Back to Journals » International Medical Case Reports Journal » Volume 19
Pulmonary Aspergillosis Developing After the First Chemotherapy Session in a 15-Year-Old Boy: A Case Report
Authors Ghadirioghani A ![]() , Tamadoni A, Esmailzade F
, Tamadoni A, Esmailzade F
Received 1 August 2025
Accepted for publication 15 January 2026
Published 4 February 2026 Volume 2026:19 549936
DOI https://doi.org/10.2147/IMCRJ.S549936
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tanvi Dhere
Alborz Ghadirioghani,1 Ahmad Tamadoni,2,3 Firuze Esmailzade3,4
1Department of Medicine and Health Sciences, Babol University of Medical Sciences, Babol, Iran; 2Department of Pediatrics and Neonatology, Babol University of Medical Sciences, Babol, Iran; 3Non-Communicable Pediatric Diseases Research Center, Health Research Institute, Babol University of Medical Sciences, Babol, Iran; 4Department of Radiology, Babol University of Medical Sciences, Babol, Iran
Correspondence: Ahmad Tamadoni, Non-Communicable Pediatric Diseases Research Center, Health Research Institute, Babol University of Medical Sciences, Babol, Iran, Email [email protected] Alborz Ghadirioghani, Department of Medicine and Health Sciences, Babol University of Medical Sciences, Babol, Iran, Email [email protected]
Abstract: A 15-year-old boy diagnosed with acute myeloid leukemia (AML) was readmitted to the hospital with a fever and an atypical lung infection just one day after being discharged following his initial chemotherapy session. The symptoms continued and worsened with time even though multiple levels of antibiotic treatment were tried. It was the typical radiological findings aided in diagnosing the cause and demonstrated to be invasive pulmonary aspergillosis. Furthermore a dramatic response to the standard treatment and positive serum GM test confirmed the diagnosis.
Keywords: febrile neutropenia, invasive pulmonary aspergillosis, pulmonary aspergillosis, acute myeloid leukemia
Introduction
Aspergillosis, primarily caused by the fungus Aspergillus fumigatus, is the most common mold-related infection affecting the lungs. Its clinical manifestations vary widely, mainly influenced by the immune status of the host.1 In patients with asthma or cystic fibrosis, A. fumigatus can trigger allergic bronchopulmonary aspergillosis (ABPA), characterized by hypersensitivity reactions in the lungs.2 Chronic pulmonary aspergillosis, on the other hand, predominantly occurs in individuals who are either immunocompetent or only mildly immunocompromised and often have pre-existing lung diseases such as chronic obstructive pulmonary disease, post-tuberculosis scarring, nontuberculous mycobacterial infections, or lung cancer. Chronic pulmonary aspergillosis can present with a spectrum of overlapping conditions, ranging from isolated aspergillomas (fungal balls in pre-existing lung cavities) to more complex forms such as chronic cavitary, fibrosing, and microinvasive aspergillosis.1,3 A more severe variant of chronic pulmonary aspergillosis, termed subacute invasive aspergillosis (also referred to as semi-invasive or chronic necrotizing aspergillosis), develops as a progressive disease with tissue invasion and necrosis, typically affecting patients who are mildly immunocompromised.4 Acute invasive pulmonary aspergillosis, the most aggressive form, occurs in individuals with significant immune compromise, such as those with hematologic malignancies, chemotherapy-related neutropenia, or those receiving immunosuppressive therapies for autoimmune conditions or following organ transplantation.1 Notably, IPA has recently been observed in intensive care unit (ICU) patients undergoing mechanical ventilation due to severe influenza or COVID-19, including those considered to have an intact immune system.1 While Aspergillus fumigatus is the predominant cause of aspergillosis worldwide, other species such as Aspergillus flavus (more frequent in certain parts of Africa and Asia), Aspergillus terreus, and Aspergillus niger contribute to a smaller proportion of cases. Less commonly, species like Aspergillus nidulans, Aspergillus calidoustus, Aspergillus glaucus, Aspergillus versicolor, and cryptic species such as Aspergillus lentulus and Aspergillus udagawae account for fewer than 3% of cases.1
Diagnosing and managing pulmonary aspergillosis remains challenging due to suboptimal sensitivity and specificity of diagnostic tools, which frequently cause delays in diagnosis and treatment initiation.1 Therapeutic management is further complicated by limited treatment options, significant drug interactions—particularly involving triazole antifungals—adverse effects, and the increasing problem of antifungal resistance.
