Back to Journals » International Medical Case Reports Journal » Volume 18
Pulmonary Air Embolism Caused by an Air Turbine During Oral Surgery Under General Anesthesia: A Case Report
Authors Abe S, Wakamatsu K ![]() , Takahashi K
, Takahashi K ![]() , Sato H
, Sato H ![]() , Yoshida K
, Yoshida K ![]() , Yamazaki S, Kawaai H
, Yamazaki S, Kawaai H ![]()
Received 24 June 2025
Accepted for publication 21 October 2025
Published 7 November 2025 Volume 2025:18 Pages 1439—1446
DOI https://doi.org/10.2147/IMCRJ.S547085
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Shota Abe, Keiichiro Wakamatsu, Koji Takahashi, Hikaru Sato, Kenji Yoshida, Shinya Yamazaki, Hiroyoshi Kawaai
Department of Dental Anesthesiology, Ohu University, School of Dentistry, Koriyama, Fukushima, Japan
Correspondence: Hiroyoshi Kawaai, Department of Dental Anesthesiology, Ohu University, School of Dentistry, 31-1 Misumido, Tomita, Koriyama, Fukushima, 963-861, Japan, Tel/Fax +81-24-932-9337, Email [email protected]
Background: In clinical scenarios like wisdom tooth extractions, compressed air may infiltrate tissue gaps or venous vessels. We observed a patient who developed a pulmonary air embolism secondary to subcutaneous emphysema (SE) during a wisdom tooth extraction performed with an air turbine. The patient required immediate cardiopulmonary resuscitation (CPR) and was successfully revived from pulseless electrical activity (PEA).
Case Description: This case was a 47-year-old female, and upper and lower pericoronitis on the right side and multiple dental caries were noted. Due to her intellectual disabilities (ID), so the extraction of the upper and lower right wisdom teeth was scheduled under general anesthesia. At approximately 10 minutes after starting the oral surgery, the monitor showed plethysmograph and the end-tidal carbon dioxide (ETCO2) waveform disappeared following the sudden drop in SpO2. Based on these findings, cardiopulmonary arrest (CPA) was diagnosed, and PEA was confirmed on the ECG. CPR was immediately initiated on the dental unit. However, because the dental unit remained in a supine position, it sank with each chest compression. To stabilize the surface and prevent vertical movement, a dental chair was placed under the backrest of the dental unit. Approximately 3 minutes after starting CPR, the SpO2 plethysmograph reappeared on the monitor during artificial ventilation. A CT scan was performed, and she was diagnosed pulmonary air embolism resulting from SE caused by the use of an air turbine with compressed air.
Conclusion: This case highlights that SE can easily occur when using an air turbine with compressed air in dental procedures. In severe instances, an air embolism resulting from SE may lead to CPA. Therefore, caution is needed when using dental instruments and drills that utilized compressed air during dental procedures.
Keywords: pulmonary air embolism, air-turbine, pulseless electrical activity, PEA, subcutaneous emphysema, SE, oral surgery
Introduction
Complications that may arise during dental procedure include vasovagal reflex, hyperventilation, and drug allergies.1 Common therapeutic devices used in these procedures include air turbine, electric motor-powered handpieces, and CO2 laser. Among these instruments, air turbine -a high-speed drilling tool powered by compressed air— is frequently used in routine dental care. However, compressed air from the air turbine can sometimes be forced into soft tissue spaces, leading to subcutaneous emphysema (SE).2–5 In terms of the incidence of SE, Jones et al5 investigated 180 reports of iatrogenic SE of dental origin, from which 135 cases with sufficient details were extracted. The majority cases (51.1%) resulted from the use of an air-driven dental handpiece following disruption of the oral mucosa. In the severe cases, this compressed air may spread through soft tissues into the mediastinum, and if the air is contaminated, it may lead to infection in the mediastinum, resulting in a serious complication such as mediastinitis.6–8 Additionally, there is a potential for a dose-dependent response if the compressed air enters the venous blood vessels.9
For patients with intellectual disabilities (ID), cooperation during dental treatment is often unfeasible, making general anesthesia necessary. In such procedures, air turbines are commonly employed, and depending on the specific treatment, compressed air may be forced into tissue spaces. This is particularly relevant in the extraction of wisdom teeth, which are frequently impacted and require sectioning with an air turbine. In clinical practice like wisdom tooth extractions, compressed may infiltrate tissue gaps or venous vessels.
