and non-pharmacological interventions, 43.2% of leprosy patients with grade 1 disabilities improved to grade 0, while in patients with Grade 2 disabilities, 21.3% showed improvement to grade 1 and 20% improved to grade 0. Non-pharmacological interventions for leprosy disability management include physiotherapy and reconstructive surgery.23,25 Physiotherapy and bandaging are performed to maintain muscle strength, prevent contractures, restore joint mobility, and preserve skin elasticity, thus preventing deformities.25 Before and after reconstructive surgery, physiotherapy is crucial to maintaining limb function.23,25 The patient in this case report experienced grade 2 disabilities at diagnosis, including contractures of the fingers and toes. The patient was referred to the Physical Medicine and Rehabilitation Department for further management of physical deformities and was also planned for consultation with the Orthopedics and Traumatology Department.
Malaviya22 categorized the levels of leprosy disabilities based on the provided management to facilitate selection and prevent delays in addressing these disabilities. Grade 1 disability includes reduced sensory nerve function in the hands and feet; Grade 2 disability involves mild hand bone injuries and resorption, trophic ulcers, and claw toes on the feet; Grade 3 disability includes claw fingers, thumb weakness, wrist drop in hands, and foot drop in feet; Grade 4 disability comprises significant contractures and resorption in finger and toe bones. Grade 1 and 2 disabilities can be managed by doctors in basic healthcare facilities. Grade 3 disability is a deformity due to muscle weakness that can be addressed with early surgical intervention, while Grade 4 disability involves apparent deformities requiring more complex surgical management.22 Tendon transfer is a surgical intervention that can correct claw hand and claw toe conditions.26,27 and can only be performed once joint stiffness has been addressed.26 Surgical contracture release procedures need to be carried out before tendon transfer in patients with contractures not responsive to physiotherapy. Intensive physiotherapy is required post-contracture release to maintain range of motion. Contracture release cannot be performed simultaneously with tendon transfer because immobilization is necessary for tendon recovery after transfer.26 The patient in this case report experienced contractures at diagnosis, leading to a consultation with the Orthopedics and Traumatology Department and planning for contracture release and tendon transfer surgery after the patient completes school.
Trophic ulcers frequently observed in leprosy on the feet are suspected to be due to sensory disturbances in the feet, which are often undetected before the occurrence of a wound.28 Trophic ulcers are caused by continuous pressure-related ischemia, resulting in tissue necrosis.29 This type of ulcer typically has distinct borders, occurs in bony prominence areas, is resistant to topical and systemic antibiotic therapies, and tends to recur.30 During observation, the patient in this case report experienced recurring trophic ulcers that were difficult to heal on both feet due to foot deformities causing difficulty and impaired movement when standing and walking. The condition led to frequent trauma and abnormal pressure distribution on the feet.
Principles of trophic ulcer management involve cleaning the ulcer and surrounding tissue, keeping the ulcer consistently clean with bandaging, and providing foot rest.29,30 Hydrocolloid wound dressings can maintain a moist environment to facilitate keratinocyte migration to the ulcer’s base.30 Education on cleaning, bandaging, and resting the ulcerated foot has been provided to the patient in this case report, along with the application of hydrocolloid wound dressings to hasten the ulcer healing.
Conclusion
There are still challenges in the diagnosis of PNL. Therefore, clinicians need to have a thorough understanding of the signs and symptoms of PNL in order to avoid delays in diagnosis and treatment.
Ethic Statement
The publications of images were included in the adult guardian of the patient’s consent for publication of the case. The institutional approval has obtained to publish the case details from the Research Ethics Committee of Dr. Hasan Sadikin Hospital No. DP.04.03/D.XIV.6.5/41/2024.
Consent Statement
The authors certify that they have obtained all appropriate patient consent forms. The adult guardian of the patient signed a consent form for the publication of the case details and images.
Acknowledgments
The authors would like to thank the staff of Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia.
Funding
The authors declare that this study has received no financial support.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Venkatesan K, Deo N. Biochemical aspects of leprosy. In: Kumar B, Kar HK, editors. Ial Textbook of Leprosy.