We present a case of an unusual lung infection in a 15-year-old boy with newly diagnosed acute myeloid leukemia, occurring immediately after his first chemotherapy cycle. This case serves to frame a broader discussion on current diagnostic methodologies, therapeutic strategies, and recent advancements in the management of invasive pulmonary aspergillosis, while also considering future directions for improving patient outcomes.
The patient’s signs and symptoms were common in many other pulmonary infections and clinical symptoms were mild at the beginning and worsened by time. The patient’s radiological findings remained persistent until the best possible treatment was performed. This case presents some highly intriguing radiological findings. Although the imaging is consistent with typical patterns seen in fungal infections, efforts to determine the exact cause of the lung infection were hindered as the patient’s guardians declined the bronchoscopy procedure. However serum GM test was reported positive and confirmed the probable diagnosis of invasive pulmonary aspergillosis. Also a dramatic response to the choice treatment of pulmonary aspergillosis besides the typical radiological findings and positive serum GM made us confident about the exact diagnosis.
Case Report
A 15-year-old boy, recently diagnosed with acute myeloid leukemia (AML), was readmitted to the hospital just one day after being discharged. His diagnosis was confirmed about two weeks before this second hospitalization. During his initial stay, he had undergone his first round of chemotherapy, which included Daunorubicin, Cytarabine, Etoposide, and Intrathecal Cytarabine. One day after his discharge from hospital he developed fever and cough. His fever was unresponsive to acetaminophen and NSAIDs. He was noted to be neutropenic (WBC 400/µL). He was admitted with febrile neutropenia and the following vital signs. Temperature, 38.1°C; heart rate, 97 bpm; Blood Pressure, 110/70 mmHg; Respiratory rate, 23/m. Laboratory tests were taken and treatment began empirically with cefotaxime and GCSF. His admission Chest X-ray revealed consolidation in the left perihilar region (Figure 1).
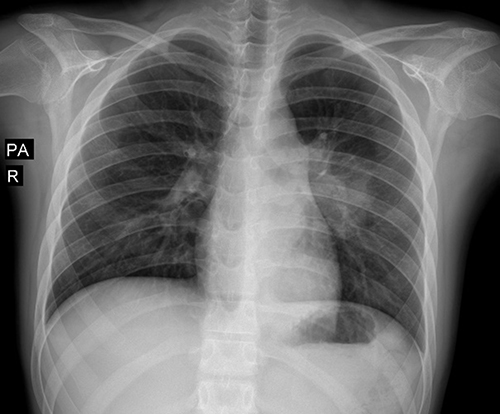 |
Figure 1 Chest X-ray shows a consolidation opacity in the left perihilar region. Additionally, there is mild haziness observed in the middle and lower lobes of the left hemithorax. No overt pleural effusion or pneumothorax is identified. |
After 4 days of treatment he was still febrile so antibiotic changed to meropenem and vancomycin. After 7 days of treatment there was no clinical improvement, so another Chest X-ray was performed to reassess the previous opacity and Liposomal amphotericin B was added to the regimen due to suspicion of fungal infections. In the second Chest X-ray haziness and ground glass opacities were increased in left lung (Figure 2).