We experimented a patient who developed a pulmonary air embolism secondary to SE during a wisdom tooth extraction performed with air turbine. The patient required immediate cardiopulmonary resuscitation (CPR) and able to be saved from pulseless electrical activity (PEA).
In the present case report, the patient has intellectual disability and is unable to give consent to us. So, we obtained the informed consent from the guardians of patient and we did not need institutional approval. Moreover, the guardians and her brother understand that we submitted this case report, and they want us to publish this case report for the safety management in Dentistry.
Case Description
A patient was 47-years-old female with a height of 154cm and a weight of 43kg (BMI 18.1). She was diagnosed with mental retardation (IQ 30) at the age of 3 and developed during her elementary school. At the age of 39, she sustained a traumatic subarachnoid hemorrhage after falling down due to a collision with another individual at her nursing facility. She was able to walk slowly, feed herself, and manage toileting independently but required assistance with bathing and dressing in terms of daily living activities. Her daily oral medications included eszopiclone, ramelteon, lubiprostone, and sodium ferrous citrate. Blood test, chest X-ray (Figure 1), and electrocardiogram (ECG) results showed no abnormalities.
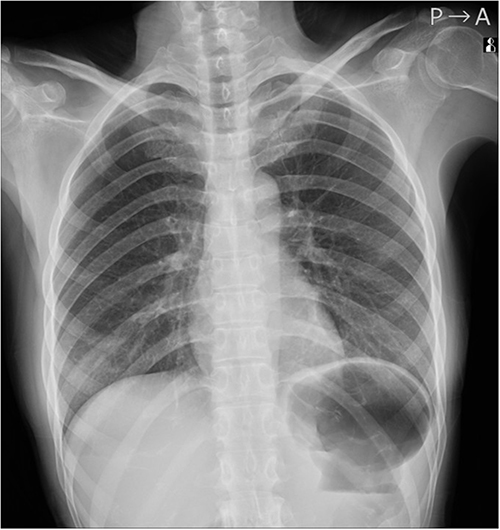 |
Figure 1 Preoperative chest X-ray in the present case. The lung fields were bilaterally clear without normal shadows detected. |
She presented to our hospital in October 2022 with right cheek swelling. During the initial examination, upper and lower pericoronitis on the right side and multiple dental caries were noted (Figure 2). Due to her ID, she was unable to undergo dental treatment while conscious, so the procedure was scheduled under general anesthesia. Her first general anesthesia was performed using propofol and remifentanil, with no complications observed during and after the procedure.
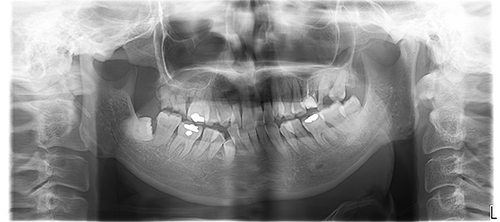 |
Figure 2 Panoramic tomography in the present case. A panoramic tomography was taken during the initial visit. The preoperative examination revealed lower pericoronitis on the right side and multiple caries in her mouth. |
The second general anesthesia was scheduled for the extraction of the upper and lower right wisdom teeth. After establishing intravenous access, general anesthesia (Figure 3) was induced using propofol and remifentanil followed by nasal tracheal intubation via the nasal cavity with 4% lidocaine sprayed around the larynx (without the use of a muscle relaxant). Antibiotic infusion was initiated prior to the surgery. A total dose of 2% lidocaine with 1/80,000 epinephrine was administered around the upper and lower right wisdom teeth, after which the extraction of the lower wisdom tooth began. Approximately 10 minutes into the extraction using the air turbine, the patient’s percutaneous oxygen saturation (SpO2) suddenly dropped to 82%, prompting immediate order to suspend the procedure. Rocuronium 20 mg was administered due to suspicion of a lead pipe phenomenon associated with the drop in SpO2. She was immediately ventilated with 100% oxygen, her SpO2 rose to above 90%. The blood pressure (BP) in the monitor showed a reading of 60/16 mmHg. While administering 4mg of ephedrine and 0.2mg of phenylephrine was being instructed, chest auscultation was performed. Breath sounds were clearly audible, and chest movement was observed on both sides without any noticeable