2. Bhat RM, Prakash C. Leprosy: an overview of pathophysiology. Interdiscip Perspect Infect Dis. 2012;2012:181089. doi:10.1155/2012/181089
3. Bhalla M, Poonia K, Jain S, Thami GP, Sharma P. Clinical profile of patients with pure neuritic leprosy: 20 years’ experience at a tertiary referral centre from north India. Leprosy Rev. 2022;93:131–137. doi:10.47276/lr.93.2.131
4. Kumar B. Pure or primary neuritic leprosy (pnl). Leprosy Review. 2016;87(4):450–455. doi:10.47276/lr.87.4.450
5. Kolleri JJ, Sasidharanpillai S, Vadakkayil B, Chathoth AT. A 10-year retrospective descriptive study on pure neuritic leprosy from a tertiary referral centre. Indian Dermatol Online J. 2019;10(1):13–18. doi:10.4103/idoj.IDOJ_118_18
6. Jardim MR, Antunes SL, Simons B, et al. Role of pgl-i antibody detection in the diagnosis of pure neural leprosy. Lepr Rev. 2005;76(3):232–240. doi:10.47276/lr.76.3.232
7. Narang T, Vinay K, Kumar S, Dogra S. A critical appraisal on pure neuritic leprosy from India after achieving who global target of leprosy elimination. Lepr Rev. 2016;87(4):456–463. doi:10.47276/lr.87.4.456
8. Pitta IJR, Hacker MA, Vital RT, et al. Leprosy reactions and neuropathic pain in pure neural leprosy in a reference center in rio de janeiro - Brazil. Front Med Lausanne. 2022;9:865485. doi:10.3389/fmed.2022.865485
9. Rathod SP, Jagati A, Chowdhary P. Disabilities in leprosy: an open, retrospective analyses of institutional records. An Bras Dermatol. 2020;95(1):52–56. doi:10.1016/j.abd.2019.07.001
10. Misra RS, Kataria JK. Classification. In: Kumar B, Kar HK, editors. Ial Textbook of Leprosy. New Delhi: Jaypee Brothers Medical Publishers Ltd.; 2017:
11. Nascimento OJ. Leprosy neuropathy: clinical presentations. Arq Neuropsiquiatr. 2013;71(9b):661–666. doi:10.1590/0004-282X20130146
12. Rodriguez G, Pinto R, Gomez Y, et al. Pure neuritic leprosy in patients from a high endemic region of Colombia. Lepr Rev. 2013;84(1):41–50. doi:10.47276/lr.84.1.41
13. Razdan N, B V, Sadhu S. Pure neuritic leprosy: latest advancements and diagnostic modalities: diagnosis of pure neuritic leprosy. Diagn Microbiol Infect Dis. 2024;110(4):116529. doi:10.1016/j.diagmicrobio.2024.116529
14. Hui M, Uppin MS, Challa S, Meena AK, Kaul S. Pure neuritic leprosy: resolving diagnostic issues in acid fast bacilli (afb)-negative nerve biopsies: a single centre experience from south India. Ann Indian Acad Neurol. 2015;18(3):292–297. doi:10.4103/0972-2327.162284
15. Jardim MR, Chimelli L, Faria SC-R, et al. Clinical, electroneuromyographic and morphological studies of pure neural leprosy in a Brazilian referral centre. Leprosy Rev. 2004;75:242–253.
16. Jardim MR, Antunes SL, Santos AR, et al. Criteria for diagnosis of pure neural leprosy. J Neurol. 2003;250(7):806–809. doi:10.1007/s00415-003-1081-5
17. Antunes SL, Chimelli L, Jardim MR, et al. Histopathological examination of nerve samples from pure neural leprosy patients: obtaining maximum information to improve diagnostic efficiency. Mem Inst Oswaldo Cruz. 2012;107(2):246–253. doi:10.1590/S0074-02762012000200015
18. Pitta IJR, Hacker MAV, Andrade LR, et al. Follow-up assessment of patients with pure neural leprosy in a reference center in rio de janeiro-Brazil. PLoS Negl Trop Dis. 2022;16(1):e0010070. doi:10.1371/journal.pntd.0010070
19. Garbino JA, Marques W Jr, Barreto JA, et al. Primary neural leprosy: systematic review. Arq Neuropsiquiatr. 2013;71(6):397–404. doi:10.1590/0004-282X20130046
20. Jardim MR, Illarramendi X, Nascimento OJ, et al. Pure neural leprosy: steroids prevent neuropathy progression. Arq Neuropsiquiatr. 2007;65(4a):969–973. doi:10.1590/S0004-282X2007000600009
21. Mowla MR, Angkur D, Hasan Z, Sultana M, Afrin S, Akhter M. Leprosy patients with deformities at post‐elimination stage: the Bangladesh experience. Skin Health and Disease. 2020;1:e5.
22. Malaviya G. Deformity and Disability Prevention. Dalam: Kumar B, Penyunting. Ial Textbook of Leprosy. India: Jaypee Brothers Medical Publishers Ltd.; 2017:
23. Shah A, Shah N. Deformities of face, hands, feet and ulcers and their management. Kumar B, Kumar KH. IAL Textbook of Leprosy 2nd Ed. New Delhi. 2017:
24. Gonçalves SD, Sampaio RF, Antunes CM. predictive factors of disability in patients with leprosy. Rev Saude Publica. 2009;43(2):267–274. doi:10.1590/S0034-89102009000200007
25. Álvarez C, Filho G. Leprosy and physiotherapy: a necessary approach. J Human Growth Develop. 2019;29:416–426. doi:10.7322/jhgd.v29.9541
26. Sammer DM, Chung KC. Tendon transfers: part ii. transfers for ulnar nerve palsy and median nerve palsy. Plast Reconstr Surg. 2009;124(3):212e–21e. doi:10.1097/PRS.0b013e3181b037c7
27. Steensma MR, Jabara M, Anderson JG, Bohay DR. Flexor hallucis longus tendon transfer for hallux claw toe deformity and vertical instability of the metatarsophalangeal joint. Foot Ankle Int. 2006;27(9):689–692. doi:10.1177/107110070602700906
28. Reyila VP, Betsy A, Riyaz N, et al. Clinico-epidemiological study of disability due to leprosy at the time of diagnosis among patients attending a tertiary care institution. Indian J Dermatol. 2019;64(2):106–111. doi:10.4103/ijd.IJD_185_17
29. Chauhan VS, Pandey SS, Shukla VK. Management of plantar ulcers in hansen’s disease. Int J Low Extrem Wounds. 2003;2(3):164–167. doi:10.1177/1534734603257986
30. Riyaz N, Sehgal V. Leprosy: trophic skin ulcers. SKINmed. 2017;15:45–51.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.