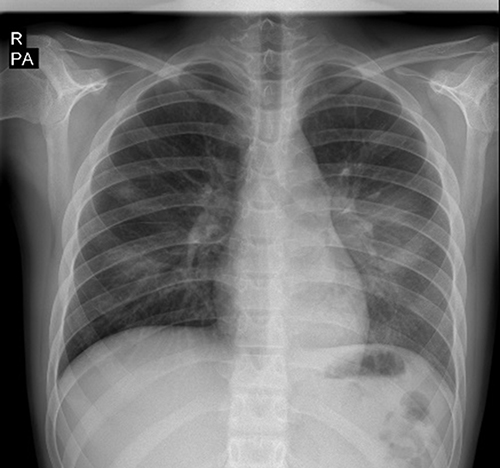 |
Figure 2 Second Chest X-ray demonstrates diffuse haziness and ground-glass opacity in the middle and lower zones of the left lung. Compared to the prior Chest X-ray, there is increased retrocardiac opacity. Additionally, two nodular consolidations are noted in the lower and middle zones of the right hemithorax, which were not previously noted. |
At the 13th day of admission the patient still had no clinical improvement and started to experience respiratory distress. Bilateral lung crackles and skin lesions indicative of a fungal infection were observed and clotrimazole ointment was started. Pulmonary consultation was performed and suggested performing a CT scan and adding oseltamivir and azithromycin to the regimen. CT scan showed consolidation like air space opacity with air bronchogram and ground glass opacity in inferior lobe of left lung, air crescent was seen peripherally to a hypodense area with liquid density suggested necrosis, 6 nodular consolidations with ground glass halo sign around them were seen in both lungs which some of them were cavitary (Figures 3–5). The overall findings were in favor of opportunistic infections, primarily fungal infections, particularly aspergillosis. Among other differential diagnoses with lower probability, pulmonary mucormycosis, Staphylococcal pneumonia and other gram-negative bacteria were considered.
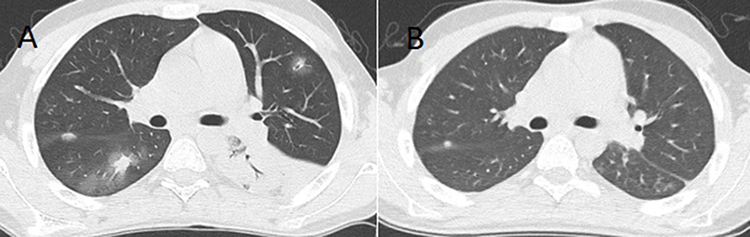 |
Figure 3 Thoracic CT scan parenchymal window. Axial view (A) shows multiple nodular consolidation with peripheral ground glass opacity (halo sign) and alveolar consolidation at left lower lobe. Some nodules show central cavitary change. In view (B), after 4 weeks of treatment almost all the consolidations have been cleared. |
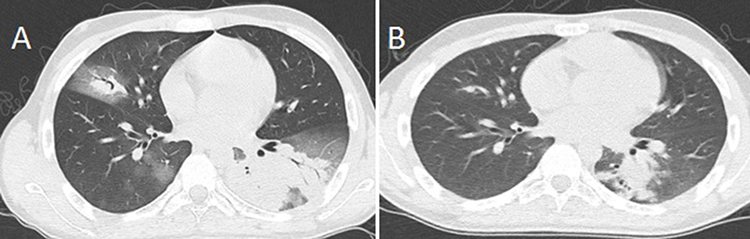 |
Figure 4 In axial view (A), Lung CT shows nodular consolidation with peripheral ground glass halo and central air-crescent in right middle lobe. Also patchy ground glass opacities at right lower lobe and alveolar consolidations with central cavitary changes and peripheral ground glass opacity halo at left lower lobe were noted. In view (B), most of the opacifications are gone and only a part of consolidation opacities in the left lung remained. |
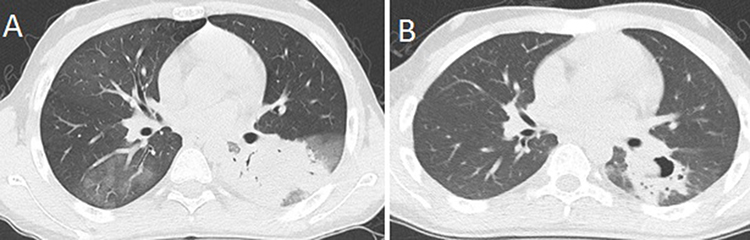 |
Figure 5 Thoracic CT shows ground glass opacifications at right lower lobe and alveolar consolidations with peripheral ground glass halo and central air-crescent at left lower lobe (A). 4 weeks after treatment, most of the opacities have been cleared and central area has been excavated (B). |
After viewing the CT scan, the team decided to start intravenous voriconazole and sent a serum sample for galactomannan testing. Blood cultures (the first test was performed on the day of admission, with a second test following a day 7 chest X-ray) were all negative but serum GM had been reported positive (GM 1.2) which confirmed the probable diagnosis. There was an impressive clinical improvement 3 days after receiving voriconazole. The second serum GM test was reported negative 11 days after the first test (GM 0.4). After 4 weeks of hospitalization the patient was discharged with voriconazole tablets 200 mg twice a day and CT-Scan was repeated 4 weeks after the first CT-Scan (Figures 3–5).