asymmetry. However, cyanosis was observed on her face and lips, and the monitor showed no plethysmograph on the SpO2 reading. Simultaneously, the radial artery pulse was not palpable, and SpO2 could no longer be measured. In addition, the end tidal carbon dioxide (ETCO2) waveform disappeared following the sudden drop in SpO2. The monitor also indicated that BP could not be measured. Based on these findings, cardiopulmonary arrest (CPA) was diagnosed, and PEA was confirmed on the ECG. CPR was immediately initiated on the dental unit. However, because the dental unit remained in a supine position, it sank with each chest compression. To stabilize the surface and prevent vertical movement, a dental chair was placed under the backrest of the dental unit. Subsequently, the previously instructed dose of ephedrine 4 mg and phenylephrine 0.2 mg (ordered before CPA) were administered while preparations were made to administer 1 mg of epinephrine. Approximately 3 minutes after starting CPR, the SpO2 plethysmograph reappeared on the monitor during artificial ventilation. The carotid pulse was then assessed, and a pulse was detected in the common carotid artery. Simultaneously, the monitor showed a BP of 110/50 mmHg. Moreover, the ETCO2 waveform was able to be observed and BP was able to be measured continuously. Infusions of remifentanil and propofol were resumed, and a continuous infusion of nicorandil at 3 mg/h was started due to ST depression observed on the ECG.
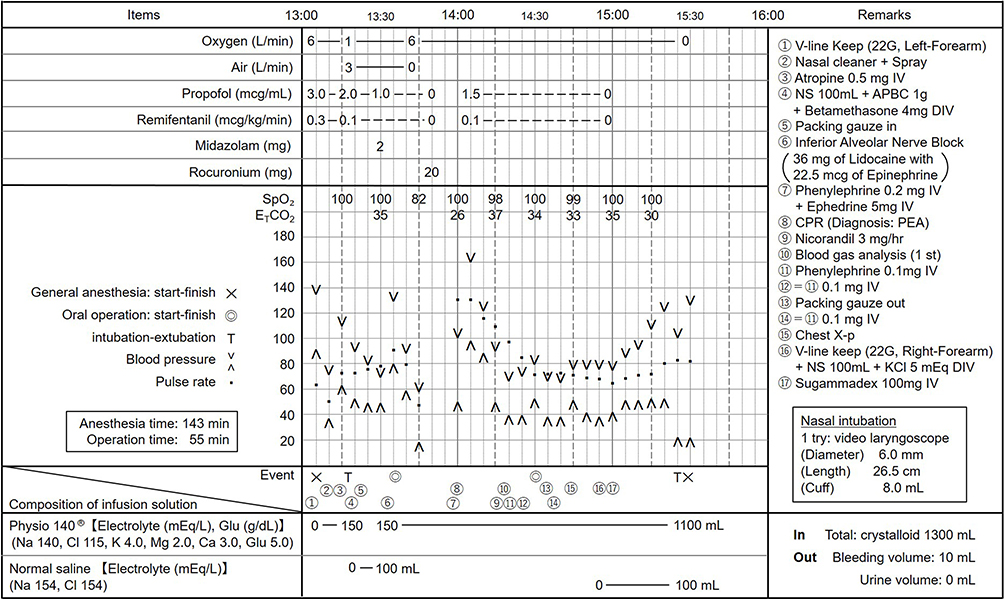 |
Figure 3 Second general anesthesia record. The SpO2 and ETCO2 waveforms were absent during oral surgery for approximately 10–15 minutes after the procedure began. |
After the oral surgeons sutured the area around the lower wisdom tooth, swelling was observed on the right side of her face. When the facial tapes were removed, the appearance looked like SE. Blood gas analyses conducted at 15minutes, 35minutes, and 3hours after the return of spontaneous circulation (ROSC) are presented in Table 1. A chest X-ray (Figure 4) was taken 35 minutes after the ROSC. The blood gas analyses at 15 and 35minutes post-ROSC revealed hypokalemia, prompting the insertion of additional intravenous line and the initiation of treatment for hypokalemia. Approximately 80 minutes after ROSC, extubation was performed following the administration of 100 mg of sugammadex, as the patient had regained full consciousness. After returning to the ward, extensive swelling was noted from the right facial area to the left cervical region (Figure 5). However, due to the unclear of cause of CPA, she was transferred to another facility, referred to as I-hospital, about 9 hours after ROSC. At I-hospital, SE was confirmed in the right facial area extending to the left cervical region, and significant emphysema was identified in the mediastinal space on computed tomography (CT). I-hospital suspected that the SE and mediastinal emphysema were caused by the airway mucosal damage due to the nasal intubation and determined that case exceeded their capacity for management. Consequently, she was transferred back to N-hospital. A CT scan was performed at N-hospital (Figure 6) and the ICU there diagnosed her with pulmonary air embolism resulting from SE by caused by an air-turbine with compressed air. Following the diagnosis, antibiotics were administered to prevent infection. A follow-up CT scan taken on the fourth postoperative day at N-hospital showed that the SE from the right facial area to the left cervical region and the emphysema in the mediastinal space had resolved.