Discussion
Invasive pulmonary aspergillosis is a serious and potentially fatal fungal infection that predominantly targets individuals with weakened immune systems.5 This case report discusses the difficulties encountered in the diagnosis and treatment of IPA, especially when compounded by underlying risk factors like neutropenia and intensive chemotherapy. The patient in this case presented with nonspecific symptoms, including fever and cough which are common in many respiratory conditions, underscoring the diagnostic complexity of IPA.1,6 While histopathological examination and culture of Aspergillus species from respiratory specimens remain the gold standard, these methods are often invasive and may not be feasible in all patients.5,7 Non-invasive diagnostic methods, such as serum galactomannan assay and beta-D-glucan testing, have improved the ability to detect IPA, but false positives and negatives can occur and do not rule out IPA.8–10 Serial Galactomannan testing is advised for early detection and ongoing monitoring of patients with invasive pulmonary aspergillosis. It serves as a valuable prognostic tool for assessing disease progression and evaluating the effectiveness of antifungal therapy.11 The phenomenon of false positivity in the galactomannan assay may be attributed to a multitude of factors. Galactomannan is present in specific fungal and bacterial species, which can lead to erroneous positive results. Cross-reactivity may arise with certain beta-lactam antibiotics and with GM produced by some other fungal taxa, along with various epidemiological and biological factors that contribute to this issue. The ability to detect galactomannan in serum is diminished when mold-active antifungal therapy is administered concurrently. For example, in patients undergoing prophylactic treatment with posaconazole or voriconazole, these therapies may interfere with the circulation of galactomannan.1,12 In comparison between IPA and pulmonary mucormycosis, the halo sign is more indicative in patients with IPA, while the reverse halo sign is more frequently observed in patients with PM. Peribronchial consolidations, clusters of centrilobular nodules, ground-glass opacities, and smooth bronchial wall thickening are more frequently observed in patients with IPA compared to those with pulmonary mucormycosis.13,14 Due to the lack of distinct clinical symptoms and the restricted sensitivity or specificity of radiological and mycological tests, diagnosing IPA is categorized based on a probability scale, ranging from possible to probable and proven cases. The European Organization for Research and Treatment of Cancer and Mycoses Study Group Education and Research Consortium (EORTC-MSGERC) has developed standardized definitions to determine these diagnostic categories specifically for immunocompromised patients.1 According to the EORTC-MSGERC criteria, the diagnosis of IPA is based on four key components. Host factors, identifying immunocompromised patients at risk. Clinical criteria, including specific radiological findings on a CT scan. Mycological evidence, positive laboratory tests, such as GM in serum or bronchoalveolar lavage fluid. Proven infection, definitive proof from positive histopathology or culture, supported by clinical and radiological evidence.1 In this case, the combination of host immunosuppressive condition, radiological findings, such as the halo sign, ground glass opacities and cavitary lesions on CT imaging, along with clinical improvement after starting proper antifungal therapy for IPA and a positive serum GM test provided strong supportive evidence for IPA. However, the absence of histopathological confirmation emphasizes the necessity of maintaining a high level of suspicion in patients with compromised immune systems.1,9 The management of IPA requires a multidisciplinary cooperation, involving antifungal therapy, optimization of immune status, and, in some cases, surgical intervention. Voriconazole serves as the primary treatment option for IPA, supported by Cheng’s meta-analysis demonstrating its superiority over amphotericin B.15 Patients treated with voriconazole showed a higher favorable response rate by week 12, achieving 53% compared to 32% in those treated with amphotericin B. Additionally, the 12-week survival rate was higher for voriconazole patients at 71%, versus 58% for amphotericin B recipients.1,6,9,15,16 However, the azole-resistant Aspergillus strains pose a growing concern, necessitating antifungal susceptibility testing when feasible.5 The standard treatment for PM is liposomal amphotericin B, which did not respond adequately in this case.17 In our case voriconazole response was much better than amphotericin B which strongly supported our diagnosis of IPA. Adjunctive therapies, such as granulocyte transfusions or interferon-gamma, may be considered in refractory cases, although their efficacy remains controversial.5,18