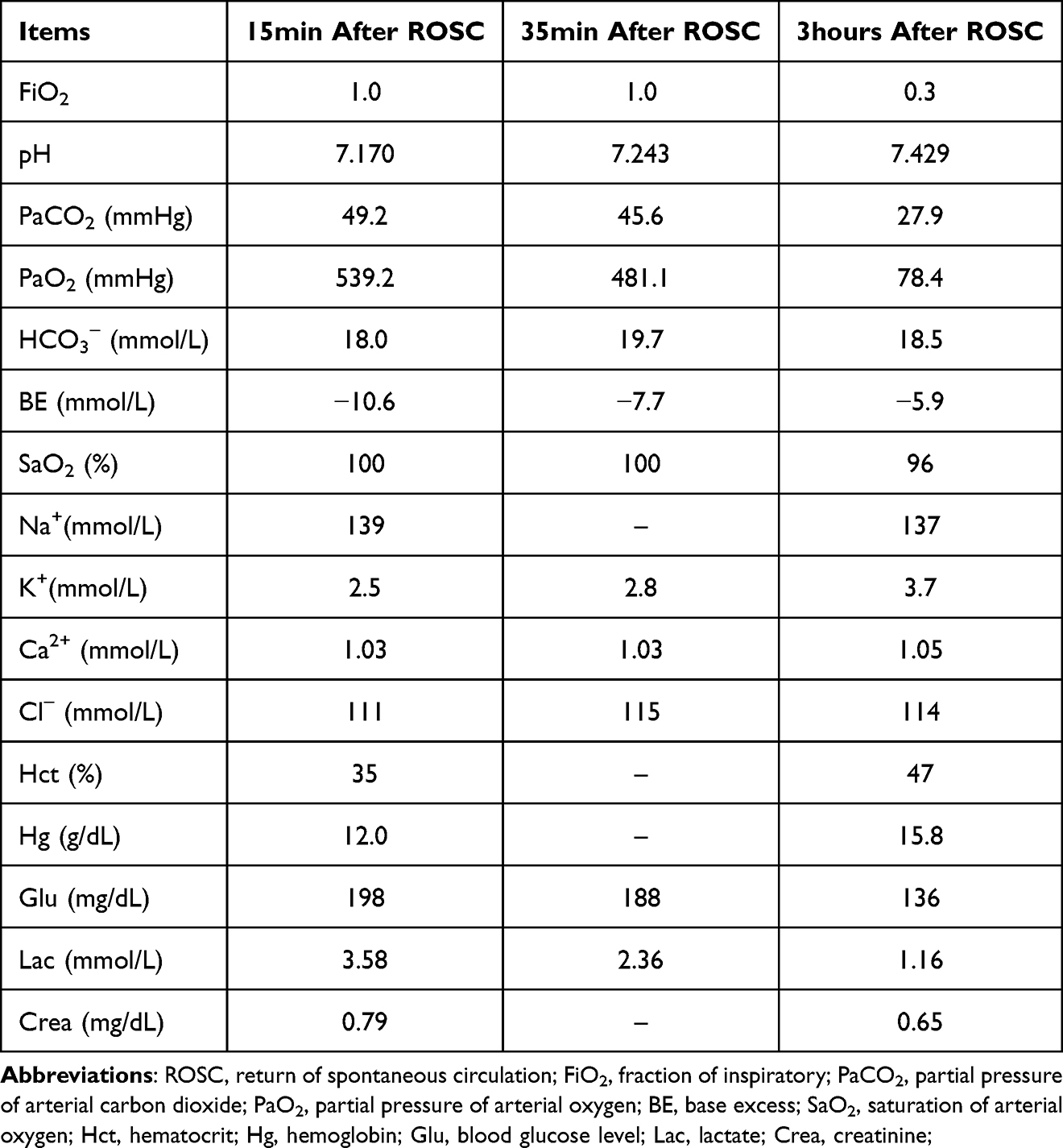 |
Table 1 The Acidosis Due to CPA Was Improved Between 15 minutes and 3 hours After ROSC |
 |
Figure 4 Chest X-ray taken at 35 minutes after the ROSC. The chest X-ray taken at 35 minutes after the ROSC showed no evidence of complications such as heart failure or pneumothorax. |
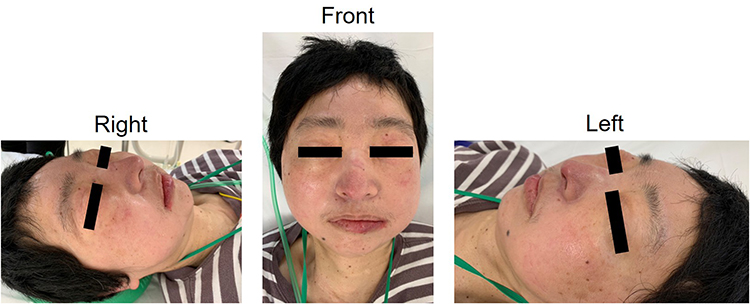 |
Figure 5 Facial appearance of the patient after extubation following ROSC. Facial photographs obtained after extubation, showing swelling from the cheek to the neck in right, front, and left views. |
 |
Figure 6 Horizontal (a) and frontal (b) images of the neck and chest. A CT scan of the neck and chest was performed after the patient was transferred to the N-hospital. Both images (a and b) from the CT scan show SE in the neck and emphysema in the mediastinal space. The space outlined in yellow was filled with compressed air from the air turbine and was widely observed around the neck. |
Discussion
In reports of deaths associated with dental treatment, the number of fatal cases related to general anesthesia, and sedation medications exceed those related to cardiovascular events, airway obstruction, and infection diseases.10 As a result, dental anesthesiologists are more likely to encounter clinical cases. In contrast to these findings, reports from Japan have indicated that severe complications associated with dental procedures often arise during or after the administration of local anesthesia.11 Furthermore, Miyakoshi et al11 reported that life-threatening complications such as heart failure, cerebrovascular events, and anaphylactic shock more likely to occur within 30 minutes following local anesthesia.12 However, the present case was not associated with local anesthesia. As a related incident case, Magni et al13 reported a case where a patient developed SE after the extraction of four wisdom teeth and subsequently entered a comatose state accompanied by seizures postoperatively. In another case, Parekh et al14 described a patient who developed cervicofacial and mediastinal emphysema following the use of an air syringe during root canal treatment. In comparison with these cases, our case is rare in that air embolism was caused by the compressed air from air turbine, and additionally, CPA occurred.
From the perspective of pathogenic mechanism, most of cases of pulmonary air embolism have been reported in association with central venous catheter use, as well as procedure such as head and neck surgery, laparoscopic surgery, cesarean section, and total hip replacement.9 In the present case, SpO2 dropped suddenly within a few minutes after the start of the procedure, and the ETCO2 waveform disappeared at the same time. A muscle relaxant was administered due to suspicion of a lead pipe phenomenon. However, lung auscultation revealed no abnormalities on either side. These sighs were similar to those seen in pulmonary thromboembolism. The patient had received ambulatory anesthesia prior to surgery. Moreover, dehydration was unlikely, adequate intake was maintained during general anesthesia, and the first general anesthesia had been completed without any complications. Based on these factors, the probability of pulmonary thromboembolism was considered to be low.