The prognosis of IPA is closely tied to the timeliness of diagnosis and the underlying immune status of the patient.1,19 Delaying the start of antifungal therapy has been linked to a notable increase in mortality rates, highlighting the critical need for prompt diagnosis and timely treatment.1,20 In this case, the patient’s favorable outcome was attributable to the prompt initiation of voriconazole and the gradual recovery of neutrophil counts. However, long-term follow-up is crucial, as relapses can occur, particularly in patients with persistent immunosuppression.1,19 One important point of this case was that the patient was infected just after the first session of chemotherapy showing that every chemotherapy-induced immunosuppression is an opportunity for IPA. This case also shows the importance of preventive strategies in high-risk populations. Antifungal prophylaxis with posaconazole or voriconazole is recommended in patients with prolonged neutropenia or those undergoing hematopoietic stem cell transplantation. Environmental actions, including the application of HEPA (high-efficiency particulate air) filters, can further reduce the risk of Aspergillus exposure in healthcare settings.5
Conclusion
Invasive pulmonary aspergillosis continues to be a significant contributor to morbidity and mortality among immunocompromised individuals. Challenges associated with IPA emphasize the importance of maintaining a high level of suspicion, early initiation of appropriate antifungal therapy and a multidisciplinary approach to management. Febrile neutropenia is a significant risk factor for opportunistic infections, including fungal infections. We recommend CT-Scan in patients who have abnormal CXR or in patients who do not show clinical improvement after three or four days of hospitalization with febrile neutropenia. Also early initiation of combined antifungal therapies should be considered. Radiologists can play a significant role in these cases. They can help in diagnosing and anticipate complications such as air-crescent signs. IPA is angio-invasive and carries a risk of catastrophic bleeding. In cases of suspected angioinvasion or refractory localized aspergillus infection, early surgical interventions should be taken into consideration. Further research should focus on improving diagnostic accuracy and optimizing preventive strategies to reduce the burden of this infection. For such patients multidisciplinary hospital case conferences can be recommended to determine the best treatment strategy and despite the high mortality rate, full recovery is achievable.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
The authors did not use artificial intelligence (AI)-assisted writing tools when preparing this work.
Abbrevations
IPA, invasive pulmonary aspergillosis; WBC, white blood cell count; ANC, absolute neutrophil count; BAL, bronchoalveolar lavage; GM, galactomannan; GCSF, granulocyte colony stimulating factor; CXR, chest x-ray; PM, pulmonary mucormycosis; CT, computed tomography.
Consent and Ethical Approval
Written informed consent was obtained from the patient’s guardian for publication of this case report and any accompanying images. The patient has been informed about the details of the case and has provided approval for the information to be published in this case report. This study was also approved by the ethical committee of Babol University of Medical Sciences and the following number of IR.MUBABOL.HRI.REC.1404.045. The authors confirm that the approval of an institutional review board was not required for this work but it was done in good faith.
Acknowledgments
The authors would like to thank the Clinical Research Development Unit of Amirkola Children’s Hospital, Babol University of Medical Sciences for their collaboration.
Funding
The authors declare that they have not received any financial support for this study.
Disclosure
All authors report no conflicts of interest in this work.