After ROSC, swelling and SE extending from the right side on the face to the left side of the neck were observed when the facial tapes were removed. At that time, diagnosis of pulmonary air embolism had not yet been made. It was determined that her CPA was due to pulmonary air embolism after CT imaging was performed at N-hospital. The CT findings imaged confirmed that the symptoms were not a result of airway mucosal damage. Additionally, nasal intubation at our hospital had been performed smoothly without the use of stylet. Based on these factors, the possibility that the pulmonary air embolism was caused by mucosal damage during nasal intubation was ruled out.
Analyzing the mechanism of pathogenesis, this case suggested that the air embolism was caused by a large volume of compressed air. Upon further consideration, it was recognized that during the extraction of wisdom tooth, a gum is typically elevated, allowing compressed air from air turbine to enter the soft tissue spaces between the gum flap and mandibular bone. It is believed that the large volume of compressed air then spread from the right side of the face in to the left side of the neck and into the mediastinal space via the soft tissue. During this process, small venous blood vessels within the soft tissue were raptured, following the compressed air to be absorbed into venous blood vessel system. The absorbed air traveled through the superior vena cava, right atrium, and right ventricle, ultimately accumulating in a wide area of pulmonary arteries. As a result, blood flow within the pulmonary arteries became stagnant. This led to reduced blood return to left atrium and ventricle, causing a decrease in cardiac output. Consequently, circulatory collapse occurred, resulting in PEA.
Clinical symptoms vary depending on the volume of air that enters the venous blood vessels. In terms of classification, when volume of air in the venous circulation is less than 0.5 mL/kg, the ETCO2 waveform disappears; when the volume ranges from 0.5 mL/kg to 2.0 mL/kg, hypotension and ischemic changes on ECG are observed; when it exceeds 2.0 mL/kg, circulatory failure occurs.9 The present case falls into the severe category, as it involved disappearance of the ETCO2 waveform, ischemic changes on ECG, and circulatory failure.
One factor contributing to her successful resuscitation without any sequelae was the early recognition of CPA and prompt initiation of chest compressions. According to a report by Nguyen et al15 survival to hospital discharge was 22.4% when bystander CPR was started within 1 minute of cardiac arrest, but this rate dropped to 10.5% when CPR was delayed beyond 10 minutes. This underscores the importance of initiating CPR immediately if the carotid pulse is not palpable. Another contributing factor to her recovery may have been that the air trapped in the pulmonary arteries was broken into small bubbles by chest compressions, allowing blood flow in the pulmonary arteries to resume and cardiac output to be adequately maintained.
This case suggests that CPA could occur during wisdom tooth extractions under awareness, as air turbines are commonly used in dental procedures performed with the patient conscious. Patients with ID are unable to understand or communicate effectively with the dentist, as cannot respond to questions during dental treatment when awareness. If the patient in this case had undergone wisdom tooth extraction under awareness, the recognition of CPA would likely have been delayed. In contrast, the patient in this case was intubated nasally and monitored with ECG, ETCO2, and SpO2. Because general anesthesia was used, medications could be administered promptly in response to any complications. As a result, CPA was detected earlier during general anesthesia than it might have been during a dental procedure under awareness in patients with ID. This early detection is likely why the patient in this case was successfully resuscitated. However, pulmonary air embolism could not be diagnosed in the actual clinical situation, and no alternative approach was available, therefore, resuscitation was initiated according to the PEA algorithm in the American Heart Association (AHA) advanced cardiovascular life support (ACLS) guidelines, as this was feasible approach.
In general, emergency treatments related to dental procedures are carried out in the dental unit, so CPR would begin there in the worst-case scenario. In Chest compressions may need to be performed in the dental unit, depending on the situation. In this case, a dental chair was placed under the backrest of the dental unit to prevent excessive movement during chest compressions. The dental chair helped stabilize the backrest minimizing any swaying. While this may seem like a minor detail, placing the dental chair under the backrest of the dental unit proved to be effective for supporting chest compressions.16
Conclusion
We presented a case of CPA in which a patient developed pulmonary air embolism during tooth extraction under general anesthesia. This case highlights that SE can easily occur when using air turbine with compressed air in dental procedures. In severe instances, an air embolism caused by SE may lead to CPA. Therefore, caution is needed when using dental instruments and drills that utilized compressed air during dental procedures.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Matsuura H. Analysis of systemic complications and deaths during dental treatment in Japan. Anesth Prog. 1989;36(4–5):223–225.
2. Kost M. Thoracic complications associated with utilization of the air turbine dental drill. AANA J. 1996;64(3):288–292.
3. Zemann W, Feichtinger M, Karcher H. Cervicofacial and mediastinal emphysema after crown preparation: a rare complication. Int J Prosthodont. 2007;20(2):143–144.
4. Tan S, Nikolarakos D. Subcutaneous emphysema secondary to dental extraction: a case report. Aust Dent J. 2017;62(1):95–97. doi:10.1111/adj.12464
5. Jones A, Stagnell S, Renton T, Aggarwal VR, Moore R. Causes of subcutaneous emphysema following dental procedures: a systematic review of cases 1993-2020. Br Dent J. 2021;231(8):493–500. doi:10.1038/s41415-021-3564-0
6. Durukan P, Salt O, Ozkan S, Durukan B, Kavalci C. Cervicofacial emphysema and pneumomediastinum after a high-speed air drill endodontic treatment procedure. Am J Emerg Med. 2012;30(9):2095.e3–6. doi:10.1016/j.ajem.2012.01.006
7. Nożewski JB, Dura ML, Kłopocka M, Kwiatkowska MM, Konieczny JP, Nicpoń-Nożewska KK. A 39-year-old woman with cervicofacial and mediastinal emphysema 10 hours after an elective lower molar dental extraction. Am J Case Rep. 2021;5(22):e931793. doi:10.12659/AJCR.931793
8. Ye LY, Wang LF, Gao JX. Pneumomediastinum and subcutaneous emphysema secondary to dental extraction: two case reports. World J Clin Cases. 2022;10(27):9904–9910. doi:10.12998/wjcc.v10.i27.9904
9. Mirski MA, Lele AV, Fitzsimmons L, Toung TJ, Warltier D. Diagnosis and treatment of vascular air embolism. Anesthesiology. 2007;106(1):164–177. doi:10.1097/00000542-200701000-00026
10. Reuter NG, Westgate PM, Ingram M, Miller CS. Death related to dental treatment: a systematic review. Oral Surg Oral Med Oral Pathol Oral Radiol. 2017;123(2):194–204.e10. doi:10.1016/j.oooo.2016.10.015
11. Miyakoshi M, Sato J, Wada M, et al. Possible cases of dental treatment-associated death under local anesthesia in Japan: a review of the literature. J Oral and Maxillofac Surg Med Pathol. 2017;29(4):289–294. doi:10.1016/j.ajoms.2017.02.005
12. Kimura Y, Tonami K, Toyofuku A, Nitta H. Analysis of incident reports of a dental university hospital. Int J Environ Res Public Health. 2021;18(16):8350. doi:10.3390/ijerph18168350
13. Magni G, Imperiale C, Rosa G, Favaro R. Nonfatal cerebral air embolism after dental surgery. Anesth Analg. 2008;106(1):249–251. doi:10.1213/01.ane.0000289634.24785.04
14. Parekh A, McCormick J, Hussain-Amin A, Barnosky B, Edwards M. A case of cardiac arrest caused by air embolism from routine root canal procedure. Methodist DeBakey Cardiovasc J. 2022;18(1):68–72. doi:10.14797/mdcvj.1067
15. Nguyen DD, Spertus JA, Kennedy KF. Association between delays in time to bystander CPR and survival for witnessed cardiac arrest in the United States. Circ Cardiovasc Qual Outcomes. 2024;17(2):e010116. doi:10.1161/CIRCOUTCOMES.123.010116
16. Hitosugi T, Awata N, Miki Y, Tsukamoto M, Yokoyama T. A comparison of two stool positions for stabilizing a dental chair during CPR. Anesth Prog. 2022;69(2):11–16. doi:10.2344/anpr-68-03-13
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.