References
1. Lamoth F, Calandra T. Pulmonary aspergillosis: diagnosis and treatment. Eur Respir Rev. 2022;31(166):220114. doi:10.1183/16000617.0114-2022
2. Roboubi A, Audousset C, Fréalle É, et al. Allergic bronchopulmonary aspergillosis: a multidisciplinary review. J Med Mycol. 2023;33(3):101392. doi:10.1016/j.mycmed.2023.101392
3. Zarif A, Thomas A, Vayro A. Chronic pulmonary aspergillosis: a brief review. Yale J Biol Med. 2021;94(4):673. doi:10.1186/s13256-021-02721-9
4. Tamkeviciute L, Tumenas A, Zaveckiene J, et al. Different forms of pulmonary aspergillosis: a pictorial essay. Eur J Radiol. 2024;171:111290. doi:10.1016/j.ejrad.2024.111290
5. Patterson TF, Thompson GR, Denning DW, et al. Practice guidelines for the diagnosis and management of aspergillosis: 2016 update by the Infectious Diseases Society of America. Clinl Infect Dis. 2016;63(4):e1–7. doi:10.1093/cid/ciw326
6. Kousha M, Tadi R, Soubani A. Pulmonary aspergillosis: a clinical review. Eur Respir Rev. 2011;20(121):156–174. doi:10.1183/09059180.00001011
7. Jensen HE, Becker CB. Pathological diagnosis of pulmonary aspergillosis. In: Seminars in Respiratory and Critical Care Medicine. Thieme Medical Publishers, Inc; 2024.
8. Tong T, Xu Y. Serum galactomannan for diagnosing invasive aspergillosis in pediatric patients: a meta-analysis. Microb Pathogenesis. 2018;118:347–356. doi:10.1016/j.micpath.2018.03.059
9. Aljutaily HI, Al-Shamrani A. Invasive pulmonary aspergillosis in children: a case report and literature review. Am J Case Rep. 2022;23:e935971. doi:10.12659/AJCR.935971
10. Bukkems LM, van Dommelen L, Regis M, et al. The use of galactomannan antigen assays for the diagnosis of invasive pulmonary aspergillosis in the hematological patient: a systematic review and meta-analysis. J Fungi. 2023;9(6):674. doi:10.3390/jof9060674
11. Koo S, Bryar JM, Baden LR, et al. Prognostic features of galactomannan antigenemia in galactomannan-positive invasive aspergillosis. J Clin Microbiol. 2010;48(4):1255–1260. doi:10.1128/JCM.02281-09
12. Avcu G, Karapinar DY. A review of a diagnostic tool: galactomannan. J Immunol Sci. 2018;2(4).
13. Jung J, Kim MY, Lee HJ, et al. Comparison of computed tomographic findings in pulmonary mucormycosis and invasive pulmonary aspergillosis. Clin Microbiol Infect. 2015;21(7):684.e11–684.e18. doi:10.1016/j.cmi.2015.03.019
14. Jang HM, Kim MY, Lim SY, et al. CT findings for differentiating pulmonary mucormycosis from invasive pulmonary aspergillosis, prior to invasive procedure such as a biopsy or surgery: a 22‐year single‐center experience. Mycoses. 2025;68(9):e70115. doi:10.1111/myc.70115
15. Cheng J, Han H, Kang W, et al. Comparison of antifungal drugs in the treatment of invasive pulmonary aspergillosis: a systematic review and network meta-analysis. Front Microbiol. 2024;15:1504826. doi:10.3389/fmicb.2024.1504826
16. Herbrecht R, Denning DW, Patterson TF, et al. Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis. N Engl J Med. 2002;347(6):408–415. doi:10.1056/NEJMoa020191
17. Cornely OA, Alastruey-Izquierdo A, Arenz D, et al. Global guideline for the diagnosis and management of mucormycosis: an initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium. Lancet Infect Dis. 2019;19(12):e405–e421. doi:10.1016/S1473-3099(19)30312-3
18. Stewart AG, Baidya S, Daly J, et al. Prolonged granulocyte transfusions sourced from buffy coats used to treat Aspergillus spp. infection in chronic granulomatous disease. Pathology. 2022;54(3):358–361. doi:10.1016/j.pathol.2021.05.098
19. Segal BH, Walsh TJ. Current approaches to diagnosis and treatment of invasive aspergillosis. Am J Respir Crit Care Med. 2006;173(7):707–717. doi:10.1164/rccm.200505-727SO
20. Maertens JA, Raad II, Marr KA, et al. Isavuconazole versus voriconazole for primary treatment of invasive mould disease caused by Aspergillus and other filamentous fungi (SECURE): a Phase 3, randomised-controlled, non-inferiority trial. Lancet. 2016;387(10020):760–769. doi:10.1016/S0140-6736(15)01159-9
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.